
Abstract
Background and Purpose. The use of virtual reality (VR) therapy among individuals with spinal cord injury (SCI) is a relatively new rehabilitation approach replicating real-life scenarios. The aim of this study was to evaluate the effectiveness of VR therapy for improving gait and balance in individuals with SCI. Methods. Databases of PubMed, Web of Science, Scopus, SportDiscuss, and CINHAL were searched from inception until September 2019. Two independent reviewers screened articles for inclusion, extracted data, and evaluated methodological quality of the trials. Results. Ten trials, including 3 randomized clinical trials (RCTs) and 7 pre-post trials, with a total of 149 participants were analyzed. Meta-analysis of RCTs demonstrated significant improvement in sitting balance (standardized mean difference [SMD] = 1.65; 95% CI 1.21-2.09; P < .01) after VR therapy with conventional rehabilitation compared with only conventional rehabilitation. Also, pre-post studies using VR therapy without a control group showed improvement in standing balance (Berg Balance Scale, MD = 4.22; 95% CI 1.78-6.66; P < .01 and Activities-specific Balance Confidence scale, MD = 8.53; 95% CI 2.52-14.53; P = .01) and a trend for improvement in gait (SMD = 0.34; 95% CI 0.02-0.66; P = .04). Conclusion. This study demonstrated the beneficial effects of VR therapy to enhance sitting and standing balance and showed a trend of gait improvement in individuals with SCI. This conclusion is based on mainly preliminary data and therefore, more RCTs are needed to confirm the effects of the use of VR in individuals with SCI.
Introduction
Many individuals with spinal cord injury (SCI) present with complete or incomplete injury of any portion of the spinal cord leading to motor and sensory impairments, activity limitations, and reduced community participation. Approximately 60% of individuals living with SCI sustain incomplete damage to the spinal cord as a result of trauma or infection 1 and have the potential to recover important functions such as gait and balance, depending on the level of injury. Walking movement and trunk stability were rated as 2 of the top 5 priorities of functional recovery among individuals with SCI independent of the level of injury.2,3 Also, a recent study reported that mobility training may help optimize quality of life 1 year following an SCI. 4 Gait and balance rehabilitation therefore represent an important aspect of rehabilitative programs in individuals with SCI.
Recovery of functional balance and gait in SCI highly depends on the demographics of the individual and the characteristics of the neurologic impairment. Walking recovery is limited in individuals with complete sensory and motor spinal cord lesions. In cases of incomplete injury of the spinal cord, however, the likelihood of walking recovery is higher. 5 Similarly, the possibilities of achieving functional walking ability decrease as the individual gets older. 5 Additionally, functional balance recovery is a strong predictor of walking ability in individuals with incomplete SCI. 6
Recovery is also influenced by the rehabilitation process. A study showed that the amount of therapy measured by the total hours and intensity of therapy per week may have an impact on motor functional change and outcome measures in individuals with SCI. 7 Challenging individuals with SCI to walk faster and longer by working on their walking endurance might result in improving walking capacity outcomes such as distance, number of strides, and speed. 8 However, this long-term process in clinical settings is difficult, tedious, and resource-intensive for physical therapists and individuals with SCI.
In recent years, technological advances such as virtual reality (VR) have been introduced in the field of SCI rehabilitation and are being used as a therapeutic tool. VR is a computer-based technology that allows users to interact in a computer-generated environment. The simulated environment provided by VR allows individuals to practice rehabilitation exercises in a safe, standardized, reproducible, and controlled environment.
Depending on the level of immersion, VR can be classified into 3 general categories: non-immersive, semi-immersive, and immersive. 9 Non-immersive VR displays a virtual image onto a screen or a wall in front of a person while semi-immersive VR displays a real image, providing more informative content. Highest immersion is obtained using a head-mounted display that blocks view of the external environment and allows the user to get totally immersed in a 3-dimensional virtual environment. The use of VR therapy can be considered an additional therapeutic tool that helps practitioners provide external feedback to their patients about their performance and increase their motivation in adhering to intensive and repetitive exercise training. 10
Previous systematic reviews showed positive effects of VR therapy on balance and walking ability in other neurological populations such as stroke,11-13 multiple sclerosis,14,15 and Parkinson’s disease.16,17 Also, a recent structured review reported positive effects of VR therapy on mobility in individuals with SCI. 18 However, no study has systematically reviewed the effect of VR therapy on gait and balance among individuals with SCI. Since gait and balance rehabilitation is challenging, a synthesis of the evidence of VR intervention on gait and balance may enhance evidence-based practice of VR therapy in individuals with SCI. VR therapy may also constitute an additional treatment option to assist rehabilitation professionals such as physical therapists and occupational therapists to enlarge their scope of action in the provision of care. Therefore, the main objective of this systematic review and meta-analysis was to evaluate and synthesize the effects of VR therapy on gait and balance rehabilitation among individuals with SCI.
Methods
Protocol and Registration
The systematic review and meta-analysis were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 19 The study was registered with the International Prospective Registry of Systematic Reviews (PROSPERO): CRD 42019139316.
Data Sources and Search Strategy
This systematic review was based on a literature search using the databases: PubMed, Web of Science, Scopus, SportDiscuss, and CINHAL. We searched for articles published from inception up to September 2019, using a combination of the keywords “spinal cord injury,” “paraplegia,” “tetraplegia,” “virtual reality,” “gaming,” “postural gaming,” “gait,” “walking,” locomotion,” “ambulation,” “walking speed,” “velocity,” “spatiotemporal parameters,” “postural balance,” “postural stability,” “postural equilibrium,” “postural instability,” “somatosensory impairment,” “sensory changes,” “dynamic stability,” “dynamic control,” and “postural impairment.” The PubMed database was searched using the corresponding MeSH terms. The searches were adjusted according to each database and filters were used to exclude animal studies and reviews. Supplementary Appendix 1 shows the full search strategy used for each database.
Two authors (VDM) and (RY) independently screened the titles and abstracts to identify a list of potential articles investigating VR therapy on gait and balance in individuals with SCI. Full text articles were then screened based on the eligibility criteria to identify trials for this review. A manual search in the reference lists (forward and backward searches) of selected articles was conducted to identify other relevant studies. Any disagreements were resolved through discussion until a consensus was reached with a third author (LA).
Eligibility Criteria
A framework based on the Participants, Interventions, Comparisons, Outcomes, and Study designs (PICOS) was adopted to define the inclusion and exclusion criteria.
Participants
We included studies involving adults (≥18 years old) with a traumatic or nontraumatic SCI, regardless of the time since injury, level of injury, and completeness of injury. Studies in which individuals with SCI were compared with able-bodied participants were also included, but only data collected from individuals with SCI were analyzed. We excluded studies where individuals with SCI were treated together with other neurological populations.
Interventions
We included studies examining any type of VR (immersive, semi-immersive, or non-immersive) or a combination of physical therapy intervention with VR administered with or without biofeedback. This included gait training, such as robotic, overground, and bodyweight-supported treadmill, and general exercises, such as home-based exercise programs with VR. We excluded studies investigating the effectiveness of non–physical therapy (PT) treatments, such as deep brain stimulation and drug therapies.
Comparisons
We included studies comparing:
VR therapy versus conventional PT intervention (eg, conventional rehabilitation balance training) or no intervention.
VR therapy + conventional PT intervention versus conventional PT intervention only (eg, VR therapy + conventional rehabilitation balance training versus conventional rehabilitation balance training)
Pre-post VR therapy (before and after)
We considered conventional PT interventions as any standardized exercises applied by a physical therapist that encouraged sitting or standing balance and gait training as well as exercises for strengthening and/or stretching musculature.
Outcomes
We were interested in gait and balance (sitting and standing) outcome measures. Gait was defined as locomotion following a specific pattern achieved through movement of lower limbs with or without an assistive device. 20 Outcome measures suitable to measure the construct gait in individuals with SCI include Walking Index for SCI II (WISCI II), the 10-Meters Walking Test (10 MWT), gait speed, spatiotemporal gait parameters. 20 Balance was defined as the ability of an individual to maintain stability in sitting or standing position within the limits of the base of support during static or weight shifting activities. 21 Outcome measures suitable to measure the construct balance in individuals with SCI include the Berg Balance Scale (BBS), the Activity Balance Confidence (ABC scale), and the modified Functional Reach Test (mFRT).20,22 Trials were included if they clearly stated the outcome measures that were used as a primary or secondary outcome. If studies included more than one measure to reflect gait or balance, we extracted all outcome measures of interest. Both ambulatory and nonambulatory measures of balance were included. Two review authors (VDM) and (RY) independently identified the relevant outcomes, and any differences were resolved by the third author (LA).
Study Designs
We included randomized and nonrandomized clinical trials (including pre and post studies) that were published in English. We included nonrandomized clinical trials because there are few randomized clinical trials (RCTs) on this specific topic, as VR therapy is a relatively new area of study. The analysis of the preliminary results of intervention studies is important to guide future research.
Data Extraction
Data were extracted separately by 2 reviewers (VDM) and (RY) and put into a standardized Excel spreadsheet table specifically designed for this review. Any discrepancy during data extraction was resolved through discussion with a third author (LA). The following data were extracted from the selected articles: study ID, content of intervention (experimental group and control group when appropriate), dosage (duration of the session, frequency, and total period of intervention), clinical trial design (RCT or pre-post), total number of participants (enrolled and concluded the intervention), participant characteristics (chronicity, type of injury, level of injury, and percentage of male), outcome measures related to gait and balance, and a brief summary of the main findings in measures of balance and gait.
Quality Assessment
Methodological quality of all RCTs was assessed using the Cochrane Risk of Bias Tool. 23 The following 6 items of the tool were rated: Random sequence generation (selection bias), Concealment of allocation (selection bias), Blinding participants and personal (performance bias), Blinding of assessors (detection bias), Incomplete outcome data (attrition bias), and Selective reporting (reporting bias). Each item was rated as high, low, or unclear risk of bias according to Cochrane guidelines. 23 Methodological quality of all pre-post studies was assessed using the Quality Assessment Tool for Before-After (Pre-post) Studies with no Control Group. 24 This tool includes 12 criteria that are subjectively rated according to five responses: yes, no, cannot determine (CD), not applicable (NA), or not reported (NR). 24 Overall scientific quality is then assigned to each study as good, fair, or poor. 24 Two reviewers (VDM) and (AA) independently assessed all the studies included in this review and consensus was reached through discussion with a third reviewer (LA).
Statistical Analysis
Meta-analyses were conducted across studies that made similar comparisons and, used similar outcome measurements. Groupings also required that there were at least 2 studies without excessive clinical heterogeneity. Clinical heterogeneity was defined by considering the intervention dosage, participant characteristics, and study design. All analyses were conducted using Review Manager 25 version 5.3.5 and the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions. 23 For all RCTs included in the meta-analysis, data were extracted from each study to determine standardized mean between-group differences and 95% confidence interval (95% CI) based on the change scores of means (postintervention – baseline) and standard deviations (SDs). In case of SD missing data, an estimation of the SD was calculated using the following formula proposed by the Cochrane handbook 23 :
where SDbaseline is the standard deviation at baseline, SDfinal is the standard deviation at postintervention, and corr is the correlation.
We used a correlation of 0.8 as recommended by the Cochrane handbook to calculate the SDs. I2 statistics was used to determine statistical heterogeneity among the studies. 26 A fixed effect model (FEM) was used for the meta-analysis of the RCTs because the heterogeneity was low (I2 < 30% for the T-shirt test analysis and I2 = 0% for the mFRT analysis). 26 Because different outcome measurements were pooled together to determine the effect of VR therapy combined with conventional therapy compared to conventional therapy only on sitting balance, the effect size was reported as standardized mean difference (SMD) with 95% CI. Where the reported outcome had a scale where a higher value is indicative of worse outcome (e.g. T-shirt test), the reported values were multiplied by –1 so that in all analyses a higher value is indicative of better outcome.
For all pre-post studies included in the meta-analyses, baseline and postintervention means and SDs were extracted to perform the analyses. A FEM was also used for the pre-post studies because the heterogeneity was I2 = 0% for all the analyses. 26 Mean difference (MD) was used to express in separate meta-analyses the effect size of VR therapy before and after intervention on standing balance (BBS and ABC scale). Because different outcome measurements were pooled together to determine the effect of VR therapy before and after intervention on gait, the effect size was also reported as SMD with 95% CI.
Results
Search Process
The searches retrieved a total of 754 articles. After removal of duplicates and screening of titles and abstracts, 38 articles were assessed for eligibility. Ten studies27-36 were included in this systematic review and 6 studies in the meta-analysis.27,29,31,32,35,36 Four studies were not included in the meta-analysis because of missing data or use of unique outcome measures. Some studies could not be grouped together with other studies due to differences in study designs or types of comparisons.28,30,33,34 Figure 1 shows the flow diagram for this study based on the PRISMA guidelines.
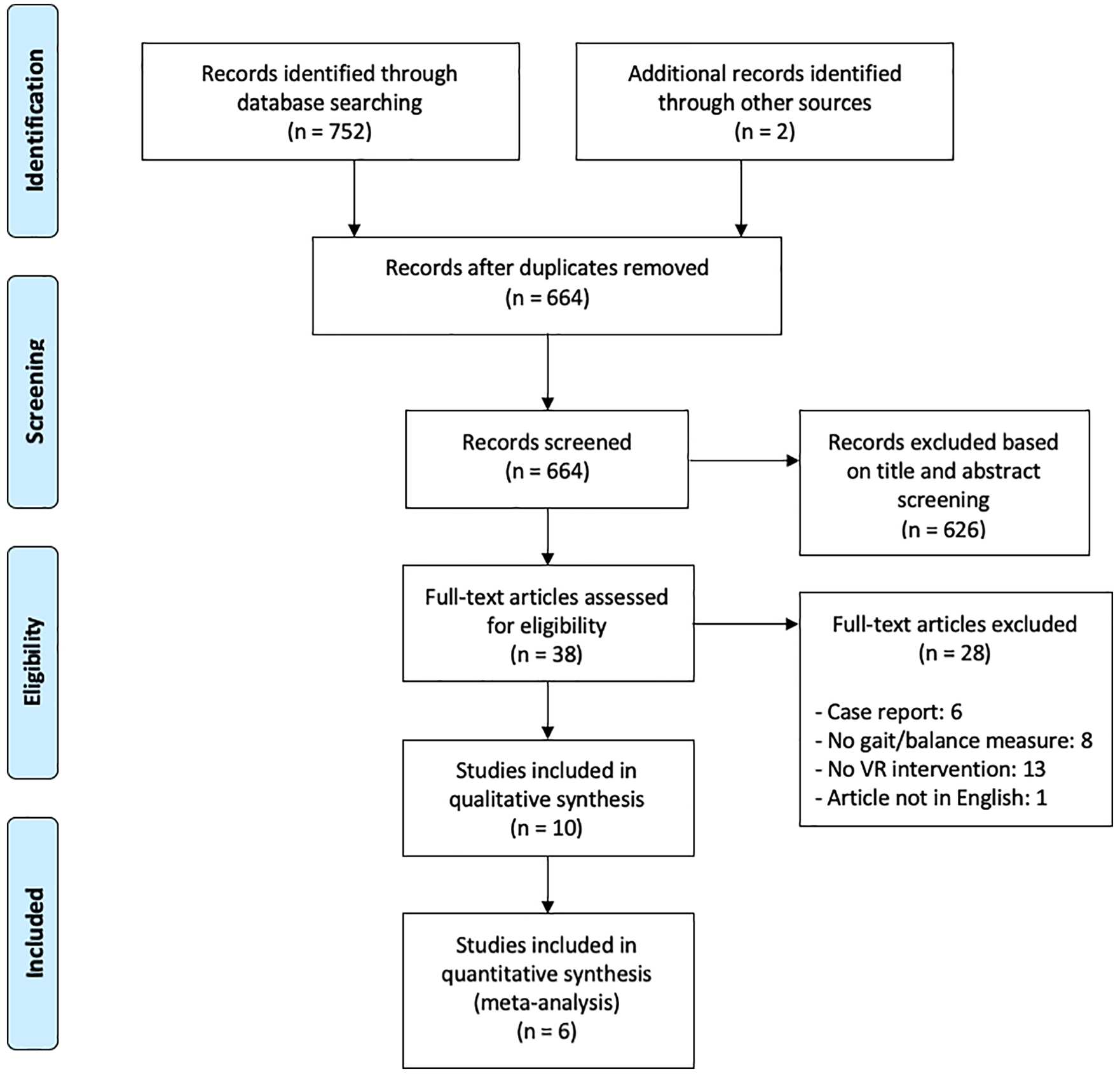
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flow chart.
Characteristics of Included Studies and Participants
Data from 10 studies were extracted and are presented in Table 1. Three studies were RCTs29,34,35 and 7 studies27,28,30-33,36 were pre-post trials in individuals with SCI using a VR as a treatment and assessing gait and/or balance. A total of 149 participants with time since injury of at least 6 months, American Spinal Injury Association Impairment Scale (AIS) A, B, C, and D, injury level from C2 to L3, and male population of 79% were included in the review. One study compared individuals with SCI to able-bodied participants but only data related to individuals with SCI were extracted for this review. 34 Five studies used only VR therapy, including Nintendo Wii Fit balance training, 34 semi-immersive VR, 27 individualized VR gait therapy, 36 lower limb VR augmented therapy, 31 and home-based lower limb VR augmented therapy. 32 The other studies used a combination of VR therapy with balance or coordination training.28-30,33,35
Details of the Included Studies.
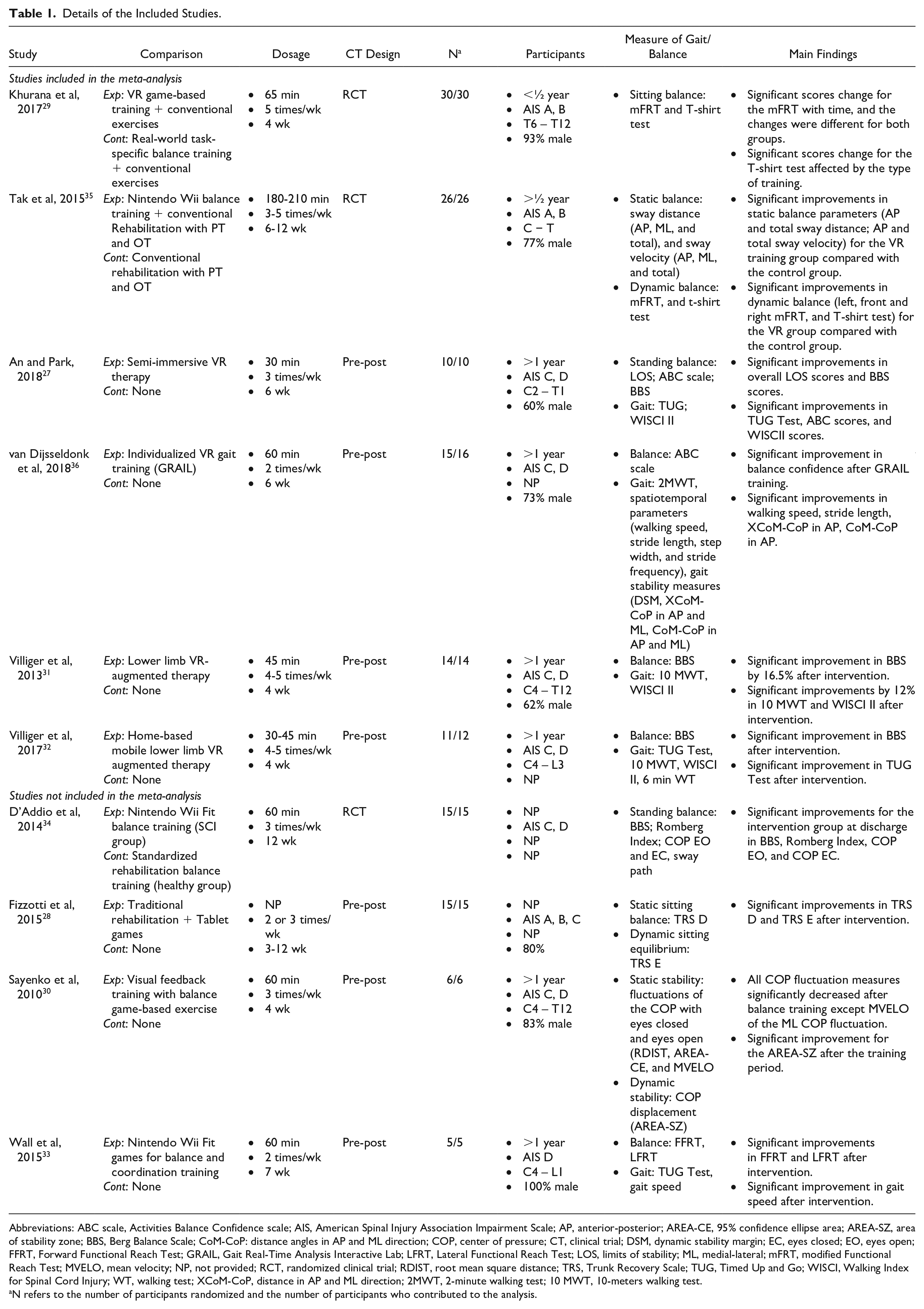
Abbreviations: ABC scale, Activities Balance Confidence scale; AIS, American Spinal Injury Association Impairment Scale; AP, anterior-posterior; AREA-CE, 95% confidence ellipse area; AREA-SZ, area of stability zone; BBS, Berg Balance Scale; CoM-CoP: distance angles in AP and ML direction; COP, center of pressure; CT, clinical trial; DSM, dynamic stability margin; EC, eyes closed; EO, eyes open; FFRT, Forward Functional Reach Test; GRAIL, Gait Real-Time Analysis Interactive Lab; LFRT, Lateral Functional Reach Test; LOS, limits of stability; ML, medial-lateral; mFRT, modified Functional Reach Test; MVELO, mean velocity; NP, not provided; RCT, randomized clinical trial; RDIST, root mean square distance; TRS, Trunk Recovery Scale; TUG, Timed Up and Go; WISCI, Walking Index for Spinal Cord Injury; WT, walking test; XCoM-CoP, distance in AP and ML direction; 2MWT, 2-minute walking test; 10 MWT, 10-meters walking test.
N refers to the number of participants randomized and the number of participants who contributed to the analysis.
Balance and Gait Outcome Measures
The main outcomes measures analyzed in this review were clinical and biomechanics gait and balance assessments. The most commonly used sitting balance measures, the T-shirt test29,35 and the mFRT,29,33,35 were pooled in a meta-analysis. In addition, the Trunk Recovery Scale (TRS) item D 28 and sway distance and velocity 35 were used as a static sitting balance assessment, and TRS item E 28 was used as a dynamic sitting balance assessment. The most commonly used standing balance assessments were the BBS,27,31,32,34 and the ABC scale,27,36 which were pooled in a meta-analysis. In addition, the limits of stability (LOS), 27 the Romberg Index (RI), 34 the parameters of the center of pressure (COP),30,34 and the forward and lateral standing reaching Tests (FFRT and LFRT) 33 were used as standing balance measures. The most commonly used gait outcomes measures were the Walking Index for SCI II (WISCI II),27,31,32 the 10 MWT,31,32 and the Timed Up and Go (TUG) test27,32,33 and were pooled in a meta-analysis. In addition, the 2-MWT, 36 the spatiotemporal gait parameters, 36 6-minute WT, 32 and gait speed 33 were also used to assess gait.
Quality of Studies
The results of the risk of bias assessment for the RCTs are presented in Figure 2. Two of the three RCTs included in this review presented a low risk of bias.29,35 The third RCT was not included in the meta-analysis due to clinical heterogeneity with the other RCTs and was rated as high risk of bias. 34 The most common deficiencies among the RCTs were selection bias (concealment of allocation) and performance bias (blinding personal). The results of the methodological quality assessment for the pre-post studies are presented in Table 2. Four31-33,36 out of the 7 pre-post studies included in this review presented an overall good quality and 3 studies27,28,30 were rated as fair overall quality.
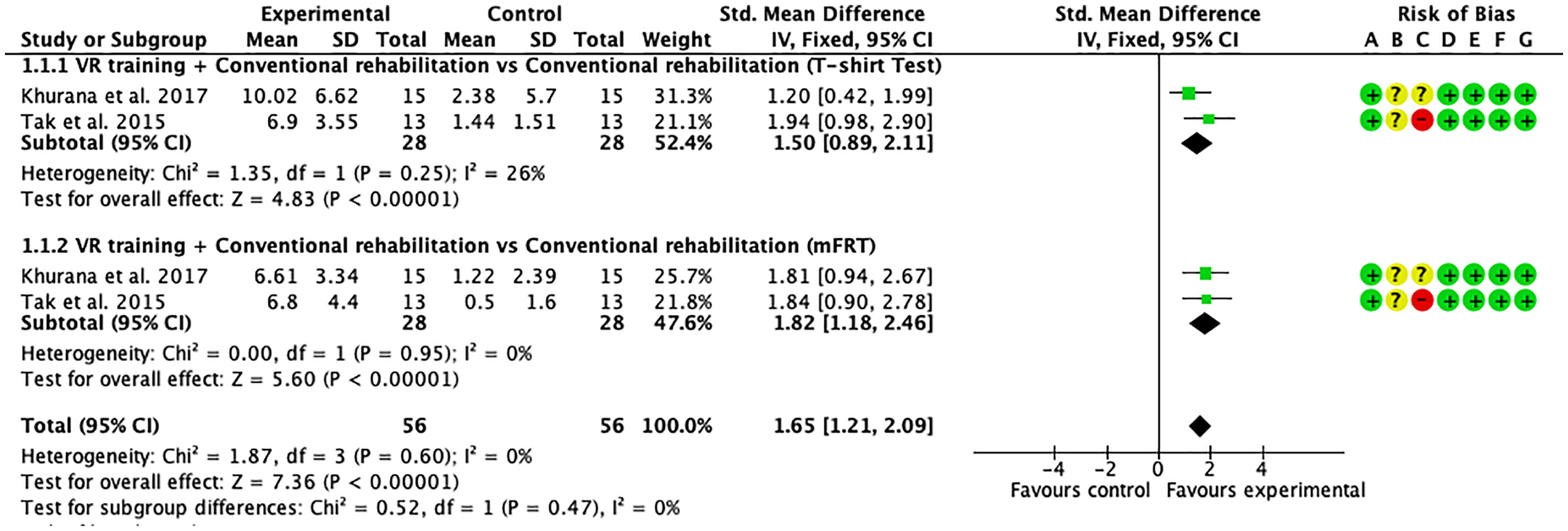
Sitting balance: forest plot of randomized clinical trials (RCTs) comparing virtual reality (VR) training combined with conventional rehabilitation to conventional rehabilitation only.
Quality Assessment for Before-After (Pre-Post) Studies With No Control Group.
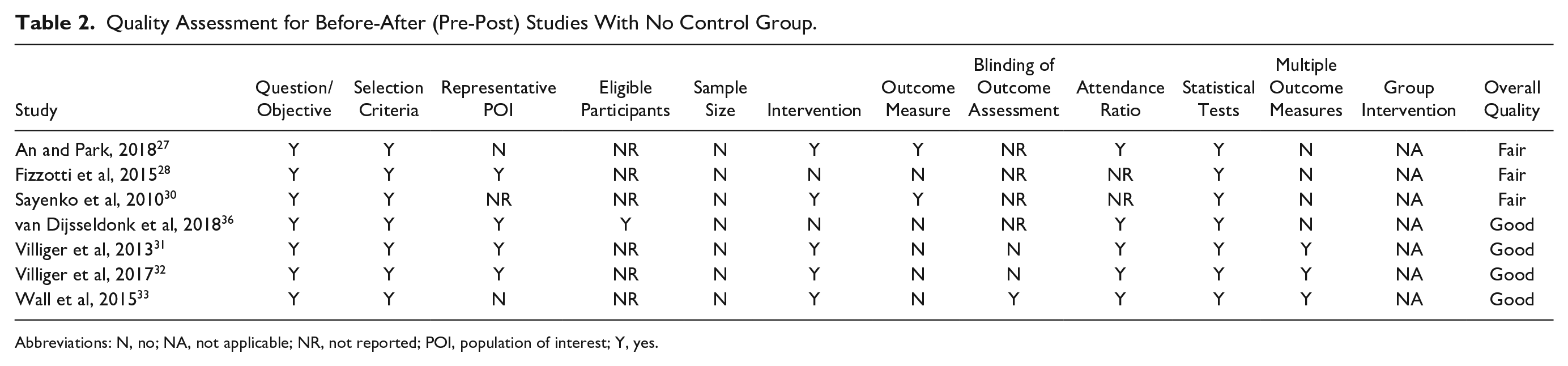
Abbreviations: N, no; NA, not applicable; NR, not reported; POI, population of interest; Y, yes.
Effect of VR Interventions
Sitting Balance
Figure 2 includes 2 RCTs that examined the effect of VR therapy with conventional balance rehabilitation compared to conventional balance rehabilitation only using the T-shirt test and the mFRT. The results of these 2 RCTs were pooled in 2 meta-analyses (FEM) with the results expressed as SMD. The analysis of the T-shirt test showed a statistically significant between-group difference (SMD = 1.50; 95% CI 0.89-2.11; P < .01). In addition, the analysis of the mFRT showed a statistically significant between-group difference (SMD = 1.82; 95% CI 1.18-2.46; P < .01). The combination of these 2 meta-analyses showed a statistically significant between-group difference (SMD = 1.65; 95% CI 1.21-2.09; P < .01). VR therapy with conventional balance rehabilitation was more effective in improving sitting balance compared with conventional sitting balance rehabilitation only. Both studies included in this analysis showed a low risk of bias (Figure 2).
Standing Balance
Figure 3 includes 4 pre-post studies that examined the effect of VR therapy without a control group using the BBS and the ABC scales. The results of these 4 pre-post studies were also pooled in 2 meta-analyses (FEM) with results expressed as MD. The analysis of the BBS scale showed a statistically significant within-group difference (MD = 4.22; 95% CI 1.78-6.66; P < .01). In addition, the analysis of the ABC scale showed a statistically significant within-group difference (MD = 8.53; 95% CI 2.52-14.53; P < .01). The meta-analyses of the BBS and the ABC scale were not pooled together because both measures assess different constructs of standing balance (standing stability and confidence in standing balance, respectively). Results indicate that after completion of VR therapy, standing balance significantly improved compared with baseline. Three out of the 4 studies included in this analysis were rated as good overall quality and 1 was rated as a fair overall quality (Table 2).
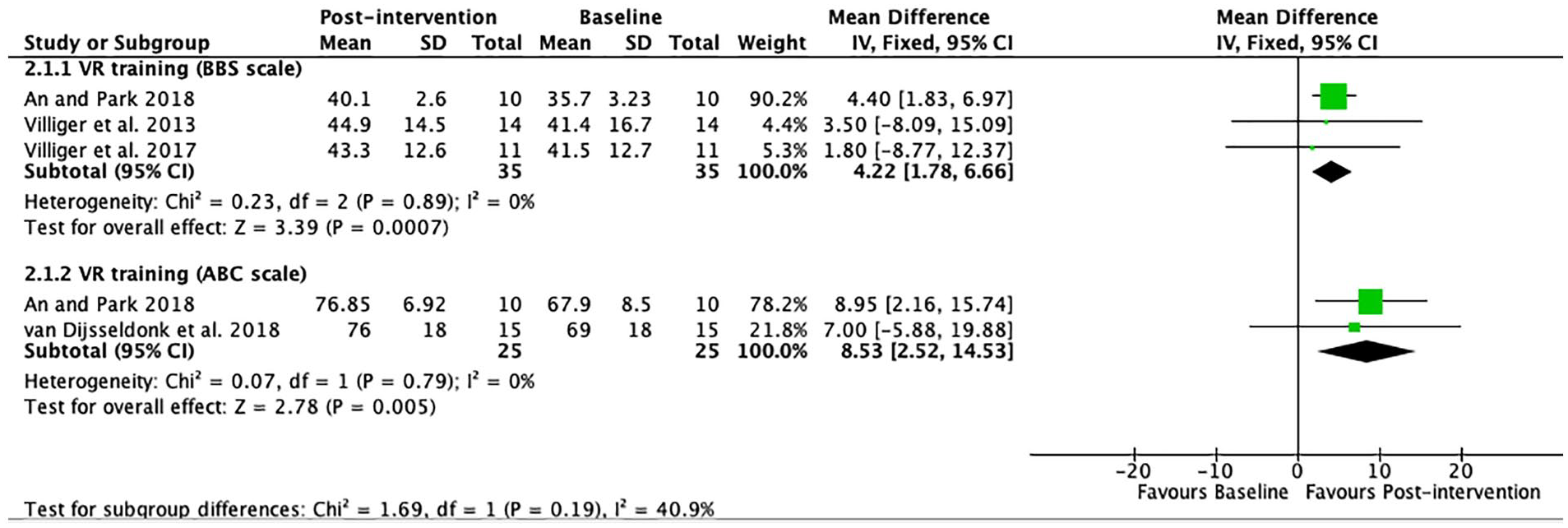
Standing balance: forest plot of trials comparing virtual reality (VR) training before and after intervention.
Gait
Figure 4 includes 3 pre-post studies that examined the effect of VR therapy without a control group using the WISCI II, the 10 MWT, and the TUG test. The results of these 3 pre-posts were also pooled in 3 meta-analyses (FEM) with the results expressed as SMD. None of the 3 meta-analyses showed a statistically significant within-group difference (P > .05). However, the combination of these 3 meta-analyses showed an overall statistically significant within-group difference (SMD = 0.34; 95% CI 0.02-0.66; P = .04). After completion of VR therapy, results show that there is a trend toward improvement in overall gait function compared with baseline. Two out of the 3 studies included in this analysis were rated as a good overall quality and 1 was rated as a fair overall quality (Table 2).
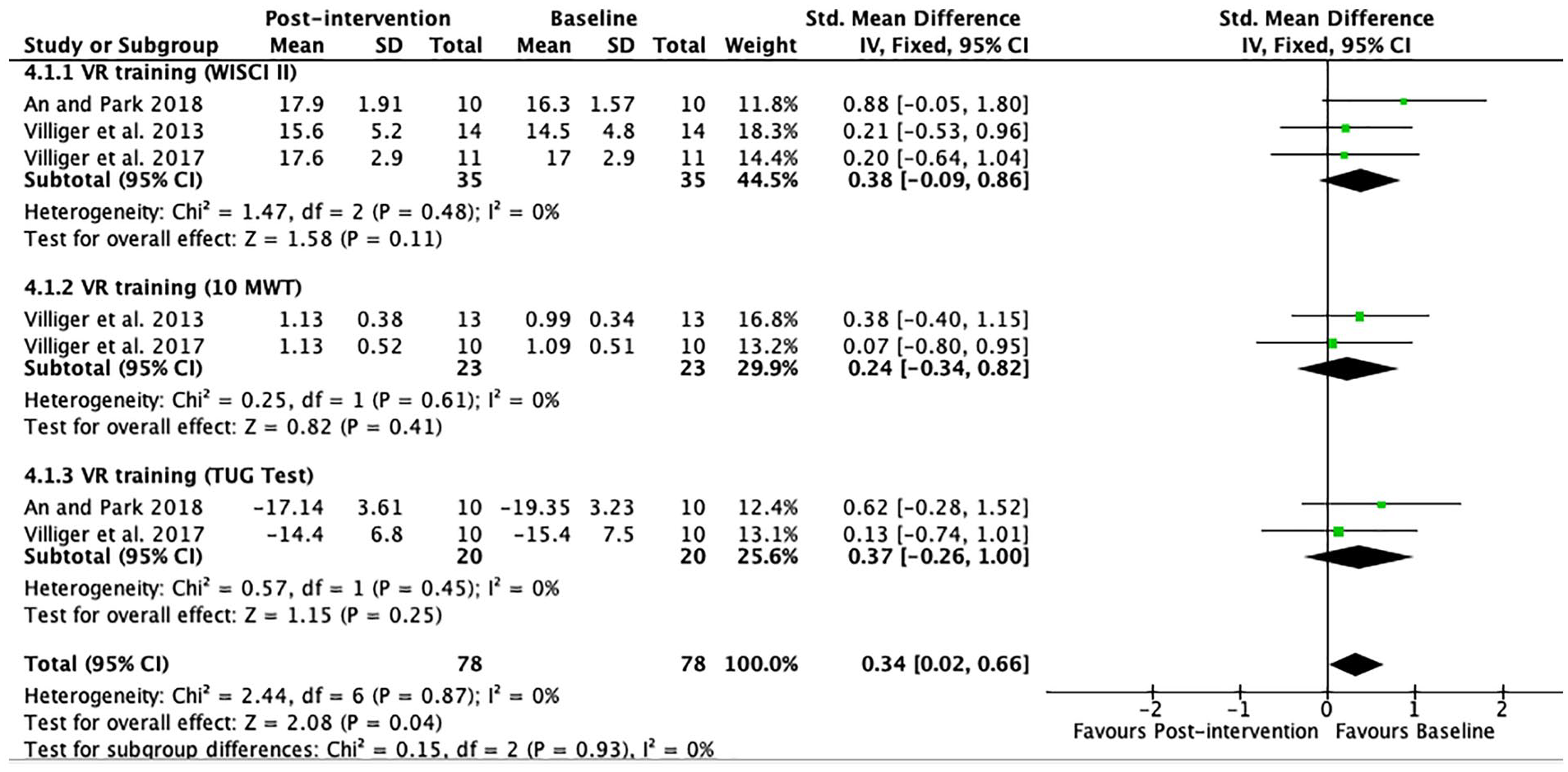
Gait: forest plot of trials comparing virtual reality (VR) training before and after intervention.
Trials Not Included in Meta-analysis
One of the 4 studies not included in the meta-analysis was an RCT, and the other 3 were pre-post studies. The studies were not included in the meta-analysis because of missing data, or they could not be grouped together with the other studies due to excessive clinical heterogeneity. The study by D’Addio et al 34 showed significant improvements in the group trained with a Nintendo Wii Fit after 12 weeks in standing balance (BBS scale, the RI, the COP eyes closed and open). Similarly, the study by Sayenko et al 30 showed significant improvements in static balance and dynamic stability measured with COP parameters after 4 weeks of visual feedback training with balance game-based exercise. No improvement was obtained for the mean velocity of the medial-lateral COP fluctuation. 30 Significant improvements were reported in TRS items D and E by Fizzotti et al 28 after 3 to 12 weeks of traditional rehabilitation plus tablet games. The study by Wall et al 33 showed significant improvements after 7 weeks in balance (FFRT and LFRT) and gait (gait speed) but no difference was found in the TUG Test.
Discussion
The aim of this systematic and meta-analysis was to investigate the available published data on the effectiveness of VR therapy for the improvement of gait and balance (sitting and standing) in individuals with SCI. We identified 10 trials in this study and included 6 in our meta-analysis. Four studies were not included because of missing data, the use of unique outcome measures, or the inability to be grouped together with other studies due to differences in study designs or types of comparisons. Results indicate significant and beneficial effects of VR therapy on sitting and standing balance. VR therapy with conventional balance rehabilitation was more effective in improving sitting balance compared with only conventional balance rehabilitation. In addition, we found a trend for significant effects of VR therapy on overall gait function in this population. However, the results of this study are based on only 2 RCTs. The majority of the data guiding these findings come from pre-post trials with no control groups.
Our first meta-analysis related to VR therapy and sitting balance provides insights into the effectiveness of VR therapy combined with conventional sitting balance rehabilitation compared to the use of only conventional sitting balance rehabilitation. The results showed that VR therapy with conventional rehabilitation is superior to conventional sitting balance rehabilitation only. Similar findings have been reported in another review where the authors discussed positive results of interactive gaming to facilitate balance among individuals with SCI. 18 The results are also in line with the findings reported by Santos et al 16 where traditional PT balance training plus VR therapy was superior to only traditional PT balance training in improving balance among individuals with Parkinson’s disease. There are 2 hypothetical explanations that support the findings. First, the combination of VR therapy with conventional rehabilitation provides more intense and challenging tasks to individuals than only conventional rehabilitation. In addition, the VR therapy used in the studies (VR game–based training 29 and Nintendo Wii balance training 35 ) involves performing tasks regarding changes in the center of gravity movements, such as switching positions, avoiding obstacles, and reaching for objects in different directions and heights. As the games advance, the level of difficulty increases leading the participants to develop new skills to maintain postural stability. VR therapy might be considered a good additional and “fun” treatment to conventional rehabilitation in order to improve postural stability among non-ambulatory individuals with SCI.
The second meta-analysis of our study examined standing balance before and after a VR therapy without a control group. After exposure to VR therapy, BBS and the ABC scales scores increased, indicating enhancements of standing stability and confidence in balance, respectively. Our results showed that VR therapy has the potential of improving standing balance among individuals with SCI. A similar result was reported by de Rooij et al 11 on standing balance where a VR therapy group was compared to a control group of individuals with stroke. The study by An and Park 27 particularly influenced our analyses. The BBS and the ABC scale significantly improved after intervention may be due to the nature of the VR therapy used (semi-immersive VR therapy). The semi-immersive VR therapy increases the motivation of the participants to practice the game and therefore to perform the rehabilitation exercises. This hypothesis is supported by a recent study which highlighted the beneficial effects of VR therapy on psychological and motivational aspects of individuals with SCI. 37 By increasing the motivation and providing a safe environment, VR therapy may enhance the interest of individuals with SCI to exercise. Improving interest, participation levels, and confidence might lead to adherence to the therapy 10 and improvement in standing balance in this population. However, the results of this comparison should be interpreted with caution because they are based on pre-post study data and might not provide reliable information about the effect of the VR therapy itself. A pre-post study using VR therapy is not controlled and therefore it is not possible to differentiate whether the results are caused by the effect of the VR therapy or by other possible factors. 38
Our last meta-analysis explored gait before and after VR therapy without a control group. VR therapy was not effective in separately improving the WISCI II, the 10 MWT, and the TUG Test which represent measures of functional mobility, gait velocity, and upright mobility, respectively. Interestingly, a combination of the meta-analyses showed a trend to a significant improvement in overall gait functions in this population (SMD = 0.34; 95% CI 0.02-0.66; P = .04). Inconclusive results have also been reported regarding the effect of VR therapy on gait in individuals with Parkinson’s disease. 17 This might be because gait involves several functions, including lower limb strength, spatiotemporal parameters such as stride length, step width, and the use of assistive devices such as a walker, cane, or crutches. A single measure such as WISCI II alone does not necessarily correlate with walking ability. In addition, the WISCI II assesses the amount of physical assistance, assistive devices, and the use of a brace, and these aspects are not necessarily addressed in VR therapy. However, these aspects are addressed and trained in conventional PT gait training. Thus, since particular details of the WISCI II, TUG test, 10 MWT are not taken into consideration during VR therapy, the measures may not have shown significant improvements. For an adequate transfer of gait VR therapy to actual community ambulation, assistive devices and some environmental aspects, such as slopes and obstacles should be considered. VR therapy might be an effective additional treatment to conventional PT gait training. Ultimately, the results of this comparison only constitute preliminary results since they are based on pre-post studies.
Limitations
There are several limitations to this review. First, our results rely on a few numbers of trials. Only 3 RCTs were identified and 2 included in the meta-analysis. The meta-analysis based on the RCTs compared 2 interventions (VR therapy plus conventional rehabilitation and convention rehabilitation only). This type of comparison provides no insight into the effectiveness of interventions per se. It only indicates whether one treatment is superior or not to another. In addition, when VR therapy is combined with conventional rehabilitation, it is impossible to conclude whether changes in outcomes should be attributed to VR therapy or conventional rehabilitation. To overcome this limitation, a VR therapy group should be compared to a true control group (sham group) in an RCT study design. Also, some results are based on pre-post trials, which might not provide reliable information about the real effect of VR therapy. The type of VR (non-immersive, semi-immersive, and immersive) also varied vastly among the included studies, which might hinder the generalizability of the results. Finally, it should be noted that we only included published trials in English language. This is a common limitation of systematic review since several trials related to the topic might be published in other languages such as French and Chinese.
Conclusion
This systematic review and meta-analysis demonstrated significant and beneficial effects of VR therapy on balance (sitting and standing) and a trend to improve gait functions. VR therapy increases tasks repetition, the amount of treatment time, interest, and confidence to perform rehabilitation exercises. Therefore, VR therapy might constitute a good additional treatment to conventional therapy to improve gait and balance in individuals with SCI. However, the results should be interpreted with caution since the findings related to gait and standing balance are based on preliminary data. The results emphasize the need for further well-designed RCTs investigating the effect of VR therapy on different outcomes such as gait and balance among individuals with SCI. Future RCTs should focus on comparing VR therapy in an isolated way with traditional rehabilitation or with a real control group with a clear and well-detailed description of the intervention protocol.
Supplemental Material
Appendix_1 – Supplemental material for Effects of Virtual Reality Therapy on Gait and Balance Among Individuals With Spinal Cord Injury: A Systematic Review and Meta-analysis
Supplemental material, Appendix_1 for Effects of Virtual Reality Therapy on Gait and Balance Among Individuals With Spinal Cord Injury: A Systematic Review and Meta-analysis by Libak Abou, Vonjiniaina Domohina Malala, Rebecca Yarnot, Aditya Alluri and Laura A. Rice in Neurorehabilitation and Neural Repair
Supplemental Material
PRISMA_2009 – Supplemental material for Effects of Virtual Reality Therapy on Gait and Balance Among Individuals With Spinal Cord Injury: A Systematic Review and Meta-analysis
Supplemental material, PRISMA_2009 for Effects of Virtual Reality Therapy on Gait and Balance Among Individuals With Spinal Cord Injury: A Systematic Review and Meta-analysis by Libak Abou, Vonjiniaina Domohina Malala, Rebecca Yarnot, Aditya Alluri and Laura A. Rice in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.