
Abstract
Background. In Parkinson disease (PD), gait impairments often coexist with nonmotor symptoms such as anxiety and depression. Biofeedback training may improve gait function in PD, but its effect on nonmotor symptoms remains unclear. This study explored the cognitive and global effects of Ambulosono, a cognitive gait training method utilizing step size to contingently control the real-time play of motivational music. Objective. This study examined the feasibility of music-contingent gait training and its effects on neuropsychological test performance and mood in persons with PD. Methods. A total of 30 participants with mild to moderate PD were semirandomized via sequential alternating assignment into an experimental training group or control music group. The training group received 12 weeks of music-contingent training, whereby music play was dependent on the user achieving a set stride length, adjusted online based on individual performance. The control group received hybrid training beginning with 6 weeks of noncontingent music walking, whereby music played continuously regardless of step size, followed by 6 weeks of music-contingent training. Global cognition, memory, executive function, attention, and working memory assessments were completed by blinded assessors at baseline, 6 weeks, and 12 weeks. Motor function, mood, and anxiety were assessed. Results. Average training adherence was 97%, with no falls occurring during training sessions. Improvements on cognitive measures were not clinically significant; however, significant decreases in depression and anxiety were observed in both groups over time (P < .05). Conclusions. Music-contingent gait training is feasible and safe in individuals with PD. Further investigation into potential therapeutic applications of this technology is recommended.
Keywords
Introduction
Gait dysfunction is widely accepted as one of the most debilitating motor symptoms of Parkinson disease (PD). 1 Two prominent characteristics of Parkinsonian gait include shortened stride length (shuffling) and slowing of movement (bradykinesia). 1 Gait impairment can coexist with or precede declines in cognition—a relationship that has been well established in studies of the interplay between gait variability, cognitive dysfunction, and falls risk. 2 Although poorly understood, the relationship between gait and cognition may be attributable to neural networks mutually involved in gait and cognition.2,3 In PD populations, gait has been identified as a noninvasive clinical biomarker for predicting cognitive decline. 3 Although drug therapies are common treatments for individuals with PD, accumulating evidence supports the integration of nonpharmacological interventions to improve both gait dysfunction and cognition.4,5 In older adults with and without PD, a variety of exercise interventions, including walking, have been shown to benefit cognition across multiple domains (executive function, attention, working memory, perceptual and motor timing) in response to a broad range of activity types, frequencies, durations, and intensities.6-12
Contemporary gait training, which incorporates technological cues and feedback to facilitate gait improvements, has become increasingly popular in treating the gait deficits of PD.4,13,14 Although the most common form of gait cueing is rhythmic auditory stimulation using a simple stimulus (eg, a metronome), these fixed-tempo designs have been criticized for increasing cognitive demand and failing to be interactive or adaptive to individual gait parameters. 13 In contrast, using a complex stimulus such as music provides multiple opportunities for the listener to map movements—cueing that goes beyond fixed temporal intervals. 15 Music shifts the listener’s focus from mobility limitations to enjoyment of the music. 16 Significant improvements in gait parameters such as cadence, stride length, stride time, and velocity have resulted from music-based gait interventions in PD that used rhythmically accentuated instrumental music and playlists consisting of songs that were tempo to cadence matched.17,18 Music-based gait interventions may also benefit cognition; improvements to perceptual and motor timing have been reported from gait training with rhythmically accentuated instrumental music. 10 As with fixed-tempo designs, concerns regarding increased cognitive demand during music-based gait training have been raised. However, gait training with music has been verified as a safe activity for individuals with mild to moderate PD. 18
The GaitReminder iPod application is a method of musical gait training that rewards desirable gait behaviors with music play via a wearable sensor and music player. 19 Collectively referred to as Ambulosono, this gait training system’s rich repertoire of sensorimotor cueing is purposely designed to activate physiological endogenous dopaminergic and nondopaminergic systems to stimulate attentional and motivational networks. 19 Using behavioral conditioning to remodel brain neuroplasticity and compensation mechanisms, Ambulosono intervenes on gait dysfunction in PD by creating a contingency between gait parameters and music playback, generating real-time biofeedback that may help patients to self-motivate and self-activate reward and motivational networks with training.19-21 Ambulosono interventions have been shown to reduce freezing episodes, increase motor automaticity, and increase step size and velocity.20,22 Although general cognitive function did not improve in response to a 4-week in-home, music-contingent stepping-in-place training protocol, 20 the effect of community-based music-contingent gait training on specific cognitive function and mood in persons with PD has not been investigated.
Our objectives were (1) to examine the feasibility of community-based music-contingent gait training in individuals with PD and (2) to investigate the effects of community-based music-contingent gait training on cognition and mood in individuals with PD in a music-contingent-only training group and a control group exposed to noncontingent music for 6 weeks followed by 6 weeks of music-contingent training. We hypothesized that improvements in cognition would result for both groups based on prior evidence of cognitive improvements resulting from physical activity interventions. We hypothesized that greater cognitive improvements would be seen with increased volumes of music-contingent gait training. We also examined the impact of music-contingent gait training on mood (anxiety and depressive symptoms) in PD. We hypothesized that both groups would experience mood improvements in response to music and physical activity exposure.
Methods
Participants
A total of 30 participants with mild to moderate PD were recruited from the Kaye Edmonton Clinic Movement Disorders Clinic, Parkinson Alberta, and the Michael J. Fox Foundation Fox Trial Finder (Supplemental Figure 1). Participants had a clinical diagnosis of PD consistent with UK brain bank criteria, 23 had the ability to walk for 15 minutes independently (without the use of walking aids), and were on stable medications. Exclusion criteria included active medical conditions that might interfere with safe participation (including active cancer, cardiac disease, pulmonary disease, disabling musculoskeletal disease in addition to PD), severe cognitive impairment with functional consequences (dementia), and spontaneous balance impairment or inability to walk as indicated by the Hoehn and Yahr (HY) Stage Assessment (stages 4 and 5). 24 Throughout the duration of the study, participants continued usual activities such as physiotherapy, exercise groups, and regular activities of daily living. Data collection occurred between October 2014 and February 2017.
Ethics
Ethics approval was obtained from the University of Alberta Health Research Ethics Board in accordance with the Declaration of Helsinki (Pro00040237). Informed written consent was obtained from participants at baseline prior to participation.
Intervention
Participants were semirandomized into 2 groups via sequential alternating assignment at the time of enrollment according to order of enlistment (eg, first participant in music-contingent training group, second participant in control group, third participant in music-contingent training group). Clinical and cognitive assessments were performed at baseline, 6 weeks, and 12 weeks by blinded assessors. Between assessments, participants used a gait training system comprising wireless headphones and a combination music player/wearable sensor (iOS gyroscope and accelerometer housed within a fourth-generation iPod Touch [Apple Inc, Cupertino, CA]) anchored above the knee with a Velcro thigh band. The music-contingent training group received 12 weeks of gait feedback training during which time music play was dependent on the user achieving a set stride length. Steps of insufficient length resulted in silence, whereas strides that met or exceeded the step size threshold were rewarded with music play.20,21,25 The control group received 6 weeks of noncontingent music walking, whereby music played continuously regardless of step size (control arm), followed by 6 weeks of the feedback training. During training sessions, music play was randomized from preset playlists. Where applicable, the sensor was worn on the more affected side. Where symptoms were equal bilaterally, the participant chose a preferred leg on which to wear the apparatus. The gait training application and database were developed by the University of Calgary and have been previously described (ISRCTN registry: https://doi.org/10.1186/ISRCTN06023392). Following baseline assessments, participants completed an onsite equipment training session with research staff. To minimize the risk of falling, participants were encouraged to walk indoors (eg, a mall, indoor track) in inclement weather. A minimum of 15 minutes of music-contingent gait training, 3 times a week, was prescribed to each participant. Participants were instructed to walk at their usual pace.
To encourage participants to psychologically link music play and step length during music-contingent training, customized step size thresholds were set to achieve music play approximately 80% of the time. Accordingly, participants had to be purposeful and consistent with stride length for continuous music play. Walking files, recorded by the software, were sent automatically by the application via wireless internet to a central online database where research staff monitored data transfers, program adherence, and gait performance. Performance monitoring was remotely conducted twice a week, and remote threshold adjustments were made when indicated by participant feedback (eg, subjective experience of effort required to maintain 80% music play) and gait performance parameters (eg, changes in step size, speed, and/or cadence). Feasibility outcome measures included the number of walks completed and average walk duration.
Outcome Measures
At baseline, the following measures of disease severity were collected: HY stage assessment, 24 Schwab and England Activities of Daily Living, 26 Activities of Daily Living, 27 and the Modified Cumulative Illness Rating Scale. 28 Additional assessments included the AD8 Dementia Screening Interview 29 and the American National Adult Reading Test. 30
At each study visit (baseline, 6 weeks, and 12 weeks), clinical and cognitive assessments were conducted. Clinical assessments included the Unified Parkinson Disease Rating Scale Motor Examination (UPDRS-III), 31 the Geriatric Depression Scale (GDS) Short Form, 32 the Beck Anxiety Inventory (BAI), 33 a 10-m walking single task (usual pace), and a 10-m walking dual task (name generation) with dual task cost calculated. 34 At weeks 6 and 12, participants were asked to report any falls that had taken place since their previous study visit. Cognitive assessments tested participants across multiple cognitive domains. Measures of global cognition were assessed using the Standardized Mini Mental State Exam (SMMSE) 35 and the Montreal Cognitive Assessment. 36 Attention, memory, and executive function were evaluated using the Hopkins Verbal Learning Test—Revised 37 (HVLT-R; memory), Stroop Color-Word Test 38 (interference), Trail Making Tests A and B 39 (set shifting), Attention Network Test 40 (attention), and the Digit Ordering Test 41 (working memory). Where available and appropriate, alternative test versions were used at each assessment to avoid potential learning effects. Alternative versions of the Montreal Cognitive Assessment, HVLT-R, Trail Making Tests A and B, and the Digit Ordering test were used in this study.
Statistical Analysis
All analyses were conducted in Statistical Analysis System (SAS) 9.4. A P value less than .05 was considered statistically significant in this exploratory study. Baseline variables were compared between 2 groups (Table 1). Because of the small sample, the nonparametric Wilcoxon rank-sum test was used to test the statistical significance in numerical variables, and the Fisher exact test was used to test the differences in categorical variables. The mean and SD at each time point by group are summarized in Table 2 for clinical outcomes and Table 3 for cognitive outcomes.
Baseline Clinical and Demographic Participant Characteristics.
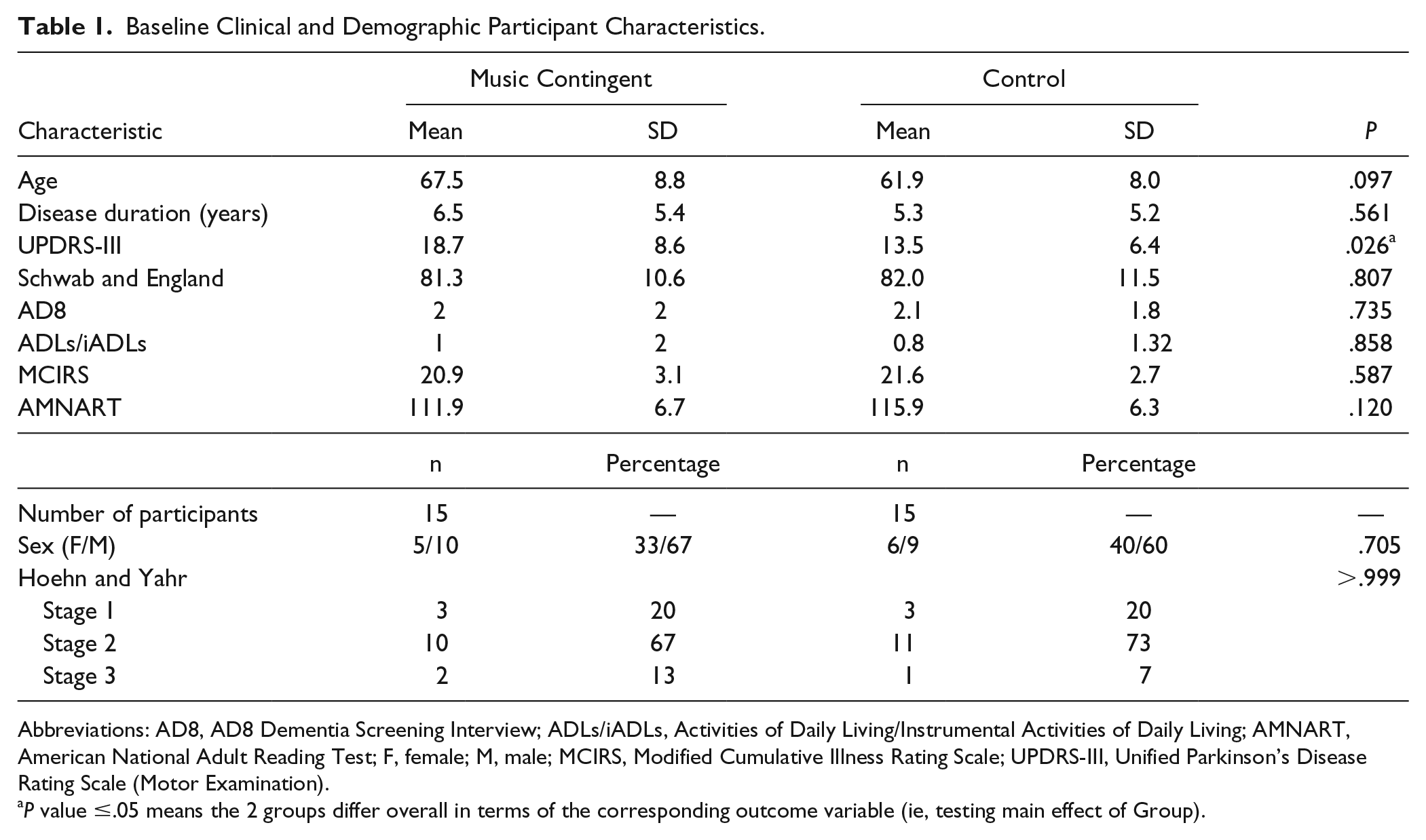
Abbreviations: AD8, AD8 Dementia Screening Interview; ADLs/iADLs, Activities of Daily Living/Instrumental Activities of Daily Living; AMNART, American National Adult Reading Test; F, female; M, male; MCIRS, Modified Cumulative Illness Rating Scale; UPDRS-III, Unified Parkinson’s Disease Rating Scale (Motor Examination).
P value ≤.05 means the 2 groups differ overall in terms of the corresponding outcome variable (ie, testing main effect of Group).
Summary Statistics (Mean and SD) of Outcome Variables at Each Visit by Group for Clinical Outcomes.
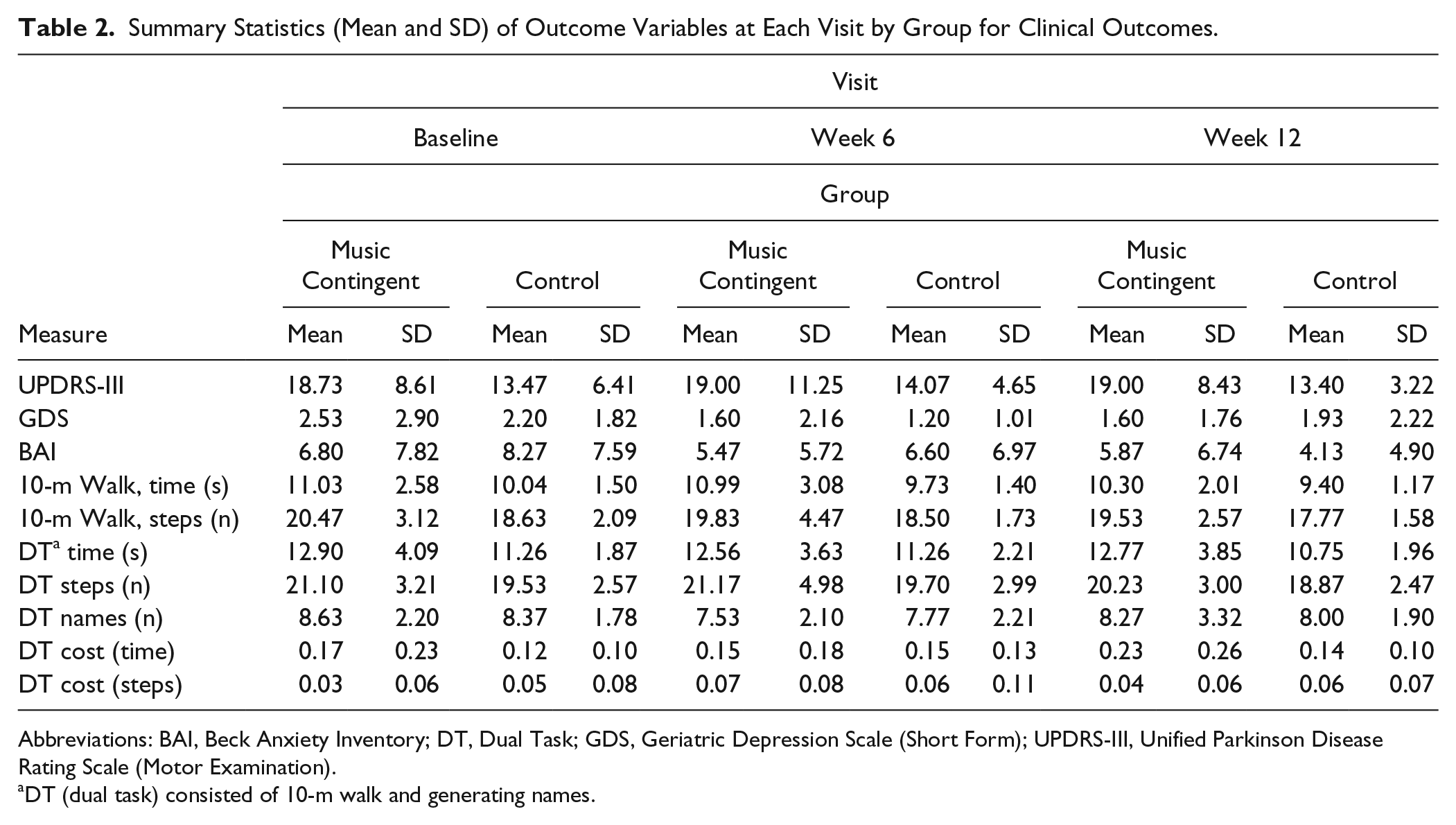
Abbreviations: BAI, Beck Anxiety Inventory; DT, Dual Task; GDS, Geriatric Depression Scale (Short Form); UPDRS-III, Unified Parkinson Disease Rating Scale (Motor Examination).
DT (dual task) consisted of 10-m walk and generating names.
Summary Statistics (Mean and SD) of Outcome Variables at Each Visit, by Group, for Cognitive Outcomes.
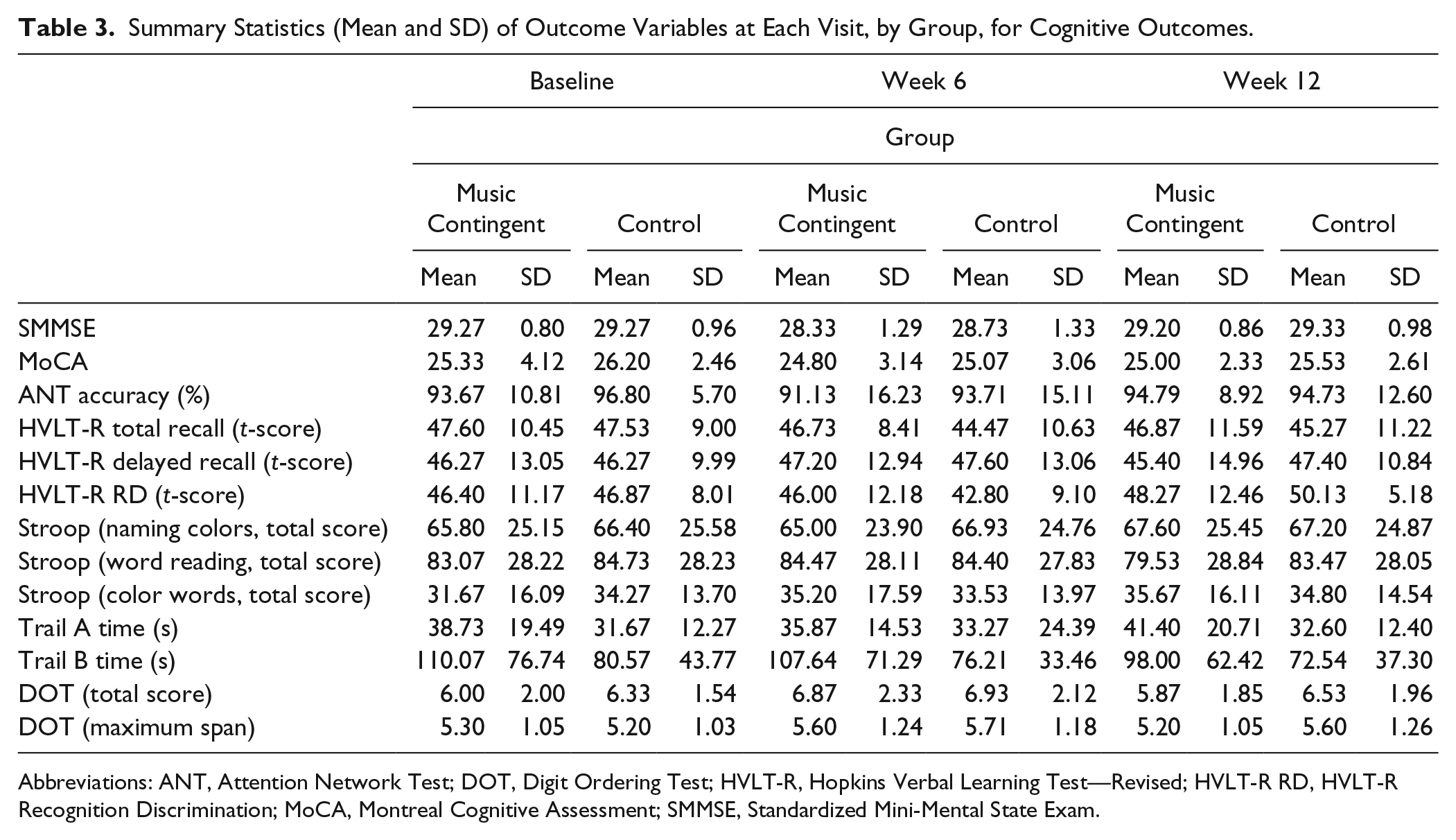
Abbreviations: ANT, Attention Network Test; DOT, Digit Ordering Test; HVLT-R, Hopkins Verbal Learning Test—Revised; HVLT-R RD, HVLT-R Recognition Discrimination; MoCA, Montreal Cognitive Assessment; SMMSE, Standardized Mini-Mental State Exam.
The mixed model was used to test whether there was a significant difference between the 2 groups with regard to the outcome variables, which were measured repeatedly over time. In the analysis, the independent variables were participant groups, time, and their interaction. The interaction was also added to the model to test if the difference between groups changed over time. The P value of the main effect of participant group, main effect of time, and the Participant group × Time interaction effect are given in Table 4 for clinical outcomes and Table 5 for cognitive outcomes.
Modeling Results From Mixed Model of Clinical Battery.
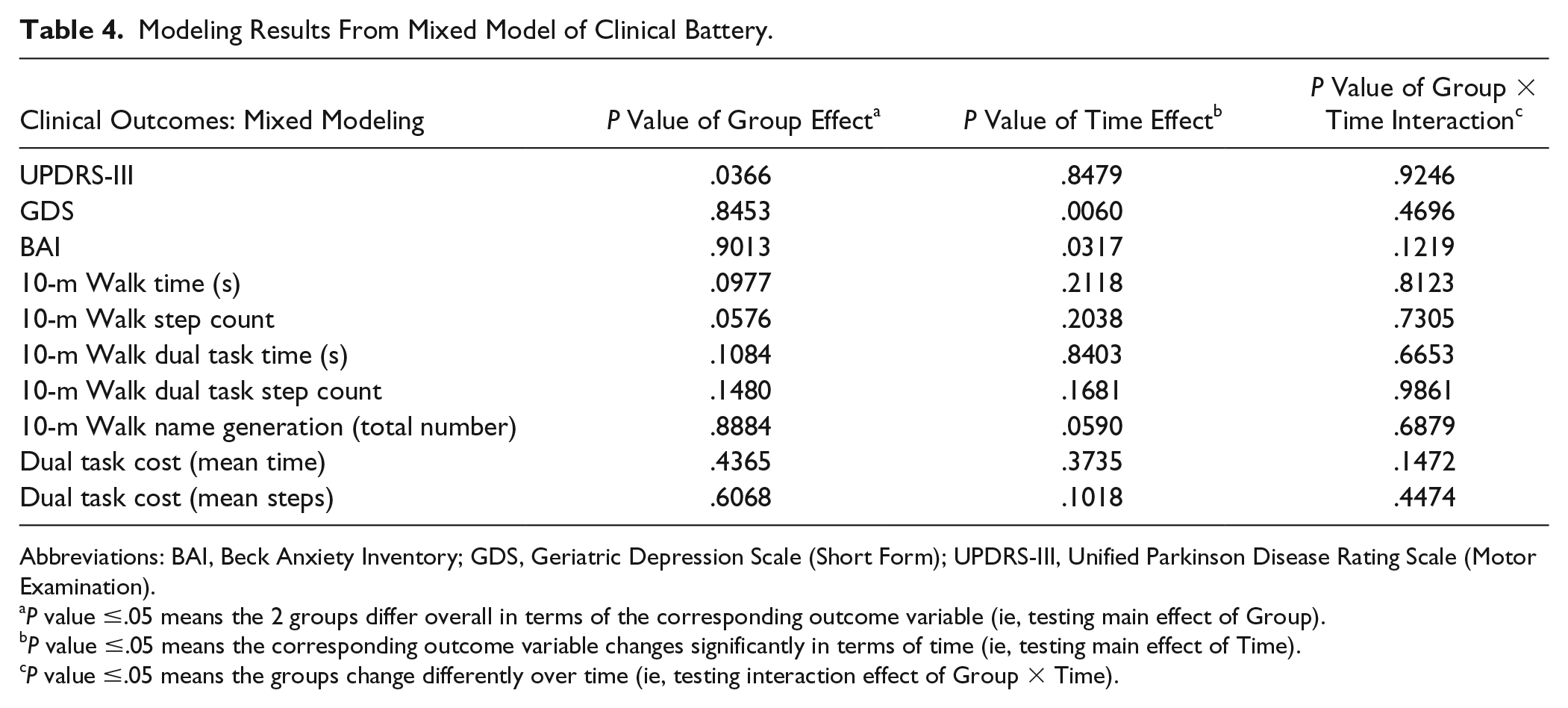
Abbreviations: BAI, Beck Anxiety Inventory; GDS, Geriatric Depression Scale (Short Form); UPDRS-III, Unified Parkinson Disease Rating Scale (Motor Examination).
P value ≤.05 means the 2 groups differ overall in terms of the corresponding outcome variable (ie, testing main effect of Group).
P value ≤.05 means the corresponding outcome variable changes significantly in terms of time (ie, testing main effect of Time).
P value ≤.05 means the groups change differently over time (ie, testing interaction effect of Group × Time).
Modeling Results From Mixed Model of Neuropsychology Battery.
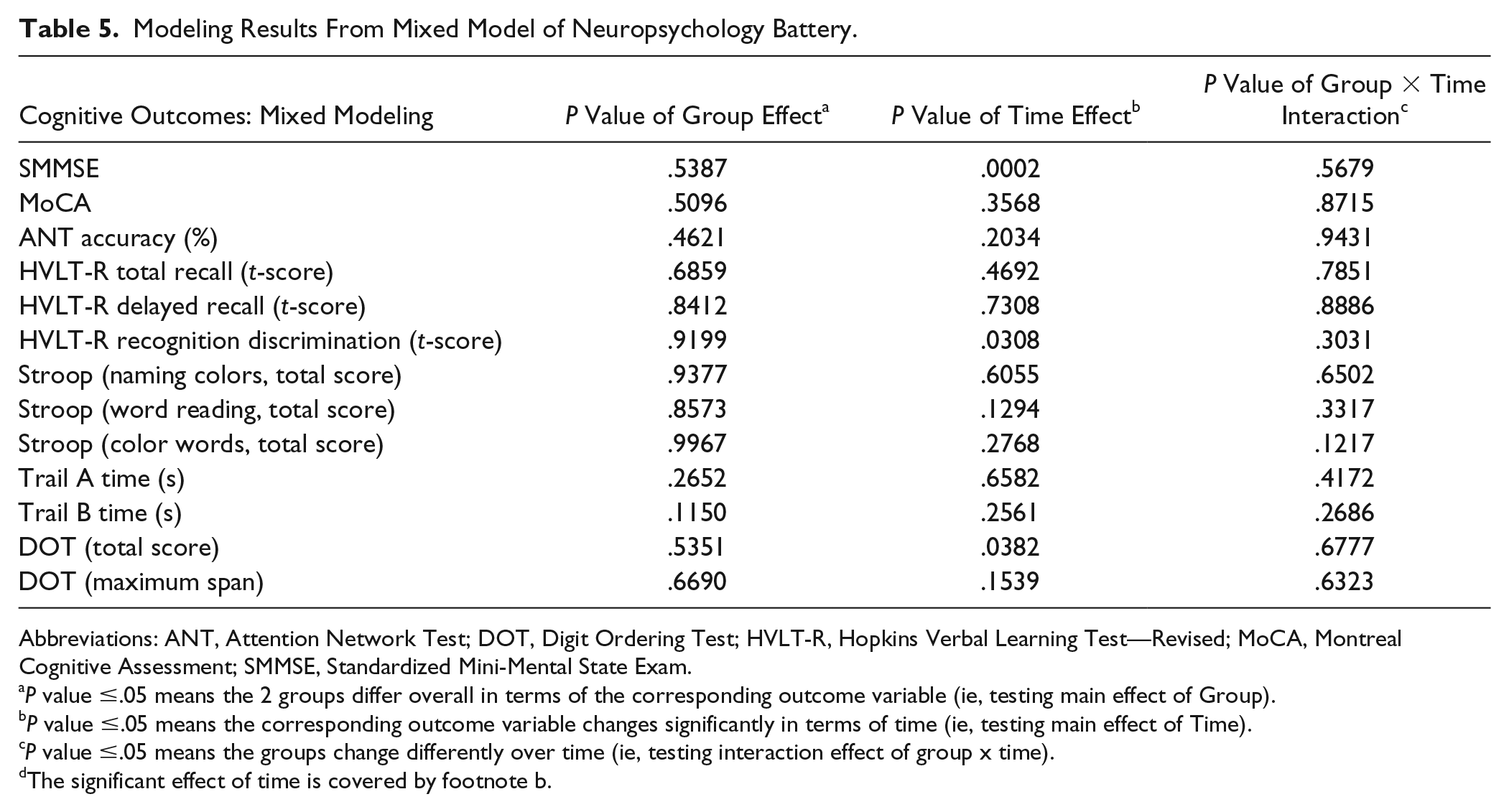
Abbreviations: ANT, Attention Network Test; DOT, Digit Ordering Test; HVLT-R, Hopkins Verbal Learning Test—Revised; MoCA, Montreal Cognitive Assessment; SMMSE, Standardized Mini-Mental State Exam.
P value ≤.05 means the 2 groups differ overall in terms of the corresponding outcome variable (ie, testing main effect of Group).
P value ≤.05 means the corresponding outcome variable changes significantly in terms of time (ie, testing main effect of Time).
P value ≤.05 means the groups change differently over time (ie, testing interaction effect of group x time).
Given possible effects of music-contingent gait training on memory, executive function, and working memory, a planned secondary analysis was conducted on specific exemplary tests for which normative values were available (HVLT-R and Trails A and B). Using a nonparametric Wilcoxon rank-sum test, we examined test performance at baseline compared with 6 weeks to determine if exposure to the different modalities (music alone versus music-contingent training) had differential effects (Table 6).
Comparison of Groups on Changes for Trails A/B and HVLT Measures Between Baseline and 6-Week Follow up.
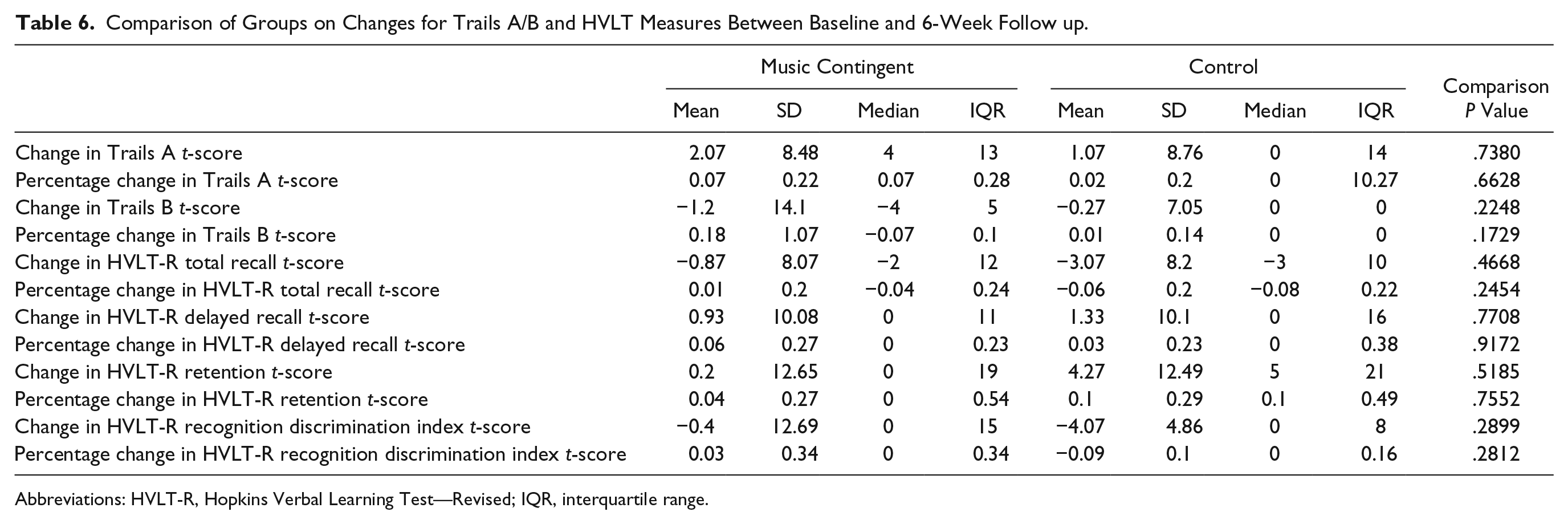
Abbreviations: HVLT-R, Hopkins Verbal Learning Test—Revised; IQR, interquartile range.
Results
A total of 30 individuals completed the study with equal allocation to the music-contingent training and control groups (n = 15 per group). Two participants in the music-contingent training group discontinued training during weeks 7 to 12; 1 participant reported lack of motivation, whereas the other did not find the apparatus comfortable to wear. Both participants agreed to finish final clinical and cognitive assessments. Subsequently, complete clinical and cognitive data were available for all participants, and intent-to-treat analyses were performed. Table 1 shows baseline characteristics of participants by group. The 2 groups were similar at baseline in terms of demographics and health conditions. At baseline, the control group had significantly lower scores (ie, less impairment) on the UPDRS-III (P = .026) than the music-contingent training group. When adjusted for, the UPDRS was not statistically significant in the mixed models and did not change the significance of the other variables; it was excluded accordingly. There were no significant differences between groups on any other measures of activity or disability. The majority of patients in both groups had a HY score of stage 2: bilateral or midline involvement without impairment of balance.
Intervention Feasibility
During the study period, a total of 9 falls were reported by 6 individuals. None of the falls occurred during walking sessions for the study. In the music-contingent training group, 2 participants had 1 fall each and 2 participants had 2 falls each (4 individuals, 6 falls). In the control group, 1 participant had 1 fall and another participant had 2 falls (2 individuals, 3 falls). Additionally, a participant in the control group experienced an episode of transient global amnesia lasting several hours. This adverse event was deemed unrelated to the study because it did not occur during or immediately after a walking session; it did not interfere with participation. Because of technological complications, walking data were only available for analysis in the first 20 participants. Given the sample size of the incomplete data set, gait parameter results will not be reported here. From data available for the first 10 participants in each group, the intervention appeared well adhered to. In the music-contingent training group, participants completed 34 walks on average over the course of the study (compared with the target 3 walks per week ×12 weeks = 36 walks), with a mean training time of 26 minutes. Similarly, participants of the control group averaged 40 walks, with a mean training time of 34 minutes per walk.
Clinical Outcomes
The analysis (Table 4) showed a significant main effect of group on UPDRS-III score (P = .037): the control group consistently performed better on motor assessments (ie, less impairment at baseline and subsequent assessments) than the music-contingent training group. There was no main effect for time (P = .8) or Group × Time interaction (P = .9), indicating that there was no differential impact of training protocol. Significant effects of time were observed on both the GDS (P = .006) and the BAI (P = .032). On both scales, scores decreased from baseline to the final assessment, indicating that symptoms abated. However, no Group × Time interactions were observed, indicating that both groups showed similar changes.
Cognitive Outcomes
On the HVLT-R, a significant main effect of time was observed for the recognition discrimination index t-score (P = .031), indicating that both groups experienced an improvement in recognition memory (Table 5). Likewise, a significant main effect of time was observed for the Digit Ordering Test total score (P = .038) and MMSE (P = .0002). In the secondary analysis, no differences were observed between groups from baseline to the 6-week assessment when comparing the HVLT-R and Trails A and B (Table 6).
Discussion
This study investigated the feasibility of community-based music-contingent gait training and its effects on cognition and mood in individuals with PD. Overall, the intervention was found to be well tolerated by participants who demonstrated high adherence without incident during training sessions. Falls reported during the intervention period were attributed by the participants to tripping or slipping while going about daily activities. The absence of falls during training sessions supports previous findings that walking with music is a safe method of gait training in PD. 18 Moreover, although a formal questionnaire was not administered to assess feasibility, participants anecdotally reported high satisfaction with the training apparatus. Research staff repeatedly fielded questions concerning its commercial availability.
Both training groups showed improved mood and anxiety although changes to cognition were minimal. The observed time effects (Tables 4 and 5) may have been a result of increased comfort with the assessments over the course of the study or random variability (eg, catching a participant on a “good” day). Observed improvements over time are not likely a result of assessment familiarity solely, because the majority of cognitive test scores were unchanged; participants neither improved nor deteriorated over the course of the study. The significant time effect that was observed on the Digit Ordering Test (total score), MMSE, and HVLT-R is unlikely to be clinically significant given that participants in both groups performed extremely well on the assessments at each time point (within normal clinical ranges where available). Moreover, the observed effects may be related to chance given multiple comparisons (Table 3). Nevertheless, these measures would be worth including in future studies given their relevance to patients with PD. There was no change in motor function or gait measures, including dual-task gait. Because there were no major between-group differences, we did not further adjust for baseline scores.
We found a time, but not group, effect of music-contingent training on several measures of cognitive function in the primary analysis. Although we had hypothesized that improvements in cognition would result for both groups, we did not see greater cognitive improvements with increased exposure to music-contingent gait training as hypothesized. There are several possible reasons for why improvements in cognition did not differ between music-contingent and control walking groups. It is possible that music-contingent training may preferentially benefit individuals with greater initial gait impairment. As described by Redgrave et al, 42 sensory inputs are received by both goal-directed and stimulus-response habitual control systems. Reliance on the goal-directed control system increases in individuals with greater motor impairment compared with those with less impairment in whom the habitual system may still be intact to a greater extent. In other words, sensory cueing in less impaired individuals may engage the goal-directed system to a lesser degree. Because the goal-directed system is the basis for music-contingent walking, those with greater initial impairment may benefit more from Ambulosono compared with those with milder impairment, who may use other strategies reliant on the habitual control system to maintain music play (eg, increasing walking speed to increase stride length by default rather than intentionally increasing stride length at a usual walking pace). Although UPDRS-III scores were statistically lower in the control group at baseline, both groups had mild clinical disease severity overall. 43 Because our participants had only mild to moderate impairment, goal-directed pathways may not have been optimally engaged in either group. It is also possible that the amount or intensity of contingent walking may not have been sufficiently different between the 2 groups given that only 6 weeks of noncontingent music listening was included in the control group. Previous goal-based exercise interventions in PD vary immensely in type/intensity (eg, dance, boxing, tai-chi, treadmill walking, resistance training) and duration (eg, from 4 weeks up to 16 months). 44 In fact, long-term follow-up of people with PD using Ambulosono has shown clear dosing effects, with individuals with greater initial motor impairment responding better clinically to high-dose Ambulosono. 45 On average, high-dose users completed 146 walks, 89 hours of training, and 9.2 walks/month over 15.6 months and saw an average decrease of 3 points on UPDRS-III score over a 13.4-month period. 45 In contrast, no significant changes were seen in low-dose users who averaged 45 walks, 23 hours of training, and 2.4 walks/month over a period of 17.6 months. This may suggest that physical activity rather than the music-contingent component may be responsible for improvements seen on UPDRS-III scores. In our study, users completed an average of 38 walks, 19 hours of training, and 12.7 walks/month over 3 months. Therefore, the current intensity and duration of our intervention may not have been sufficient to tease out the hypothesized effects of music-contingent walking. Although it is possible that the music component may lead to improvements in motor impairment and/or cognition via motivating individuals to be involved in physical exercise, these outcomes were not observed in this study.
There were significant improvements in anxiety and depression in both arms of the study. This finding is consistent with existing evidence that physical activity can lessen neuropsychiatric symptoms in parkinsonian and nonparkinsonian populations.46-49 Because music with high emotional valence has been demonstrated to have a strong inhibitory effect on the amygdala, 50 improvements in anxiety and depression may be explained by music exposure or familiarity with the testing situation. Anxiety in PD patients with freezing of gait is often associated with abnormal connectivity between the amygdala and putamen. 51 Our study did not target PD patients with freezing of gait; however, previous Ambulosono interventions have been shown to benefit this population. 22
Whereas the majority of PD gait training studies with external rhythmic cueing are conducted in gait laboratories, 52 a strength of our study is that Ambulosono training can be generalized to home and community environments and integrated into patients’ exercise routines and familiar walking routes. In this study, music was presented in an unaltered and randomized state (ie, without tempo fixing or cadence matching), similar to what participants would experience when walking with personal music devices. Given that a major critique of portable rhythmic auditory cueing devices is that their widespread availability is bottlenecked by investigational use development protocols, 53 an advantage of this study is that it used commercially available technology, which is not only more likely to already be familiar to patients but might expedite its clinical availability. Future software development should focus on smartphone technology given its utility, accessibility, and affordability in free-living environments. 54
Although this feasibility study was open to a spectrum of PD patients with compromised physical and cognitive abilities, the volunteers who participated were generally high functioning. A ceiling effect may have been present, whereby room for improvement was limited. Similarly, a volunteer bias may have been present; the majority of participants in this study reported high levels of physical activity in addition to the study’s prescribed gait training. In highly active participants, gait training may have comprised a mere fraction of overall activity, with the implication of participants completing more activity without music-contingent training than with it. The highly motivated nature of the study participants and small sample size may restrict the generalizability of our results to the parkinsonian population at large.
Technical aspects of the GaitReminder application require further development. Quantitative wearable sensors for use in PD have been promoted for their ability to provide relevant, factual, accurate, and continuous data in an objective manner. 55 However, to extract accurate and unbiased data, hardware and software resources must be capable of handling large quantities of multidimensional data. 56 Development issues in data transfer protocols, version stability, and database upgrades rendered walking data for some participants unfit for full post hoc group analysis. However, to the best of our knowledge, these issues did not interfere with the participants’ experiences of gait training because data were available in real time to research staff during the study for monitoring of performance and for regular provision of performance feedback. Based on available data and participant feedback, the intervention was carried out as intended. Although promising, as with many emerging technologies, additional software development is required before further research is recommended.
Conclusions
To our knowledge, the effects of community-based music-contingent gait training on cognition and mood in individuals with PD have never before been investigated. Music-contingent gait training is a promising technology with which to enhance the experience of gait training in individuals with PD beyond rhythmic auditory stimulation. Although we did not see clear cognitive improvements in this feasibility study of high-functioning individuals with PD, future studies should investigate the effects of music-contingent gait training on individuals with cognitive impairment given the documented benefits of physical activity on cognition in the literature. Similarly, the potential of music-contingent gait training to provide therapeutic reductions in anxiety and depression warrants additional investigation and may further support the use of such technologies in individuals with PD.
Supplemental Material
Ambulosono_CONSORT2010FlowDiagram – Supplemental material for The Effects of Music-Contingent Gait Training on Cognition and Mood in Parkinson Disease: A Feasibility Study
Supplemental material, Ambulosono_CONSORT2010FlowDiagram for The Effects of Music-Contingent Gait Training on Cognition and Mood in Parkinson Disease: A Feasibility Study by Jacqueline Burt, Einat (Natalie) Ravid, Sandra Bradford, Nancy J. Fisher, Yiye Zeng, Taylor Chomiak, Lesley Brown, Martin J. McKeown, Bin Hu and Richard Camicioli in Neurorehabilitation and Neural Repair
Supplemental Material
AmbuloSono_SupplementaryFigure – Supplemental material for The Effects of Music-Contingent Gait Training on Cognition and Mood in Parkinson Disease: A Feasibility Study
Supplemental material, AmbuloSono_SupplementaryFigure for The Effects of Music-Contingent Gait Training on Cognition and Mood in Parkinson Disease: A Feasibility Study by Jacqueline Burt, Einat (Natalie) Ravid, Sandra Bradford, Nancy J. Fisher, Yiye Zeng, Taylor Chomiak, Lesley Brown, Martin J. McKeown, Bin Hu and Richard Camicioli in Neurorehabilitation and Neural Repair
Footnotes
Authors’ Note
For individuals interested in further supplemental materials, please contact the corresponding author.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BH invented the Ambulosono data system and GaitReminder App, which is under investigational use, and is the founder of SonoStep Inc. The remaining authors declare no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.