
Abstract
Background. Context-dependent behavior is a phenomenon in which people demonstrate superior performance in the context where a motor task was originally learned, but show poorer performance in an unfamiliar context. Previous studies found that people with Parkinson’s disease (PD) demonstrated greater context-dependency than nondisabled adults. Moreover, the frontostriatal circuit appeared to play a role in mediating context-dependent behavior. Neuroimaging studies showed that people with PD and freezing of gait (FoG) had difficulty recruiting the frontostriatal circuit when performing a set-shifting task, known to be mediated by this neural network. Objective. This study aimed to investigate whether individuals with PD and FoG (PD + FoG) would be more context-dependent than those without FoG (PD − FoG). Furthermore, the association between context-dependent behavior and set-shifting ability would be determined. Methods. Sixteen individuals with PD + FoG, 15 participants with PD − FoG, and 15 nondisabled adults (Control) were recruited. The participants practiced 3 numerical sequences, each associated with a specific context. One day following practice, the participants were tested under 2 conditions: the sequence-context associations remained the same as practice or were changed. Set-shifting ability was measured by the Trail Making Test (TMT). Results. Compared to the PD − FoG group, the PD + FoG group showed a greater decrement in normalized motor performance when the sequence-context associations were changed. Context-dependency correlated with the TMT in the PD − FoG group but not in the PD + FoG or Control groups. Conclusion. While people with PD + FoG appeared to be more context-dependent than individuals without FoG, a relationship between context-dependent behavior and set-shifting existed only in those without FoG.
Introduction
Context-dependent behavior is a phenomenon in which an individual demonstrates superior motor performance in the environmental context where a motor task was originally learned, and may show poorer performance in a changed/different context. 1 While context-dependency is a natural phenomenon observed in the general population (eg, home-field advantage), it could become problematic if an individual over-relies on the environmental context to perform a well-learned motor task. For example, a patient may experience difficulty generalizing what he/she learns in the clinic back to the home environment.
An earlier study conducted by Lee and colleagues 2 found that people with Parkinson’s disease (PD) were more context-dependent than age-matched nondisabled adults when learning a finger sequence task. In the study, the participants were required to practice 3 numerical finger sequences. Unknown to the participants, each sequence was embedded within a specific incidental context (ie, colored circles and location on the computer screen) that was not essential for task performance. One day following practice, the participants were tested under 2 conditions: the sequence-context associations remained the same as practice or the sequence-context associations were changed from that of practice. It was observed that when the sequence-context associations were changed from practice, individuals with PD demonstrated a significantly greater decrement in motor performance than nondisabled adults. The findings suggested that people with PD were more obligated to the incidental contextual information when performing learned motor tasks. 2
Subsequent studies further demonstrated that context-dependent behavior was associated with the frontostriatal circuit, neuronal connections between the prefrontal cortex and the dorsal striatum.3,4 A nonhuman primate study found that while the prefrontal cortex encodes all available information (both intentional and incidental information) received from the environmental context, the dorsal striatum mainly functions as a modulator to select task-relevant information in order to produce the most appropriate movement to fit the context. 5 People with PD, with known striatal impairment, would have difficulty selecting task-relevant and filtering task-irrelevant information leading to an obligated context-dependent behavior as previously observed. 2 On the other hand, perturbing the neuronal processing of the prefrontal cortex using low-frequency repetitive transcranial magnetic stimulation (rTMS) led to a reduced context-dependency in nondisabled adults and in patients with PD.3,4 Altogether, our previous data suggest that a balanced neural activation of the prefrontal cortex and the dorsal striatum is important for generating appropriate context-dependent behavior.
From the review above, we were further interested in determining whether context-dependent behavior underlies freezing of gait (FoG), a debilitating clinical phenomenon of PD characterized by a sporadic onset of an inability to progress the feet forward despite the intention to walk.6,7 Individuals with PD who have FoG are known to have greater impairment of the frontostriatal circuit than those without FoG. 8 Using standardized neuropsychological tools, people with FoG demonstrated poorer executive function than nonfreezers, especially set-shifting ability.6,9,10 Functional imaging studies also revealed that people with FoG have difficulty recruiting and activating the frontostriatal circuit when performing a set-shifting task.11,12 Since context-dependent behavior appears to be mediated by the frontostriatal circuit, this study aimed to determine whether people with PD and FoG are more context-dependent than those without FoG.
In addition to investigating the context-dependent behavior in participants with PD and FoG, we were also interested in understanding whether context-dependent behavior was associated with set-shifting ability. Set-shifting can be easily measured in the clinic by using the Trail Making Test (TMT). By establishing a relationship between context-dependent behavior and set-shifting ability, clinicians could quickly identify individuals with PD who may be more obligated to context-dependent behavior. It was hypothesized that an individual with a greater set-shifting deficit would also demonstrate greater context-dependency.
Materials and Methods
Participants
Three groups of participants, including individuals with PD and FoG (PD + FoG; n = 16; mean age = 68.13 ± 6.34; male/female = 9/7), individuals with PD who did not have FoG (PD − FoG; n = 15; mean age = 64.67 ± 4.42; male/female = 7/8), and age-matched nondisabled adults (Control; n = 15; mean age = 68.40 ± 5.08; male/female = 7/8) were recruited (Figure 1). Participants with PD were included if they were diagnosed with idiopathic PD, and classified as freezers or nonfreezers based on the New Freezing of Gait Questionnaire (NFOG-Q), 13 which was then verified by a chart review of the medical history. Nondisabled adults were recruited if they did not have any neurological disorders and were age-matched to the PD participants. Participants were excluded if they had difficulty following study instruction or had neurological or psychological disorders other than PD. All individuals signed an informed consent approved by the Institutional Review Board of National Taiwan University Hospital before participating in the study. This study conformed to the World Medical Association Declaration of Helsinki.
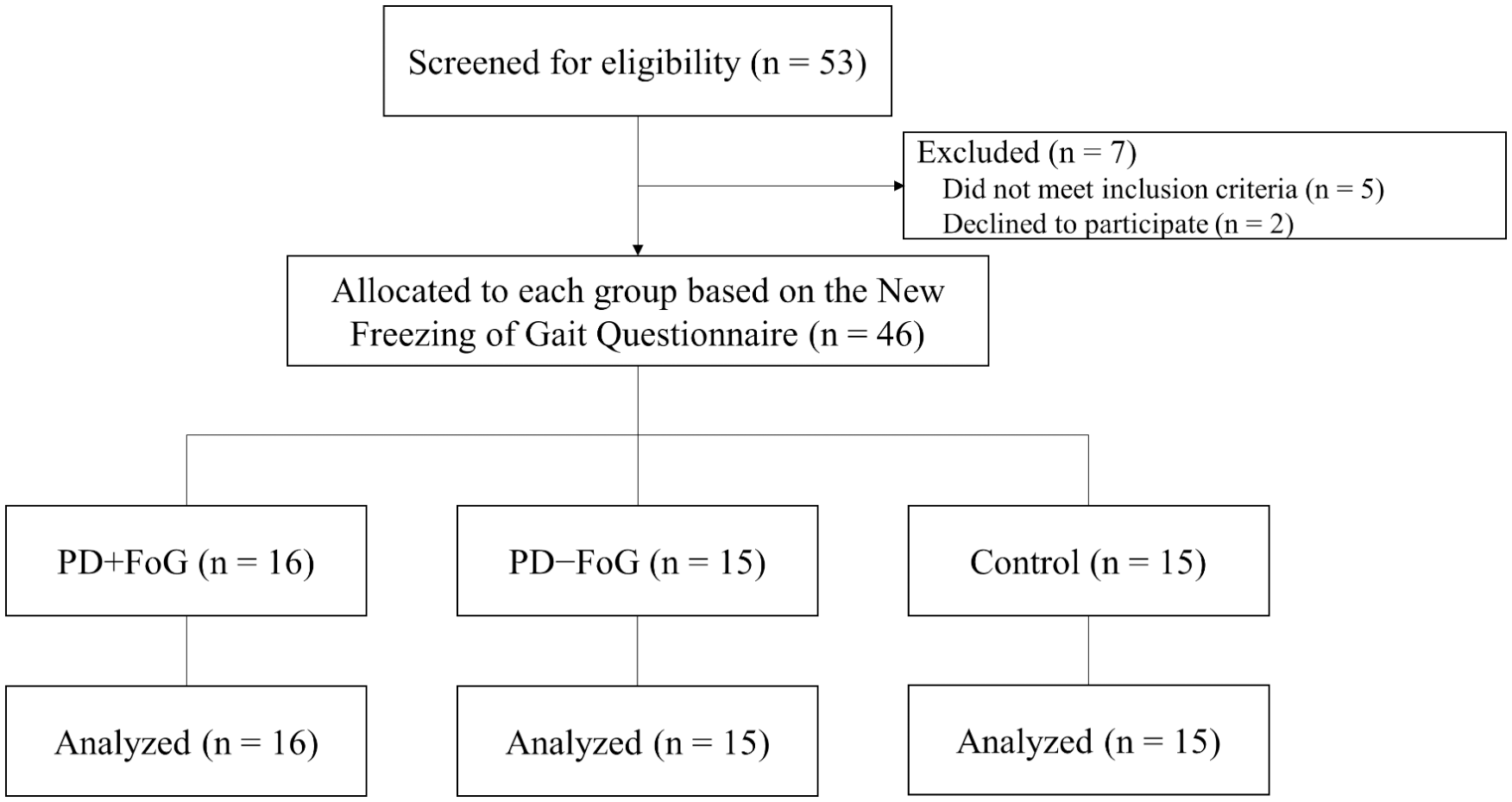
CONSORT flow diagram. PD, Parkinson’s disease; FoG, freezing of gait.
Study Procedure
The participants completed the study over 2 consecutive days with 24 hours apart. On arrival on the first day, the participants were examined with the Part III section of the Unified Parkinson’s Disease Rating Scale (UPDRS-III) to determine disease severity and the Montreal Cognitive Assessment (MoCA) to assess general cognitive function. 14 Following the MoCA, the participants completed the set-shifting assessment using the TMT and then practiced a finger sequence task. When the participants returned for the second day, they were required to complete the testing conditions (ie, SWITCH and SAME tests as described below) of the finger sequence task. All the participants with PD completed the study procedures during the “ON” medication cycle and at the same time of day to control for medication status.
Outcome Measures
Freezing of Gait
The NFOG-Q, composed of 3 parts, was used to classify individuals with PD into freezers and nonfreezers. 13 In the beginning of the questionnaire, a video clip with different freezing conditions was shown to the participants with PD, and they were asked whether they had similar experience(s) in the past month. A nonfreezer would be identified if a person answered “no” to this question. If an individual answered “yes,” he/she would be recognized as a freezer and was further required to complete the second and third parts of the questionnaire. Part 2 of the NFOG-Q assessed the severity of FoG according to the frequency and duration of the freezing episodes, while Part 3 evaluated the impact of freezing on daily activities. The psychometric properties of the NFOG-Q has been established to be good to excellent for patients with PD. 13
The Unified Parkinson’s Disease Rating Scale–Part III
The UPDRS was used to evaluate disease severity of the participants with PD. The original UPDRS consists of 4 main sections: (1) Mentation, Behavior, and Mood; (2) Activities of Daily Living; (3) Motor Examination; and (4) Complications of Therapy. 15 In this study, the patients were assessed with the Part III Motor examination section of the UPDRS. Test-retest reliability of UPDRS-III has been established to be good to excellent for early untreated patients with PD 16 as well as those in more advanced stages of the disease. 17
Montreal Cognitive Assessment
The MoCA has been identified as an appropriate measure to determine general cognitive function for people with PD. 14 It contains several cognitive domains, including executive function, visuospatial ability, short-term memory, attention, verbal fluency, calculation, digit span, abstract thinking, and orientation. The total score of the MoCA ranges from 0 to 30, with a higher score suggesting better cognitive function. The psychometric properties of the MoCA are good to excellent. 18
Context-Dependent Behavior
Context-dependent behavior was evaluated with a specifically designed finger sequence key pressing task. 2 The finger sequence task consisted of three 4-element numerical sequences for the participants to practice and learn. Unknown to the participants, each sequence was embedded within a specific incidental context, which were colored circles and 1 of the 3 locations on the computer screen (Figure 2). To minimize the confounding factor of movement difficulty between individuals with PD and nondisabled adults, all participants were instructed to place their index and middle fingers of both hands on the keys of C, V, B, N on an enlarged standard keyboard. The participants were instructed to view the sequence on the computer and press the corresponding key vertically aligned with the circled number on the computer screen in the sequential order of 1-2-3-4 as accurately and as fast as possible. For example, if the blue sequence shown in Figure 2A (sequence: 4-2-1-3) was presented on the computer screen, the participant would press “B” (as the number 1 would be in line with this key); then “V” (as the number 2 would line up with this key); followed by “N,” which aligns with the number 3; and finally the “C” on the keyboard aligning with the number 4. After completion of each trial, feedback regarding correct performance of the sequence and the amount of time to complete the sequence would be provided on the screen. The participants practiced the sequences in a pseudorandom order for 12 practice blocks. Each block contained 27 practice trials resulting in a total of 324 trials (108 trials per sequence) on the first day. The participants were given 3 to 5 minutes of rest after every 4 blocks of practice.
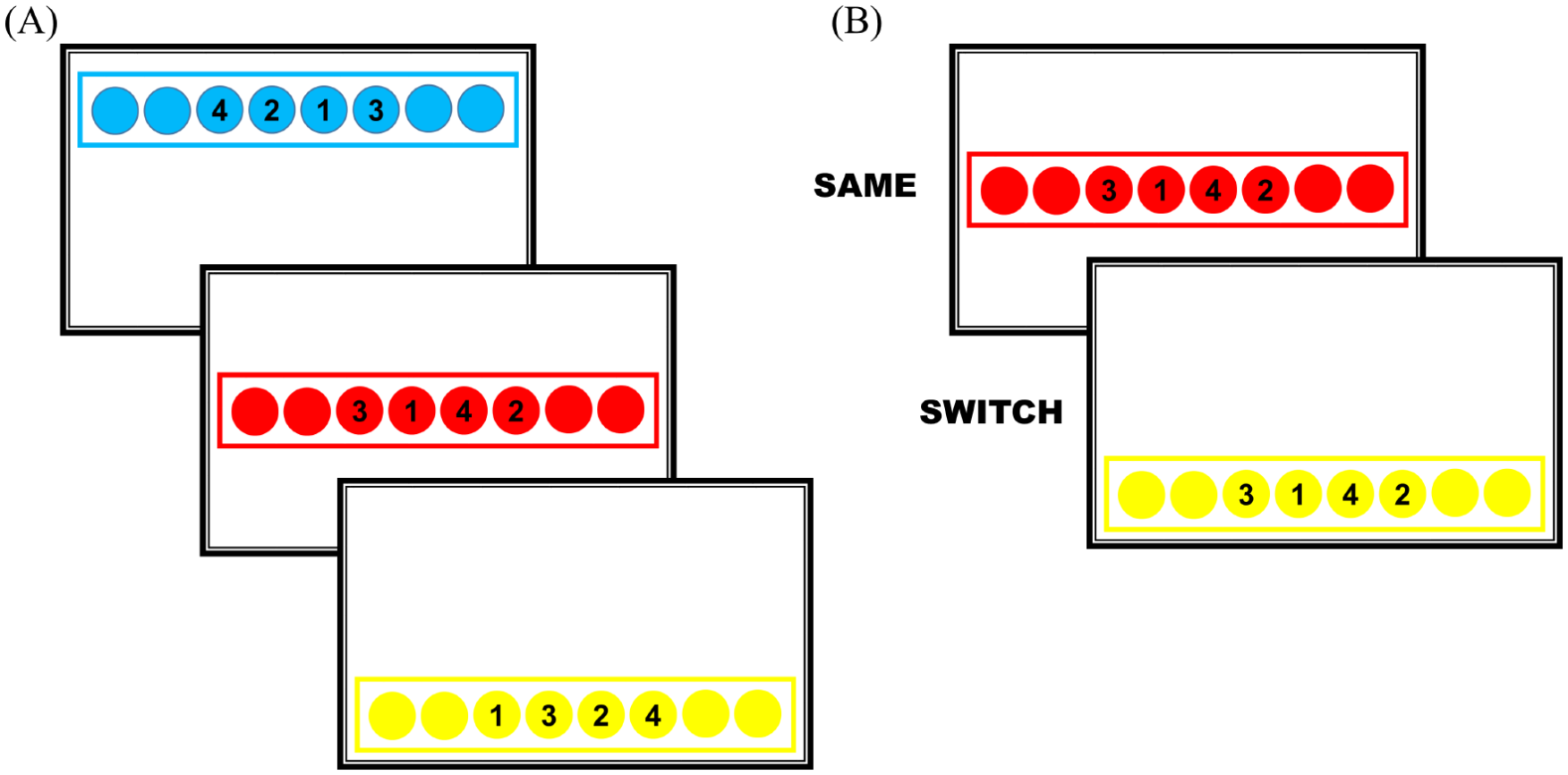
A figure illustration of the finger sequence task. (A) Three numerical sequences practiced on the first day. (B) An example of the SAME and SWITCH testing conditions on the second day.
All participants returned to the laboratory 24 hours after practice and were tested under the SWITCH and SAME testing conditions. Under the SWITCH condition, the original sequence-context associations changed from that of practice; while in the SAME condition, the sequence and context associations remained the same as practice (Figure 2B). The only difference between the 2 testing conditions was the incidental context associated with the sequences, while the finger movements for the sequences were exactly the same. Nine trials (3 trials of each sequence) were completed under each testing condition. With these 2 testing conditions, we were able to calculate switch cost to represent context-dependency. 2 Switch cost was the performance difference between the SWITCH and the SAME conditions normalized by the SAME condition [100 × (SWITCH − SAME)/SAME condition]. Calculation of the switch cost enabled us to account for the baseline performance differences among the 3 groups.
The primary outcome measure for the finger sequence task was total time accuracy cost (TTAC), which took both movement speed and accuracy into consideration. Total time (TT) was the period from stimulus presentation to the participant’s last finger key press. An error trial occurred when an individual failed to carry out all 4 key presses in the correct order. In each practice and testing block, mean TT was normalized by performance accuracy (1 − error rate) to obtain TTAC (equation: mean TT of a block/accuracy of a block). Considering the potential movement difficulties for people with PD compared to nondisabled adults, calculation of TTAC enabled us to account for the different error rates and compare overall motor performance of the 3 groups during the acquisition and retention phases.19,20 With the second day testing results, switch cost of TTAC was then calculated to determine differences in context-dependent behavior among the 3 groups.
Set-Shifting Ability
To determine whether context-dependent behavior was associated with the set-shifting ability, the TMT was evaluated. The TMT is an easily administered neuropsychological test that has often been utilized to evaluate visuospatial tracking, visuomotor control, and set-shifting/mental flexibility. 21 The participants in this study were required to complete 2 parts, Part A (TMT-A) and Part B (TMT-B), of the Chinese version of the TMT. In TMT-A, participants were presented with an array of numbered circles and were required to connect the circles consecutively in numerical order. The array of circles in TMT-B contains numbers and letters, and the participants were required to connect the circles with alternating numbers and letters in a sequential order. 22 The participants were instructed to connect the circles as accurately and as fast as possible, and the time to complete each part was recorded. The time ratio between Part A and Part B (TMT-B/TMT-A) was used as a quantitative indicator of set-shifting ability. 23
Statistical Analysis
All data was analyzed with the PASW statistics 18.0 (SPSS Inc, Chicago, IL). To compare the baseline characteristics of the 3 groups, the χ2 test and 1-way analysis of variance (ANOVA) were used for dichotomous and continuous variables, respectively. To analyze the acquisition and retention data of the finger sequence task, a group (PD + FoG vs PD − FoG vs Control) by practice block repeated-measures ANOVA was used. One-way ANOVA was used to compare the group differences in TTAC switch cost. The Tukey’s post hoc tests were performed if interactions or main effects were found. In addition to P values, the partial η2 (η2 = SSb/[SSb + SSe], where SSb is the between-groups sum of squares and SSe is the error sum of squares from the ANOVA table) 24 was reported to determine the performance differences among the 3 groups. A partial η2 value ≥0.138 would suggest a large effect, ≥0.059 a moderate effect, and ≥0.010 a small effect. 24 Finally, the Pearson correlation coefficient analysis was performed to determine the relationship between TTAC switch cost and the TMT score. The significance level was set at α = .05.
Results
Basic Demographic Data
Basic demographic data for the 3 groups are presented in Table 1. The 3 groups did not differ in age, sex, and MoCA and TMT scores. The participants in the PD + FoG group had significantly longer PD diagnosis duration and higher UPDRS scores than those in the PD − FoG group, while there was no statistically significant difference between the 2 groups in the dosage of levodopa equivalent medication.
Baseline Demographic Data of the Participants a .
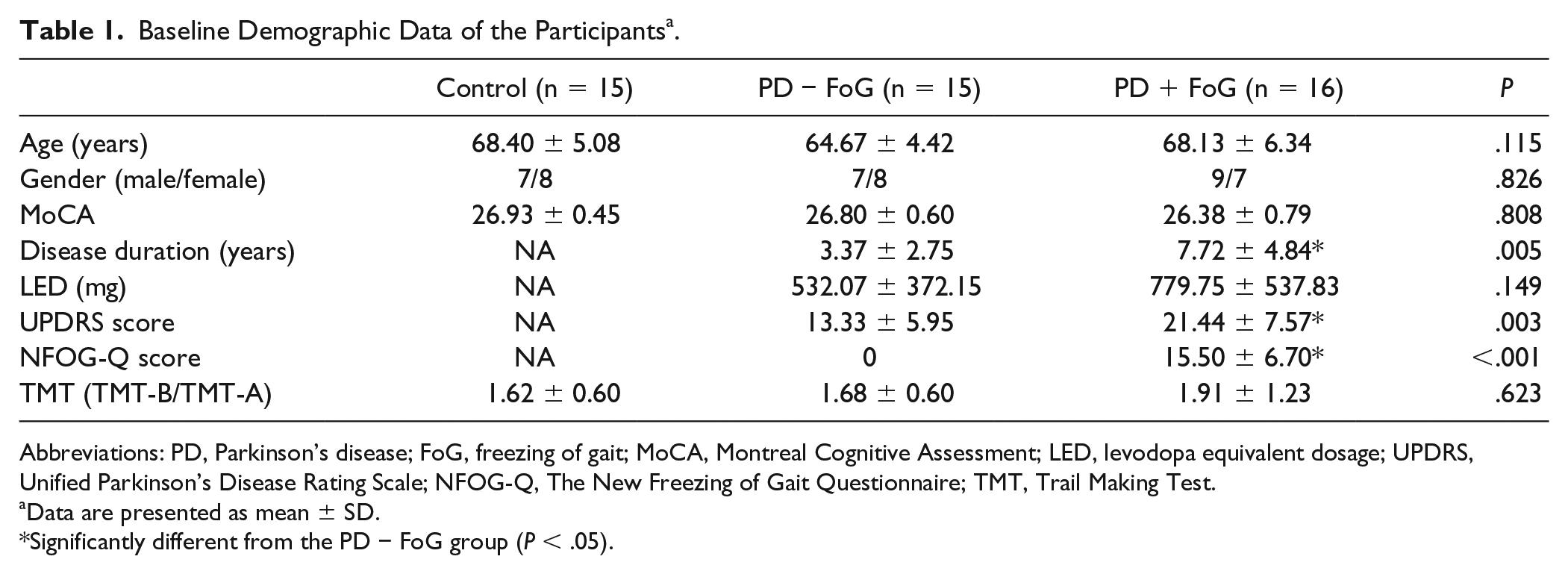
Abbreviations: PD, Parkinson’s disease; FoG, freezing of gait; MoCA, Montreal Cognitive Assessment; LED, levodopa equivalent dosage; UPDRS, Unified Parkinson’s Disease Rating Scale; NFOG-Q, The New Freezing of Gait Questionnaire; TMT, Trail Making Test.
Data are presented as mean ± SD.
Significantly different from the PD − FoG group (P < .05).
Context-Dependent Behavior
Group × practice block repeated-measures ANOVA of TTAC revealed a significant practice block main effect (F11,473 = 7.367, P = .001, η2 = 0.146), but no significant group main effect (F2,43 = 0.567, P = .572, η2 = 0.026) or group by practice block interactions (F22,473 = 0.443, P = .793, η2 = 0.020). These results showed that all 3 groups improved significantly throughout the first day of practice with no significant differences in the amount of improvement among the 3 groups (Figure 3).
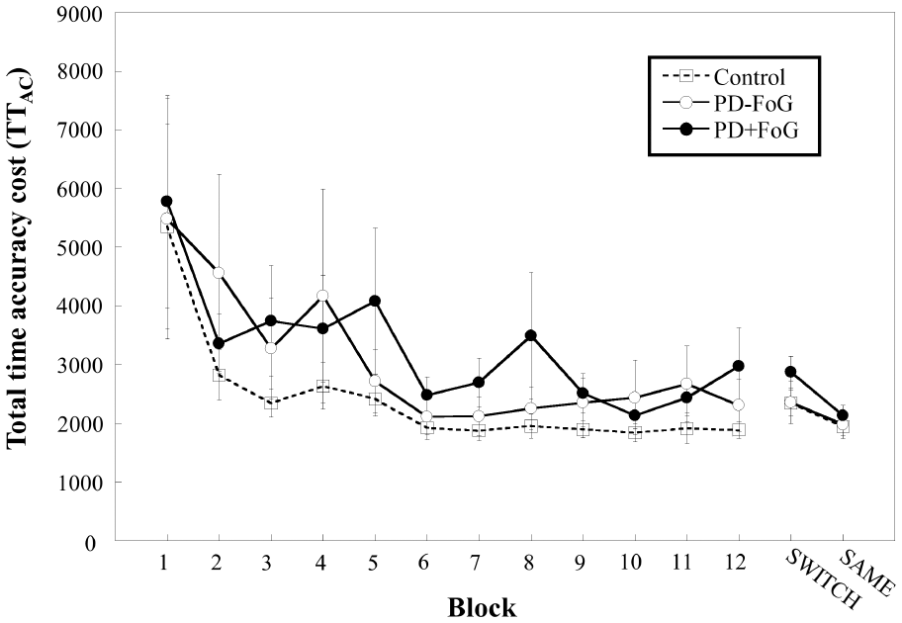
Total time accuracy cost (TTAC) throughout first day practice, and second day SWITCH and SAME testing conditions. Range bars represent standard error. PD, Parkinson’s disease; FoG, freezing of gait.
On the second day testing, repeated-measures ANOVA showed a significant testing condition main effect (F1,43 = 49.285, P < .001, η2 = 0.534) with no significant group main effect (F2,43 = 0.728, P = .489, η2 = 0.033) or group by testing condition interaction (F2,43 = 2.746, P = .075, η2 = 0.113). Post hoc analyses revealed that all groups had poorer performance under the SWITCH compared to the SAME testing condition (P < .001).
To take into account potential differences in baseline performance among the 3 groups, TTAC switch cost was calculated and analyzed. The result of the TTAC switch cost showed a significant group difference (F2,45 = 5.193, P = .010), and post hoc analysis showed that the PD + FoG group had significantly higher switch cost than the PD − FoG group (P = .010). A close to statistically significant difference was found between the PD + FoG and Control groups (P = .061), while there was no significant difference between the PD − FoG and the Control groups (P = .752; Figure 4).
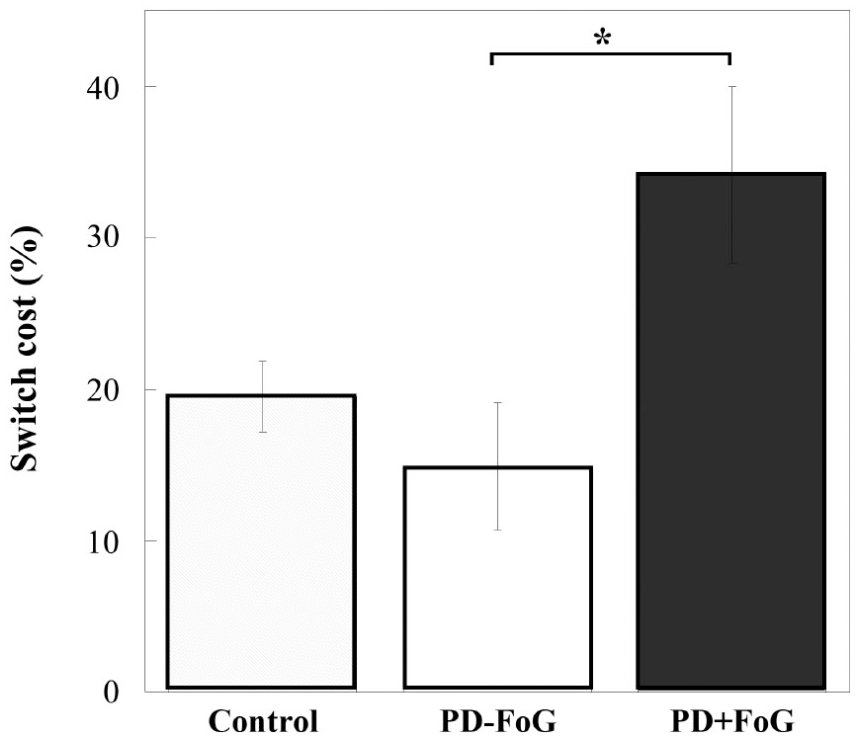
Total time accuracy cost (TTAC) switch cost of the 3 groups. Range bars represent standard error. *P < .05. PD, Parkinson’s disease; FoG, freezing of gait.
Correlation Analysis of Switch Cost and Set-Shifting Ability
Table 1 presents the set-shifting results using the TMT score of the 3 groups. There were no statistically significant group differences in the TMT score (F2,45 = 0.479, P = .623). The error rates also did not differ among the 3 groups (Control: 0.27 ± 0.80; PD − FoG: 0.27 ± 0.80; PD + FoG: 0.31 ± 0.70; F2,45 = 0.019, P = .982). Figure 5 shows the correlation results between TTAC switch cost and the set-shifting ability. For the PD − FoG group, TTAC switch cost significantly correlated with the TMT-B/TMT-A ratio (r = 0.700, P = .004). However, there was no significant relationship between the 2 variables in the PD + FoG group (r = 0.114, P = .675) or the Control group (r = 0.064, P = .822).
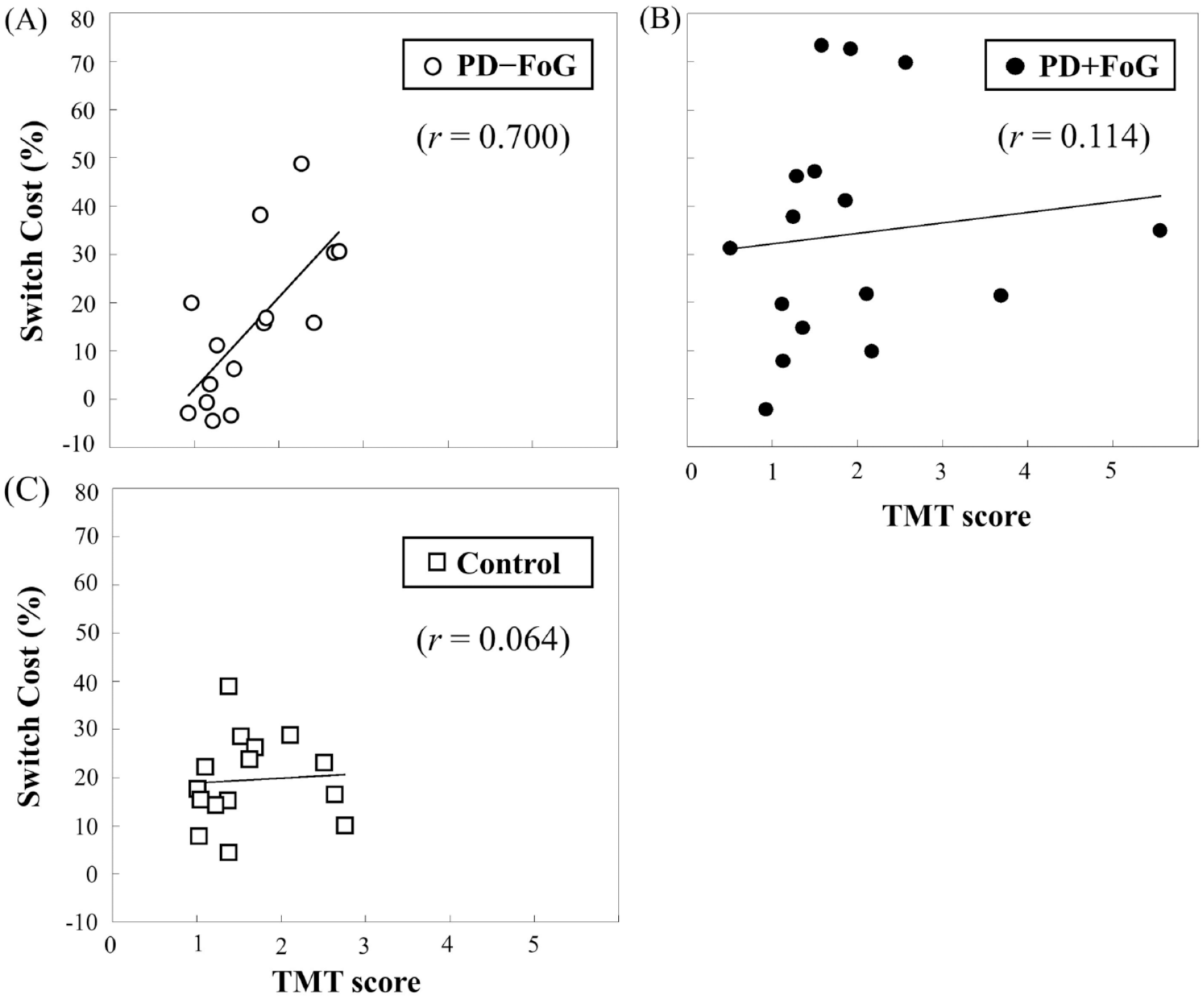
Pearson’s correlation results between TTAC (total time accuracy cost) switch cost and TMT (Trail Making Test) score for the (A) PD − FoG, (B) PD + FoG, and (C) Control groups. PD, Parkinson’s disease; FoG, freezing of gait.
Discussion
The first goal of this study was to determine whether context-dependent behavior underlies FoG by investigating whether people with PD and FoG were obligated to the incidental context to perform a learned motor task. The second goal was to determine whether context-dependent behavior correlated with set-shifting ability in people with PD. The main findings of this study were 2-fold. First, individuals with PD who had FoG were found to be more context-dependent than those who did not have FoG when performing a learned finger sequence task. Second, context-dependent behavior was associated with the TMT scores in the PD − FoG group, but not in the PD + FoG or Control group.
Clinical observations suggest that both intentional and incidental information from the environment have significant influences on motor behavior in patients with FoG. Intentional information could have “positive” or “negative” impacts on freezing behavior. For example, placing colored visual strips on the floor could improve walking ability for people with FoG (positive effect), 25 while walking through a narrow doorway may induce freezing episodes (negative effects). 26 While multiple studies have investigated the influences of intentional cues on motor behavior in people with FoG, it is not clear how incidental contextual information affects motor performance in people with FOG. Hence, this study aimed to investigate context-dependent behavior in individuals with PD + FoG. Using TTAC switch cost as an outcome to represent context-dependency, the results revealed that participants with PD + FoG were more context-dependent than those without FoG. The finding suggested that changes in the incidental context, even though the motor requirement of the task remained the same, significantly influenced motor performance in participants with PD and FoG.
The greater context-dependent behavior observed in people with PD + FoG could be related to the dysfunction of the frontostriatal circuit, also designated as the cognitive control network. The frontostriatal circuit, composed of the prefrontal cortex and the dorsal striatum, is responsible for effectively processing contextual information. 27 While evidence from animal and human studies showed that the prefrontal cortex encodes and updates all contextual information received from other cortical areas, the dorsal striatum selects and integrates task-relevant information for movement production. Thus, a balanced interplay of the prefrontal cortex and the striatum is important to generate appropriate movement responses according to the environmental stimuli.5,28-30 To successfully produce a movement, an interaction between the automatic (ie, the motor circuit) and the cognitive controlling processes (ie, the frontostriatal circuit) is crucial.28,31 When the processing in the automatic circuit is affected, the cognitive resources would become increasingly pressured. Compared with nondisabled adults or nonfreezers, people with PD and FoG appear to rely more on cognitive controlling processes to execute and accomplish a task. 31 Thus, a compensatory shift of neural activation from subcortical regions to prefrontal cortical areas would be expected. 31 Since the prefrontal cortex plays an important role in receiving and maintaining contextual information, increased neural activity of the prefrontal areas in individuals with PD + FoG would result in an encoding of all available (both intentional and incidental) contexts. Additionally, difficulty filtering task irrelevant information or incidental context as a result of striatal dysfunction in patients with PD and FoG would all together cause enhanced context-dependency in the PD + FoG group.3,4
Since cognitive function tends to decline as the disease becomes more severe over time, one might speculate that the enhanced context-dependency observed in the PD + FoG group may be a result of greater cognitive impairment. In the current study, the MoCA was examined and no significant group differences were observed, suggesting that the groups did not differ in gross cognitive function. Previous studies have shown that while people with FoG might not necessarily have poorer general cognitive function than nonfreezers, individuals with FoG appeared to have impairments in some specific cognitive domains, such as dual-task ability, attention, or executive function.31,32 Since a comprehensive cognitive assessment was not performed in the current study, we cannot rule out the possibility that the obligated context-dependent behavior observed in people with PD + FoG might be due to cognitive deficits not detected by the MoCA. Future studies that involve a more thorough cognitive examinations are needed to unravel this issue.
One thing to note is that the TTAC switch cost of the PD + FoG group was only close to being significantly greater than the Control group (P = .061). There was also no significant group by testing condition interaction (P = 0.075, η2 = 0.113) in the raw data of TTAC on the second day testing conditions (Figure 3). These non–statistically significant differences were probably the result of large variations in the characteristics of patients with PD and FoG. Individuals with PD + FoG in the current study had a wide range of disease duration and disease severity. Additionally, people with FoG have been shown to fatigue more easily and have greater depression than those without FoG. 33 Last, usage of levodopa and related medications may alter the neural networks and contribute to the variability of patients with PD, especially those with FoG.34,35 These factors all together may contribute to greater variability of motor performances for patients with FoG.
A previous study showed that patients with PD in general were more context-dependent than age-matched controls, 2 while the results from this study showed no group differences between the Control and the PD − FoG group. The differences between the 2 studies may be the result of different patient characteristics. In the previous study, participants diagnosed with PD were recruited regardless of whether they were identified as freezers or nonfreezers. In addition, set-shifting ability or the function of the frontostriatal circuit of the participants from the previous study was not known. Thus, it is possible that the previous data were largely driven by participants with PD who would be considered freezers or those with greater set-shifting deficits. The design of the current study could facilitate a deeper understanding of the characteristics of patients who may demonstrate context-dependent behavior.
Different from our initial hypothesis, the correlation results showed that context-dependent behavior was associated with set-shifting ability only in the PD − FoG group, but not in the Control nor the PD + FoG group. Since previous studies have already shown that set-shifting ability and context-dependent behavior are both mediated by the frontostriatal circuit,3,36 it was initially hypothesized that an individual with greater frontostriatal dysfunction would show a greater set-shifting deficit as well as greater context-dependency. However, this anticipated relationship was only observed in the PD − FoG group; those individuals who had greater set-shifting deficit also had greater switch cost (Figure 5A). It is possible that dopamine depletion was more restricted to the putamen and dorsal caudate for the nonfreezers; thus, the frontostriatal circuit was less disrupted.28,37 As the disease progresses and the frontostriatal circuit becomes more involved, an individual with PD might demonstrate greater difficulty performing the set-shifting task, 38 while at the same time demonstrate greater difficulty selecting task relevant information leading to a larger switch cost. This is clear in the nonfreezer group, in which a strong linear relationship was found between greater switch cost and greater time to complete the TMT (Figure 5A) could be owing to the progressive disruption of the frontostriatal circuit.
On the contrary, no correlations were observed between set-shifting ability and switch cost in the Control nor the PD + FoG group. We speculate that the findings could be related to the neural resources available in the brain. The frontostriatal circuit is presumably intact in nondisabled adults, and both the prefrontal cortex and the striatum have the capacity to perform the set-shifting task as well as process contextual information for the finger sequence task. 39 Thus, no correlation was observed between set-shifting ability and switch cost for the control participants. On the other hand, the nonsignificant correlation between the set-shifting task and context-dependent behavior in the PD + FoG group could be related to the pronounced reduction of “neural reserve.” Because of the severely disrupted and limited neural resource of the frontostriatal circuit, individuals with PD and FoG may suffer from a decreased compensatory capacity and would have to utilize all available neural resources in order to appropriately perform a motor task.40,41 Neuroimaging studies have found that people with FoG activated extended cortical areas and neural network to process multimodal information leading to a less efficient use of the neural resources. 41 Due to the reduced neural reserve, participants with PD + FoG would probably utilize all available neural resources and not only the frontostriatal circuit when performing the TMT or the finger sequence task. Hence, no correlation could be found between these 2 tasks in this group.
One possible limitation of this study was that all PD participants were evaluated during the “ON” medication cycle; thus, the performance during the “OFF” phase is not known. It is recognized that dopaminergic medications can improve some cognitive functions, while impairing others. 42 Patients with PD who took medication were found to have better performance on set-shifting tasks than during an unmedicated condition.42,43 This may explain the nonsignificant differences in the TMT score between the 3 groups (Table 1). It is yet unclear whether medication would exacerbate or alleviate context-dependent behavior in people with PD. Thus, future studies are needed to address this issue in order to further understand the relationship between FoG and context-dependent behavior in a nonmedicated state. For the current study, we chose to test the participants “ON” medication because some patients with PD, especially those with FoG, might have great difficulty performing the finger sequence task during the “OFF” state. The participants were specifically requested to come to the laboratory at the exact time relative to medication intake on 2 consecutive days in order to control for medication status. Since patients with PD are required to take medication regularly, it is most logical and important to understand the learning abilities and/or deficits when the medication is on board.
The findings of this study have important clinical implications for people with PD. Since individuals with PD + FoG were found to be context-dependent, clinicians can no longer assume that training those patients in the clinic will transfer back to their home environment. As a result, optimal training benefits may occur if interventions are provided in the same environmental context in which the patients will perform the task. On the other hand, if the goal of a patient is to be able to carry out a learned motor task in various environmental conditions, then training could be carried out in a variety of contexts to challenge the patient’s ability to generalize what he/she learned in one environment to another. This treatment approach may also be suitable for individuals without FoG who demonstrate set-shifting deficits, since a set-shifting deficit was found to correlate with context-dependency in this patient population. Additionally, since context-dependent behavior is not easy to identify in the clinic, clinicians could administer the TMT to individuals with PD without a history of freezing to quickly gain insight as to whether the patient is prone to context-dependent behavior. By identifying individuals who may demonstrate context-dependency, a more effective training regimen could be determined.
Conclusion
The findings of this study suggested that context-dependent behavior may underlie FOG. People with PD who suffered from FoG, compared with nonfreezers, were more obligated to the incidental context to perform learned motor task. Correlation analysis revealed that context-dependent behavior was associated with TMT in the PD − FoG group but not in the Control or PD + FoG groups, suggesting that the frontostriatal circuit may be differentially active to perform set-shifting and context switching in the 3 groups.
Footnotes
Authors’ Note
This study was conducted at the School and Graduate Institute of Physical therapy, College of Medicine, National Taiwan University. The Institutional Review Board of National Taiwan University Hospital approved the study protocol. Clinical registration number: NCT02987140.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science and Technology (MOST 105-2314-B-002-202 and 106-2314-B-002-044-MY3).