
Abstract
Background
Freezing of gait (FOG) in Parkinson’s disease (PD) is associated with gait asymmetry and switching difficulty. A split-belt treadmill may potentially address those deficits.
Objective
To investigate the immediate and retention effects of one-session split-belt treadmill training (SBT) in contrast to regular tied-belt treadmill training (TBT) on gait asymmetry and adaptation in people with PD and FOG (PD + FOG) and healthy controls (HC). Additionally, to investigate differential effects of 3 SBT protocols and compare different gait adaptation outcomes.
Methods
PD + FOG (n = 45) and HC (n = 36) were randomized to 1 of 3 SBT groups (belt speeds’ ratio 0.75:1; 0.5:1 or changing ratios) or TBT group. Participants were tested at Pre, Post, and Retention after one treadmill training session. Gait asymmetry was measured during a standardized adaptation test on the split-belt treadmill
Results
SBT proved beneficial for gait adaptation in PD + FOG and HC (P < .0001); however, HC improved more. SBT with changing ratios demonstrated significant effects on gait adaptation from Pre to Post in PD + FOG, supported by strong effect sizes (d = 1.14) and improvements being retained for 24 hours. Mean step length asymmetry during initial exposure was lower in HC compared with PD + FOG (P = .035) and differentiated best between the groups.
Conclusions
PD + FOG improved gait adaptation after a single SBT session although effects were smaller than in HC. SBT with changing ratios was the most effective to ameliorate gait adaptation in PD + FOG. These promising results warrant future study on whether long-term SBT strengthens adaptation in PD + FOG and has potential to induce a better resilience to FOG. Clinical trial ID: NCT03725215.
Introduction
People with Parkinson’s disease (PD) show various gait disturbances, including reduced step length and gait speed.1,2 Additionally, individuals with PD may suffer from freezing of gait (FOG), a highly disabling symptom prevalent in about 38% of early PD, and increasingly present in those with greater disease severity. 3 FOG is characterized by a “brief, episodic absence or marked reduction of forward progression of the feet despite having the intention to walk.”4,5 FOG is thought to occur when multiple gait deficits deteriorate simultaneously and thus surpass the FOG-threshold. 6 Among these gait deficits are a higher gait variability, higher gait asymmetry, and worse bilateral coordination of gait.7-9 Furthermore, FOG often occurs when gait needs to be adapted to external requirements, such as during turns, walking through narrow passages or when initiating gait. 10 Additionally, cognitive load when performing a dual task may elicit FOG. 11 As well as motor switching deficits, people with FOG (PD + FOG) show more difficulty with cognitive set shifting12,13 compared to those without FOG (PD − FOG). 14 The association between FOG and motor adaptation deficits is further supported as walking on a split-belt treadmill under changing belts’ speed conditions elicited FOG episodes, 15 even if not many. Besides adaptation, split-belt walking challenges bilateral coordination of gait and asymmetrical walking. 16
Split-belt walking has been investigated in healthyindividuals17-19 as well as in various neurologicalconditions,20-23 including PD (for review see Seuthe et al 24 ). Most studies have focused on the immediate split-belt walking effects on gait adaptation, tied-adaptation (when the belts return back to tied speed) and readaptation (when split-belt walking is repeated) in one session using steady contrasts between belt speeds of 0.75:1 or 0.5:1. In PD, these studies revealed that adaptation was not significantly different during early (first 5 strides) split-belt walking in people with PD compared with healthy controls (HC). 19 Additionally, adaptation ability was reduced in PD + FOG compared with PD − FOG15,25 and after effects were greater with levodopa intake. 26 Finally, PD + FOG had impaired speed difference perception compared with PD − FOG 27 during split-belt walking. Split-belt conditions can incur gait perturbations subconsciously, demanding largely implicit adaptation to asymmetrical conditions, but whether this can also lead to substantial changes in the capacity to adapt in daily life is still unclear. Interestingly, a recent study showed that implicit surface perturbation training in older adults was retained and led to reduced injurious falls over a period of 3 months. 28 This led to the hypothesis that split-belt training (SBT) may lead to maintaining of adaptive behavior in PD. If consolidated gait adaptation could be achieved after prolonged and progressive exposure (not investigated here), it is possible that individuals with FOG could develop a more resilient gait pattern for handling FOG-provoking circumstances. However, even the short-term training responses to split-belt perturbations in one session are still unknown in PD. Also, it is unclear which split-belt contrasts would lead to the best practice results. Besides the split-belt contrasts, it is also still not known if SBT is superior to regular treadmill walking to improve FOG related gait deficits. Although regular treadmill training is successful in improving several gait measures such as gait speed and stride length,29,30 its effects to improve adaptation ability is not known yet in PD.
For all these reasons, we conducted a proof-of-principle study into the effects of SBT on gait adaptation in PD + FOG. First (aim 1), we aimed to investigate if SBT versus tied-belt training (TBT) led to similar immediate gains and retention in healthy individuals as in PD + FOG. Second (aim 2), we wanted to determine which of the following 3 SBT-contrasts was most effective to improve gait adaptation and asymmetry in PD + FOG: (1) SBT75 with a belt speed ratio of 0.75:1, 15 (2) SBT50 with a belt speed ratio of 0.5:1 20 have been used previously in PD to target adaptation, and (3) SBTCR changing ratios, which was newly introduced to bring in a switching component, not addressed by the steady contrasts. Previous studies, quantified gait changes during SBT-walking using gait asymmetry outcomes. Hence, as a third aim, we explored which outcome best captured gait adaptation differences when comparing PD with HC in a standardized test protocol, which we developed for the purpose of this study.
Methods
This study was conducted at Christian-Albrechts-University (CAU) Kiel, Germany and Katholieke Universiteit (KU) Leuven, Belgium. Regular meetings were held either at one of the sites or online to design the trial and to get a detailed view of the conditions at each site. Furthermore, during a pilot period, one of the testers from Kiel visited the Leuven laboratory to follow assessment and training in order to ensure high comparability of the procedures, instruments and environment between the centers. The trial was registered at ClinicalTrial.gov (ID: NCT03725215). Participants were included in this study between January 2018 and May 2019. Recruitment was continuously ongoing during this period.
Participants
A total number of 45 individuals with PD + FOG and 36 healthy age-matched controls (HC) were included in the study. People with PD were included if they were diagnosed with idiopathic PD with confirmed FOG according to the New Freezing of Gait Questionnaire (NFOG-Q, item 1), 31 had no other neurological diseases and a stable medication for at least 4 weeks. Age-matched HC were included if they had no history of neurological disease. Exclusion criteria for both PD and HC were (1) unable to walk without assistive devices (eg, walking aid) for a minimum of 5 minutes, (2) cognitive impairment (Mini Mental State Examination [MMSE] ≤24), 32 and (3) orthopedic or other health conditions that could influence walking. None of the participants had previous SBT experience. The study was approved by ethical committees of CAU Kiel (Approval number: D 454/13) and KU Leuven (Approval number: B322201734218) and participants gave written informed consent prior to participation.
Study Design
We employed a nonblinded randomized controlled design. Participants were randomly allocated to 1 of 4 training groups (SBT75; SBT50; SBT-CR and TBT) stratified by H&Y (Hoehn and Yahr) stage (PD + FOG) and age (HC). Random blocks were generated for each H&Y stage and each age group to ensure balanced distribution among training groups. Randomization was performed by an external person in each center who was not involved in the conduct of the study. The study protocol consisted of 3 assessments, which were conducted before (Pre), after (Post), and 24 hours after (Retention) the training session to investigate short-term consolidation (Figure 1).
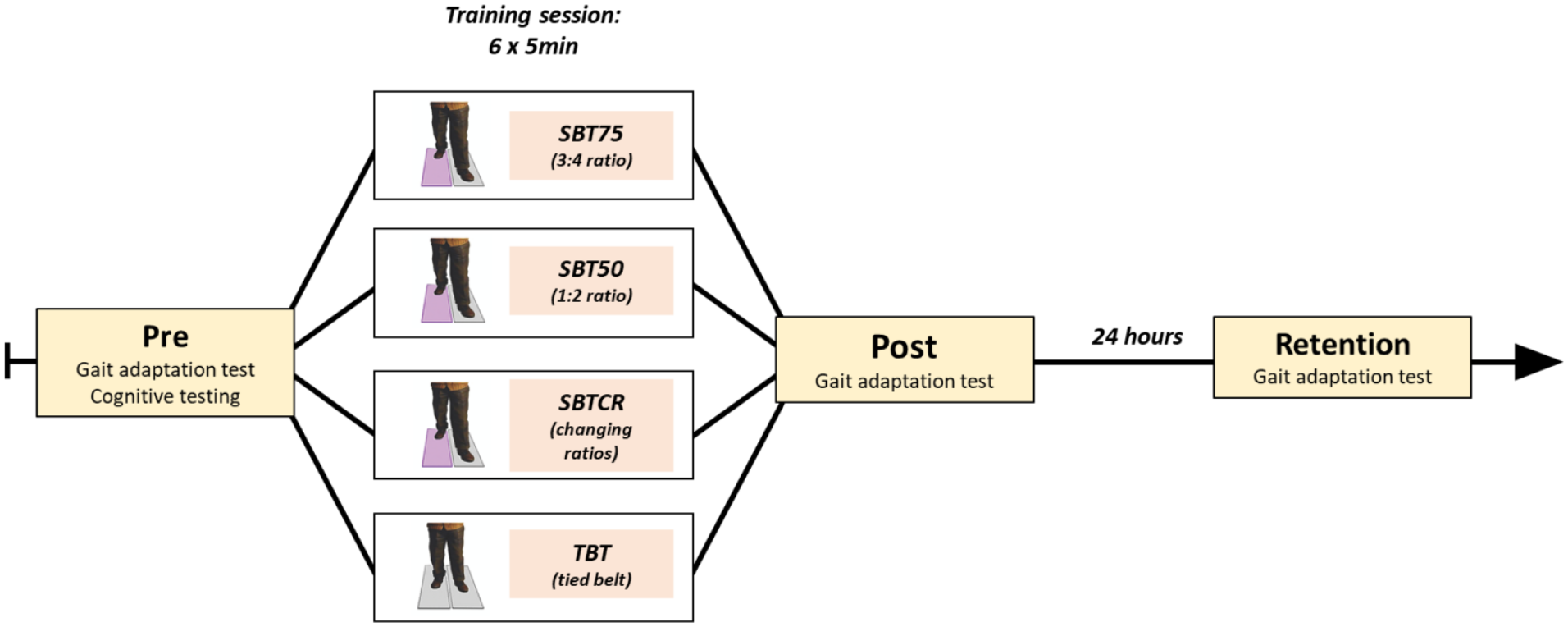
Study protocol with Pre, Post, and Retention assessment and training groups.
Testing and training were conducted in the ON state of medication. Medication intake was recorded and rigorously standardized between tests. Subjective self-reported medication status was checked at the beginning of the tests. Subjects were asked to walk without holding onto the handrails of the treadmill if possible. Participants who could not walk without holding the handrails, always kept their hands onto the handrails. During testing and training, all participants wore a safety harness (climbing harness with shoulder straps, a middle strap around the hips and leg loops) secured to the ceiling without providing body weight support.
Standardized Gait Adaptation Test
To test the ability of people with PD + FOG to adapt to changing gait conditions, we designed an adaptation test in which participants had to walk on the split-belt treadmill for 90 seconds (see Figure 2). For the first 30 seconds, belts ran at the participants’ comfortable over-ground speed (Tied-Baseline), which was assessed through prior over-ground gait analysis with reflective markers using initial and terminal contact for the calculation. 33 Then, speed was reduced by 50% on one side for 30 seconds (Split-Adaptation). Next, both belts were brought back to the same speed for 30 seconds (Tied-Adaptation) (Figure 2.) Thus, 2 switches of belt speeds were administered per test. The belt speed switches were administered by a computerized protocol. The gait adaptation test was performed twice so that both legs were exposed to the reduced belt speed and this at the 3 time points (Pre, Post, and Retention). The order of the leg that was reduced first was counterbalanced across participants but kept consistent within each participant.
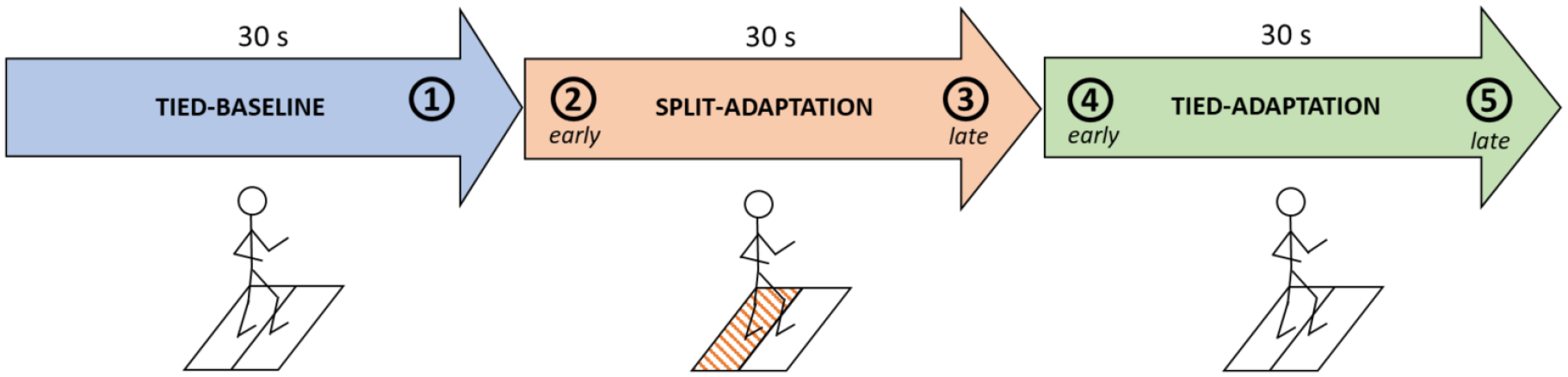
Split-belt treadmill (SBT) adaptation test (shaded area indicates a reduction of belt speed by 50% on one side; phases: 1 = baseline, 2 = early-split, 3 = late-split, 4 = early-tied, 5 = late-tied.).
Descriptors and Outcome Measures
At Pre assessment, the Movement Disorders Society–Unified Parkinson’s Disease Rating Scale Part III (MDS-UPDRS-III) was assessed (PD only). Cognitive and balance functions were tested using the Montreal Cognitive Assessment (MoCA) and the Mini-Balance Evaluation System Test (Mini-BESTest), respectively.
At Pre, Post, and Retention, gait was measured using six reflective passive markers placed at the lateral malleolus and heel and tip of the shoes of both right and left foot, allowing precise measurements with limited skin movements. Gait parameters were calculated with custom Matlab scripts 34 using 3D data from a motion capture system (Kiel: Qualisys Motion Capture Systems; Leuven: Vicon Motion Systems Ltd). Both systems were calibrated according to the respective manufacturers instructions before each test session and provide highly comparable results. 35 Sampling frequency was 100 Hz. Test-retest and interrater reliability has been reported to be good for this method. 36
Step length asymmetry and limb excursion asymmetry were calculated following according to previous SBT research 24 :
For this formula, a value of “‘0’” indicates perfect symmetry, positive values indicate a longer step length of the fast leg and negative values a longer step length of the slow leg. Limb excursion was calculated as the distance traveled during the stance phase while walking on the treadmill. 37 To get one overall measure of gait adaptation, gait variables were averaged over the whole adaptation test (90 seconds). This was done to simplify the model allowing to investigate the various interactions between group, training group, and time points (Pre, Post, Retention). In order to investigate the changes in gait adaptation in more detail for the different training groups, parameters were evaluated at the different parts of the adaptation test (averaged over the initial 5 seconds in the part) including (1) baseline, (2) early-split, (3) late-split, (4) early-tied, and (5) late-tied (Figure 1).
Physical and mental fatigue were measured using visual analogue scales in the style of a visual analogue scale to evaluate fatigue severity (VAS-F) 38 prior to and immediately after the training.
Treadmill Training
Participants were trained for 30 minutes in blocks of 5 minutes with a 1-minute rest between blocks. They completed 1 of 4 different training protocols: The 3 SBT training groups trained with a reduction in speed of one belt of 25% (SBT75) or 50% while the other belt run at 100% of their individual over-ground gait speed. The first group trained with one belt running at 75% (SBT75) of the individual over-ground walking speed, the second group with one side at 50% (SBT50) and the third group trained with one belt changing between 50% and 75% (SBTCR, for details see Supplementary Material S2) while the other belt ran at 100% of the individual over-ground gait speed. For SBTCR the belt speed switches were administered by a computerized protocol. The last group trained under tied-belt (TBT) condition with both belts running at the same speed. For SBT purposes, the leg with the initial longer step length during over-ground walking was reduced (best side reduction [BSR]), as previously Fasano et al 39 found this paradigm to have positive aftereffects in multiple gait domains (symmetry, bilateral coordination, sequence effect).
Statistical Analysis
Descriptive statistics for PD + FOG and HC contrast were compared using Mann-Whitney U tests. Furthermore, the Kruskal-Wallis test was used to test for baseline differences in age, disease severity, motor score, and cognitive state between PD + FOG in the 4 different training groups. With regard to study aim 1, multilevel regression models were applied to investigate the group × time × training-group interaction on mean gait adaptation variables with the factor group (2 levels: PD + FOG vs HC), the factor time (3 levels: Pre, Post, Retention), and the factor training-group (2 levels: pooled SBT vs TBT). To address study aim 2, the model was adapted and ran only for the PD + FOG group to investigate the training-group × time interaction for mean gait adaptation variables with the factor training-group (4 levels: SBT75, SBT50, SBTCR, and TBT) and the factor time (Pre, Post, Retention). Furthermore, to investigate the differences between the training groups and time points with regard to the different parts of the gait adaptation test the model was ran for each part (baseline, early-split, late-split, early-tied, and late-tied) separately. Models were run on the dependent variables step length asymmetry and limb excursion asymmetry for nonnormalized data as different baseline asymmetry was accounted for in the statistical models. Additionally, center (2 levels, Kiel and Leuven) and treadmill velocity were added as covariates to investigate potential influence on the results. The used models deal with missing data using maximum likelihood estimation. Normality of residuals was assessed with histograms and Q-Q plots. Post hoc tests were performed to interpret the effects using Tukey adjustment (95% confidence interval) for multiple comparisons. Furthermore, effect sizes (Cohen’s d) were calculated for the PD + FOG to compare effects of the different training modes for the reduction of step length asymmetry (Pre-Post) and interpreted as follows: large: d ≥ 0.8, medium: d 0.5 to 0.8, small: d 0.2 to 0.5. 40 Finally, in line with the exploratory aim, to verify which outcomes are most suitable to capture for gait adaptation ability (study aim 3), differences in mean gait asymmetry in PD + FOG and HC (at Pre) were tested using Student’s t test. To account for different baseline asymmetry, for this analysis mean gait asymmetry was normalized by subtracting baseline asymmetry during preceding tied-belt phase. Furthermore, outcome measures were Pearson correlated with measures of fatigue (visual analogue scale for physical and mental fatigue) and clinically assessed motor performance (MDS-UPDRS III). A priori sample size calculation was not conducted due to the proof-of-principle character of this study and the novelty of outcome measures. Statistical analysis was performed in RStudio software. 41
Results
PD + FOG and HC did not differ in baseline characteristics regarding age and sex. People with PD had compromised balance and cognitive function compared to HC (see Table 1). Furthermore, individuals with PD were evenly distributed amongst the 4 different training groups regarding age, cognition, disease duration, disease severity, FOG severity, and daily levodopa dosage. Eleven participants used handrail support during SBT walking (3 HCs and 8 PD + FOG) and there were no adverse events. The flowchart (S1) in the Supplementary Material presents the flow of subjects through the study. Table 2 illustrates that there was no difference in age, disease severity, and cognitive or motor function measures in PD + FOG between the 4 training groups (P range: .6-.84) with similar FOG-severity (P = .83).
Participant Characteristics (n = 81). a
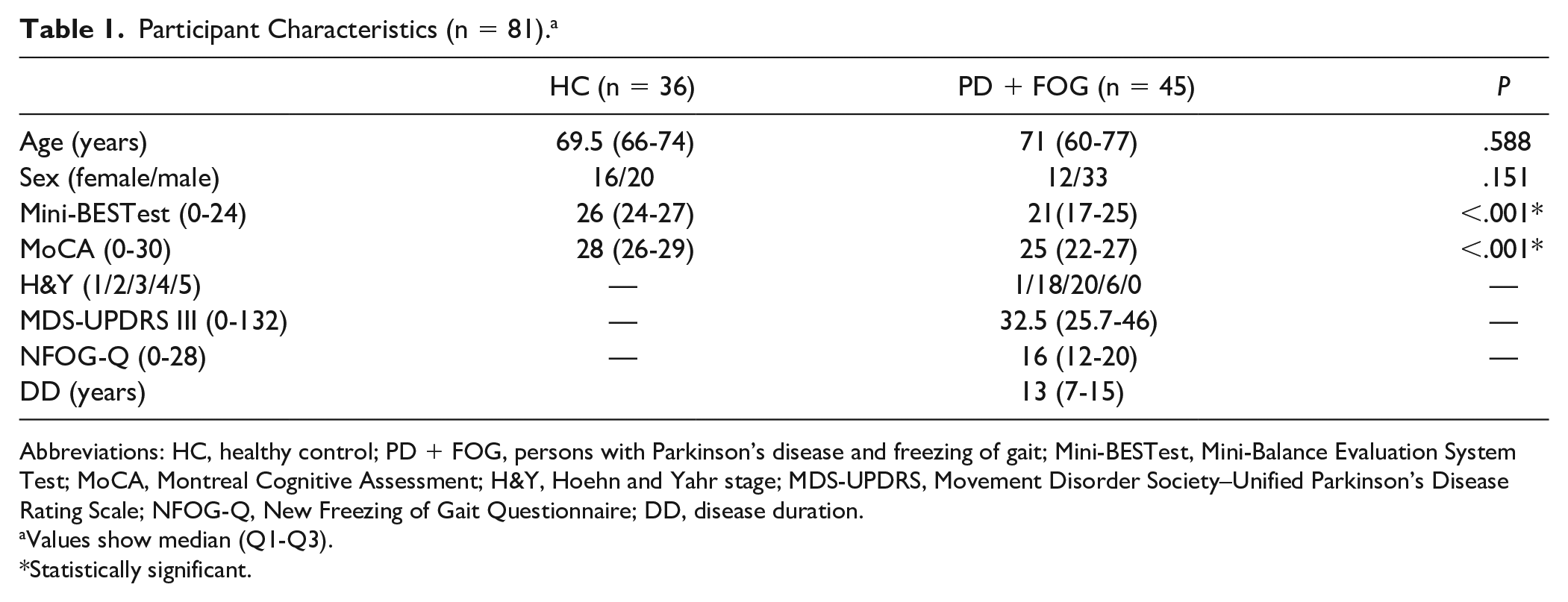
Abbreviations: HC, healthy control; PD + FOG, persons with Parkinson’s disease and freezing of gait; Mini-BESTest, Mini-Balance Evaluation System Test; MoCA, Montreal Cognitive Assessment; H&Y, Hoehn and Yahr stage; MDS-UPDRS, Movement Disorder Society–Unified Parkinson’s Disease Rating Scale; NFOG-Q, New Freezing of Gait Questionnaire; DD, disease duration.
Values show median (Q1-Q3).
Statistically significant.
Characteristics of Individuals With PD + FOG.
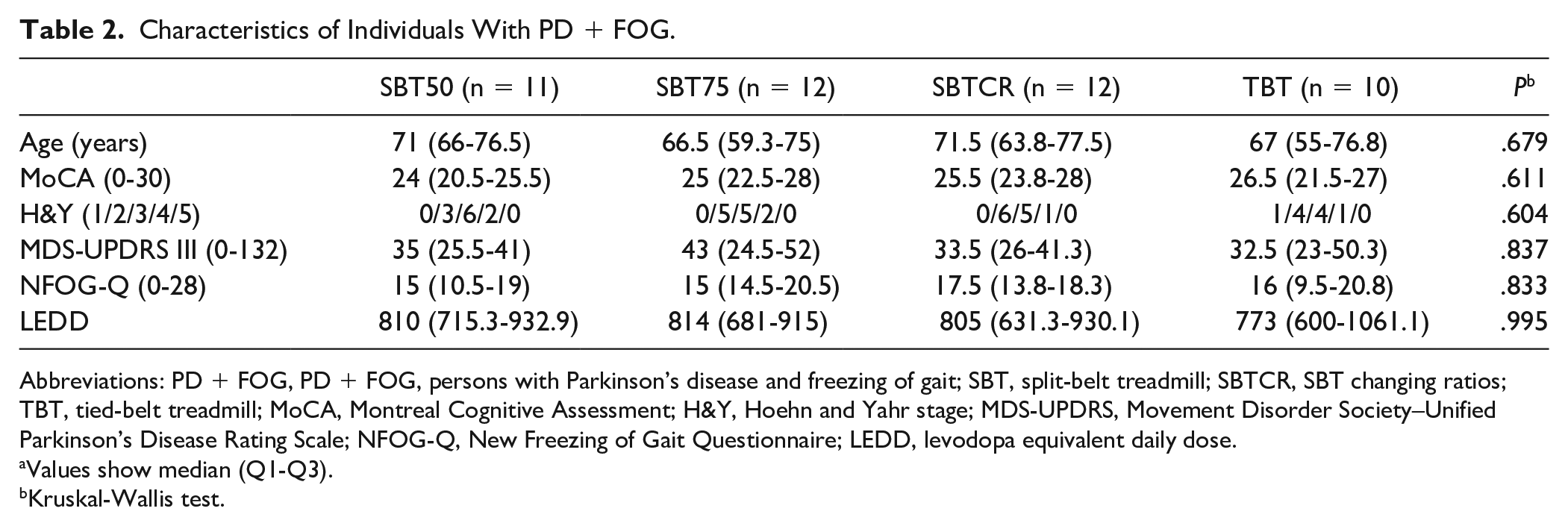
Abbreviations: PD + FOG, PD + FOG, persons with Parkinson’s disease and freezing of gait; SBT, split-belt treadmill; SBTCR, SBT changing ratios; TBT, tied-belt treadmill; MoCA, Montreal Cognitive Assessment; H&Y, Hoehn and Yahr stage; MDS-UPDRS, Movement Disorder Society–Unified Parkinson’s Disease Rating Scale; NFOG-Q, New Freezing of Gait Questionnaire; LEDD, levodopa equivalent daily dose.
Values show median (Q1-Q3).
Kruskal-Wallis test.
The following results will only focus on the gait adaptation test during which the belt side with the longer step length was reduced, as this was most aligned with the training purpose.
Effect of SBT in PD + FOG Compared With Healthy Controls
When investigating study aim 1, there was a significant group × time interaction (P = .005) for mean step length asymmetry, showing that HCs improved to a higher extent compared with PD + FOG, regardless of the training protocol they finished. Despite this finding PD + FOG did benefit from the training session as they could reduce their gait asymmetry significantly from Pre to Retention (P < .001). For the comparison of the training modes we found a significant training-group × time interaction (P < .0001) for the pooled SBT groups versus TBT for all participants. Post hoc tests revealed that mean step length asymmetry changed significantly in SBT groups (pooled data) from Pre to Post (P < .001) and Pre to Retention (P < .001), whereas no significant differences were found for the TBT group. Interaction of group × time × training-group for the pooled data (SBT vs TBT) was not significant (P = .249).
With respect to mean limb excursion asymmetry, no significant group × time × training-group, group × time, or training-group × time interactions were found.
PD + FOG showed significantly higher levels of physical fatigue (P < .0001) after the training compared with HC, but no correlation was found between fatigue and the reduction in step length asymmetry. However, motor performance as measured with the MDS-UPDRS III was associated with physical fatigue in people with PD, showing that those individuals with poor motor ability showed higher levels of physical fatigue after the training session (P = .02, r = 0.38).
Different SBT Training Protocols in People With PD + FOG
For the comparison of the different training groups within PD there was a significant training-group × time interaction for mean step length asymmetry (P = .015). Post hoc tests revealed that only the group that trained under changing ratios condition significantly reduced their mean step length asymmetry during the gait adaptation task from Pre to Post (P = .046, Figure 3). The effect sizes of the changes from Pre to Post for the SBT groups versus TBT group were as follows: SBT75% versus TBT: d = 0.81; SBT50 versus TBT: d = 0.63; and SBTCR versus TBT: d = 1.14.
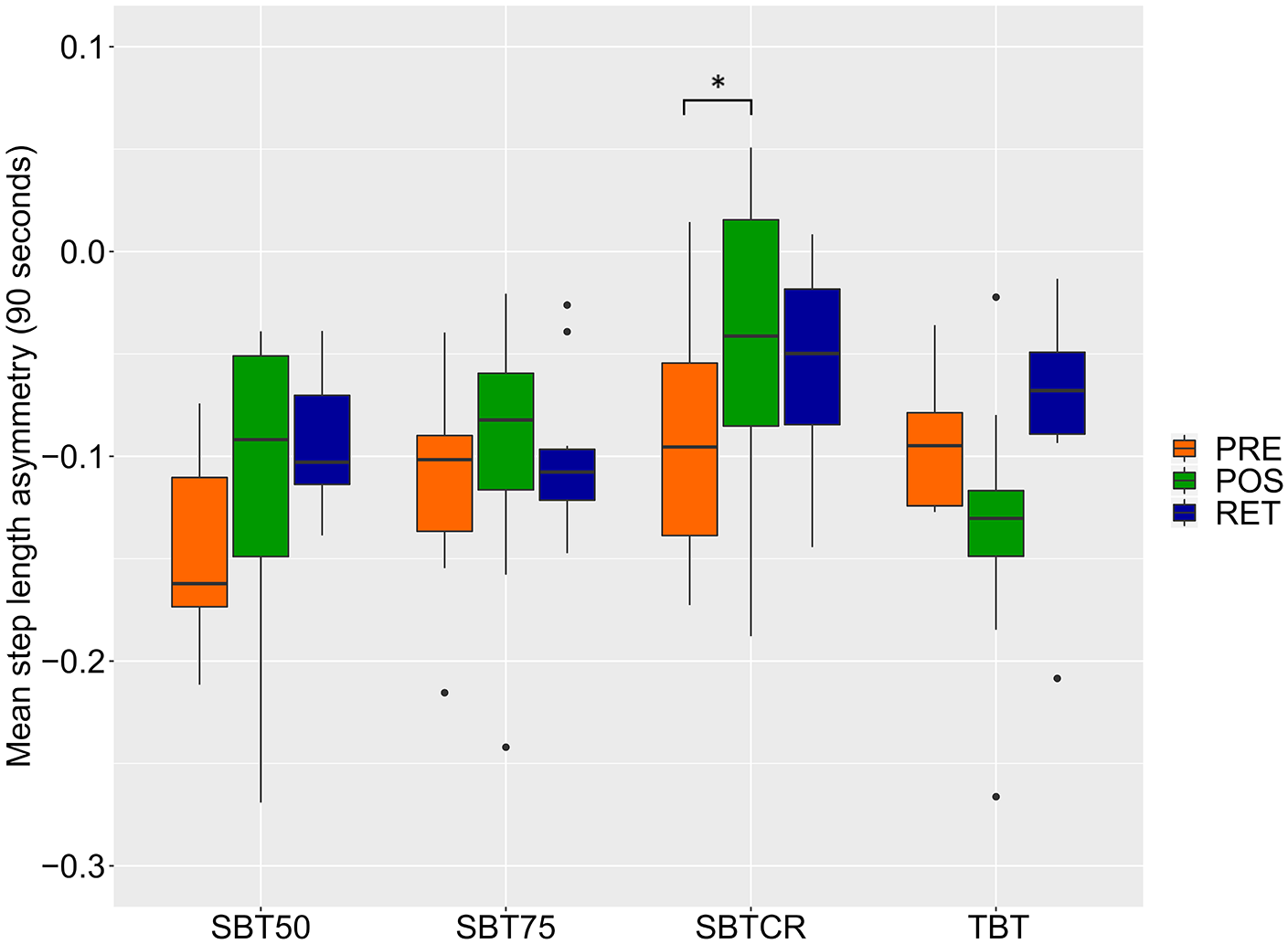
Mean step length asymmetry in people with Parkinson’s disease and freezing of gait (PD + FOG) before, after, and 24 hours after an split-belt treadmill (SBT) training session. A value of zero indicates a perfect gait adaptation. Displayed is the median with the lower and upper hinges representing the first and third quartile. Data points outside the mentioned quartiles are displayed as outliers. *Significance level of P < .05.
When investigating the different parts of the gait adaptation test in more detail, there was a significant time × training-group interaction (P < .022) in the early-split (first 5 seconds). During that part of adaptation, SBT50 significantly reduced the step length asymmetry from Pre to Post (P < .05) as well as from Pre to Retention (P < .005). The SBTCR group also showed improvements during early-split, but this did not reach statistical significance. There were no significant effects for the other phases of the gait adaptation test.
For mean limb excursion asymmetry there was no significant training-group × time interaction. Adding the individual treadmill velocity or the center as a covariate to the respective models did not change the results. The various training groups did not differ in physical or mental fatigue between after completing the training session in PD + FOG.
Clinical Associations of SBT Adaptation
To explore which outcome captures gait adaptation most appropriately (study aim 3), differences in mean step length and mean limb excursion asymmetry between PD and HC were investigated at Pre. Mean step length asymmetry and mean limb excursion asymmetry were significantly lower in HC compared with PD + FOG (P = .035 and P = .015, respectively) during the adaptation test. Regarding the different parts of the adaptation test, step length asymmetry was significantly different between the groups at late-split (P = .03) and early-tied (P = .003) and for limb excursion asymmetry during early-split (P = .0009) and late-split (P = .03). Mean step length asymmetry of PD + FOG at Pre was negatively correlated with disease duration (r = −0.305, P = .049) and MDS-UPDRS-III (r = −0.384, P = .012). However, mean step length asymmetry was not correlated with freezing severity as captured by the NFOG-Q score or age.
Discussion
People With PD + FOG Improve Gait Adaptation With SBT
This study explored the potential of using SBT as a rehabilitation method for people with FOG by practicing their ability to adapt their gait pattern to asymmetrical circumstances in one session. For this aim, the immediate and retention effects of a single SBT session were compared with TBT in PD + FOG and HC. Results showed that SBT but not TBT improved gait adaptation immediately after the training and, even more importantly, improvements were retained up till 24 hours. Although the effects were larger in HC, PD + FOG still significantly benefited from SBT. Another study comparing split-belt adaptation in people with PD and HC found that despite different baseline asymmetry, PD showed the ability to adapt their step length asymmetry similarly to HC particularly in the early phase of adaptation. 19 This is in contrast with our findings, but may be explained by the fact that our PD participants were highly affected by the disease in terms of motor ability (MDS-UPDRS III) and had a long disease duration. Additionally, our participants experienced FOG, a gait deficit that was shown to be correlated to greater step length and limb excursion asymmetry during split-belt walking compared to people without FOG or HC. 15
Given the association between FOG and motor adaptation deficits as well as the link between FOG and gait asymmetry that have been shown in previous research, our findings are promising since gait deficits related to FOG were improved and retained after a single session of SBT. The finding that effects were retained after 24 hours highlights the potential to use SBT within longer rehabilitation programs.
The advantage of SBT is that it modulates gait more implicitly without attention being consciously drawn to the adaptation task. Furthermore, repeated adaptations of the gait pattern may improve the flexible adaptation of the movement to new tasks and may train motor switching, which could potentially improve motor performance in a more sustained manner. 42 Especially, prolonged training could positively affect the connectivity in specific brain circuits like the cerebellar locomotor region, 43 as this area is known to have an important role in the adjustment of gait to asymmetrical speeds. 44 Darter et al. 45 found an association between symmetry and dynamic stability during split-belt walking in healthy young adults, suggesting that improving symmetry might also be an approach to improve an individual’s’ walking stability through the use of SBT. Additionally, Reisman et al. 46 stated that locomotor adaptation helps with automatization of gait, which is affected in PD and even more in PD + FOG. This is particularly important in situations where attentional focus is required for simultaneous tasks (eg, talking while walking). The fact that people with FOG were able to automatically modulate their gait is a surprising result, knowing that indirect locomotor pathway, involving the basal ganglia, is more affected in this subgroup. 47 This could point to the fact that the cerebellar circuits became more involved in the processing of gait adaptation with repeated exposure to SBT. 46
Usually improvement of step length asymmetry would be expected to be largest immediately after the training and then diminish 24 hours later, like observed in HCs. However, in PD + FOG the improvement was the largest from Pre to Retention. The smaller improvement at Post within PD + FOG compared with HC might be due to fatigue as PD + FOG reported higher rate of physical fatigue than HC after the training session.
Training With Changing SBT Conditions Is Most Effective
As our second aim, we investigated which of the SBT conditions was most effective to improve gait adaptation in PD + FOG. The condition with changing belt speed ratios (SBTCR) showed strongest effects to improve gait adaptation and effect sizes were the largest compared with tied-belt training. We speculate that the changing ratio condition led to the greatest gains because it specifically trained the ability to rapidly and flexibly switch between motor patterns, which is usually difficult for people with PD. 48 Through the changing ratio condition participants were exposed to recurring switches, which required constant adjustments of the motor pattern. Task variability is known to be necessary to retain newly learned motor skills in neurorehabilitation 49 which could have facilitated adaptation in the SBTCR group.
SBT50 seemed to be especially effective to modulate step length asymmetry during the early phase of the SBT adaptation test. This could have been derived from the long exposure to the split-belt condition with the high ratio during the training.
The identification of the most effective SBT contrast is important to design long-term SBT protocols. The evidence suggests, that SBTCR is most effective and by implementing a greater amount of high contrast that effect could be enhanced even more. However, step length asymmetry during Retention was quite similar in SBTCR and TBT. There were no differences in mental or physical fatigue in PD + FOG between training groups, which could have explained the differences between the training protocols.
Gait Asymmetry to Quantify Adaptation Ability
Study aim 3 focused on the assessment of gait adaptation using an SBT adaptation test, possibly relevant as a future treatment outcome. We averaged different measures of gait asymmetry over the 90-second SBT adaptation test. HC showed lower average values of step length asymmetry during the SBT adaptation test compared to PD + FOG, indicating better gait adaptation. In PD + FOG this was also correlated with disease duration and MDS-UPDRS III, showing that PD + FOG with longer disease duration and more severe motor symptoms present with greater asymmetry (lower values below zero). Similarly, limb excursion asymmetry showed differences between groups with lower values in HC. Therefore, we concluded that lower values of averaged gait asymmetry (step length asymmetry or limb excursion asymmetry) during the adaptation test represented better gait adaptation and therefore could serve as a future outcome. This conclusion is supported further by lower values of gait adaptability after SBT, showing that it was responsive to training.
Limitations
First, because of combining Pre and Post assessments and the 30-minute training session, the first day of testing was potentially fatiguing. Although we had 3 dropouts due to fatigue, we found no correlation between fatigue and the observed improvement in gait adaptability. However, fatigue could have influenced assessment at the Post test. Second, we allowed participants to hold handrails if necessary, shown to affect motor adaptation. 50 More PD + FOG than HC held the handrails, which may explain the different results between groups. However, even with handrails positive results were found, testifying the feasibility of the SBT-approach for rehabilitation. Especially for the subgroup with FOG, who often have more sever balance deficits and higher fall risk, 51 it is common practice and unavoidable to use handrails. Therefore, it appears that the current findings generalize to clinical practice. Another limitation is the unblinding of the assessors. Although for most of the testing movement analysis systems were used limiting an influence of the assessor, a bias by the unblinding cannot be ruled out. Additionally, although the overall sample size was solid, this study is not safe of underestimating the observed effects due to the smaller sample sizes in the 4 training groups. Last, medication state can limit the interpretability of results in clinical trials with people with PD, as On and Off states can change individually and are difficult to assess. Additionally, responsiveness of FOG to medication (eg, Off-FOG; On-Off-FOG) was not evaluated.
Conclusions
This proof-of-principle study evaluated the value of a single SBT versus a TBT session in HCs and PD + FOG, a group with notoriously serious gait disorders, on their ability to adapt and readapt gait to asymmetrical and symmetrical belt speeds. We found SBT to be superior to TBT to improve gait adaptation in people with PD + FOG, although effects were smaller compared with HCs. Improvements were retained after 24 hours, illustrating the potential of this training approach for future intervention studies. We also found that the changing ratios mode led to the greatest effect sizes, when compared with TBT in PD. Training proved feasible as fatigue was not associated with adaptation ability. Finally, we also found that measuring gait asymmetry during the gait adaptation test could be used to quantify adaptation ability in PD. Future studies should investigate whether long-term SBT using the changing ratios conditions leads to improved gait adaptability on over-ground tasks and whether training effects can be retained over a longer period. Additionally, further investigation needs to be done on whether improved gait adaptation can lead to a reduction in the occurrence of FOG.
Supplemental Material
S1_Supplementary_clean – Supplemental material for The Effect of One Session Split-Belt Treadmill Training on Gait Adaptation in People With Parkinson’s Disease and Freezing of Gait
Supplemental material, S1_Supplementary_clean for The Effect of One Session Split-Belt Treadmill Training on Gait Adaptation in People With Parkinson’s Disease and Freezing of Gait by Jana Seuthe, Nicholas D’Cruz, Pieter Ginis, Jos Steffen Becktepe, Burkhard Weisser, Alice Nieuwboer and Christian Schlenstedt in Neurorehabilitation and Neural Repair
Supplemental Material
S2_Supplementary – Supplemental material for The Effect of One Session Split-Belt Treadmill Training on Gait Adaptation in People With Parkinson’s Disease and Freezing of Gait
Supplemental material, S2_Supplementary for The Effect of One Session Split-Belt Treadmill Training on Gait Adaptation in People With Parkinson’s Disease and Freezing of Gait by Jana Seuthe, Nicholas D’Cruz, Pieter Ginis, Jos Steffen Becktepe, Burkhard Weisser, Alice Nieuwboer and Christian Schlenstedt in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Jacques & Gloria Gossweiler Foundation, Switzerland and the Franz & Ursula Coppenrath Foundation, Germany (CS).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.