
Abstract
Background. Intensive bimanual training results in more improvement in hand function in children with unilateral spastic cerebral palsy (USCP) than lower intensity conventional interventions. However, it is not known whether combined upper and lower extremity training in an intensive protocol is more efficacious for upper and lower functional abilities than conventional therapies provided in usual customary care. Objective. To determine the efficacy of Hand and Arm Bimanual Intensive Therapy Including Lower Extremity (HABIT-ILE) for children with USCP. Methods. Twenty-four children with USCP were randomized into 2 groups: an immediate HABIT-ILE group (IHG, initially receiving HABIT-ILE, 10 days = 90 hours), and a delayed HABIT-ILE group (DHG), which continued their conventional/ongoing treatment for an intended total duration of 90 hours. In phase 2, children in the DHG were crossed over to receive HABIT-ILE and children of the IHG were followed in their ongoing conventional therapy. Children were assessed using the Assisting Hand Assessment (AHA, primary outcome), the ABILHAND-Kids, and the Pediatric Evaluation of Disability Inventory. Dexterity (Box and Blocks Test [BBT]) and pinch strength were also measured. Locomotor abilities were assessed with Six-Minute Walk Test (6MWT, primary outcome) and ABILOCO-kids. Social participation was measured with the Assessment of Life-HABITs. Results. A 2 (groups) × 3 (test sessions) analysis of variance indicated significant improvements for primary outcomes (AHA, P < .001; 6MWT, P = .002) and all secondary assessments except BBT, step length and bodyweight distribution following HABIT-ILE, but not conventional therapy. Conclusion. The findings suggest that combined upper and lower extremity in an intensive training protocol may be efficacious for improving both upper and lower extremity function in children with USCP.
Keywords
Introduction
Unilateral spastic cerebral palsy (USCP) represents one of the most common subtypes of cerebral palsy.1,2 Various motor impairments may be observed, depending on the timing, extent, and location of the lesions and the subsequent reorganization of the cortical pathways, including descending motor pathways, thalomocortical ascending pathways, and intracortical connections. 3 These impairments are largely lateralized to one body side, affecting both upper (UE) and lower (LE) extremity function.
Intensive rehabilitation strategies have been successfully developed for the UE over the past decade. These strategies, either unimanual therapy (constraint-induced movement therapy [CIMT]) or bimanual therapy (eg, Hand-Arm Bimanual Intensive Therapy [HABIT]), combine principles of motor learning (practice specificity, feedback, etc), 4 and neuroplasticity (practice-induced brain changes arising from repetition, increasing movement complexity, motivation, and reward)5,6 in intensive blocks of training. HABIT is an intensive bimanual training intervention where use of both hands in cooperation is required, aiming to increase functional independence during daily living. Principles of CIMT are applied, but constraint of the less affected UE is replaced by activities necessitating the combined use of both hands. 7 The results of pediatric CIMT8-12 and bimanual training13-21 are promising for inducing changes in children’s functional abilities. These interventions have been shown as more efficacious than usual and customary care, albeit typically provided at lower dose, in a more distributed fashion.9,13,22-24
To date, these intensive approaches have largely ignored the LE, with children sitting during table activities for much of the training. However, 2 studies have documented carryover to the LE, where some gait variables improve after CIMT.25,26 These unexpected changes were interpreted as due to better interlimb coordination linked to the tasks (eg, retrieving objects from the floor 26 ) or to postural reorganization during walking due to the weight of the casts that are used to constrain less-affected UE in CIMT. 25 Other studies have suggested that CIMT may be of benefit to gross motor outcomes.27-29 While these studies demonstrate a window of opportunity, they were not specifically designed to engage the LE. These results, added to the knowledge that intensive gait training in other subtypes of CP is effective, 30 and that treatments such as botulinum toxin in the LE may have an effect on the UE, 31 suggest that the LE may benefit from being directly targeted in combination with the UE. Such a combined approach may benefit not only the LE but also postural function and interlimb coordination. Interlimb coordination commonly occurs during everyday life (eg, walking while speaking on a cell phone) and has been shown to be impaired above and beyond UE or LE impairments in children with USCP. 32
Based on this rationale, we designed a new intensive training for individuals with USCP: Hand and Arm Bimanual Intensive Therapy Including Lower Extremity (HABIT-ILE). HABIT-ILE is a form of bimanual training that continuously incorporates postural control and LE function. 33 Like HABIT, 7 it is a motor learning–based approach, which is the common feature of all protocols with good evidence of efficacy for improving motor activities in children with cerebral palsy. 24 The objective of this study was to compare the changes induced by HABIT-ILE with an equivalent amount of time of ongoing contemporary treatment interventions used in Belgium, with focus on remediation of impairments affecting hand function, locomotor abilities and social participation. We hypothesized that HABIT-ILE would lead to greater improvements in these domains than conventional rehabilitation.
Methods
Participants
Children were recruited from centers dedicated to treat-ment of children with cerebral palsy in Belgian university hospitals (mandated by social security to coordinate interventions for these children). Potential participants were contacted by e-mail or telephone. Those who were available/interested to participate were invited to receive a baseline examination.
Consistent with previous HABIT trials,13,15 inclusion criteria included (a) age 6 to 13 years, (b) ability to grasp light objects and lift the more affected arm 15 cm above a table surface, (c) school level equal to that of typically developing peers of the same age, (d) ability to follow instructions and complete testing, and (e) an LE impairment reported by medical examination. Exclusion criteria were (a) uncontrolled seizures, (b) botulinum toxin injections or orthopedic surgery within the previous 12 months/planned within the study period, and (c) visual problems likely to interfere with treatment/testing. This study was approved by the Ethical Committees of the Université catholique de Louvain (Mont-Godinne/Saint-Luc), Belgium. Children and parents provided informed consent.
Design
This study lasted 2 years, including summer camps during 2 consecutive summers. Each year, all participants (12 per camp) underwent a baseline assessment during the fall/winter preceding the camp. On the basis of this assessment they were assigned by the principal investigator to 2 balanced groups stratified by age, manual dexterity (score on the Box and Blocks Test [BBT]) and lesion side. The groups as a whole were then randomly assigned offsite (by a clinician not involved in the study) to one of the study arms using concealed allocation: one group being randomized to an immediate HABIT-ILE group (IHG) and the other to a delayed HABIT-ILE group (DHG). In phase 1 (Figure 1), children from DHG were followed during an intended duration of 90 hours of conventional/ongoing therapy (average of 20 weeks, see below) before receiving HABIT-ILE during a summer holiday camp. Children in the IHG first participated in the summer holiday camp and were then crossed over and followed during an intended duration of 90 hours of conventional/ongoing therapy (on average 18 weeks). No wash-out period was possible since all children continuously receive conventional therapy before and after the HABIT-ILE participation as part of their ongoing treatment.
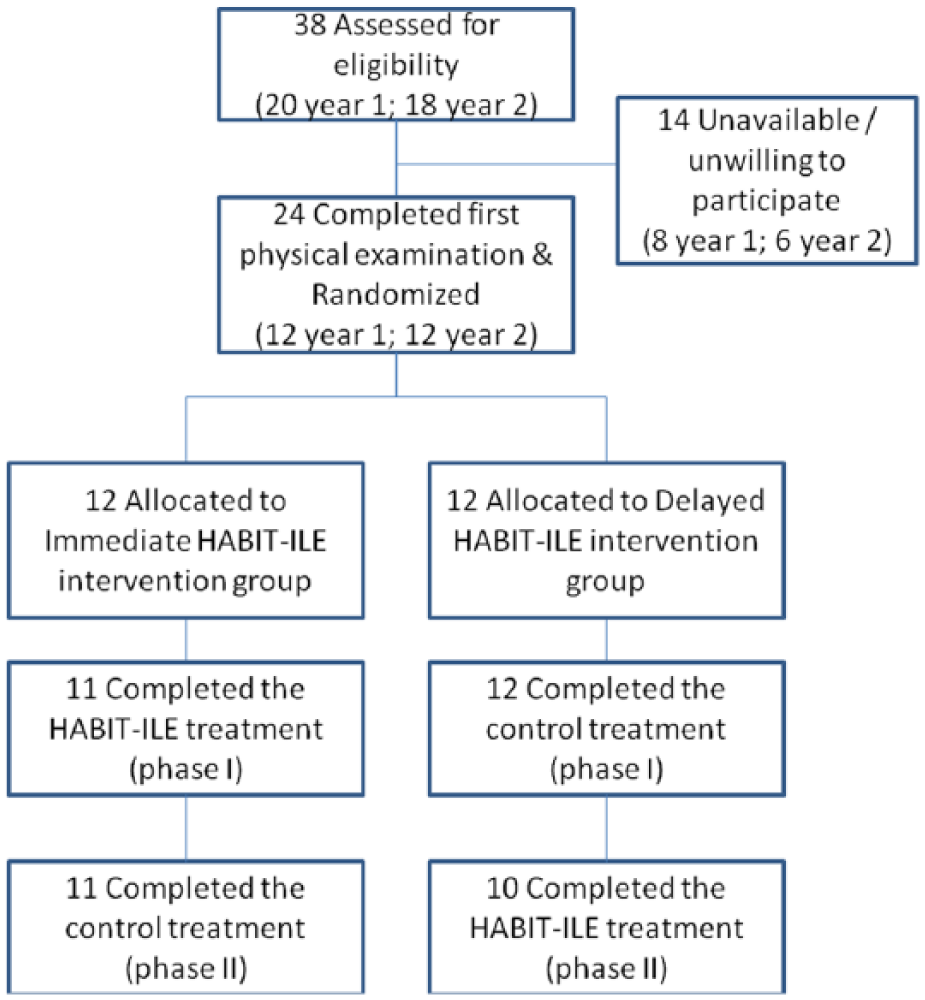
CONSORT flow diagram illustrating participant flow during the different phases of the study. Flow of participants, withdrawals, and inclusion in analyses are described. Databases of the referring centers were searched by the corresponding MDs to identify children with USCP meeting the criteria. Of the 38 children identified who met the inclusion criteria, 24 (6 males and 18 females, 6-13 years old, mean age = 8.7 ± 1.7 years) agreed to participate (also see in Table 1). They were randomized into the IHG or DHG group. Three dropped out before the end of the study, during the HABIT-ILE process (2 in DHG and 1 in IHG). Among the 2 of the DHG group, who dropped out in phase 2, one presented with active seizures despite a report of none, the other had a severe gastroenteritis. The child who dropped out in the IHG (phase 1) was homesick during the camp, and the parents decided to withdraw her after 1 week. A total of 21 individuals completed the 2 interventions and all testing sessions.
Conventional Intervention Procedure
In Belgium, the social security system provides children with cerebral palsy a lifelong reimbursement of physiotherapy (PT, 1-5 h/wk), which can be received either at home, at the clinic/ hospital or at a special education school. Children attending special education schools or followed at hospitals may receive additional occupational therapy (OT). Most of them are also involved (either at school or outside) in adapted sports programs.
The main focus of treatment is thus PT, which in Belgium is generally focused on remediation of impairments based on neurodevelopmental concepts: either the Bobath concept 34 or the neurodevelopmental theories of LeMétayer. 35 These approaches are directed toward motor skills along a developmental continuum and correcting movement patterns. Additional OT was provided in 9 of 24 children in this sample. While OT focuses more on functional abilities, skilled motor learning theories are not generally taught to/used by OTs in Belgium. Children recruited here pursued their ongoing conventional treatment during the control phases of the study, administered by their regular PT/OT and specific adapted physical education teachers, with the number of hours being reported by the parents. The focus was on the upper and lower extremities, and it was not altered in any way during the study period.
HABIT-ILE Procedures
HABIT-ILE 33 sleepover camps were conducted in Brussels in July 2011 and 2012. Participants were engaged in treatment 9 hours per day for 10 consecutive days (90 hours). One trained interventionist was assigned to each child. Most interventionists were PT/OT students, while 2 were certified PTs and 1 was an OT. Interventionists were trained prior to the camp on the basis of a manual of procedures and were required to provide only HABIT-ILE procedures. Compliance with this instruction was monitored during the camp and daily meetings dedicated to discussions of therapeutic goals and strategies. The matching of participants and interventionists was made using family-centered approaches, considering parents and supervisors’ recommendations. Trained supervisors were in charge of the organization and provided guidance to the interventionists. Two of the supervisors (1 PT and 1 OT) were in charge of both camps to ensure consistent procedures and interventionist training. HABIT-ILE is described in detail elsewhere. 33 Briefly, it uses structured bimanual tasks with increasing motor difficulty and functional tasks requiring the use of both hands associated with systematic postural/LE requirements. As in HABIT 7 , this intervention takes into account functional goals defined by children and parents and is designed to be child friendly. Precamp assessments were used to determine initial impairments. From this basis, a selection of activities and tasks were primarily selected evolving toward more challenging bimanual coordination and greater postural/ LE challenges. At the beginning of each activity, children were provided with cues to induce problem solving and avoid compensations.
HABIT principles 7 were used to provide bimanual activities, where the more affected UE was initially used as a passive support, evolving progressively toward more complex use of this hand. This could be elicited by modifying the task constraints or by introducing tasks/games progressively requiring more skilled use of the more affected UE. Both whole (15/30 min; eg, building towers with Lego blocks) and part task practice (eg, making piles of blocks, one with each hand during 30-second periods) were used to provide skilled, repetitive UE movements.
The concomitant LE/postural challenges were also progressively increased in the 3 subtypes of tasks used: (a) table activities, (b) activities of daily living (mainly in standing/walking), and (c) gross motor play/physical activities (standing, walking, running, or jumping).
First, table activities—defined as tasks/activities performed playing at a table—started sitting on a fitness ball partly deflated (sitting position with knees and hip at 90° and table adjusted for elbow support). The stability was further challenged by progressively inflating the ball. Once ball sitting was mastered, stability was challenged by having children stand on a balance board (left–right instability), with graded difficulties. The balance board use was combined with manipulative tasks already performed successfully in ball sitting. More skilled/challenging tasks for the UE were introduced while on the ball until they were successful enough to be performed in more challenging LE conditions. Second, more challenging LE/posture conditions were also progressively introduced for activities of daily living (eg, position tying shoes). Finally LE challenges progression was introduced during gross motor play/physical activities involving the UE progressing from standing to walking and finally to running or jumping (see Bleyenheuft and Gordon 33 ).
Assessment
Assessments were performed across the 3 domains of the International Classification of Function (ICF) model before/after each phase of the study. Manual ability and gross motor function were categorized using the Manual Ability Classification System (MACS 36 ) and the Gross Motor Function Classification System (GMFCS 37 ). Magnetic resonance imaging reports were used by a neuroradiologist to categorize brain lesions. The primary outcome measures included 1 UE measure (Assisting Hand Assessment [AHA] 38 ) and 1 LE measure (Six-Minute Walk Test [6MWT] 39 ).
Four secondary assessments were performed for the UE: the ABILHAND-Kids, 40 the Pediatric Evaluation of Disability Inventory (PEDI 41 ), the BBT on both hands, 42 and the finger strength (key pinch) on both hands. 43
Three secondary LE assessments were performed: the mean step length measured at self-selected and maximal walking speed, the difference of body weight distribution over each LE during upright standing (Wii Balance Board, Nintendo 44 ), and the ABILOCO-Kids questionnaire. 45 Finally, social participation was measured using the Assessment of Life Habits (Life-H) questionnaire adapted for children. 46 Social participation and satisfaction were scored by the parents. For more details about assessments, see Supplementary Material.
Sample Size
Sample size calculations were performed based on AHA scores derived from an earlier HABIT study. 13 A mean improvement of 0.94 ± 0.54 logits after HABIT was reported. With α = .05 and 1 − β = 0.7, 12 participants per group were required.
Statistics
Groups were compared at baseline assessment using t tests. A 2 (groups) × 3 (test sessions) analysis of variance with repeated measures on test session was performed on each measure. The overall group × test session interaction tested whether the time course differed between treatment groups. Post hoc analysis was performed using the Newman–Keuls procedures, including an adjustment for multiple comparisons. Since homoscedasticity was never violated, we used repeated-measures analysis of variance without any transformation for data analysis. Outliers were not excluded from this analysis. In case of missing data at one point, the participant was excluded for the analysis of this variable. The effect size was estimated using the value of the η2. In addition the number of children reaching a clinically meaningful degree of difference is reported using the empirical rule of effect size (ERES; change of each child considered as clinically meaningful if >0.5 SD). 47
Results
Participants Flow and Characteristics
Participant flow is presented in Figure 1. Each year, from baseline assessment, children were allocated to the IHG or DHG (see Methods section). Across the 24 children included, 3 were excluded before the end of the study (2 in DHG and 1 in IHG, details in Figure 1 legend). For technical reasons, some data were not completed at all points in a few participants (details in Supplementary Material). A t test on variables at baseline showed no significant initial differences between groups on any measure (all P > .05, Table 1). No harms or unintended effects were observed in this study.
Characteristics of the Children and Comparison Between Groups at First Assessment. a
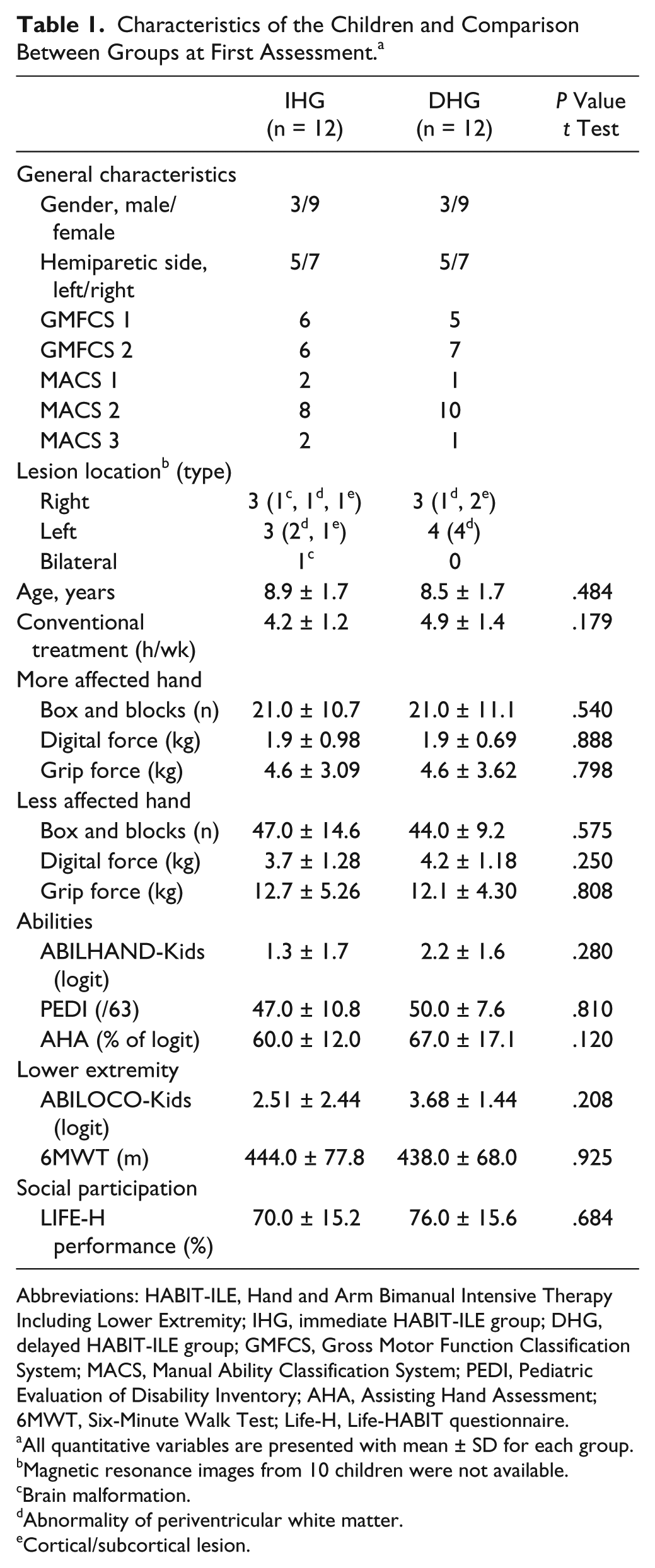
Abbreviations: HABIT-ILE, Hand and Arm Bimanual Intensive Therapy Including Lower Extremity; IHG, immediate HABIT-ILE group; DHG, delayed HABIT-ILE group; GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification System; PEDI, Pediatric Evaluation of Disability Inventory; AHA, Assisting Hand Assessment; 6MWT, Six-Minute Walk Test; Life-H, Life-HABIT questionnaire.
All quantitative variables are presented with mean ± SD for each group.
Magnetic resonance images from 10 children were not available.
Brain malformation.
Abnormality of periventricular white matter.
Cortical/subcortical lesion.
Treatments Characteristics
Over the 10 days of HABIT-ILE, 90 hours of treatment were delivered (5400 minutes). During this period, as measured through their daily systematic reporting sheets of treatment content (completed by interventionists), children were engaged in functional and play activities on average for 5225 minutes (±192 minutes), representing 96% (range, 89% to 98%) of the time. For the UE, this treatment consisted on average of 21% of part-practice and 79% of whole practice tasks. The UE activities were categorized as 27% gross dexterity (including 2% virtual reality), 27% manipulative games, 5% card games, 5% arts and crafts, and 36% activities of daily living. For the LE, 54% of the intervention was spent sitting on a ball (evolving from 60% at day 1 to 45.5% at day 8), 2% on a balance board (evolving from 0% at day 1 to 4% at day 8), 24% standing (28% day 1 to 19.5% day 8), and 20% walking/running or jumping (12% day 1 to 31% day 8).
For conventional treatment, children continued their ongoing treatment. Assessments were planned in order to complete 90 hours (before camp for DHG, after camp for IHG). However, because of various events (illness, missing sessions, etc), the mean total amount of conventional therapy was 80 hours (SD, ±16). During this period, 61% of the time was individual therapy, either PT (80% of individual intervention) or OT (20% of individual intervention–only 9 of 24 children). In our sample, 19 of 24 children had conventional PT following Bobath concepts, 34 3 had PT following LeMétayer concepts, 35 and 2 of 24 had PT not following a specific method. In adapted sports (39% of conventional intervention time) children had mainly psychomotor training 48 (84% of time recorded as adapted sports). Some of them had other adapted activities: hippotherapy/hydrotherapy/adapted judo/tennis. Conventional intervention was provided continuously throughout both school and holiday time.
Upper Extremity
For the AHA, a main effect of test session and a group × test session interaction was observed (Figure 2A, Table 2). Post hoc tests showed that for the IHG, AHA scores were significantly higher in test sessions 2 and 3 than they were in test session 1. In the DHG, test session 3 had significantly higher AHA scores than test sessions 1 and 2.
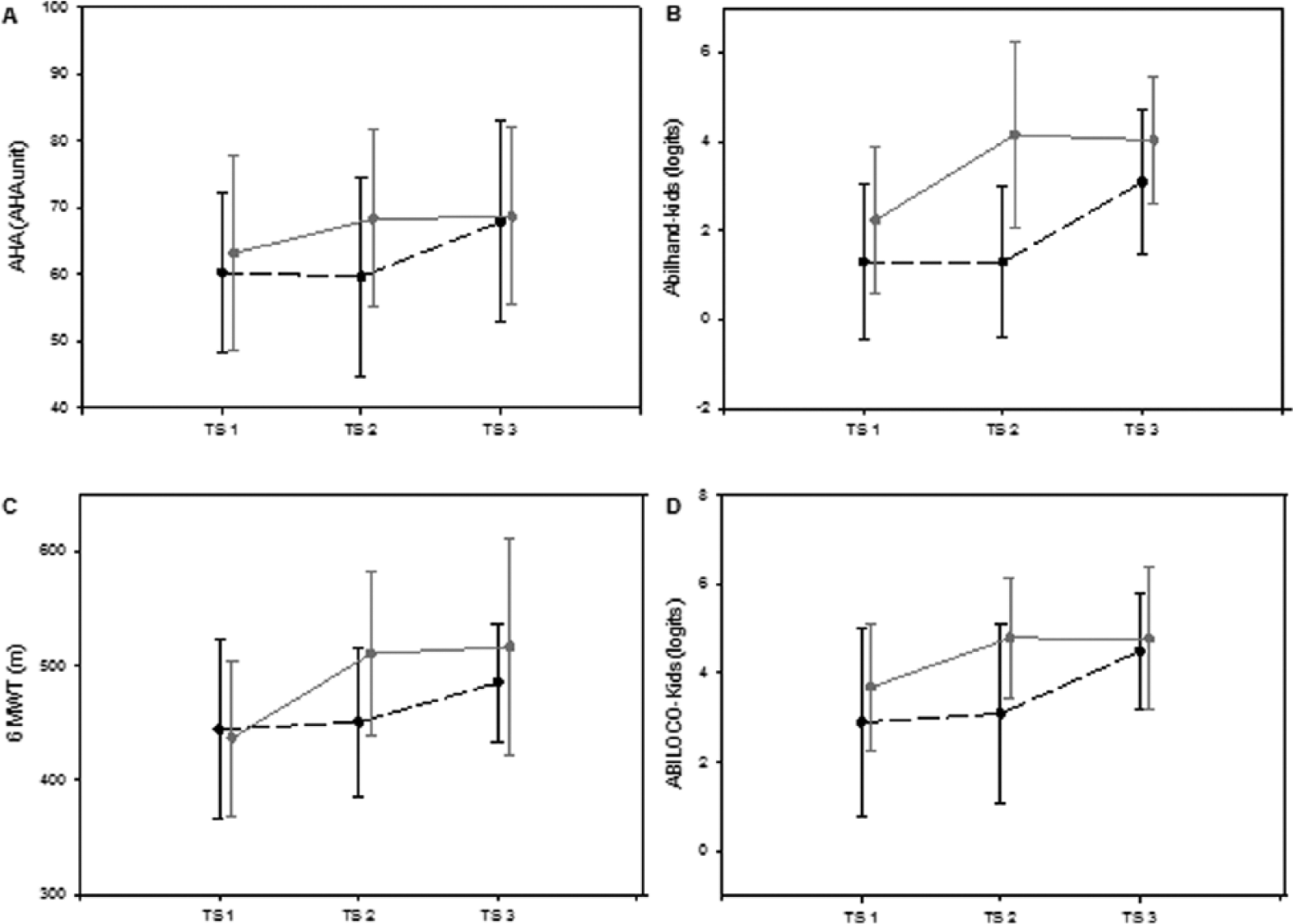
Mean and SD values observed for UE activities as measured with the AHA (A) and the ABILHAND-Kids (B). Mean and SD values observed for locomotor ability as measured by the 6MWT(C) and the ABILOCO-Kids (D). Black dotted lines represent mean values of the DHG (before conventional intervention – after conventional intervention – after HABIT-ILE intervention), gray lines represent the mean value of the IHG (before HABIT-ILE – after HABIT-ILE and after the following conventional intervention). The bars represent the SD of each group. TS represents testing session.
Upper Extremity Changes.
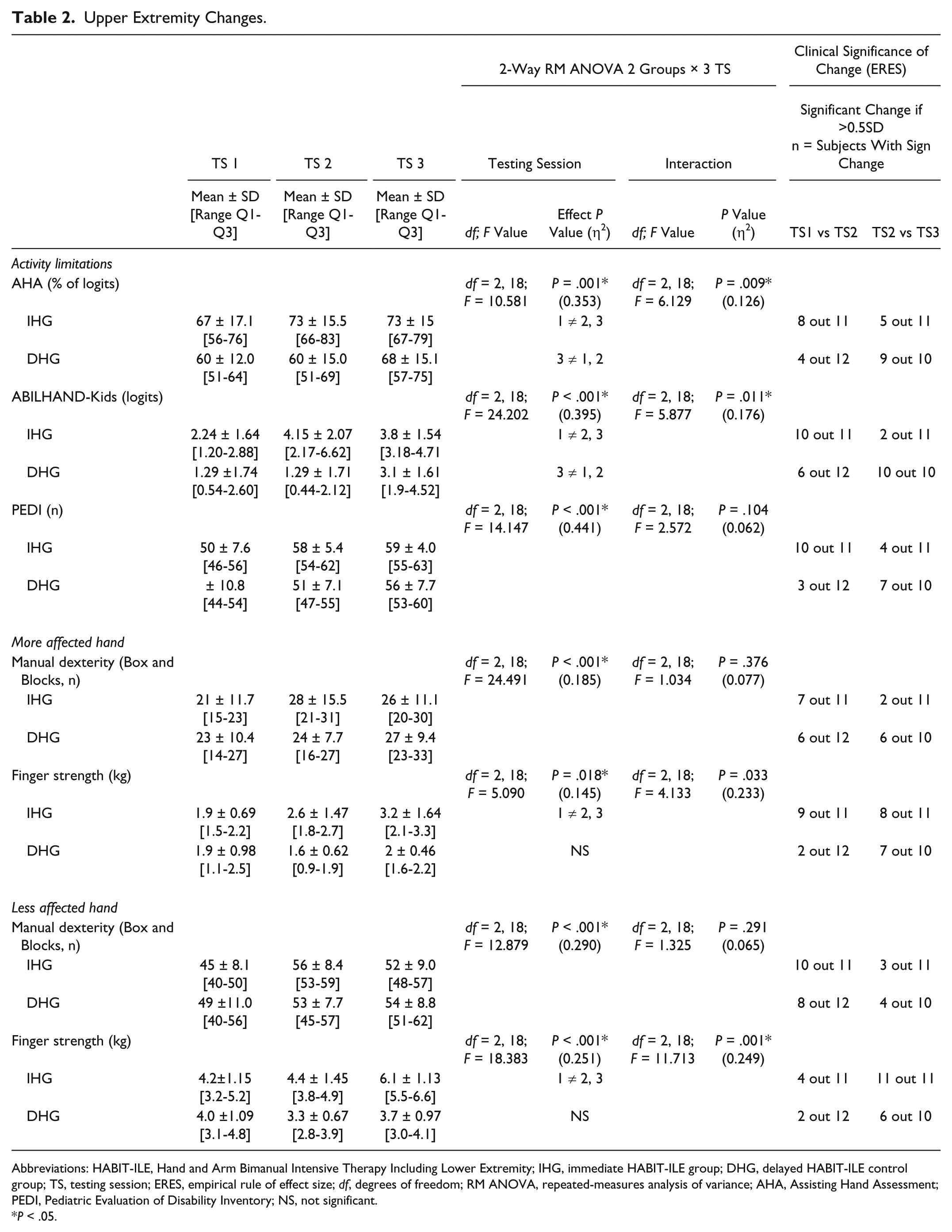
Abbreviations: HABIT-ILE, Hand and Arm Bimanual Intensive Therapy Including Lower Extremity; IHG, immediate HABIT-ILE group; DHG, delayed HABIT-ILE control group; TS, testing session; ERES, empirical rule of effect size; df, degrees of freedom; RM ANOVA, repeated-measures analysis of variance; AHA, Assisting Hand Assessment; PEDI, Pediatric Evaluation of Disability Inventory; NS, not significant.
P < .05.
The ABILHAND-Kids questionnaire showed the same pattern of results: a main effect of test session with a group × test session interaction. The post hoc tests indicated that in the IHG, scores were significantly higher in sessions 2 and 3 than they were in session 1. For the DHG, there were higher scores at test session 3 than sessions 1 and 2 (Figure 2B). A main effect of test session was observed for the PEDI, although no interaction was observed (P = .104).
The Box and Blocks Test showed a main effect of test session on both hands (Table 2), but no group × test session interaction was observed on either hand.
For finger strength there was a main effect of test session and group × test session interaction for both hands. Post hoc tests showed that in the IHG there were higher strength values at test sessions 2 and 3 than in test session 1. In the DHG, no significant differences were observed between test sessions (Table 2).
Lower Extremity
For the 6MWT (Figure 2C, Table 3), a main effect of test session and group × test session interaction was observed, with post hoc tests showing that in the IHG, children walked further in test sessions 2 and 3 than in test session 1. In the DHG, post hoc tests did not show differences between test sessions.
Lower Extremity and Social Participation Changes.
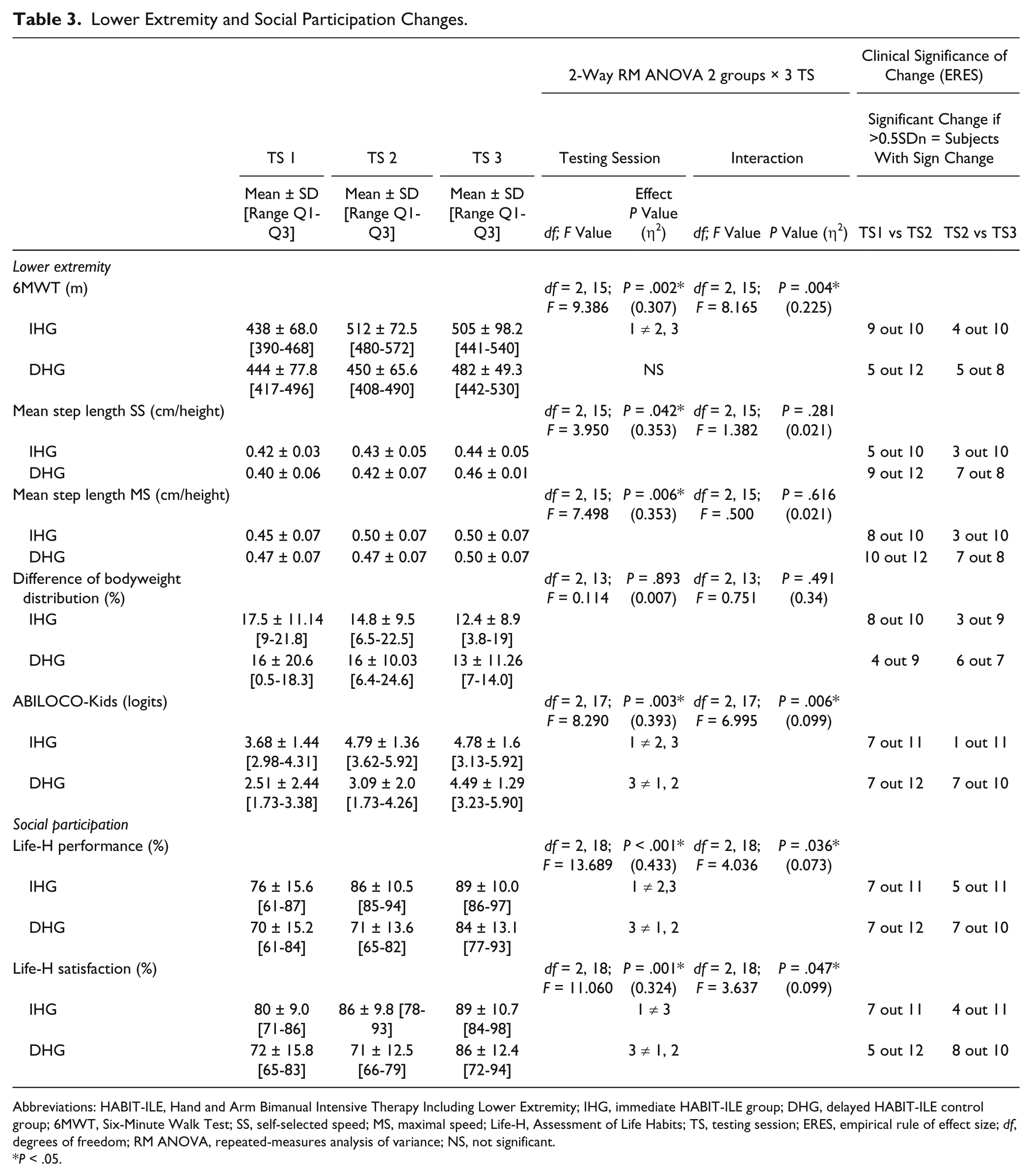
Abbreviations: HABIT-ILE, Hand and Arm Bimanual Intensive Therapy Including Lower Extremity; IHG, immediate HABIT-ILE group; DHG, delayed HABIT-ILE control group; 6MWT, Six-Minute Walk Test; SS, self-selected speed; MS, maximal speed; Life-H, Assessment of Life Habits; TS, testing session; ERES, empirical rule of effect size; df, degrees of freedom; RM ANOVA, repeated-measures analysis of variance; NS, not significant.
P < .05.
The mean step length at self-selected and maximal speed showed a main effect of test sessions (Table 3). However, no group × session interactions were observed. The bodyweight distribution did not show changes across assessments (Table 3).
The ABILOCO-Kids questionnaire showed a main effect of test session with an interaction whereby scores were higher in the IHG at test sessions 2 and 3 than in session 1. For the DHG, the scores were higher at session 3 than at sessions 1 and 2 (Figure 2D).
Social Participation
For performance in social participation (Table 3, Figure 3A), a main effect of test session and group × test session interaction was observed, with post hoc tests showing that in the IHG, there were higher scores for test sessions 2 and 3 than test session 1. In the DHG, the scores were higher for test session3 (postcamp) than test sessions 1 and 2.
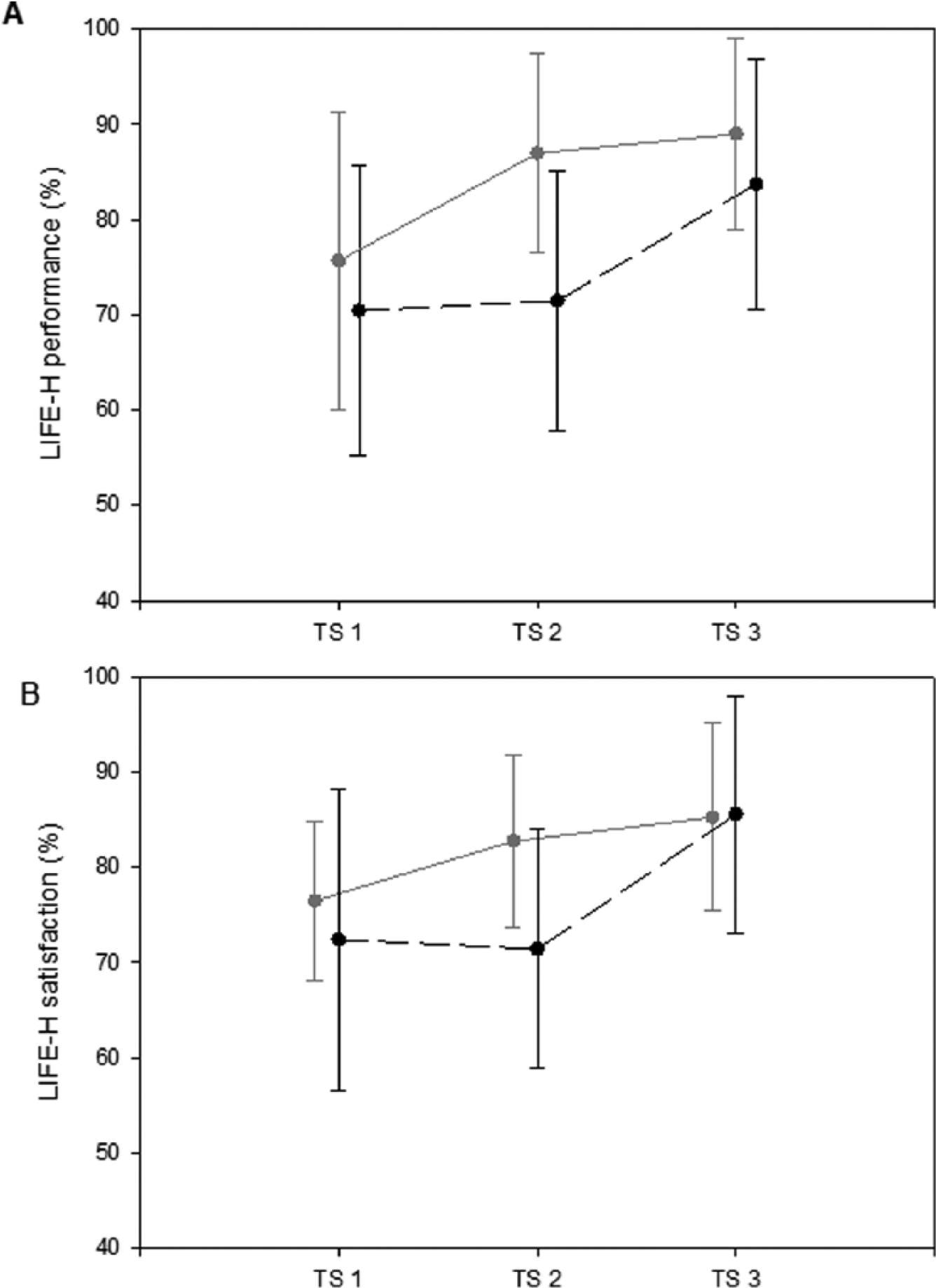
Mean and SD values observed for the performance of the children (A) and the satisfaction of the parents (B) in the LIFE-HABIT questionnaire. Black dotted lines represent mean values of the DHG (before conventional intervention – after conventional intervention – after HABIT-ILE intervention), gray lines represent the mean value of IHG (before HABIT-ILE – after HABIT-ILE and after the following conventional intervention). The bars represent the SD of the group. TS represents testing session.
For parents’ satisfaction about social participation, a main effect of test session and group × test session interaction was observed, with post hoc tests indicating that in the IHG, scores were higher for test session 3 than test session 1. In the DHG, scores were higher for test session 3 than sessions 1 and 2 (Figure 3B).
Magnitude of the Changes
The η2 (Tables 2 and 3) indicated that 35% and 31% of the variance in AHA and 6MWT, respectively, and up to 44% for secondary measures, is attributable to the treatments.
Discussion
There were significant improvements in the primary outcome measures (AHA, 6MWT) between the pre- and post-HABIT-ILE assessments while no significant differences were observed following conventional treatment. Most of the secondary measures also improved between pre- and post-HABIT-ILE intervention while not changing following conventional treatment. To our knowledge, this is the first evidence of successful application of intensive rehabilitation approaches simultaneously targeting both the upper and lower extremities for children with USCP.
Improvements in Upper Extremity Performance
The changes in the AHA scores following HABIT-ILE are congruent with previous studies on intensive bimanual therapies for children with CP, showing increases at the activity level.15-17,19,49 This suggests that the introduction of continuous LE/postural engagement during bimanual training does not decrease the possibility to enhance UE activity. This was supported by the fact that the changes observed for the UE primary outcome measure (AHA, Table 2) during the HABIT-ILE intervention averaged 6 (IHG) or 8 (DHG) AHA units, which is higher than previous UE trials, 21 while baseline scores and ranges were similar to these trials.
The same result was observed for the ABILHAND-Kids questionnaire, measuring manual ability in daily life. 40 Together these results show promise for this new intensive approach on the activity level of a population that already receives conventional intervention focused on remediation of impairments.
Lower Extremity Function
The 6MWT showed improvements following the HABIT-ILE intervention. In 2 weeks, children gained an average of 50 m in this endurance test. As this test has been specifically tested in the CP population and shown to be reliable,50,51 this result demonstrates that HABIT-ILE had a significant effect on both gait and UE abilities. An increase in the walking distance during the 6MWT can be due either to an increased step frequency and/or length. As the step length based on video records did show a significant increase but no interaction effect, more detailed kinematic analysis is needed in future studies to determine whether HABIT-ILE affects kinematic gait parameters.
Body weight was not better distributed (more symmetric) after HABIT-ILE than conventional therapy. Body weight distribution is complex in children with USCP and does not follow a systematic pattern. 52 Domagalska et al 52 have shown that children with USCP are unable to achieve postural symmetry, with half of the children overloading the more affected side and half overloading the less affected side. It is possible that the HABIT-ILE training did help in rebalancing body weight distribution only in some subgroups of participants. Finally, since the number of participants considered for this test was reduced for technical reasons, insufficient statistical power may have contributed to the lack of significant findings.
The ABILOCO-Kids questionnaire showed improvements following HABIT-ILE with retention after crossover to conventional treatment. Since ABILOCO-Kids is directed to activities, the changes show that not only is gait improved, but also transfer occurs to everyday life situations. It should be noted that the ABILOCO-Kids scale did present a ceiling effect for the most mobile children (3/24 achieved the best possible score at first testing session, 8/22 at the second, and 10/21 at the third testing session).
Changes in LE of children with USCP have been previously observed using a specific gait trainer (modified treadmill) at regular frequency as an adjunct to traditional PT. 53 However, this training has never been tested intensively (ie, several hours a day, 2 or more weeks) as this is not likely feasible.
While gait variables such as base of support, normalized step length, 25 velocity over a short distance and cadence improved following CIMT,25,26 more challenging/functional assessments such as the Standardized Walking Obstacle Course or Pediatric Balance score did not show improvements. 26 Furthermore, follow-up of these trials were not documented, thus retention is not known.
Social Participation
Social participation performance, as well as satisfaction of the parents, also improved after HABIT-ILE. While improvement in activities and goal attainment due to intensive training is now well established,15-17 the standardized measurement of social participation is less common. A recent paper focusing on quality of life, including a section dedicated to social participation, showed some changes after CIMT and bimanual UE training. 54 In the present study, we used a scale that is specific to social participation and validated for using with children. 46 The results obtained after HABIT-ILE and maintained after conventional treatment for the IHG highlight the effects of intensive training on transfer of newly learned activities in the environment and the changes it may introduce in social participation.
Intragroup Variability
Considerable intragroup variation is present in these data due to the heterogeneity of children’s impairment and age. However, as this phenomenon is present in both groups (see Tables 2 and 3), it is not likely to account for our findings. Variability was also observed in the ERES: the percentage of children achieving a clinically meaningful change was higher during HABIT-ILE than in conventional intervention. However, both groups had children reaching the threshold of clinical meaningful difference. This illustrates that while conventional intervention did not show significant differences in the group, some children (albeit fewer than in HABIT-ILE) achieved a clinically significant change.
Limitations
While the initial design intended to compare 90 hours of HABIT-ILE with 90 hours of conventional treatment, the dropouts of some sessions resulted in a mean of 80 hours of conventional treatment. This may have provided an underestimation of changes during conventional treatment.
This study shows that intensive training using one (motor learning) approach over a brief interval is more efficacious in various assessments (3 levels of the ICF) than another treatment (mainly focused on impairment remediation) more spread out. Either the training used in HABIT-ILE is more efficient than conventional therapy currently practiced in Belgium, or the intensity may be the key to develop neuroplasticity and improve children’s abilities. In the latter case, delivery models that currently prevail in many European countries (ie, focusing on impairment remediation) may not be optimal for treatment of children with USCP. Ultimately HABIT-ILE and conventional treatment should be compared at a similar frequency, either at usual and customary schedules or following intensive training sessions. This would require an increase of engagement time during conventional therapy that seems difficult to reach. In HABIT-ILE, this is reached through the continuous performance of voluntary movements, combined with the high level of motivation of the children, gained through the use of games and constant positive/rewarding interactions with the interventionists.
Conclusion
This study showed that high-intensity training continuously directed to UE and LE (HABIT-ILE) during a short period was more efficacious than a conventional intervention delivered over a longer period. After HABIT-ILE but not after conventional therapy, changes were observed in both upper and lower extremities at the 3 levels of the ICF. To our knowledge, it is the first time intensive training for children with USCP has targeted both UE and LE and has been shown to improve abilities in both. It raises interesting questions regarding clinical practice and especially current prevailing rehabilitation models, suggesting that brief episodes of more intensive rehabilitation might be better.
Future investigations are needed to determine (a) if HABIT-ILE and conventional interventions provided at same intensity show the same results, (b) whether the UE improvements are attenuated by the introduction of systematic LE engagement (ie, HABIT vs HABIT-ILE), and (c) whether children with bilateral cerebral palsy benefit from this approach.
Footnotes
Acknowledgements
We are grateful to all children, families, and therapists who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “Fonds de mécénat d’ING en Belgique (2011)” and the “Hors piste” program 2012 of the Fondation Roi Baudouin, Belgium. ![]() reference: NCT01700777.
reference: NCT01700777.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.