
Abstract
Background. Understanding the relationship between movement quality (impairment) and performance (activity) in poststroke patients is important for rehabilitation intervention studies. This has led to an interest in kinematic characterization of upper limb motor impairment. Since instrumented motion analysis is not readily clinically available, observational kinematics may be a viable alternative. Objective. To determine if upper limb movement quality during a reach-to-grasp task identified by observation could be used to describe the relationship between motor impairments and the time to perform functional tasks. Methods. Cross-sectional, secondary analysis of baseline data from 141 participants with stroke, age 18 to 85 years, who participated in a multicenter randomized controlled trial. Clinical assessment of movement quality using the Reaching Performance Scale for Stroke (RPSS–Close and Far targets) and of performance (activity) from the Wolf Motor Function Test (WMFT–7 items) was assessed. The degree to which RPSS component scores explained scores on WMFT items was determined by multivariable regression. Results. Clinically significant decreases (>2 seconds) in performance time for some of the more complex WMFT tasks involving prehension were predicted from RPSS–Close and Far target components. Trunk compensatory movements did not predict either increases or decreases in performance time for the WMFT tasks evaluated. Overall, the strength of the regression models was low. Conclusions. In lieu of kinematic analysis, observational clinical movement analysis may be a valid and accessible method to determine relationships between motor impairment, compensations and upper limb function in poststroke patients. Specific relationships are unlikely to generalize to all tasks due to kinematic redundancy and task specificity.
Introduction
Following stroke, persistent upper limb (UL) impairment occurs in more than 65% of patients despite intensive and prolonged rehabilitation. 1 UL hemiparesis may be associated with decreased strength and sensation, increased muscle tone, and impaired control of voluntary movement resulting in slow, imprecise, and uncoordinated task-related movement.2-4 Compensatory movement patterns are adopted frequently, especially excessive trunk displacement, shoulder elevation, and shoulder abduction.3,5
A critical question in rehabilitation intervention studies is whether improvements in motor function occur due to recovery of lost motor elements or to the use of compensatory motor patterns. Most UL motor outcome measures at the Activity level of the International Classification of Functioning (ICF), 6 however, mainly quantify the time or degree of task completion on ordinal scales without considering movement quality.7,8 In order to identify true motor recovery, measures should be able to distinguish between restitution of premorbid movement patterns and the use of alternative (compensatory) movement patterns during task accomplishment. 9 This requires the characterization of motor behavior at 2 levels: the performance level describing the movements of the end-effector (ie, hand) in space and the movement quality level describing the joint rotations in body-centered coordinates. At the performance level, the speed, precision, and straightness of endpoint movement can be measured. At the movement quality level, spatial and temporal characteristics of individual joint and segment (ie, trunk) movement is characterized as well as interjoint coordination and muscle activation patterns. 9
The relationship between movement quality and recovery of the ability to perform functional activities is unclear. Clinical trials typically assess the effectiveness of different UL interventions using clinical impairment and/or activity scales as primary outcome measures (eg10-14). However, gaining a better understanding of this relationship depends on a detailed analysis of which joints/body segments are involved in accomplishing a particular task, which can be accessed through the use of high-precision motion analysis systems.
The use of instrumented kinematic analysis has helped identify deficits even in individuals considered well-recovered clinically. 15 While kinematic measures are objective and have excellent psychometric properties, they may not be feasible for clinical use. One solution is the use of outcomes measuring movement quality using observational kinematics or low-cost tracking technology.8-16 The Reaching Performance Scale for Stroke (RPSS) is one such measure that was specifically designed to fill the gap in current outcome measures for the assessment of movement quality. 17 The scale uses numerical ratings to score UL and trunk movement quality and compensations during 2 standardized reach-to-grasp tasks from a seated position. RPSS scores have been shown to differentiate between patients with different levels of arm impairment (discriminant validity17,18).
To assess UL function at the Activity level, the time to completion scores of tasks on the Wolf Motor Function Test (WMFT) are commonly used. The WMFT was originally developed to assess the effects of constraint-induced movement therapy in individuals with mild to moderate stroke. 19 However, the ability of timed scores to capture UL movement quality and therefore identify true motor recovery has been questioned. 8
The objective of the study was to determine if kinematics of UL movement quality during reach-to-grasp tasks identified by observation can be used to describe the relationship between UL motor impairments and the time to perform functional UL tasks (motor performance). We modeled the relationship between scores for each component of the RPSS and the time to complete different functional items of the WMFT. We hypothesized that better movement kinematics during the reach-to-grasp task at the impairment level would be related to better accomplishment of UL functional tasks at the activity level.
Methods
This study is a secondary analysis of baseline data of 141 participants with stroke who participated in the multicenter EVREST (Efficacy of Virtual Reality Exercises in STroke Rehabilitation) randomized controlled trial. 13 In the original study, the primary outcome was UL motor function after a 2-week intervention comparing exergaming in virtual reality using the Nintendo Wii to recreational activities.
Participants aged 18 to 85 years were included if they were in-patients at the time of the study, alert, medically stable, and could follow simple verbal commands. They had to be within 90 days after an ischemic stroke confirmed by neuroimaging (computed tomography or magnetic resonance imaging scan), have a score of <2 on the Modified Rankin Scale (mRS) for functional independence and ≥3 on Chedoke McMaster Arm or Hand Scale. 20 Participants were excluded if they had severe illness and life expectancy less than 3 months, uncontrolled hypertension, unstable angina or recent myocardial infarction, heart failure class III and IV, a history of seizures, global aphasia, visual neglect, pain or joint problems limiting arm and trunk movement, arm or leg amputation, or if they were participating in another clinical trial. All participants signed informed consent forms approved by their local institutions.
Procedure
Demographic and clinical data of participants were collected at baseline and describe, age, gender, handedness, comorbid conditions, type, side, and site of stroke (Table 1). Baseline disability was based on the mRS, Barthel Index (BI) for activities of daily living, and Functional Independence Measure (FIM) score. 21 Stroke severity was assessed using the valid and reliable Canadian Neurological Scale (CNS).22,23 The CNS estimates neurological status of an individual in which scores of ≥8, 5 to 7, and 1 to 4 indicate mild, moderate, and severe stroke severity, respectively.
Demographic and Clinical Characteristics of Study Participants. a
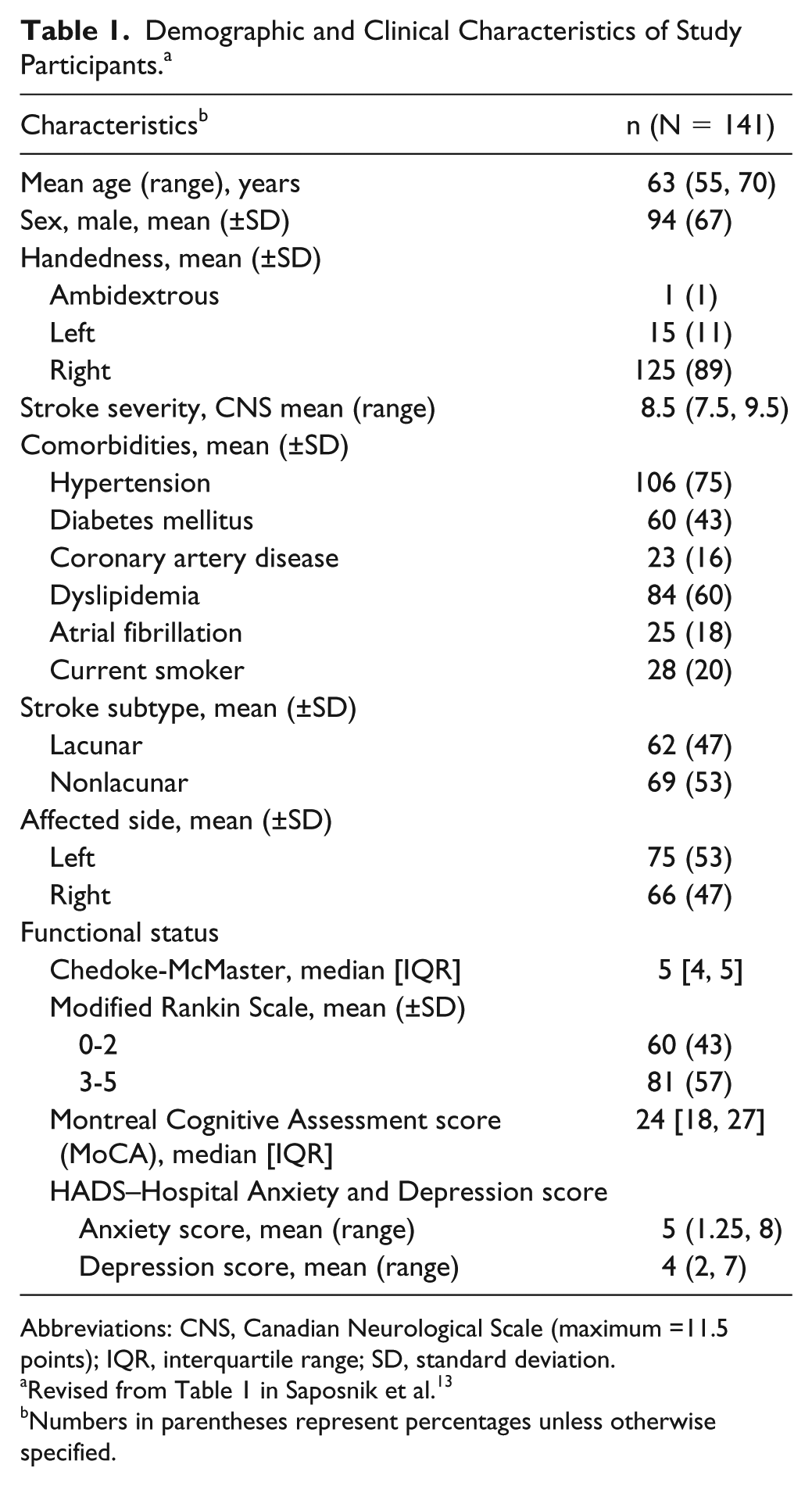
Abbreviations: CNS, Canadian Neurological Scale (maximum =11.5 points); IQR, interquartile range; SD, standard deviation.
Numbers in parentheses represent percentages unless otherwise specified.
Outcome Measures
We determined the relationship between UL impairment and activity based on clinical scales to determine whether and how movement quality affected the ability to perform specific motor activities of the affected limb. Our primary outcomes were values of individual items from 2 clinical scales, assessed at baseline in the original study by trained physiotherapists. These were the RPSS 17 and 7 items from the WMFT. 19 Standardization of assessment was addressed by providing assessors with equal amounts of training on how to apply each scale, but interrater reliability was not assessed.
Reaching Performance Scale for Stroke
The RPSS quantifies UL and trunk movement patterns and compensations used when reaching to grasp a cone located close to (RPSS-Close) and far (RPSS-Far) from the body. In patients with acute to chronic stroke, Levin et al 17 reported that RPSS has excellent intra- and interrater reliability (intraclass correlation coefficients [ICCs] >0.8, both targets) and moderate to excellent convergent validity with grip force (Pearson r = 0.60 to 0.64), arm and hand impairment (Chedoke McMaster Stroke Assessment, CMSA, Gowland et al 20 ; r ≥ 0.9 both targets) and activity (Test d’évaluation des Membres Superieurs de Personnes Agées, TEMPA 24 ; r = −0.84 to −0.88). The reaching target (cone) is placed in the subject’s midline in the Close or Far UL workspaces. The Close target is within the subject’s arm length while the Far target is beyond their arm reach, thus requiring a combination of arm joint rotations and trunk sagittal movement. Six movement components are scored individually to assess reaching quality to each target: trunk displacement, movement smoothness, shoulder movements, elbow movements, prehension, and global score. Each item is scored on 4-point scales ranging from 0 (only compensations used) to 3 (no compensations used), for a total score of 18 for each target distance. Movement components evaluated are: trunk displacement, endpoint movement smoothness, shoulder movements (eg, shoulder flexion, abduction and scapular elevation), elbow movements (eg, extension), quality of prehension, and a measure of global task performance. The first 5 items quantify the quality of specific components of the movement pattern, while the global task performance item scores task accomplishment based on the presence or absence of compensatory strategies. Assessors viewed each participant performing the movement to Close and Far targets 3 times each, and indicated their score on a checklist.
Wolf Motor Function Test
Seven standardized items from the original WMFT were evaluated (Item 1: Forearm to Table; Item 4: Extend Elbow horizontally with a weight; Item 6: Hand to Box placed in the front; Item 9: Lift Can; Item 11: Lift Paper Clip; Item 13: Flip Cards; Item 16: Fold Towel; Wolf et al. 2001). These items were chosen to represent tasks that did (items 9, 11, 13, 16) and did not require (items 1, 4, 6) prehensile ability. Performance on each item was scored as task completion time with a stopwatch where 120 seconds per item was the maximal time allowed.
Statistical Analysis
Categorical data were summarized by frequencies and percentages, and continuous variables by means, standard deviations (SD), median, and interquartile ranges (IQR). Multivariable regression models were used to examine the association between individual RPSS component scores and each of the WMFT outcome items, while adjusting for Chedoke McMaster Scale (Stage) and the baseline CNS scores. Separate analyses were done for the RPSS-Close and RPSS-Far target data. For these analyses, a time of 1.5 to 2 seconds was considered the minimal clinically important difference (MCID), or the smallest change in score that would indicate a meaningful difference in the function of the upper limb. 25 This range was determined from anchor- and distribution-based MCID analysis of the whole WMFT scale 26 and MCIDs for individual items on the scale. 27 Transformations of the data were not done to preserve the interpretability of the results in the original units of each variable.
The estimated effects and 95% confidence intervals for the individual RPSS components were reported for all WMFT outcome items. The apparent and corrected R2 values were reported as measures of model fit for the multivariable regressions. Model validation was performed using bootstrap with 200 iterations to estimate the optimism on the apparent R2 for the primary outcomes. Statistical analysis was performed using R 3.5.1 (R Core Team, Vienna, Austria, 2018) and a significance level of .05.
Results
Total scores and scores for each item of the WMFT and RPSS are summarized in Table 2. For the WMFT, both mean (SD) and median (IQR) values are shown due to the skewness of the data. Data from all participants were included for each analysis except for the relationship between the WMFT Extend Elbow task and both RPSS Close and Far target components for which data from 1 participant was excluded since their value was 25 times greater than the group mean in each case. Overall, the multivariable models had low explanatory power with corrected adjusted R2 values ranging from −0.0043 to 0.380 (Table 3). The best models were those for the more functional WMFT tasks of Lift Can, Flip Cards, and Fold Towel, for which the regression explained 20% to 38% of the variance, while the models explained less than 17% of the variance for the remaining 4 tasks.
Values of Total and Individual Item Scores of the Wolf Motor Function Test (WMFT) and the Reaching Performance Scale for Stroke (RPSS) for 141 Patients. a
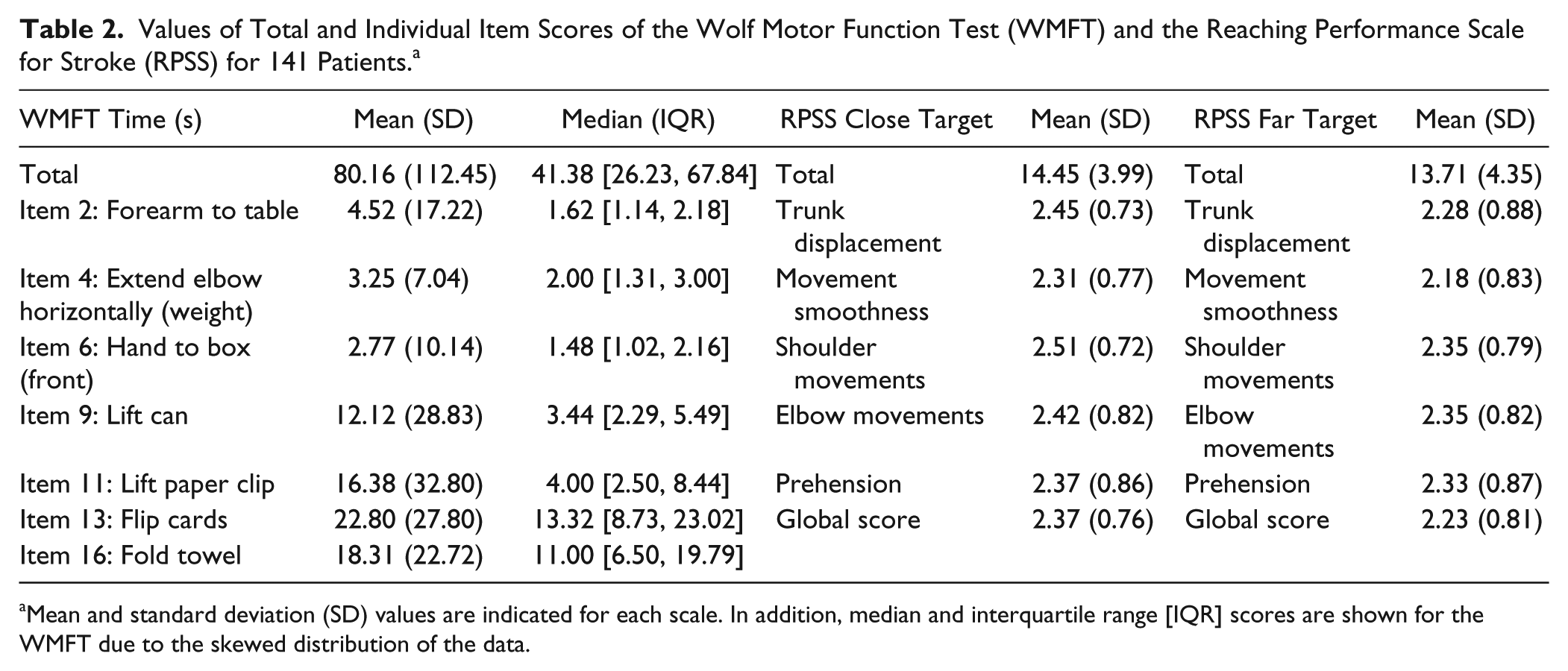
Mean and standard deviation (SD) values are indicated for each scale. In addition, median and interquartile range [IQR] scores are shown for the WMFT due to the skewed distribution of the data.
Coefficient Estimates and Confidence Intervals for Multivariable Regression Models Between Items on the Wolf Motor Function Test (WMFT) and Components of the Reaching Performance Scale for Stroke (RPSS) for the (A) Close and (B) Far Targets. a
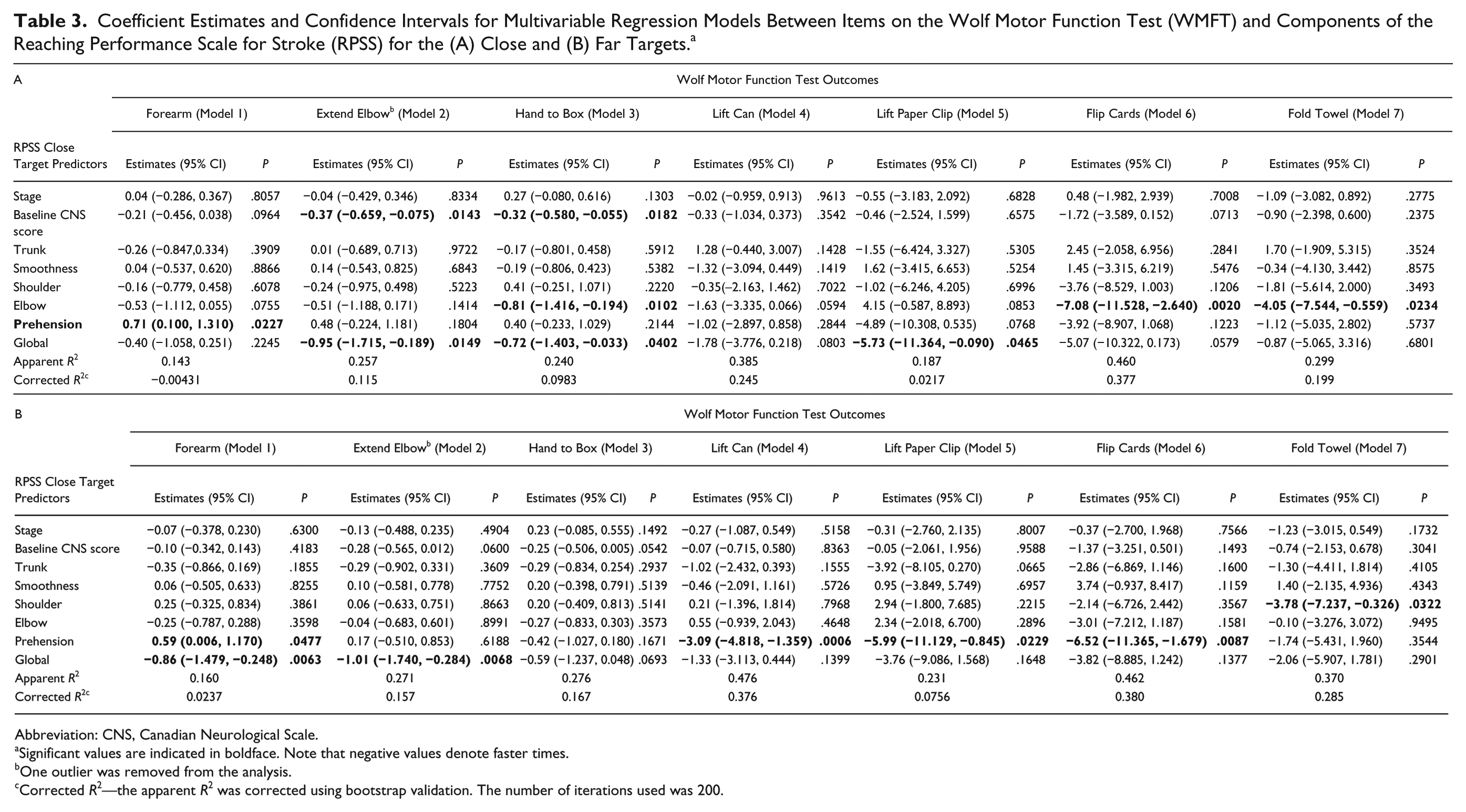
Abbreviation: CNS, Canadian Neurological Scale.
Significant values are indicated in boldface. Note that negative values denote faster times.
One outlier was removed from the analysis.
Corrected R2—the apparent R2 was corrected using bootstrap validation. The number of iterations used was 200.
Relationships Between WFMT Tasks and RPSS Close Target Component Scores
Overall, the trunk, shoulder, and endpoint smoothness components of the RPSS did not predict the performance of any of the WMFT tasks (Table 3, panel A). However, elbow, prehension, and global component scores predicted the performance on some items of the WMFT.
For the Close target, every unit increase in the elbow score of the RPSS predicted a faster performance time of 0.81 seconds (95% CI −1.416 to −0.194, P = .01) for the Hand to Box task, 7.08 seconds (95% CI −11.528 to −2.640, P = .002) for Flip Cards; and 4.05 seconds (95% CI −7.544 to −0.559, P = .0234) for Folding a Towel. The evidence of a decrease in the time spent on performing the Flip Cards task is strongest for the elbow predictor, as the confidence interval excludes zero and the upper 95% confidence limit is −2.64, which exceeds the magnitude of the MCID of 1.5 to 2 seconds.
Every unit increase in the prehension component predicted slower performance on the Forearm to Table task of 0.71 s (95% CI 0.100 to 1.310, P = .0227), but this value was below the MCID90 of 1.8 seconds. 27
For the global component, every unit increase in score predicted faster performance on 3 WMFT items: Extend Elbow (0.95 seconds, 95% CI −1.715 to −0.189, P = .0149), Hand to Box (0.71 seconds, 95% CI −1.403 to −0.033, P = .0402), and Lift Paper Clip (5.73 seconds, 95% CI −11.364 to −0.090, P = .0456). For this component, the first 2 values were below the MCID while that for the Lift Paper Clip presented the strongest evidence.
Relationships Between WFMT Tasks and RPSS Far Target Component Scores
Far target components of trunk movement, endpoint smoothness, and elbow movement did not predict performance on any of the WMFT tasks (Table 3, panel B). For the Far target, every unit increase in the shoulder movement score predicted a 3.78 seconds faster performance on the Fold Towel task (95% CI −7.237 to −0.326, P = .0322). The prehension component predicted behavior on 4 of the WMFT items tested. Better scores on the prehension component predicted slower performance on the Forearm to Table task (0.59 seconds) and was a strong predictor for faster performance on the Lift Can (3.09 seconds), Lift Paper Clip (5.99 seconds), and Flip Cards (6.52 seconds) tasks (Table 3, panel B). Finally, each unit increase in global score on the Far Target RPSS predicted faster performance by 0.86 seconds on the Forearm to Table task of the WMFT, though this value was also below the MCID.
Discussion
This study sought to determine if observational clinical outcome measures could be used to describe the relationship between UL motor impairments and the time to perform functional UL tasks. We showed that estimates of the quality of individual movement components during standardized reaching tasks to a close and far target were related to significant changes in the performance of both simple (ie, Forearm to Table, Extend Elbow, Hand to Box) and complex functional tasks (ie, Lift Can, Lift Paper Clip, Flip Cards, Fold Towel) included in the WMFT. While overall the predictive power of changes in movement elements on functional activities was small, they were more clinically significant for predicting faster performance on the more complex functional tasks than the simpler movements. Specifically, only better global performance on the RPSS-Far target was related to faster performance times for the Forearm to Table task, while better prehension scores for both the RPSS-Close and RPSS-Far target tasks predicted slower movement times for this task. However, the magnitude of the changes in performance times, although statistically significant, were well below (ie, <1 second) the MCID of 1.5 to 2 seconds for meaningful clinical change. Similar statistically but nonclinically significant relationships were found for the Extend Elbow and Hand to Box WMFT tasks.
In contrast, clinically significant decreases (>2 seconds) in performance time for WMFT tasks of Lift Can, Flip Cards, and Fold Towel were predicted from RPSS-Close and RPSS-Far target components. For the other task involving prehension (Lift Paper Clip), although clinically significant decreases in performance time were linked to better global performance on the RPSS-Close target and better prehension on the RPSS-Far target task, the overall strength of the regression models was low.
For the more complex functional tasks, our results were similar to previous studies describing relationships between kinematics assessed with motion analysis equipment and specific reaching tasks or activities. In previous studies, the main kinematics associated with a broad class of UL tasks are spatial characteristics of the endpoint (trajectory straightness) and 2 angle/segment excursions (elbow and trunk) as well as temporal characteristics of endpoint displacement (movement time, trajectory smoothness); for review, see Collins et al. 28 These kinematics are similar to 3 of the 5 movement components evaluated with the RPSS (endpoint smoothness, elbow, trunk). One caveat, however, is that the observer scoring movement smoothness on the RPSS cannot visually distinguish between spatial and temporal qualities of smoothness, often described kinematically by endpoint path straightness (spatial) and the number of peaks in the endpoint velocity profile (temporal).
Studies using kinematics have assessed their relationship to different UL tasks such as pointing, reaching and drinking from a glass.29-31 For example, Subramanian et al 30 related different UL kinematics to total scores on the Fugl-Meyer Assessment (FMA). The majority of variance in FMA scores was explained by a combination of trunk displacement and shoulder flexion (51%) for a pointing task and by trunk displacement alone (52%) for a reach-to-grasp task. Trunk displacement alone distinguished between levels of motor impairment on the FMA. Alt-Murphy et al 31 similarly found that only 1 movement (trunk displacement) and 1 temporal variable (endpoint smoothness) used during a standardized reach-to-grasp task explained 67% of the variance in the Action Research Arm Test. Our results, using observational kinematics, are similar in that we found that up to 38% of the variance of some tasks on the WMFT could be explained by movement variables used for a reach-to-grasp task. The lower values in our study may be related to our attempt to map different aspects of UL kinematics during a standardized reaching task to specific types of arm gestures from the WMFT instead of matched tasks 30 or global scores. 31 It is likely that due to task-specificity, kinematics related to one task do not directly predict performance on a different task. Evidence to support this assertion is that trunk displacement, often identified as a compensatory movement to assist reaching tasks, 3 was not found as a predictor of the performance of any of the WMFT tasks involving reaching. This is reassuring as it suggests that better performance on these WMFT items may not have been due to greater use of compensatory trunk movement, but rather to better levels of behavioral recovery. The remaining variance in the WMFT items may have been related to movement elements not quantified in the RPSS such as interjoint coordination and muscle efficiency.
Explanations Based on the Principle of Redundancy
How the system combines joint rotations to accomplish a movement is strongly task-specific and object-related.32,33 In addition, even simple reaching tasks can be accomplished by a large variety of combinations of movements of arm and trunk joints.34-37 Transport of the hand to an object is potentially accomplished by the coordinated movements of 4 joints contributing 10 degrees of freedom. Thus, in terms of motor control, the system is considered to be redundant since there are more degrees of freedom than necessary to perform a task. 34 Rather than being considered an impediment to movement, the large number of degrees of freedom is thought of as being “abundant” since it allows the system to accomplish tasks using a large amount of interjoint variability. 38 Such variability has been characterized using methods such as principal component 39 and uncontrolled manifold analyses 29 based on a large number of trials recorded during the performance of carefully prescribed tasks. In subjects with stroke, these analyses have revealed that the composition of principal components and the structure of variability is altered compared with controls, even if patients are still capable of performing the task, that is, the task is performed in a different way. For example, Reisman and Scholz 29 examined the variance across trials of 10 degrees of freedom during performance of a reaching task and found that patients with chronic mild-to-moderate stroke used different patterns of joint couplings compared with age-matched controls. We found that individual joint kinematics did not explain much of the variance in the performance of simple tasks such as placing the forearm on a table or extending the elbow. This is likely because the time score on the WMFT does not directly indicate what problems may have been encountered in performing these actions or that the task could be performed in different ways. In contrast, the RPSS components explained more of the variance for the more complex WMFT tasks, but still, this amount was low. The tasks on the WMFT are complex since they require not only the transport of the hand to the target but also the manipulation of the target object with the hand. Thus, the remaining variance may be related to characteristics not measured by the RPSS, such as anticipatory adjustments, temporal aspects of arm transport and grasping, prehension forces, sensory deficits, and so on.28-31
Relationship Between Motor Compensation and Task Performance
The elbow movement element on the RPSS-Close target scale predicted performance on 3 of the WMFT tasks, while the prehension and shoulder elements on the RPSS-Far target scale predicted performance on 4 of the tasks. In particular, faster accomplishment of WMFT tasks involving arm movements (ie, Extend Elbow, Hand to Box) was partially explained by components measured in the RPSS-Close target task while better performance of tasks involving manipulation (Lift Paper Clip, Flip Cards, Fold Towel) depended on multiple elements captured in the Close target measure as well as prehension and shoulder movement from the RPSS-Far target measure. The RPSS scale was originally intended to identify motor compensations during the performance of a reach-to-grasp task. One of the elements, trunk displacement, is a major compensation often observed during reaching. 3 Although the RPSS trunk movement component had large estimated effects, the 95% CIs were large and crossed zero. This suggests that trunk movement was highly variable and could either decrease or increase the time to perform functional arm activities. The question of the influence of trunk compensatory movement on accomplishment of functional arm tasks cannot therefore be fully addressed in this study.
Study Limitations
While there are several advantages to the use of observational kinematics over motion analysis approaches, there are also some limitations. Evaluation of the extent to which a movement element is used during performance of a task may be affected by the clinician’s level of experience with observational motion analysis and may require a period of familiarization and training. Comparison of RPSS observational scoring with instrumented motion analysis would be necessary to further validate the RPSS scale. It should also be recognized that the RPSS does not assess movement planning but only movement execution. Another limitation of the RPSS scale is that only one reach-to-grasp task is evaluated to objects located at 2 different distances in the sagittal plane. Given the known task-specificity of how the redundant system may organize kinematics, it is unclear to what extent a reach-to-grasp task to a sagittal target may generalize to other tasks involving movement in other directions. Since participants in this study had mild-to-moderate motor deficits, results may not generalize to those with greater motor impairment. In addition, although we used scales with high interrater reliability, we did not measure or standardize potential differences between blinded assessors.
Conclusions
Our results from the pretest data of a randomized controlled study comparing Nintendo Wii with recreational activities suggest that clinical movement analysis based on observation may be used as a low-cost, clinically accessible alternative to sophisticated motion analysis to better understand the relationship between motor impairment and functional movement. In contrast, motion analysis–based kinematic recording requires costly and complicated equipment that is not easily accessible in the clinic. It is also time consuming to record and then analyze kinematic data, which is another barrier to the clinical uptake of this technology. Alternatively, use of the RPSS scale to quantify the contribution of movement quality to the performance of a task may be an accessible and valid alternative to recording kinematics in the laboratory and clinic. It should be noted, however, that due to task specificity, the movement quality elements assessed with the RPSS are likely more valid for assessing the influence of kinematic elements of similar functional tasks involving reaching and grasping.
Footnotes
Acknowledgements
The authors are indebted to all participants of the EVREST Multicenter clinical trial.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by initial funding from the South East Toronto Stroke Network and a grant from the Heart and Stroke Foundation of Canada (HSFC), the Ontario Ministry of Health and Long Term Care and the Ontario Stroke Network (OSN).