
Abstract
We investigate if rTMS has a therapeutic role in the treatment of dysphagia in patients with Parkinson’s disease (PD). Material and Methods. Thirty-three patients with PD and dysphagia were randomly classified with ratio 1:2 to receive sham or real rTMS (2000 pulses; 20 Hz; 90% resting motor threshold; 10 trains of 10 seconds with 25 seconds between each train) over the hand area of each motor cortex (5 minutes between hemispheres) for 10 days (5 days per week) followed by 5 booster sessions every month for 3 months. Assessments included the Unified Parkinson’s Disease Rating Scale part III (UPDRS), Instrumental Activities of Daily Living (IADL), and Arabic–Dysphagia Handicap Index (A-DHI) before, after the last session, and 3 months later. Video-fluoroscopy measures of pharyngeal transit time (PTT) and time to maximal hyoid elevation (H1-H2) were taken before and after the treatment sessions. Results. There were no significant differences between groups. There was a significant improvement on all rating scales (analysis of variance) after real rTMS with a significant time × group interaction. In particular, there was a significant and long-lasting (3 months) effect of time on all subitems of the A-DHI (functional, P = .0001; physical, P = .0001; emotional, P = .02) but not in the sham group. This was associated with significant improvement in H1-H2 (P = .03) and PTT (P = .01) during solid swallows in the real rTMS but not the sham group. Conclusion. Real rTMS improves dysphagia in PD as documented by A-DHI scores and by video-fluoroscopy.
Keywords
Introduction
Swallowing dysfunction is common in idiopathic Parkinson’s disease (PD), being symptomatic in up to 54.5% of patients especially in patients with predominantly akinetic rigidity 1 but seen in more than 90% using video-fluoroscopy.2-4 It is usually considered multifactorial with abnormalities documented in all phases of swallowing. 3 The underlying neurogenic mechanisms of swallowing dysfunction in PD are not well established although involvement of nondopaminergic mechanisms has been suggested. 5 Indeed, even though levodopa treatment improves limb symptoms in PD 6 deglutitive dysfunction may fail to respond,5,7,8 and may even occasionally deteriorate. 9
Current dysphagia management in PD patients is unsatisfactory. A number of approaches including dietary modification and swallowing maneuvers, 10 dopaminergic and anticholinergic pharmacotherapy, 11 expiratory muscle strengthening, 12 video-based biofeedback therapy, 13 cricopharyngeal myotomy, 14 and cricopharyngeus botulinum toxin injection 15 have all been utilized with variable outcomes.
More recently, there have been a number of trials testing possible neuromodulatory techniques in PD patients with dysphagia. One of these studies recruited 90 patients with PD and applied surface electrical stimulation over the submental region. At the end of the study there was significant improvement in the treated groups. 16 Dysphagia in other groups of patients has been treated with noninvasive brain stimulation (NIBS) techniques such as transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). A meta-analysis found that repetitive TMS (rTMS) has a positive effect on dysphagia after stroke although the best frequency (low vs high frequency) and site (affected, unaffected, or bilateral hemispheres) are yet to be resolved.17-20 However, there have been no studies of the effects of brain stimulation methods for dysphagia in patients with PD.
Given that rTMS has been shown to have beneficial effects on limb motor control in PD, 21 we decided to conduct a trial to test its effectiveness on dysphagia. Given the proximity of the hand area of M1 (5 cm lateral to Cz and 1 cm anterior to Cz) to the esophageal motor area (6.6 cm lateral to Cz and 3.0 anterior to Cz), 19 we hypothesized that we might achieve beneficial effects on both dysphagic and limb symptoms.
Patients and Methodology
Patients
Ninety PD patients with dysphagia using UK brain bank criteria for PD 22 were recruited from the outpatient clinic in Assiut University during the period from May 2016 to Jan 2018. Each patient was aged between 50 and 75 years and all fulfilled the UK brain bank criteria for PD. Patients were excluded if they had a history of repeated head injury, cerebrovascular strokes, encephalitis, oculogyric crisis, supranuclear gaze palsy, drug intake as antipsychotics or MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) exposure, severe dementia (Mini-Mental State Examination [MMSE] ≤23), 23 severe depression (Hamilton Rating Scale for Depression [HAM-D]), 24 severe dysautonomia, cerebellar signs, Babiniski sign, strictly unilateral features after 3 years, hydrocephalus, or intracranial lesion on neuroimaging. To allow delivery of rTMS patients were also excluded if they had intracranial metallic devices or with pacemakers or any other device. Patients who were unable to give informed consent were also excluded. Treatment was maintained constant throughout the trial with no change in dosage. All received levodopa (Sinemet 250/25; ½ tablet 3 times per day) and anticholinergic (cogenitol ½ tablet 3 times per day).
The sample size was calculated using G power software based on the following assumptions: proportion of expected outcome in the intervention group = 30% (according to the previous study), proportion of the expected outcome in the placebo group = 1%, alpha level = 0.05, power = 0.80 with allocation ratio N2/N1 = 1, using 2-tailed test.
Methods
All cases were assessed with modified Hoen and Yahr staging, 25 Unified Parkinson’s Disease Rating Scale (UPDRS) part III, 26 Instrumental Activities of Daily Living (IADL), 27 Self-Assessment scale, 28 Swallowing Disturbance Questionnaire (SDQ) for dysphagia for diagnosis of dysphagia, 29 and Arabic -Dysphagia Handicap Index (A-DHI). 30 Video-fluoroscopy examination while patients were on levodopa therapy was performed for 9 patients in the real rTMS group and 6 from the sham group.
The SDQ consists of 5 questions related to the oral phase of swallowing and 10 questions related to the pharyngeal phase. Fourteen questions were rated on a 4-point (0-3) scale (0 for no disability and 3 for severe disability) and 1 was a “yes/no” question (yes was scored 2.5 and no was scored 0.5). A score on the SDQ of ≥11 indicates dysphagia.
Arabic-DHI (A-DHI) is a patient-administered, 25-item questionnaire, in which the patient can assign 3 responses for each question (never, sometimes, and always), adding a value to each response (0, 2 and 4, respectively) and reaching a score ranging from 0 to 100. Moreover, each patient performs a self-evaluation of their dysphagia, assigning a score from 0 (normal) to 7 (severe difficulty). 31 The DHI has 9 questions in the functional subscale, 9 question in the physical subscale, and 7 questions in the emotional subscale. 32
Randomization (Parallel Design)
Out of 90 PD patients, 33 patients had dysphagia and participated in the study (see flowchart in Figure 1). Group allocations (real or sham with ratio 2:1) were placed in serially numbered opaque closed envelopes. As we performed a pilot study before starting the trial and found a good response for dysphagia so we thought it ethical to reduce the size of the control group in order to reduce the numbers of patients who had to wait to receive real treatment at the end of the trial. Each patient was placed in the appropriate group after opening the corresponding sealed envelope.
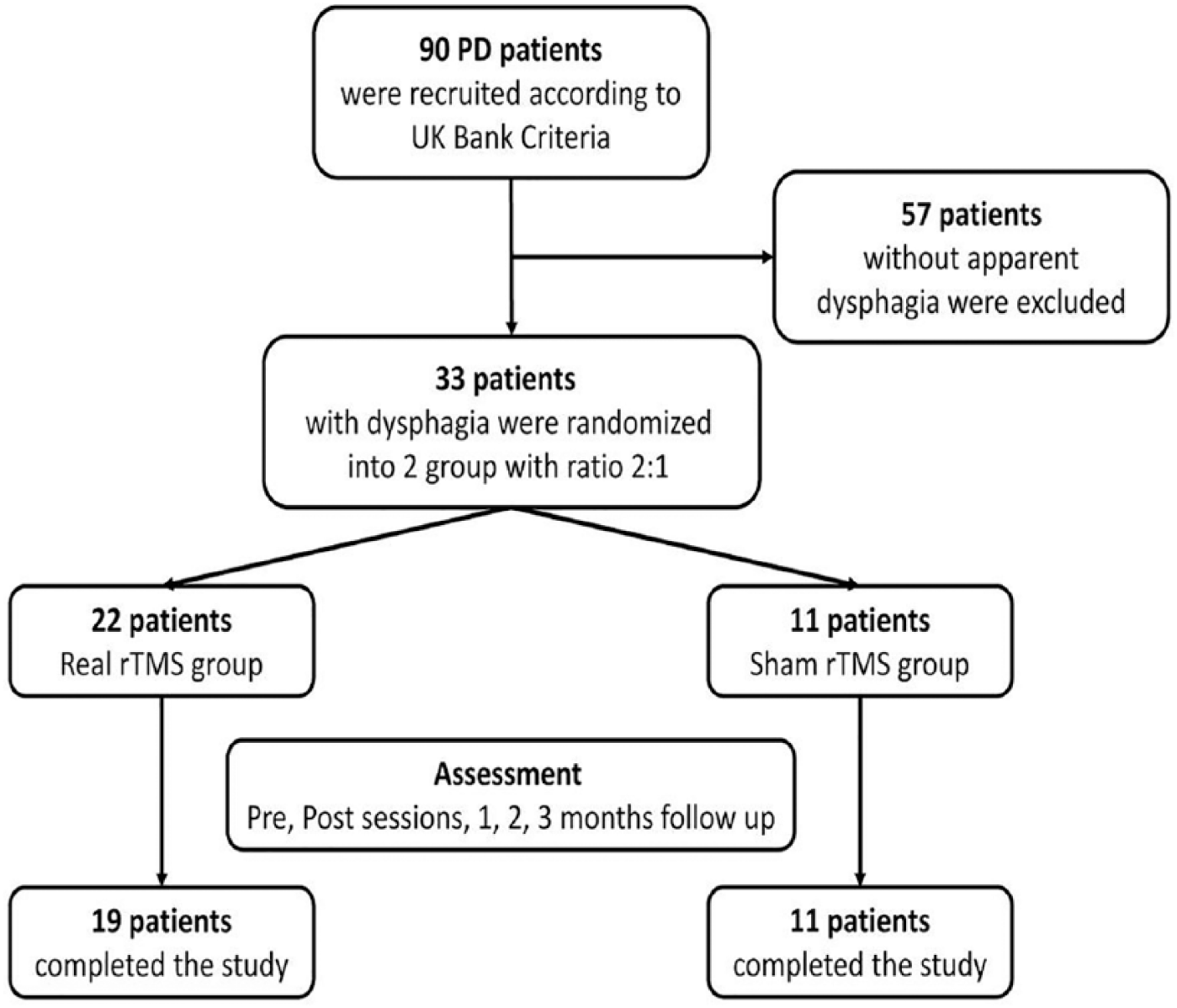
Flowchart.
Measuring Resting Motor Threshold
Resting motor threshold (RMT) was measured with a monophasic magnetic stimulator (Magstim model 200; Magstim, Whitland, UK) connected to a 90-mm outer diameter figure-of-8 coil, which had a maximal output of 2.2 T. We located the optimal scalp location of each hemisphere from which TMS evoked motor-evoked potentials of greatest amplitude by moving the figure-of-8 coil systematically in 1-cm steps to determine the site of maximum peak-to-peak motor-evoked potentials in the first dorsal interosseous for each hemisphere. We used silver–silver chloride surface electrodes, using a muscle belly–tendon montage, with a 3-cm diameter circular ground electrode placed on the wrist. A Nihon Kohden Machine model 9400 (Tokyo, Japan) was used to amplify and record the signals.
Repetitive Transcranial Magnetic Stimulation Procedure
Real rTMS was applied for 10 sessions (5 days per week) using a figure-of-8 coil (9-cm diameter loop) positioned over the hand area. A session of stimulation consisted of sequential stimulation of each hemisphere (right then left hemisphere) with 10 trains of 20-Hz stimulation, each lasting for 10 seconds with an intertrain interval of 25 seconds. The intensity of stimulation was set at 90% of the RMT for the first dorsal interosseous of the contralateral hand with a total 2000 pules for each hemisphere. Given our previous experience in treating PD, 39 we decided to give 5 booster sessions every month for 3 months follow-up. Sham rTMS was applied using the same parameters, but with the coil held so that the edge was in contact with the head perpendicular to the scalp while the remainder was rotated 90° away from the scalp in the sagittal plane to reproduce the noise of the stimulation.
Video-Fluoroscopy Examination (Pre and Post 10 Sessions)
Video-fluoroscopy was performed before and after rTMS sessions while patients were on levodopa therapy using a GE Prestige II (Milwaukee, WI, USA) machine. The examination was performed in an upright lateral position. The field of examination involved the oral cavity and extended down to the upper esophagus. Five milliliters of 3 different consistencies of barium sulphate (fluid, semisolid, solid) were given to patients by a spoon. Cocoa was added to the barium to improve its flavor. Patients were requested to hold the barium in their mouth and only start to swallow when asked by the clinical investigator.
Assessment
Examinations were recorded and assessment was further performed in slow motion in addition to the frame by frame analysis.
Temporal Measures
The pharyngeal transit time (PTT) was measured, in seconds, from the point where the bolus head moved from the hold position and passed the posterior nasal spine until it fully entered the esophagus after the closure of the upper esophageal sphincter. The time of the first superior-anterior movement of the hyoid bone was assigned as H1, and the time when the hyoid bone reached its maximum elevation was assigned as H2. The time required for maximum elevation of the hyoid bone was therefore H2 − H1. The temporal measures of the hyoid bone movement have been previously described. 33
Scoring Measures
Penetration (passage of the bolus into the larynx, above the level of the vocal cord) and aspiration (passage of the bolus into the larynx, below the level of the vocal cord) were assessed using the previously validated 8-point penetration-aspiration scale. 34 Finally, postswallow residue was scored as follows: patients with no residue after swallowing were given a score of 0, those who had residue either in the vallecular or in the pyriform sinus were given a score of 1, while those who had had residue both in the vallecula and pyriform sinus were scored 2.
Follow-up
At the end of the therapy, patients were asked whether they thought they had real or sham rTMS. We followed up the patients clinically after the end of the 10th session, 1, 2, 3 months later after the end of booster sessions using the DHI as a primary outcome. The secondary outcome measures were changes in video fluoroscopy after the 10th session.
Assessment of the different scales (A-DHI and UPDRS and other) were performed by an assessor who was unaware of the type of stimulation. Likewise, the patients also did not know which type of stimulation they received.
We also asked patients specifically whether they experienced any of the common side effects of rTMS. Three patients of the real group refused to complete the sessions: 1 developed headache and insomnia and the other 2 refused to stay in the hospital.
Ethics
Informed consent was obtained from all subjects and the methodology was approval by the faculty of medicine ethical committee.
Statistical Analysis
All data were analyzed with the aid of the SPSS version 16. The results were expressed as mean ± SD. Since some measures were not distributed normally at baseline, age, onset, and duration of illness, nonparametric Mann-Whitney test were used for comparison between groups. Spearman correlations between base line scores were also performed. Statistical analysis of the scores in each test was performed with repeated measures analysis of variance (ANOVA) with Time, as the within-subject factor, and treatment condition (real and sham rTMS) as the between subject measure. Greenhouse-Geisser degree of freedom corrections were applied to correct for the nonsphericity of the data. P < .05 was considered significant for all statistical analysis. Spearman correlation between the changes in the total UPDRS III (Pre-Post 10th session) and the changes in DHI (Pre-Post 10th session).
Results
Clinical characteristics are summarized in Table 1. There were no significant differences between groups in age, sex, duration of illness, and total scores in the UPDRS III, IADL, self-assessment scale, and dysphagia scales. There was a significant positive correlation between UPDRS part III and SDQ and total A-DHI at baseline with r = 0.77 (P = .0001) and r = 0.79 (P = .0001), respectively.
Demographic, Clinical, and Staging Data at Baseline Assessment.
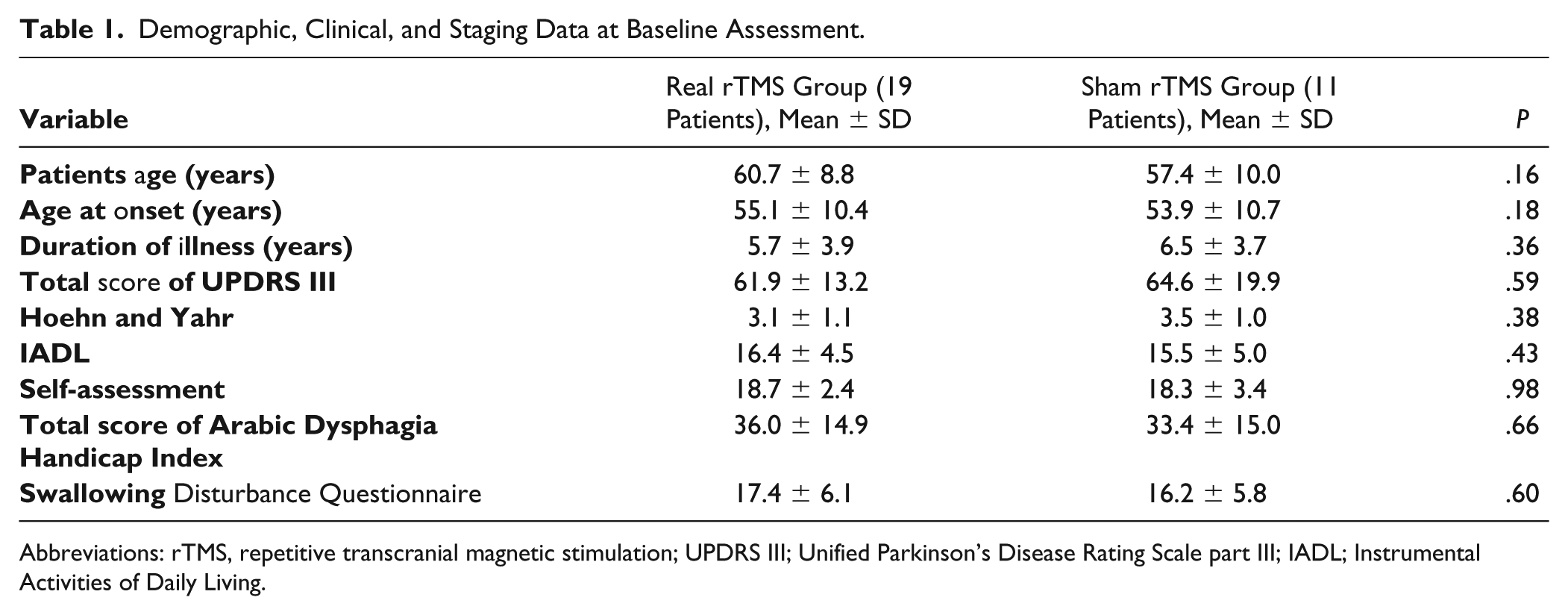
Abbreviations: rTMS, repetitive transcranial magnetic stimulation; UPDRS III; Unified Parkinson’s Disease Rating Scale part III; IADL; Instrumental Activities of Daily Living.
Clinical Scores (UPDRS III, Self-Assessment Scale, and IADL)
One-way repeated measures ANOVA (pretreatment, posttreatment and 1, 2, and 3 months later) showed a significant effect of time on all rating scales (UPDRS III, IADL, self-assessment) in the real group while no such changes were observed in the sham group. Two-way repeated-measures ANOVAs on the scores for each rating scale (Table 2), with treatment Condition (real and sham) and Time (baseline, posttreatment, 1, 2, and 3 months later) as main factors revealed a significant interaction effect for UPDRS III and Self-Assessment scores. There was no significant interaction for IADL. The mean change in UPDRS III (Pre-Post 10th session) was significantly higher in the real group (22.0 ± 9.9) than in the sham group (2.3 ± 5.4; P = .0001).
Effect of 10 Sessions of High-Frequency rTMS on Different Clinical Rating Scales (UPDRS III, IADL, and Self-Assessment) Among Studied Groups.
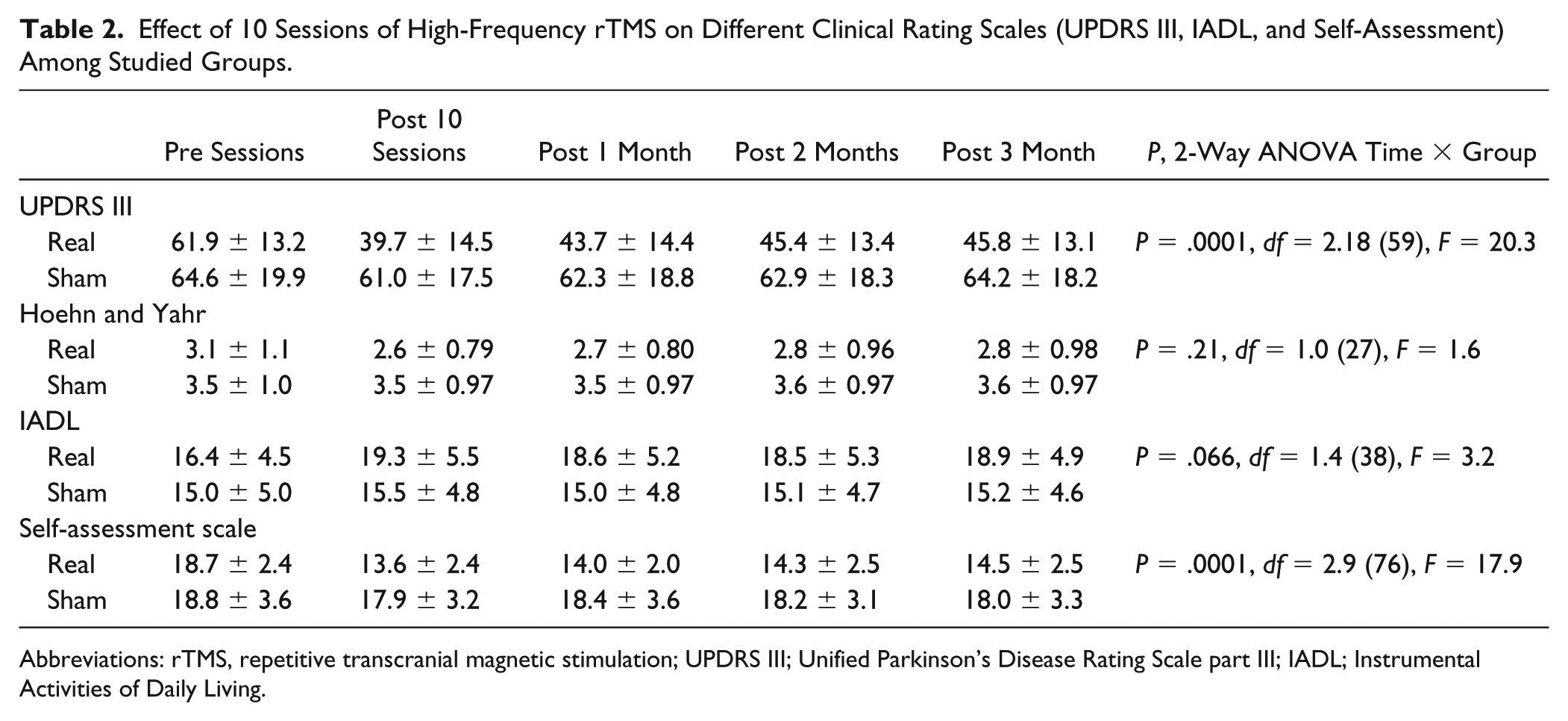
Abbreviations: rTMS, repetitive transcranial magnetic stimulation; UPDRS III; Unified Parkinson’s Disease Rating Scale part III; IADL; Instrumental Activities of Daily Living.
Dysphagia Scores (A-DHI)
One-way repeated-measures ANOVA (pretreatment, post treatment and 1, 2, and 3 months later) showed a significant effect of time on all sub items (functional, physical, and emotional) as well as the total score of the A-DHI in the real group while no such changes were observed in the sham group. Two-way repeated-measures ANOVAs on the scores for each rating scale, with treatment Condition (real and sham) and Time (baseline, posttreatment, 1, 2, and 3 months later) as main factors revealed a significant interaction effect for A-DHI subitems and total scores (Figure 2 and Table 3). The mean reduction in the A-DHI (Pre-Post 10th session) was significantly greater (good improvement) in the real group (14.4 ± 9.9) than the sham group (0.9 ± 3.0) (P = .0001). There was a significant positive correlation between the changes of UPDRS III and the changes in DHI score (r = 0.68 and P = .0001).
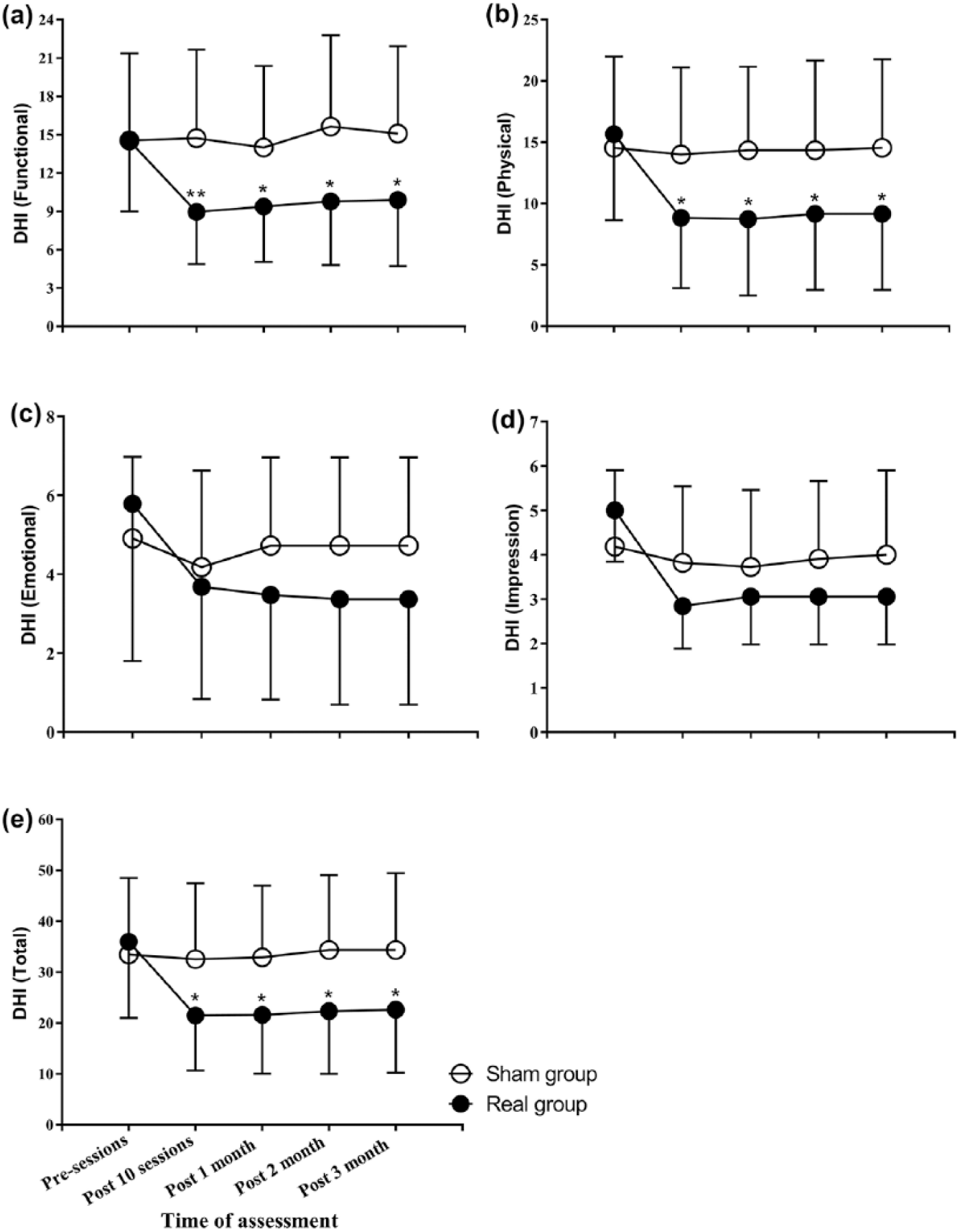
Changes in the Arabic–Dysphagia Handicap Index (A-DHI) among the studied group. A significant effect of time (pretreatment, posttreatment and 1, 2, and 3 months later) on all subitems (functional, physical, and emotional) as well as the total score of the A-DHI in the real group while no such changes were observed in the sham group. A significant interaction effect (Time × Group) for A-DHI subitems and total scores.
Effect of 10 Sessions of High-Frequency rTMS on A-DHI Among Studied Groups.
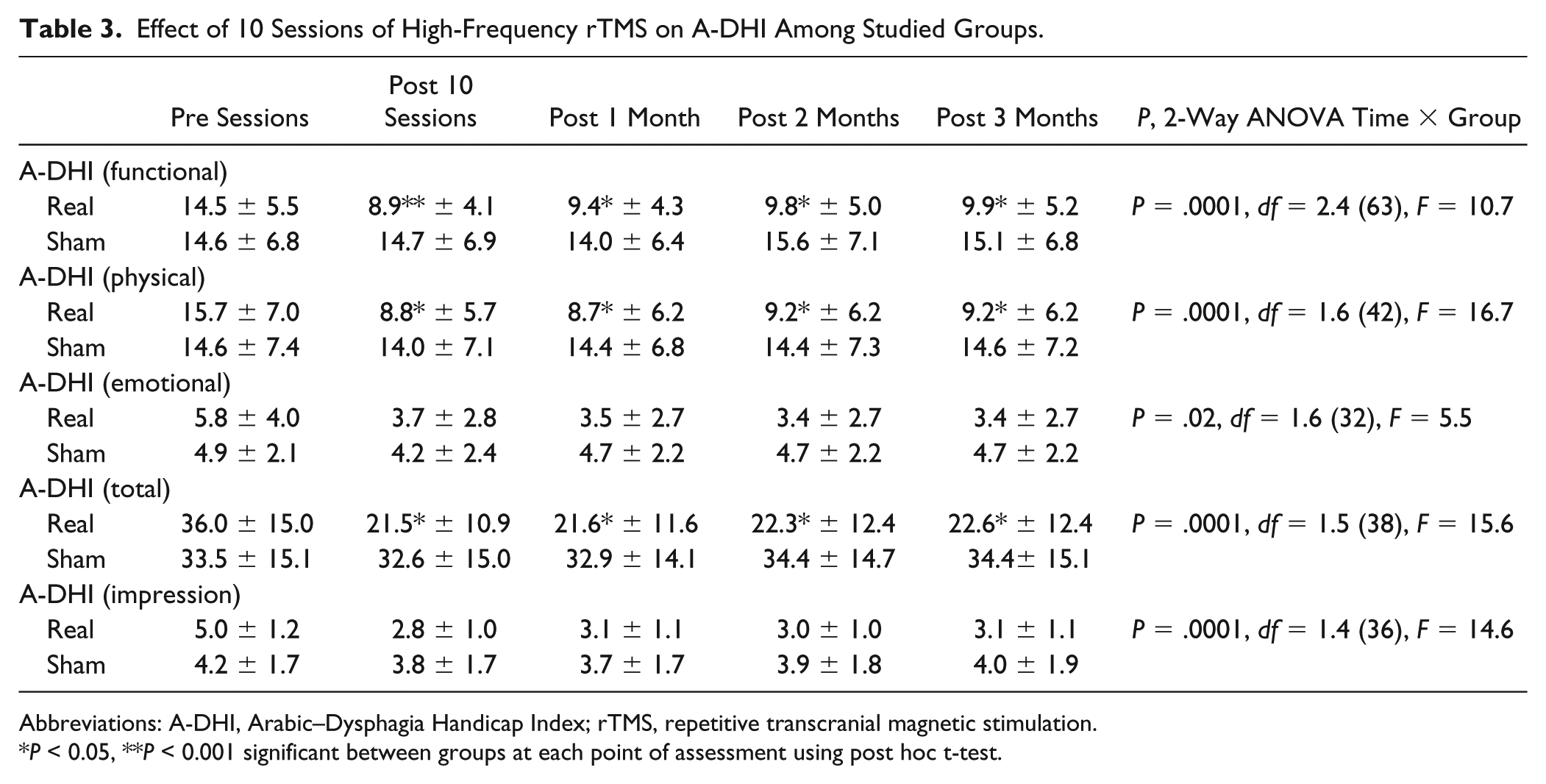
Abbreviations: A-DHI, Arabic–Dysphagia Handicap Index; rTMS, repetitive transcranial magnetic stimulation.
P < 0.05, **P < 0.001 significant between groups at each point of assessment using post hoc t-test.
Video-Fluoroscopy
Two-way ANOVA showed significant Time (pre, post) × Group (real, sham) interaction between groups for solid swallows (P = .007 and P = .03, respectively), due to a significant improvement in the real rTMS group but not sham. There were no significant interactions for fluid or semisolid swallows. However, paired t tests showed a significant improvement in H1-H2, and PTT for fluid swallowing in the real rTMS group (P = .04 and P = .03, respectively) while no such changes were observed in the sham group. There was no difference between groups in the scores of penetration-aspiration or residue (Table 4 and Figures 3 and 4).
Video-Fluoroscopy Details of Each Item Pre and Post Sessions in Studied Groups.
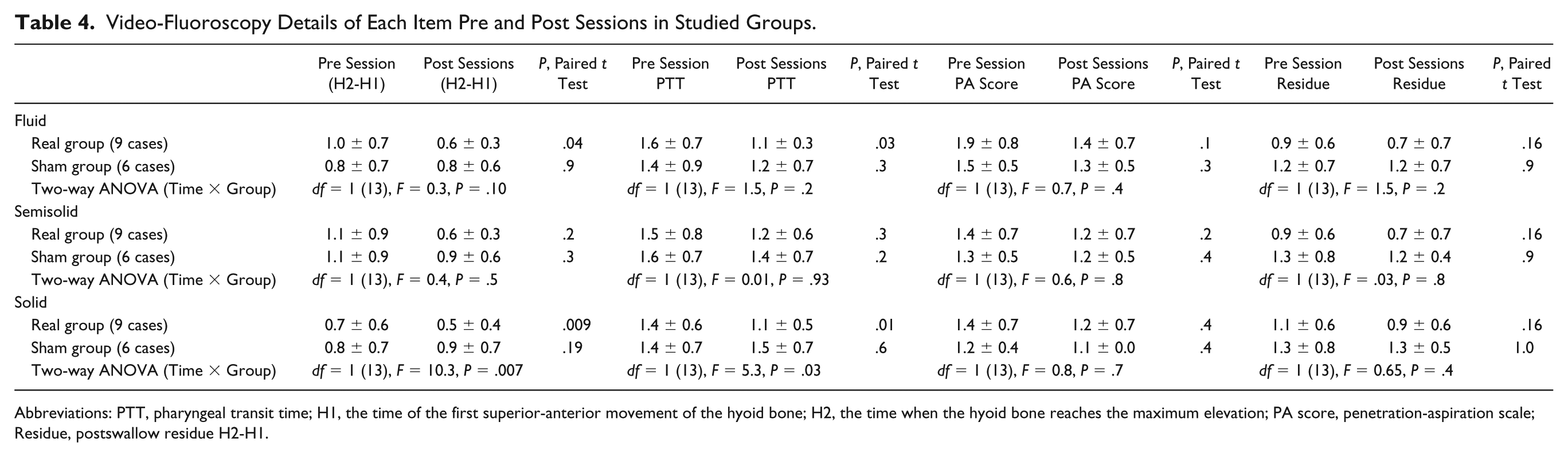
Abbreviations: PTT, pharyngeal transit time; H1, the time of the first superior-anterior movement of the hyoid bone; H2, the time when the hyoid bone reaches the maximum elevation; PA score, penetration-aspiration scale; Residue, postswallow residue H2-H1.
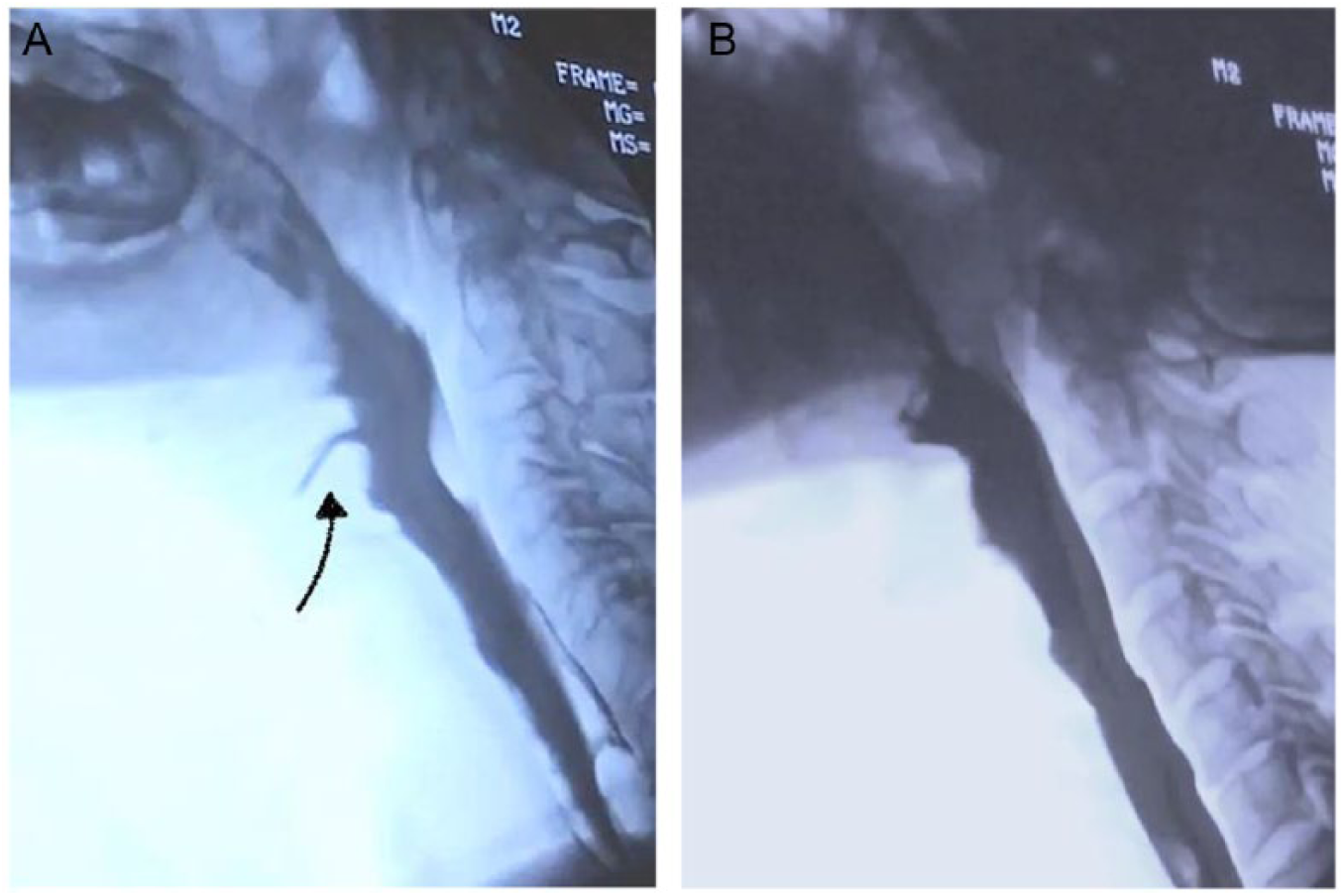
Lateral fluoroscopic views in a Parkinson’s disease (PD) patient with dysphagia. (A) Before repetitive transcranial magnetic stimulation (rTMS) sessions, there is a penetration, scored as (3) on the penetration-aspiration scale, with fluid bolus entering the airway (arrow). (B) Notable improvement is shown after rTMS sessions, with no evidence of penetration. Sore (1) on the penetration-aspiration scale.
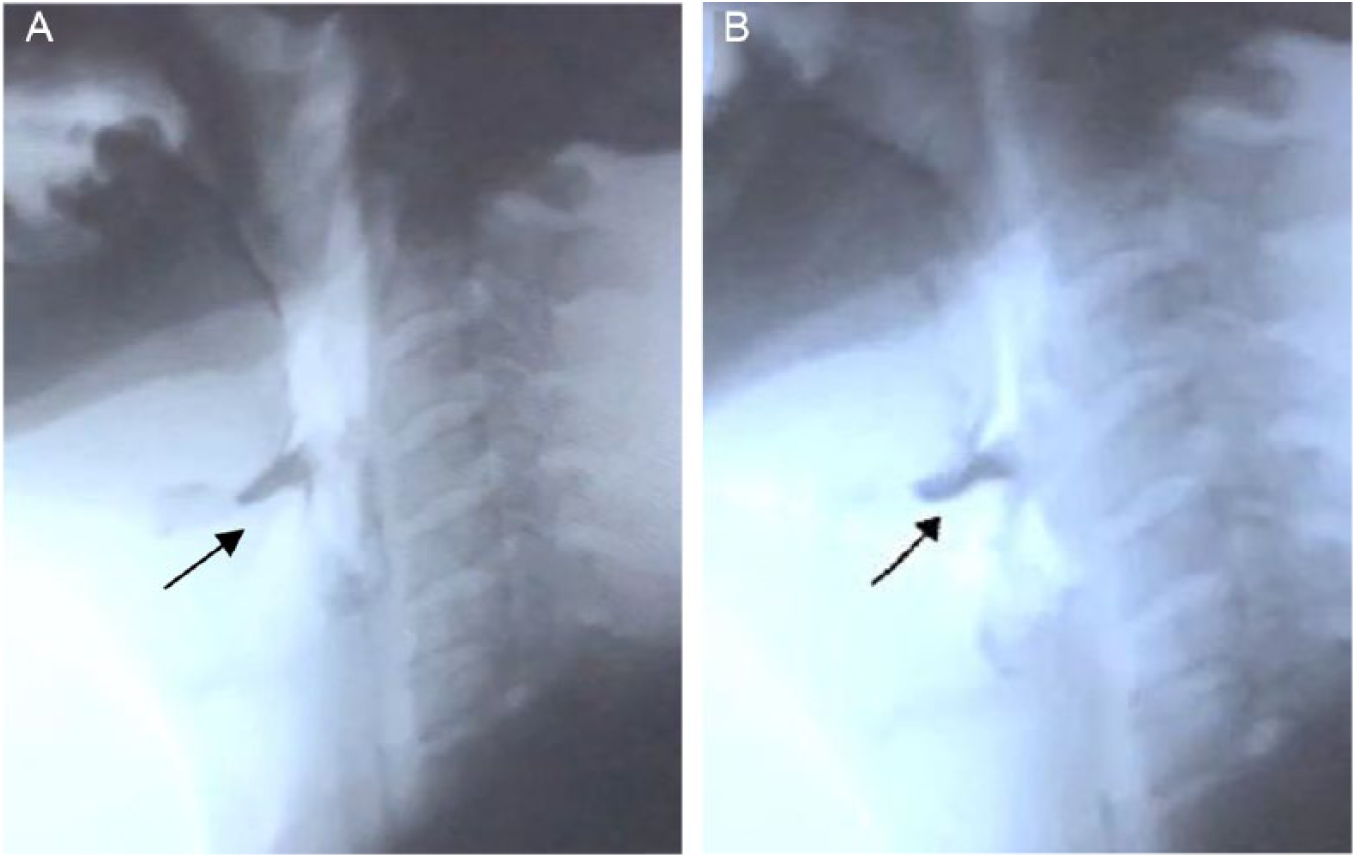
Lateral fluoroscopic views in a Parkinson’s disease (PD) patient with dysphagia. (A) Before repetitive transcranial magnetic stimulation (rTMS) sessions, residual barium is filling the vallecula (arrow). (B) No notable clearance of the barium after rTMS.
Discussion
The mechanisms of dysphagia in PD are still unclear and this has limited progress in the management dysphagia. Levodopa treatment generally is accepted to have little effect on dysphagia in PD, 8 and there are even a few (small-sized) studies with formal assessments reporting that levodopa has an unfavorable effect on swallowing.5,35 Here we explored the possibility of employing new neuromodulatory methods to tackle dysphagia in PD. As noted in the introduction, several previous studies have shown that rTMS can have beneficial effects in poststroke dysphagia as well as dysphagia following a lateral medullary syndrome.36,37 rTMS has also been reported to have beneficial effects on limb movement symptoms in PD. Thus, a logical progression is to assess the effect of rTMS in treating dysphagia in PD. Applying rTMS approaches to different disease etiologies will provide us further information about the endogenous plastic changes in humans with regard to swallowing function.
In the present study, we applied bilateral high-frequency rTMS to treat dysphagia in PD. The rationale was that our previous work had shown that high-frequency rTMS increases the excitability of M1 in healthy volunteers 38 and improves motor performance in patients with PD. 39 This was confirmed by Lomarev et al 40 who applied high-frequency rTMS bilaterally (4 cortical targets: left and right motor and dorsolateral prefrontal cortex) in 18 patients with PD and also reported that times for executing walking and complex hand movement tests gradually decreased. 40 Since we have shown that high frequency rTMS can improve poststroke dysphagia, we chose to use the same parameters in the present study, reasoning that if we applied the TMS over motor cortex, we would achieve a positive effect on movement control as well as dysphagia. Indeed, we found that rTMS over the motor hand area improved both dysphagia and motor scores as measured by A-DHI rating scores, UPDRS III, and self-assessment, respectively, whereas there was no effect of sham. Our results were confirmed by video-fluoroscopy, at least for solid swallows.
The rigidity, hypertonia, bradykinesia, and involuntary movements in PD can interfere in the motor control of swallowing, increasing the risk for penetration and laryngeal aspiration. It has been suggested that rigidity and bradykinesia of may compromise the oral preparatory phase, which is under volitional motor control. These are the symptoms most likely to be ameliorated by rTMS, and it therefore would seem logical to have some improvement of swallowing. However, whether these are the most important factors in producing the improvement we observed is unclear since treatment with levodopa, which has good positive effects on bradykinesia and rigidity is usually reported to have little or even an unfavorable effect on swallowing.5,8,35
Although we targeted the hand/arm area of motor cortex, its close proximity to structures including the esophageal motor area cannot fully exclude the possibility that the after-effects we saw were due to excitability changes at esophageal motor cortex, which might have more direct effects on corticobulbar activity and excitability.
In recent years, neuroimaging and neurostimulation studies have provided insights into the activation patterns of the swallowing sequence.41,42 A meta-analysis of imaging studies on swallowing 43 showed that the most consistent areas that are activated in these neuroimaging studies include the primary sensorimotor cortex (M1/S1), sensorimotor integration areas, the insula and frontal operculum, the anterior cingulate cortex, and supplementary motor areas. In the present study, stimulation of M1 could enhance the functional connectivity of swallowing network and interactions of involved brain regions as it has been described for resting state and during swallowing.44-46
Video-fluoroscopy is an objective measure of swallowing function but was only available in about half of the patients, limiting the statistical power. Nevertheless, we observed a significant difference in the effect of real versus sham rTMS on the PTT and H1-H2 times for solid swallows. Interestingly, both measure movement speed and are related to the bradykinesia and hypokinesia of limb movement. 47 A similar result could be seen in fluid swallows, but this was not significant, perhaps because this is more difficult to quantify in the absence of computerized methods of assessment. However, despite this improvement in speed of transit of the food bolus through the pharyngeal cavity there was no difference in the penetration-aspiration or residue scores. The pharyngeal residue reflects impairment of pharyngeal muscle contractility and the subsequent weak propulsion of the bolus. 48 The small size of the bolus used in our study might have contributed to the lack of the difference in the residue scores. The mild degree of penetration reported in our population, might explain the lack of effect on penetration-aspiration scores.
Limitations
Small sample size limits the power of this study and a larger sample size is recommended for future investigations. In addition, obtaining an adequate sham for rTMS is tricky. However, given that our participants had not received any TMS previously, we do not think they would have perceived they were being given sham treatment. A possible solution in future trials might be to consider active stimulation at an inactive scalp site as we have done in previous study. 39 Another limitation was the absence of a healthy control arm for video-fluoroscopy.
Conclusions
The main conclusion is that real rTMS improves dysphagia in Parkinson’s disease as documented by A-DHI scores and by video-fluoroscopy. The effect can be seen immediately following the last treatment session and up to 3 months later. However, it should be noted that over that 3-month follow-up period, patients were receiving a “top-up” treatment of 5 rTMS sessions every month, and this may have been instrumental in maintaining the effect.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.