
Abstract
Background. Mobility dysfunctions are prevalent in persons with multiple sclerosis (PwMS), thus novel rehabilitation mechanisms are needed toward functional training. The effect of auditory cueing is well-known in Parkinson’s disease, yet the application of different types of auditory stimuli at different tempi has not been investigated yet. Objectives. Investigating if PwMS, compared with healthy controls (HC), can synchronize their gait to music and metronomes at different tempi during walking and the effects of the stimuli on perceived fatigue and gait. Additionally, exploring if cognitive impairment would be a factor on the results. Methods. The experimental session consisted of 2 blocks, music and metronomes. Per block, participants walked 3 minutes per tempi, with instructions to synchronize their steps to the beat. The tempi were 0%, +2%, +4% +6%, +8%, +10% of preferred walking cadence (PWC). Results. A total of 28 PwMS and 29 HC participated. On average, participants were able to synchronize at all tempi to music and metronome. Higher synchronization was obtained for metronomes compared with music. The highest synchronization for music was found between +2% and +8% of PWC yet pwMS perceived less physical and cognitive fatigue walking to music compared with metronomes. Cognitive impaired PwMS (n = 9) were not able to synchronize at tempi higher than +6%. Conclusion. Auditory-motor coupling and synchronization was feasible in HC and PwMS with motor and cognitive impairments. PwMS walked at higher tempi than their preferred walking cadence, and lower fatigue perception with music. Coupling walking to music could be a promising functional walking training strategy.
Introduction
Cognitive and motor impairments are present in persons with multiple sclerosis (PwMS).1-3 In terms of rehabilitation, exercise therapy has shown to be effective for improving or maintaining motor and cognitive functions such as mobility and cognitive processing speed in PwMS.4,5 Another approach for rehabilitation of these functions is task-oriented training. 6 Walking is an ecological type of functional task-oriented training that supports neuroplastic changes as it is activity-specific, involving spinal pattern generators and other motor pathways in the brain.6,7 Walking is also a form of physical activity necessary for activities of daily living in PwMS. 8 However, PwMS are significantly less physically active than healthy subjects, and only a small portion is actually achieving adequate amounts of daily moderate to vigorous physical activity requirements. 9 A contributing limitation to engage in exercise and physical activity, other than motor and cognitive symptoms.10,11—even in mild disabled PwMS—is perceived fatigue 12 ; a symptom highly prevalent in PwMS. 13
In order to overcome the shortcomings of engaging in exercise and physical activity in the presence of impairments described above, we investigated if walking as a form of physical activity can be supplemented by coupling it to auditory stimuli. Auditory-motor coupling can occur when entraining the motor rhythm (recurrent footsteps) to an auditory rhythm (recurrent beats, or pulses).14,15 Once the steps and beats/pulses become locked and aligned in time, they are coupled and said to be synchronized; this can be measured. 16 The auditor-motor coupling component is known to activate alternative neural pathways, such as the reticulo-spinal pathways, to supplement the cortical-spinal pathways and central pattern generators to execute the movement. 17 Additionally, cognitive components are also needed for auditory-motor coupling.15,18,19
The current work expands on the existing evidence in support of different music-based interventions in neurological populations. 20 More specifically, rhythmic-based interventions such as rhythmic auditory stimulation (RAS)—an auditory cueing technique—have been widely investigated to increase gait functions in persons with stroke, 21 cerebral palsy, 22 persons with Parkinson’s disease, 23 aging population, 24 and PwMS. 25 However, when applying RAS across the studies and diseases, tempi used during training were rather inconsistent and ranging from fast and slow, so that recommendations for rehabilitation applications remain open. For Parkinson’s disease, for example, a meta-analysis advised the use of +10% of preferred cadence to enhance gait by increasing cadence, speed, and stride length. 23 However, it is uncertain whether this proposal is also applicable in other neurological conditions which differ in pathophysiology.
Investigating the use of different auditory stimuli such as music and metronome pulses is also relevant. On a series of experiments on healthy subjects, Fritz and colleagues 26 have shown that the musical agency—the feeling of being in control—reduces perceived fatigue when strenuously exercising with music as compared with exercising without music. Additionally, the engagement of the dopaminergic mesolimbic and reward circuit pathways27,28 due to the direct and phenomenal motivational characters of music may contribute to reduced perceived fatigue. The use of different auditory stimuli is not reported in persons with Parkinson’s disease, 29 while in PwMS, it has been reported in one study only, however, in the context of rhythmic-cued motor imagery. 30 Therefore, it is of clinical interest to explore the effect of music in comparison with metronome pulses on perceived fatigue when walking.
The aims of the present study are, first, to investigate in PwMS, compared with healthy controls, if coupling the motor and auditory systems at different tempi is possible with music compared with metronomes. Second, to investigate if the coupling to music compared with metronomes has an effect on perceived fatigue and gait in PwMS compared with healthy controls. We thereby hypothesize that a process of auditory-motor coupling to both stimuli can allow PwMS to surpass the usual walking levels that are determined by their motor or cognitive impairments, and that the use of music as auditory stimuli would be superior over metronomes for perceived fatigue in PwMS. As the process of the coupling requires cognitive components, 19 we also explored if cognitive impairment posed to be a factor in the coupling, and its effects on perceived fatigue and gait.
Methods
Participants
This observational nonblinded case-control study was approved by the Medical Ethical Committees of Hasselt University and Ghent University (Belgium) and multiple sclerosis (MS) centers on November 23, 2016. The study was registered in the clinical trials.gov registry (NCT03281330). We aimed to include 60 participants, 30 PwMS, and 30 age- and gender-matched healthy controls (HCs). Study flyers were used to recruit all participants from the MS centers, the universities, and from several public events organized by the Flemish MS League. Once recruited, the informed consents were signed, and participants were tested for the following inclusion criteria: a diagnosis of MS (>1 year), no exacerbation in the past month, an average comfortable walking speed between 0.4 and 1.4 m/s 31 and older than 18 years. Participants were excluded if they were pregnant, had hearing impairment, or had cognitive impairment hindering the understanding of instructions. Figure 1 illustrates the study selection process, participant flow and experimental procedure.
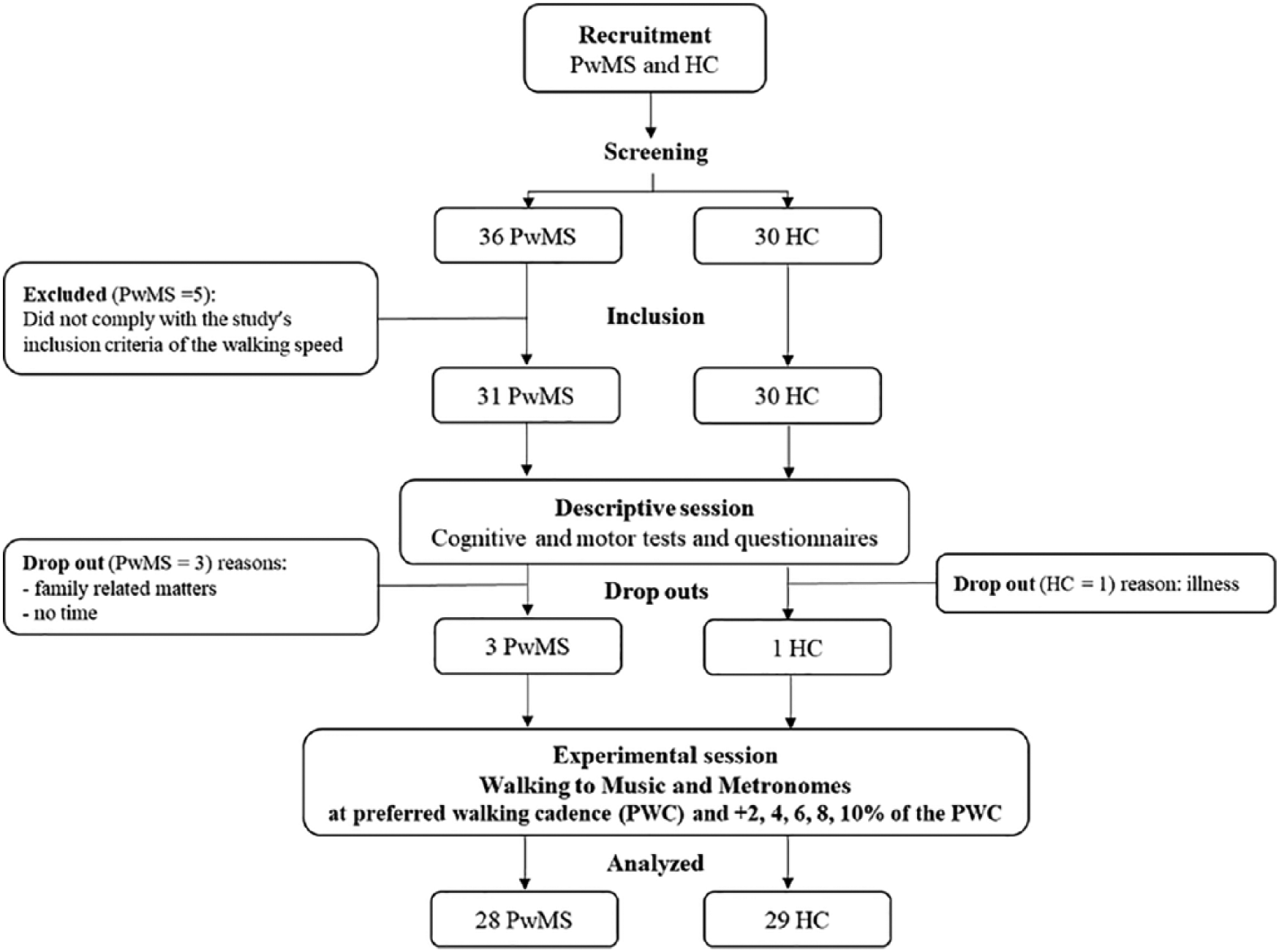
Flowchart illustrating the study selection process, participant flow, and experimental procedure. PwMS, persons with multiple sclerosis; HC, healthy controls.
Descriptive Tests
Descriptive tests were collected in a separate session and included general demographic, disease information, and musical experience. The subscales of rhythm and scale of the Montreal Battery for Amusia were conducted to evaluate amusia. Additionally, the following tests were conducted.
Motor Functions
Timed Up and Go (TUG) and Timed 25-Foot Walk (25FWT) for mobility and Modified Ashworth Scale for muscle tone of the hamstrings and quadriceps.
Cognitive Functions
The 7/24 Spatial Recall Test, to asses visual learning and recall, the Word-List Generation for verbal fluency, the Paced Auditory Serial Addition Test for sustained attention and information processing speed, the Buschke Selective Reminding Test for verbal learning and memory, the Symbol Digit Modality Test for information processing speed and the Stroop color test task for executive function and inhibition.
Self-Reported Questionnaires
The Twelve-Item MS Walking Scale (MSWS), which questioned walking abilities, Modified Fatigue Impact Scale (MFIS), for the impact of their fatigue.
Experimental Procedure
Participants were asked to walk in their comfort tempo in a room with dimensions of 4.5 m × 6 m 3 times for 1 minute, to determine the average preferred walking cadence (PWC) of the day. This was followed by a familiarization task, using the song Sanctum by the artist Shades of the Abyss to instruct participants to synchronize by stepping to the beat. This song was chosen because of its clear beats. A similar familiarization was conducted with metronomes as well. Thereafter, participants were equipped with the D-jogger system and the OPAL sensors (see equipment section below).
All participants walked to 6 tempi, grouped in 2 blocks: Music and Metronome. A 15-minute rest period was allocated between each block. The experimental tempi were: 0% (PWC), +2%, +4%, +6%, +8%, and +10% of the participant’s PWC. For example, if a participant had a baseline of 100 steps per minute, then they received the stimuli at 100, 102, 104, 106, 108, and 110 beats/min, respectively. Each condition consisted of walking for 15 seconds in silence and 3 minutes with the auditory stimuli, followed by 3 minutes of rest. All blocks and tempi were randomized by a digital randomization program. Participants that used a cane were asked to walk with a rollator, to ensure that each step corresponded to a beat.
The Equipment and Stimuli Used
Participants were equipped with 5 APDM sensors (OPAL, USA) to measure the spatiotemporal gait parameters, 32 2 strapped on their ankles, 2 on their wrists, and 1 on the sternum (held in place by a sternum strap). Additionally, participants were equipped with the D-jogger, 33 an adaptive music player, able to provide auditory stimuli at any given tempo by changing the beat frequency of the music and metronome and calculate gait-music synchronization. D-jogger 33 consisted of a software, headphones (Sennheiser, Germany) and 2 iPods (Apple, USA) which were strapped at the ankles. Participants’ PWC was always used as the individual baseline reference.
Personalizing the Music
A personalized music database was used containing songs ranging from 80 to 130 beats/min (see Buhmann et al 34 for details). The songs were sorted into 6 different genres. Participants were asked to choose one genre to walk to in the music block. The available genres were: disco, instrumental, pop, softpop, poprock, and variety.
Primary Outcome Measures
Auditory-Motor Coupling and Synchronization Parameters 16
Relative Phase Angle (rPA) is expressed in degrees and measures the timing of the footfall relative to the beat. This is either a negative (footfall before the beat) or a positive (footfall after the beat) angle.
Resultant Vector Length (RVL) is expressed as a value from 0 to 1 and measures the coherence or stability of the rPA over time. If the distribution of the rPA over time is steep, it results in a high RVL (maximum value 1) and indicates that all footfalls coincide with the auditory beats. If the distribution of the rPA over time is broad or multimodal, it results in a low RVL (minimum value 0) and indicates no stable synchronization. Step and beat data were continuously logged by the D-jogger. 33 Matlab (MathWorks, USA) was used to calculate the rPA and RVL. See Moumdjian et al 16 for a detailed overview of these metrics and their calculations. The cutoff of 0.75 was used to divide participants into those who comply to synchronize (≥0.75) and who do not (<0.75). This cutoff was derived from previous research. 35
Secondary Outcome Measures
Perceived Physical and Cognitive Fatigue and Motivation
Before and after each experimental condition, participants were asked to rate perceived physical and cognitive tiredness on a visual analogue scale (VAS) on a scale of 0 to 10 (0 = not tired at all and 10 = exhaustion). After each condition, participants were asked to rate how motivating it was to walk to the stimuli on a Likert scale of 1 to 5 (1 not motivating at all and 5 highly motivating).
Spatiotemporal Gait Parameters
Cadence (steps/min), velocity (m/s), and stride length (m). Percentage changes were calculated and used in the analysis using the following formula: ((experimental result data – baseline data)/baseline data) × 100.
Statistical Analysis
The descriptive data were checked for normality using the Shapiro-Wilk test, and thereafter, normal distributed data were analyzed by a t test to investigate the difference between groups. Not normally distributed data were analyzed by Wilcoxon signed rank test. The cognitive tests were used in order to classify participants into cognitively impaired (CI) and non-CI persons according to Fischer et al. 36 These were used as a factor in the analysis. A mixed model analysis of variance (ANOVA) was applied by backward model building to the primary (RVL and rPA) and secondary gait (cadence, speed, and velocity) outcome measures, with group (HC vs PwMS) and CI (yes or no) as between-subjects factors and stimuli (Music vs Metronome), experimental tempi (0%, +2%, +4%, +6%, +8%, and +10% of the PWC) and timepoints (minute 1, minute 2, minute 3) as within-subjects factors. For the perceived physical and cognitive fatigue and motivation, the same model as above was used but with the exclusion of timepoints as these data were collected at the end of each condition. A multiple comparisons Tukey’s test was further performed as a post hoc test when interactions were present. All analyses were performed using SAS JMP Pro 13.2.0 (copyright SAS Institute Inc, USA). Missing data accounted <5% of all data collected. When missing data were present, the software ignored that data-point when fitting the model. The significance level was set at P < .05.
Results
Participants
Of 66 participants that were screened (36 PwMS and 30 HC), 61 fit the inclusion criteria (31 PwMS and 30 HC) of which 57 participants (28 PwMS and 29 HC) completed the experimental session as seen in Figure 1. No significant differences in demographic, musical experience, or amusia were detected between groups. Nine PwMS used an assistive device, and 3 PwMS used an ankle-foot orthosis (AFO). PwMS had a range of mild to moderate motor disability based on baseline walking speed (lowest 0.6 m/s, highest 1.4 m/s). The impact of physical, cognitive and psychological fatigue was significantly higher in PwMS than in HCs. Nine PwMS and 3 HC were found to have CI; however, no statistical differences of the motor characteristics were found at baseline between CI and non-CI PwMS as shown in Supplementary Table e-1 (available online). Table 1 shows the descriptive demographic, motor, cognitive characteristics and self-reported questionnaires of the study participants.
Descriptive Demographic, MS-Specific, Motor and Cognitive Characteristics and Self-Reported Questionnaires of the Study Participants.
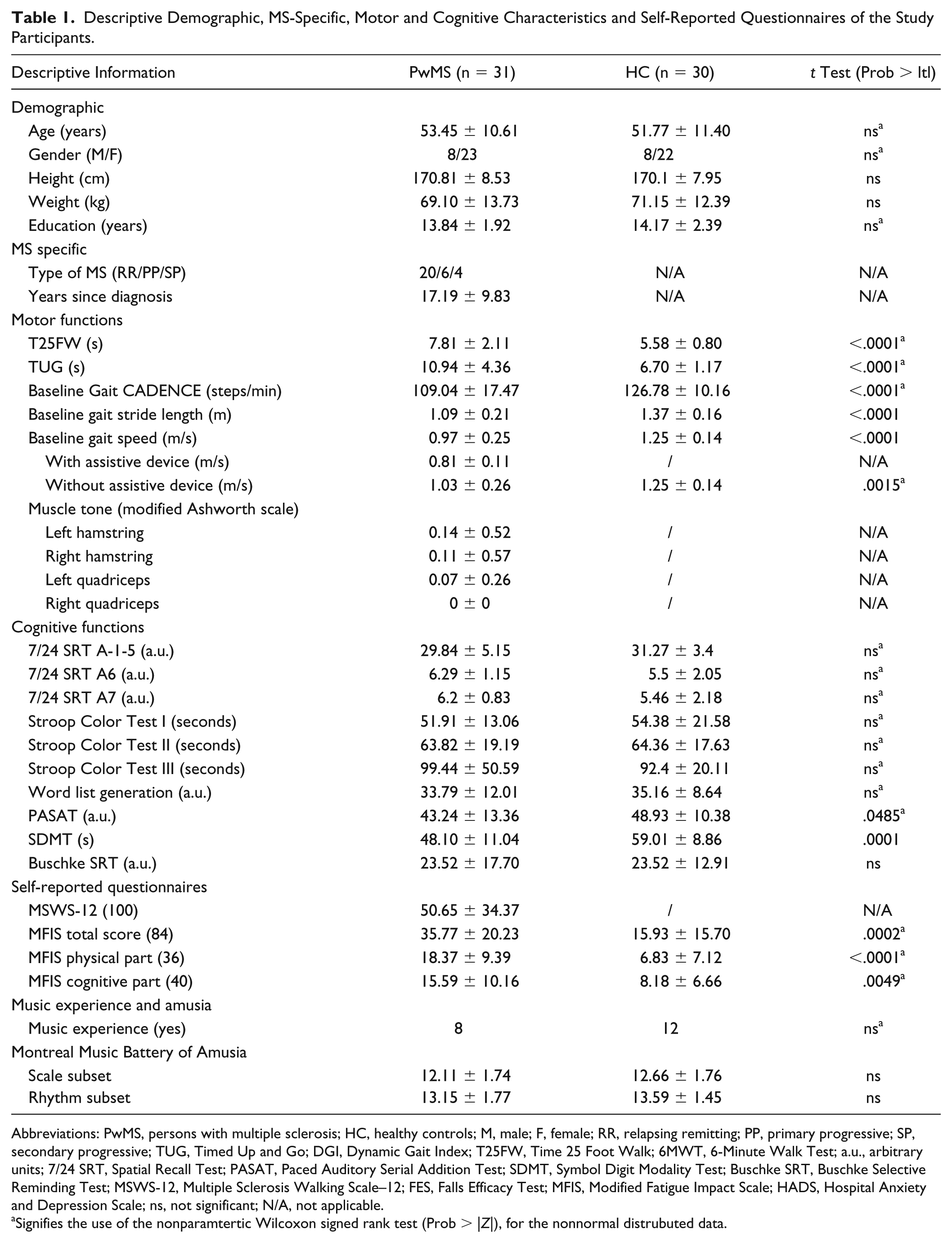
Abbreviations: PwMS, persons with multiple sclerosis; HC, healthy controls; M, male; F, female; RR, relapsing remitting; PP, primary progressive; SP, secondary progressive; TUG, Timed Up and Go; DGI, Dynamic Gait Index; T25FW, Time 25 Foot Walk; 6MWT, 6-Minute Walk Test; a.u., arbitrary units; 7/24 SRT, Spatial Recall Test; PASAT, Paced Auditory Serial Addition Test; SDMT, Symbol Digit Modality Test; Buschke SRT, Buschke Selective Reminding Test; MSWS-12, Multiple Sclerosis Walking Scale–12; FES, Falls Efficacy Test; MFIS, Modified Fatigue Impact Scale; HADS, Hospital Anxiety and Depression Scale; ns, not significant; N/A, not applicable.
Signifies the use of the nonparamtertic Wilcoxon signed rank test (Prob > |Z|), for the nonnormal distrubuted data.
Synchronization to Music and Metronome at Different Tempi and Its Effects on Perceived Fatigue and Gait
The experimental results from all participants when walking to music and metronome at different tempi are found in Tables 2 and 3.
Experimental Results of Walking to Music and Metronome at Different Tempi on Auditory-Motor Coupling, Perceived Cognitive and Physical Fatigue, Perceived Motivation and Gait Parameters.a
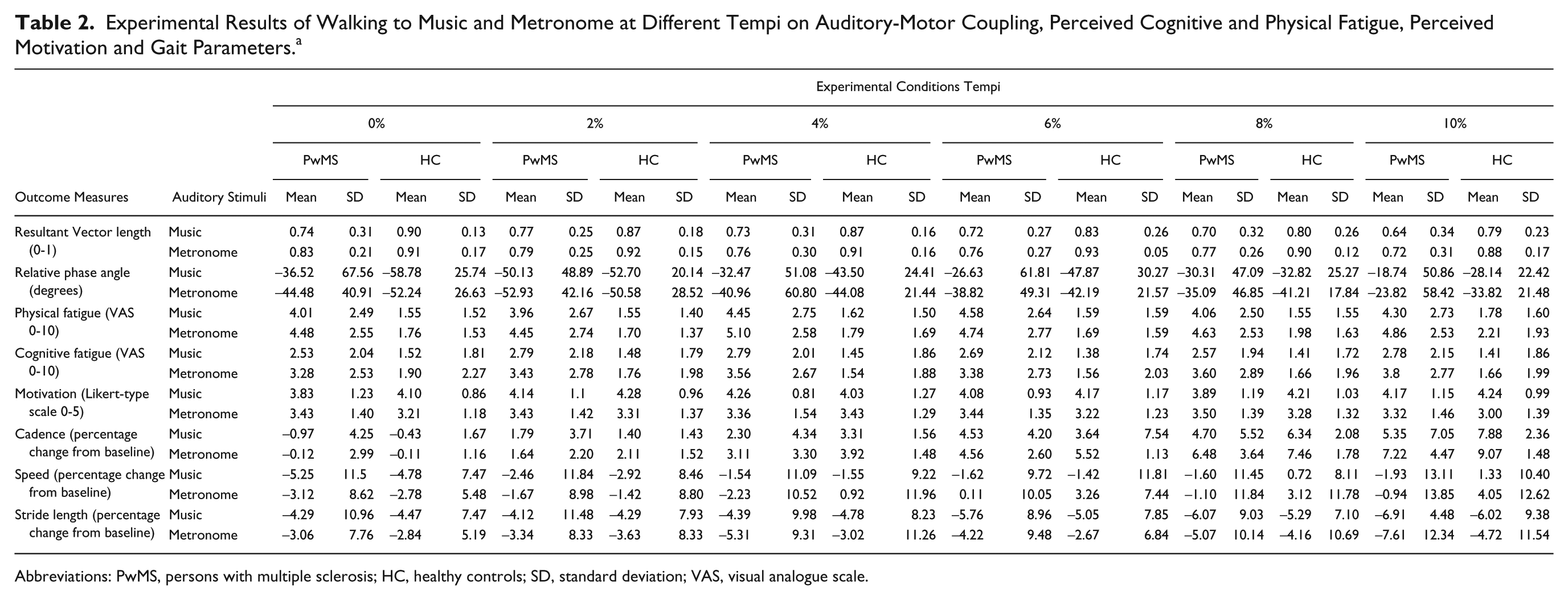
Abbreviations: PwMS, persons with multiple sclerosis; HC, healthy controls; SD, standard deviation; VAS, visual analogue scale.
Experimental Results of the Main Effects and Interactions of the Statistical Mixed Model ANOVA Test of Walking to Music and Metronome at Different Tempi on Auditory-Motor Coupling, Perceived Cognitive and Physical Fatigue, Perceived Motivation, and Gait Parameters. a
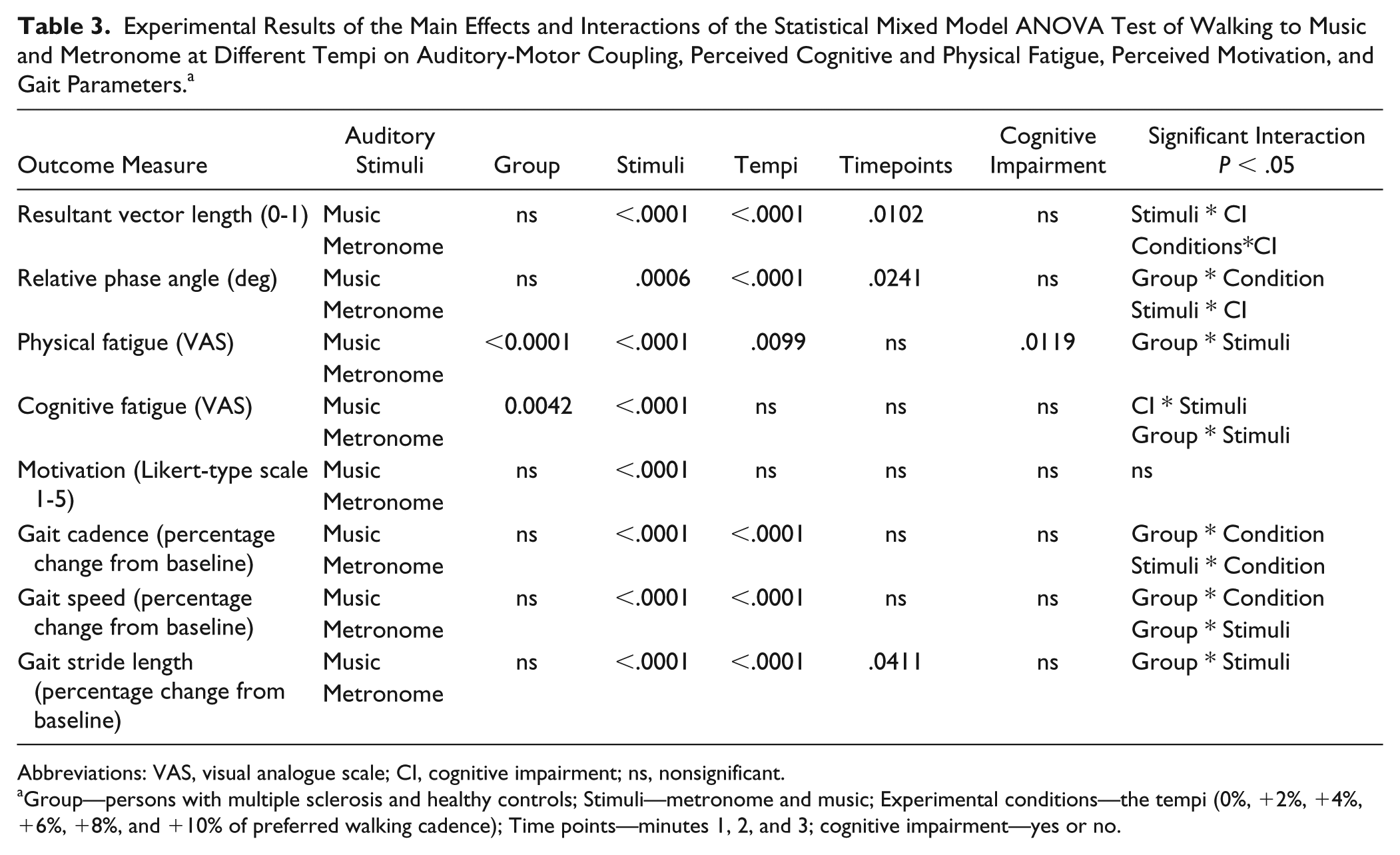
Abbreviations: VAS, visual analogue scale; CI, cognitive impairment; ns, nonsignificant.
Group—persons with multiple sclerosis and healthy controls; Stimuli—metronome and music; Experimental conditions—the tempi (0%, +2%, +4%, +6%, +8%, and +10% of preferred walking cadence); Time points—minutes 1, 2, and 3; cognitive impairment—yes or no.
Primary Outcome Measures
Resultant Vector Length
Overall, participants were able to synchronize to the different tempi. Significant main effects were found for stimuli, F(1, 1819) = 22.44, P < .0001; tempi, F(5, 1819) = 14.28, P < .0001; and time points, F(2, 1818) = 4.60, P = .01. Significant interactions were found for stimuli ∗ CI, F(1, 1819) = 22.65, P < .0001, and tempi ∗ CI, F(5, 1819) = 3.49, P = .0039. The first post hoc test indicated significantly higher RVL for the non-CI group in the metronome session compared to the music session (t = 9.99, P < .0001), and the second indicated that CI persons were able to synchronize from 0% to 6% tempi only (t = 4.34, P < .0009). Figure 2A presents a graphical summary of the RVL.
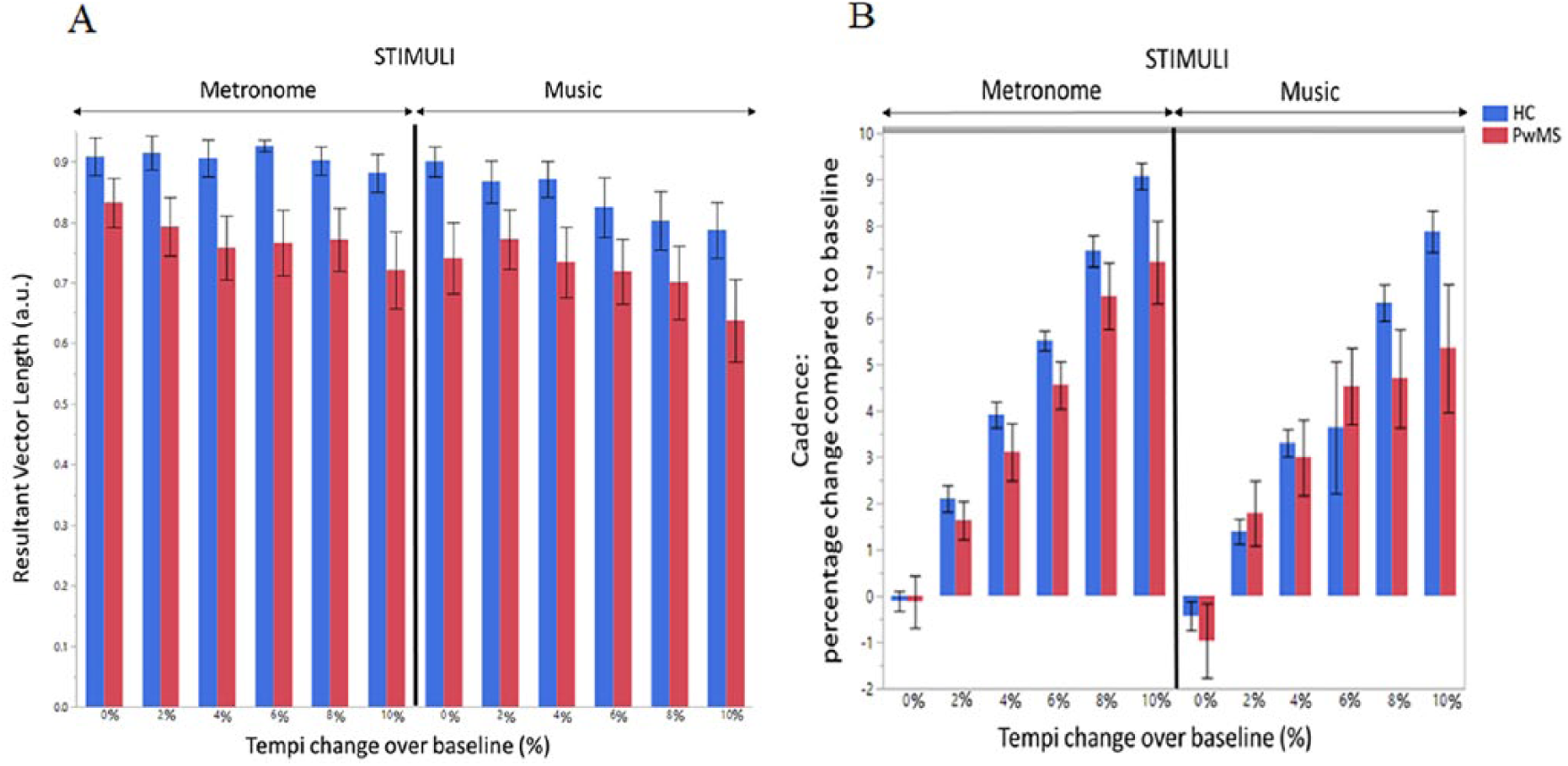
(A, B) Reports on the results between persons with multiple sclerosis (PwMS) and healthy controls (HC) walking to metronome and music at different tempi, 0% and +2%, +4%, +6%, +8%, and +10% of preferred walking cadence. (A) Resultant vector length and (B) Cadence. Mean standard errors are shown.
Relative Phase Angle
Overall, the steps of the participants proceeded the beat, indicating that entrainment was occurring. Significant main effects were found for stimuli, F(1, 1832) = 11.80, P < .0006; tempi, F(5, 1833) = 31.12, P < .0001; time points, F(2, 1832) = 3.73, P = .02. Significant interactions were found for group ∗ tempi, F(5, 1833) = 3.48, P = .0039, and stimuli ∗ CI, F(1, 1832) = 6.79, P = .0092. The first post hoc test indicated PwMS significantly stepped closer to the beat as the tempi increased (t = −504, −3.57, −6.26, P < .001, P = .02, P < .001, respectively, for tempi +6%, +8%, and +10% as compared with PWC). The second post hoc test indicated that CI PwMS stepped significantly closer to the beat when walking to music compared with when walking to metronome (t = −3.43, P = .0034).
Secondary Outcome Measures
Perceived Physical Fatigue
Significant main effects were found for group, F(1, 55) = 23.32, P < .0001; stimuli, F(1, 604) = 29.60, P < .0001; and tempi, F(5, 604) = 2.46, P = .0099. Significant interaction effects were found for group ∗ stimuli, F(1, 604) = 4.85, P = .03. The post hoc test indicated that PwMS perceived significantly less fatigue when walking to music compared with metronomes (t = 5.33, P < .0001).
Perceived Cognitive Fatigue
Significant main effects were found for group, F(1, 52) = 5.40, P = .02, and stimuli, F(1, 590) = 105.11, P < .0001. Significant interaction effects were found for group ∗ stimuli, F(1, 590) = 13.49, P < .0001, and CI ∗ Stimuli, F(1, 590) = 3.57, P = .0003. The post hoc tests indicated that PwMS significantly perceived walking to metronomes to be more fatiguing than HC (t = −2.76, P = .03) and that PwMS perceived walking to music to be less significantly fatiguing than metronomes (t = 10.81, P < .0001), as well as that cognitive impaired persons perceived lower fatigue walking to music compared with metronomes (t = 8.45, P < .0001). Figure 3 presents a graphical summary of the perceived physical and cognitive fatigue.
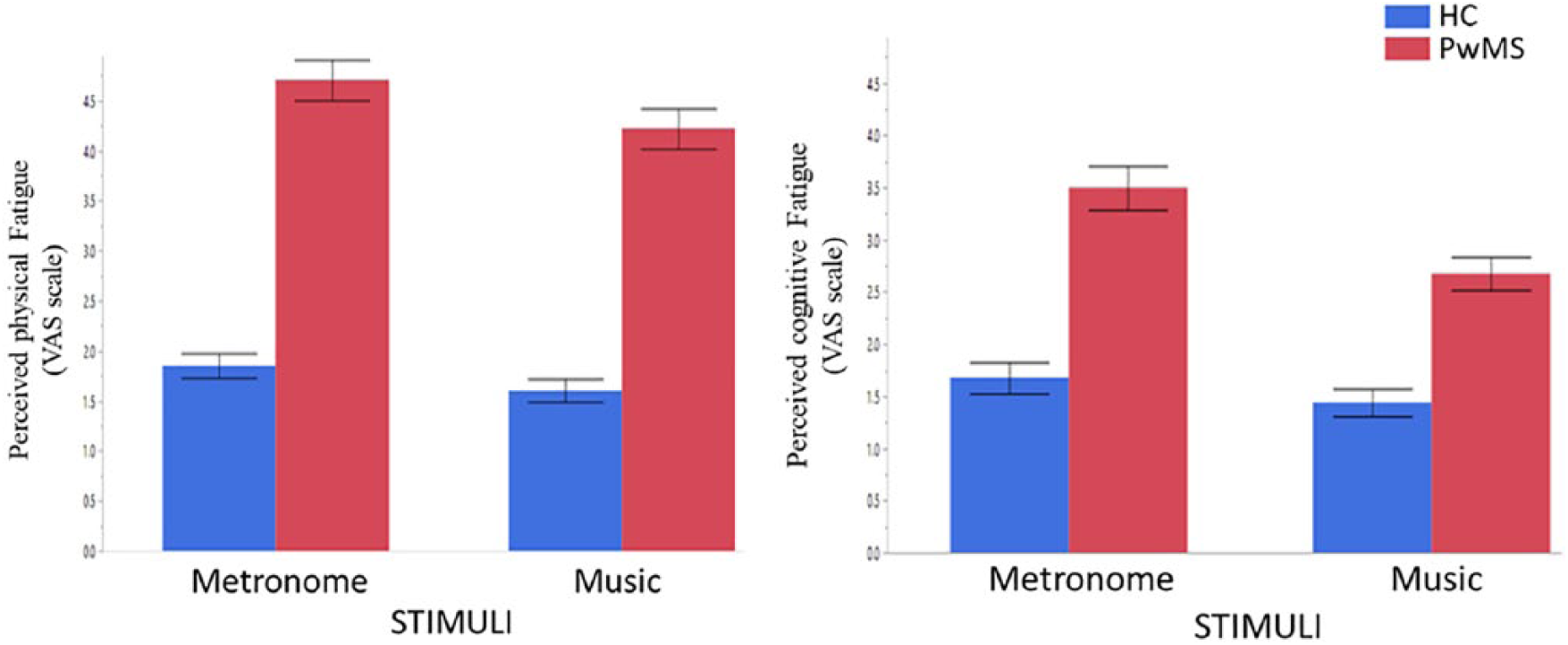
Perceived physical and cognitive fatigue when walking to metronome and music average across all tempi in persons with multiple sclerosis (PwMS) and healthy controls (HC). Mean standard errors are shown.
Motivation
Significant main effects were found for stimuli, F(1, 609) = 25.96, P < .0001, indicating a higher motivation when walking to music compared with metronomes.
Cadence
Significant main effects were found for stimuli, F(1, 1880) = 38.59, P < .0001, and tempi, F(5, 1880) = 225.00, P < .0001. Significant interactions were found for group ∗ tempi, F(5, 1880) = 8.08, P < .0001, and stimulus ∗ tempi, F(5, 1880) = 2.35, P = .04. The first post hoc test indicated that HC had significantly higher cadence at higher tempi compared with PwMS at the +6%, +8%, and +10% tempi (t = −6.23, −7.40, −8.47, P < .0001, respectively). The second post hoc tests indicated higher cadence with metronomes at the +8% and +10% tempi (t = 3.73, 3.60, P = .01, .02, respectively). Figure 2B presents a graphical summary of cadence.
Speed
Significant main effects were found for stimuli, F(1, 1883) = 32.14, P < .0001, and tempi, F(5, 1883) = 31.18, P < .0001. Significant interactions were found for group ∗ tempi, F(5, 1883) = 5.69, P < .0001, and stimulus ∗group, F(1, 1883) = 11.89, P = .0006. The first post hoc test indicated HC increased their speed at tempi +6%, +8%, and +10% (t = −6.03, −8.62, 9.92, P < .0001, respectively). The second post hoc test indicated that HC increased their speed when walking to metronomes as compared with the music (t = 7.62, P < .0001). While PwMS speed decreased in both stimuli (t = 2.64, P = .04) as compared with the HC.
Stride Length
Significant main effects were found for stimuli, F(1, 1886) = 19.22, P < .0001, and tempi, F(5, 1886) = 11.26, P < .0001, and time points, F(2, 1886)= 3.20, P = .04. Significant interactions were found for stimulus ∗group, F(1, 1886) = 11.57, P = .0007. The post hoc test indicated that HC had a shorter stride length when walking to music than metronome (t = 5.56, P < .0001).
Discussion
This observational study investigated auditory-motor coupling to music and metronome at different tempi by means of intentional synchronization and its effects on perceived physical and cognitive fatigue and gait patterns in PwMS and HCs. Additionally, we investigated if cognitive impairment posed as a factor in this analysis. We hypothesized that a proper auditory-motor coupling could influence PwMS to surpass the usual walking levels impinged by their motor or cognitive impairments (CI).
The results showed that all participants (HC and PwMS) were able to synchronize to both stimuli at all tempi, although the synchronization level was highest with metronomes. Although HC synchronized with higher values than PwMS. The use of a rollator by some participants posed no constraints on the synchronization ability. The reason for easier synchronization with metronome has been previously evidenced in healthy subjects. 37 It can be explained by the fact that the pulses of a metronome are stable and unambiguous, and therefore easier to predict, whereas music has more rhythmic complexities. 38
In healthy subjects, successful synchronization suggests that auditory-motor coupling engages a process termed entrainment. 39 To elaborate, the entrainment of the steps with the beats/pulses occur due to the dynamic oscillatory properties of the 2 entraining systems, and due to prediction-error minimization, whereas synchronization results as an outcome of entrainment.15,16,39 However, it has been reported that the prediction-error minimization process during entraining steps to music at various tempi differ in both PwMS and HC. 19 At tempi closer to the comfort tempo and +2% of the comfort tempo, passive cognitive processes occur in order to entrain and achieve synchronization. However, at tempi higher than +2% of comfort tempo, active cognitive processes are required in order to entrain and achieve synchronization. 19 The observed relative phase angle which showed steps ahead of the beat/pulse, is a typical sign of action prediction and anticipation mechanisms during auditory-motor coupling 15 ; see also other studies with healthy controls.35,40 It was present in all participants, indicating that the coupling occurred at all tempi with both stimuli. While PwMS with CI (n = 9) were able to couple and synchronize to tempi 0% to +6% of their baseline walking cadence. In this subgroup, the synchronization level was higher to music than to metronomes. This may suggest that synchronized walking to metronomes required more cognitive resources than walking to music. Although motor characteristics of CI patients did not significantly differ from the non-CI patients, future research with a larger sample size is required to confirm if confounding MS symptoms other than CI contribute toward the inability to synchronize past +6% of the preferred walking cadence.
As PwMS synchronized the most to tempi +2% to +8%, we suggest that these are the thresholds where PwMS engaged their cognitive and motor systems maximally in order to entrain (in other words, their maximal cognitive/motor capacity). The ability to maintain synchronization by auditory-motor coupling at thresholds higher than the normal walking ability in all our PwMS participants at their maximal thresholds, even the ones with a higher motor disability, is suggested to be a result of the neural mechanisms of entrainment. That is, the activation of the reticulospinal pathways supplement the spinocortical, 17 and possibly engagement of central pattern generators.
Perceived physical and cognitive fatigue were reported to be lower when walking to music, compared to walking to metronome in PwMS. PwMS were, as expected, more fatigued than HC as revealed by the VAS scale. This was also manifested during walking in the experimental conditions in all tempi and stimuli. HC did not show significant differences in perceived physical fatigue between stimuli. This is contrary to other studies in sport performance were music during training did reduce perceived fatigue. 26 An explanation for the difference in results could be that our walking tempi were not physically challenging for our HC population.
PwMS perceived lower physical fatigue levels while walking to music than to metronomes. This could be related to the dopaminergic-mesolimbic and reward circuits, 41 which are activated by music. This is also supported by a recent scoping review 42 suggesting that these are potential central nervous system pathways resulting in MS fatigue.
The lower cognitive perceived fatigue found in PwMS, including in persons with CI, when walking to music compared with metronomes can be explained by the cognitively enriching context of music and its appeal to the biosocial nature of human expression, compared with the repetitive continuous pulses heard in the metronomes. On a subjective level, many participants commented that walking to metronomes was not pleasant. Additionally, the reward system activation is also evidenced by our results, which showed higher perceived motivation when walking to music at all the tempi as compared with metronomes. 43 The higher effect of motivation with music can also be explained by a cognitive-motivational theory involving the experience of musical agency (the feeling of being in control). The theory assumes that successful sensorimotor prediction, in combination with physical effort and expression, engages emotional arousal of satisfaction and experience of pleasantness. 39
An increase of cadence was seen when walking to music and metronomes for all participants at all tempi, although in HC, the increase in cadence with the metronomes were more linear (the cadence increase matched the tempo goals). However, the speed and stride length decreased across tempi in all participants with both music and metronomes. The decrease of stride length observed could be a compensation of the gait, as a result of increase of cadence. The decrease of stride length is contrary to studies using rhythmic auditory stimulation on persons with Parkinson’s disease. 44 Yet, the previous studies did not compare different walking percentages as presented in this study, and therefore direct comparisons cannot be made.
Some methodological considerations apply. We acknowledge the limitation that the Expanded Disability Status Scale (EDSS) scores of the study participants is not reported in the current article because of an incomplete dataset due to the recruitment process. However, the motor and cognitive characteristics of the PwMS are reported to provide information on the behavioral characteristics of our participants. Our experimental track of 4.5 m × by 6 m is a limitation to our study on walking as it induced many turns. However, we believe that it did not have an impact on the results as all walking conditions were conducted in the same standardized track by all participants. However, in future studies, we do recommend the use of a larger space, where a person can walk and take a semicircular wide turns (and avoid 180° sharp turns) or walk in a figure of eight as seen in experiments with patients with Parkinson’s disease. 45 Another limitation is the music selection. Although songs were grouped by genre and participants could choose one preferred genre to complete the entire experiment, different songs were used for each tempi. While in the case of the metronome, the same stimulus was continuously used. As such, this might explain the results of the lower level of synchronization with the music compared with the metronome.
Clinical Indication and Future Directions
The study results are valuable to indicate the potential for coupling walking to auditory stimuli to be applied in rehabilitation for PwMS with low and high motor disabilities, as well as having cognitive impairments. The higher tempi led to an increase in cadence above usual thresholds but at the cost of stride length. Future research should investigate whether stride length can be maintained when walking at higher tempi, in the presence of instruction. This knowledge is important for guiding rehabilitation interventions.
Conclusion
The present study demonstrates that healthy controls and PwMS with mild and moderate motor impairments were able to walk at a range of higher tempi than their preferred walking cadence by synchronizing their steps to music and to higher tempi to metronomes. Furthermore, walking to music was perceived less fatiguing than walking to metronomes at all tempi in PwMS. Synchronization was also present in cognitive impaired persons with MS. The results imply that coupling walking to music at an individualized tempo may be used for functional walking training for PwMS.
Supplemental Material
Supplemental_Table – Supplemental material for Walking to Music and Metronome at Various Tempi in Persons With Multiple Sclerosis: A Basis for Rehabilitation
Supplemental material, Supplemental_Table for Walking to Music and Metronome at Various Tempi in Persons With Multiple Sclerosis: A Basis for Rehabilitation by Lousin Moumdjian, Bart Moens, Pieter-Jan Maes, Johan Van Nieuwenhoven, Bart Van Wijmeersch, Marc Leman and Peter Feys in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We acknowledge the financial support of Ruben Donné (Sailing for MS project), the statistical support provided by Robin Bruyndonckx, and the assistance in data collection of master students Juul Janssen and Iris Willems. We also want to thank Joren Six for proofreading. The authors acknowledge the Methusalem project (awarded by the Flemish Government) at UGent and the UHasselt BOF grant for funding this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the financial support of Ruben Donné (Sailing for MS project). The authors acknowledge the Methusalem project (awarded by the Flemish Government) at UGent and the UHasselt BOF grant for funding this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.