
Abstract
Background. Physical rehabilitation programs can lead to improvements in mobility in people with multiple sclerosis (PwMS). Objective. To identify which rehabilitation program elements are employed in real life and how they might affect mobility improvement in PwMS. Methods. Participants were divided into improved and nonimproved mobility groups based on changes observed in the Multiple Sclerosis Walking Scale–12 following multimodal physical rehabilitation programs. Analyses were performed at group and subgroup (mild and moderate-severe disability) levels. Rehabilitation program elements included setting, number of weeks, number of sessions, total duration, therapy format (individual, group, autonomous), therapy goals, and therapeutic approaches. Results. The study comprised 279 PwMS from 17 European centers. PwMS in the improved group received more sessions of individual therapy in both subgroups. In the mildly disabled group, 60.9% of the improved received resistance training, whereas, 68.5% of the nonimproved received self-stretching. In the moderately-severely disabled group, 31.4% of the improved, received aerobic training, while 50.4% of the nonimproved received passive mobilization/stretching. Conclusions. We believe that our findings are an important step in opening the black-box of physical rehabilitation, imparting guidance, and assisting future research in defining characteristics of effective physical rehabilitation.
Introduction
Although numerous trials have established the benefits of immunomodulatory drugs in decelerating the inflammatory-related progression of multiple sclerosis (MS), 1 the disease remains incurable with ambulation difficulties worsening with disease progression. Consequently, physical rehabilitation remains a key factor in improving (or maintaining) mobility in people with MS (PwMS).
Rehabilitation programs comprise various therapeutic approaches (eg, resistance training, balance training), intensity (eg, how hard the body is taxed), volume (eg, frequency, number, and duration of sessions), and format (eg, individual or group based, home or center based). It has been reported that the content and approach of physical therapy for PwMS differs throughout certain European countries. 2 Nevertheless, very few studies have hitherto investigated which elements are currently being employed during rehabilitation sessions and which are of sufficient importance in improving mobility in PwMS. In terms of therapeutic approaches, several systematic reviews have examined the effect of physical rehabilitation programs on ambulatory outcomes in PwMS.3-7 Although there is strong evidence showing that exercise therapy improves mobility related activities,3,4 others have demonstrated only a limited beneficial impact.5,8
Recently, Khan and Amatya 9 published a systematic review of systematic reviews examining rehabilitation in PwMS reporting strong evidence for physical rehabilitation programs and moderate evidence for a range of rehabilitative treatments and approaches available for PwMS. Nevertheless, there is still a lack of evidence for most modalities and limited comparative knowledge of their efficacy across the disability spectrum due to the use of different outcome measures and limited standardized reporting of the elements in rehabilitation programs (eg, combination of modalities and delivery modus). As such, it is difficult to provide sufficiently detailed guidelines to clinicians and patients. Additional information is needed in order to identify core elements in physical rehabilitation programs, aimed at improving mobility in PwMS.
In our previous publication of 290 PwMS from 17 European centers, we examined the responsiveness and clinically meaningful improvement of 5 walking measures. 10 The participating centers collaborated with the European Rehabilitation within the Multiple Sclerosis (RIMS) network. Our main finding was that long walking tests and the self-reported Multiple Sclerosis Walking Scale–12 (MSWS-12) could detect clinically meaningful improvement after physical rehabilitation. 10 The aim of the present study (a secondary analysis) was to assess real-life physical rehabilitation programs across Europe and explore the elements (format, volume, therapy goals, and approaches) that could positively affect mobility in PwMS. Our hypothesis was that active treatment approaches (eg, muscle strengthening, aerobic training) would greatly affect mobility compared with passive approaches (eg, stretching).
Methods
Participants
A convenience sample of 290 PwMS were recruited from 17 centers within the RIMS network. A full description of participating centers was presented in our previous publication. 10 This study was approved by the Ethical Committee of the Hasselt University, Belgium and local ethics committees from each participating center. Inclusion criteria comprised a definite diagnosis of MS 11 and the Expanded Disability Status Scale (EDSS) 12 score of ≥ 2 and ≤6.5 as determined by neurologists. All patients participated in a physical rehabilitation program for 3 to 12 weeks. Inclusion criteria included a minimum of 10 sessions and a maximum duration of 3 months. Subjects were excluded if afflicted with other medical conditions interfering with walking. All subjects provided written informed consent.
Rehabilitation Program Format and Volume
The physical rehabilitation programs varied from center to center and included guided or supervised sessions by physiotherapists and/or sport/fitness instructors. We acknowledge that there are differences in the educational level of professionals providing physical therapy in MS across Europe. 13 Each participating site supplied information regarding their program, that is, setting; number of weeks; number of sessions; total duration and therapy format (individual, group, or autonomous). Settings were neurorehabilitation centers with or without an overnight stay, hospitals with or without an overnight stay, private physical therapy practices, community centers, fitness centers, research facilities, and patient residences. These were dichotomized as in- and outpatient rehabilitation settings. A maximum of 2 settings were indicated when settings were combined. Individual therapy was defined as a 1:1 ratio between therapist and patient. The duration of each session lasted 40 to 50 minutes. Number of sessions and total duration were recorded for each therapy format.
Therapy Goals and Therapeutic Approaches
Classification of therapy goals and therapeutic approaches were based on the study by Rasova et al.14,15 Therapists were required to describe for each patient one primary goal of the physical rehabilitation program: “improving balance”, “improving walking capacity,” “maintenance of balance and walking,” and “others, unrelated to balance and walking.” To identify the main therapeutic approaches employed during the intervention program, the therapist selected a maximum of 5 items (out of 21) from a list of approaches (eg, resistance training with equipment, balance training, gait training, passive mobilisation, aerobic training).
Walking Measures
Clinical walking tests used at entry and discharge of the rehabilitation program included
Two- and 6-minute walk test (2mWT, 6mWT). The participants were instructed to complete the test “at their fastest speed” and cover as much distance as possible by walking up and down a 30-m hallway, using their own walking aid. The 2mWT and 6mWT have been validated and used extensively in PwMS. 16
The Multiple Sclerosis Walking Scale–12 (MSWS-12) is a valid patient-reported questionnaire rating walking ability in PwMS.17,18 Each item is scored on a scale of 1 to 5; the higher the score, the more perceived walking difficulties. A total score is generated and converted to a scale of 0 to 100 with negative change scores indicating improvement.
Timed 25-foot walk (T25FW) was performed at a normal and fastest walking speed. Participants were instructed to walk at their own comfortable pace for the normal trial and as quickly as possible for the fast trial. The T25FW has been validated as 1 of the 3 components of the Multiple Sclerosis Functional Composite. 19
Statistical Analysis
The sample group was divided into 2 groups: improved and nonimproved walkers. Allocation was determined according to the MSWS-12’s minimally important change (MIC) scores as presented in our previous publication. 10 The MSWS-12 was selected due to its acceptance in clinical trials investigating rehabilitation and pharmacological interventions in the MS population. Additionally, its validity has been confirmed in community-residing and hospital outpatient samples of PwMS.17,18
The MIC cutoff point for the total group was −11.35, in the mildly disabled subgroup −10.7, and in the moderately-severely disabled −11.85. PwMS with change scores equal or above the MIC were assigned to the improved group and those scoring below the MIC were assigned to the nonimproved group. Furthermore, the participants were categorized as either “mildly” (EDSS ≤4) or “moderately-severely” disabled (EDSS >4), according to their disability level. Classification of disability subgroups corresponded with our previous publications on walking measures in PwMS.10,20 All data followed a normal distribution according to the Kolmogorov-Smirnov test. Box plots determined outliers for each outcome.
Descriptive statistics were used for demographic, clinical characteristics, rehabilitation elements and mobility measures. Differences between the improved and nonimproved walkers were examined by the chi-square test for MS type, gender, setting, therapy goals, and by analysis of variance tests (ANOVA) for age, disease duration, EDSS, mobility measures, volume of therapy, and therapeutic approaches.
Binary logistic regression analyses, with a forward method, examined the relationship between the improved/nonimproved status (dependent variable) and the rehabilitation elements (setting, therapy goal, volume of therapy and therapeutic approaches) (independent variables). The regression analysis was performed separately according to disability subgroups. For all models, the assumptions underlying regression were tested by inspecting the distribution of the error term. All analyses were carried out using the SPSS software (version 25.0 for Windows; IBM Corp, Armonk, NY, USA). Reported P values were 2-tailed. The level of significance was set at P < .05.
Results
Out of the total 290 PwMS, 11 participants were missing data, therefore, only a total of 279 PwMS were included in the final analysis: 131 were assigned to the improved; 148 to the nonimproved group. No significant differences between groups were observed for age, gender distribution, type of MS, disease duration and mean EDSS score. Descriptive characteristics of the sample according to group allocation and disability level are provided in Table 1.
Descriptive Characteristics According to Study Groups and Disability Level.
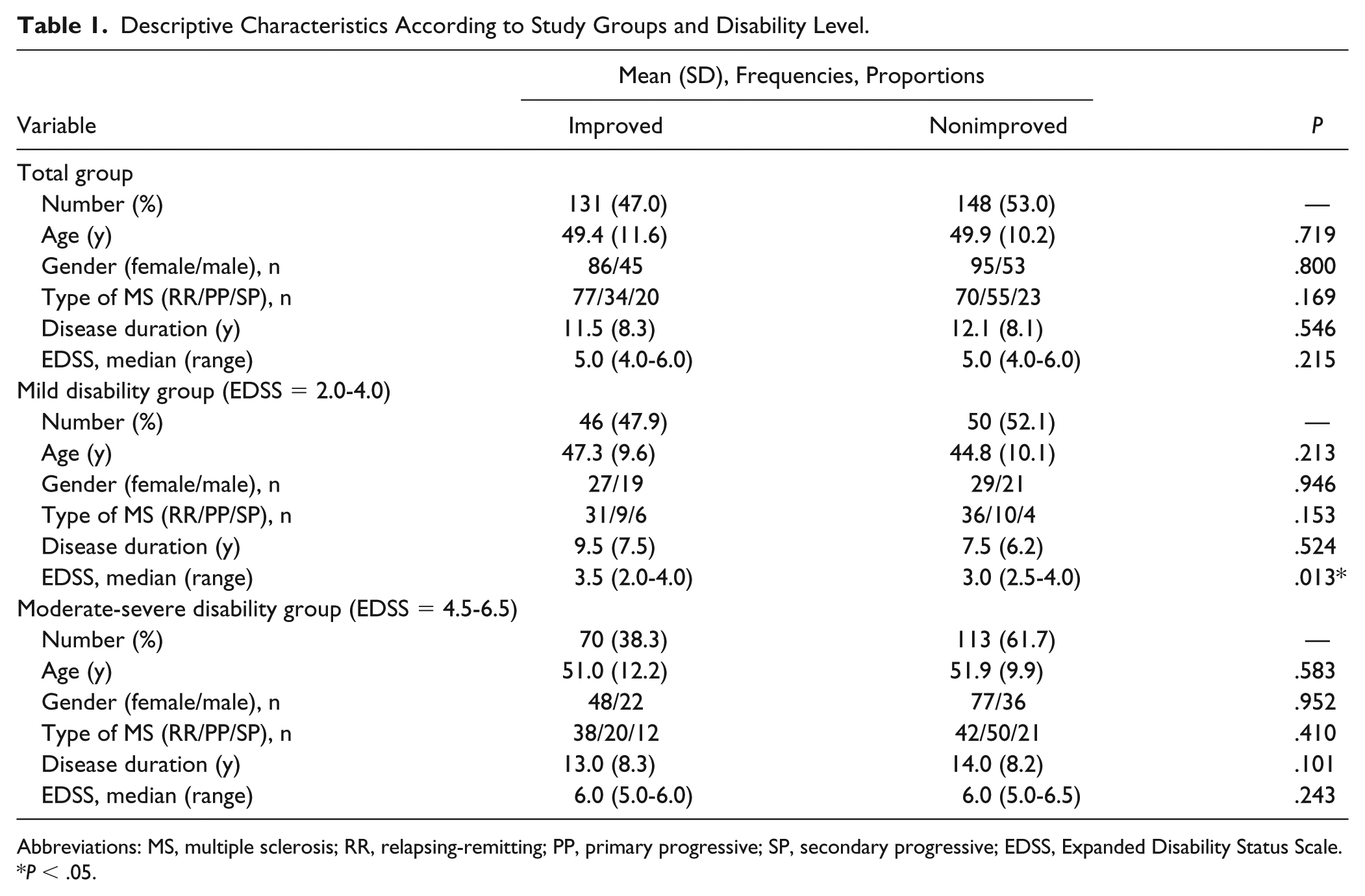
Abbreviations: MS, multiple sclerosis; RR, relapsing-remitting; PP, primary progressive; SP, secondary progressive; EDSS, Expanded Disability Status Scale.
P < .05.
In terms of disability subgroups, 46 patients (47.9%) in the mildly disabled and 70 (38.3%) in the moderately-severely disabled, improved in mobility. No differences were detected between the improved and non-improved subgroups as to demographic and clinical characteristics on the moderately-severely disability level. A similar observation was recorded in the mildly disabled group, with the exception of the mean EDSS score, which was higher in those who improved compared to those who did not, 3.3 (SD = 0.8) versus 2.8 (SD = 1.0), P = .013. Descriptive and clinical characteristics according to group allocation and disability level are provided in Table 1.
Table 2 and Figure 1 present the mobility outcome measures according to group allocation and disability level. For the total sample, significant differences were found in favor of the improved compared with the nonimproved group for the 2mWT and the 6mWT. No differences between groups were found for the T25FW. According to the 2mWT and 6mWT, PwMS improved their walking distance by approximately twice the length of the nonimproved PwMS. Although, individuals in the nonimproved group showed improvements in the long-distance walking tests, it was below the MIC cutoff score.
Mobility Outcome Measures According to Study Groups and Disability Level.
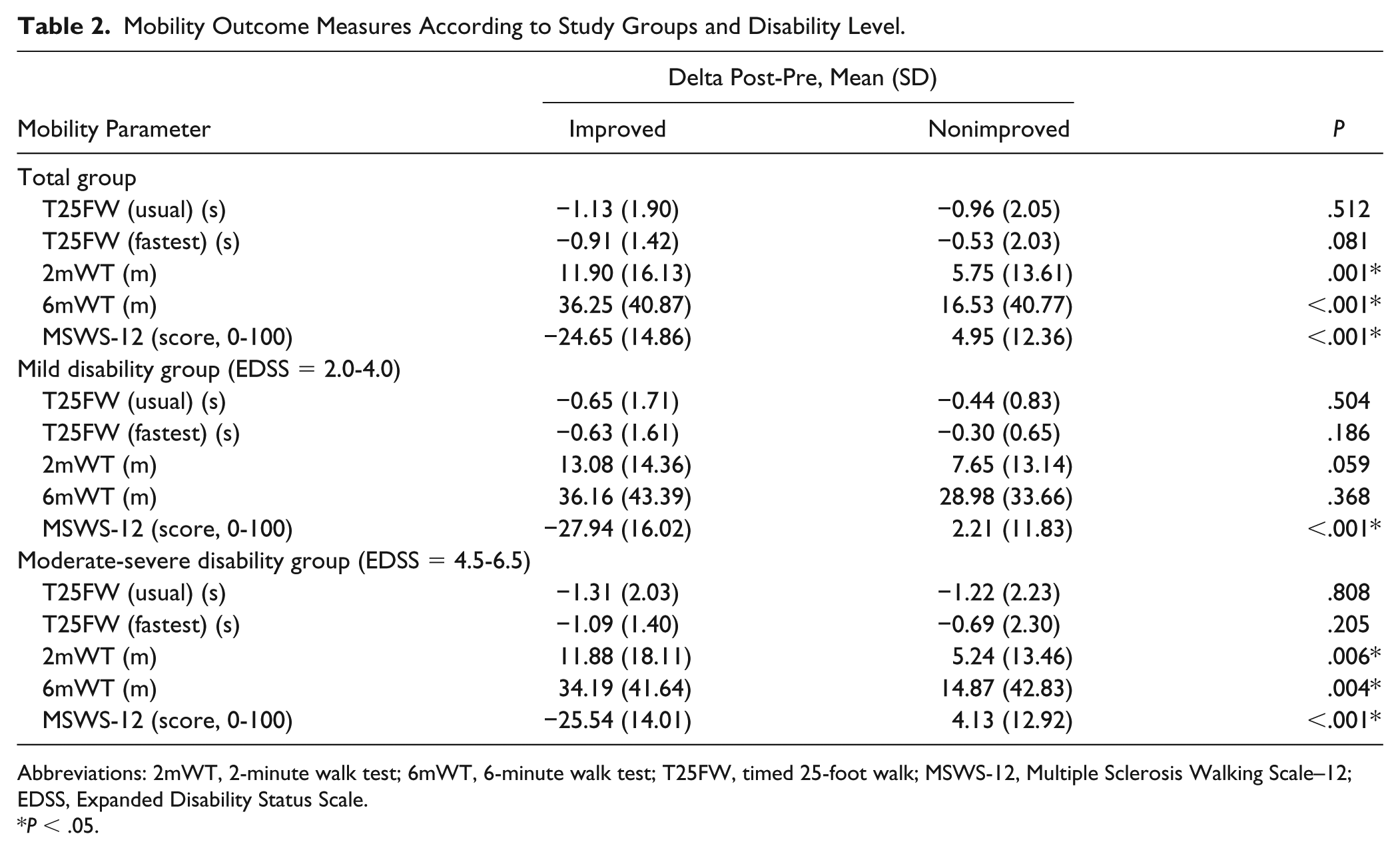
Abbreviations: 2mWT, 2-minute walk test; 6mWT, 6-minute walk test; T25FW, timed 25-foot walk; MSWS-12, Multiple Sclerosis Walking Scale–12; EDSS, Expanded Disability Status Scale.
P < .05.
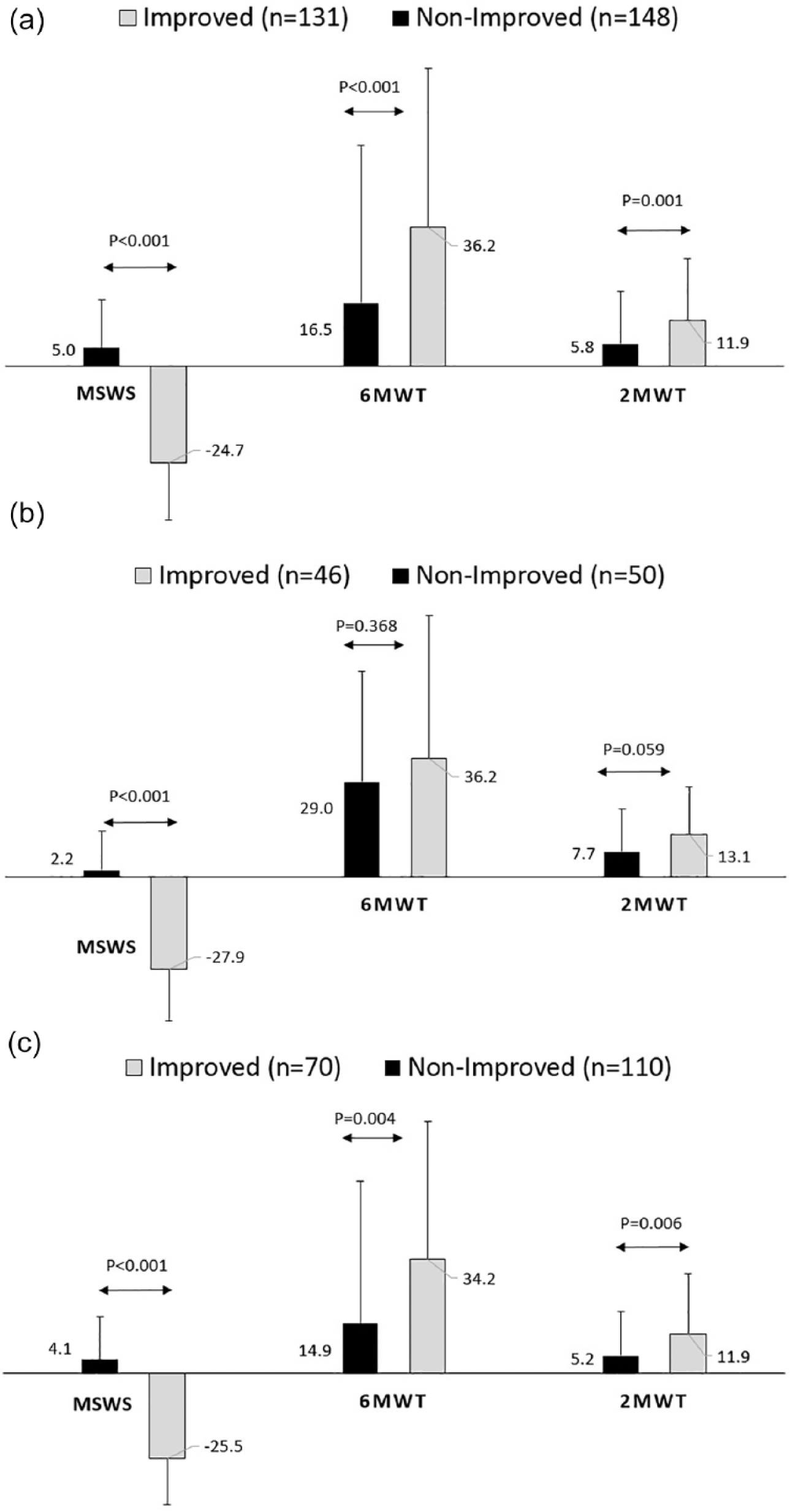
Mobility outcome measures according to group allocation of the total group (a), the mildly disabled group (b) and the moderately-severely disabled group (c).
No differences were found between the improved and nonimproved groups in the T25FW, 2mWT and 6mWT mobility tests for people with mild MS. In contrast, significant differences in favor of the improved group were found for the long-distance walking tests in moderately severe PwMS. As for the MSWS-12 questionnaire, participants in the improved group (both disability levels) presented with a ~26% improvement at discharge. Conversely, people with mild or moderately severe MS, categorized as nonimproved, reported more mobility difficulties (according to the MSWS-12) following the physical rehabilitation program.
The majority (72%) of the MS sample received rehabilitation in an outpatient setting. No significant differences in the amount of therapy was found between the mildly and moderately-severely disabled subgroups. PwMS in the improved group received a greater amount of individual therapy compared with the nonimproved in both disability subgroups. People with mild MS who had improved, received approximately twice the number of individual therapy sessions and double the duration of therapy hours compared with those who had not improved. Participants in the improved group, classified as moderately-severely disabled, received approximately 25% more individual therapy compared to those in the nonimproved group. No differences were observed between the improved and nonimproved groups in program settings and amount of autonomous therapy, regardless of disability level. Table 3 presents the rehabilitation program elements according to group allocation and disability level.
Rehabilitation Program Format and Volume According to Study Groups and Disability Level.
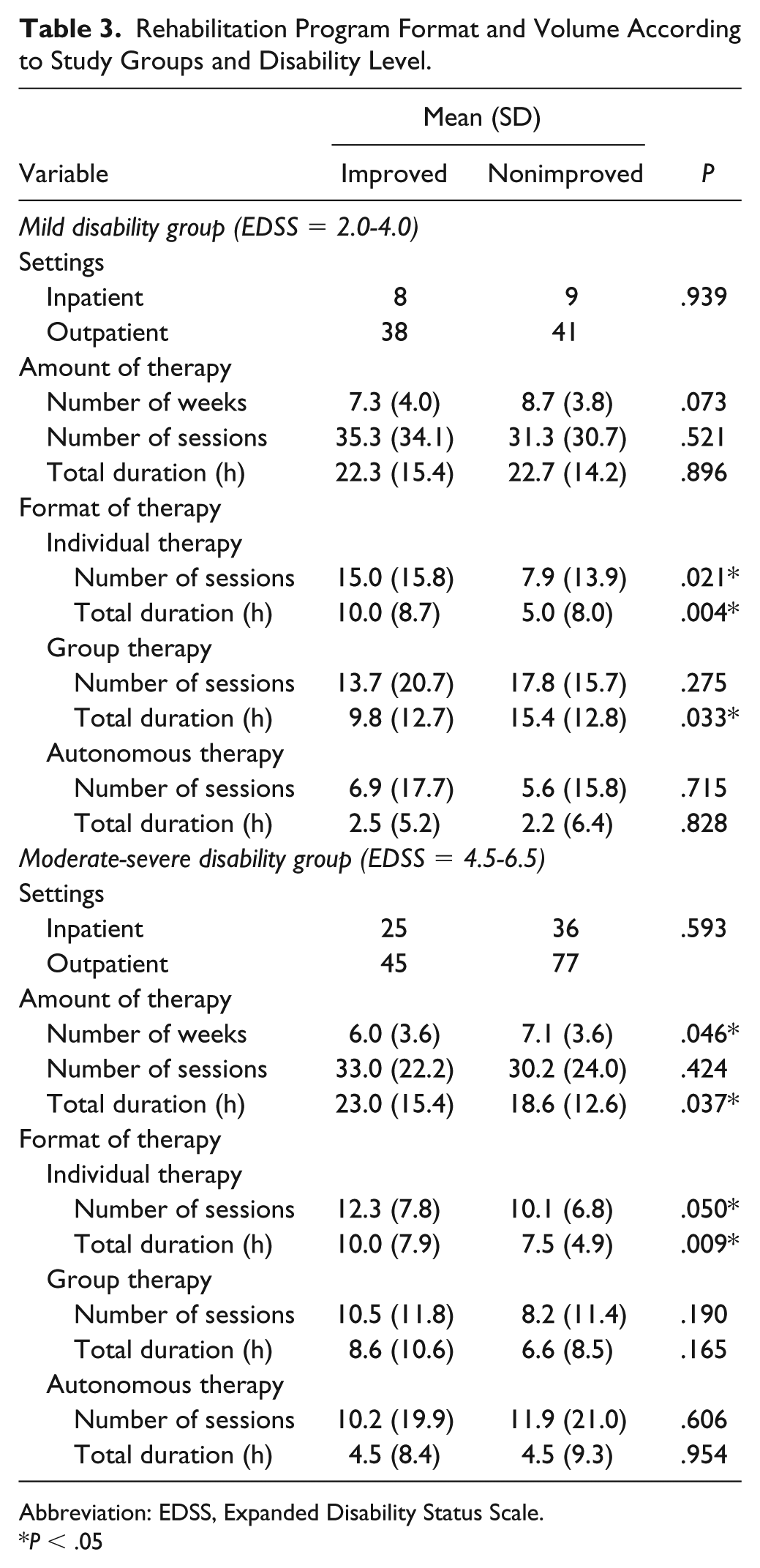
Abbreviation: EDSS, Expanded Disability Status Scale.
P < .05
Approximately 42% of the therapists, selected “improvement in walking capacity” as the primary goal for participants who had improved, irrespective of disability level. According to the chi-square tests, there were significant differences in therapy goals between the improved and nonimproved groups in the mildly disabled subgroup; χ2(3) = 18.537, P < .001 and in the moderately-severely disabled subgroup; χ2(3) = 16.538, P = .001. Figure 2 illustrates therapy goal distribution according to group allocation and disability level.
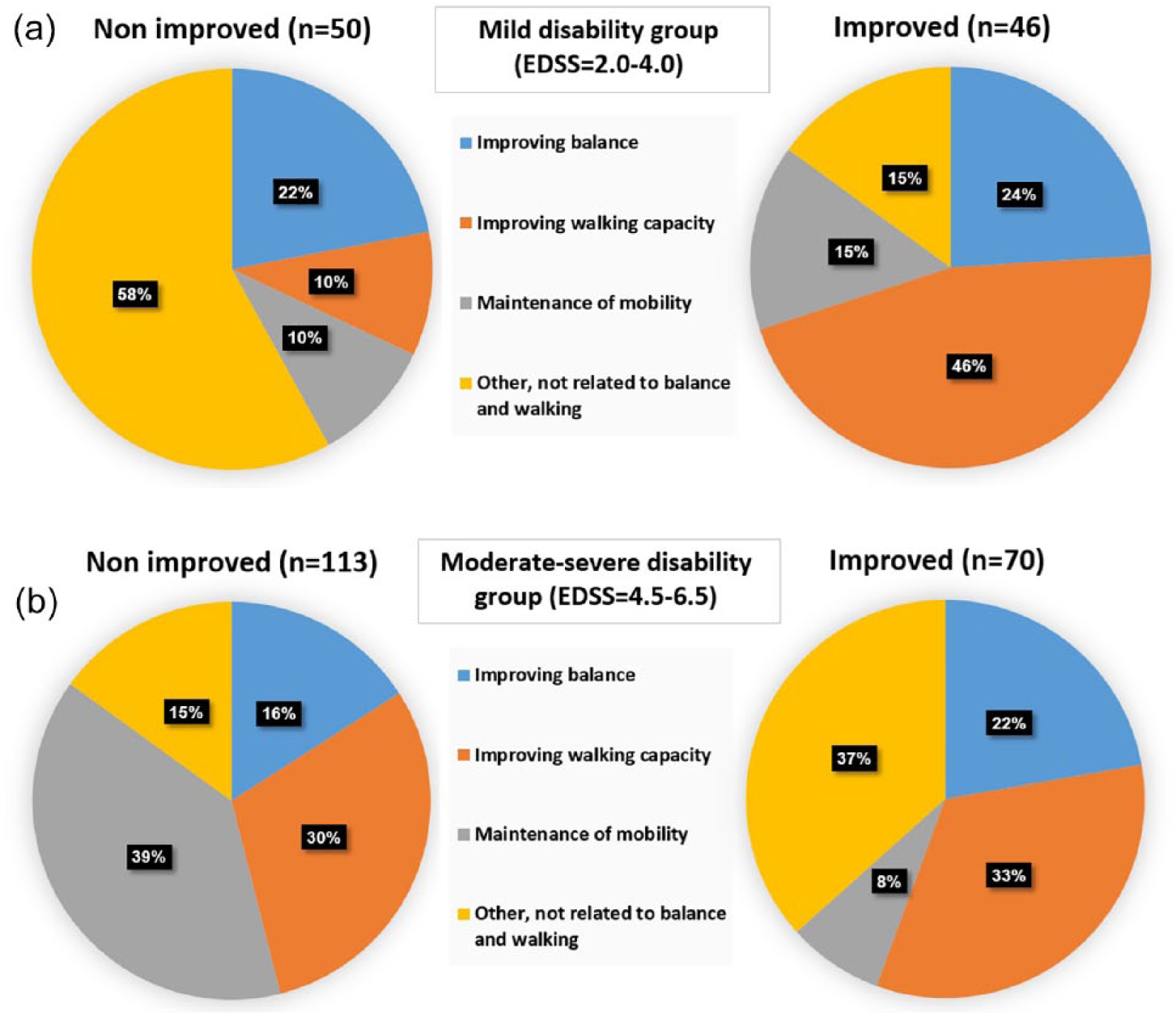
Therapy goal distribution according to group allocation in the mildly disabled group (a) and the moderately-severely disabled group (b).
The therapist was instructed to select a maximum of 5 items (out of 21) from a list of therapeutic approaches. Significant differences were found in the mildly disabled group for 2 items; 60.9% of the participants who had improved, had received resistance training compared with 26.0% who had not improved; whereas, 68.5% of those who had not improved, had received self-stretching compared with 39.1% who had improved. As for the moderately-severely disabled group, 31.4% who had improved had received aerobic training compared with 14.2% who had not improved. In patients who had not improved, 50.4% received passive mobilization/stretching compared with 31.4% who had improved, 38.9% received resistance training compared with 21.4% who had improved. Table 4 presents the therapy approaches according to group allocation and disability level.
Intervention Approaches According to Study Groups and Disability Level.
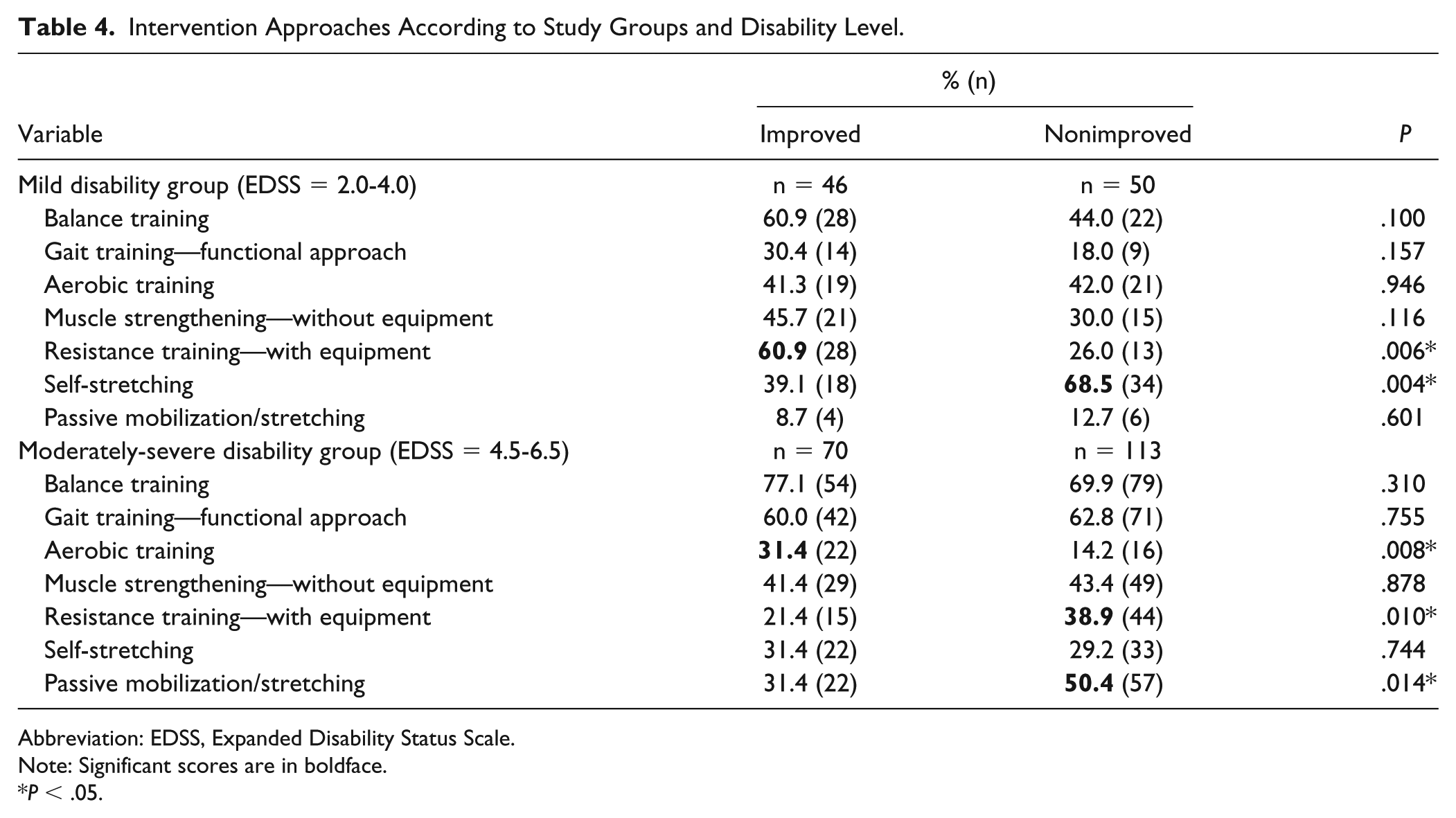
Abbreviation: EDSS, Expanded Disability Status Scale.
Note: Significant scores are in boldface.
P < .05.
Table 5 presents the results of the binary regression analysis in the mildly and moderately-severely disabled subgroups. A significant relationship was found between group allocation with resistance training and self-stretching therapeutic approaches in the mildly disabled subgroup. These variables explained 21.8% of the variance related to improved/nonimproved group allocation. As for the moderately-severely disabled subgroup, passive mobilization/stretching, and individual therapy volume explained 14.3% of the variance related to improved/nonimproved status.
Binary Logistic Regression Analysis in the Mild and Moderate Disability Subgroups.
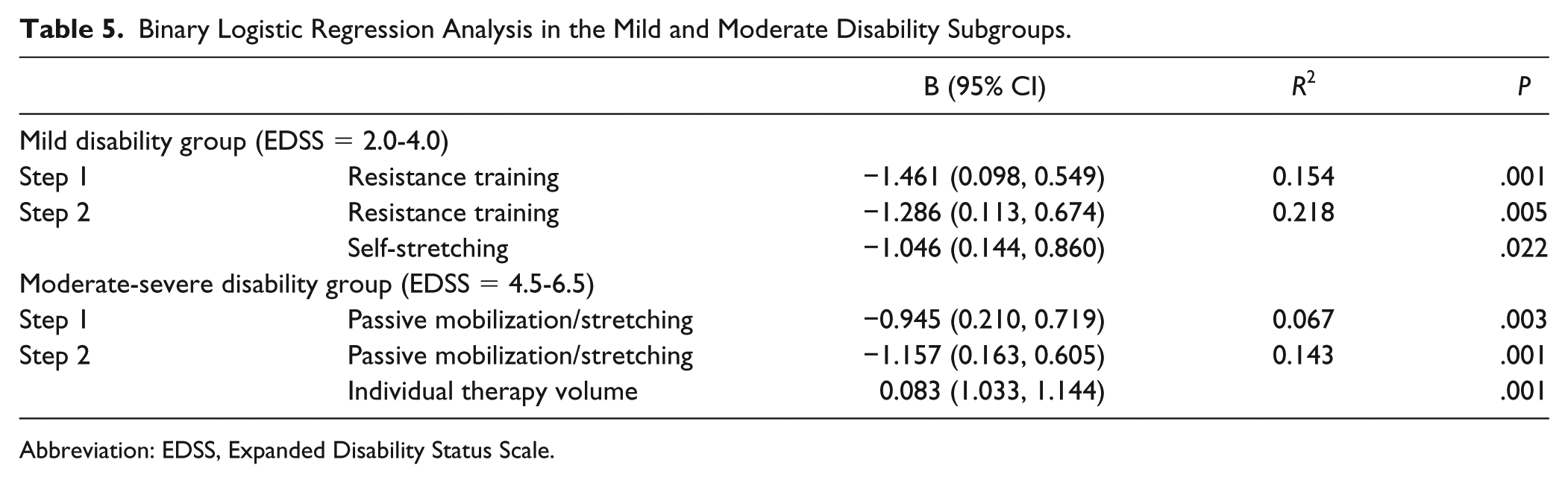
Abbreviation: EDSS, Expanded Disability Status Scale.
Discussion
We report herein on a secondary analyses of a RIMS multicenter study primarily aimed at investigating the responsiveness of outcome measures in rehabilitation. Our aim was to assess physical active rehabilitation programs and explore the elements of these programs which positively affect mobility in PwMS. On conclusion of the rehabilitation program, 47% of PwMS participants demonstrated a clinical meaningful improvement in the MSWS-12. A novel feature of the current study was that while most of the previous studies investigating physical rehabilitation in PwMS had observed improvements in mobility according to the standard significance level, we defined mobility improvements according to meaningful clinical values. 10
To the best of our knowledge, this is the first multicenter study encompassing a wide range of physical rehabilitation programs applied in the MS population, using identical outcome measures and standardized reporting terminology. We combined the data obtained from 17 MS rehabilitation centers in 9 countries. Each center had constructed their program according to the needs of their local MS population, rehabilitation facilities, and the regulations/guidelines of its health care providers. Mobility assessments were performed in a standardized manner at all centers according to a detailed instruction booklet provided by the project steering group. Although the diverse rehabilitation programs and the possibility that therapists employed multiple approaches per patient may affect the data and can be considered a limitation, we feel that it might strengthen the ecological validity of our findings. Furthermore, in the current study we did not want to change the existing physical rehabilitation programs. The format was to observe and record the current status of physical rehabilitation across Europe in PwMS,14,15 without formulating up a well-designed (controlling confounders), scientifically strong robust study. We believe that our findings are an important step in opening the black-box of physical rehabilitation, imparting guidance and assisting future research in defining characteristics of effective physical rehabilitation.
There is a wide-ranging consensus as to the amount of physical rehabilitation needed for PwMS: More practice is probably better, but “how much more” remains an unanswered question. We found that the volume of individual therapy was significantly higher in improved versus non-improved patients, consistent in both disability groups, suggesting that the volume of rehabilitation is a key factor for a successful rehabilitation in PwMS. This statement is in accordance with a Cochrane review examining physical rehabilitation approaches in patients recovering function and mobility following stroke. 21 Nevertheless, our findings partially contrast with the systematic review of Snook and Motl, 4 which reported on the effect of exercise on mobility performance in PwMS. They found no differences in effect size according to the number of sessions per week and minutes per session. 4 Unfortunately, the authors did not calculate the total amount of exercise therapy and consequently, a direct comparison with our findings is not possible.
Findings related to the therapy goals were somewhat confusing. The goal “Other” was the main choice in the mildly disabled participants who did not improve, however, this was also the main goal of choice in the moderate-severe disabled patients who improved. According to the study protocol, the therapists were asked to record only the primary goal, although the training sessions may have included additional secondary goals (reflecting real life practice), such as improving walking capacity and/or balance. For instance, in cases where improving aerobic capacity was the main goal, the therapist chose the option “Other.” However, this choice does not necessarily mean that secondary objectives such as improving walking and/or balance, were not included in the session. We therefore, advise to consider this finding with caution.
Currently, there is no consensus as to whether group or individual therapy (or a combination of both) sessions are preferred when seeking to improve mobility functions in PwMS.22,23 Although, group-based physical rehabilitation sessions may be more efficient by potentially allowing more visits per patient than individual physical therapy sessions, there are still several potential disadvantages to this approach. One disadvantage is the lack of flexibility in tailoring interventions according to the varied functional levels of individual MS patients. Moreover, it is more difficult to match the patient’s cognitive and psychological function in group therapy compared with individual therapy treatment goals. On the other hand, advantages of group therapy include social interaction and peer support between participants. Our findings suggest that individual therapy should be preferred over group or autonomous therapy in order to improve mobility in the MS population. Nevertheless, future research is warranted with a direct comparison of an identical rehabilitation program provided in individual versus group therapy settings.
In the mildly disabled group, a significant higher proportion of patients received resistance training in the improved group versus the nonimproved. The opposite result was seen in the moderately-severely disabled group (Table 4). A positive contribution of resistance training on mobility has been well-documented in the MS population.24-26 The mechanisms involved may include increases in the neural drive, 27 a larger muscle fiber size 28 and enhanced neuromuscular adaptations. 29 For patients with a moderate-severe disability, aerobic training, rather than resistance training, was associated with clinical meaningful mobility improvements. This finding supports the results of previous studies investigating the effect of aerobic exercise in PwMS with severe mobility deficits.30,31
Self-stretching and passive mobilization/stretching were more commonly used as a treatment approach in PwMS who did not improve. Passive movements, joint mobilization and stretching techniques generally produced only modest beneficial effects or even detrimental effects on performance in athletes. 32 Our results also indicate that these therapy modalities appear to be less beneficial compared to more physically demanding modalities aiming to improve mobility in PwMS. The fact that stretching did not emerge as most effective, may be related to the patient sample composition, with limited patients demonstrating a need for stretching.
Group classification was based on the MSWS-12, the most widely used patient-reported measure of perceived limitation in walking due to MS. This decision was reached due to evidence from multiple studies supporting its robust measurement performance.10,17,18,20,33-35 Furthermore, the MSWS-12 includes running, stair climbing, balance, concentration and effort needed to walk, therefore, measuring broader aspects of mobility. Moreover, Pilutti et al 32 have shown that the MSWS-12 scores correlate with the T25FW, 6mWT, and gait kinematics in PwMS. Some argue that this scale might not be an ideal choice for measuring walking impairment in mildly disabled PwMS or those who walk without a device. 34 Nevertheless, Langeskov-Christensen et al 35 recently reported that the MSWS-12 captures impairments more gradually than the 2MWT and 6MWT in people with mild MS, thus, suggesting that the MSWS-12 is acceptable when assessing walking in PwMS with a low disability status.
Our study has some limitations. First, mobility was evaluated only by clinical walking tests and a patient-reported questionnaire. Utilizing instrumented gait devices that provide definite gait characteristics, might have expanded our knowledge. However, only a few of the centers participating in this study possessed these tools. 36 Second, we did not explore the impact of different combinations of treatment modalities on an individual level. An alternative could have been to apply a standardized recording form of rehabilitation taxonomy which requires time recordings of different components per session. 37 More detailed data would have strengthened our findings, however, recording such detailed information after each session was not feasible for the majority of involved therapists. Finally, the aim was not to improve mobility in all patients. As such, applied intervention modalities may have also suited other therapy goals.
Conclusion
This report presents data of the core elements of physical rehabilitation programs associated with improving mobility in PwMS from 17 MS centers across Europe. Suggested elements to improve mobility include the volume of individual therapy sessions, resistance, and aerobic therapeutic approaches and placing less emphasis on passive therapeutic techniques. Future studies should investigate these treatments.
Footnotes
Acknowledgements
Coordination of this study was partially funded via an unrestricted educational grant from Novartis Pharma AG to the European RIMS network, acknowledged for facilitating inter-European consultation and testing. The staff of each participating site and participating subjects are acknowledged for their cooperation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded via an unrestricted educational grant from Novartis Pharma AG to RIMS.