
Abstract
Background. Energy cost of walking (Cw) is elevated in persons with multiple sclerosis (MS), perhaps because of gait impairment, and may impact daily activity and fatigue. Objective. The authors examined for associations between Cw, spatiotemporal gait parameters, daily activity, and perceived fatigue in persons with mild MS. Methods. Forty-four participants completed 4 trials of walking on a GAITRite mat and one 6-minute trial of walking on a treadmill at a constant, controlled speed of 54 m min−1 while expired gases were analyzed for oxygen consumption. Participants also completed the Fatigue Severity Scale (FSS) and wore a waist-mounted accelerometer for 7 days. Results. C w was significantly and inversely associated with gait speed (r = −.25) and stride length (r = −.32) and positively associated with double limb support (r = .27). C w was significantly and inversely associated with daily accelerometer activity counts (r = −.35) and positively associated with FSS scores (ρ = .31). Conclusion. The results support the development and application of rehabilitation strategies to address impaired gait parameters as an approach to improve Cw, daily activities, and fatigue.
Introduction
The energy cost of walking (Cw), defined as the amount of oxygen consumed per kilogram of body weight per unit distance traveled (ie, mL kg−1 m−1), 1 is higher in persons with multiple sclerosis (MS) who have mild disability than controls. 2 Maximal oxygen consumption, by comparison, is reduced in persons with MS who have mild disability. 3 This indicates that persons with MS who have mild disability would expend more energy and use a greater percentage of maximal metabolic capacity when completing everyday activities of daily living. Such effects seemingly would reduce the level of daily activity and increase the sense of fatigue and activity-related fatigability.
The Cw has been linearly associated with self-reported disability in mobility in persons with mild MS, 2 and this would suggest that parameters of impaired gait are associated with Cw in this population. 4 There is evidence that both gait speed and stride length are reduced and double limb support is prolonged in persons with mild MS compared with controls. 5 To date, researchers have not examined the association between those gait parameters and Cw in persons with mild MS, but there is evidence of an association between pathological gait and energy costs of walking in some neurologic and orthopedic disorders. 1 Such an examination might identify targets of gait rehabilitation for reducing the Cw and its association with daily activity and fatigue.
We examined the hypotheses that (a) gait speed, stride length, and time spent in double support would be associated with Cw and (b) Cw would be associated with daily activity and perceived fatigue in persons with mild MS.
Methods
Participants
The sample was recruited through direct contact with support groups of a Midwestern chapter of the National Multiple Sclerosis Society that were located within an approximately 90-minute drive of our facility. The inclusion criteria involved (a) clinically definite diagnosis of MS; (b) relapse free during the past 30 days before testing; (c) being ambulatory without an assistive device including cane, crutch, or walker; (d) being 18 to 64 years of age; (e) having the visual ability necessary to read 14-point font; (f) being willing and able to wear the accelerometer and oxygen analysis system while walking on a treadmill; and (g) absence of risk factors for undertaking exercise testing based on the Physical Activity Readiness Questionnaire (PAR-Q). 6 We screened 69 persons with MS and enrolled 44 of the 69 persons who underwent screening (64%).
Primary Measurements
Energy cost
Oxygen consumption (
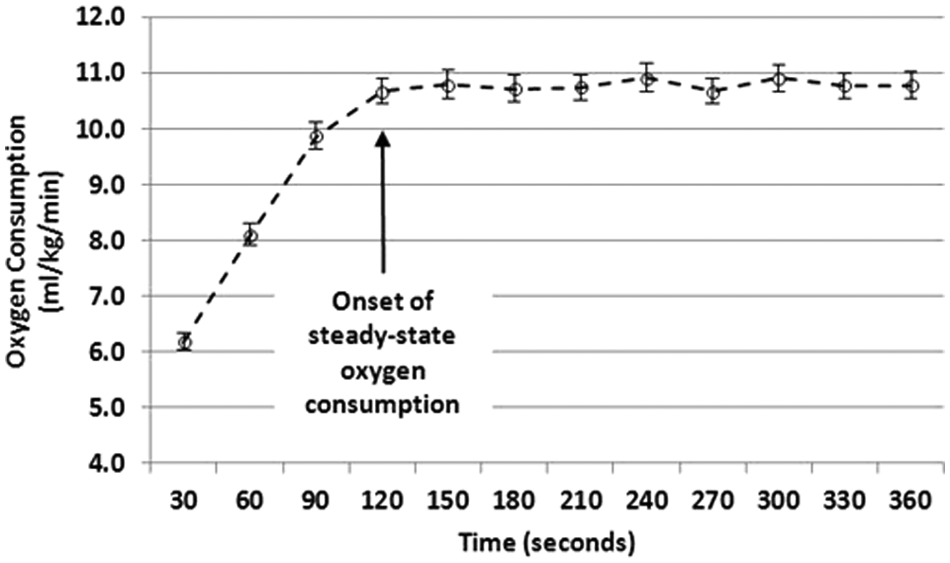
Oxygen consumption over the 6-minute period of treadmill walking in persons with mild multiple sclerosis.
Gait parameters
Participants completed 4 trials of walking on a 26-foot GAITRite (CIR Systems, Inc, Havertown, Pennsylvania) electronic walkway at a comfortable pace as done in previous research involving persons with MS.8,9 We recorded the velocity (m s−1), stride length (m), and double limb support (percentage of gait cycle) per walking trial based on previous research involving persons with mild MS. 5 The average of the 4 trials for each variable was used in the analysis. 9 Higher values for velocity and stride length indicate faster speed and longer steps while walking, respectively, whereas higher values for double support indicate a greater portion of the gait cycle with both feet on the ground during walking.
Daily activity level
Daily activity level was measured objectively using the ActiGraph Model 7164 accelerometer. 10 This accelerometer contains a single, vertical axis piezoelectric bender element that generates an electrical signal proportional to the force acting on it. The acceleration/deceleration signal is digitized by an analog-to-digital converter and numerically integrated over a preprogrammed epoch interval. At the end of each interval, the integrated value of movement counts is stored in random access memory and the integrator is reset. The monitor is programmed for start time and data collection interval, and data are retrieved for analysis via a personal computer interface and software provided with the unit. The data that are downloaded from the accelerometers are entered into Microsoft Excel for data processing. The epoch was 1 minute in this study, and the accelerometers were worn on an elastic belt around the waist on the side of the body in-line with the nondominant hip during the waking hours, except while showering, bathing, and swimming, for a 7-day period. Regarding data processing, we summed the minute-by-minute counts across each of the 7 days and then averaged the total daily movement counts across the 7 days (counts per day). 10 Higher total daily movement counts reflect greater daily activity.
Perceived fatigue
Fatigue was measured with the 9-item Fatigue Severity Scale (FSS). 11 The items were rated on a 7-point scale (1 = Strongly disagree and 7 = Strongly agree) and item scores were averaged into an overall measure of a person’s severity of fatigue symptoms across the past 4 weeks that ranges between 0 and 7. Higher FSS scores reflect greater severity of fatigue.
Patient Determined Disease Steps (PDDS)
The PDDS scale 12 is a self-report measure of walking mobility using an ordinal scale of 0 (Normal) through 8 (Bedridden). The PDDS scale was developed as an inexpensive surrogate for the Expanded Disability Status Scale (EDSS), 13 and scores from the PDDS are linearly and strongly related with physician-administered EDSS scores (r = .93). 12
Multiple Sclerosis Walking Scale–12 (MSWS-12)
The MSWS-12 is a 12-item patient-rated measure of the impact of MS on walking. 14 The items are rated on a 5-point scale of 1 (Not at all) to 5 (Extremely), and the items represent limitations of walking during the past 2 weeks. The MSWS-12 is scored by summing the item scores, subtracting 12, dividing the difference by 48, and then multiplying the result by 100. Scores range between 0 and 100, and higher scores indicate worse walking mobility or more walking difficulty.
Protocol
The protocol was approved by our university institutional review board. All participants provided written informed consent. The protocol included 2 testing sessions that were separated by 7 to 14 days. On the day of the first testing session, all participants completed a demographic questionnaire and then the PDDS, MSWS-12, and FSS. The PDDS and MSWS-12 were administered for confirming the mild disability level of the sample. The participant’s height and weight (while wearing clothing) were measured using a scale-stadiometer unit (Detecto Model 3P7044, Webb City, Missouri), and participants performed 4 trials of walking at a comfortable pace on the GAITRite mat. The participants then engaged in an accommodation trial that involved wearing the oxygen analysis system while walking on a motor-driven treadmill for 5 to 10 minutes. The participants were provided with an accelerometer to wear over the next 7 days.
On the day of the second testing session, participants returned the accelerometer and then sat and rested in a comfortable chair in the laboratory for 10 minutes. We next connected the open-circuit spirometry system and sampled expired gases for 2 to 3 minutes as a method of confirming proper functioning of the system and stabilizing participant physiological data. This was followed by the participant sitting quietly in an armchair for 5 minutes while wearing the oxygen analysis system for generating an estimate of resting energy expenditure. The participants then undertook a 6-minute walk at a constant, controlled speed of 54 m min−1 on the motor-driven treadmill while wearing the oxygen analysis system. This combination of duration and treadmill speed was consistent with previous research 2 and known to be within the comfortable tolerance for walking of all participants. The speed was verified by measuring belt length and the time for 25 revolutions of the belt. The treadmill grade (0%) was verified by a digital inclinometer (Beall Tilt Box, The Beall Tool Company, Newark, Ohio).
Statistical Analysis
All analyses were performed using SPSS, version 18 (SPSS, Chicago, Illinois). Descriptive statistics are presented in text and tables as mean ± standard deviation (SD). Distributional statistics are presented in the tables as estimates of skewness and kurtosis. Associations among C w, gait parameters, and daily activity were examined using Pearson product–moment correlations (r). Associations involving fatigue with the aforementioned variables were estimated using Spearman rho rank-order correlations (ρ) considering the ordered nature of data from the FSS.
Results
The sample consisted of 44 persons with a definite diagnosis of MS (38 women and 6 men) who had a mean age, height, and weight of 47.2 ± 9.1 years, 168.2 ± 8.3 cm, and 75.7 ± 19.4 kg, respectively. There were 40 persons with relapsing–remitting MS, 2 persons with secondary progressive MS, and 2 persons with primary progressive MS. The mean duration of MS was 10.8 (SD = 7.7) years, and the median PDDS score was 1 (interquartile range = 0-3) indicating minimal disability (ie, some noticeable, but minor symptoms from MS with minimal effect on one’s lifestyle). The mean MSWS-12 score was 23.2 (SD = 20.6), further indicating minimal mobility disability in those with MS.
The descriptive data along with the range of scores for Cw, resting and steady-state
Energy Cost of Walking, Gait Parameters, Daily Activity, and Perceived Fatigue in 44 Participants With Multiple Sclerosis
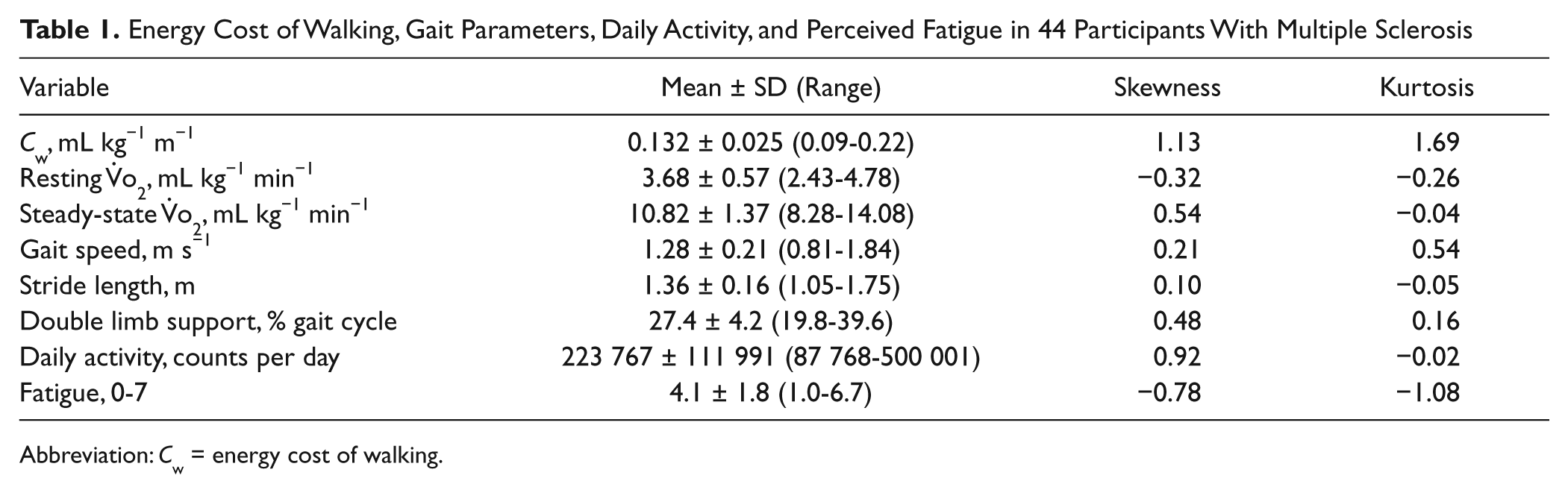
Abbreviation: Cw = energy cost of walking.
The correlations among variables are provided in Table 2. Regarding gait parameters, C w was inversely associated with gait speed (r = −.25, P < .05) and stride length (r = −.32, P < .05) and positively associated with double limb support (r = .27, P < .05). Scatter plots for the associations are provided in Figure 2. For daily activity and fatigue, C w was inversely associated with daily accelerometer activity counts (r = −.35, P < .01) and positively associated with FSS scores (ρ = .31, P < .05). Scatter plots for the associations are provided in Figure 3.
Associations Among Energy Cost of Walking, Gait Parameters, Daily Activity, and Fatigue in the Sample of 44 Participants With Multiple Sclerosis a
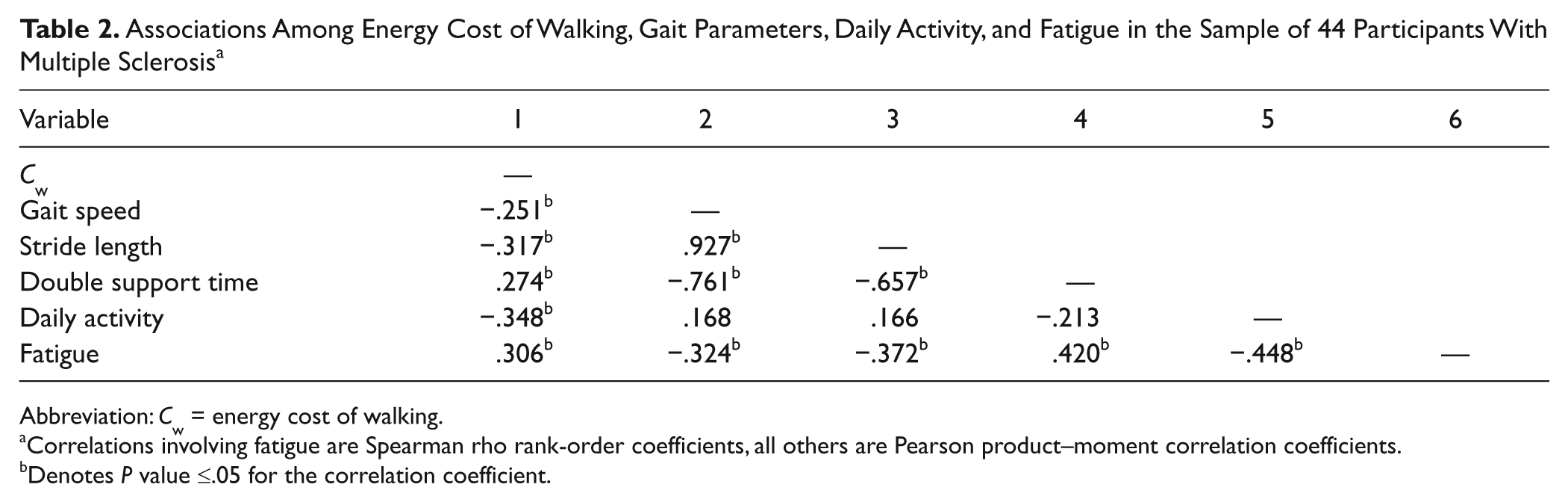
Abbreviation: Cw = energy cost of walking.
Correlations involving fatigue are Spearman rho rank-order coefficients, all others are Pearson product–moment correlation coefficients.
Denotes P value ≤.05 for the correlation coefficient.
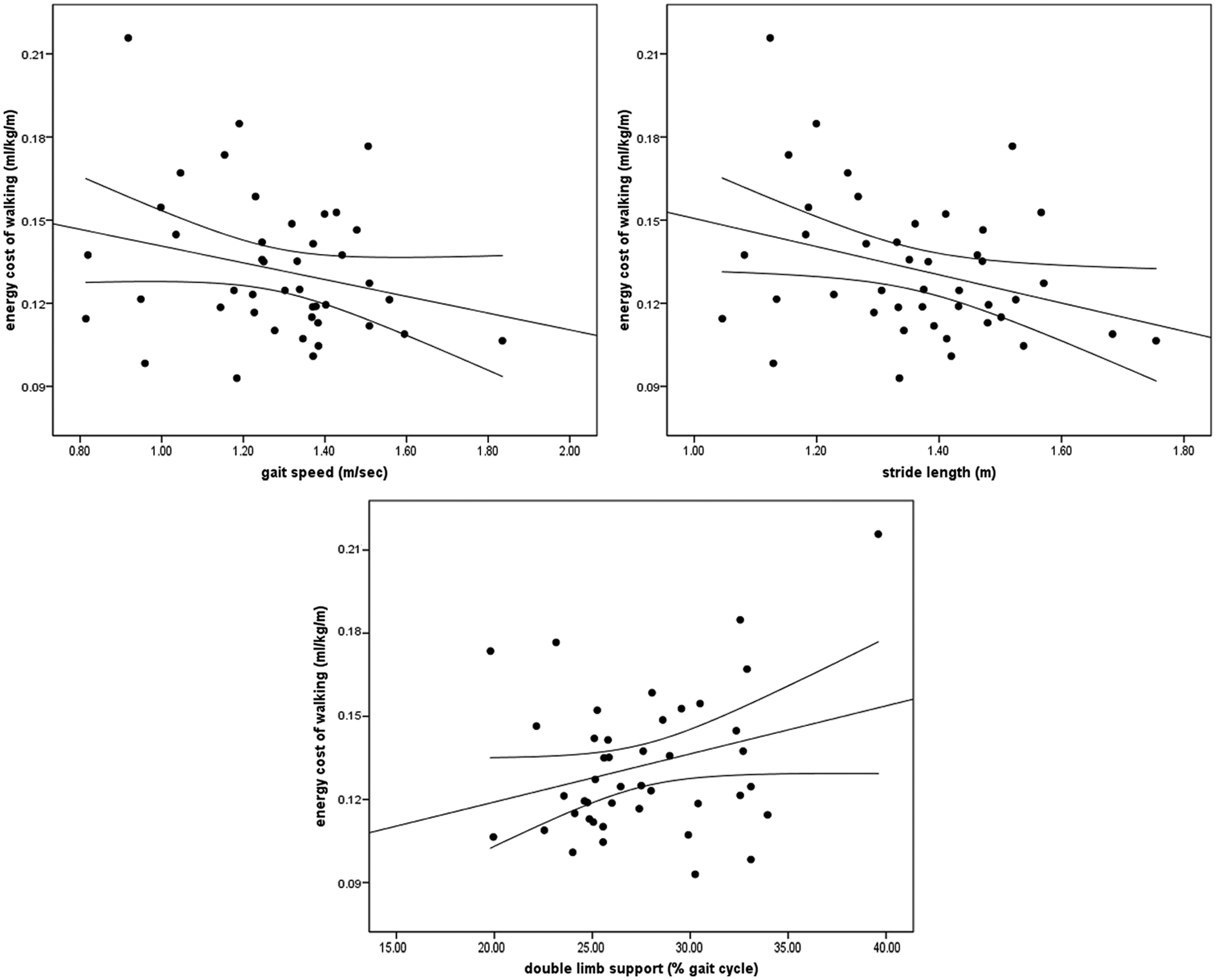
Scatter plots along with lines of best fit and 95% confidence intervals for associations among energy cost of walking, gait speed, stride length, and double limb support in persons with mild multiple sclerosis.
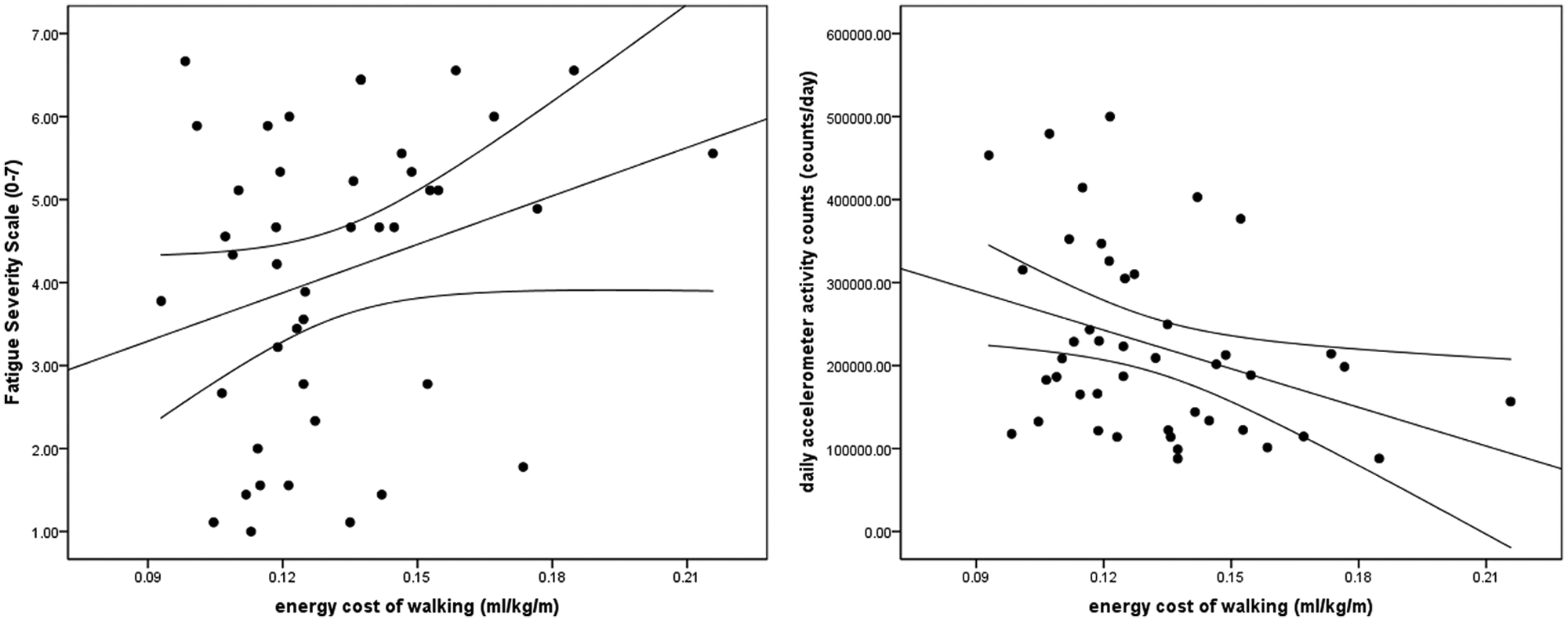
Scatter plots along with lines of best fit and 95% confidence intervals for associations among energy cost of walking, fatigue, and daily activity in persons with mild multiple sclerosis.
Discussion
Our results indicated that (a) gait speed, stride length, and double support were associated with Cw and (b) Cw was associated with daily activity and perceived fatigue in this sample of persons with mild MS. Collectively, these novel results indicate that persons with MS who have mild disability are likely to expend more energy when completing activities of daily living, at least partly due to impaired gait, and this increase in energy expenditure may reduce the level of daily activity and increase the perception of fatigue severity. Such results might support the development of rehabilitation interventions that target gait impairment and fitness to reduce Cw with possible downstream effects on daily activity and fatigue levels in persons with mild MS.
This study was motivated, in part, by previous reports of differences in Cw and gait parameters between persons with mild MS and age, sex, height, and weight matched controls.2,5 For example, one previous study compared Cw between persons with mild MS (n = 18) and age-, sex-, height-, and weight-matched controls (n = 18) and reported a similar difference in Cw while walking on a treadmill at a speed of 54 m min−1. 2 Another study reported that persons with early MS walked with altered gait speed, stride length, and double limb support compared with age- and sex-matched controls. 5 Importantly, we extended the results of that previous research2,5 by demonstrating that the same gait parameters were associated with C w in persons with mild MS. Persons with mild MS who had reduced gait speed and stride length and prolonged double limb support demonstrated an increased energetic cost of walking on a treadmill. We do note that those gait parameters are highly interrelated and might have overlapping associations with C w. Nevertheless, this finding is consistent with previous reports that physiological energy expenditure is adversely penalized by gait abnormalities in some neurologic and orthopedic disorders, 1 although such an association has not been previously demonstrated in persons with mild MS. This would support the development and application of rehabilitation strategies for mitigating the energetic penalties of gait abnormalities during ambulation, and possible approaches for this might involve a walking program with rhythmic auditory stimulation 16 or functional electrical stimulation cycling. 17 For example, the administration of a home-based walking program with rhythmic auditory stimulation has recently resulted in a statistically significant reduction in double limb support and trends with moderate-to-large effect sizes for increases in velocity and step length in persons with MS, 16 and this might translate into improved energetic efficiency during walking.
The C w among persons with mild MS was associated with both daily activity and the severity of fatigue, and we are unaware of previous research documenting such associations in this population. Indeed, those with mild MS who had an elevated C w engaged in less daily activity as measured by free-living accelerometry and reported a greater level of perceived fatigue severity as measured by FSS. Such associations are logical as persons with MS would expend more energy when completing activities of daily living, and this seemingly would reduce the level of daily activity and increase the likelihood of severe fatigue. This further supports the importance of the development and application of rehabilitation strategies for mitigating the energetic penalties of gait abnormalities because such programs might translate into participation in more daily activity and reduced fatigue among persons with mild MS.
This study measured C w during a fixed, constant walking speed of 54 m min−1 on a motor-driven treadmill. The fixed, constant walking speed was considerably slower than the mean gait velocity recorded from the GAITRite for the sample of persons with MS. Importantly, the mean gait velocity from the GAITRite for the sample with MS was within the range for usual gait speed among adults. 18 The fixed, constant walking speed used for measuring C w was considerably slower than usual for those with MS and this difference could have meaningfully 19 affected gait kinematics on the treadmill and, based on the speed–energy relationship, 20 might have resulted in a more costly gait. By extension, perhaps there is an association between gait parameters and C w during a fixed walking speed in persons with MS because of the reduced capacity for adapting to a different gait speed brought on by manifestations of this disabling disease.
This study was not focused on examining the association between gait speed and daily activity, but we note that there was not a significant association between those variables in the present study. This is inconsistent with some previous research 21 that has reported an association between performance on walking tests such as the timed 25-foot walk (T25FW) or timed up-and-go (TUG) and daily steps from an ankle-worn accelerometer in persons with MS. One possible reason for the lack of an association in the present study is that we measured gait velocity during a comfortable walking speed on the GAITRite, whereas that previous research measured gait velocity during the T25FW and TUG that involve walking as quickly as possible. We further note that we relied on the metric of total activity counts per day, whereas that previous research relied on total step counts per day. Last, the sample in the present study had minimal disability, and the association between gait speed and daily activity has been stronger in those with moderate than mild MS. 21 Such differences between the current and previous research might account for the discrepancy in the association between gait speed and free-living daily activity.
Despite the novelty and strengths of the current study, there are some limitations that should be considered in interpreting and generalizing the results. One limitation is that gait parameters are highly correlated as seen in Table 2 and might have overlapping associations with Cw. We did not examine the unique contribution of the gait variables in association with Cw and this should be the aim of subsequent research. The cross-sectional study design is a limitation because it does not provide longitudinal data on the possibility that an elevated Cw results in worsening of community ambulation and fatigue over time in persons with mild MS. This design further does not identify the direction of causality among Cw and gait parameters, but cross-sectional data are generally a precursor for the design of randomized controlled trials that isolate causality. We further note that the sample mostly consisted of women with relapsing–remitting MS and the results might not be representative of men and other clinical courses of MS. Last, Cw was measured on a treadmill rather during over-ground walking. We do note that previous research has reported a similar increase in the Cw during both treadmill and over-ground walking, 2 and we adopted an adaptation trial for minimizing the likelihood that novelty with treadmill walking itself was attributable for an elevated C w in persons with mild MS compared with matched controls.
The sense of fatigue and fatigability with activity are common complaints in persons with MS.22-24 Our study demonstrated that a higher C w was associated with gait parameters, daily activity, and fatigue in persons with mild MS. This supports the application of rehabilitation strategies to manage impaired gait parameters so that persons with mild MS can lessen the energy cost of mobility and fatigue that may interfere with the amount of their daily activities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Foundation of the Consortium of Multiple Sclerosis Centers.