
Abstract
Keywords
Background
Falls occur in up to 70% of persons with stroke (PwS) during the first 6 months after discharge from hospital or rehabilitation facility.1-5 Compared with general population of fallers, PwS who fall are twice as likely to sustain a hip fracture, usually involving the paretic side. 6 Falls are major causes of functional decline, poor quality of life, dependency, and mortality. Studies indicate that 30% to 80% of PwS report fear of falling. 7 Fear of falling in PwS can lead to reduced physical activity levels and deconditioning, creating a vicious circle that may result in greater inactivity and social isolation. 8 Although falls are an enormous burden, the evidence of benefit from fall interventions in stroke is limited.5,8 A meta-analysis showed no significant effect of exercise as the intervention (ie, postural symmetry training and routine community physical therapy) on fall rate (rate ratio, 1.22; 95% CI, 0.76-1.98) or proportion of fallers (risk ratio, 0.77; 95% CI, 0.24-2.43) in PwS. 5
Previous studies found associations between fall risk and impaired balance control during “fixed support” balance reactions (e.g., spontaneous postural sway in stance, reactions to external perturbations in stance without changing the base of support) in older adults. However, the ability to avoid falling depends on the ‘change in support’ balance reactions that involves a rapid limb movement (ie, a step or a grasp response) to alter the base of support.9,10 Consequently, interventions to improve balance reactive responses resulting from unexpected loss of balance were suggested to have a more significant impact on fall risks. 11 A recent meta-analysis reported that anticipatory balance capacities (assessed by the Berg Balance Scale, functional reach test, sensory organization test, and mean postural sway velocity) can be improved in PwS by exercises targeting balance, weight shifting, and gait. 12 Most fall prevention programs are directed toward improving voluntary movements (ie, anticipatory postural adjustment). These postural adjustments can be trained through voluntary exercises and they are the traditional target of most well-designed balance training regimes. However, it is well known that unexpected loss of balance triggers automatic reactive balance responses that act to recover equilibrium. Such responses are faster than the fastest volitional movements. 9 Therefore, in order to increase the ecological validity and specificity of training regimen training conditions should include real-life conditions (eg, unexpected loss of balance). Balance perturbation exercises targeting reactive balance responses might be a more effective and specific approach for fall prevention than general balance training focused on maintaining balance during voluntary movement.
Perturbation-based balance training (PBBT) is a task-specific intervention aiming to improve reactive balance control after loss of balance in a safe and controlled environment. 13 Participants are exposed to unannounced balance perturbations in order to simulate the unpredicted nature of falls in real-life. We used a surface translation system that moves unexpectedly. This has the potential to be ecologically valid because it specifically demonstrates the ability or inability to recover from trips and slips that account for about 60% of older adult falls in the community.14,15 Recent systematic review and meta-analyses of randomized controlled trials (RCTs) and clinical controlled trials found a positive effect of PBBT in reducing the risk of falls among older adults and individuals with Parkinson’s disease.16-18 In an RCT, Pai et al 19 found a 50% reduction in falls 12 months after training in older adults who participated in a single training session of 24 unannounced slips during walking. In an RCT, Mansfield et al 20 also found an improvement in reactive stepping responses in older adults (ie, decreased the frequency of multiple stepping and foot collisions) through repeated exposure to external perturbations. Additionally, in an open trial, persons with Parkinson’s disease who participated in a 10-day perturbation training significantly improved their reactive step length, step initiation, and gait velocity and the improvement was retained after 2 months. 21
Studies of reactive balance capacity in PwS have shown impaired responses characterized by inability to step with either lower limb and falls into harness system.22-26 Also, PwS demonstrated impaired multiple-step threshold (ie, initiating more than 1 recovery step at lower perturbation intensities compared with healthy adults), which shows a poorer capacity to recover balance in response to unexpected surface perturbations. 27 Multiple step response is a strong predictor for falls in older adults. 28 A recent RCT 29 reported no significant difference in fall rate in chronic PwS that performed PBBT versus controls. On the other hand, a case-control study of subacute PwS who completed PBBT during inpatient rehabilitation reported fewer falls 6 months postdischarge compared with a nonperturbation control group. 30
Motivated by previous studies and the lack of RCTs in subacute PwS, we aimed to study the effect of a short-term PBBT on reactive balance responses, balance confidence as well as balance and gait clinical measures compared with nonperturbation balance training in PwS. We also aimed to determine the effects of PBBT on balance confidence and balance and gait. We hypothesized that PBBT would result in greater improvements in reactive balance capacity (ie, higher multiple-step threshold and higher fall threshold) due to the specificity principle of physical training. According to the principle of specificity of physical training and exercise physiology, in the training process an effective intervention should incorporate exercises that closely mimic a specific function, in our case balance recovery exercises. 31
Methods
Participants
PwS were recruited during their hospitalization at the Loewenstein Rehabilitation Hospital (LRH), Ra’anana, Israel between November 2016 to February 2018. Inclusion criteria included first unilateral stroke, being able to walk with or without a walking aid independently or under supervision. Exclusion criteria included body weight greater than 135 kg, other neurological disorders, severe arthritis, joint replacement surgery and blindness, confirmed by the individuals’ physician and medical record at the time of enrollment. The study was approved by the Institutional Review Board at the Loewenstein Hospital (approval number LOE-14-0021, ClinicalTrials.gov Registration number #NCT02619175). Participants signed a written informed consent according to the declaration of Helsinki.
Study Design
Subacute PwS were randomized to perturbation-based balance training (PBBT) or weight shifting and gait training (WS>). Allocation was made by an investigator not involved in the assessments using computer random allocation software (Random Allocation Software Version 1.1, Isfahan Iran). Participants were tested before and after the training period by a blinded investigator. PwS in the PBBT and WS> groups received 12 training sessions, each session lasted 30 minutes, 1 training session per day over a period of 2.5 weeks. Pretraining (T1) and posttraining (T2) assessments included laboratory balance capacity functions and clinical measures of balance, gait, motor impairments, and balance confidence. Follow-up assessment (T3) conducted 5 weeks after intervention completion and included only assessment of reactive balance capacity. All assessment sessions were performed at the same time of day and in the same order (Figure 1).
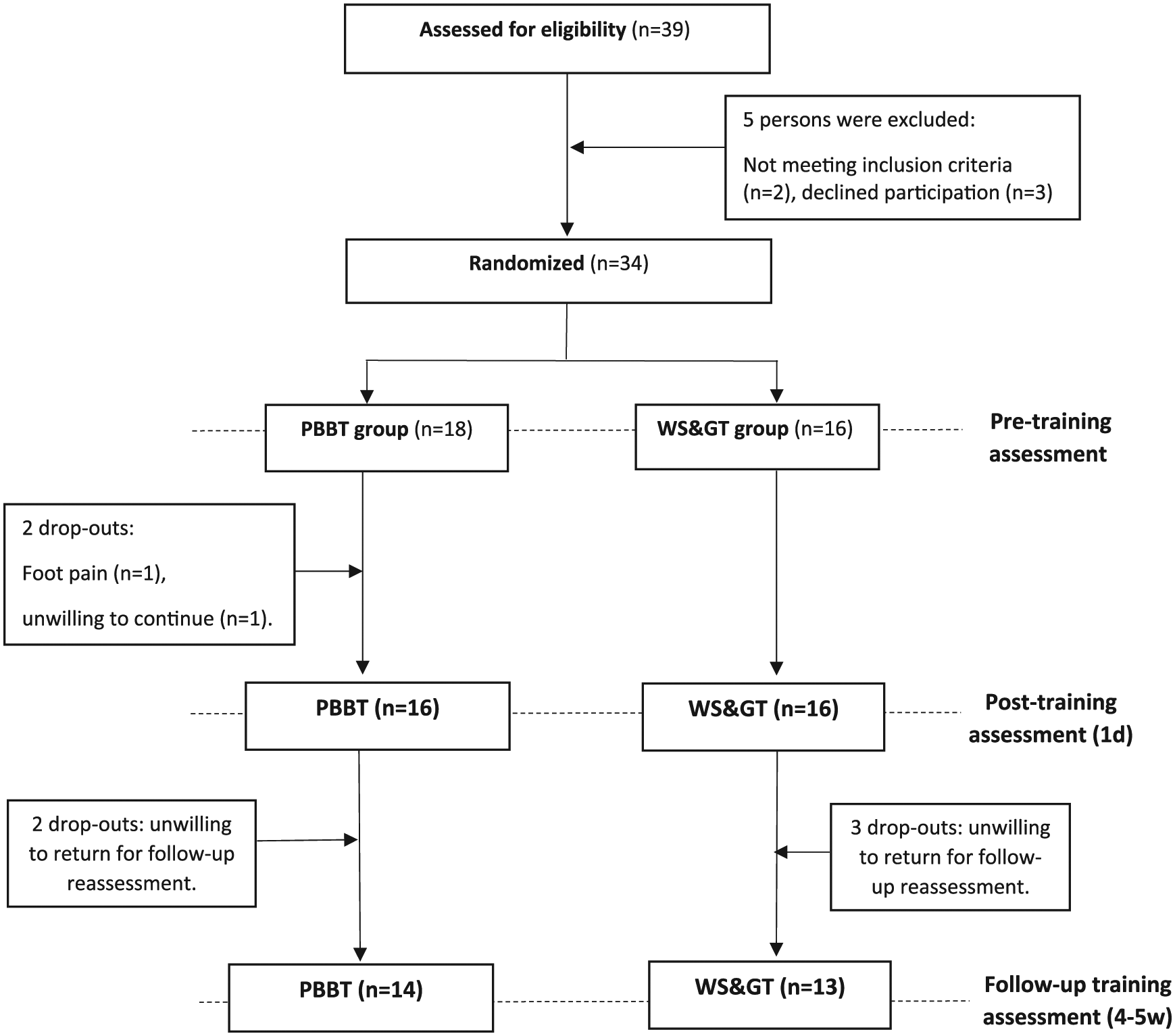
Trial flowchart. PBBT, perturbation-based balance training; WS>, weight shifting and gait training.
Assessment Protocol
Participants stood on a computerized mechatronic treadmill system that provides unannounced perturbations by a horizontal movable platform (Balance Tutor, MediTouch Ltd, Israel), wearing a safety harness that prevented falls but did not restrict their movements. Surface translations were increased systematically in 6 intensities from low (intensity 1) to high (intensity 6) for a total of 24 perturbation trials (characteristics of perturbation intensities are described in Table 1). In this study, perturbation direction refers to the direction of the platform translation. Participants were instructed to stand with feet placed together and to react naturally to prevent themselves from falling. A safety harness system was attached to an overhead track via rope. Rope length was adjusted individually so it would prevent participants’ knees from touching the treadmill belt in case of fall. In case of a fall into harness, the participant did not continue to higher intensity. Participants performed all trials wearing their own sport shoes and foot orthosis in case they needed ankle support.
Perturbation Characteristics of the Assessment Protocol. a
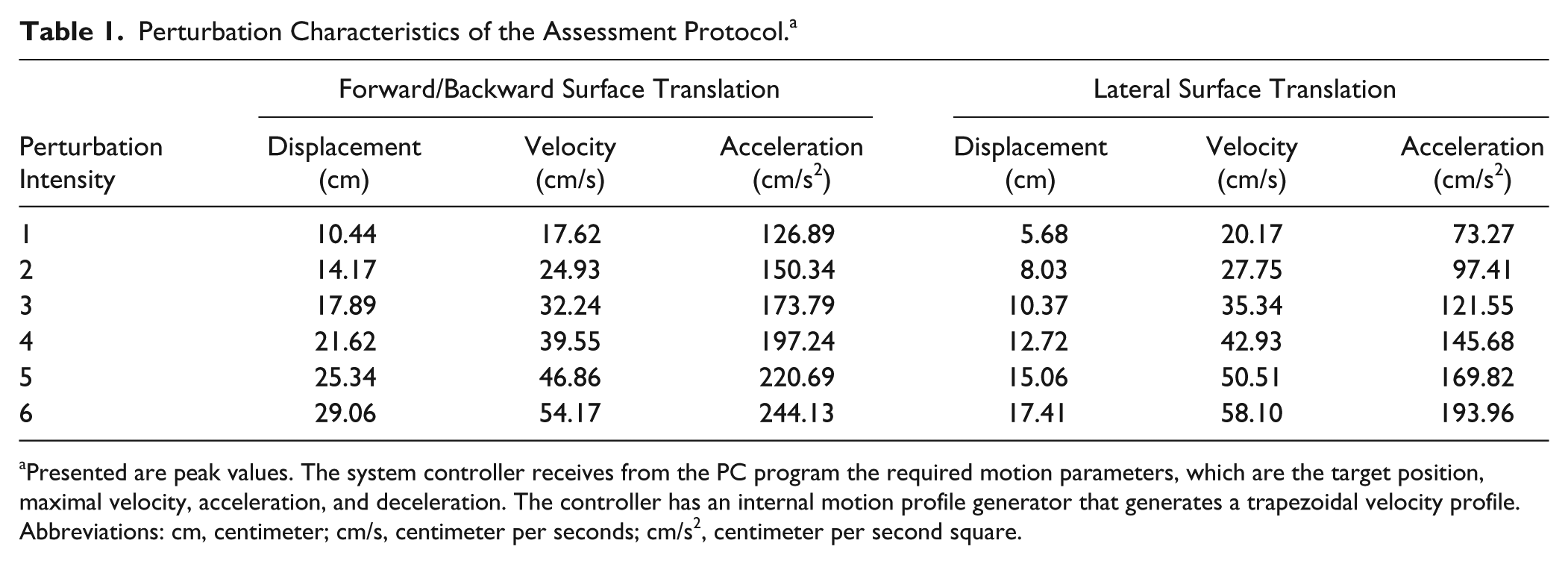
Presented are peak values. The system controller receives from the PC program the required motion parameters, which are the target position, maximal velocity, acceleration, and deceleration. The controller has an internal motion profile generator that generates a trapezoidal velocity profile.
Abbreviations: cm, centimeter; cm/s, centimeter per seconds; cm/s2, centimeter per second square.
Primary Outcomes
Reactive balance capacity was assessed by multiple-step threshold and fall threshold. Multiple-step threshold was defined as the minimum perturbation intensity that consistently elicits 2 or more compensatory steps that extended the base of support in at least 2 consecutive perturbation intensities. Fall threshold was defined as the perturbation intensity that results in unsuccessful balance recovery, that is, when a subject was unambiguously supported by the harness system. 22 Multiple-step threshold and fall threshold have been found to demonstrate high interrater and test-retest reliability in healthy adults.32,33 In case a participant did not fall at the highest perturbation intensity (intensity 6), his or her fall threshold was calculated as intensity 7.
Secondary Outcomes
A day prior to the reactive balance assessment, PwS underwent a clinical assessment that included the lower extremity Fugl-Meyer (LEFM) assessment, Berg Balance Scale (BBS), 10-meter walk test (10MWT), 6-minute walk test (6MWT), and Activity-specific Balance Confidence (ABC) scale. These measures have been found to demonstrate strong interrater and test-retest reliability in PwS.34-39
Intervention Programs
In the PBBT group, each training session consisted of 36 random right/left/forward/backward unannounced platform translations while standing (ie, 3 blocks of 12 perturbations) and 30 random right/left perturbations during a 10- to 12-minute treadmill walk (Balance Tutor, MediTouch Ltd, Israel). Perturbations were synchronized to the single support phase of gait cycle using the Balance Tutors’ inertial sensors. Perturbations were unpredicted in terms of time and direction. The instruction was “try to prevent yourself from falling.” In the first training session, the initial perturbation intensity was individually adjusted according to participant’s maximal ability, that is, the maximal perturbation intensity that could be recovered without falling into harness system during the baseline assessment. Progression to higher intensity occurred if the participant was able to recover from 24 consecutive perturbations (2 blocks of 12 perturbations) without a fall and felt that he or she could be further challenged. The increase in intensity during training was constant and a function of the following perturbation parameters: in forward and backward perturbations: distance = 1.86 cm, velocity = 3.65 cm/s, and acceleration = 11.72 cm/s2 and in response to lateral perturbations: distance = 1.17 cm, velocity = 3.79 cm/s, and acceleration = 12.07 cm/s2.
In the WS> group, each session consisted of 36 voluntary weight shifting exercises (3 blocks of 12 targets) delivered in a random order while standing on a computerized force platform (Balance Master, NeuroCom International Inc) and a 10- to 12-minute treadmill walk without perturbations. For weight shifting, participants stood on a force platform while viewing a display of their center of pressure position relative to a target on a screen. They were instructed to shift weight in order to reach the target without changing their feet position or falling. In the first session, the initial distance for weight shifting was individually adjusted for each participant as the maximal distance he or she could shift weight without falling into harness or changing their feet position. The distance to target was increased by 5% if the participant was able to complete a set of 24 consecutive weight siftings without falling or changing their feet position and felt that he or she could be further challenged (Figure 2).

Participants in the perturbation-based balance training (PBBT) group (left) practiced while standing and walking on a mechatronic device that provides controlled and unexpected forward, backward, right and left surface translations. Perturbation intensity was individually adjusted according to participant’s maximal ability (ie, the maximal perturbation intensity that could be recovered without falling into harness system). Participants in the weight shifting and gait training (WS>) group (right) practiced voluntary weight shifting to forward, backward, right, and left directions while standing. Participants viewed a display of their center of pressure position relative to a target on a screen. The distance for weight shifting was individually adjusted for each participant as the maximal distance he or she could shift weight without falling into harness system or changing base of support. The WS> group practiced walking on a treadmill without perturbations.
Participants in both groups walked at their preferred treadmill walking speed that was adjusted during sessions according to their abilities. In case the participants needed, support was given by the therapist’s hand. To increase task difficulty in both groups a concurrent cognitive task was added (backward counting by 3 or 7) in training sessions 9 to 12. Participants were provided information regarding knowledge of the results of the balance reaction, that is, the occurrence of a fall into harness, through information inherent in the task (the pull of the harness) and verbal feedback regarding perturbation intensity/weight shifting distance and walking speed. At the end of each session participants were asked to rate their perceived level of challenge on a 0-to-10 scale where 0 represents no challenge and 10 represents very high challenge. During the study period, PwS continued with their regular rehabilitation therapies that included daily physical therapy and occupational therapy treatments and if needed, speech therapy treatment. All measurement and training sessions were conducted by physical therapists working in neurological rehabilitation.
Statistical Analysis
Statistical analyses were performed using SPSS version 24.0 (IBM Corp, Armonk, NY). Baseline characteristics were compared using independent-samples t test for continuous variables, Mann-Whitney U test for ordinal variables or variables with nonnormal distributions, and chi-square test for categorical data. Descriptive data analysis and tests for the assumption of normal distribution (Shapiro-Wilk test P > .05) were followed by a mixed factorial analysis of variance for normally distributed dependent variables (6MWT and 10MWT). The independent variables were group (PBBT, WS>) and time (baseline-T1, postintervention-T2, follow-up-T3). In case of nonnormal distributions or ordinal variables (fall threshold, multiple-step threshold, LEFM, BBS, and ABC) the Mann-Whitney U test was used to compare group-by-time interactions by computing the differences between postintervention and baseline performances (T2 − T1) and between follow-up and baseline performances (T3 − T1). Significance levels were set at P < .05.
PwS who completed the postintervention assessment were included in the data analysis. Intention-to-treat analysis was performed so that the last observation of all outcome measures was carried forward for PwS who dropped out during the follow-up period. In addition, spaghetti plots were used to demonstrate the fall threshold and multiple-step thresholds for each PwS in the PBBT and WS> groups so that each line represents the individual’s change over time (baseline-T1, postintervention-T2, follow-up-T3).
The effect size (ES) (Hedges’ g) between the 2 independent groups was calculated by dividing the difference between the means of each group by the pooled baseline standard deviation (SD) of both groups. Values between 0.2 and 0.49 were considered a small, between 0.5 and 0.79 a moderate, and 0.8 and higher a large effect.
Results
Thirty-nine PwS underwent the pre-enrollment screening evaluation. Of those, 2 did not meet inclusion criteria and 3 declined participation. From the 34 ultimately included patients, 2 dropped out in the PBBT group (Figure 1). At baseline no significant differences were found between groups for demographic data or measures of gait and balance (Table 2), except for significantly more hemorrhagic stroke in the PBBT group compared with the WS> group (5 vs 0, P = .015).
Characteristics of PBBT and WS> Groups, and Baseline (T1) Performance. a
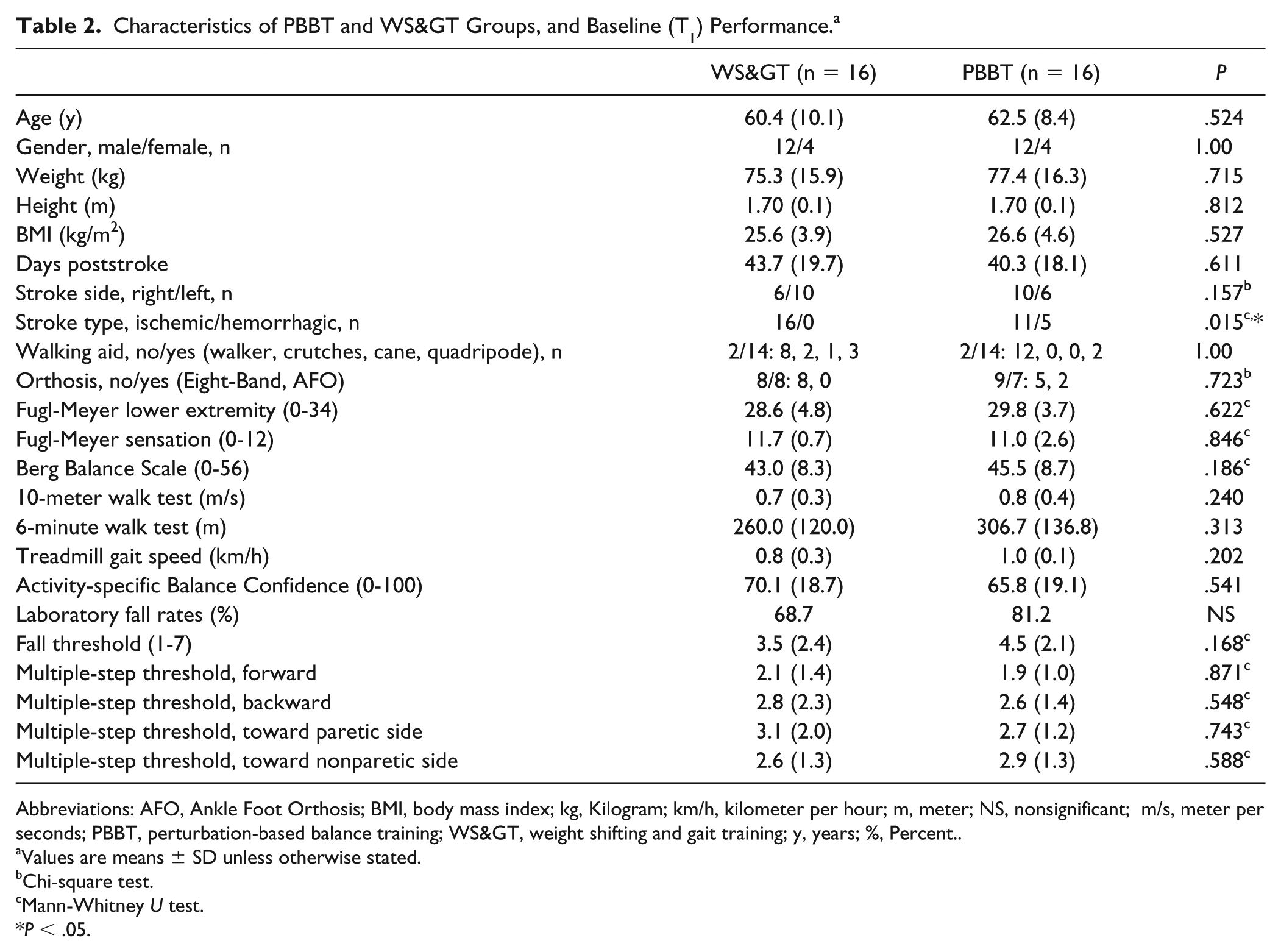
Abbreviations: AFO, Ankle Foot Orthosis; BMI, body mass index; kg, Kilogram; km/h, kilometer per hour; m, meter; NS, nonsignificant; m/s, meter per seconds; PBBT, perturbation-based balance training; WS>, weight shifting and gait training; y, years; %, Percent.
Values are means ± SD unless otherwise stated.
Chi-square test.
Mann-Whitney U test.
P < .05.
Multiple-Step Threshold
Table 3 shows significant group-by-time interaction and a large effect size for multiple-step thresholds in response to forward surface translation in PBBT group compared with WS> group for ΔT2 − T1 (z = −2.49, P = .013, effect size [ES] = 1.07). Also, a large effect size (ES = 0.97) and a trend toward significant group-by-time interaction were found for ΔT3 − T1 (z = −1.68, P = .092). In response to backward surface translations PBBT also showed a significantly higher multiple-step threshold with a large effect size compared with WS> group for both ΔT2 − T1 (z = −2.55, P = .011, ES = 1.10) and ΔT3 − T1 (z = −2.86, P = .004, ES = 1.48). There were no significant differences between groups for the multiple-step thresholds in response to lateral surface translations and the effect sizes were small. Figure 3B-E demonstrates the multiple-step thresholds changes over time for each PwS in the PBBT and WS> groups by direction of perturbation.
Comparison of Fall Threshold and MST Between PBBT and WS> Groups at Baseline (T1), Postintervention (T2), and Follow-up (T3). a
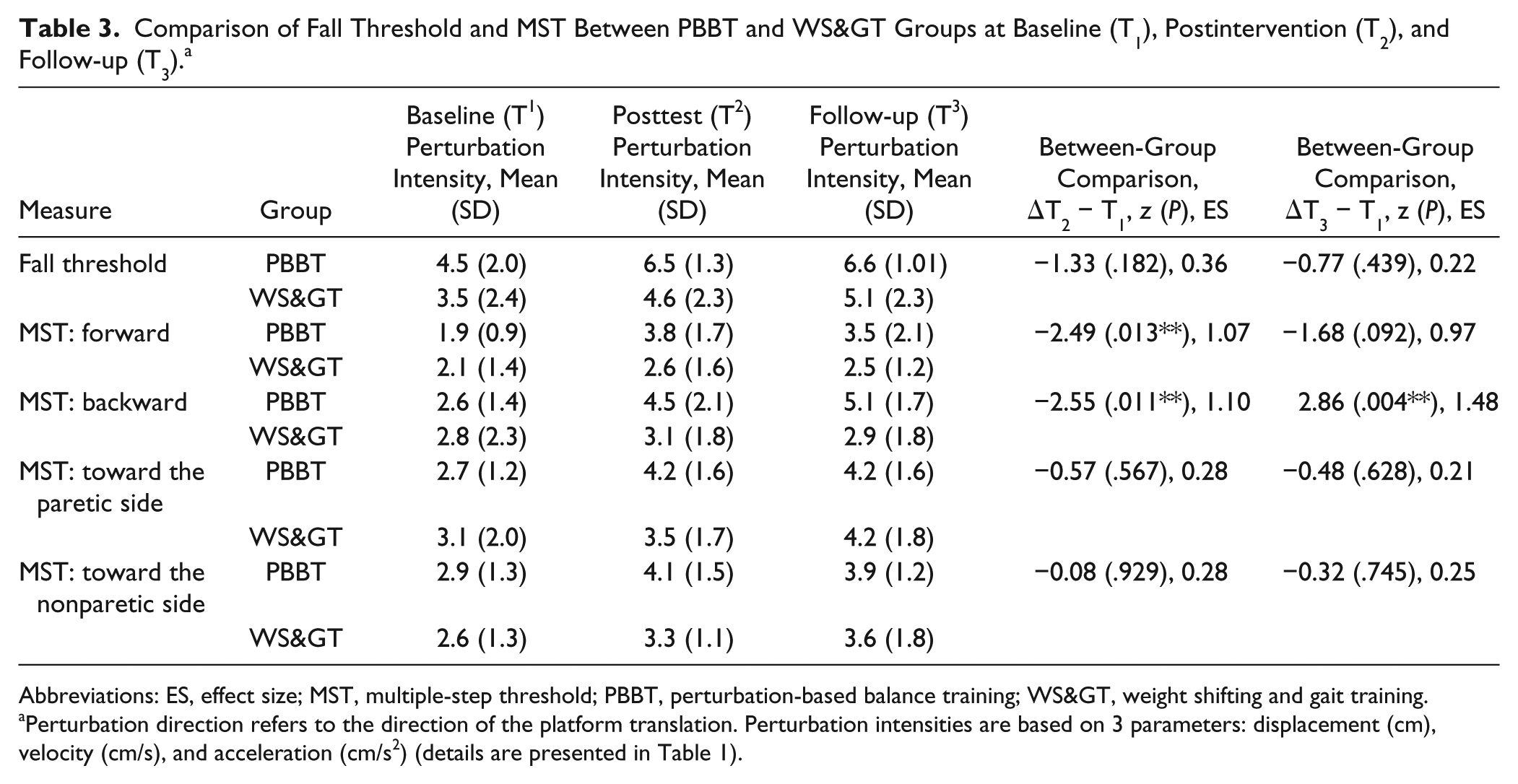
Abbreviations: ES, effect size; MST, multiple-step threshold; PBBT, perturbation-based balance training; WS>, weight shifting and gait training.
Perturbation direction refers to the direction of the platform translation. Perturbation intensities are based on 3 parameters: displacement (cm), velocity (cm/s), and acceleration (cm/s2) (details are presented in Table 1).
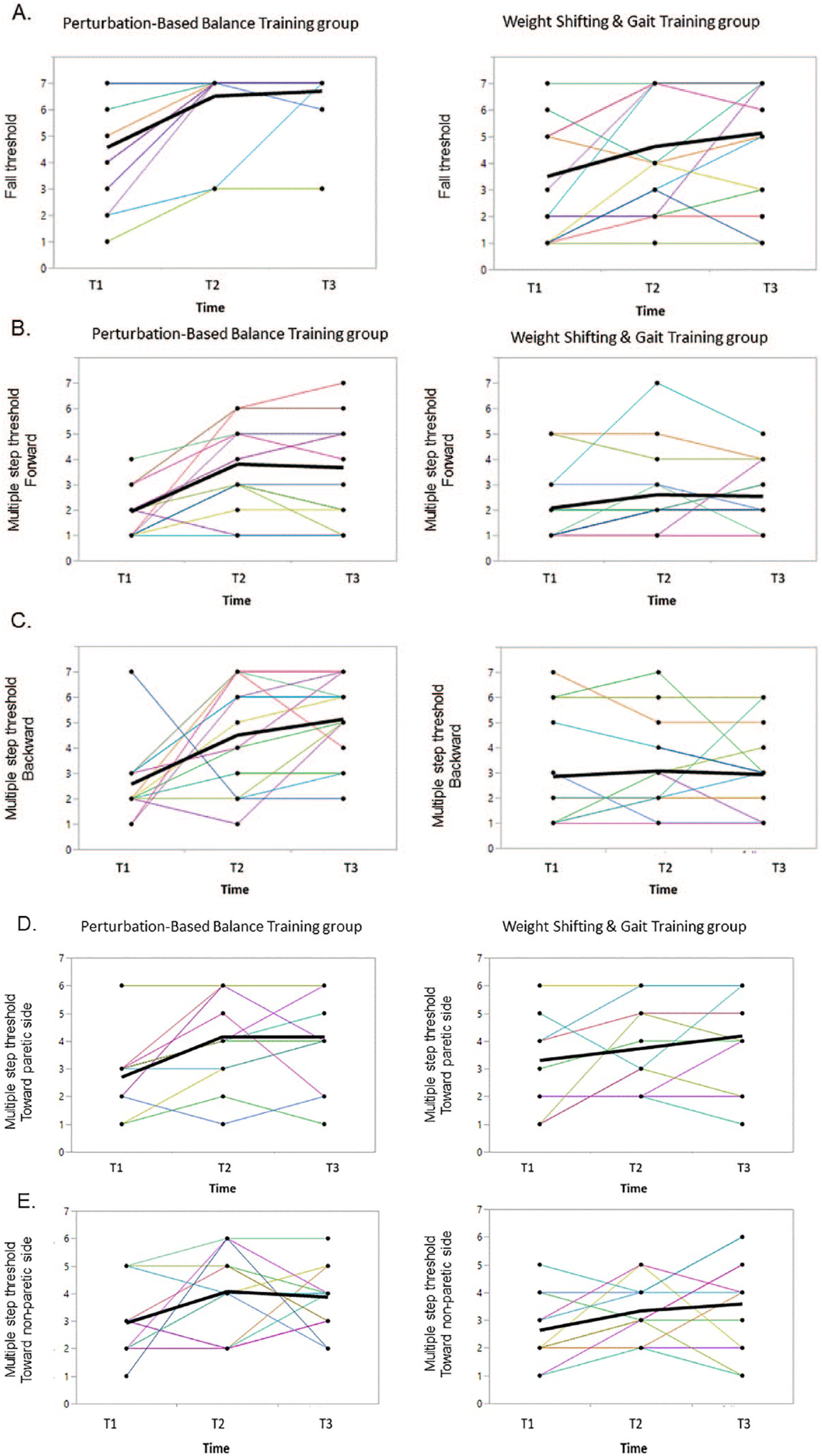
(A) Fall threshold. Multiple-step thresholds in response to forward (B), backward (C), toward the paretic side (D), and toward the nonparetic side (E) surface translations at baseline (T1), postintervention (T2), and follow-up (T3). Lines in the left columns represent participants in the perturbation-based balance training (PBBT) group, lines in the right columns represent participants in the weight shifting and gait training (WS>) group.
Fall Threshold
No significant group-by-time interactions and only small effect sizes were found for ΔT2 − T1 (z = −1.33, P = .182; ES = 0.36) and for ΔT3 − T1 (z = −0.77, P = .439; ES = 0.22) (Table 3). In the PBBT group 11, 2, and 2 PwS fell into the harness system at T1, T2, and T3, respectively. The spaghetti plots (Figure 3A) show that 9 out of 11 PBBT participants that fell into the harness system at baseline (T1) did not fall postintervention (T2). The fall threshold for the 2 participants that fell at T2 increased from T1 to T2. The fall threshold for the 2 participants who fell at T3 remained the same for 1 participant and decreased for the other from T2 to T3. In the WS> group, 13, 9, and 8 PwS fell at T1, T2, and T3, respectively (Figure 3A). Four of the 13 WS> participants that fell into the harness system at baseline (T1) did not fall postintervention (T2).
Reactive Balance Strategies
The following observations were also made: The frequency of crossover step strategy during surface translations toward the nonparetic side was almost doubled from baseline to postintervention in the PBBT group (27.9% vs 52.2%), while in the WS> group it remained similar (31.1%, vs 34.5%). Note: the crossover step in response to surface translations toward the nonparetic side were performed with the nonparetic leg (ie, single leg stance on the paretic leg).
Performance-Based Functional Measures
A significant group-by-time interaction and a moderate effect size were found for the ABC scale demonstrating advantage for the PBBT group compared with WS> group (z = −1.96, P = .049, ES = 0.74). Both groups demonstrated improvements postintervention while no significant differences were found between the groups in BBS, LEFM, 6MWT, and 10MWT (Table 4).
Performance-Based Measures of Balance and Gait and Balance Self-Efficacy: Comparison Between PBBT and WS> Groups.
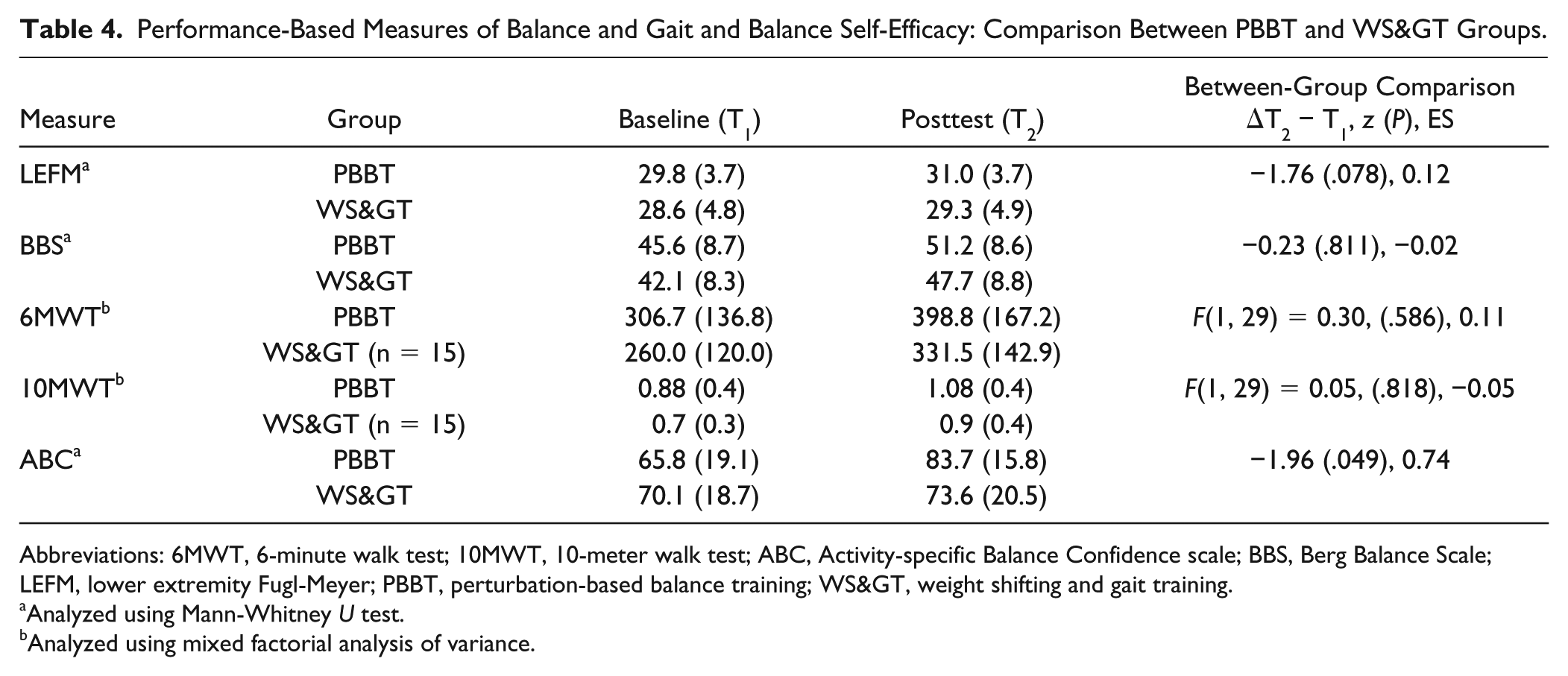
Abbreviations: 6MWT, 6-minute walk test; 10MWT, 10-meter walk test; ABC, Activity-specific Balance Confidence scale; BBS, Berg Balance Scale; LEFM, lower extremity Fugl-Meyer; PBBT, perturbation-based balance training; WS>, weight shifting and gait training.
Analyzed using Mann-Whitney U test.
Analyzed using mixed factorial analysis of variance.
Adverse Effects and Compliance
One participant in the PBBT group reported foot pain during the intervention period and as a result he was not able to complete the training. For all other participants, there was neither any report of discomfort nor adverse effect during the intervention period or during the time between postintervention and follow-up assessments. One participant in the PBBT group dropped out during the training period due to unwillingness to continue (Figure 1). Fourteen out of 16 participants in the PBBT group attended all 12 training sessions, 2 participants attended 10 sessions. In the WS> group, 13 out of 16 participants attended all 12 training sessions, 1 participant attended 11 training sessions and 2 participants attended 10 training sessions. The mean perceived level of challenge was similar in the PBBT and the WS> groups (7.23 ± 1.31 and 6.43 ± 1.68, respectively, t = −1.44, P = .160).
Discussion
The current study supports our main hypothesis that PBBT can improve balance recovery performance in subacute PwS. Participants in the PBBT group showed greater improvements and high effect size in multiple-step threshold in response to forward and backward surface translations as well as significant improvement and moderate effect size in balance confidence (ABC scale) compared with the WS> group. Both groups improved their fall thresholds as well as balance and gait function (ie, BBS, 10MWT, and 6MWT) with no advantage to PBBT versus WS>.
Recent studies have reported high frequency of “laboratory falls” and lower multiple-step threshold in response to perturbations in PwS compared with healthy adults.22,23,26,40 Multiple steps response is considered a strong predictor for real-life falls. 28 Here, we found high effect size for the PBBT demonstrating improvements in multiple-step threshold in response to forward and backward surface translations. Improvement in response to backward surface translations was retained at follow-up (Table 3). We found high laboratory fall rates at baseline assessment in PBBT and WS> groups (68.7% and 81.2%, respectively). There was a reduction in the number of falls as well as a significant improvement in fall threshold postintervention in both groups, with no significant group-by-time interaction. However, a careful inspection of the data shows that while 11 PwS in the PBBT group fell into harness system at baseline (T1), only 2 PwS fell into harness system postintervention at both T2 and T3. In the WS> group, however, while 13 fell into harness system at baseline (T1), 9 and 8 PwS fell at T2 and T3, respectively (Figure 3). We also found that participants in the PBBT group have doubled the use of crossover step response with the nonparetic leg during perturbations as a result of training (ie, single leg stance on the paretic leg). This shows that by exposure to perturbations (ie, inducing errors), participants in the PBBT group were able to find and learn an efficient strategy to maintain the center of mass over the base of support. The results suggest greater improvement in balance recovery capacity in PBBT group compared with WS> group; however, since no significant group-by-time interaction was found for fall threshold and only small effect size (Table 3), it should be treated with caution. We assume that it was not statistically significant because of our study protocol, which exposed PwS to only 6 perturbation intensities. Adding higher intensities might have revealed significant group-by-time interaction in fall threshold. Previous PBBT studies examined long-term effects through either prospective fall monitoring or perturbation recovery performance assessed in laboratory settings. In an RCT study, Marigold et al 40 showed that the number of falls experienced during platform translations was significantly reduced following agility exercise training compared to stretching/weight-shifting exercise training in chronic PwS. In another RCT study, Bahtt et al 41 reported that the incidence of laboratory falls was reduced from 44% to 0% after one perturbation training session and was retained after 6 months in community-dwelling older adults. In a case-control study, Mansfield et al 30 reported fewer falls 6 months postdischarge in PwS who completed PBBT during inpatient rehabilitation compared with PwS who did not complete PBBT. A recent RCT found no significant difference in real-life fall rate between PBBT compared with a control group in PwS. 29
The improvements in balance recovery in PBBT was accompanied with a significant improvement in balance confidence. Fear of falling is a major psychological barrier that may restrict participation in everyday activities, limit functioning, and increase the risk of falls. Pang and Eng 42 found that balance confidence, but not balance and mobility performance, was a significant determinant of falls in chronic PwS. Botner et al 37 found that in chronic PwS, an increment in the ABC scale of 6.81 points or more is required to surpass the standard error of measurement (SEM) level. Table 4 shows that the improvement in ABC score in the PBBT group was 17.9 points, indicating also clinical improvement in balance confidence while ABC in the WS> participants was improved in 3.5 points only. It should be noted that improved balance confidence may not only increase the willingness to walk but may also result in overconfidence and taking some risks. Therefore, findings should be examined over a longer period of time and in association with falls in daily life. In addition, we found no significant advantage for the PBBT versus WS> in the performance-based measures of balance and gait in either group (ie, BBS, 6MWT, and 10MWT). This suggests that perturbation training which specifically targets reactive balance responses can improve recovery responses but has no advantage on tasks that involve voluntary balance control. Our results are in line with a recent RCT in chronic PwS, 29 demonstrating significant improvements in reactive balance control (reactive subscale of the mini-BEST [mini-Balance Evaluation Systems Test]) in PBBT compared with a control group, while both groups improved anticipatory balance control (BBS and mini-BEST anticipatory subscale score) and mobility (mini-BEST gait subscale score).
In the present study we compared PBBT vs. WS>, a training method which was previously identified as a successful balance training for PwS. 12 Both training modes were well-adjusted in terms of number of repetitions, treatment duration and progression mode and both were adjusted personally according to the highest balance capacity of each participant. This was supported by the similarity in the perceived level of challenge in both groups. In terms of learning, the beneficial effects of PBBT suggest that experiencing errors, which are equivalent to a fall or a near fall in response to surface translations, may implicitly accelerate re-learning of strategies for balance control.
Several limitations of the study should be acknowledged. First, the results are based on a fairly small sample that was drawn from subacute PwS with a moderate/high level of function (ie, able to walk independently or under supervision), a fact that limits generalization of the conclusions to more severely affected PwS. However, the high frequency of falls during the first 6 months after discharge from rehabilitation highlights the importance of conducting training targeting fall prevention during the subacute phase. Second, because the primary outcomes (ie, multiple-step threshold and fall threshold) are novel, sample size estimation was not conducted. Thus, future studies could establish sample size for larger phase II or even phase III trials based on this study. Third, some of the outcome measures were obtained with the same mechatronic device that served for the PBBT. Thus, one can argue that improved balance recovery responses in these measurements may reflect task familiarity. Yet it should be noted that in earlier PBBT studies in older adults, improvement in balance recovery capacity in the laboratory was shown to generalize and relate to reduced falls in real life. This highlights the fourth limitation, we did not monitor falls prospectively. Consequently, based on the current results we cannot assert with confidence that improvements in reactive balance behavior after PBBT shown in the laboratory predict reduced fall rate in real-life conditions. These limitations should be taken into considerations when designing further clinical trials testing PBBT.
In conclusion, our results show that reactive balance responses and balance confidence can be improved through PBBT. The results support conducting reactive balance training during rehabilitation of PwS.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IM owns a patent on some of the technology used in the BalanceTutor system and receives a part of the standard royalty distribution for the BalanceTutor system.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by a grant from the Ben-Gurion University, by the Helmsley Charitable Trust through the Agricultural, Biological, and Cognitive Robotics Initiative of Ben-Gurion University of the Negev, by a trust from the Loewenstein Rehabilitation Hospital for the doctoral program (to SH), and by Raphael Rozin prize for excellent study in rehabilitation.