
Abstract
Background. Individuals with stroke fall more often than age-matched controls. Although many focus on the multifactorial nature of falls, the fundamental problem is likely the ability for an individual to generate reactions to recover from a loss of balance. Stepping reactions to recover balance are particularly important to balance recovery, and individuals with stroke have difficulty executing these responses to prevent a fall following a loss of balance. Objective. The purpose of this study is to determine if characteristics of balance recovery steps are related to falls during inpatient stroke rehabilitation. Methods. We conducted a retrospective review of individuals with stroke attending inpatient rehabilitation (n = 136). Details of falls experienced during inpatient rehabilitation were obtained from incident reports, nursing notes, and patient interviews. Stepping reactions were evoked using a “release-from-lean” postural perturbation. Poisson regression was used to determine characteristics of stepping reactions that were related to increased fall frequency relative to length of stay. Results. In all, 20 individuals experienced 29 falls during inpatient rehabilitation. The characteristics of stepping reactions significantly related to increased fall rates were increased frequency of external assistance to prevent a fall to the floor, increased frequency of no-step responses, increased frequency of step responses with inadequate foot clearance, and delayed time to initiate stepping responses. Conclusions. Impaired control of balance recovery steps is related to increased fall rates during inpatient stroke rehabilitation. This study informs the specific features of stepping reactions that can be targeted with physiotherapy intervention during inpatient rehabilitation to improve dynamic stability control and potentially prevent falls.
Introduction
Individuals with stroke are at an increased risk for falls compared with age-matched controls.1,2 Recovery from stroke tends to be most rapid during the early stages (ie, the first 3 months 3 ), which is when most patients attend inpatient rehabilitation. This is also a stage when the risk of falling is specifically high. As many as 39% of stroke patients attending inpatient rehabilitation will fall,4,5 and falls occurring during inpatient rehabilitation can impede the course of recovery from stroke.6,7 Therefore, the inpatient rehabilitation phase is an opportune time to identify poststroke physical impairments related to falls risk such that falls prevention–based physiotherapy interventions can be prescribed. 8
Although many factors contribute to falls, 9 a fall is fundamentally a failure to recover from a postural perturbation. 10 Executing stepping reactions ultimately prevents a fall to the ground following a stance perturbation.11,12 Therefore, individuals who show impaired control of stepping reactions are likely at an increased risk for falls. Indeed, previous studies among older adults have found relationships between characteristics of reactive steps and falls.13-16 Compared with older adults who have not fallen, fallers are more likely to step, 13 use multistep reactions,13,16 fall, 13 experience foot collisions, 16 or show difficulty controlling lateral stability 16 following postural perturbations in the laboratory. In terms of timing of the responses, fallers step faster than nonfallers when responding to a postural perturbation, but their overall swing duration is longer. 15
Whereas among older adults, the control of compensatory stepping is an important index of balance recovery capacity and is linked to fall risk, it is likely even more important after stroke, given the unique challenges to recovering from a loss of balance. Whereas older adults tend to respond to postural perturbations as quickly as young adults, 17 markedly delayed stepping responses are often observed among individuals with stroke.18,19 The asymmetric nature of the injury can lead to challenges in the choice of stepping limb.19,20 Additionally, individuals with stroke show ineffective step responses, such as attempts to step with a limb that is physically blocked,18-20 steps with inadequate foot clearance, 18 or not attempting to step at all.19,20 Identifying specific characteristics of stepping reactions related to falls among stroke patients could inform fall prevention physical interventions such as perturbation-based training.18,21
This study aims to determine if characteristics of stepping reactions are related to falls during inpatient stroke rehabilitation. We hypothesize that compared with those who do not fall, fallers will show increased frequency of external assistance, multistep reactions, no-step reactions, step reactions with inadequate foot clearance and attempts to step with a physically blocked limb, and increased time to initiate and complete stepping used to recover balance.
Methods
Participants
We conducted a retrospective chart review of patients admitted to the Toronto Rehabilitation Institute within a 2-year period who received inpatient rehabilitation poststroke. Patients were included in the review if they were able to stand independently and completed assessment of perturbation-evoked stepping reactions in a specialized balance and mobility clinic (as described below) soon after admission to rehabilitation; 136 patients met these criteria and were included in the analysis (Figure 1). To describe the cohort, patients’ age, sex, time poststroke, stroke type and location, affected side, length of stay, National Institutes of Health Stroke Scale 22 scores, Clinical Outcome Variables Scale (COVS) 23 scores, and STRATIFY falls risk assessment 24 were extracted from clinical charts (Table 1). The review was approved by the institution’s research ethics board. A waiver of patient consent for inclusion in the review was approved.
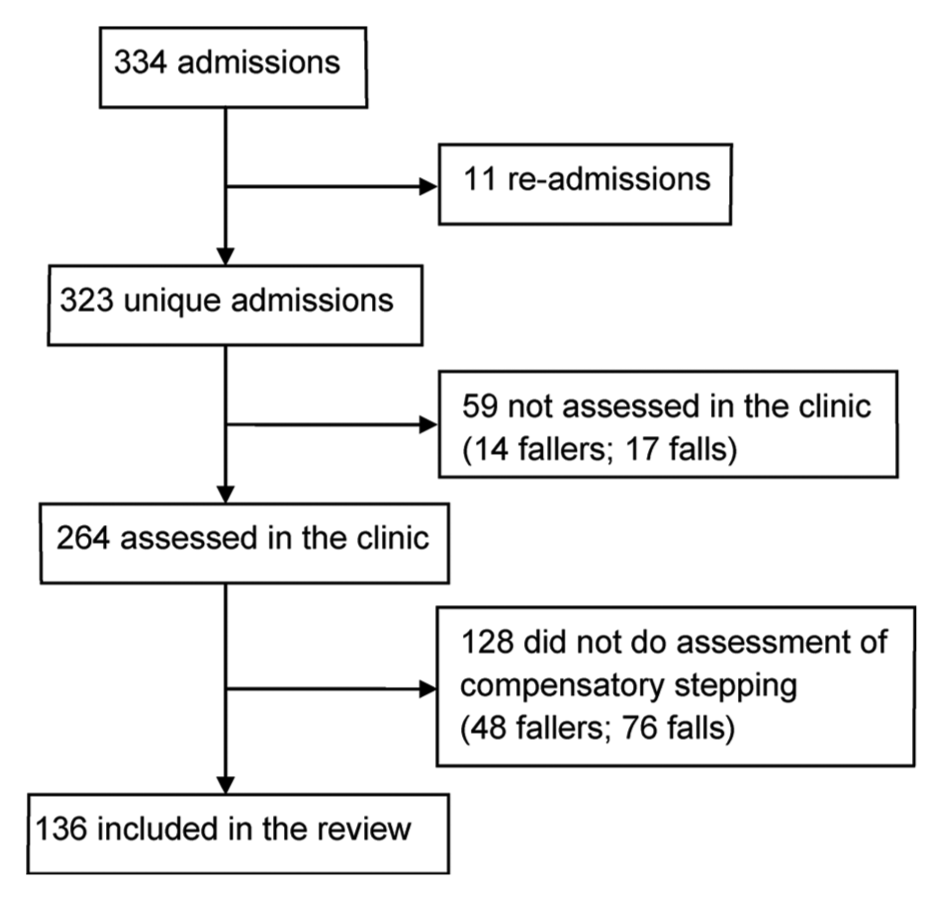
Patients included in the review: there were 334 admissions to the stroke unit in the 2-year period; 11 admissions were individuals who had been admitted previously in the 2-year period and were excluded because they were not unique individuals; 264 individuals were assessed in the balance and mobility clinic. Of these, 136 completed assessment of perturbation-evoked stepping reactions and were included in the review.
Participant Characteristics. a
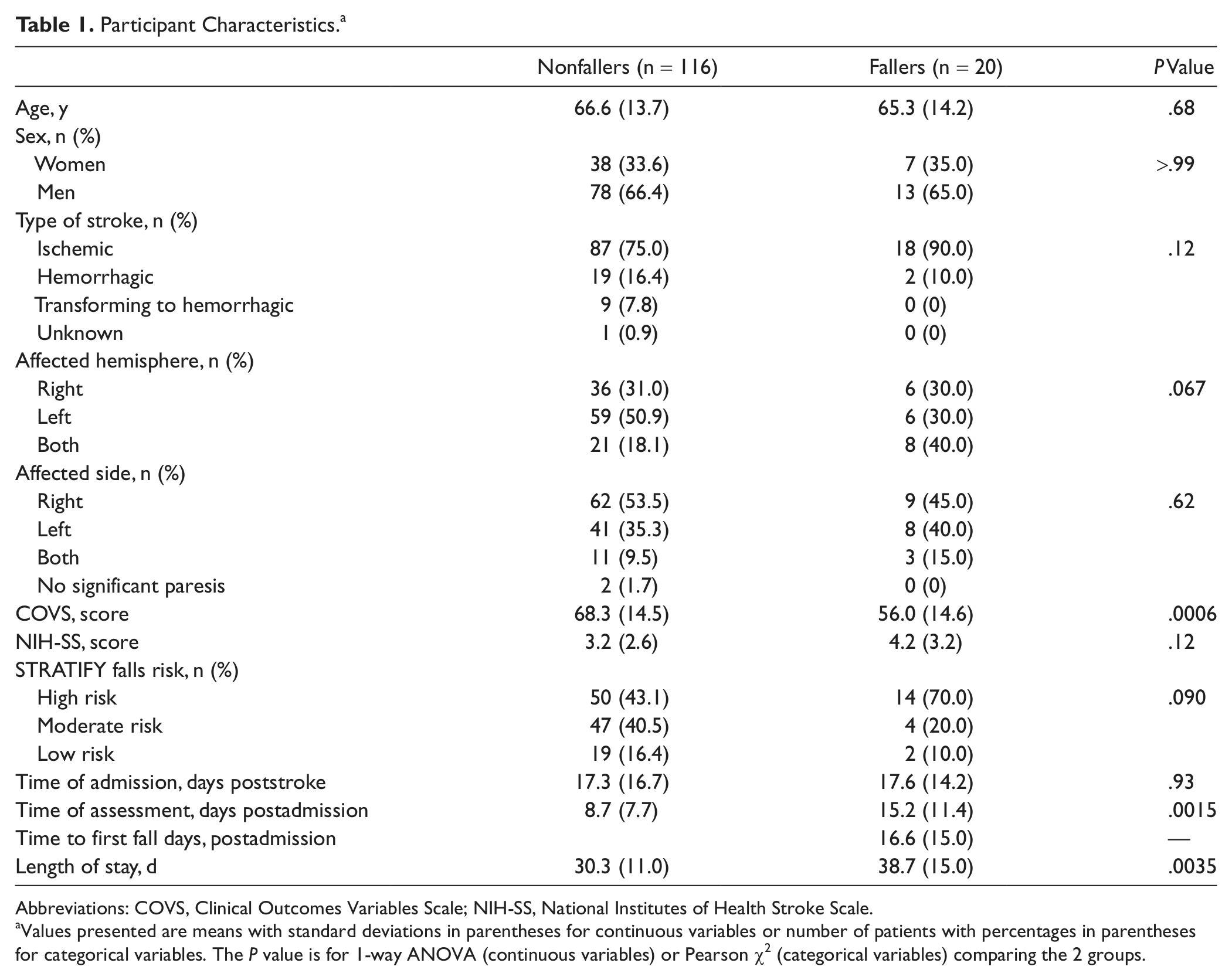
Abbreviations: COVS, Clinical Outcomes Variables Scale; NIH-SS, National Institutes of Health Stroke Scale.
Values presented are means with standard deviations in parentheses for continuous variables or number of patients with percentages in parentheses for categorical variables. The P value is for 1-way ANOVA (continuous variables) or Pearson χ2 (categorical variables) comparing the 2 groups.
Assessment of Reactive Balance Control
Stepping reactions were assessed using a “release-from-lean” perturbation system.20,25 Patients stood with 1 foot on each of 2 force plates (25 cm wide, 50 cm long) and leaned forward such that approximately 10% of body weight was supported by a cable attached to their backs. A third force plate (50 cm × 50 cm) was located directly in front of the 2 smaller force plates. A load cell placed in series with the cable recorded the force on the cable prior to the perturbation and was used to maintain consistency of lean across trials. At an unexpected time, the cable was released causing the patient to start to fall forward such that a step was required to regain stability and prevent a fall to the floor. Patients wore a safety harness attached to an overhead track and 1 or 2 physiotherapists stood next to them to prevent a fall in the event of a failure to recover balance by stepping alone. Patients completed up to 5 trials in each of 2 conditions: usual response and encouraged use. In the usual response condition, patients were instructed to take any necessary action to regain stability following the perturbation. In the encouraged-use condition, the preferred limb for initiating stepping (determined from the usual response condition) was physically blocked by placing the physiotherapist’s hand or foot approximately 5 cm from the shin. Load cell and force plate data were sampled at 256 Hz and stored for offline processing. All trials were video recorded for offline review.
Perturbation onset time was the time when the force recorded by the load cell was <1 N. All timing measures were defined relative to perturbation onset time. Onset of unloading was the time prior to foot-off when the peak vertical force was recorded under the stepping limb. Foot-off time was the time when the vertical force under the stepping limb was <1% of body weight. Foot contact time was the time when the vertical force recorded by either the force plate under the stepping limb or the front force plate was >1% of body weight (Figure 2). Video recordings were viewed to determine balance-recovery behaviors. The number of steps taken to regain stability was recorded. Because of the nature of the perturbation, a 2-step reaction is often appropriate; that is, a step forward with 1 limb is followed by a step with the contralateral limb, such that the patient stands stable with both feet side-by-side at the end of the response. Therefore, multistep reactions were defined as reactions in which 3 or more steps were used to recover balance. An assist was a trial in which assistance from the physiotherapist or the safety harness was required to prevent a fall to the floor. A “slide” or “drag” step was a step with limited foot clearance and was defined by a horizontal motion of the foot, evident on the video recording, without completely unloading the force plate. For slide steps, foot-off time was estimated as the time when the least amount of vertical force was recorded by the force plate under the stepping limb; foot contact time was not defined for slide steps (Figure 2B). The limb used to initiate the stepping response was determined for encouraged-use trials.
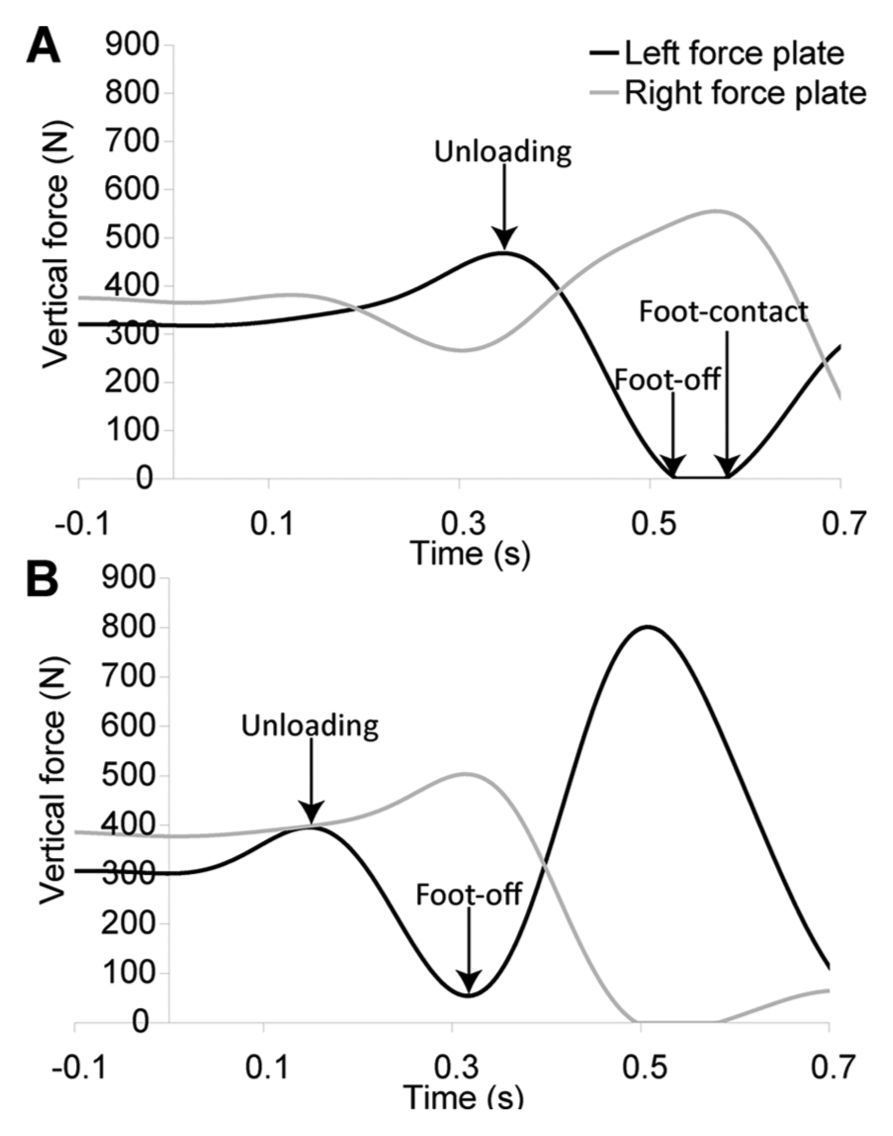
Identification of step-timing variables: vertical forces recorded on both the left and right force plates during the trial are plotted. Perturbation onset occurred at 0 s. The first step was with the left foot in both trials. Panel A shows a trial with complete unloading of the force plate during the step. Foot-off time is the time when <1% of body weight is recorded by the force plate under the stepping limb (in this case, the left force plate). Unloading onset was the time before foot-off when the peak force was recorded by the force plate under the stepping limb. Foot contact time was the time after foot-off when the vertical force under the stepping limb was >1% body weight. Panel B shows a trial with a “slide” step. The left foot moved forward following the perturbation, but there was no complete unloading of the force plate under the stepping limb. Foot-off time is estimated as the time when the minimum vertical force was recorded by the force plate under the stepping limb. Unloading time is defined as before. Foot contact time is undefined.
Falls During Inpatient Rehabilitation
Information on falls that occurred during inpatient rehabilitation was obtained from incident reports, nursing notes, and patient interviews on discharge from rehabilitation. 26 Patient interviews allowed for inclusion of falls that were not captured by the hospital reporting system—for example, falls that occurred when the patient was home on a weekend visit. Falls were defined as any time the patient came to rest unintentionally on the ground, floor, or other lower level. 27 We also examined near-miss incident reports for events that may have been classified as near misses by hospital staff but that met the definition of a fall above—for example, if the patient was lowered to the floor by a staff member. The following details were obtained for each fall: date of fall, suspected cause, location, time of day, motor and/or cognitive activity at the time of the fall, and fall-related injuries.
Statistical Analysis
Individuals who suffered one or more falls during inpatient rehabilitation were classified as fallers. Demographic and stroke information, and COVS and National Institutes of Health Stroke Scale scores were compared between fallers and nonfallers using 1-way analysis of variance (ANOVA) for continuous data or Pearson χ2 for categorical data. Poisson regression was used to relate measures of reactive balance control to fall rates. For the usual response condition, the independent variables were proportion of assists, multistep reactions, no-step reactions, and slide steps and unloading-onset, foot-off, and foot contact times. For the encouraged-use condition, the independent variables were proportion of steps with the blocked limb and no-step reactions. The mean value for each independent variable across all trials completed within each condition was calculated for each patient. The means of each variable were then related to fall rates, expressed as number of falls divided by length of stay, in univariate Poisson regression analyses. For all statistical analyses, α was .05.
Results
In all, 20 patients (14.7%) experienced 29 falls during inpatient rehabilitation; 5 patients had more than 1 fall; and 1 patient had 6 falls. The average fall rate was 6.8 falls per 1000 patient-days. On admission to rehabilitation, fallers had lower functional mobility than nonfallers, as measured by the COVS (P = .0006). On average, the length of stay for fallers was 9 days longer than for nonfallers (P = .0035), and fallers completed assessment of reactive balance control 1 week later in their rehabilitation stay than nonfallers (P = .0015). There were no other significant differences in demographic or stroke information between fallers and nonfallers (Table 1).
Data for 21 falls were obtained from incident reports, data for 21 falls were obtained from nursing notes (not necessarily the same 21 falls as included in incident reports), and data for 17 falls were obtained from patient interviews. There were at least 2 sources of information for 20 falls; 6 falls occurred when patients were at home on a weekend visit. Characteristics of the falls are included in Table 2. Most falls (15/29) occurred in the patient’s bedroom, either in the hospital or at home. Injuries resulting from falls were generally rare (3/29) and were limited to cuts or bruises. Two patients hit their heads following their falls; these patients were monitored with a head injury reporting protocol, but no adverse consequences were noted.
Fall Characteristics. a
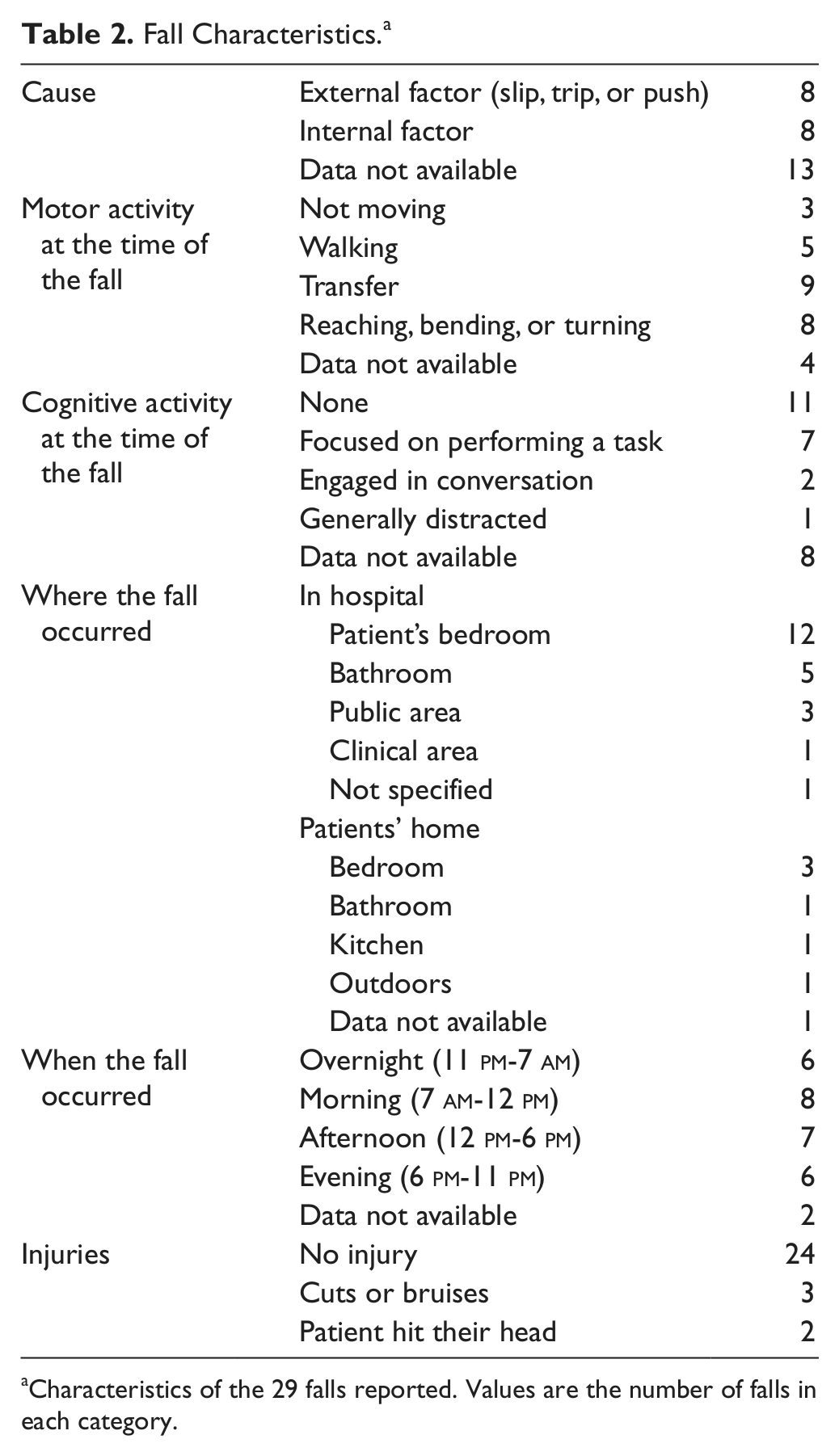
Characteristics of the 29 falls reported. Values are the number of falls in each category.
When considering the relationship between stepping reactions and fall risk, there were relationships between the strategy as well as the response characteristics. Increased frequency of assists (relative risk, RR = 2.9; P = .014), no-step responses (RR = 6.2; P = .0012), and slide steps (RR = 5.9; P = .008) were related to increased fall rates. Increased unloading onset times (RR = 7.2; P = .044) and foot-off times (RR = 7.4; P = .033) were also related to increased fall rates. No other measures of reactive balance control were statistically related to fall rates. Mean values for reactive balance control measures are presented in Table 3.
Relationship Between Measures of Reactive Balance Control and Fall Rates. a
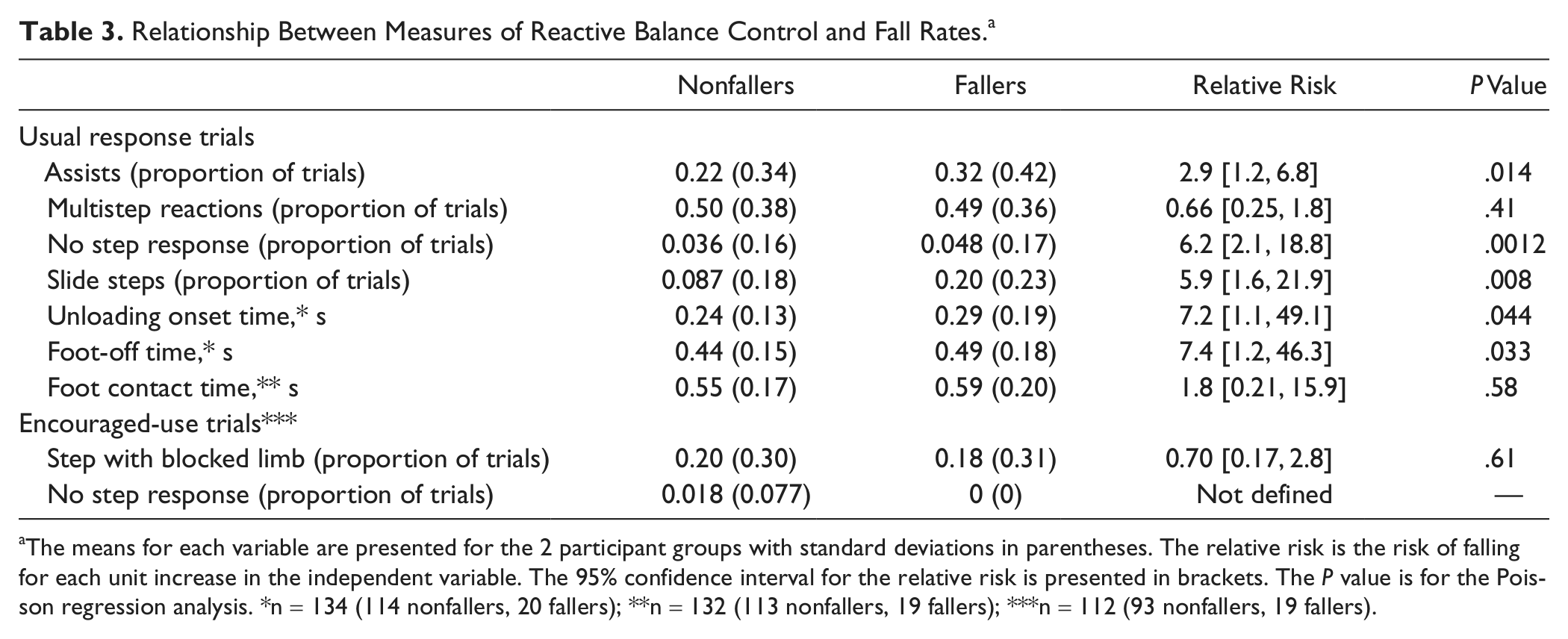
The means for each variable are presented for the 2 participant groups with standard deviations in parentheses. The relative risk is the risk of falling for each unit increase in the independent variable. The 95% confidence interval for the relative risk is presented in brackets. The P value is for the Poisson regression analysis. *n = 134 (114 nonfallers, 20 fallers); **n = 132 (113 nonfallers, 19 fallers); ***n = 112 (93 nonfallers, 19 fallers).
Discussion
This study demonstrates that impaired control of reactive stepping is strongly related to increased fall rates during inpatient stroke rehabilitation. Specifically, increased fall rates were related to: increased frequency of assistance from the physiotherapist or the overhead harness to prevent a fall following the perturbation, increased frequency of trials in which a step response was not initiated, increased frequency of trials with inadequate foot clearance (ie, slide steps), and delayed time to initiate stepping responses. This work reinforces the important need to provide an assessment that can evaluate the capacity of an individual to perform balance reactions. Although other measures may provide an index of fall risk, the specific measures of capacity for balance recovery control not only yields insight into fall risk but also guides clinical decision making regarding strategies to improve reactive balance control and prevent further falls.
The relationship between frequency of assists and fall rates is not surprising. This relationship has been previously found in a study among older adults. 13 Failure to prevent a fall following a perturbation delivered in the clinic is potentially indicative of the ability to prevent a fall following a real-life postural perturbation. However, this variable is of little use to treating physiotherapists without some further insight regarding the underlying impairments that led to difficulty recovering balance. An inability or unwillingness to execute a stepping response was also related to increased fall risk. Such behavior might be linked to an inability to bear weight on the paretic limb in order to execute a step with the nonparetic limb or an inability to rely on the paretic limb to execute the step.19,20 Initial steps with poor foot clearance (ie, slide or drag steps) were also related to increased fall risk. Such steps might occur if the patient is unable to lift the limb high enough to clear the ground. Alternatively, slide steps may result from patients’ discomfort or unwillingness to fully load the stance limb during step execution. Delayed time to initiate stepping reactions was also related to increased fall risk. A previous study that included older adults found that fallers actually initiated stepping reactions faster than nonfallers. 15 However, delayed stepping reactions appear to be more prevalent among individuals with stroke18,19 than older adults. 17 Delayed stepping could be indicative of overall poststroke slowing. 28 Markedly delayed balance recovery reactions to real-life postural perturbations might occur too late to prevent a fall.
Despite the introduction of clinically feasible postural perturbation tools for stroke almost 20 years ago, 29 reactive balance control is not assessed routinely in physiotherapy practice, 30 possibly because of a lack of commercially available equipment to deliver the perturbation or safety concerns. In addition, few clinical balance scales involve assessment of perturbation-evoked responses.31,32 We used, as part of the standard assessment of dynamic balance control, a simple release-from-lean postural perturbation that can easily be implemented in clinical practice. The addition of a load-monitoring device (ie, the load cell in series with the cable) provided a means of standardizing the magnitude of the perturbation across trials. 33 The overhead harness system added safety to the assessment and was modified from a patient-lift system that is common in many hospitals. Additionally, the majority of outcome measures were obtained from observation; although we used video recordings in the current study, these outcomes could also be obtained in real time during the assessment. Measurement of step timing required expensive and specialized equipment (ie, force plates); however, recently, gaming technology has been used as an inexpensive alternative to force plates. 34 Therefore, a quantitative and standardized assessment of this essential stepping behavior, such as the method described in this article, could be inexpensively incorporated into routine clinical practice.
This study was limited to patients who could complete the assessment of perturbation-evoked stepping responses. Only 82% of unique admissions (264/323) were assessed in the balance and mobility clinic, of these, only 52% (136/264) completed assessment of stepping reactions close to admission. Patients did not complete the assessment, because they were deemed to be unable (eg, could not stand independently), refused, or had comorbid medical conditions (eg, back pain). Because of the higher functional levels of the group included in this study, fall rates were lower than that for all individuals on the stroke unit. Specifically, 25% (82/323) of unique admissions fell during inpatient rehabilitation compared with just 15% (20/136) of individuals who completed assessment of reactive stepping. Therefore, the results of the current study are specifically relevant to individuals who are capable of independent standing.
It is also noteworthy that falls were monitored over a narrow window of time; the mean length of stay was 30 to 39 days, and length of stay was shorter for nonfallers than fallers. Some patients in the nonfaller group who had impaired stepping reactions might have been discharged before they had the “opportunity” to fall but instead might have fallen after discharge from rehabilitation. Additionally, inpatient rehabilitation is a relatively predictable and safe environment. The hospital is designed with falls prevention in mind; for example, lighting is generally good, and grab bars and railings are present in the hallways, bedrooms, and bathrooms. Hospital staff are typically present to assist or supervise patients while they walk or perform activities such as toileting. On discharge, patients might experience more challenging environments 35 in which impaired control of reactive stepping poses a greater problem for fall prevention. The relationships between stepping reactions and fall risk after discharge from rehabilitation will be investigated in a future study.
This study identified specific impairments in control of reactive stepping that were related to increased fall rates during inpatient stroke rehabilitation. These findings can be used to inform patient-specific falls prevention rehabilitation strategies, such as perturbation-based training.18,21
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Heart and Stroke Foundation Centre for Stroke Recovery and the Ministry of Health and Long-Term Care, Ontario Stroke System. We also acknowledge support of the Toronto Rehabilitation Institute, which receives funding under the Provincial Rehabilitation Research Program from the Ontario Ministry of Health and Long-Term Care.