
Abstract
Introduction. Physiological responses are rarely considered during walking after stroke and if considered, only during a short period (3-6 minutes). The aims of this study were to examine physiological responses during 30-minute robot-assisted and body weight–supported treadmill and overground walking and compare intensities with exercise guidelines. Methods. A total of 14 ambulatory stroke survivors (age: 61 ± 9 years; time after stroke: 2.8 ± 2.8 months) participated in 3 separate randomized walking trials. Patients walked overground, on a treadmill, and in the Lokomat (60% robotic guidance) for 30 minutes at matched speeds (2.0 ± 0.5 km/h) and matched levels of body weight support (BWS; 41% ± 16%). Breath-by-breath gas analysis, heart rate, and perceived exertion were assessed continuously. Results. Net oxygen consumption, net carbon dioxide production, net heart rate, and net minute ventilation were about half as high during robot-assisted gait as during body weight–supported treadmill and overground walking (P < .05). Net minute ventilation, net breathing frequency, and net perceived exertion significantly increased between 6 and 30 minutes (respectively, 1.8 L/min, 2 breaths/min, and 3.8 units). During Lokomat walking, exercise intensity was significantly below exercise recommendations; during body weight–supported overground and treadmill walking, minimum thresholds were reached (except for percentage of heart rate reserve during treadmill walking). Conclusion. In ambulatory stroke survivors, the oxygen and cardiorespiratory demand during robot-assisted gait at constant workload are considerably lower than during overground and treadmill walking at matched speeds and levels of body weight support. Future studies should examine how robotic devices can be Future studies should examine how robotic devices can be exploited to induce aerobic exercise.
Introduction
After stroke, cardiorespiratory fitness is low—about half that of healthy individuals1-3—increasing the risk of developing secondary cardiovascular diseases. 4 Two-thirds of patients with stroke subsequently die from cardiovascular diseases, making cardiovascular diseases the leading cause of death (4 times higher rate than the general population). 5 This high rate stresses the importance of implementing fitness training in stroke rehabilitation.
Aerobic exercise improves cardiorespiratory fitness after stroke.6,7 Common forms of aerobic exercise are walking (overground or on a treadmill) and cycling (arm or legs). 8 Stroke guidelines recommend large-muscle exercising activities 3 to 5 times per week for 20 to 60 minutes at moderate intensity. 9 The American Stroke Association defines moderate intensity as 40% to 70% of peak oxygen consumption, 40% to 70% of heart rate reserve, 55% to 80% of maximum heart rate, and 11 to 14 rating of perceived exertion. 9
Patients with stroke spend the majority of rehabilitation time on practicing walking (25% to 45%). 10 Hence, walking offers a time-efficient way of fulfilling 2 important rehabilitation goals at once: improving gait and improving cardiorespiratory fitness. Because physiotherapists’ time is sparse—patients often receive less than the recommended minimum of 45 minutes to 1 hour of physiotherapy per weekday11-15—it is important that physiotherapists use their time highly efficiently. To improve gait, daily practice is desirable; to improve cardiorespiratory fitness, a minimum of 3 times per week is recommended. 9
Current inpatient stroke rehabilitation induces no or only little cardiovascular stress to result in a cardiorespiratory training effect.16,17 Patients’ physical impairment and lack of therapeutic staff hinder the implementation of fitness training in inpatient rehabilitation. 18 The use of recumbent steppers and cycle ergometers, or body weight support (BWS) systems and robotic devices may solve these barriers. Especially these latter two facilitate the administration of aerobic exercise to those who cannot walk in a task-specific manner while reducing the number of required therapists. 19 However, physiological responses during robot-assisted gait are rarely considered, 20 making it unclear what the exercise intensity of this type of training is and whether it elicits adequate intensity to reach an aerobic training effect. The Lokomat is an example of a robotic device used in gait rehabilitation after stroke. This device automates locomotion on a treadmill by providing robotic guidance at the knee and hip joints. Varying degrees of robotic guidance (0%-100%), BWS (0%-100%), and walking speed (0-3.2 km/h) can be set according to the patient’s abilities. 21 These numerous combinations of settings lead to different effects on individual exercise intensity. Although decreasing the body weight and assisting the hip and knee joints may allow longer durations of task-oriented practice, it may also decrease exercise intensity below recommended levels for aerobic exercise. In turn, robotic assistance may allow walking faster, which may increase exercise intensity.
Current studies—which are few in number—indicate that the oxygen consumption and cardiorespiratory load during robot-assisted gait after stroke is low (lower than walking without robot assistance). 20 van Nunen et al 22 classified Lokomat walking as light-intensity exercise in 10 patients with stroke; only 1 patient reached an exercise intensity over 30% heart rate reserve. 22 Two other studies examined Lokomat walking with various degrees of robotic guidance, BWS, and walking speed, but neither reached considerably higher oxygen rates (4.89 to 8.09 mL/kg/min).23,24 Likewise, walking in the Gait Trainer, an end-effector device, with 50% weight reduction induced similar rates of oxygen consumption (4.78-8.0 mL/kg/min). Without weight reduction, patients consumed slightly more energy (5.57-10.7 mL/kg/min).25,26
Until now, the number of studies investigating oxygen consumption and cardiorespiratory demand during robot-assisted gait have been limited. Moreover, it is not yet known whether the physiological responses and perceived exertion change with respect to the duration of walking. Although, in the literature, gait training often lasts 30 minutes,27,28 previous work only analyzed the physiological responses during short duration walking (3 to 6 minutes22-26,29). However, decreased cardiorespiratory fitness levels after stroke 2 may result in a state in which the aerobic metabolism alone is unable to generate enough adenosine triphosphate (ATP)—the cells’ primary energy source—and the less-efficient anaerobic metabolism is needed to supplement ATP formation. 30 If the exercise intensity of gait training is around the patients’ anaerobic threshold, the anaerobic metabolism will raise lactate levels, which will elevate carbon dioxide production as a result of lactic acid buffering, and trigger the respiratory system to increase the amount of air exhaled per minute (ie, minute ventilation). 31 The increased lactate production and carbohydrate consumption may result in an increased susceptibility to fatigue.
The aims of this study were 3-fold: (1) to compare the physiological responses and perceived exertion of robot-assisted gait with body weight–supported treadmill and overground walking, (2) to investigate if the physiological responses and perceived exertion change with respect to the duration of walking, and (3) to investigate if the physiological responses and perceived exertion reach aerobic training recommendations. This study is the first to examine poststroke physiological responses and perceived exertion during robot-assisted and body weight–supported gait for 30 minutes.
Methods
Study Design
This study was an experimental, cross-sectional study with randomized crossover design. The study protocol was registered prospectively (NCT02680496) and approved by the medical ethics committees of the University Hospital Brussels and Jessa Hospital Hasselt (B U N 143201526040).
Participants
We recruited 14 participants in the Rehabilitation Centre St Ursula (Herk-de-Stad, Belgium) from February 2016 to July 2017. All participants gave written consent to participate in this trial.
We included adult stroke survivors up to 1 year poststroke, who had a lower-limb motor impairment assessed by visual inspection (eg, poor foot clearance, knee instability, excessive hip circumduction, or gait asymmetry). To analyze training durations up to 30 minutes, we selected participants who could walk overground (functional ambulation category [FAC] 2-4) for at least 10 minutes at self-selected comfortable walking speed (CWS); BWS was allowed (LiteGait, Mobility Research, Tempe, AZ).
We excluded stroke patients with contraindications to exercise testing according to the American College of Sports Medicine, 32 contraindications for Lokomat training, 33 musculoskeletal problems—other than stroke—affecting the ability to walk, concurrent pulmonary diseases, concurrent neurological diseases, communicative and/or cognitive problems affecting the ability to follow or comprehend instructions, and other problems affecting the execution of the interventions (eg, severe spasticity or dermatological conditions).
Experimental Walking Conditions
Participants completed 3 randomized walking trials within 1 week (Monday, Wednesday, and Friday between 3 and 5
Physiological Measures and Rating of Perceived Exertion
At the start of each walking condition, a flexible facemask (small/medium, Cortex, Germany), lightweight chest-carrying gas analysis system (MetaMax 3B, Cortex, Germany), and heart rate belt (Polar H7, Polar Electro, Finland) were fitted. Participants were seated for 5 minutes of rest and afterward installed in one of the walking conditions (Figure 1). Breath-by-breath gas analysis and heart rate monitoring were conducted continuously from the beginning of rest to the end of walking. At the end of rest and at the end of every minute during walking, we asked participants to point their rating of perceived exertion on a 6 to 20 Borg Scale (6 representing no exertion; 20 representing maximal exertion).
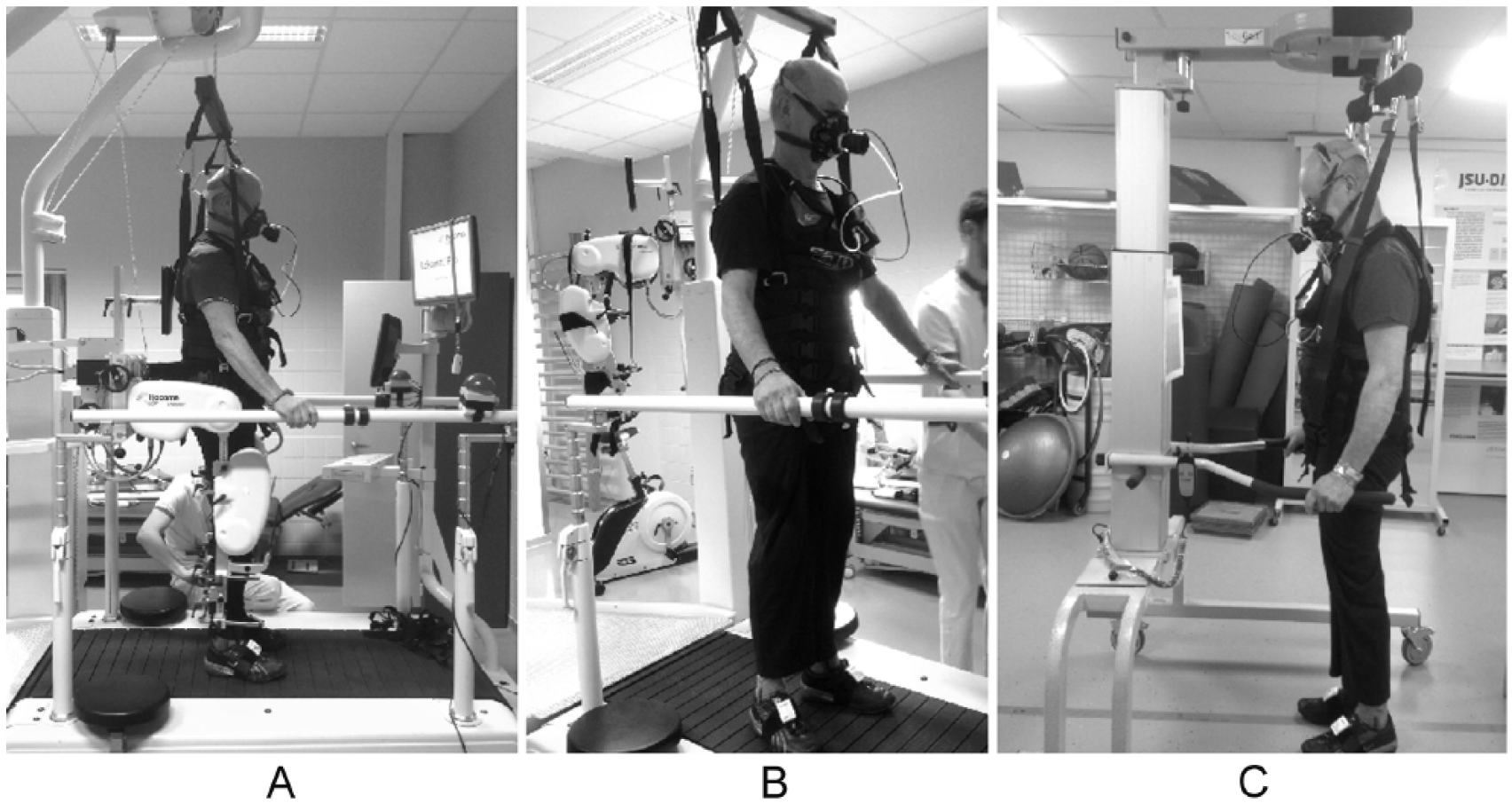
Experimental setup of the walking conditions: A. Lokomat V5.0 with Levi body weight support system. B. Woodway treadmill with Levi body weight support system. C. 30-m Overground track with LiteGait body weight support system.
Before the start of each walking condition, gas and volume calibrations were performed in accordance with the manufacturer’s instructions. We asked participants not to consume food, alcohol, caffeine, or nicotine at least 3 hours prior to the interventions and not to perform additional strenuous activities (apart from their regular therapy) at least 12 hours prior to the interventions. 32 Usual medication intake was allowed with small amounts of water.32,34
Outcomes
To investigate the effect on physiological responses, we analyzed: net oxygen consumption (mL/kg/min), net carbon dioxide production (mL/kg/min), net heart rate (beats/min), net minute ventilation (L/min), net breathing frequency (breaths/min), net respiratory exchange ratio (no unit), and net rating of perceived exertion (0-14). We analyzed net values, because net values take into account testing conditions (eg, variation in environmental factors or personal routines) and show less variability.35,36 Net values were obtained by subtracting resting values (median of minute 5) from gross values. The first 5 minutes of walking were used to reach a steady-state condition and were not used in the analyses. Minutes 6, 18, and 30 were statistically analyzed (see below).
To compare the exercise intensity with aerobic guidelines for stroke survivors (ie, 40%-70% heart rate reserve, 55%-80% maximum heart rate, 11-14 rating of perceived exertion), 9 we calculated: percentage of predicted heart rate reserve {[(Heart ratewalking − Heart raterest)/(Maximum heart ratepredicted − Heart raterest) × 100]}, percentage of predicted maximum heart rate [(Heart ratewalking/Maximum heart ratepredicted) × 100], and gross rating of perceived exertion. Because we could not perform incremental exercise tests to determine the participants’ maximum heart rate, we predicted maximum heart rate using the following formulas: 164 − 0.7 × Age (for persons taking β-blocking medication 37 ) or 206.9 − 0.67 × Age (for persons not taking β-blocking medication 32 ). Because predictions for people after stroke are not available, we adopted formulas for people with heart failure and healthy adults.38,39
Data Processing
We found no universal standard for the data processing of breath-by-breath data. A common procedure in the corresponding literature is time averaging over 30- to 120-s intervals.23-26,29 We chose to calculate medians over 60-s intervals because medians are less affected by irrelevant outliers caused by coughing or talking unintentionally during perceived exertion scoring.
Statistical Analysis
A 3 × 3 2-way repeated-measures ANOVA was conducted to compare the main effects of condition (Lokomat, treadmill, overground) and duration (6, 18, 30 minutes) with the interaction effect between condition and duration on net oxygen consumption, net carbon dioxide production, net heart rate, net minute ventilation, net breathing frequency, net respiratory exchange ratio, and net rating of perceived exertion (SPSS, IBM, Chicago, IL). Significance level was set at 5%. Bonferroni corrections were applied in post hoc analyses to adjust for multiple pairwise comparisons. Effect sizes were calculated to interpret the magnitude of effects: omega-squared (ω2) for repeated-measures ANOVA 40 and Hedges’ gaverage for pairwise comparisons. 41 Effect sizes were rated small (ω2 = 0.01 and Hedges’ gaverage = 0.2), medium (ω2 = 0.06 and Hedges’ gaverage = 0.5), or large (ω2 = 0.14 and Hedges’ gaverage = 0.8). The Shapiro-Wilk test and Q-Q plots were interpreted to check normality and the Mauchly’s test to test sphericity. If sphericity was violated, the Greenhouse-Geisser (ε < 0.75) or Huynh-Feldt (ε > 0.75) correction was applied. 40 One-sample t-tests were used to test whether percentage of heart rate reserve, percentage of predicted maximum heart rate, and gross rating of perceived exertion were above minimum and below maximum threshold for aerobic exercise at minutes 6, 18, and 30. Bonferroni corrections were applied to adjust for multiple testing.
Results
Participant Flow and Characteristics
A total of 14 participants were enrolled in this study; 8 participants completed all three 30-minute walking trials. Table 1 lists the demographic and clinical characteristics of each participant, including reasons for dropping out.
Demographic and Clinical Characteristics of Included Participants With Reasons for Dropping Out.
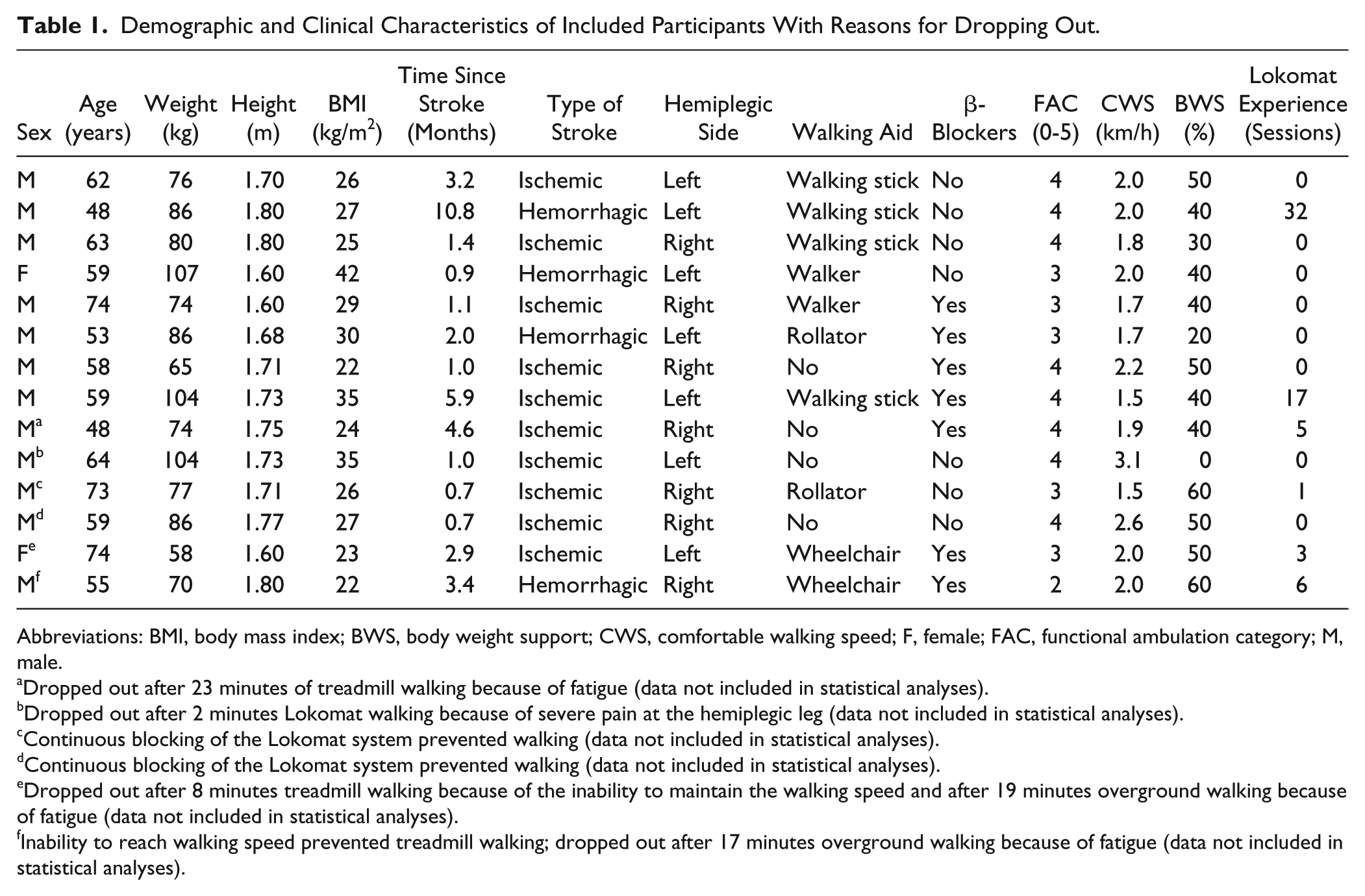
Abbreviations: BMI, body mass index; BWS, body weight support; CWS, comfortable walking speed; F, female; FAC, functional ambulation category; M, male.
Dropped out after 23 minutes of treadmill walking because of fatigue (data not included in statistical analyses).
Dropped out after 2 minutes Lokomat walking because of severe pain at the hemiplegic leg (data not included in statistical analyses).
Continuous blocking of the Lokomat system prevented walking (data not included in statistical analyses).
Continuous blocking of the Lokomat system prevented walking (data not included in statistical analyses).
Dropped out after 8 minutes treadmill walking because of the inability to maintain the walking speed and after 19 minutes overground walking because of fatigue (data not included in statistical analyses).
Inability to reach walking speed prevented treadmill walking; dropped out after 17 minutes overground walking because of fatigue (data not included in statistical analyses).
Participants (12 male and 2 female) were between 48 and 74 years old (median: 59 years) and 1 to 11 months after stroke (median: 1.7 months). Eight participants walked independently on level surfaces (FAC 4); 5 required verbal supervision or stand-by help (FAC 3); and 1 needed support of a person for balance and coordination (FAC 2). Participants walked at a median CWS of 2.0 km/h in combination with a median BWS of 40%. Six participants previously walked in the Lokomat (1 to 32 sessions).
Effect of Walking Condition and Duration on Physiological Responses and Perceived Exertion
Because of listwise deletion, we could only include data of 8 participants. Table 2 describes the descriptive statistics for each outcome.
Physiological Responses and Perceived Exertion During Lokomat, Treadmill, and Overground Walking. a
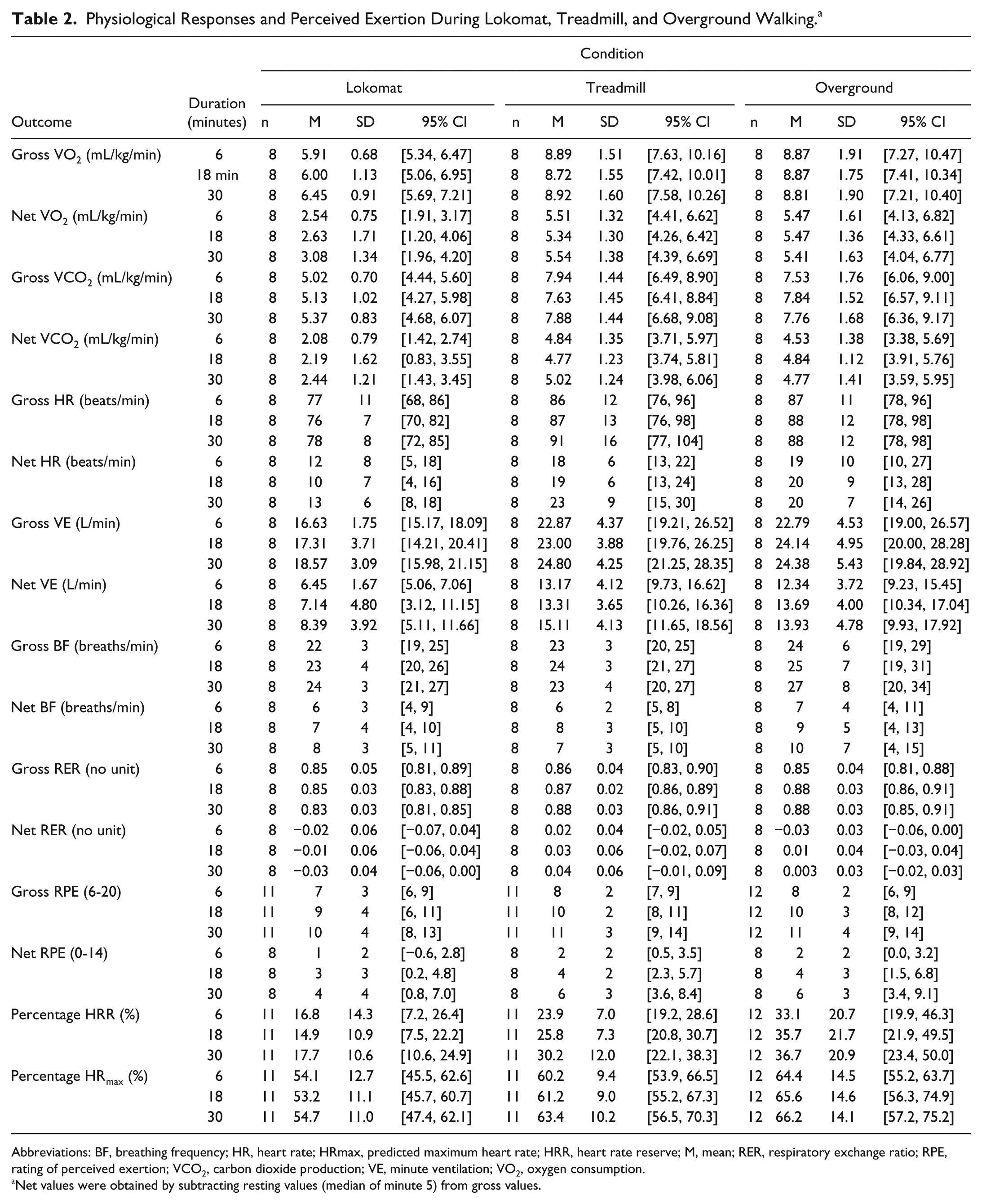
Abbreviations: BF, breathing frequency; HR, heart rate; HRmax, predicted maximum heart rate; HRR, heart rate reserve; M, mean; RER, respiratory exchange ratio; RPE, rating of perceived exertion; VCO2, carbon dioxide production; VE, minute ventilation; VO2, oxygen consumption.
Net values were obtained by subtracting resting values (median of minute 5) from gross values.
We found no significant interaction effects between condition and duration, except for net respiratory exchange ratio; the magnitude of the effect was small (Supplementary Material 1, available online). Post hoc tests indicated that net respiratory exchange ratio significantly increased between 6 and 18 minutes and between 6 and 30 minutes overground walking; the magnitudes of the effects were large (Supplementary Material 2, available online). No significant changes were found during Lokomat and treadmill walking.
The main effect of condition was significant for net oxygen consumption, net carbon dioxide production, net heart rate, and net minute ventilation; the magnitudes of the effects were large (Supplementary Material 1, available online). Post hoc tests showed that net oxygen consumption, net carbon dioxide production, net heart rate, and net minute ventilation were significantly lower during Lokomat walking compared with treadmill and overground walking. The magnitudes of the effects were large. No significant differences were found between treadmill and overground walking (Supplementary Material 3, available online).
The main effect of duration was significant for net heart rate, net minute ventilation, net breathing frequency, and net rating of perceived exertion; the magnitudes of the effects were small to large (Supplementary Material 1, available online). Post hoc tests showed that net heart rate significantly increased between 18 and 30 minutes; net minute ventilation significantly increased between 6 and 30 minutes, and between 18 and 30 minutes; and net breathing frequency significantly increased between 6 and 18 minutes, and between 6 and 30 minutes. The magnitudes of the effects were small. Net rating of perceived exertion significantly increased between each duration; the magnitude of the effect was large (Supplementary Material 4, available online). Figure 2 illustrates these results.
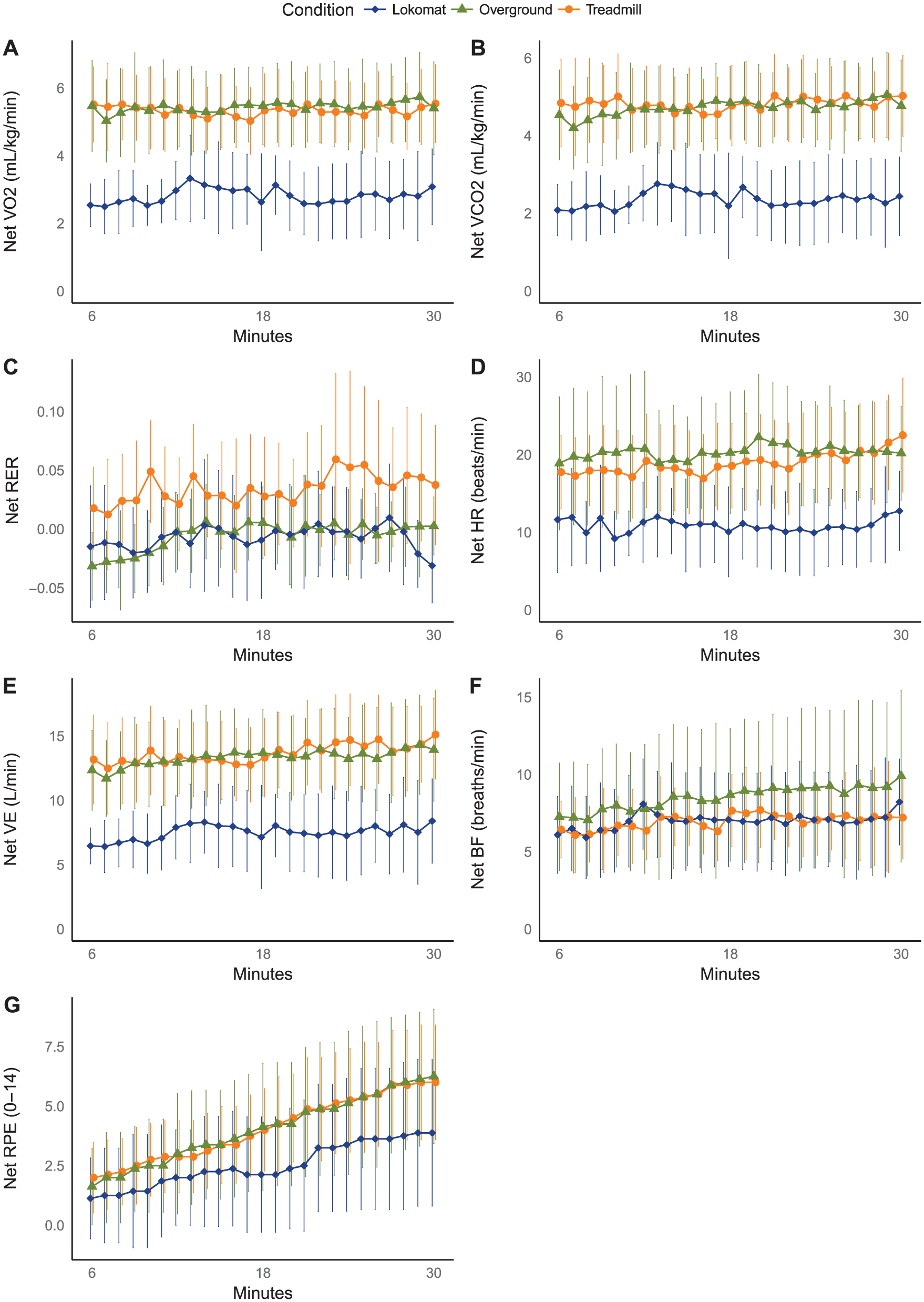
Net physiological responses and perceived exertion during 30-minute Lokomat, treadmill, and overground training. Means and 95% CIs are plotted (n = 8).
Comparison With Aerobic Training Recommendations
Lokomat Walking
Throughout Lokomat walking, mean percentage of heart rate reserve was significantly below the minimum threshold for aerobic exercise, whereas mean percentage of predicted maximum heart rate was at the lower border. Mean gross rating of perceived exertion increased toward the aerobic target zone by the end (Figure 3; Supplementary Material 5 available online).
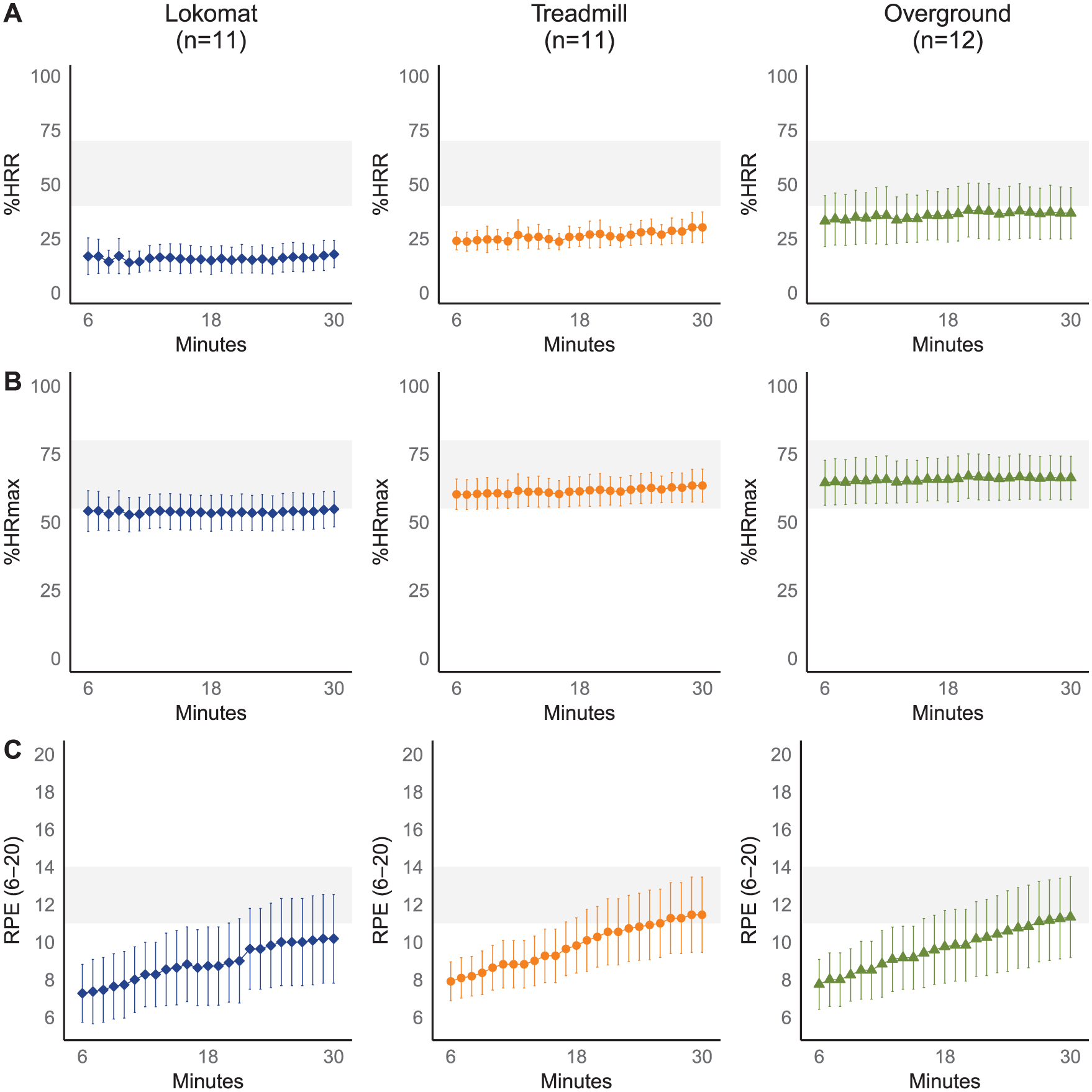
Exercise intensity of Lokomat, treadmill, and overground training compared with aerobic training recommendations for stroke survivors. Means and 95% CIs are plotted as well as aerobic training recommendations (gray zones).
Treadmill Walking
Throughout treadmill walking, mean percentage of predicted maximum heart rate fell within the aerobic target zone, and mean percentage of heart rate reserve was below the minimum threshold. Halfway to the end, mean gross rating of perceived exertion increased toward the aerobic target zone (Figure 3; Supplementary material 5, available online).
Overground Walking
From the beginning to the end, mean percentage of predicted maximum heart rate fell within the aerobic target zone, whereas mean percentage of predicted heart rate reserve was at the lower border. Perceived exertion increased during overground walking and reached aerobic guidelines halfway to the end (Figure 3; Supplementary Material 5, available online).
Discussion
This study compared physiological responses and perceived exertion between Lokomat, treadmill, and overground walking at matched speeds and levels of BWS and investigated the effect of prolonged walking duration on physiological responses and perceived exertion.
In our sample, net oxygen consumption, net carbon dioxide production, net heart rate, and net minute ventilation were about half as high during 30-minute robot-assisted gait than during 30-minute body weight–supported treadmill and overground walking. These results were in line with van Nunen et al, 22 who reported that Lokomat walking was less intensive than 6-minute unsupported overground walking with usual walking aids (patients consumed 27% less oxygen), even though patients walked much slower overground. 22 Lower physiological responses during Lokomat walking may be explained by a general reduction in muscle activity of the lower-limb muscles (both at the affected and nonaffected side), resulting in an overall reduction in active contribution. 42 Stroke survivors also consume less energy when they walk more symmetrically. 43 Lokomat walking reduces temporal asymmetry, which occurs during treadmill walking, because of a prolongation of the relative single support duration in the affected limb. 42
By the end, patients took slightly deeper breaths (MD = 1.58 L/min; P < .05) and breathed a bit faster (MD = 2 breaths/min; P < .05), somewhat demonstrating that the anaerobic metabolism supplements the ATP formation and triggers the respiratory system to remove excess carbon dioxide. However, the differences were small—clinically irrelevant—and we did not detect a significant rise in the net carbon dioxide production. The net respiratory exchange ratio slightly increased during prolonged overground walking (MD = 0.03; P < .05), somewhat indicating that less fats and more carbohydrates are being metabolized to supply the body with energy. The reason why we did not detect a rise is because the exercise intensity of body weight–supported walking (~8.9 mL/kg/min) and especially robot-assisted walking (~6.0 mL/kg/min) may have been below these patients’ anaerobic threshold. In the literature, the ventilatory threshold of patients with stroke was around 9.6 ± 0.4 mL/kg/min in subacute patients (n = 34) 44 and around 10.6 ± 2.8 mL/kg/min in chronic patients (n = 59). 45
Although our patients consumed less energy, they felt equally as tired during robot-assisted gait as during body weight–supported gait. Nevertheless, patients felt more tired when the walking duration increased. Patients perceived that walking was two and a half times more strenuous by the end. To our knowledge, only a single study investigated whether physical exertion increased with respect to the duration of overground walking after stroke (6- vs 18-minute walk). 46 Carver et al 46 demonstrated that patients with stroke were tired at the end of an 18-minute walk (shifted from very light to somewhat hard perceived exertion), but they were able to sustain their effort throughout the walk (ie, they kept their walking speed constant). 46 In our sample, we found an analogous—yet smaller—increase in perceived exertion (shift from extremely light to light perceived exertion).
Overall, the exercise intensity of Lokomat walking was below current exercise recommendations for stroke survivors—only mean percentage of maximum heart rate was at the lower bound of the minimum threshold. The exercise intensity of body weight–supported treadmill and overground walking was at the lower border or within the aerobic training zone, except for percentage of heart rate reserve during treadmill walking. This result was in line with that of van Nunen et al 22 who found a similar mean percentage of predicted heart rate reserve during Lokomat walking (22% ± 7%). 22 Although these results suggest that according to current stroke guidelines the exercise intensity of Lokomat walking is insufficient to induce an aerobic training effect, Chang et al 47 found that 2-week Lokomat training improved peak oxygen consumption by 13% in patients with subacute stroke. This discrepancy may imply that in patients with stroke, light-intensity exercise may be sufficient to induce a cardiorespiratory training effect (requiring a revision of the current exercise guidelines for stroke survivors) or that the exercise intensity of Lokomat training is currently underestimated.
Oxygen consumption and heart rate levels in our patients during Lokomat walking were within the ranges of those observed in the literature.22-24 We found somewhat lower oxygen rates than those observed by both Krewer et al 23 and van Nunen et al, 22 but in those studies, patients walked with a lower percentage of BWS (~30%). Because walking with lower loads requires less oxygen consumption, we can probably designate dissimilarities to the differences in loading.23,26 In the study of van Nunen et al, 22 patients also walked with a lower percentage of robotic guidance (~30%). 22 However, this lower percentage would probably not explain the higher oxygen rates, because lowering the robotic guidance in previous studies either left oxygen uptake unchanged or induced a decline.23,24 The walking ability of these patients, however, was a bit lower than the ability of our patients (mean FAC 2.6 vs 3.5). This may also add to the higher oxygen rates. 48 We found slightly higher oxygen rates and heart rates than those observed by Lee et al, 24 but in their study, patients walked with a fixed percentage of BWS (50%). In our study, the percentage was individually adjusted (as low as possible, with an average of 41%). Using an individual approach could make walking more intensive, whereas using a fixed percentage could provide too much support for some patients and too little for others. Another reason why we found slightly higher rates may be a result of the degree of familiarization with the Lokomat. In our study, not all patients were familiarized with the Lokomat, whereas in the study of Lee et al, 24 patients trained 3 times a week for 2 weeks prior to the experiments. 24 Sawicki and Ferris 49 demonstrated in healthy individuals that the metabolic benefit of waking with a powered ankle exoskeleton increased with practice: they found a 22% reduction in metabolic power between the beginning of the first and the end of the third session.
Future studies should further explore how robotic devices can be exploited to induce aerobic training after stroke. Currently, the highest oxygen demands have been achieved by combining higher walking speeds (1.8 km/h or higher) with lower levels of BWS (50% or lower).23,24 Nonetheless, the effect of changing the settings appears to be quite small. Stoller et al 50 were able to reach 26% higher exercise intensities (in terms of percentage of heart rate reserve) by using progressive feedback-controlled robot-assisted treadmill training rather than conventional robot-assisted treadmill training providing constant physical support by the actuated exoskeleton. The feedback-controlled approach was based on the forces applied on the exoskeleton by the participant. Participants had to keep the visualized work rate as close as possible to the target work rate by volitional muscle activity. 51 Although this study showed promising results—they found a significant overall increase in cardiorespiratory fitness after a 4-week training period early after stroke—the majority of participants (4 out of 7) in the feedback-controlled group still did not reach the aerobic threshold (ie, 40% heart rate reserve). 50 Future research should further examine the effect of variable workload and asymmetrical settings as well as overground exoskeleton walking. Current evidence is based on static robotic devices in combination with BWS systems (ie, the Lokomat and the Gait Trainer),22-26 but it is possible that the exercise intensity of walking with wearable exoskeletons—dynamic overground systems that do not provide weight reduction—may induce higher cardiometabolic demands.
This study has a couple of limitations. A first limitation is our limited sample size, which compromises the generalizability of our results—a problem that often occurs in this area of research. 20 This is not unusual because recruiting patients for studies like these is challenging. A previous study reported that it is hard to convince patients, who already face many problems and discomforts, to engage in studies requiring active participation, food restriction, breathing through a facemask, and so on. 52 Nevertheless, in future research, we should keep investing in obtaining large samples to be able to draw well-founded conclusions.
A second limitation is the possible under- or overestimation of maximum heart rate, affecting comparisons with aerobic training recommendations. Because we were unable to perform incremental exercise tests and predictions for people after stroke are not yet available, we predicted participants’ maximum heart rate based on formulas for people with heart failure and people taking β-blocking medication. Although these predictions are quite often used,22,38,39 they may be less accurate for people with stroke. Future studies should invest in validating predictions for stroke survivors. Furthermore, physiological resting values were measured pre-exercise, possibly causing excitement or stress (similar to a white-coat effect 53 ), slightly overestimating true resting values and underestimating percentages of heart rate reserve.
A third limitation is a possible discrepancy between CWS overground, on a treadmill, and in a Lokomat-system. In this study, we defined patients’ CWS during an overground walking test. This speed was used in the different walking conditions, although stroke survivors often walk faster overground than on a treadmill. 54 This discrepancy may be one reason why the Lokomat system kept blocking in one patient and data could not be used. This patient reached a high overground CWS (3.2 km/h), 54 matching the maximum Lokomat speed. During Lokomat walking, the pelvis is secured in a harness and fixed between 2 hip cushions, leading to restrictions in the amplitudes of thorax and pelvis movements.55,56 Higher walking speeds (starting between 2.7 and 3.6 km/h) have been associated with larger transverse pelvic and trunk rotations57,58—movements that are hindered in the Lokomat.
Conclusion
Our results suggest that in ambulatory stroke survivors, the oxygen and cardiorespiratory demand during robot-assisted gait with 60% robotic guidance at constant work load is considerably lower than during overground or treadmill walking at matched speeds and levels of BWS (below aerobic thresholds). To train the cardiorespiratory system, it is important that patients who can walk (with or without BWS) train without the help of robotic devices (or that settings should be done differently). Nevertheless, lower physical requirements during robot-assisted gait can enable certain patients (in our case two) to train longer. Future studies should examine how robotic devices can be exploited to meet the exercise guidelines for stroke survivors.
Footnotes
Acknowledgements
The authors would like to thank the therapists of the Rehabilitation Centre St Ursula (Herk-de-Stad, Belgium) for managing the Lokomat system and recruiting participants; Ken Janssens, Nicolas Haegeman, Laura Vander Goten, Antoine Verbeylen, Nikkie Dassen, and Sam De Buyzer for their help with data gathering; and Patricia Van de Walle and Bas De Geus for their advice on breath-by-breath gas analyses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: N.L. is a Strategic Basic Research fellow funded by the Research Foundation – Flanders (FWO).
Supplementary material for this article is available on the Neurore-habilitation & Neural Repair website along with the online version of the article.