
Abstract
Background and objective. Ambulatory subjects after stroke may benefit from gait-oriented cardiovascular fitness training, but trials to date have not primarily assessed older persons. Methods. Thirty-eight subjects (age >60 years) with residual hemiparetic gait were enrolled >6 months after stroke. Participants were randomized to receive 3 months (3×/week) progressive graded, high-intensity aerobic treadmill exercise (TAEX) or conventional care physiotherapy. Primary outcome measures were peak exercise capacity (Vo2peak) and sustained walking capacity in 6-minute walks (6MW). Secondary measures were gait velocity in 10-m walks, Berg Balance Scale, functional leg strength (5 chair-rise), self-rated mobility (Rivermead Mobility Index), and quality of life (SF-12). Results. Thirty-six participants completed the study (18 TAEX, 18 controls). TAEX but not conventional care improved Vo2peak (difference 6.4 mL/kg/min, P < .001) and 6MW (53 m, P < .001). Likewise, maximum walking speed (0.13 m/s, P = .01), balance (P < .05), and the mental subscore of the SF-12 (P < .01) improved more after TAEX. Gains in Vo2peak correlated with the degree at which training intensity could be progressed in the individual participant (P < .01). Better walking was related to progression in treadmill velocity and training duration (P < .001). Vo2peak and 6MW performances were still higher 1 year after the end of training when compared with the baseline, although endurance walking (6MW) at 1 year was lower than immediately after training (P < .01). Conclusion. This trial demonstrates that TAEX effectively improves cardiovascular fitness and gait in persons with chronic stroke.
Introduction
Gait impairment is a major determinant of disability after stroke. At least 1 of 2 stroke survivors suffers from persistent hemiparetic gait deficits resulting in reduced mobility.1,2 Reduced mobility leads to a decrease in cardiorespiratory fitness3,4 in an already unfit elderly population.5,6 Low fitness further perpetuates the reduction in mobility considering that hemiparetic gait requires 55% to 100% more energy than normal gait. 7 Immobility-related deconditioning also promotes cardiovascular risk,8,9 placing the stroke survivor in a vicious cycle of worsening cardiovascular risk furthering disability.
Interventions to improve cardiorespiratory fitness are still not part of routine neurorehabilitation programs in many rehabilitation centers, and therapy is often dominated by standard rehabilitative therapies based on neurodevelopmental principles such as the Bobath concept. These standard therapies are an insufficient stimulus to increase fitness levels after stroke.10,11 Indeed, exercise is often considered unsafe, especially for the elderly patient. Several studies and meta-analyses investigating physical fitness interventions, such as circuit class training, cycling exercise, and water-based exercises, demonstrated beneficial effects on cardiovascular fitness and walking performance in all phases after stroke.12-16
Aerobic treadmill exercise (TAEX) also has been proposed as a promising, task-oriented intervention to improve gait and cardiovascular fitness. TAEX is simple and safe. 17 A Cochrane Review reported no benefits of treadmill training in acute and chronic stroke. 18 But only the trial of Macko et al involved progressive aerobic training of sufficient intensity to improve cardiorespiratory fitness and used fitness as the outcome measure. 17 According to the guidelines of the American College of Sports Medicine, first adaptations of the cardiovascular system are expected after 2 to 6 weeks of training. In addition, an adaptation period of several weeks is recommended for untrained subjects. 19 Thus, a training period less than 6 weeks is probably insufficient.
This randomized controlled trial was designed to test the efficacy of aerobic treadmill exercise (TAEX) in chronic stroke survivors aged 60 years and older compared with conventional care physiotherapy according to the standard prescription in Germany (1-3 sessions per week). After following their conventional care prescription for 3 months, the control group crossed over to TAEX (TAEX-cross). Their TAEX protocol was different from the protocol of the TAEX group: inclination of the treadmill was added. Walking with inclination has been suggested to render hemiparetic gait on a treadmill more symmetrical. 20 Our hypothesis was that TAEX would improve sustained walking capacity and cardiovascular fitness out to a 1 year follow-up.
Material and Methods
Study Participants
Chronic stroke survivors >60 years with residual hemiparetic gait were enrolled >6 months after stroke. Subjects were recruited via local newspapers in the area of Stuttgart, Germany.
All subjects received a screening assessment including medical history, physical examination, resting electrocardiogram, a customized exercise stress test, 17 blood chemistry and counts, the National Institute of Health Stroke Scale, and Center for Epidemiological Studies Depression Scale (CES-D). 21 Cerebral computed tomography and/or magnetic resonance imaging scans were available for all participants. The presence of a lesion on imaging was used to affirm the diagnosis of ischemic stroke. Lesion location was used for stratification in the randomization procedure into cortical (territorial lesions in the territory of the middle cerebral artery [MCA]) versus subcortical (lacunar) infarctions.
Inclusion criteria were hemiparetic gait as evaluated by a neurologist with at least 1 clinical sign for paresis, spasticity or circumduction of the affected leg while walking, and the ability to walk on the treadmill at ≥0.3 km/h for 3 minutes with handrail support. Exclusions were made for unstable angina pectoris, heart failure (New York Health Association > II°), hemodynamically significant valvular dysfunction, peripheral arterial occlusive disease, dementia (Mini Mental State Examination < 20), aphasia (unable to follow 2 commands), major depression (CES-D > 16), and other medical conditions precluding participation in aerobic exercise, 22 as well as patients already performing aerobic exercise training for >20 min/d and >1 d/wk.
The study protocol was approved by the ethics committee of the University of Tuebingen, Germany. All subjects provided written informed consent. The trial was registered at www.clinicaltrials.gov (NCT00614224).
Study Design
A randomized controlled design was used comparing the effects of 3 months (39 sessions) TAEX with usual care physiotherapy (control) according to the typical German prescription (1-3 sessions/week). All participants were assessed in primary and secondary outcome measures before and after the intervention period. The control group then crossed over to receive 3 months of treadmill exercise using a modified protocol (see below) and retested after finishing this program. To assess retention of treatment effects, participants were reassessed regarding cardiovascular fitness, walking function, and functional leg strength 1 year after completion of training. The follow-up period included no standardized training program. Subjects were simply taught to stay active.
Baseline and endpoint investigations at 3 months (posttraining) and follow-up examination at 12 months were conducted by the same therapist (JC) under supervision of a physician (CG). Both examiners were independent for treatment allocation.
Randomization
Randomization was performed using a stratified block allocation scheme (variable block size from 12 to 14 subjects, 3 blocks, allocation ratio 1:1). A computer-based pseudorandom number generator and the Moses–Oakford assignment algorithm were used to develop the randomization schedule. 23 The procedure was performed by study-independent staff at the Department of Biostatistics, University of Ulm, Germany. Randomization was stratified based on age (<68 vs ≥68 years) and cortical versus subcortical infarctions.24-26 Walking speed was not included because it did not predict response to aerobic treadmill training in previous studies.17,27
Assessments
Exercise testing
Determination of peak Vo 2 is a reliable measure of cardiovascular fitness after stroke. 6 A treadmill exercise test at maximum effort with open circuit spiroergometry under continuous monitoring of vital signs and electrocardiogram was conducted to obtain peak Vo 2 values by using a modified Balke protocol (constant treadmill velocity adjusted to 60% to 70% of comfortable walking speed in 10-m test and increase of incline by 2% every 2 minutes until maximum effort). The test was terminated on patient request, if gait instability was observed, or according to the guidelines of the American Heart Association (AHA). 22
Outcomes
Cardiorespiratory fitness as measured in peak Vo 2 during maximum effort treadmill walking was a primary endpoint. Sustained walking ability measured in 6-minute walks28-30 was another primary outcome measure. Secondary outcomes included 10-m timed walks (10mW) performed at comfortable (self-selected) and maximum walking speeds to determine gait velocity for short distances as required for home-based mobility. Another secondary outcome was a measure of functional leg strength, the 5-Chair-Rise (5CR) test. 31 Subjects were asked to rise from a chair 5 times as fast as possible. The test was conducted twice and the fastest performance analyzed. The Berg Balance Scale quantified balance during stance and gait.32,33 Further secondary outcomes were self-rated mobility and activities for daily living function assessed by the Rivermead Mobility Index (RMI) 34 and physical and mental health measured by the Medical Outcomes Study Short-Form 12 (SF-12).35,36
Treadmill Training
Treadmill training (TAEX) consisted of 39 sessions (3×/week; 3 months) supervised by a physician and/or physiotherapist in an outpatient rehabilitation center. The goal was to achieve 30 to 50 minutes of training (beginning with 10-20 minutes) at 60% to 80% of the maximum heart rate reserve (HRR) (starting with 40% to 50% HRR) determined according to the formula of Karvonen (Training HR = intensity factor (%) × [HRmax − HRrest] + HRrest). HRmax was defined as peak heart rate obtained from the maximum effort treadmill exercise test performed before training. These training intensities were chosen according to the recommendations of the AHA 22 and on the experience of former trials. 17 Nevertheless, with regard to several limitations on heart rate–based training (eg, beta-blocker medication, arrhythmia), intensity of training was additionally monitored by ratings of perceived exertion (Borg Scale 37 ). Duration was increased as tolerated by 1 to 5 min/wk, and treadmill speed was progressed by 0.1 to 0.3 km/h every 1 to 2 weeks. The progression of each protocol was determined by the trainer, adjusted for individual capability. Treadmill inclination remained at 0°. Subjects were allowed to use the handrail or forearm support while being encouraged to walk without support if possible. Hip protection devices were used in subjects with poor balance and osteoporosis. Participants with silent, reversible myocardial ischemia in peak exercise testing were enrolled if their primary physicians and cardiologist approved the intervention. These subjects were trained at intensities below their myocardial ischemia level similar to cardiac rehabilitation protocols. 22 Training was carried out as a group intervention with subjects being trained on 3 treadmills in parallel. Interruption to a maximum of 3 consecutive training sessions was allowed. Missed sessions—the maximum was 6—were added at the end.
Participants initially assigned to the control group crossed over to TAEX (TAEX-cross). They were trained using a slightly modified protocol. Because Werner et al 20 proposed that walking on a treadmill at moderate inclination (2% to 8%) promotes gait symmetry in hemiparetic subjects, TAEX-cross subjects were trained at an inclination of 2%. Target training duration and intensity were the same as for the TAEX group. Participants were allowed to obtain prescribed therapy sessions during the study, if therapy did not comprise training elements for the lower extremities or cardiorespiratory fitness (eg, isolated arm training or speech therapy).
Conventional Care Physiotherapy
Conventional care physiotherapy included passive, muscle tone–regulating exercises for the upper and lower extremities with elements of balance training conducted on an outpatient basis in physiotherapy practices or rehabilitation centers. No aerobic fitness training was performed. Duration of therapy sessions was 1 hour for 1 to 3 times per week as prescribed by the primary physician or neurologist over 3 months (13 weeks). The exposure to training was less in controls than in TAEX patients; therefore, the control intervention cannot be considered as an attention control.
Statistics
A priori power analysis was based on our previous trials17,27 and required 15 subjects per group to detect a significant (P < .05) difference between groups in Vo 2peak (a difference of 2.4 mL/kg/min) with a power of 0.8. For comparisons in clinical and demographic baseline characteristics between-groups Mann–Whitney U test was applied for ordinal variables and Fisher exact test for nominal variables. For the between-groups comparison of outcomes, analyses of variance were used with the change in the outcome variables across time (difference post–pre) as the independent variable. Analyses were carried out “per protocol” as well as “intention to treat” (last observation carried forward) for primary outcomes. Independent variables included group and the baseline value of the respective dependent variable as a covariate. Shapiro–Wilk tests were used to test for normal distribution of the difference measures. The changes in outcome measures over the periods of conventional care versus TAEX-cross were compared within the group using paired t tests. Treatment effects of standard TAEX and TAEX-cross were compared by t tests. Pearson correlation coefficients were computed to assess the relationship between adaptation of training parameters over 3 months TAEX (progression of treadmill velocity, training duration, and %HRR) and improvement in outcome measures. Retention at follow-up was assessed for all participants combining TAEX and TAEX-cross groups. Paired t tests were used to compare performance at 1 year to baseline or posttraining performance. Peak Vo 2 values were corrected for body mass (mL/kg/min). Data are expressed as mean ± standard deviation. A 2-tailed P < .05 was considered significant.
Results
The numbers of subjects screened, enrolled (79% of clinically screened subjects), randomized, and completing the trial are shown in Figure 1. There were no significant differences in demographic variables, clinical characteristics (Table 1), and performance measures at baseline between the TAEX and control groups (Table 2). Male subjects were more likely to respond to the study advertisements (about 80% of all telephone calls) and participate in the trial (82% of screened subjects) when compared with female subjects. 38 The mean age was 68.6 ± 6.3 years in both groups with a range from 60 to 84 years. Eleven participants (29%) were 70 to 80 years and 3 subjects were ≥80 years old (8.3%).
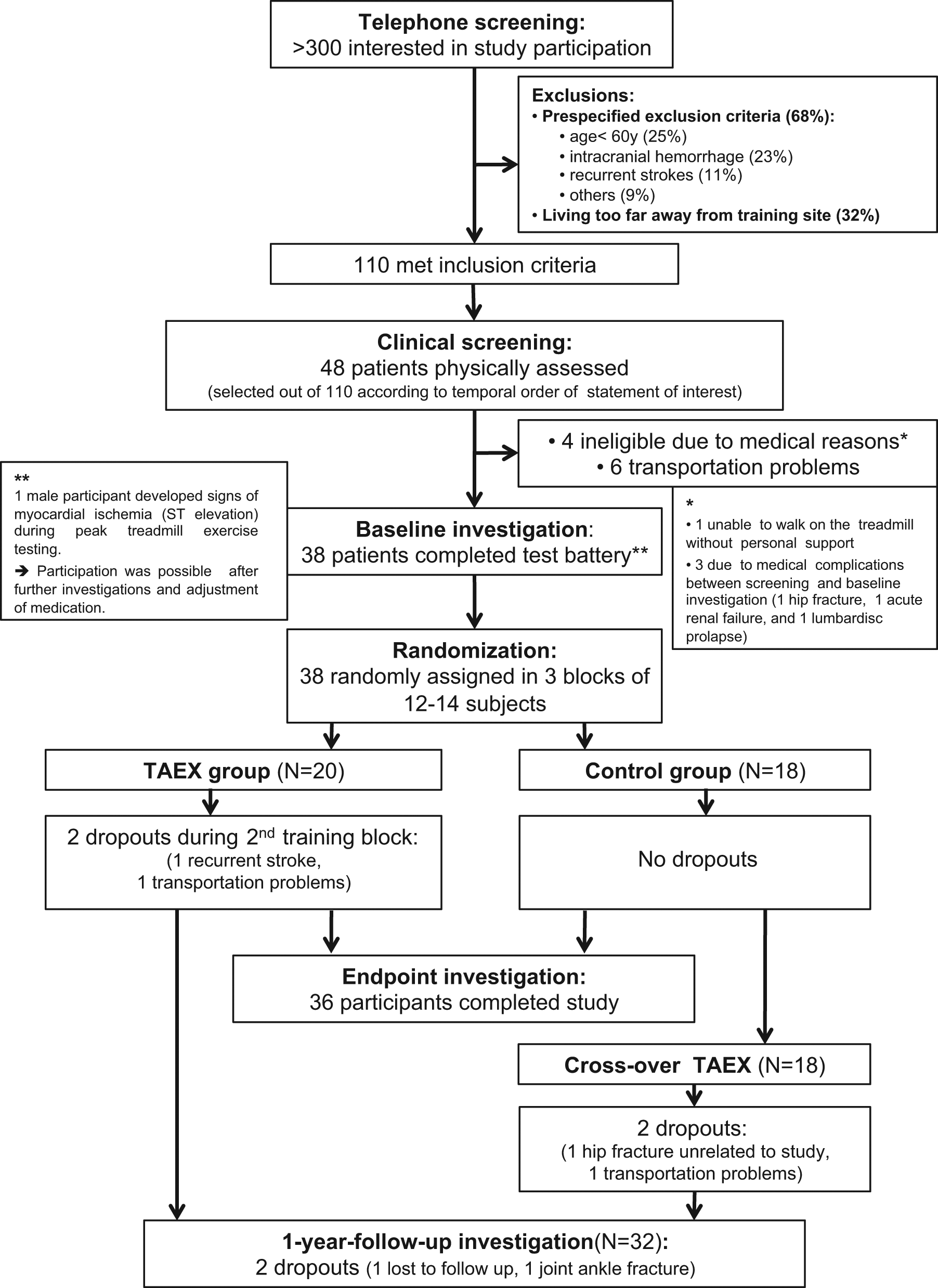
Flow of subjects through the study. Telephone screening was conducted with all individuals (patients or family members) responding to advertisements. A total of 110 stroke survivors were deemed eligible and considered for clinical screening. For constraints of trial time and training capacity, only 48 individuals (in the order they responded to advertisements) were assessed. Ten had to be excluded for medical or logistic reasons. Hence, 48 were randomized to TAEX or control. There were 2 dropouts during TAEX training, leaving 36 patients for the endpoint comparisons. Control patients then crossed over to exercise training with 2 dropping out during training. All subjects were assessed 1 year after the beginning of the trial except 2: 1 lost to follow-up and 1 with ankle fracture.
Demographic and Clinical Baseline Characteristics
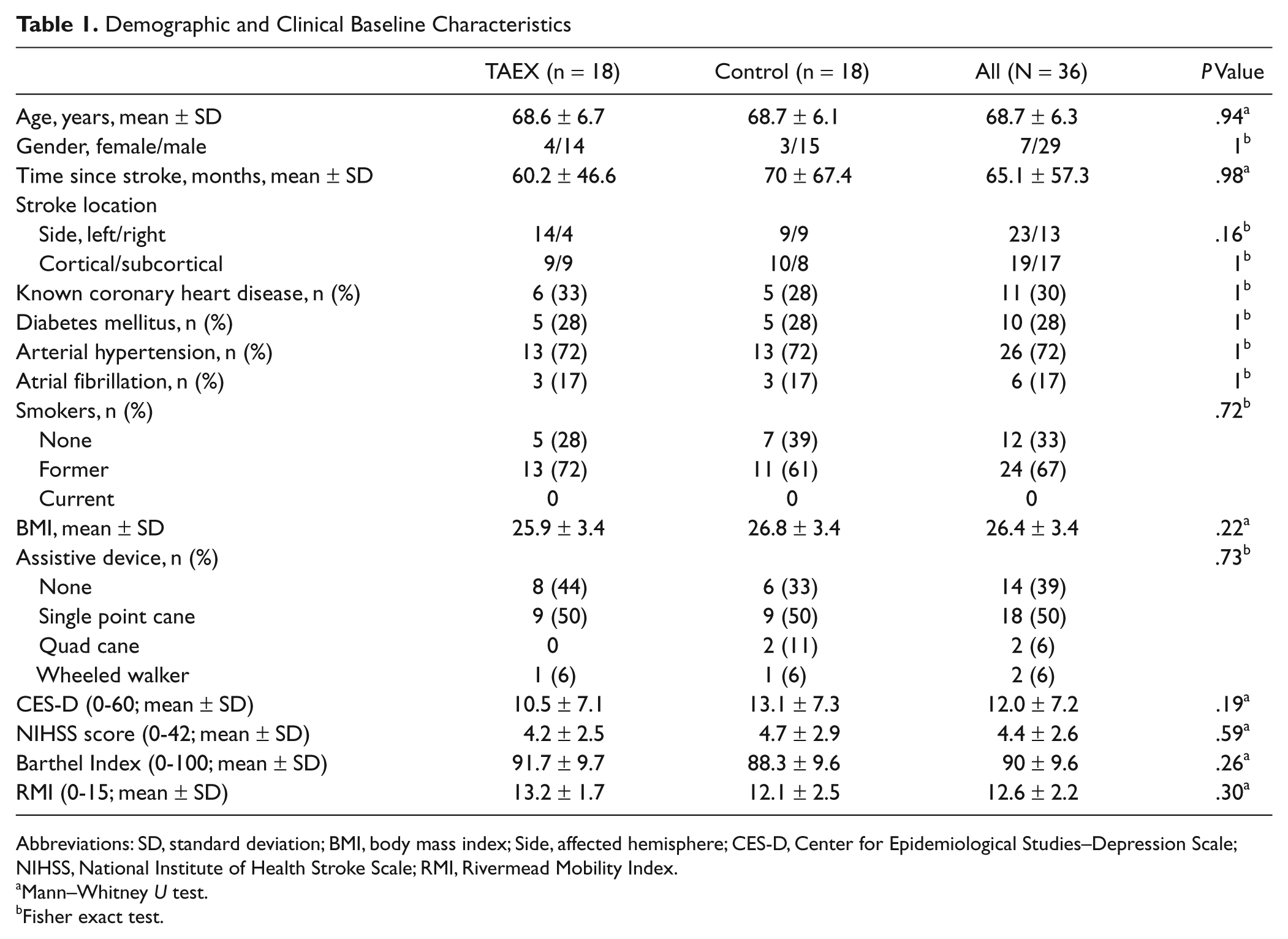
Abbreviations: SD, standard deviation; BMI, body mass index; Side, affected hemisphere; CES-D, Center for Epidemiological Studies–Depression Scale; NIHSS, National Institute of Health Stroke Scale; RMI, Rivermead Mobility Index.
Mann–Whitney U test.
Fisher exact test.
Therapy effects in Aerobic Treadmill Exercise Group (TAEX) and Control Group a
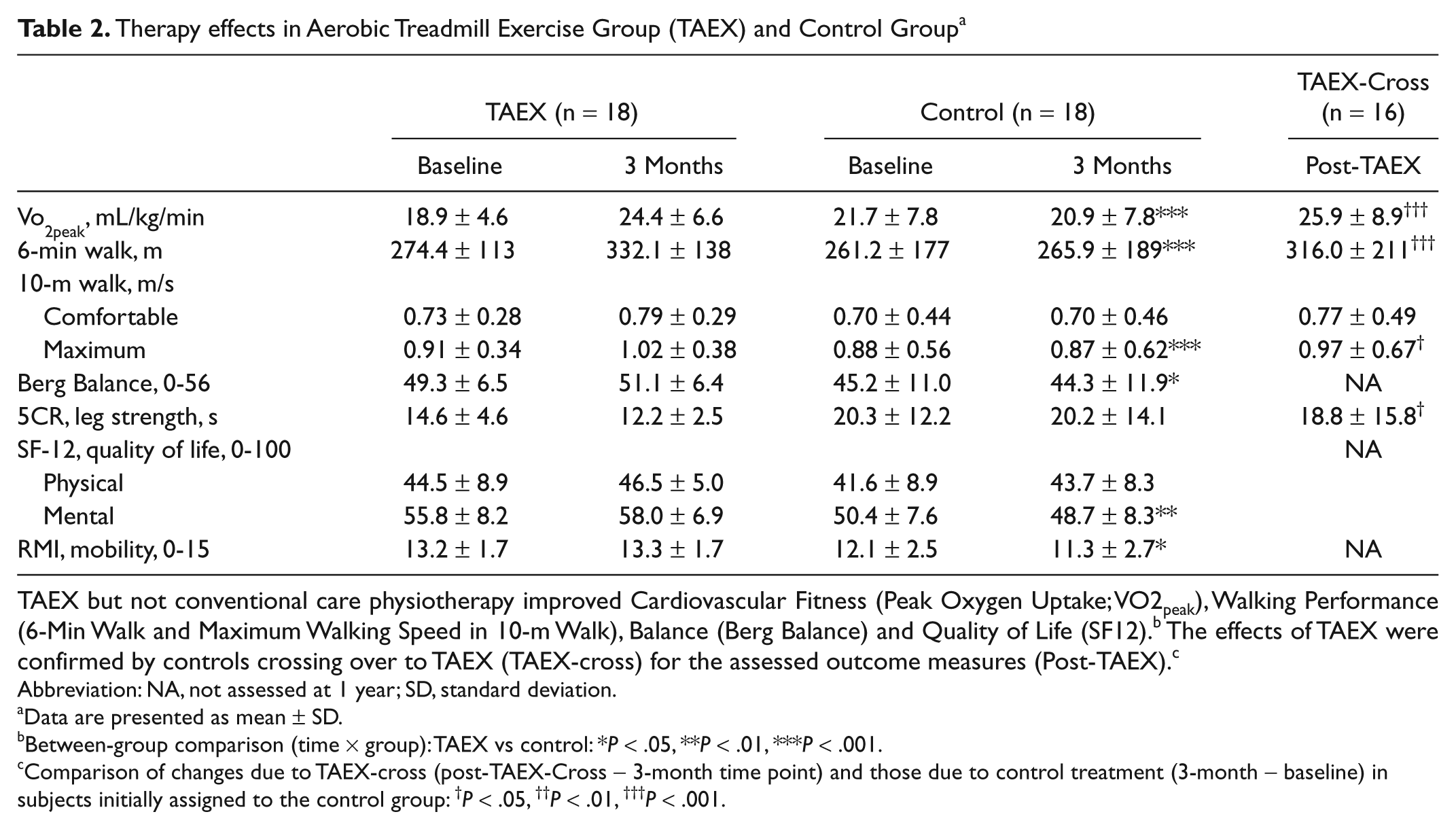
TAEX but not conventional care physiotherapy improved Cardiovascular Fitness (Peak Oxygen Uptake; VO2peak), Walking Performance (6-Min Walk and Maximum Walking Speed in 10-m Walk), Balance (Berg Balance) and Quality of Life (SF12). b The effects of TAEX were confirmed by controls crossing over to TAEX (TAEX-cross) for the assessed outcome measures (Post-TAEX). c
Abbreviation: NA, not assessed at 1 year; SD, standard deviation.
Data are presented as mean ± SD.
Between-group comparison (time × group): TAEX vs control: *P < .05, **P < .01, ***P < .001.
Comparison of changes due to TAEX-cross (post-TAEX-Cross − 3-month time point) and those due to control treatment (3-month − baseline) in subjects initially assigned to the control group: †P < .05, ††P < .01, †††P < .001.
Training Data
All subjects tolerated the training and seemed satisfied with the therapy as determined by informal interviews. All participants of the TAEX group completed 39 sessions. The mean duration of therapy was 13.2 ± 0.3 weeks and 13.1 ± 0.3 weeks for TAEX and control, respectively. One male participant showed signs of silent myocardial ischemia in initial peak exercise testing but was able to enter the study after consultation of his cardiologist. This man was trained below his myocardial ischemia level, which was again tested after 4 and 8 weeks, and thus allowed further adjustment of training intensity. One participant complained of hip pain due to activated arthritis after 4 weeks of training, which improved after transient reduction of training intensity without interruption. No study-related serious adverse events occurred. Two falls without injury were observed.
Training duration progressed from 16.1 ± 4.4 to 39.4 ± 8.6 minutes at 3 months and training velocity from 0.52 ± 0.22 to 1.01 ± 0.38 m/s. Progression of training velocity and duration led to an increase in HRR from 48.9 ± 11.8% at baseline to 76.7 ± 13.9% HRR. Control subjects received conventional physiotherapy as prescribed by the primary physician, averaging 1.8 ± 1.1 h/wk or 2 ± 0.6 times/week.
In TAEX-cross, training duration increased from 15.9 ± 5.8 to 37.6 ± 13.5 minutes and treadmill velocity from 0.55 ± 0.37 to 0.82 ± 0.45 m/s at an incline of 2%. HRR increased from 53.4 ± 18% (mean training heart rate 103 ± 20.9 bpm) to 72.3 ± 15.2% (heart rate 115 ± 20.6 bpm) at 3 months.
Primary Outcomes
Body mass–adjusted Vo 2 peak improved by 5.5 ± 1.0 mL/kg/min in TAEX and nonsignificantly deteriorated in controls (−0.8 ± 0.8 mL/kg/min). This change was significantly different between groups (per-protocol analysis: P < .001 [Table 2 and Figure 2], intention-to-treat analysis: P < .001). The distance walked in 6MW increased in TAEX by 57.7 ± 44.6 m and in controls by 4.7 ± 5.9 m (between group effect: P < .001 for both per-protocol and intention-to-treat analysis).
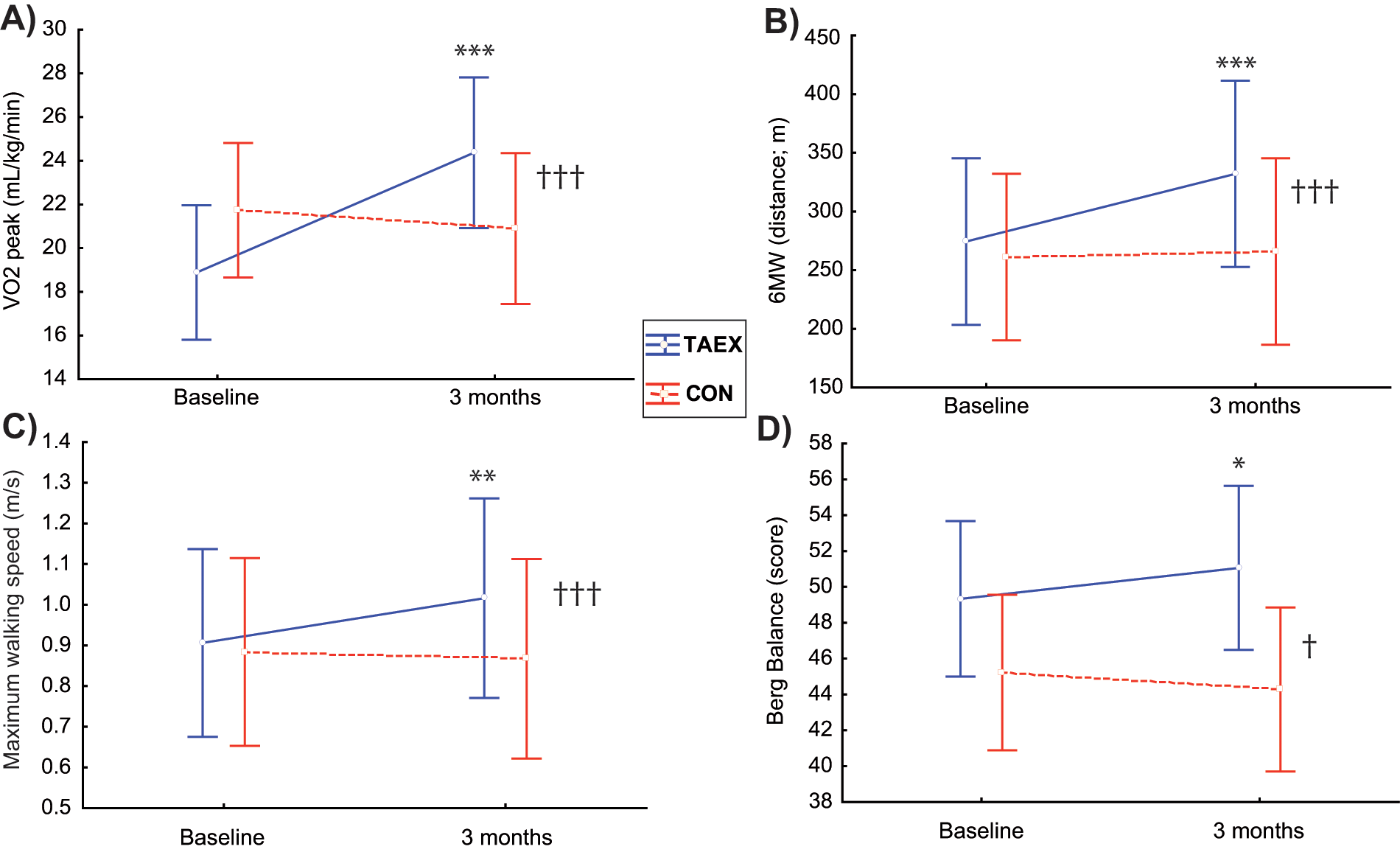
Effects of 3 months TAEX compared with conventional physiotherapy. Effects of 3 months TAEX compared with conventional physiotherapy (control) on cardiovascular fitness (A: Vo2 peak), walking parameters (B: 6 minute walk, C: maximum walking speed in 10-m timed walks), and balance (D: Berg Balance scale). Within-group comparison (paired t): *P < .05, **P < .01, ***P < .001. Between-group comparison (time × group): †P < .05, ††P < .01, †††P < .001.
Secondary Outcomes
Maximum walking speed in 10MW increased in the TAEX group by 0.12 ± 0.12 m/s and decreased nonsignificantly in controls (−0.02 ± 0.02 m/s). The between-groups difference was highly significant (P < .001). Comfortable walking speed improved in TAEX by 0.07 ± 0.02 m/s and remained largely unchanged in controls (0.0 ± 0.02 m/s), but the between-groups difference only showed a statistical trend (P = .07). The Berg Balance Scale improved by 1.7 ± 3 points in TAEX and decreased in controls (−0.9 ± 3.2; time × group interaction: P = .02; Table 2 and Figure 2). 5CR as a measure of functional leg strength improved in TAEX subjects by 2.4 ± 0.9 s and in controls by 0.1 ± 0.9 s (P = .11; Table 2).
RMI improved in TAEX (13.2 ± 1.7 to 13.3 ± 1.7) and declined in controls (12.1 ± 2.5 to 11.3 ± 2.5), rendering both groups significantly different (P = .02). The RMI had a ceiling effect: 11 TAEX subjects (61%) and 10 controls (56%) had scores ≥14 (maximum = 15 points). TAEX improved mental subscores of the SF-12 (2.2 ± 1.2 points) more than conventional care physiotherapy (−1.8 ± 1.5; between-groups difference: P = .006). Other subscores of the SF-12 did not differ (Table 2).
Crossover TAEX
When compared with TAEX, the progression of treadmill velocity was slower in TAEX-cross subjects (P = .006). There were no significant differences in the progression of training duration (P = .45) or aerobic intensity (P = .26).
Within-subject comparisons of changes in outcome parameters between conventional physiotherapy and TAEX-cross revealed significant benefits from TAEX-cross. Cardiovascular fitness improved by 4.4 ± 3.9 mL/kg/min (control period: −1.2 ± 1.5 mL/kg/min, P < .0001). TAEX-cross increased 6MW performance by 57.7 ± 44.6 m (control period: 4.6 ± 5.8 m; P < .001). Maximum gait speed over 10 m improved by +0.07 ± 0.11 m/s after TAEX-cross but had declined during the control period (0.02 ± 0.03 m/s, P = .01), comfortable walking improved by 0.04 ± 0.08 m/s after TAEX-cross (control period: 0.0 ± 0.04 m/s, P = .28) and functional leg strength in 5CR by −2.9 ± 4.0 s (control period: 0.2 ± 1.6 s; P = .04). When compared with the TAEX without inclination (TAEX group), TAEX-cross with 2% inclination produced comparable gains in outcome measures (10MW, comfortable speed: P = .41; 10MW, maximum speed: P = .35; 6MW: P = .14; 5CR, leg strength: P = .73; Vo 2peak: P = .44, Table 2).
Predictors of Therapy Response
Gains in walking velocity were larger with greater progression of treadmill speed and training duration (combined analysis of TAEX and TAEX-cross over subjects, n = 34). This association was observed for maximum gait speed in 10MW (with progression of treadmill speed: r2 = .23, P = .004; and duration: r2 = .37, P < .001) as well as for 6MW (speed: r2 = .52, P < .001; duration: r2 = .28, P = .001; Figure 3). Improvements in fitness gains, however, were not related to progression of treadmill speed (r2 = .01, P = .54) and duration (r2 = .004, P = .74).
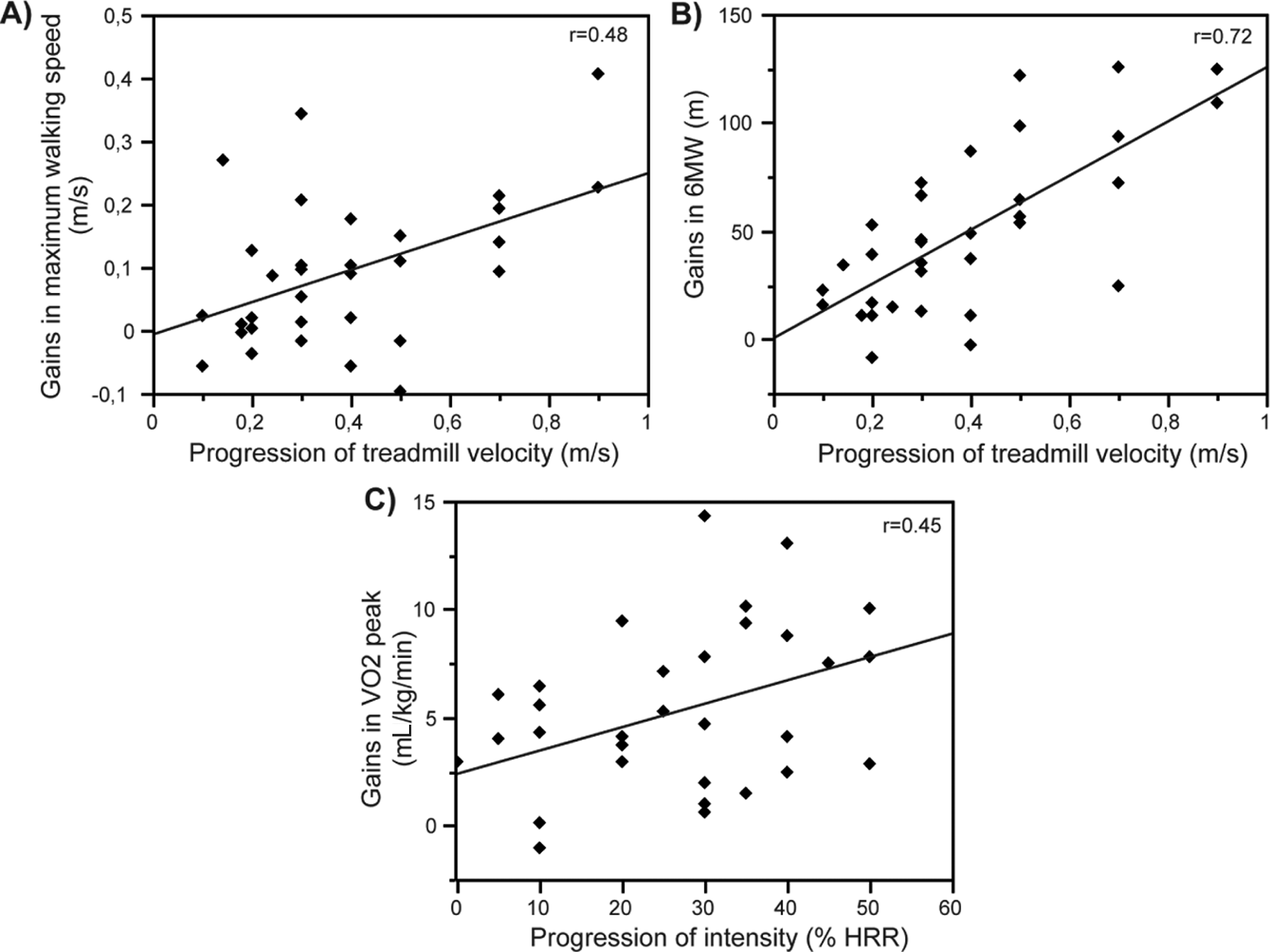
Adaptation of training parameters as predictors of therapy response, The degree of progression of treadmill velocity during the 3-month training period correlated with gains in maximum walking speed (A) and 6-minute walk (6MW; B). The degree of progression of training intensity (%HRR) was associated with gains in cardiovascular fitness (Vo2peak, C).
Cardiorespiratory fitness gains were related to the amount of heart rate increase achieved during training (r2 = .2, P = .008). Conversely, training intensity was unrelated to gains in maximum walking velocity in 10MW (r2 = .01, P = .53; Figure 3). Training intensity showed a trend for a correlation with gains in sustained walking ability in the 6MW, the performance of which requires both gait and fitness (r2 = .11, P = .05). Age and the time interval between the stroke and study enrollment did not affect therapy response.
Maintenance of Treatment Effects
One-year follow-up data were available for 32 participants (18 TAEX and 14 TAEX-cross, Figure 1). For technical and logistical reasons, Vo2peak was only available in 23 participants. Nine participants continued treadmill training once or twice per week in local sport clubs. The remaining participants did not continue any aerobic exercise. Compared with baseline, Vo 2peak (P = .04), 6MW (P < .001), and walking velocity in 10-m timed walks (comfortable: P = .01, maximum: P < .001) were still significantly increased at the time of follow-up. 5CR performance was not different from baseline (P = .07). Compared with posttraining, performance Vo2peak (P = .24), comfortable (P = .8), and maximum gait speed in 10MW (P = .25) were not different at follow-up. 6MW distance was significantly shorter (P = .002; Table 3). A comparison of the maintenance of therapy effects between those participants continuing treadmill training (n = 9) with those who did not (n = 23) revealed significantly better performance for the treadmill continuers (change in distance: 0.2 vs −23.6 m; P < .05) and in trend for Vo2peak (1.5 ± 8.0 mL/kg/min [n = 8] vs −3.5 ± 4.1 mL/kg/min [n=14]; P = .1) and maximum walking speed (0.02 ± 0.07 vs −0.03 ± 0.08 m/s; P = .01).
One-Year Follow-up Performance of TAEX-Trained Participants (TAEX and TAEX-Cross; n = 32)
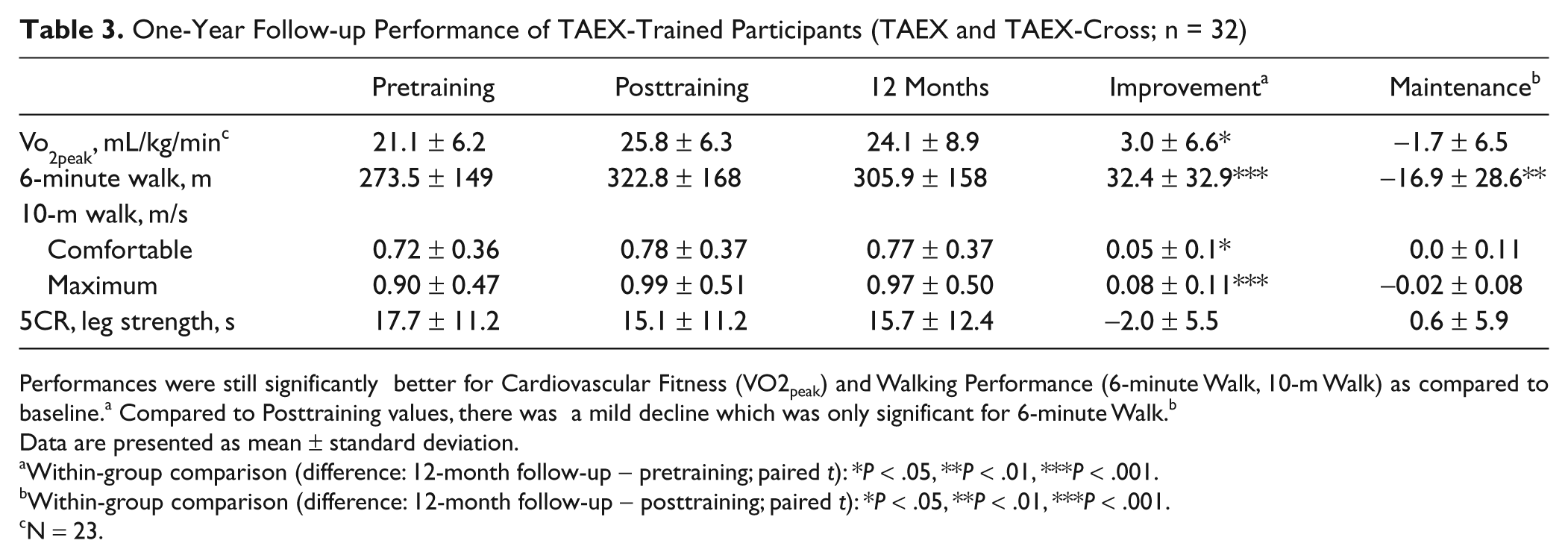
Performances were still significantly better for Cardiovascular Fitness (VO2peak) and Walking Performance (6-minute Walk, 10-m Walk) as compared to baseline. a Compared to Posttraining values, there was a mild decline which was only significant for 6-minute Walk. b
Data are presented as mean ± standard deviation.
Within-group comparison (difference: 12-month follow-up − pretraining; paired t): *P < .05, **P < .01, ***P < .001.
Within-group comparison (difference: 12-month follow-up − posttraining; paired t): *P < .05, **P < .01, ***P < .001.
N = 23.
Discussion
This randomized controlled trial demonstrates, in a stroke population aged 60 years and older with mild chronic disability, that 3 months of progressive aerobic treadmill exercise, compared with conventional care physiotherapy, leads to clinically relevant benefits in cardiovascular fitness and walking endurance, as well as statistically significant improvements in maximum gait speed, balance, self-rated functional mobility, and quality of life. Cardiorespiratory fitness improved from a mean of 18.9 to 24.4 mL/kg/min (+5.5 mL/kg/min; increase of 30%), which is clinically relevant. The range of required oxygen uptake (Vo 2) for most basic activities of daily living falls between 10 and 17.5 mL/kg/min for nondisabled elderly persons and is probably even higher in persons with physical compromise. 39 Thus, at baseline our sample was just at a level of fitness, at which daily life activities lead to exhaustion. Likewise, improvement of 50 m and more in the 6MW is regarded as clinically relevant in cardiac and pulmonary rehabilitation. 40 Reference data do not exist for those with stroke, but the threshold of clinical relevance is likely to be lower due to impaired mobility. Thus, the improvements observed here (58 m, 22% improvement) appear clinically relevant and were retained after 1 year at levels beyond the minimal difference of clinical relevance, that is, 25 m. 41 Whether walking speed gains were as relevant (maximum: 0.12 m/s—13%; comfortable: 0.06 m/s—8%) is uncertain. Comfortable walking speed after training was within the range of limited community walking (0.4-0.8 m/s) but did not the reach the level of full community ambulation (>0.8 m/s).42,43
Control subjects slightly declined in these parameters indicating that current conventional care for chronic stroke survivors in Germany does not lead to improvements over 3 months. This finding supports previous studies.2,24 The effects of TAEX were confirmed by controls crossing over to TAEX-cross after conventional care. TAEX-cross led to comparable gains in all outcome measures as TAEX. Crossover TAEX differed from standard training to test the hypothesis that treadmill inclination stimulates gait symmetry, thereby improving overground locomotion. 20 This hypothesis was not supported by our data, but we did not examine gait symmetry.
Only 4 of the 48 persons clinically screened initially had to be excluded for medical reasons (8%). This rate is comparable to younger populations and argues against the criticism that our study population was highly selected from a population with high morbidity that would be excluded from TAEX. The treatment effects were comparable or higher than in most other reports.17,27,44-46 The high treatment gains observed, especially in a study sample exclusively recruiting elderly people, seems unexpected considering the current literature.24,25 Lee et al 44 reported 20% fitness gains after 3 months of aerobic cycling exercise at an intensity of 85% of Vo 2peak. Walking performance was unchanged. A 22% gain in Vo 2peak was reported after 8 weeks of high-intensity water exercises comprising task-specific ambulatory exercises (walking, running, side stepping) at an aerobic intensity up to 80% HRR. This program also improved gait velocity by 9%. 45 Macko and colleagues 17 observed a 17% gain in fitness and 30% improvements in 6-minute walks after 6 months of progressive TAEX. 10MW and balance were unchanged. The difference in fitness gains might be explained by higher aerobic intensity of the present trial (76% HRR vs 58% HRR). Another difference is the control intervention that was conventional care as opposed to dose-matched stretching exercises combined with low-intensity treadmill training. The control intervention in our study would not yield aerobic intensity levels to increase fitness.10,11 The different control intervention likely explains why Macko et al did not find significant between-groups differences for maximum walking speed; controls also improved, as a consequence of the daily treadmill component of therapy.
The gait improvements observed here were correlated with the progression of treadmill velocity and training duration in accordance with task-relevance of training and massed practice. The improvement in cardiorespiratory fitness was not predicted by this progression. Fitness gains were a function of how much the intensity of training progressed. This finding emphasizes the importance of heart rate–controlled training. We found no significant correlations between these outcome measures and age or time since stroke. Our study was the first that demonstrates significant gains in the Berg Balance Scale score after TAEX in a study sample with rather low risk for falls, although other studies suggest the changes were not clinically important (<5.8 points 47 ). Our follow-up data confirm that maintenance training is required for sustained benefits and that patients may need structured therapy programs to adhere to these training protocols.
This trial had limitations. The small sample size in combination with strict inclusion and exclusion criteria may have selected a healthier cohort with higher mobility than the average person with chronic stroke. The outcomes were not assessed blinded to treatment group. Given that highly standardized outcome tests were used, we believe that subjective rater influence was limited. The 1-year follow-up assessment was limited by a dropout rate of 6 subjects for walking (17%) and 14 subjects for fitness assessments (39%).
In conclusion, this randomized controlled trial provides evidence that aerobic treadmill exercise in chronic stroke survivors improves cardiovascular fitness, gait, balance, mobility, and quality of life in older persons. A training intensity just below the anaerobic threshold likely provides the greatest fitness benefit. Improvements in gait, however, are not necessarily a function of training intensity but seem related to the number of repetitions of walking movements. TAEX effects were largely preserved 1 year after the intervention. Larger trials will be necessary to investigate the long-term effects of exercise interventions on mobility, independence, and vascular risk reduction.
Footnotes
Acknowledgements
The authors thank the participants and therapists of the Geriatric Rehabilitation Department at the Robert-Bosch-Hospital, Stuttgart, Germany. We thank Fernando Dimeo of the Department of Internal Medicine at the Charite, Berlin, for valuable advice.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
The study was supported by a grant of the “Forschungskolleg Geriatrie” of the Robert Bosch Foundation.