
Abstract
Background. The Body Position Spatial Task (BPST) is a novel measure of whole-body spatial cognition involving multidirectional steps and turns. Individuals with Parkinson disease (PD) are affected by motor and cognitive impairments, particularly in spatial function, which is important for mental imagery and navigation. Performance on the BPST may inform understanding of motor-cognitive and spatial cognitive function of individuals with PD. Objectives. We conducted this study to determine feasibility and validity of the BPST with standard, validated, and reliable measures of spatial cognition and motor-cognitive integration and to compare BPST performance in adults with and without PD. Methods. A total of 91 individuals with mild-moderate PD and 112 neurotypical (NT) adults of similar age were recruited for the study to complete the BPST and other measures of mobility and cognition. Correlations were used to determine construct and concurrent validity of BPST with valid measures of spatial cognition and motor-cognitive integration. Performance was compared between PD and NT adults using independent t-tests. Results. BPST was feasible to administer. Analyses show evidence of construct validity for spatial cognition and for motor-cognitive integration. Concurrent validity was demonstrated with other tests of mobility and cognition. Relationships were stronger and more significant for individuals with PD than for NT individuals. BPST performance was not significantly different between groups. Conclusion. Tests that integrate cognitive challenge in mobility contexts are necessary to assess the health of spatial cognitive and motor-cognitive integration. The BPST is a feasible and valid test of whole-body spatial cognition and motor-cognitive integration in individuals with PD.
Keywords
Introduction
Individuals with Parkinson disease (PD) experience motor and cognitive impairments, impeding activities of daily living (ADLs), increasing fall risk, and decreasing quality of life (QOL). In all, 63% of people with PD report disabling sensory/perceptual deficits,1-3 which can result in impaired proprioception and kinesthesia.4-7 Thus, patients experience impaired motion sensitivity, joint position sense, and haptic acuity; altered attention to action; and inaccurate center of gravity.7,8 Proprioceptive and kinesthetic deficits are closely linked to and underlie both motor deficits in PD4,9,10 and spatial cognitive deficits.7,8 Cognitive impairments, including in spatial domains, manifest early on in many people with PD.11,12 Cognitive domains affected include those important for mobility: executive function, working memory/attention, 13 and spatial cognition.14,15 Spatial cognition is concerned with the acquisition, organization, utilization, and revision of knowledge about spatial environments. PD patients are frequently impaired in tasks requiring spatial attention and spatial-location memory, perception of optic flow, and line orientation 16 as well as visuospatial working memory and planning15,17 and mental rotation. 18 All these functions have significant implications for navigating environments. As such, spatial-cognitive deficits result in orientation disability and interact adversely with mobility in individuals with PD, 14 resulting in impaired motor-cognitive integration (ie, cognition is embodied in action—the motor system participates in what is effectively mental processing during functional activities). Such deficits have major adverse effects on QOL because of functional activity impairments.
Processes Underlying Spatial Cognition
Individuals use visual information and perception to navigate 19 and perform successful action in the environment.20,21 Being able to orient oneself in space is important for navigation and environmental recognition and is accomplished via self-motion cues (physical location) and external cues (landmarks). 22 Accordingly, the brain represents visuospatial information in egocentric and allocentric coordinates. Egocentric reference frames integrate vision and distance in the dorsal caudate nucleus, posterior parietal cortex, precuneus, and lateral frontal cortex. These frames are self-referent and updated as one moves through the environment. 23 Egocentric frames can be provided by static visual cues (eg, size, texture), dynamic cues generated by the observer’s self-motion, and the motion of objects around them as well as muscle and joint proprioceptive cues, and motor and vestibular information. 19 Allocentric reference frames integrate vision and distance in the medial temporal lobe (hippocampus) and ventral stream structures. These frames describe how object locations are processed in reference to each other and help develop cognitive maps. 23
Spatial Issues in PD
Spatial issues in PD are thought to result from dysfunction from dopaminergic receptors disrupting cortical functioning 22 as well as impaired parietal-mediated perception of bilateral visual space. 24 Proper completion of internally or self-guided movement relies on efficient function of subcortical loops involving the basal ganglia. 25 Because of dysfunction of the striato-thalamo-cortical circuit, people with PD have particular difficulty with self-initiated tasks. 26 Internally guided movements require timing characteristics to drive motor output. These timing characteristics are largely driven by caudate and other subcortical interactions with motor planning and execution regions. Given disrupted dopaminergic communication within the basal ganglia, PD patients are challenged in maintaining internal timing patterns that are reliant on basal ganglia function. As a result, PD patients are more likely to engage externally guided circuits to assist in task execution. Indeed, over time, the cerebellar-thalamo-cortical circuit is increasingly recruited to perform self-initiated tasks. 27 In healthy individuals, internally guided behaviors benefit from automaticity of movement. But even in early PD, lost dopamine in the dorsal putamen leads to diminished automaticity and requires continually increased cognitive control of motor function. 28 As such, conceiving egocentric reference frames may be difficult for people with PD, which affects visuospatial function. Rodent studies have shown a role in egocentric navigation for the caudate and in allocentric navigation for the hippocampus. People with Huntington’s disease, another basal ganglia disorder, are more impaired on egocentric working memory. 29 Based on PD pathological impact on caudate nucleus functioning, PD may have a greater impact on egocentric processing of spatial information than on allocentric aspects. 23
Given strong overlap between cognition and mobility, referred to as motor-cognitive integration, mobility deficits are common in PD. Mobility, in particular, requires the intersection of spatial function and motor-cognitive integration. Adding a cognitive task to a motor task, thus creating a dual-task paradigm, can worsen both motor and cognitive performance in patients with PD.30,31 A cogent example of the need for motor-cognitive integration is found in spatial learning, both passive (visual information, available path of motion) and active (egocentric cues, proprioception, and kinesthesia; cognitive processing of spatial information). Spatial learning is a key component of how individuals define their location—that is, orient themselves in space—and is required for mental imagery, identifying objects, and especially navigation.32,33 As such, motor-cognitive integration is necessary for successful completion of ADLs and simply traveling from one place to another.
However, current standard, valid spatial cognition assessments (eg, Reverse Corsi blocks [Corsi]), do not require whole-body movement from one location to another in a learned sequence. 14 A clinically evaluated task requiring whole-body movement assaying spatial-cognitive functions for navigation, mental imagery, short-term memory, movement planning, initiation, and coordination may provide information on the level of motor-cognitive integration and spatial cognitive function, which is requisite for basic movement in PD patients. We created the Body Position Spatial Task (BPST) to respond to the lack of a whole-body movement evaluation instrument that engages spatial-cognitive function, motor planning, and movement initiation. We developed the BPST because (1) it requires spatial cognition, which is early and often impaired in people with PD 12 ; and (2) spatial cognitive deficits intersect with motor performance, resulting in degraded motor-cognitive integration and impaired performance on the task.
The BPST is modeled after Corsi blocks, 34 a well-validated, widely used test of visuospatial cognition. Corsi does not measure whole-body spatial cognition. BPST requires participants to observe and learn a series of multidirectional steps and turns in lengthening sequences and then execute the movement series. We studied BPST in older adults with and without mild-moderate PD to (1) establish BPST feasibility for these populations; (2) examine BPST’s construct validity as a test of spatial cognition and motor-cognitive integration; (3) examine concurrent validity with mobility, executive function, and attention tests; (4) evaluate BPST’s discriminant validity (ie, compare PD performance on BPST to that of age-matched neurotypical [NT] adults); and (5) explore relationships between disease state, cognition, and BPST performance.
Successful execution of BPST requires spatial cognition and navigation of a predetermined path, short-term memory, motor planning, and internal guidance of movement. BPST was hypothesized to have construct validity with spatial cognition and motor-cognitive integration, and concurrent validity with tests of attention, executive function, and mobility. As a result of impaired spatial cognition and motor planning 35 and deficient execution of complex, goal-directed behavior 36 in PD patients, as well as egocentric spatial reference frames being affected, 23 and impaired internal generation of movement, we hypothesized that individuals with PD would perform worse on BPST, as measured by span length (length of sequence of moves performed correctly) and number of trials successfully completed compared with similarly aged NT adults.
Materials and Methods
Participants
PD participants were recruited through flyers, referral, PD newsletters, support groups, and websites. NT adults without a history of progressive neurological disorders were recruited at diverse, senior-independent living communities, at research social events, and through word of mouth. Eligible PD and NT participants were at least 40 years of age. Potential participants with early-onset PD (ie, PD that manifested before the age of 40 years) or history of other neurological insult were excluded. 37 A total of 91 individuals with PD (38 women, 42%) and 112 NT adults (82 women, 73%) were eligible and enrolled. Although the gender percentages differ, the prevalence of women in PD is 40%, 38 and among older adults, 65 years and older, the prevalence of women is nearly 60%, a percentage that increases with age (US Census Bureau Brief, the Older Population 2010).
Procedure
The Institutional Review Board at Emory University School of Medicine approved this work. Prior to testing, all participants provided written informed consent. All measures were administered during one assessment session in invariant order (to hold constant across participants any effects of testing, such as assessment experience, order, or fatigue.) and demographics, medical history, fall history, general health, ability to perform ADLs, education, and QOL were obtained. A fall was defined as “unintentionally coming to rest on the ground or lower level, not as a result of a major intrinsic event (eg, myocardial infarction, stroke, or seizure) or an overwhelming external hazard (eg, hit by a vehicle).” 39
Participants were given breaks ad libitum and offered snacks and water during testing sessions. Testing required approximately 2 to 2.5 hours depending on the participant. PD participants were tested while “on” medications at a self-determined optimal time. Patients were instructed to come to the assessment having taken medications exactly as prescribed from their provider and when they felt that their medications were likely to be working effectively.
Measures
All tests of construct validity are valid, reliable, and widely used in middle-aged adults, older adults, and/or those with PD. The BPST 41 is modeled after Corsi, 34 which assesses visuospatial working memory. In BPST, examiners visually and verbally demonstrate a pattern of side and forward steps, and turns in place, which the participant then repeats. After a practice trial of 2 moves, the examiner begins with 2 moves and progresses to a maximum of 9 moves. The number of moves increases by 1 at each subsequent level containing 2 trials. Participants advance to the next level if they correctly completed at least 1 of the trials in a level. Once a participant misses both trials in a level, the task ends. Span (length of sequence of moves that were correctly performed) and number of trials performed correctly are used for analyses. Participants are allowed to use habitual assistive devices. The scoring of BPST is exactly as in validated and standardized Corsi blocks. Participants need to perform the trial perfectly to get a point/correct trial. If they perform all the moves but in an incorrect order, the trial is considered incorrect.
Measure of PD Severity
Unified Parkinson’s Disease Rating Scale Motor Subscale III (UPDRS-III)42-45 and Hoehn and Yahr (H&Y) Stage of Disease Severity 46 were administered to PD patients and scored by qualified and trained raters to measure disease severity. UPDRS-III scores range from 0 (asymptomatic) to 108. H&Y stages range from 0 (asymptomatic) to 5 (wheelchair bound/bedridden).
Measures of Construct Validity for Visuospatial Cognition and Motor-Cognitive Integration
Primary measure of construct validity for spatial cognition
The reverse Corsi blocks visuospatial task is valid for middle-aged and older adults and those with PD.34,47-49 The Corsi blocks requires participants to watch the examiner point to a series of blocks in a certain order and then repeat the pattern backward. The examiner began with 2 moves and progressed to a maximum of 9 moves, with 2 trials per level of equal move length. Participants were given 1 practice trial of 2 moves. At each subsequent level, the number of required moves increased by 1. A participant would advance to the next level if they successfully completed at least 1 trial in a level. The task was concluded after the participant failed, that is, received a zero, for both trails in a level. The span (the longest sequence a participant can correctly repeat) and number of trials completed correctly were considered for analyses. Participants receive 1 point for a correctly completed trial and zero points for an unsuccessful trial.
Primary measure of construct validity for motor-cognitive integration
The Four Square Step Test (FSST)50,51 measures movement planning, initiation, movement speed, and coordination. Time to complete FSST has been associated with tests of executive function as well as cognitive-motor dual task performance. 52 Participants are required to step clockwise then counterclockwise into 4 squares created by rods arranged on the ground in a cross. The task is timed and 3 successful trials recorded. If a participant steps on or touches a rod, the trial ends and a new attempt starts. The fastest time is selected for group analyses. This test is valid in middle-aged and older adults 50 and people with PD. 52
Measures of concurrent validity
Motor: all the following measures are standard, valid, and reliable for older adults with and without PD.
Timed Up and Go Test (TUG) 53 is a valid measure of functional mobility for PD patients, middle-aged adults, 54 and older adults55,56 and was administered as published. Individuals are asked to rise from a chair, walk 3 m to cross a line, turn around, and return to the chair as quickly and safely as possible. Dual Timed Up and Go Test53,57 is a valid measure of functional dual-task abilities for mobility and cognition for middle-aged and older adults and for PD patients. Participants are timed while they perform both single TUG (as described above) and a concurrent cognitive component (TUG-Cognitive; counting backward by 3s [“serial 3s”] from a random number between 20 and 100) or manual component (TUG-Manual; carrying a full glass of water). Before completing TUG-Cognitive, the participant is given three, 15-s trials of serial 3s while seated to be comfortable with the counting task while also performing the motor task.
The 6-Minute Walk Test (6MWT)58,59 assesses community ambulation and endurance. Participants are instructed to walk as far as they can in 6 minutes, without running. 6MWT is a valid measure for middle-aged and older adults and for PD patients. 60
The 30-s Chair Stand61,62 assesses lower body strength. With their arms crossed over their chest, participants are asked to rise from a chair to full standing as many times as possible in 30 s. The 30-s Chair Stand is a valid measure for middle-aged and older adults and for PD patients. 63
Gait speed59,64 assesses multidirectional preferred and fast-as-possible (fast) walking speeds. Participants perform 3 trials each of walking forward at a preferred pace, backward at a preferred pace, and forward as fast as possible over 20 feet. For the latter, participants are instructed to walk quickly but safely. Participants start walking 1 m and finish walking 1 m beyond the start and finish lines. Qualified raters time participants with a stopwatch as the first heel passes the starting line and stop when the second heel passes the end line. The 3 trials from each condition are averaged and speed (m/s) derived. Gait speed is a valid measure for middle-aged and older adults and for PD patients. 65
The Fullerton Advanced Balance Scale (FAB)66,67 predicts fall risk in older adults and people with PD with a series of items that challenge static and dynamic balance. FAB was only administered to those with PD. The use of assistive devices is prohibited during this test. Qualified raters judged performance on 10 individual items: (1) standing with feet together, eyes closed; (2) reaching forward to retrieve an object; (3) turning 360° in place (variables: number of steps taken during the turn and greatest amount of time needed to turn 360°); (4) stepping up and over an obstacle; (5) tandem walking; (6) standing on 1 leg; (7) standing on foam with eyes closed; (8) jumping for distance; (9) walking with head turns; and (10) recovering from an unexpected loss of balance. Each item is rated on a 5-point ordinal scale (0-4), with a maximum of 40 possible points.
Cognition
The Montreal Cognitive Assessment (MoCA) is a 30-point test providing a measure of global status of cognitive impairment through the assessment of a range of executive functions, including orientation, memory recall, visuospatial function, attention/concentration, and language. MoCA achieves high sensitivity and specificity for detecting mild cognitive dysfunction in middle-aged and older adults 68 and is valid and reliable in people with PD. 69 If an individual had fewer than 12 years of education, they receive an additional point. A score of 26 or greater is considered a normal screen for cognition. 70
Trail Making Tests A and B,71-73 a neuropsychological task, is valid and reliable in PD and middle-aged and older adults. 74 It tests visual attention, processing speed, and executive function. In Trails A, a test of visual motor speed and numeric sequencing, the participant connects numbers scattered on the page in ascending order. In Trails B, a test of global frontal lobe dysfunction and executive function, the participant connects numbers and letters on a page in alternating, ascending order (ie, 1-A-2-B-3-C, etc). Participants are required to connect the letters and/or numbers as quickly as possible, without lifting the writing utensil from the paper. They receive a practice attempt for both Trails A and B. Errors made while completing the task are pointed out immediately, so the participant can correct them. Time to complete each trial (up to 300 s) is recorded. The time to complete Trails A, Trails B, and the difference between Trails A and B (Trails difference = Trails B − Trails A) are considered for analyses.
Questionnaires
The participants completed the following questionnaires within 1 week prior to their testing session. These questionnaires are valid, standard, and reliable in both older adults and people with PD.
Activities-Specific Balance Confidence Scale (ABC)59,75 asks about an individual’s confidence in “not losing his/her balance” in everyday situations. Participants rated their confidence for each situation on a scale of 0% to 100% confidence. Scores are averaged, and overall percentage confidence was used for analysis. ABC is a valid measure for all middle-aged and older adults. 76
Composite Physical Function Scale (CPF)77,78 asks about an individual’s functional ability as related to basic ADLs, intermediate ADLs, and advanced activities. Participants were asked to rate activities as “can do,” “can do with difficulty or assistance,” or “cannot do.” This 24-point scale can provide estimates of risk for loss of function.
Data Analysis
Data were entered and cross-verified by research assistants. F-tests determined equality of variance between performance on outcome measures of individuals with PD and NT older adults. Independent t-tests or χ2 as appropriate were run to determine differences in performance between PD and NT scores. The association between BPST and measures to provide evidence of construct validity and measures to determine concurrent validity and self-reported data (demographics, fall incidence, psychosocial measures) were explored with Spearman’s correlation coefficient. Both concurrent and construct validity may be assessed with a correlation coefficient and are not mutually exclusive conditions to the extent that the assessment of 1 validity precludes the assessment of all others with the same statistic. Although concurrent validity may be assessed directly with a correlation coefficient, this methodology is not sufficient for assessment of construct validity. We can use the correlation to provide evidence of construct validity. Therefore, Corsi was examined for its correlation to BPST to provide evidence of construct validity for visuospatial cognition because Corsi is a validated test of visuospatial cognition. Furthermore, task structure, measures, and scoring of BPST were modeled directly from Corsi. BPST span and trials successfully completed were analyzed against FSST to provide evidence of the construct validity of the BPST for motor-cognitive function. FSST was used as a comparable measure that integrates motor and cognitive function because both BPST and FSST involve navigation and forward and side steps in multiple directions in a remembered pattern. Both interval and ordinal scale variables were gathered in this study. Spearman’s ρ can be used to identify a correlational relationship between 2 variables even if the relationship is nonlinear but still monotonic. We used a random procedure to introduce continuity to the ordinal measures—for example, BPST—in the data because of the limited number of possible values of the BPST trials and span variables. By allowing the observations to vary a little within each measurement value group, we introduced additional variability to model our data, which allows us to better estimate the linear relationship and quantify the validity of our measures. By randomly generating a small uniform deviation of up to ±0.25, we maintained the relative value of the data but removed the potential for ties (ie, equal magnitude) between observations in the same category. 79 To account for this additional level of uncertainty, we replicated the random unrounding procedure 1000 times and built 95% bootstrap CIs for our correlation estimates. 80 Bootstrapping provides empirical intervals in cases where the data may not be sufficient for methods based on the assumption of normality. The underlying data of the study meet this insufficiency criteria because of the discrete nature of the scales and the random unrounding we applied to the data make the measures satisfactory for assessing the correlations. To further explore the relationship between disease stage, cognitive status (as measured by MoCA), and performance on BPST (as measured by BPST span), the PD group was subdivided into 3 cohorts of H&Y stages 1 and 1.5, 2 and 2.5, and 3. Correlations were examined, and the data were plotted on a figure to visualize relationships. The α level was set at .05. We used Cohen conventions (.1 = small; .3 = moderate; .5 = large) to interpret the strength of each correlation. Some participants’ data were not available for some assessments. To not be coercive, research assistants did not probe for reasons when patients declined to perform a task. We used all available data for each analysis to avoid introducing bias by only using patients with complete information. By using all the data, we increase the variability in effective sample size but ensure that the results are as generalizable and replicable as possible.
Results
A total of 91 individuals with mild-moderate PD and 112 NT adults were enrolled and assessed in this study. PD participants had more prescription medications, had less balance confidence, and were more likely to need assistance with daily activities. On cognitive measures, the 2 groups performed similarly. With respect to motor tasks, PD participants were slower in completing TUG and preferred, backward, and fast gait speeds; completed fewer chair stands; and required more time and steps to turn 360° in place (Table 1).
Baseline Participant Demographics for the Enrolled Sample and Performance on Motor, Cognitive, and Psychosocial Measures. a
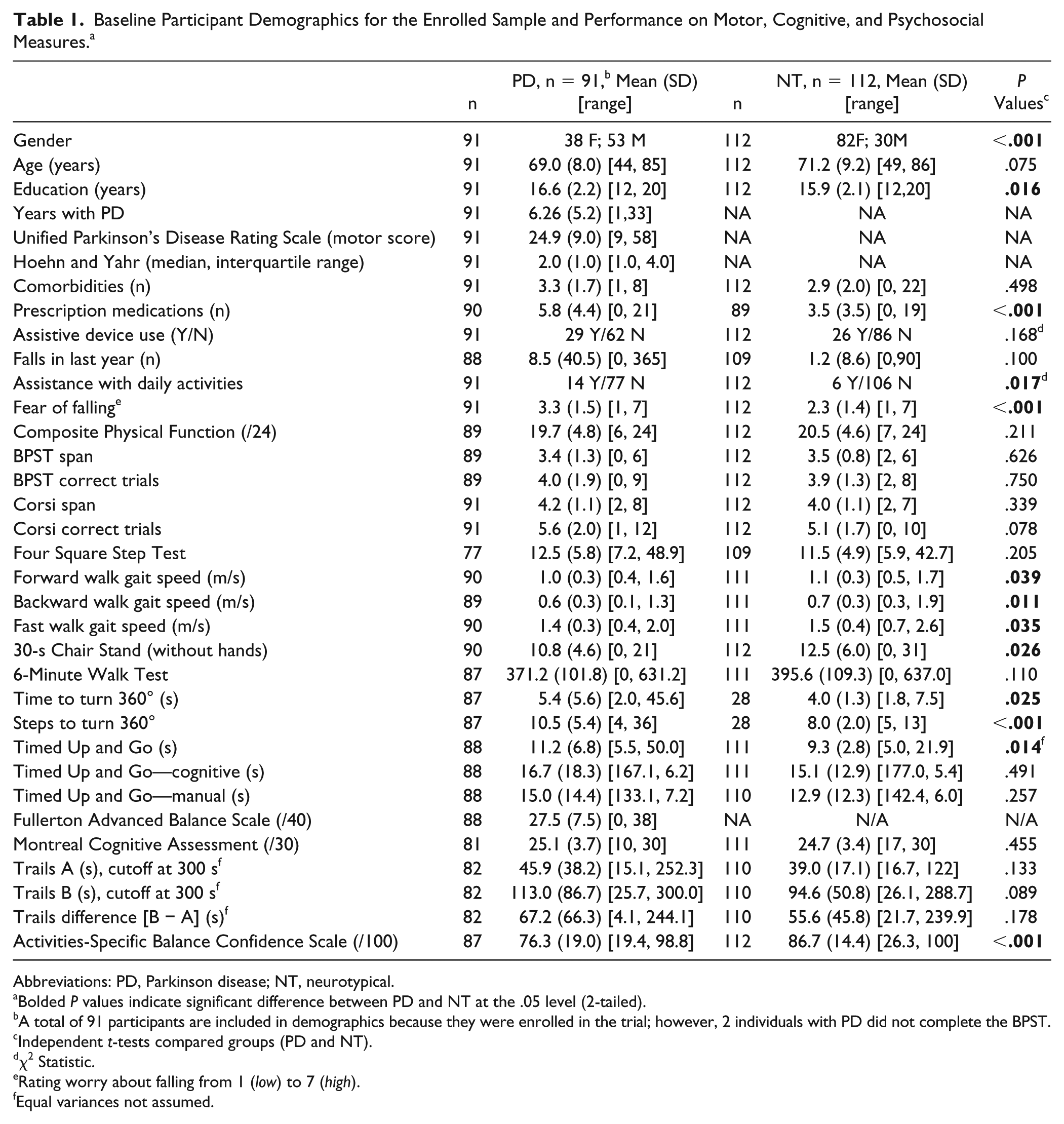
Abbreviations: PD, Parkinson disease; NT, neurotypical.
Bolded P values indicate significant difference between PD and NT at the .05 level (2-tailed).
A total of 91 participants are included in demographics because they were enrolled in the trial; however, 2 individuals with PD did not complete the BPST.
Independent t-tests compared groups (PD and NT).
χ2 Statistic.
Rating worry about falling from 1 (low) to 7 (high).
Equal variances not assumed.
Feasibility of BPST for Clinical Use for Participants With PD and NT Participants
A small space, that is a clinical office, was needed for the BPST. No adverse events (falls or injuries) occurred during testing. Only 2 PD individuals refused to perform the task for unknown reasons. All NT participants completed the task. Instruction and practice trial time took approximately 2 minutes. Altogether, BPST took 5 to 10 minutes to complete depending on how many levels the participant successfully completed. Tables 2 (PD, n = 89) and 3 (NT age-matched adults) list Spearman’s correlation means and 95% bootstrap CIs between BPST span and BPST correctly completed trials, and they list concurrent measures of mobility, cognitive and psychosocial function, disease severity, and demographics among participants.
Spearman’s Correlation Means and 95% CIs Between BPST Span and Trials Performance and Cognition, Mobility and Dual Tasking, Psychosocial Function, Disease Severity/Demographics for Individuals With PD (n = 89). a
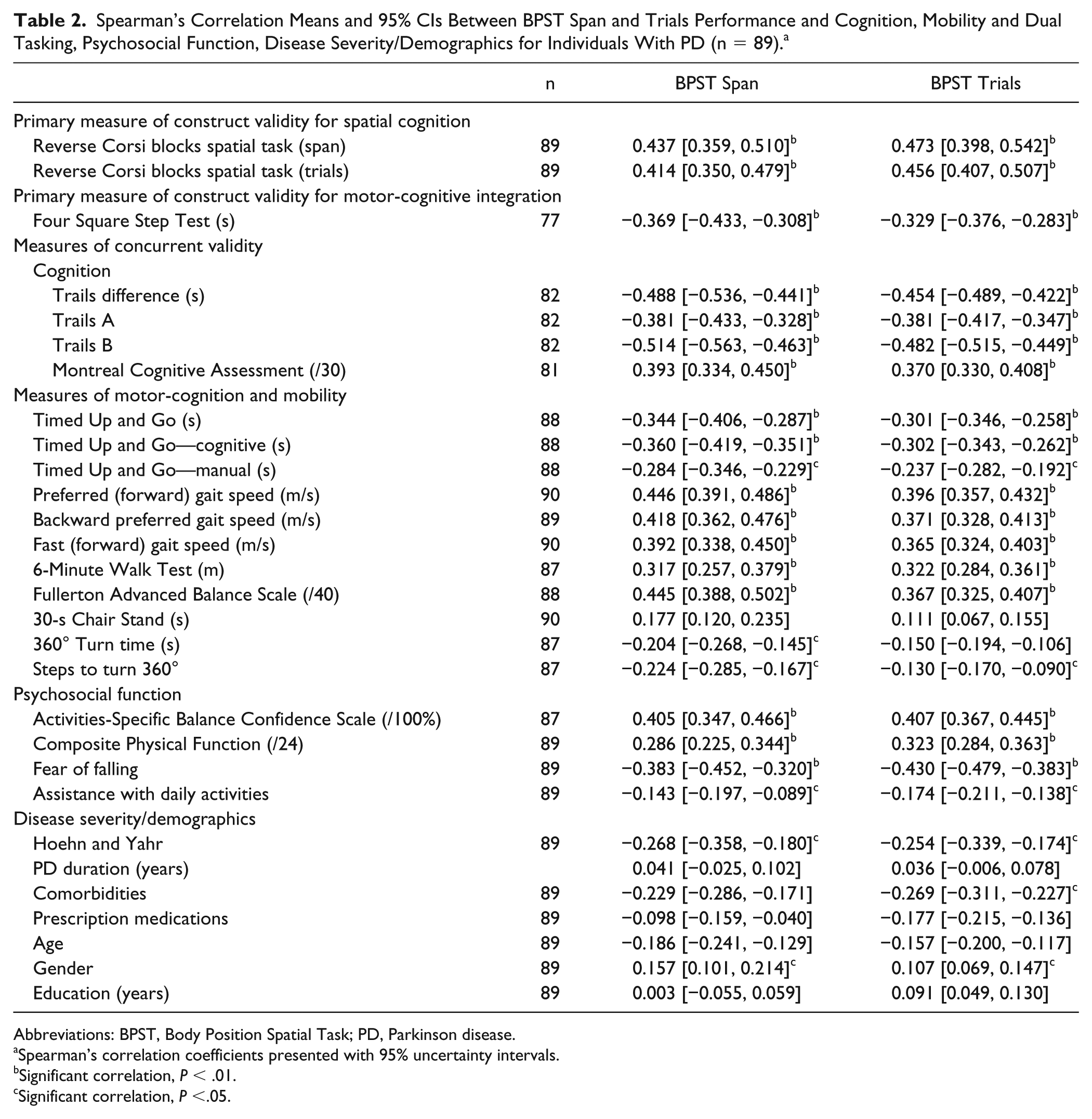
Abbreviations: BPST, Body Position Spatial Task; PD, Parkinson disease.
Spearman’s correlation coefficients presented with 95% uncertainty intervals.
Significant correlation, P < .01.
Significant correlation, P <.05.
Spearman’s Correlation Means and 95% CIs Between BPST Measures and Cognition, Mobility and Dual Tasking, Psychosocial Function, Disease Severity/Demographics for NT Individuals (n = 112). a
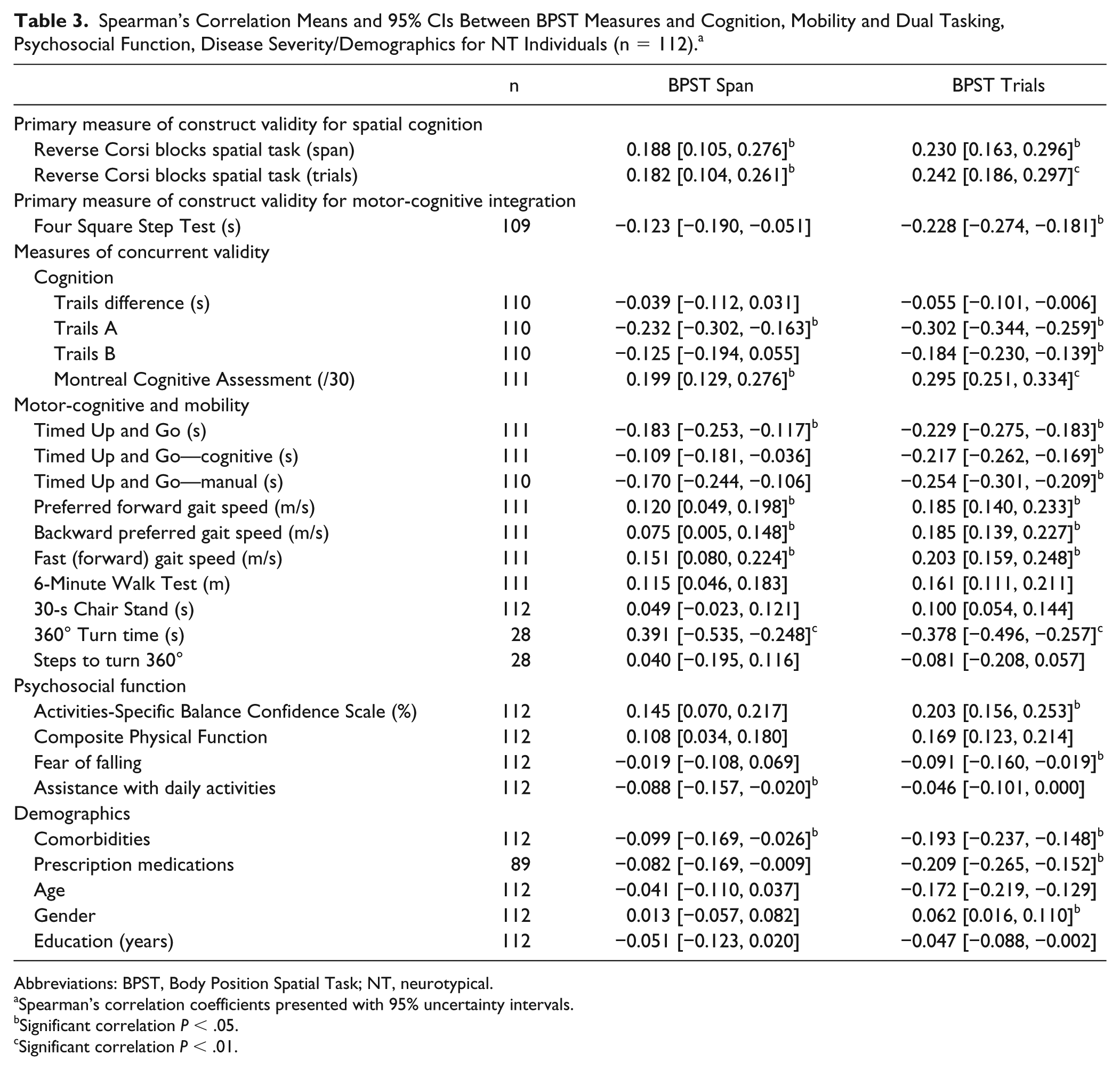
Abbreviations: BPST, Body Position Spatial Task; NT, neurotypical.
Spearman’s correlation coefficients presented with 95% uncertainty intervals.
Significant correlation P < .05.
Significant correlation P < .01.
Validity for Individuals With PD (Table 2)
Although correlations were similar between BPST span and trials, correlations were greater for BPST span than trials for all measures, except for Corsi blocks span and trials variables.
Construct validity of spatial cognition. Large, significant correlations between BPST span and Corsi span provide evidence of construct validity of BPST for visuospatial cognition in people with PD.
Construct validity of motor-cognitive integration. Moderate, significant correlations between BPST span and FSST and between BPST trials and FSST provide evidence of construct validity of BPST for motor-cognitive integration in people with PD.
Concurrent validity. Large, significant correlations between Trails difference, Trails A and Trails B, and BPST span and trials demonstrate concurrent validity of BPST with tests of attention, inhibition, and set switching. Significant, moderate correlations between BPST and MoCA demonstrate concurrent validity with global cognition. Significant, moderate correlations between BPST and TUG, TUG-M, TUG-C, preferred forward, backward, and fast gait speed, 6MWT, and FAB demonstrate concurrent validity with additional dual motor-cognitive measures, mobility, and balance measures (Table 2).
Validity for NT Adults (Table 3)
Correlations were generally stronger for BPST trials than span. Overall, correlations were less strong for NT adults compared with the PD sample.
Construct validity of spatial cognition. Small to moderate, but significant, correlations between better performance on Corsi span and trials and better BPST span and trials provide minimal evidence of construct validity for spatial cognition.
Construct validity of motor-cognitive integration. Small, but significant, correlations between better scores on FSST and BPST span and trials provide minimal evidence of construct validity for motor-cognitive integration.
Concurrent validity. Significant, moderate correlations between better performance on Trails A, Trails B, and MoCA and better BPST scores suggest concurrent validity with tests of global cognition and executive function. Significant, moderate correlations between better BPST span and trials and less than 360° turn time suggest concurrent validity with a mobility measure. Small, but significant, correlations between better BPST and better TUG-C, TUG-M, preferred forward, backward, and fast gait speed, and 6MWT scores suggest concurrent validity with measures of mobility. All other correlations were small.
BPST Relationship With Psychosocial Function
PD Participants
Greater BPST span and trials were moderately strongly correlated with greater balance confidence and fear of falling. Greater BPST span and trials were significantly and moderately correlated with CPF (Table 2).
NT Adults
A small, significant correlation between BPST trials and balance confidence was noted (Table 3).
BPST Relationship With Demographics and Metrics of Health Status
In people with PD, both greater H&Y staging and having more comorbidities were significantly and moderately correlated to lesser performance on BPST span and trials. In NT adults, having more comorbidities and prescription medications were significantly but minimally correlated with lesser performance on BPST span and moderately correlated with lesser performance on BPST trials (Table 3).
Performance in Individuals With PD Versus NT Adults
The groups did not significantly differ in BPST span and trials performance or in time needed to complete the FSST (Table 1).
Post hoc Analyses Exploring the Relationship Between Stage of PD, Executive Function, Cognitive Status, and Performance on BPST
The relationship depicted in Figure 1 shows that worse disease staging led to lesser performance on the BPST span. Higher MoCA scores were related to greater performance on BPST span.
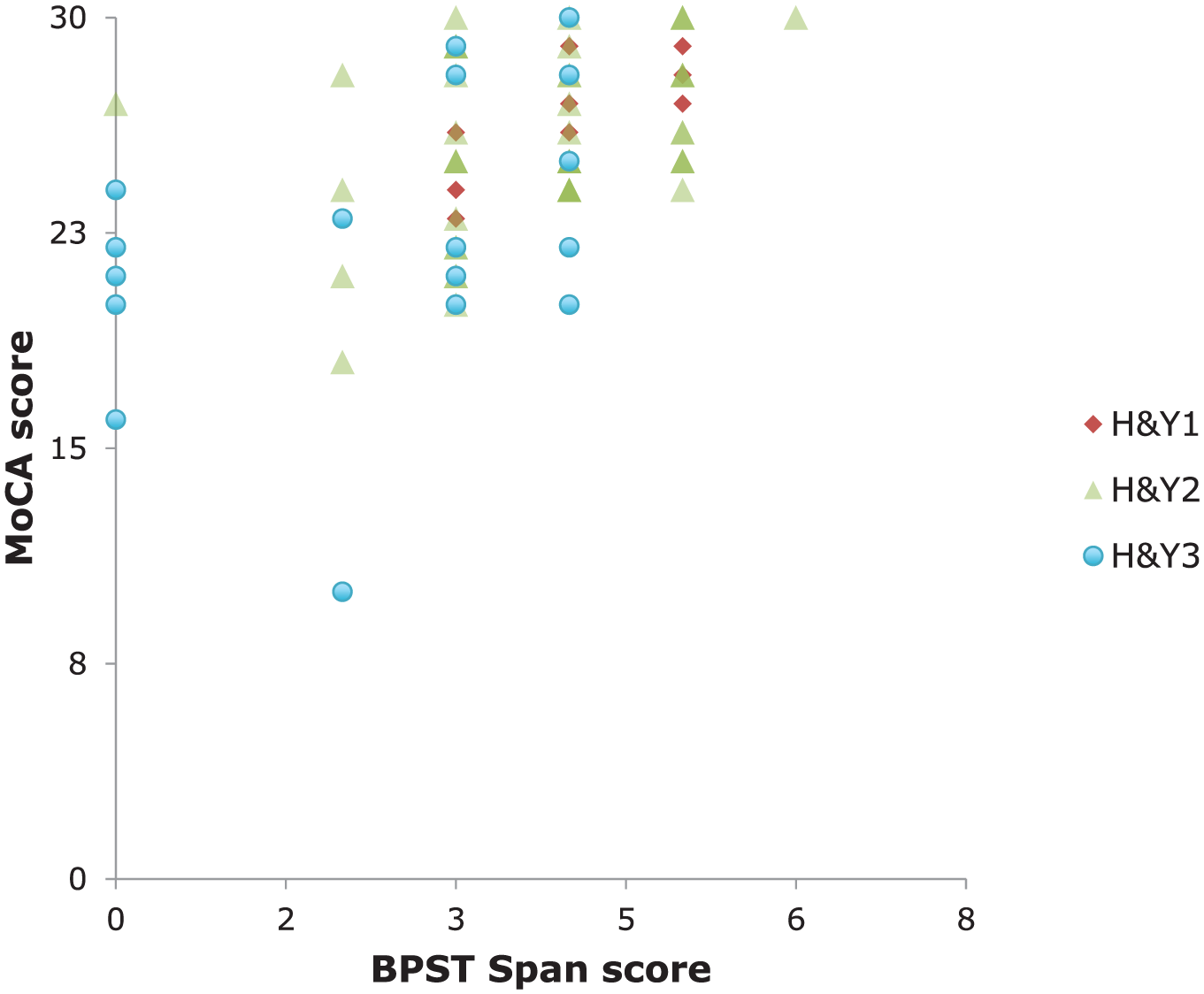
The relationship between cognitive status and performance on BPST with respect to stage of disease. The PD group was subdivided into H&Y stage 1 to 1.5 (diamonds), 2 to 2.5 (triangles), and 3 (circles). Cognitive status is more strongly related to BPST performance than is disease stage.
Discussion
BPST is feasible, and these correlations provide evidence of construct validity—that is, that BPST may be a valid measure of spatial cognition and motor-cognitive function for adults with mild-moderate PD and possibly for NT adults of similar age. Concurrent validity for other tests of cognition and mobility was demonstrated. We believed that performance on BPST would reveal deficits related to neuromotor processes that are necessary for dividing attention between mental processing and whole-body movement—that is, that the test would reveal discriminant validity. This was not the case. Performance on BPST was not significantly different between individuals with PD and NT adults. Furthermore, we observed that the relationship between cognitive status and BPST performance was stronger than that between BPST performance and disease stage in those with PD. Neither BPST span, nor trials were significantly correlated with measures of demographics, suggesting broad validity of the task for individuals beyond the populations examined with these samples.
Differences Between Men and Women in Spatial Cognition and How These Differences May Have Affected Results
Previous research has shown sex differences in seated (ie, non–whole-body movement) tasks of spatial cognition usually for mental rotation. 81 Differences may arise if men and women do indeed differ in spatial processing style, for example, allocentric (cardinal direction based) versus egocentric (personal directions, eg, left and right). 82 Some have reported that men take a more allocentric approach and women an egocentric 83 ; therefore, instructions requiring allocentric perspectives (an Euclidean approach) favor men and instructions necessitating egocentric perspective (personal directions) lead to women performing better. 84 Other work has shown that these differences are mediated by and can be eliminated by manipulations in confidence 81 and negative performance expectations and that spatial differences previously noted do not show an actual lack of ability. 85 Our sample included more males with PD than women. However, the epidemiological incidence of PD is 60% male, 38 which our study closely approximates in distribution. Future studies should investigate the differences in whole-body spatial cognition performance between men and women with and without PD to help understanding of spatial cognitive processing with respect to mobility. Because older women in particular are at greater fall risk, further study is warranted.
Clinical Use
BPST is feasible for clinical use because the test took <10 minutes to administer in a small space for both groups and could be used for individuals using assistive devices. BPST performance was associated with performance on FSST and Corsi for people with PD and to a lesser degree, NT adults. Association with these valid motor-cognitive integration/spatial cognitive tasks provides evidence of construct validity for BPST. Corsi is an accepted instrument for assessing spatial cognition and requires that examinees mentally orient in space.34,86,87 However, physically orienting oneself in a space, as measured by BPST, has more relevance for mobility contexts and for individuals with greater fall risk. Previous research shows that cognitive ability and training is important for functional mobility,86,88,89 further cementing the importance of jointly measuring spatial cognition and mobility, which BPST does. From correlations with valid spatial-cognitive and mobility tasks, BPST span and trials may accurately measure the interaction of an individual’s motor and spatial-cognitive function, especially for individuals diagnosed with idiopathic PD.
Concurrent Validity of BPST With Mobility, Cognitive, and Psychosocial Measures
A faster preferred walking speed and greater confidence in one’s ability to maintain balance were associated with better BPST performance in PD individuals. Faster walking speeds and greater balance confidence may have facilitated the task demands by decreasing the necessity to focus on balance maintenance (with or without an assistive device) while mentally retaining and executing a series of steps. Faster completion of one dual-tasking measure, TUG-Motor, was associated with better BPST performance among individuals with PD. TUG-Motor requires participants to remember multiple motor movements in a sequence, a common feature to both BPST and TUG-Motor. Physical function and fall risk are also important variables to understand and measure when considering individuals with PD. For PD participants, BPST performance was significantly correlated with ability to perform ADLs, balance confidence, and fear of falling as rated by the participant. Additionally, the FAB Scale, a challenging multi-item balance assessment not administered to NT adults, was strongly correlated with BPST. All these correlations suggest that better performance on BPST may indicate better physical function, balance confidence, and gait. Therefore, administering the BPST may open a window into an individual with PD’s fall risk and physical ability in his or her daily life.
The NT Age-Matched Adults
For the NT group, correlations between BPST performance, psychosocial measures, and gait speed were weaker, indicating that the BPST has less potential to reveal information related to these constructs in these age-matched individuals without PD. The lack of significant and strong associations between BPST performance and mobility, dual tasking, and cognitive measures among NT older adults may be a result of their ability to undertake coordinated, planned activity without the deficit in internal generation of movement that people with PD often have. This deficit and general slowness in PD should have increased the time needed to enact a movement and possibly led to increased working memory demands. Individual differences across testing measures likely made performance less associated with other tests and more associated with the innate motor and cognitive abilities of NT middle-aged and older adults.
Although the NT group performed significantly better on standard tests of motor function (eg, chair stand and gait speed) and had greater balance confidence than those with PD, the groups performed similarly on the BPST. The NT group also performed similarly to the PD group on Corsi and the FSST, which agrees with research demonstrating that individuals with mild-moderate PD do not differ significantly from healthy older adults in FSST performance. 52 Whereas other studies have shown spatial deficits in Corsi between those with and without PD, 90 their samples were considerably smaller than in this study. BPST was strongly correlated with both FSST and Corsi in the PD group, suggesting that these 2 tests make an ideal combination to measure individual advantages: a valid measure of spatial cognition in the former and a test of multidirectional mobility in the latter.
Cognition in PD
Although this PD group was not considered cognitively impaired, several individuals had moderate PD with considerable physical impairment. Among those with PD, cognitive status was more associated with BPST performance than was disease stage. Without differences in cognition between groups, yet differences in certain motor tasks, the similarities in the BPST scores may be more indicative of cognitive outcomes than motor. Interestingly, a test of executive function, Trails B, was most strongly correlated with BPST performance in the PD group, indicating that the BPST may have broader application to cognitive assessment, which is important considering the strong import that executive function has for mobility and gait in PD. 13 The large and significant correlation of BPST with “Trails Difference” may indicate that executive function, specifically inhibition and set switching, has construct validity with BPST in a PD population. This finding is reasonable, given the strong interaction between executive function and mobility. 13
Egocentric Versus Allocentric Visuospatial Abilities in PD and Impact on Task Performance and Associations
Because of striatal dysfunction, PD may have a greater impact on egocentric processing than on allocentric aspects. 23 We believe that the BPST uses both egocentric and allocentric spatial abilities. The participant is required to observe and listen to directions given by the rater and then perform the task, which is modeled off of many clinical tests that involve simultaneous visual and verbal demonstration. Likely, participants use multiple strategies to complete a BPST trial successfully. Egocentric spatial abilities make use of proprioception and kinesthesia, which are vital for movement. To move, one has to use egocentric abilities, but in addition, the verbal directions given during BPST are not to particular locations in the room, or toward particular walls or any other room-specific landmarks, for example, “the window.” The verbal directions given are from an egocentric (personal) perspective: for example, turn left, turn right, step left, step right. However, allocentric properties are also used because one observes a rater travel from one place to another, and to or away from a given wall. Thus, if more comfortable using an allocentric perspective, the participant may note in their mind different landmarks (walls of the clinic room) to which the person traveled to or away from to eventually arrive in the same places, when the participants perform the task themselves. People with PD may use an allocentric strategy to address loss of automaticity and internally guided movement ability. Therefore, people with PD might be particularly reliant on observing the spatial end points of each move and the relationship to global landmarks, rather than self-referents given by the verbal directions. People with PD may be able to make use of relatively intact (at milder stages of PD) allocentric spatial processing. But, concurrently, these participants with PD required more cognitive resources—for example, executive function—to accomplish the task, than NT adults, which was reflected in the enhanced correlations (and particularly executive function) for those with PD, observed to a lesser extent in the NT adults. The data show that those with PD who scored well on executive function also scored well on the BPST.
Limitations
The study has several limitations. One limitation of this study is that more women were in the NT group than in the PD group, which may have affected performance on BPST and/or other measures in unknown ways. Additionally, the PD group had slightly but significantly more years of education than the NT group; however, the 2 groups did not differ on MoCA, and education was not correlated to performance on the BPST in PD. Impairments beyond visuospatial short-term memory span—for example, motor learning deficits—may adversely affect performance on this test. Future tests of BPST should develop age, sex, and education norms to minimize these variables as possible sources of data distortion. Furthermore, additional tests of short-term memory and executive function (see correlation with Trails B) may have added dimensions to these findings. The small correlations noted in the NT group suggest that additional study in a more heterogeneous group of older adults is warranted. Future research should use other tests, such as the Digit Span WAIS-III that was previously used to validate Corsi blocks, to validate the BPST. It must be noted that the BPST could have correlated to Corsi for reasons other than visuospatial cognition. When examining left- versus right-onset PD, 22 using the Clock drawing test to measure visuospatial function, researchers found that people with left-side onset performed worse on the test than healthy controls and right-onset patients. As such, examining differences in BPST performance between those with left and right onset PD may be important in the future. The BPST probably measures neither allocentric nor egocentric spatial abilities purely. To our knowledge, there are no clinically available tests that do so. 23 As such, future experiments should isolate aspects of BPST or another whole-body spatial cognition task to test the influence of allocentric versus egocentric strategies and abilities on task performance.
Conclusions
The BPST, a task requiring whole-body movement, is feasible and provides a valid measure of spatial cognitive function and motor-cognitive interaction for people with PD. Several significant relationships were demonstrated between BPST and other functional abilities, which indicate the validity of the test, both as a soundly constructed measure of whole-body movement necessitating spatial cognition and as a discriminant between groups on performance of physical function and fall risk. BPST performance was significantly correlated with motor skills and cognitive ability; these abilities are integral to functioning independently and fully performing ADLs. Additionally, relationships with BPST performance and other functional abilities were strong in the PD group, indicating that BPST may be valid for examining association between motor and cognitive ability in PD individuals. Similarly, BPST was shown to be associated with measures of daily physical function, balance, and fall risk, but only for PD participants. Among PD participants, BPST performance and disease stage (as measured by H&Y stage) are only weakly correlated, indicating that BPST may reveal motor-cognitive interactions independent of disease severity. BPST should be included in clinical assessment tools utilized to measure impairments in PD individuals that may not be observed in assessments purely measuring mobility, cognition, or disease severity. Because BPST closely mirrors the mobility, motor-cognitive interaction, and spatial-cognitive demands of daily life, understanding how individuals with and without PD perform on the task is important. In doing so, performance on BPST can elucidate clinical signs and identify the impacts of the disease in people with PD.
Footnotes
Authors’ Note
The study sponsors played no design in the writing of the article, the final conclusions drawn, or in the decision to submit the manuscript for publication. Each author was involved with (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Emory Center for Injury Control, the Dan and Merrie Boone Foundation, and the Emory Center for Health in Aging supported the study. This study was also supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR000454. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Department of VA R&D Service Career Development Awards (E7108M and N0870W) supported ME Hackney. We acknowledge the participants’ time. We acknowledge Dr Kathleen E. McKee, MD, for recruitment and assessment assistance.