
Abstract
Background. Effective protective steps are critical for fall prevention, and anticipatory postural adjustments (APAs) after a perturbation but prior to protective steps affect step performance. Although APAs prior to protective steps are altered in people with Parkinson’s disease (PD), whether these changes affect subsequent step performance is poorly understood. Objective. Characterize the relationship between mediolateral APA size and protective step outcomes in response to anteroposterior balance perturbations in people with PD. Methods. Twenty-eight individuals with PD completed 25 forward and 25 backward protective steps in response to support surface translations. Multilevel linear models related mediolateral APA size to protective step outcomes. Results. During forward protective stepping, larger mediolateral APAs were associated with delayed (P < .001) and larger (P = .004) steps. Larger APAs were also associated with smaller mediolateral (P < .001) but larger anterior-posterior center of mass movement at foot off (P < .001). During backward stepping, larger APAs were associated with later steps (P < .001) and smaller anterior-posterior margin of stability at first foot contact (P < .001). During backward stepping, larger APAs were also associated with worse clinical (ie, UPDRS [Unified Parkinson’s Disease Rating Scale]; P = .005) and balance (ie, MiniBEST [Mini-Balance Evaluation Systems Test]; P = .021) outcomes. Conclusions. During forward protective stepping, larger APAs were associated with larger and later steps, suggesting APA size may have mixed effects on the subsequent step. During backward stepping, larger APAs were associated with worse stepping outcomes (ie, later steps, smaller anterior-posterior margin of stability, worse clinical outcomes). Interventions aimed at improving APAs in PD should monitor spatial and temporal protective step outcomes to ensure treatment does not negatively affect protective steps, particularly for forward stepping.
Introduction
Ineffective weight shifts are a common cause of falls in elderly and Parkinson’s disease (PD) populations.1,2 Anticipatory postural adjustments (APAs) are a specific type of weight shift that occurs prior to an internally or externally generated postural challenge. For example, prior to a voluntary step the center of pressure moves backwards and toward the eventual swing limb, facilitating stepping. 3 In people with PD, APA size prior to normal voluntary stepping is reduced, likely contributing to hypokinetic steps often observed in this population.4-8
After a loss of balance, it is often necessary to take a quick “protective” step. These protective steps are necessarily faster than voluntary steps, and the effectiveness of these steps is important for fall prevention. In some cases, an APA can occur after the loss of balance but prior to the protective step. However, in healthy older adults, the size of these postural adjustments is often smaller prior to protective steps compared with prior to voluntary steps, probably to facilitate quick protective steps. 9 Studies investigating APAs prior to protective stepping in people with PD are sparse; however, they generally show that APAs prior to protective stepping to be larger in people with PD compared to controls.10-12
APAs after a loss of balance and prior to a protective step affect the effectiveness of the subsequent step. For example, large APAs prior to protective stepping are related to later steps in healthy adults and people with PD,9-11 suggesting that reducing APA size in this context hastens stepping. However, while reducing APA size prior to protective steps may facilitate quicker stepping, it may also reduce mediolateral (ML) stability.3,9,13 Indeed, older subjects sometimes take a second, laterally directed protective step after a loss of balance, suggesting poor control of lateral movement of the center of mass (COM). 14 Maki and McIlroy further demonstrate that during protective stepping, there is a tradeoff between speed of a protective step and stability after the step, particularly in the ML direction. 15
Recent studies have shown that APAs are adaptable through training, suggesting APAs as a potential therapeutic target to improve protective step execution and reduce falls.16,17 However, a more complete understanding of how APA size relates to protective step effectiveness is necessary to facilitate the design of such interventions. To our knowledge, no studies have related APAs prior to protective stepping to both anterior-posterior (AP) and ML stepping outcomes in people with PD. Furthermore, despite the relative instability in backward postural control in people with PD,18,19 previous studies investigating APAs in people with PD have examined only forward protective stepping. Finally, previous studies investigating relationships between step outcomes and APAs typically average APA characteristics across participants and multiple trials.10,11 Other approaches, such as multilevel modelling, allow for comparisons at the trial level. Given the variability of both APA and protective step performance, 3 these models can provide a more thorough quantification of the relationship between APAs and step performance.
The goal of this manuscript is to characterize the relationship between ML APA size and protective step effectiveness in people with PD. Understanding the relationship between APAs and protective step effectiveness will inform interventions aimed at improving steps and reducing falls via APA training. These data fill important gaps in previous literature by (1) assessing APAs in people with PD during forward and backward protective steps, (2) measuring both AP and ML stepping outcomes, and (3) utilizing a multilevel modeling approach, thus harnessing individual stepping data to characterize these relationships. We hypothesize that in people with PD, larger APAs prior to protective steps will be related to later and longer steps, with improved ML stability.3,10
Methods
Subjects
Twenty-eight people with idiopathic PD were enrolled. Inclusion criteria were currently taking levodopa, ability to stand without aid for >1 hour, no neurological diagnoses other than PD, and no orthopedic injuries in the previous 6 months that interfered with gait or balance. Participants were tested approximately 2 hours after taking their prescribed dose of levodopa. Disease severity was assessed with the Unified Parkinson’s Disease Rating Scale (UPDRS) Part III. Freezing of gait (FOG) status, that is, whether participants have or have not experienced FOG, was determined by the New Freezing of Gait (FOG) Questionnaire, NFoGQ. 20 Specifically, participants were placed in the freezing group (PD+FOG) if they self-report experiencing FOG in the previous 30 days. If they report not exhibiting FOG in the past 30 days, they were placed in the nonfreezing group (PD-FOG). APA and protective stepping outcomes from a portion of this dataset have been reported previously.12,21 However, the current analysis is distinct as it (1) reports a distinct and novel analysis of the data, correlating APA size to protective stepping outcomes, and (2) contains a larger group of participants.
Protocol
The experimental protocol has been described previously. 21 Briefly, participants stood barefoot with feet 2 cm apart on independent and hydraulically driven movable force plates embedded into the ground. These data were part of a larger collection that required feet be placed close together. Participants underwent repeated perturbations in which the ground moved quickly underfoot (15 cm, 56 cm/s, approximately 2.25 cm/s 2 ) 21 either forwards or backwards. Participants were instructed to “react naturally to the perturbation when trying to keep balance.” For all trials included, participants took at least 1 protective step. First, participants completed 12 practice perturbations to familiarize themselves with the perturbation and remove any “first trial” effects.22-24 Then participants underwent 50 additional perturbations (same size, velocity, and accelerations as noted above). All but one participant stepped on every perturbation exposure. Of the 50 trials, 25 were forward, resulting in a backward step, and 25 were backward, resulting in a forward step. Direction order/sequence was varied pseudo-randomly within blocks, and participants never experienced the same direction more than twice in a row. All participants experienced the same sequence of perturbations. Trials were completed in 5 blocks of 10 trials (5 forward, 5 backward) with breaks between blocks to reduce fatigue.
Data Reduction
Vertical ground reaction force under each foot (collected at 480 Hz) was used to calculate the global center of pressure (COP) for 2 seconds before, and 5 seconds after perturbations. COP data were low-pass filtered at 20 Hz using a fourth-order Butterworth filter. Marker data (used to calculate COM and kinematic stepping outcomes) were captured by a 10-camera Motion Analysis Corporation system at 120 Hz, and stored for offline processing. After identification of markers, marker trajectory data were low-pass filtered at 5 Hz.
Calculation of APAs
APAs were calculated as the ML movement of the COP prior to a step. 3 Anterior-posterior (AP) movements of the COP are also critical components of APAs; however, given the large AP shift of the support surface, we were unable to assess AP APAs. We calculated the size of the largest single ML COP movement toward the swing leg between 75 ms after the perturbation and first foot-off. 10 This approach provided a continuous outcome that could be more robustly correlated to stepping outcomes than a binary outcome (ie, APA or no APA).
Protective Stepping Outcomes
We correlated APA size to temporal (step latency) and spatial (step length, width) stepping outcomes. APA size was also correlated to stepping outcomes that incorporate both spatial and temporal outcomes, including margin of stability (MOS), COM position at foot off, total COM displacement, and clinical (MiniBEST [Mini-Balance Evaluation Systems Test], UPDRS Part III) outcomes. A schematic showing spatial outcome variables is shown in Figure 1.
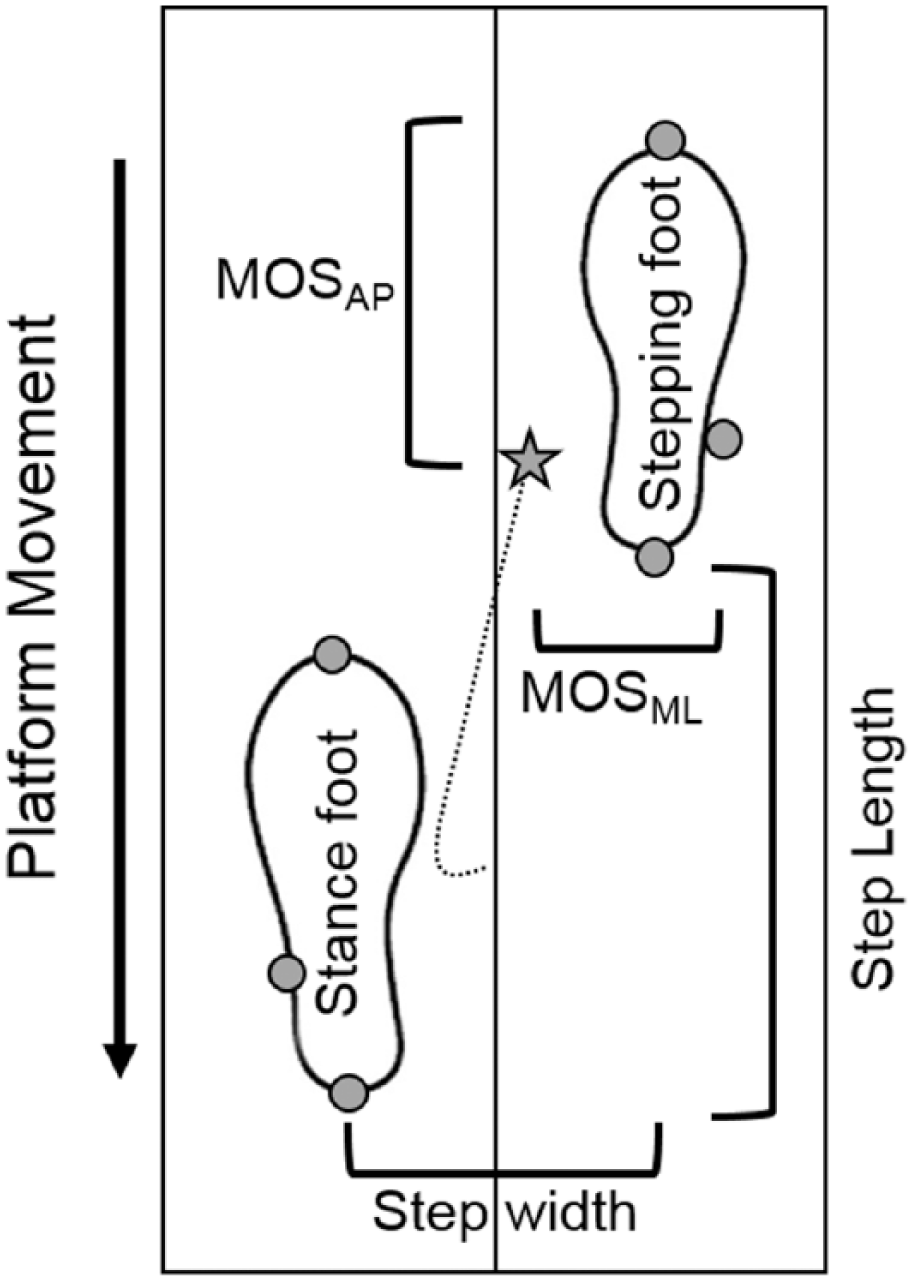
Schematic showing a forward protective step at the time of first foot contact and the associated spatial stepping outcomes in the anterior-posterior (AP) and mediolateral (ML) directions. The path (dotted line), and position (star) of the extrapolated center of mass (xCOM) is shown. The position of the xCOM at first foot contact dictates the margin of stability (MOS) in the AP (MOSAP) and ML (MOSML) directions.
Step latency was defined as the time between perturbation onset (ie, when the plates began to move) and step onset. Step onset was identified as the time point when the AP velocity of the toe-marker increased above 0.15 m/s. Visual inspection of the first 10 trials of each participant ensured that steps were appropriately identified. This is a notable departure from some previous literature,10,11 where step onset was identified via force-plate. In the current study, we investigated force-plate step identification. However, we observed several instances where steps were not picked up via force-plates because the foot slid across the ground during stepping. To calculate step length and step width, the position of the feet was first approximated by averaging the 3-dimensional position of the heel and toe markers. Then, step length and width were calculated as the AP and ML distances, respectively, between the 2 feet at first foot contact after the perturbation. To calculate COM displacement at foot off and total COM displacement, whole-body COM was first derived from the weighted sum of the individual limb COM locations using a custom-designed MATLAB program (Mathworks, Natick, MA), segment kinematics, and anthropometric data.25,26 Then the position of the COM at foot off (COMFO) relative to the initial starting position was calculated, such that larger values represent more COM movement. COMFO was calculated in the AP (COMFOAP) and ML (COMFOML) directions. COM displacement was calculated as the total AP distance that the COM traveled after the perturbation.
MOS, a measure of dynamic stability, was calculated as the position of the extrapolated COM relative to the base of support at the moment of first foot contact,27,28 such that larger values represent better performance. Extrapolated COM was calculated as the position of the vertical projection of the COM plus velocity of the COM, normalized to Wo, where Wo is equal to the square root of 9.81/leg length. 28 Extrapolated COM was calculated in the AP and ML directions, by taking the AP and ML components of COM position and velocity noted above and compared to edge of the base of support. For example, during backward stepping perturbations, MOS was defined as the distance between the AP extrapolated COM and heel marker of the stepping foot when that foot touches down. For forward stepping, MOS was defined as the distance between the AP extrapolated COM and the toe marker. For ML MOS (MOSML), the ML position of the extrapolated COM was compared with the position of the lateral malleolus of the stepping foot.
Statistical Analyses
Multilevel Analysis
Our goal was to understand the degree to which APA contributes to protective stepping performance for a set of dependent variables, accounting for several potential confounds. Given the step-to-step variability in APA and step characteristics, 29 we used linear mixed-effects regression to account for the multilevel nature of the data (ie, steps nested within participants 30 ). We used the same model-building procedure for each dependent variable. In short, models were constructed to identify the degree to which APA size was related to each protective stepping outcome. In addition to APA, each model included covariates of trial number, freezing of gait (FOG) status as determined by the NFoGQ, and the APA by FOG status interaction. It is important to control for these factors for several reasons. First, previous data show that step outcomes can change across the repeated perturbation exposures, 21 so including trial number as a factor controls for learning effects from trial-to-trial. Second, FOG status could affect the average level of performance, but FOG status could also affect the relationship between APAs and the step outcome. Thus, this model allows us to see if FOG status alters the relationship between APA and a given dependent variable while controlling for sequential trial effects.
Large deviations of initial COP position from midline could affect APA size and, potentially, the relationship between APA size and the effectiveness of the resulting step. As such, trials in which initial COP position or APA size was >2 standard deviations away from the overall group mean were excluded. This approach resulted in omission of approximately 7% of data (99 of 1345 trials excluded). We chose to remove these trials rather than include initial COP position in the statistical model for 3 reasons. One, including COP position would increase considerably the complexity of the statistical models. Two, it is not clear how COP variables should be modeled if they were to be included (eg, linear, curvilinear, or nonlinear relationships). Three, COP position may also depend on the kinematic alignment of the body, which was not explicitly considered in the current study.
For all models, we visually assessed the distribution of residuals for normality and heteroscedasticity. If normality was violated, we log-transformed the dependent variable and refit the model. This led to a more normal (but not necessarily normal) distribution of residuals, and in all but 3 cases (forward COM displacement, backward step length, and backward step width) did not change the direction or significance of the results. Furthermore, estimation of fixed-effects is relatively robust to violations of normality. 31 As such, we present the untransformed values in the Results section, indicate where these results disagree with log-transformed data, and we focus our discussion on only those effects that were statistically significant across both analyses. Data and code for all of the multilevel analyses are available from: https://github.com/keithlohse/PD_APAs.
Finally, we calculated the influence that individual participants had on each models’ fixed-effects using Cook’s distance calculations. 32
Bivariate Regression
We also correlated average APA size to clinical outcomes (MiniBEST and UPDRS). Given the nonnormality of APA data, Spearman’s ρ correlation coefficients were utilized for all bivariate correlation outcomes.
Statistical analyses were conducted in R 3.4.1.33-36 Degrees of freedom and P values for individual parameters used the Satterthwaite approximation due to the multilevel nature of the data. 37 A priori, the α level was set to .05 for all statistical tests.
Results
Twenty-seven of the original 28 participants were included in the analysis (characteristics reported in Table 1). The one excluded participant exhibited a large influence on APA-step latency models (Cooks distance = 80 and 11 for forward and backward models, respectively). Furthermore, during testing it was necessary to lower the perturbation speed for this participant, due to the severity of their impairment. For these 2 reasons, this participant was removed from all analyses. Of the included participants, 12 self-reported experiencing freezing in the previous month.
Participant Characteristics a .
Abbreviations: MoCA, Montreal Cognitive Assessment; MiniBEST, Mini-Balance Evaluation Systems Test; UPDRS, Unified Parkinson’s Disease Rating Scale.
N = 27 (18 males).
Table 2 shows parameter estimates for all models indicating the relationship between protective stepping outcomes (in rows) and APA size, trial number, FOG status, and the APA by FOG status interaction (in columns). Models for forward and backward stepping are shown in the top and bottom halves of the table, respectively. Models in which normality was violated are indicated in the table. Results for each stepping outcome are presented in detail below.
Model Results Relating Protective Stepping Outcomes (Rows) to Mediolateral Anticipatory Postural Adjustment (ML APA) Size a .
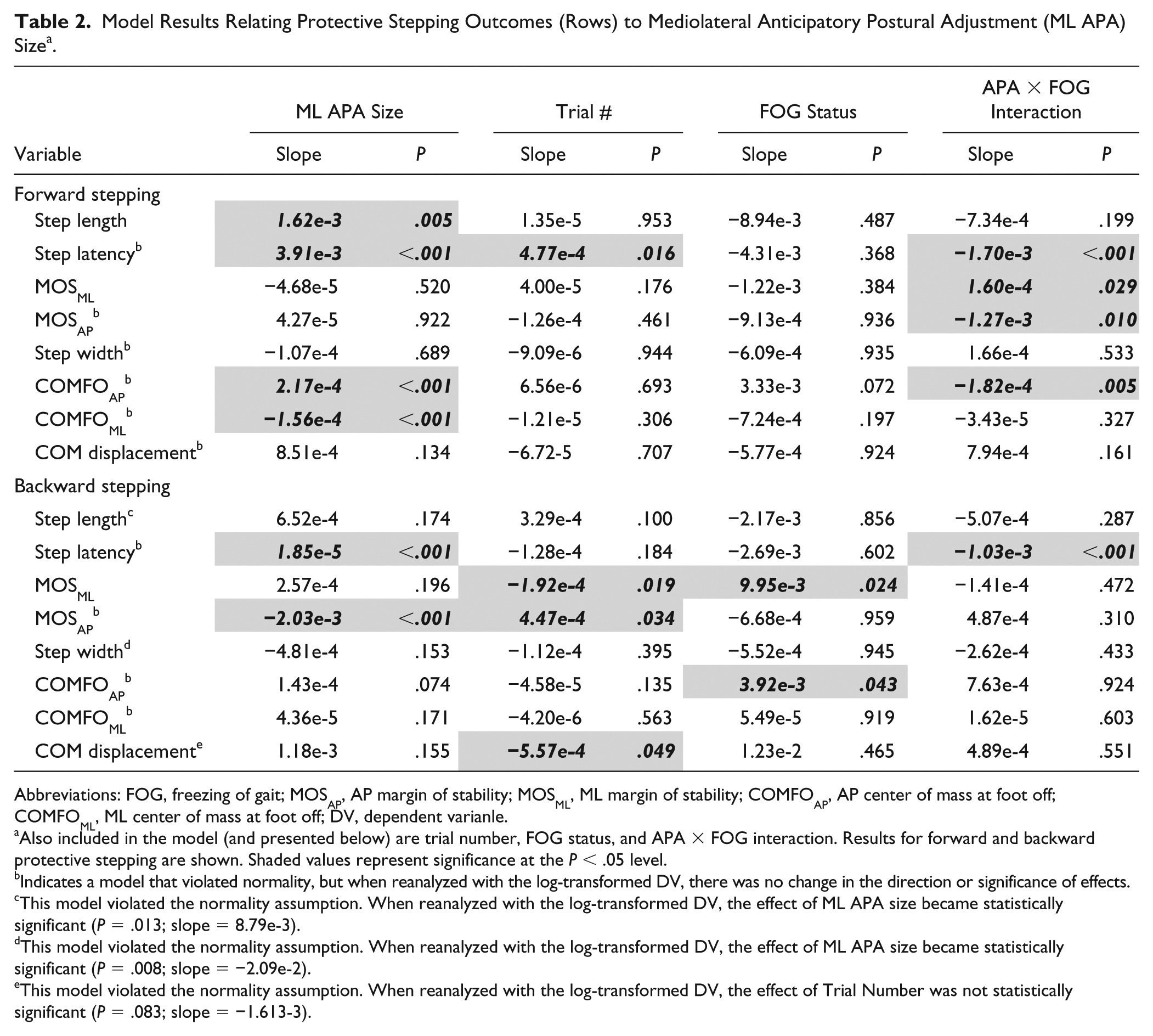
Abbreviations: FOG, freezing of gait; MOSAP, AP margin of stability; MOSML, ML margin of stability; COMFOAP, AP center of mass at foot off; COMFOML, ML center of mass at foot off; DV, dependent varianle.
Also included in the model (and presented below) are trial number, FOG status, and APA × FOG interaction. Results for forward and backward protective stepping are shown. Shaded values represent significance at the P < .05 level.
Indicates a model that violated normality, but when reanalyzed with the log-transformed DV, there was no change in the direction or significance of effects.
This model violated the normality assumption. When reanalyzed with the log-transformed DV, the effect of ML APA size became statistically significant (P = .013; slope = 8.79e-3).
This model violated the normality assumption. When reanalyzed with the log-transformed DV, the effect of ML APA size became statistically significant (P = .008; slope = −2.09e-2).
This model violated the normality assumption. When reanalyzed with the log-transformed DV, the effect of Trial Number was not statistically significant (P = .083; slope = −1.613-3).
Effect of APA Size on Stepping Outcomes
During forward protective stepping, larger APAs were associated with larger and later steps. Larger APAs were also associated with larger AP COM displacement at foot off (COMFOAP), and smaller ML COM displacement at foot off (COMFOML); see Table 2 and Figure 2.
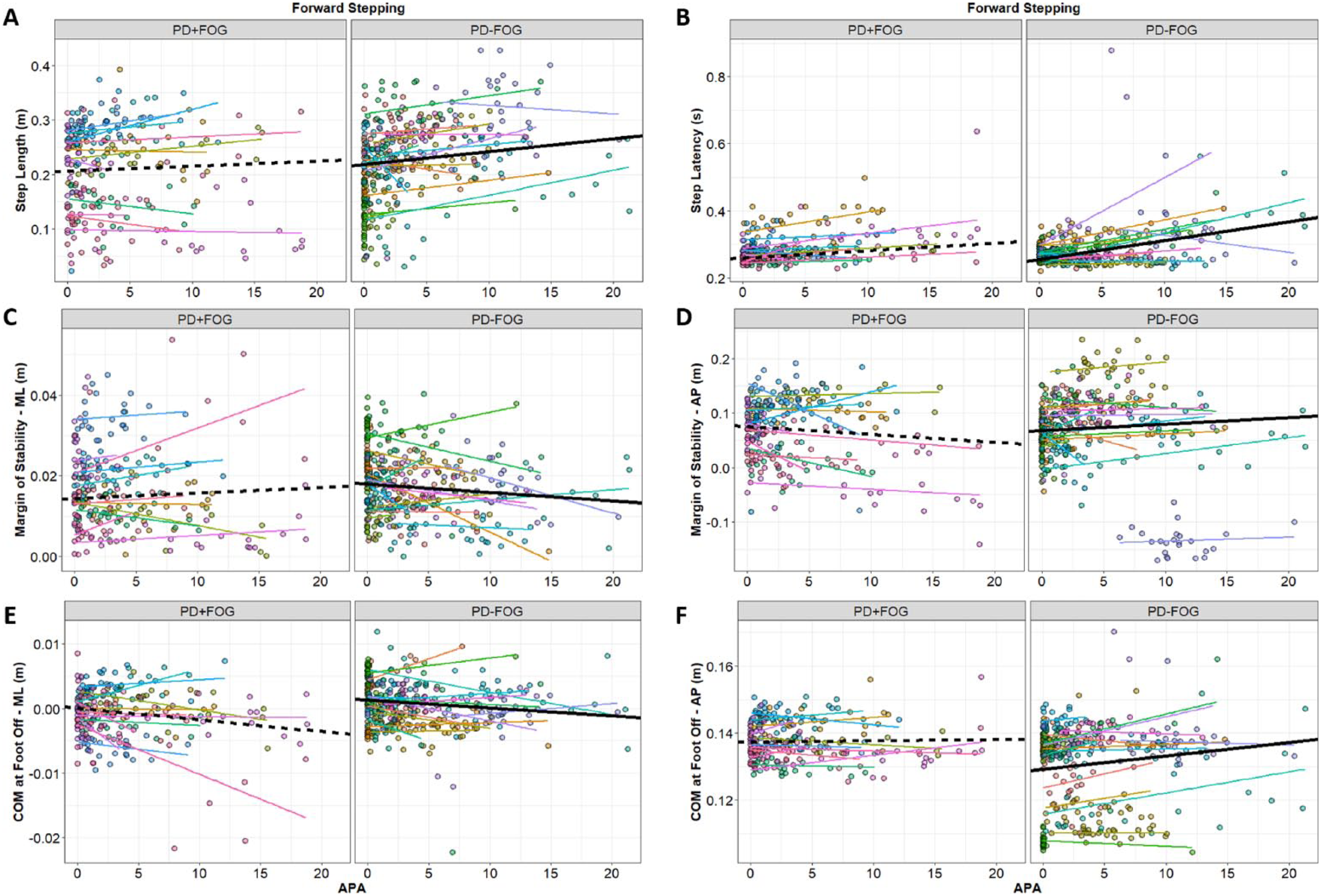
Relationship between APA size and stepping outcomes during forward stepping: (A) step length, (B) step latency, (C) ML-MOS, (D) AP-MOS, (E) ML-COM at foot-off, and (F) AP-COM at foot-off. Data points are color coded by the individual participants, and thin lines show the line of best within each participant. Thick lines represent the fixed-effect estimates from Table 2 (solid lines for nonfreezing group, PD-FOG, and dashed lines for the freezing group, PD + FOG).
During backward stepping, larger APAs were associated with later steps, and smaller (ie, worse) MOSAP (see Table 2 and Figure 3).
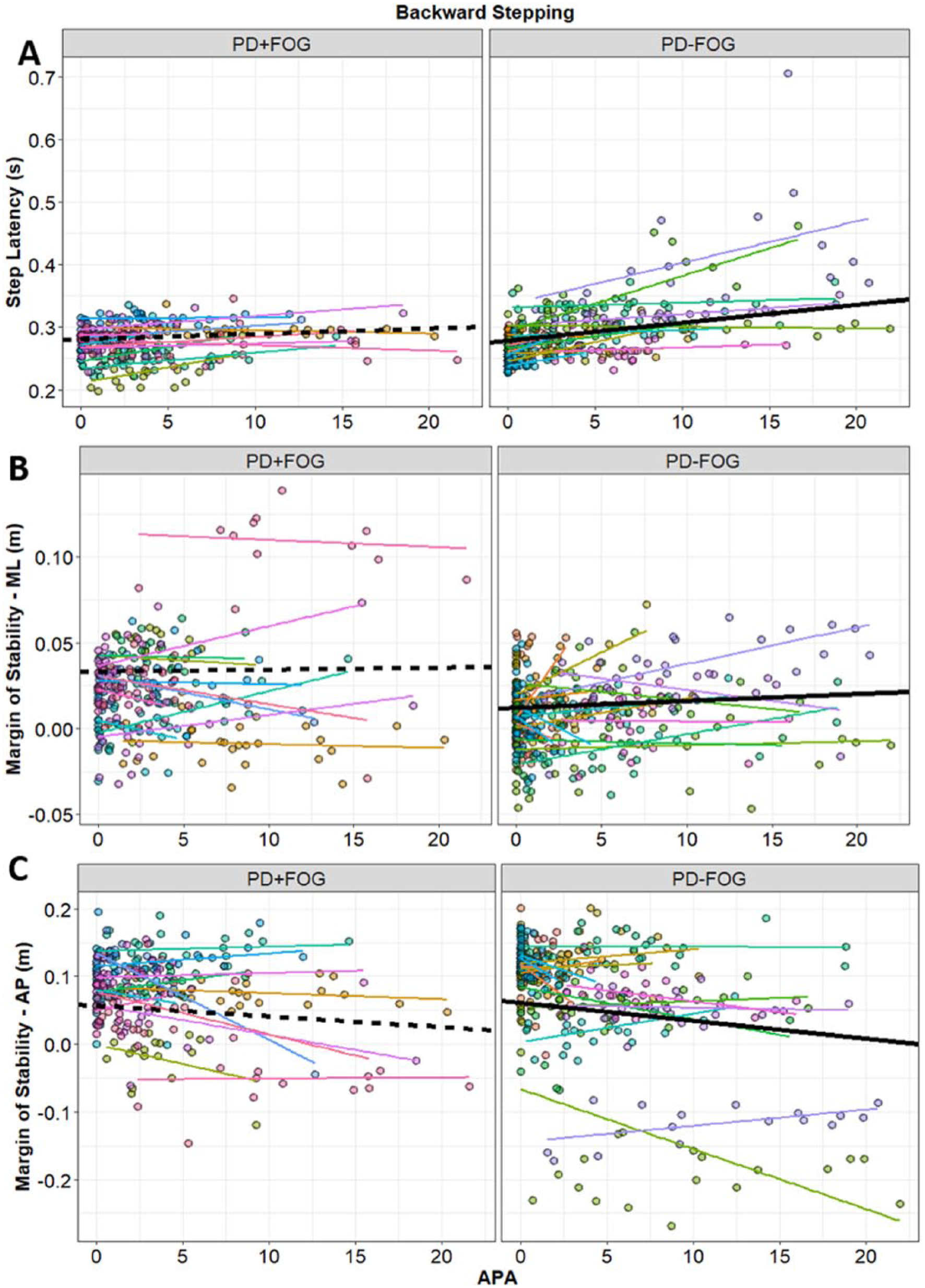
Relationship between APA size and stepping outcomes during backward stepping: (A) step latency, (B) ML-MOS, and (C) AP-MOS. Data-points are color coded by the individual participants, and thin lines show the line of best within each participant. Thick lines represent the fixed-effect estimates from Table 2 (solid lines for nonfreezing group, PD-FOG, and dashed lines for the freezing group, PD + FOG).
Effect of Trial Number on Stepping Outcomes
Trial number was a significant covariate for AP and ML MOS and COM displacement (for backward stepping) and step latency (for forward stepping). Specifically, and similarly to previous results, MOSAP and COM displacement both improved (increased and decreased, respectively) over the testing period during backward stepping (see Figure 4). Notably, however, the COM displacement relationship was not statistically significant when COM displacement was log-transformed (following a nonnormal distribution of residuals), so this effect should be treated with caution. In contrast to previous results 21 , Step latency increased across trials for forward stepping. This discrepancy may be partially due to the method of analysis: previous research ignored interrelationships between sequential effects and APAs, whereas this time-varying covariate is controlled for in the current analysis. Finally, MOSML became smaller over the course of testing for backward stepping.
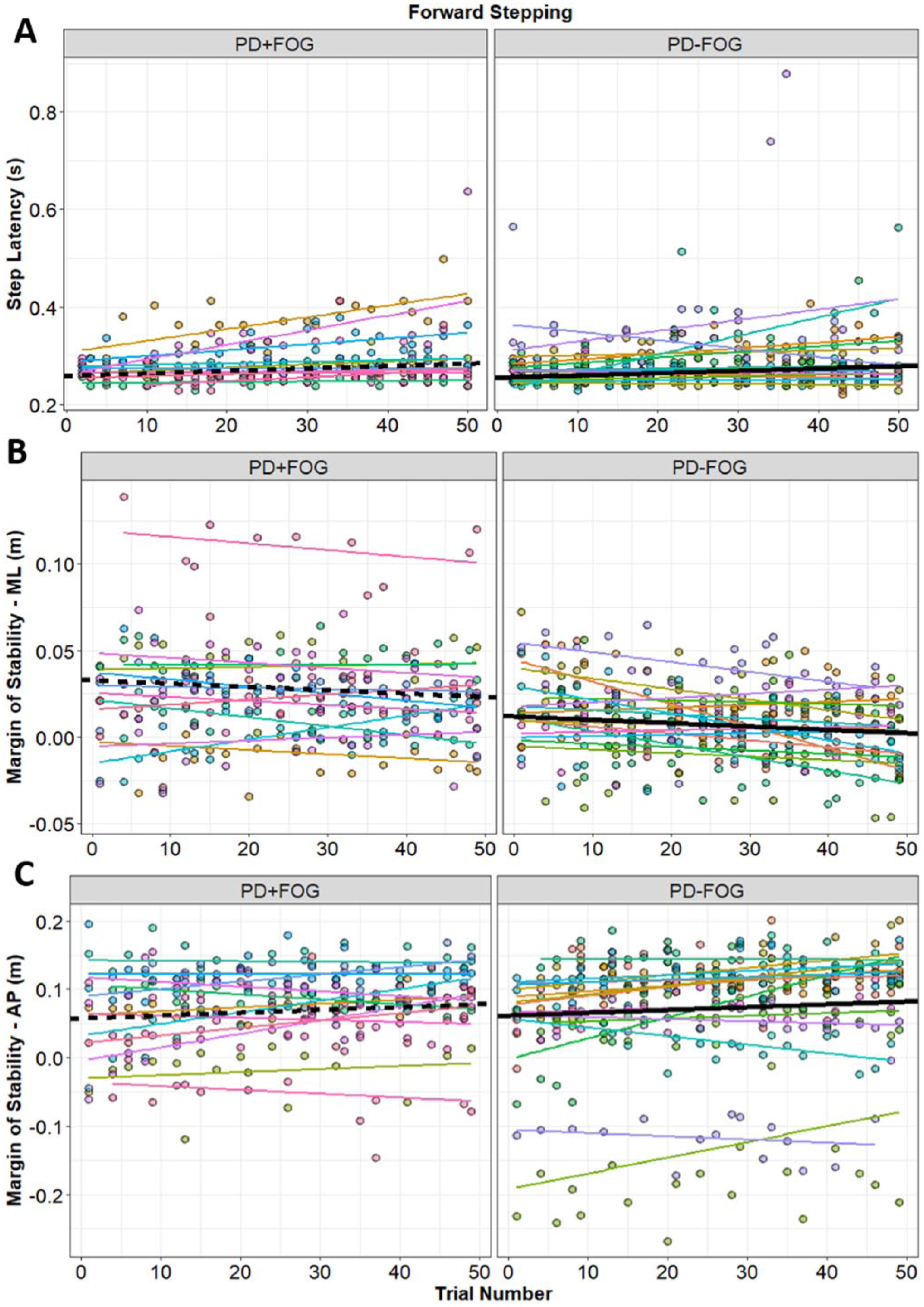
Relationship between trial number for forward and backward stepping: (A) forward step latency, (B) backward ML-MOS, and (C) backward AP-MOS. Data-points are color coded by the individual participants, and thin lines show the line of best within each participant. Thick lines represent the fixed-effect estimates from Table 2 (solid lines for nonfreezing group, PD-FOG, and dashed lines for the freezing group, PD + FOG).
Effect of FOG Status on Stepping Outcomes
Subtle but statistically significant effects of FOG status were observed, such that PD + FOG exhibited larger COMFOAP and MOSML compared to PD-FOG during backward stepping.
APA Size by FOG Status Interaction
Stepping outcome by FOG status interactions were primarily observed during forward stepping. Significant interactions were observed for step latency, MOSML, MOSAP, and COMFOAP. For MOSML, PD + FOG had a more positive relationship between these outcomes and APA size compared to PD-FOG. For MOSAP, step latency, and COMFOAP, PD-FOG had a more positive relationship between these outcomes and APA size compared to PD + FOG. For backward stepping, the only observed APA by FOG interaction was for step latency. As with forward stepping, PD-FOG had a more positive relationship between step latency and APA size than PD + FOG.
Relationship Between APA Size and Clinical Outcomes
Correlation analyses were carried out between average APA size, age, UPDRS-III, and MiniBEST. During backward stepping, average APA size was significantly correlated to UPDRS-III (ρ = 0.52; P = .005) and MiniBEST scores (ρ = −0.43; P = .02), but not age (ρ = 0.25; P = .20), such that larger APAs were related to worse scores on both assessments. Age, UPDRS-III, and MiniBEST were not statistically significantly correlated to average APA size during forward protective stepping (P = .50, .10, and .15, respectively).
Discussion
This study is the first to thoroughly describe the relationship between APA size and protective stepping outcomes in people with PD. Results show that, during forward protective stepping, larger APAs are related to steps which (1) are delayed, (2) are larger, (3) have less ML COM movement prior to foot off, and (4) have more AP COM movement prior to foot off. During backward stepping, larger APAs were related to delayed steps with smaller (ie, worse) MOSAP at the moment of first foot contact. Furthermore, APA size prior to backward, but not forward protective stepping was related to worse clinical outcomes. In sum, during forward stepping, large APAs seem to have mixed effects on protective stepping outcomes. However, during backward protective stepping, larger APAs were predominantly related to worse stepping outcomes (ie, later steps with smaller MOSAP). Understanding these relationships between APA size and the subsequent protective steps can inform therapies aimed at improving protective steps.
During protective stepping, the presence of APAs is associated with delayed steps in both healthy adults 15 and people with PD.10,11 The current analysis supports this hypothesis, showing that in people with PD, protective steps proceeded by large APAs were later than those proceeded by smaller APAs. Perhaps unsurprisingly, given the delayed stepping onset, the COM position at foot off (COMFOAP) was also further forward in trials with large APAs. For both forward and backward protective stepping, there was a significant interaction effect between the latency-APA relationship and FOG status. For both directions, the PD-FOG group exhibited a more positive slope between APA size and step latency. Together, this work suggests that for both forward and backward protective stepping, larger APAs delay the onset of the step, particularly in PD-FOG. Given the importance of quickly releasing protective steps after a loss of balance, these later steps could increase the instance of falling.
Despite the potential detrimental effect of APAs on step latency, APAs may also facilitate a larger step. Indeed, we show larger APAs were related to larger protective step length during forward protective steps. The relationship between APA size and forward protective step length partially contradicts King et al, who showed that in people with PD, protective step lengths were not statistically different on trials with or without APAs. 11 The rationale for this distinction is not entirely clear, but may be related to different data analysis techniques. The current study correlated the size of APAs on individual trials to step outcomes (including step length), across 25 forward steps and 28 participants (ie, approximately 700 individual trials), via multilevel statistical models. Evaluating a larger number of APAs prior to protective steps, and in a continuous, rather than categorical, manner increases statistical power,38,39 thus increasing our ability to detect a relationship between APA and step length size.
Interestingly, larger APAs were not related to larger step length during backward protective stepping. In fact, during backward stepping larger APAs were related to smaller (ie, worse) MOSAP. MOSAP can be affected by a number of factors, including the length and latency of steps. 28 During forward stepping, although APA size was related to later steps, it was also related to longer steps, potentially reducing the overall APA size–MOSAP relationship. In contrast, during backward steps, APA size was related to later steps, but not longer steps. This delay, without a concomitant lengthening of the step, may have resulted in the APA size–MOSAP relationship for backward protective stepping. However, this raises the question—why might larger APAs relate to longer forward, but not backward protective steps? Although speculative, this may be the result of biomechanical differences between stepping directions. Indeed, previous reports in healthy and neurological populations show that backward protective stepping is typically shorter, narrower, and faster than forward protective stepping.40-42 Furthermore, increased range of motion for hip flexion, compared to extension, and knee flexion both allow for larger step length during forward stepping. Finally, standing humans have a decreased ability to exert dorsiflexion torque (necessary to correct for backwards loss of balance) compared to plantar flexion torque. 43 It is therefore possible that these biomechanical aspects of backward stepping are more important at affecting step size during backward protective stepping than the ML position of the COM.
Given the importance of controlling the COM in both the AP 44 and ML45,46 directions, we related APA size to step characteristics and COM control in both the AP and ML directions. Of these analyses, the only ML outcome that was related to APA size was COM displacement between perturbation onset and foot off (COMFOML) during forward protective stepping. Specifically, larger APA size was associated with less lateral movement prior to foot off. This finding is somewhat unsurprising, as a larger APA may have prevented lateral displacement of the COM prior to foot off. Notably, there were no significant relationships between APA size and ML stepping outcomes such as step width or ML MOS, suggesting that despite reducing ML COM movement prior to foot off, APA size had a limited effect on ML protective stepping outcomes.
Trial number was integrated into all models in order to assess the APA-stepping outcome relationship without potential confound of changes in protective stepping outcomes with repeated perturbation exposure. Change in stepping outcomes over time has been analyzed previously in a subset of the current dataset via mixed-model repeated-measures ANOVAs. Generally, results are similar between these previous results, 21 and the current report. Specifically, MOSAP increased and COM displacement decreased over time during backward stepping, but not forward stepping. These changes represent improvements in protective stepping, as participants were able to increase the distance between their COM and limit of stability at first foot contact (MOSAP), and decrease the overall distance traveled by the COM after the perturbation (COM displacement). Interestingly, MOSML (which was not analyzed in the previous study 21 ) was reduced over time. Lower MOSML represents a smaller distance between the outer base of support (edge of foot) and the extrapolated COM at the moment of foot contact. Furthermore, and unlike previous analyses, there was a subtle but significant effect of step latency, such that latency became larger over time during forward stepping. These effects (smaller MOSML and later steps) may reasonably be perceived as worse stepping over training. Alternatively, these outcomes may reflect participants becoming more familiar and comfortable with the support surface translations over time. Indeed, Nonnekes and colleagues 47 suggest that postural perturbations can be startling in nature, thus potentially decreasing latency of movement. Therefore, in the current study, participants may have partially habituated to the stimulus over the course of repeated perturbation exposures, thus resulting in later steps or smaller MOSML. While additional work is necessary to understand why these 2 specific variables became worse with exposure, investigations from our laboratory21,48 and others49,50 suggest that, generally, perturbation training is beneficial for improving steps and reducing falls 50 in people with PD. Furthermore, we recently showed that APA size was also reduced after perturbations but prior to backward protective stepping in people with PD with repeated perturbation exposures. 51 However, whether interventions specifically aimed at altering APAs prior to protective stepping impact protective steps is currently unknown.
Finally, it is notable that when averaged within participants, APA size during backward protective stepping was correlated to worse clinical outcomes (UPDRS and MiniBEST), suggesting APA amplitude may be related to global balance and motor dysfunction outside of protective stepping. To our knowledge, only one previous study has related APA size prior to protective stepping to PD clinical symptoms, showing that APA amplitude was not related to UPDRS. 11 As such, these findings should be treated with caution until additional data can confirm or refute these findings.
Limitations and Other Considerations
First, we assessed APAs in a relatively mild group of people with PD who do and do not freeze. More severe participants with increased freezing severity may exhibit more pronounced changes in both APAs and stepping characteristics, thus changing the relationships observed in the present study. Similarly, larger perturbation sizes may elicit more pronounced differences across groups. Second, while step latency was similar between the current study and previous studies, APA size was smaller than previously reported. 11 This may be because, for all trials, participants stood with their feet together. Also, as noted above, we used marker movements to evaluate which foot stepped first and the latency of this step, as opposed to force-plates. While neither approach is without limitations, the analysis method could have meaningful impacts on observations and conclusions. Indeed, we observed that, in some trials of the current dataset, force-plate–based step detection did not identify small steps, as the foot slid across the force-plate, never fully unloading the force-plate. Therefore, classification of very small steps as a large APA (but no step), or vice versa, could affect outcomes. This raises an important point regarding both the identification of stepping during protective balance, as well as the calculation of APAs, and requires further investigation.
Finally, the novel multilevel modelling approach we employed allows investigation of trial-by-trial variation in APAs and their relationship to step characteristics. Given the variability of these outcomes across trials, this approach provides considerably increased power to assess such relationships. However, there are some challenges to using this approach. For instance, although all models met assumptions of homoscedasticity of residuals, some models violated assumptions for normality of residuals, which can bias estimates of standard errors. 52 Transformations of dependent measures did not fully address this violation, and different transformations were implemented for different sets of variables (depending on positive or negative skew of the dependent variable). However, multilevel models are robust to violations of normality. Therefore, we chose to present the untransformed data in our figures and analyses. Similarly, there was considerable heterogeneity in individual slopes and intercepts. Thus, despite a number of significant fixed effects, this heterogeneity suggests that there is residual variance that could be explained by other factors.
Conclusions
APA size is related to protective step outcomes during both forward and backward perturbations. During backward protective stepping, larger APAs are related to later steps with smaller (ie, worse) MOS, suggesting that efforts to reduce APAs prior to backward protective stepping may improve subsequent step characteristics. During forward protective stepping, APAs are related to larger, but later steps, with less ML COM displacement prior to foot off. Although additional work will be necessary to understand which protective stepping outcomes (spatial, temporal, AP, ML, etc) are most closely related to falls, efforts to train and improve APAs prior to forward protective stepping should consider the complex relationship between APA size and protective stepping.
Footnotes
Author Contributions
Dr Peterson contributed to all aspects of the project (conception, organization, and execution of research; design and review/critique of statistical analysis; writing of the first draft and review and critique of the final draft). Drs Lohse and Mancini contributed to design, execution, and review/critique of the statistical analysis, and review/critique of the manuscript drafts. Dr Peterson takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Peterson and Lohse have no conflicts of interest to report. Dr Mancini has served as a consultant for Axovant and Cadent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported directly by the US Department of Veteran’s Affairs Rehabilitation Research and Development Service (Career Development Award-1: #I01BX007080; PI: DSP) and the Medical Research Foundation of Oregon (Early Investigator Award; PI: DSP). Over the past 12 months, authors have also been funded by the Canadian Institutes of Health Research (PTJ 153330; CoI: KRL), Auburn University Internal Grants Program (IGP Project # 170138; PI: KRL), Federal Aviation Administration—Center for Excellence for Teaching Training and Human Performance (FAA 16-C-TTHP-AU; CoI: KRL), and the NIH: Career Development Award R00 HD078492 (PI, MM) and SBIR 1R43AG056012-01 (CoI: MM). The contents do not represent the views of the US Department of Veterans Affairs or the US government.