
Abstract
Background. The added prognostic value of transcranial magnetic stimulation (TMS)-induced motor-evoked potentials (MEPs) to clinical modeling for the upper limb is still unknown early poststroke. Objective. To determine the added prognostic value of TMS of the adductor digiti minimi (TMS-ADM) to the clinical model based on voluntary shoulder abduction (SA) and finger extension (FE) during the first 48 hours and at 11 days after stroke. Methods. This was a prospective cohort study with 3 logistic regression models, developed to predict upper-limb function at 6 months poststroke. The first model showed the predictive value of SA and FE measured within 48 hours and at 11 days poststroke. The second model included TMS-ADM, whereas the third model combined clinical and TMS-ADM information. Differences between derived models were tested with receiver operating characteristic curve analyses. Results. A total of 51 patients with severe, first-ever ischemic stroke were included. Within 48 hours, no significant added value of TMS-ADM to clinical modeling was found (P = .369). Both models suffered from a relatively low negative predictive value within 48 hours poststroke. TMS-ADM combined with SA and FE (SAFE) showed significantly more accuracy than TMS-ADM alone at 11 days poststroke (P = .039). Conclusion. TMS-ADM showed no added value to clinical modeling when measured within first 48 hours poststroke, whereas optimal prediction is achieved by SAFE combined with TMS-ADM at 11 days poststroke. Our findings suggest that accuracy of predicting upper-limb motor function by TMS-ADM is mainly determined by the time of assessment early after stroke onset.
Introduction
Voluntary shoulder abduction (SA) and finger extension (FE) measured within 72 hours after stroke have been shown to be important determinants for upper-limb capacity at 6 months poststroke.1-3 However, despite the high positive predictive value (PPV) of this SA and FE (SAFE) model when applied within 3 days poststroke, 1 a relatively large number of patients without initially voluntary FE have been shown to be false negatives as a result of experiencing spontaneous return of FE in the first 3 months poststroke. 4 Patient’s ability of voluntary FE is believed to reflect the intactness of the corticospinal tract system (CTS) early poststroke.1-4
Several prospective cohort studies have shown that the integrity of the CST can be reliably and validly determined by transcranial magnetic stimulation (TMS)-induced motor-evoked potentials (MEPs) of the adductor digiti minimi (ADM), the first dorsal interosseous, or abductor pollices brevis (APB) muscle. 5 TMS-MEPs were obtained within 2 days to 3 weeks poststroke onset. 5 A few prognostic studies were retrospectively conducted, and most studies recruited small samples of stroke patients ranging from 6 to maximally 52 stroke patients. 5 In addition, comparability between the prospective studies is hindered by differences in (1) criteria of recruiting stroke patients, (2) timing of measurements poststroke, (3) differences in initial motor impairment, and (4) differences in defining and timing of final outcome of upper-limb function. Furthermore, assessing the added value of the accuracy of TMS-MEPs to clinical modeling is hindered in most studies by not providing insight into the uncertainty that is associated with the accuracy of each prediction by failing to report 95% CIs for sensitivity, specificity, and positive and negative predicted values. Finally, most studies found a predictive value of TMS-MEPs for outcome of upper paretic limb function, but none of these studies investigated the added value of TMS to clinical modeling alone when measured at the same day very early poststroke.
Based on the aforementioned methodological shortcomings and differences in objectives, the surplus value of MEPs elicited with TMS in the acute stage is still unclear for outcome of upper-limb function in patients with a first-ever ischemic hemispheric stroke.
The first aim of the present study was to determine the prognostic value of SAFE and TMS-MEPs of the ADM (TMS-ADM) in predicting upper-limb motor function at 6 months in severe strokes when applied independently within the first 48 hours and at 11 days poststroke. The second aim was to determine if TMS-ADM improved the accuracy of predicting upper-limb function by the SAFE model when assessed within 48 hours or at 11 days poststroke.
Materials and Methods
Participants
Patients with a first-ever, ischemic hemispheric stroke as revealed by MRI or CT scan were prospectively screened for eligibility and when possible recruited at a hospital department of neurology in the Netherlands from August 11, 2004, until July 13, 2007. Stroke severity and etiology were classified following the TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria 6 within 24 hours by an experienced neurologist (PJSvdB) who was blinded for the TMS-ADM. To participate in this study, patients had to be hospitalized within the first day after the onset of symptoms with unilateral paralysis or significant paresis as defined by the National Institutes of Health Stroke Scale motor arm item: 0 < score < 5. 7 Patients were excluded if (1) they had loss of consciousness; (2) they had peripheral nerve pathology, including diabetes and neuromuscular disease; (3) they were unable to receive rehabilitation because of severe comorbidity; and (4) contraindications to TMS were present, such as epileptic seizures, syncope, accompanying diagnosis of head trauma, hearing problems, cochlear implants, pregnancy, metal in the brain or skull, implanted devices such as cardiac pacemaker and/or intracardiac lines, medication infusion device.8-10
All patients gave their written informed consent, and all patients were treated according to the Dutch physical therapy guidelines of rehabilitation. 11 This included early out-of-bed mobilization within 24 hours poststroke, daily physical therapy interventions related to upper-limb training, and gait- and mobility-related functions and activities. 11 The study protocol was approved by the local medical ethics committee.
Dependent Variable
The outcome in terms of upper-limb motor function was assessed at 6 months poststroke with the Fugl-Meyer upper-extremity motor score (FM-UE). The FM-UE test was administered by an experienced rehabilitation physician (MHJH) who was not aware of the TMS-ADM results. The FM-UE test is a widely used measure to assess impairments of the upper limb after stroke and has been recommended as a robust measure to evaluate the ability to make arm movements outside the synergistic pattern. 12 The test covers 5 hierarchical stages of motor recovery poststroke and contains 33 test items for the upper paretic limb. 13 The 33 items are divided into 4 subsections: shoulder-arm, wrist, hand, and upper-limb coordination. Each test item is scored on a 3-point ordinal scale, with a maximal total score of 66 points. The maximal score indicates maximal motor recovery, equaling normal motor performance. The clinimetric properties such as intraobserver and interobserver reliability; concurrent, predictive, content, and construct validity; and responsiveness of the FM-UE test are well established.12,14,15 Recently, we showed after screening 460 patients with a first-ever ischemic stroke at 6 months that FM-UE scores below 22 points correspond to “no” or “poor upper-limb capacity” based on the Action Research Arm Test (ARAT), whereas scores above 22 points represent limited to full upper-limb capacity based on the ARAT at 6 months. 16 Therefore, we dichotomized return of motor function into those who regained ≥22 points on the FM-UE (ie, favorable recovery) and those who stayed below 22 points (ie, unfavorable recovery) at 6 months poststroke.
Independent Variables
Age, gender, left/right hemispheric stroke, dysphagia, disorientation, and initial Barthel Index 17 at stroke onset were selected as clinical descriptors for baseline characteristics of the population. 18 The SAFE model was used for predicting upper-limb function at 6 months instead of 26 weeks poststroke, measured within 48 hours (first assessment) and at 11 days (second assessment) poststroke. In line with a previous prognostic study, FE was assessed with dichotomized scores of the FM-UE test using a cutoff score of ≥1 on this specific item. SA was assessed with the Motricity Index (MI), using a cutoff score of ≥9 on this specific item. 1 Nine points on the MI correspond with 1 point on the Medical Research Council Scale, reflecting visible contraction without segment movement. 1
Stimulation Procedure
The TMS technique, including measurement of MEP-ADM with EMG recordings (Nihon Kohden Neuropack 8, Nihon Kohden, Tokyo, Japan), was performed according to the recommendations of the International Federation of Clinical Neurophysiology.10,19). The primary motor cortex (M1) was stimulated with a calibrated Magstim Dantec Maglite (Dantec Dynamics, Bristol, UK). Cortical TMS was applied through a figure-of-eight shaped coil. First, the hotspot that produced the highest MEP amplitude of the abductor digiti minimi (ADM) muscle was determined by moving the coil over the scalp in the hand area of M1 of the nonlesioned hemisphere, with the stimulator at submaximal output. Subsequently, the coil positioning at the optimal position (hotspot) was mirrored to the lesioned hemisphere to elicit a MEP. A positive MEP was defined as the presence of at least 3 responses out of 3 stimuli producing a MEP amplitude of >50 µV.8,19 When no MEP could be elicited at a given position, the coil was slightly moved to find a hotspot in adjoining sites. Cervical stimulation was performed with a 90-mm circular coil to activate motor roots at the exit foramina centered over the C7/C8 cervical spine. 19 Besides proximal muscles, the ADM is one of the preferred intrinsic muscles that can easily be examined as a target muscle for TMS analysis. 19 Although all intrinsic hand muscles have nearly the same latency values, the ADM was chosen because of the relatively large data collection of normal values and bigger central representation in comparison to proximal target muscles. 19 Alternatively, TMS measurements can readily be recorded from the intrinsic hand muscles. However, the anatomical arrangement of extrinsic, more proximal muscles in the forearm muscles, such as the extensor carpi radialis muscle, just make it more difficult to record from the target muscle in isolation, resulting in polyphasic waveforms. 19 TMS-ADMs were evaluated by 2 experienced, independent assessors. Both assessors were blinded with regard to the results of the clinical assessments. In a previous study, we showed that the intraobserver and interobserver reliability of assessing TMS-ADM in 18 stroke patients and 8 healthy age-matched controls was found to be good to excellent (0.45 < κ < 0.87). 20 The TMS technique, including EMG recordings, was performed according to the recommendations of the International Federation of Clinical Neurophysiology. 10
Data Analysis
Three prediction models were developed to predict upper-limb motor function. The first model included clinical assessments alone, using voluntary SA and FE, measured within 48 hours and at 11 days poststroke. In the second model, the predictive value of TMS-ADM was investigated, whereas in the third model, the variables SA, FE, and TMS-ADM were combined for both assessment times. With regard to the third model, regression analysis was used with the manually conducted stepwise backward selection method. This involved starting with all 3 variables, deleting the variable (if any) that improved the model the most by being deleted, and repeating this process until no further improvement was possible. Multivariate logistic regression was used to calculate the probability of upper-limb motor function at 6 months poststroke using the following equation: P = 1/{1 + exp[−(B0 + B1X1 + B2X2 . . . BnXn)]}. A 2-way contingency table was used to calculate specificity, sensitivity, PPV, and negative predictive value (NPV) with corresponding 95% CIs. Receiver operating characteristic (ROC) curves of the different models at both time points poststroke were graphically displayed. Subsequently, differences between AUCs were tested for significance. For each comparison, a z-statistic was calculated using the equation: z = AUC1 − AUC2/√(SE1 2 + SE2 2 − 2rSE1SE2) with r representing the Pearson product moment correlation coefficient between the 2 models. 21 The calculated z-statistic was defined significant if z ≥1.96. To maintain adequate power for the statistical analysis, we complied with the events per variable rule, which calls for at least 10 outcomes for each variable in the regression model. 22 All tests were applied 2-tailed, with a critical value of α <.05 using SPSS software (SPSS version 21.0 SPSS Software: IBM Corporation, Armonk, New York, NY).
Results
Table 1 shows the main demographic and clinical characteristics of the study sample. Figure 1 shows the flowchart of 51 participants recruited with a first-ever, ischemic hemispheric stroke. One participant was lost to follow-up after the first measurement because of migration outside the region. At 6 months poststroke, 32 (64%) participants showed FM-UE scores of 22 points or higher, of whom 6 (12%) participants showed complete motor function (i.e., 66 points on FM-UE). None of the participants reported discomfort during the TMS assessments. TMS-ADM at 48 hours and 11 days were present in 18 (36%) and 32 participants (64%), respectively.
Demographic and Patient Characteristics Within 48 Hours After Stroke Onset.
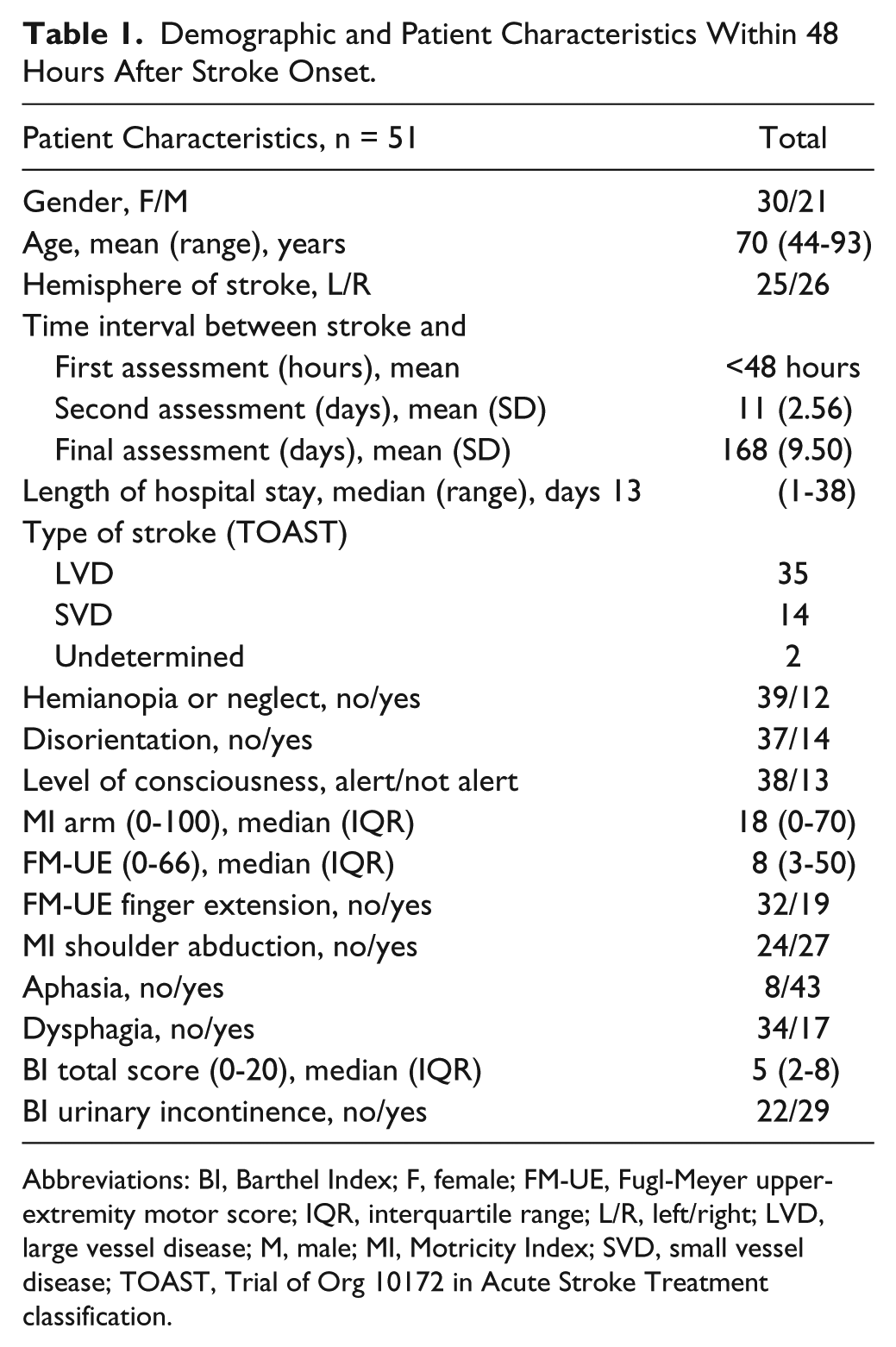
Abbreviations: BI, Barthel Index; F, female; FM-UE, Fugl-Meyer upper-extremity motor score; IQR, interquartile range; L/R, left/right; LVD, large vessel disease; M, male; MI, Motricity Index; SVD, small vessel disease; TOAST, Trial of Org 10172 in Acute Stroke Treatment classification.
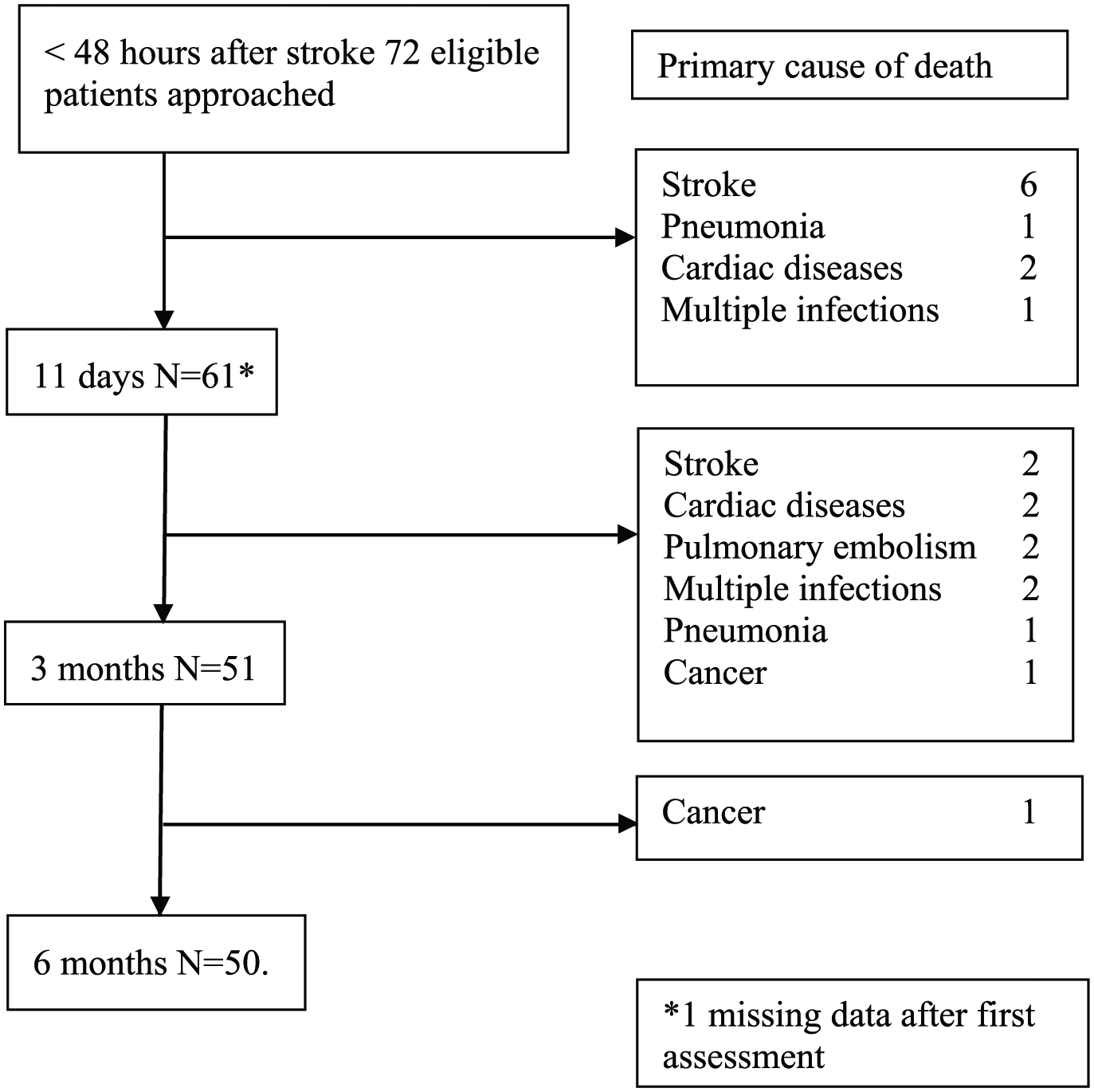
Flowchart for recruitment of first-ever, cortical ischemic hemispheric stroke patients within 48 hours and follow-up combined with dropout at 11 days, and 3 and 6 months poststroke.
Table 2 shows the SAFE model for the probability to achieve some upper-limb motor function 6 months after stroke. The probabilities when both SA and FE were present within 48 hours and at 11 days poststroke were .95 and .94, respectively. The probability of achieving some dexterity when SA and FE were both absent was estimated to be .38 within 48 hours and further decreased to .13 at 11 days poststroke. Table 2 shows also the 2-way contingency table analysis of this prediction model with SA and FE. Within 48 hours, sensitivity of the SAFE model was 0.56 (95% CI = 0.45-0.59), specificity 0.94 (95% CI = 0.75-1.00), PPV 0.95 (95% CI = 0.76-1.00), and NPV 0.55 (95% CI = 0.44-0.58). At 11 days, sensitivity of the clinical model increased to 0.75 (95% CI = 0.64-0.80), and specificity was 0.89 (95% CI = 0.69-0.98). The PPV was 0.92 (95% CI = 0.78-0.99), and NPV increased to 0.67 (95% CI = 0.52-0.74).
Prognostic Values and Probabilities of Achieving Upper-Limb Motor Function (FM-UE ≥ 22 Points) 6 Months After Stroke, Based on Active FE and SA, Measured Within 48 Hours and 11 Days Poststroke.
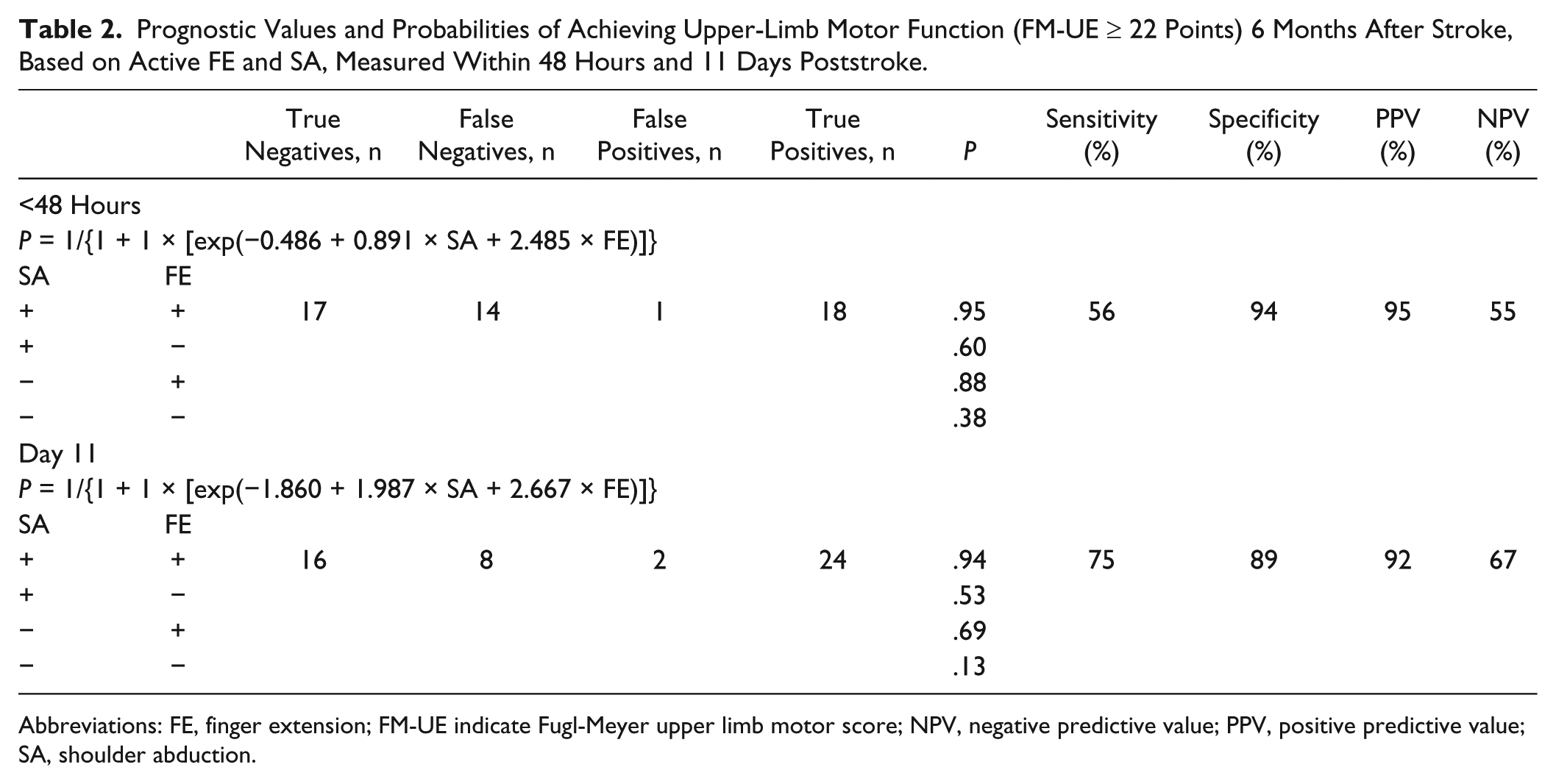
Abbreviations: FE, finger extension; FM-UE indicate Fugl-Meyer upper limb motor score; NPV, negative predictive value; PPV, positive predictive value; SA, shoulder abduction.
Table 3 presents the predictive value of TMS-ADM measured within 48 hours or at 11 days poststroke for predicting outcome of FM-UE at 6 months. Within 48 hours, the probability to achieve upper-limb function was .79 when TMS-ADM was present and .35 when TMS-ADM was absent. At 11 days poststroke, the probability of achieving some dexterity when TMS-ADM was present increased to .88 and decreased to .22 when TMS-ADM was absent. Within 48 hours, sensitivity was 0.81 (95% CI = 0.70-0.90), specificity 0.61 (95% CI = 0.41-0.77), PPV 0.79 (95% CI = 0.68-0.88), and NPV 0.65 (95% CI = 0.43-0.82). At 11 days poststroke, sensitivity was 0.88 (95% CI = 0.76-0.95) and specificity 0.78 (95% CI = 0.58-0.90). The PPV increased to 0.88 (95% CI = 0.76-0.95) and NPV increased to 0.78 (95% CI = 0.58-0.90).
Prognostic Values and Probabilities of Achieving Upper-Limb Motor Function (FM-UE ≥ 22 Points) 6 Months After Stroke, Based on TMS-ADM Measured Within 48 Hours and 11 Days Poststroke.
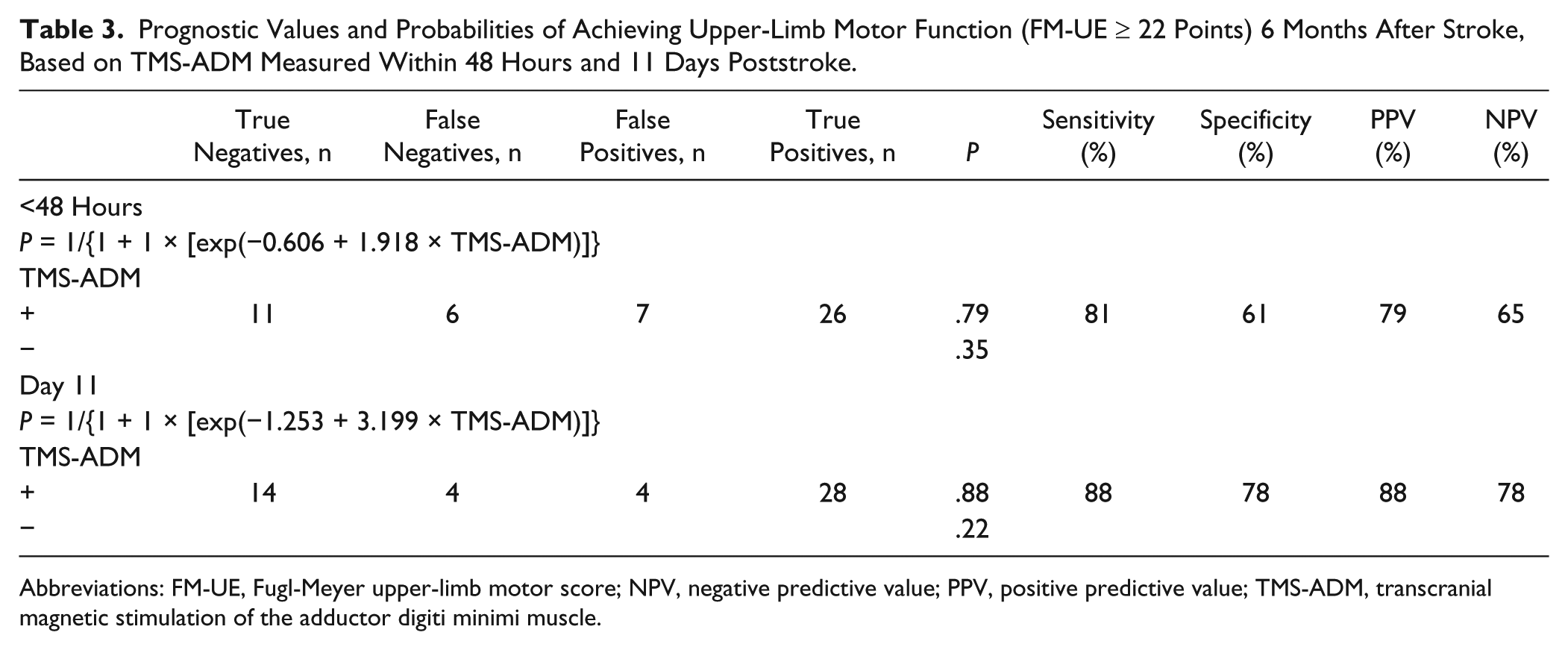
Abbreviations: FM-UE, Fugl-Meyer upper-limb motor score; NPV, negative predictive value; PPV, positive predictive value; TMS-ADM, transcranial magnetic stimulation of the adductor digiti minimi muscle.
Table 4 shows the derived multivariable prediction model in which clinical determinants of SAFE and TMS-ADM were combined for multivariable regression analyses. The probability of achieving some dexterity after 6 months poststroke was .96 when SAFE and TMS-ADM were present and .27 when SAFE and TMS-ADM were absent within 48 hours. At 11 days poststroke, the multivariable model of SAFE and TMS-ADM showed a probability of .95 when all determinants were present, whereas if all determinants were absent, the probability declined to .08. The 2-way contingency table analyses showed a sensitivity of 0.72 (95% CI = 0.60-0.80), a specificity of 0.78 (95% CI = 0.57-0.92), a PPV of 0.85 (95% CI = 0.71-0.95) and NPV of 0.61 (95% CI = 0.44-0.72) within 48 hours. At 11 days poststroke, the sensitivity increased to 0.84 (95% CI = 0.73-0.89), specificity increased to 0.89 (95% CI = 0.69-0.98), whereas the PPV increased to 0.93 (95% CI = 0.81-0.99) and NPV to 0.76 (95% CI = 0.59-0.84), respectively.
Prognostic Values and Probabilities of Achieving Upper-Limb Motor Function (FM-UE ≥ 22 points) 6 Months After Stroke, Based on Active FE, SA, and TMS-ADM Measured Within 48 Hours and 11 Days Poststroke.
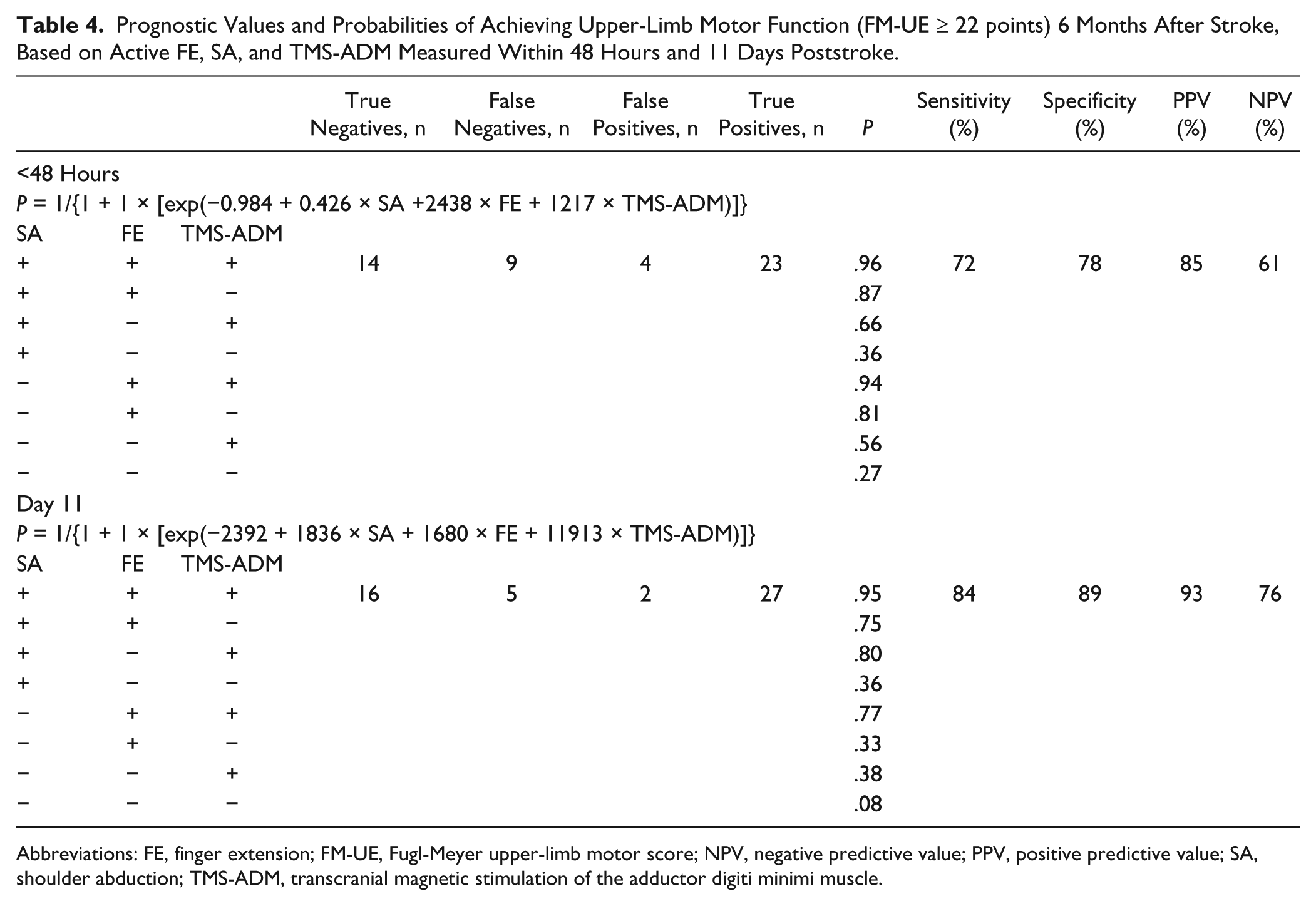
Abbreviations: FE, finger extension; FM-UE, Fugl-Meyer upper-limb motor score; NPV, negative predictive value; PPV, positive predictive value; SA, shoulder abduction; TMS-ADM, transcranial magnetic stimulation of the adductor digiti minimi muscle.
Figure 2 shows the ROC analyses of the 3 different prediction models within 48 hours poststroke. The AUC ranged from 0.793 for the SAFE model (SE = 0.064; P < .001; 95% CI = 0.667-0.919), 0.827 for the SAFE model with TMS-ADM (SE = 0.057; P < .001; 95% CI = 0.716-0.939), and 0.712 for the TMS-ADM model (SE = 0.080; P = .014; 95% CI = 0.555-0.869). Comparison of the 3 ROC curves showed that the AUC was not significantly different between the models (SAFE compared with SAFE and TMS-ADM: z = 0.8975, P = .366; SAFE compared with TMS-ADM: z = 0.8977, P = .3693; and SAFE and TMS-ADM compared with TMS-ADM: z = 0.1.9087, P = .056).
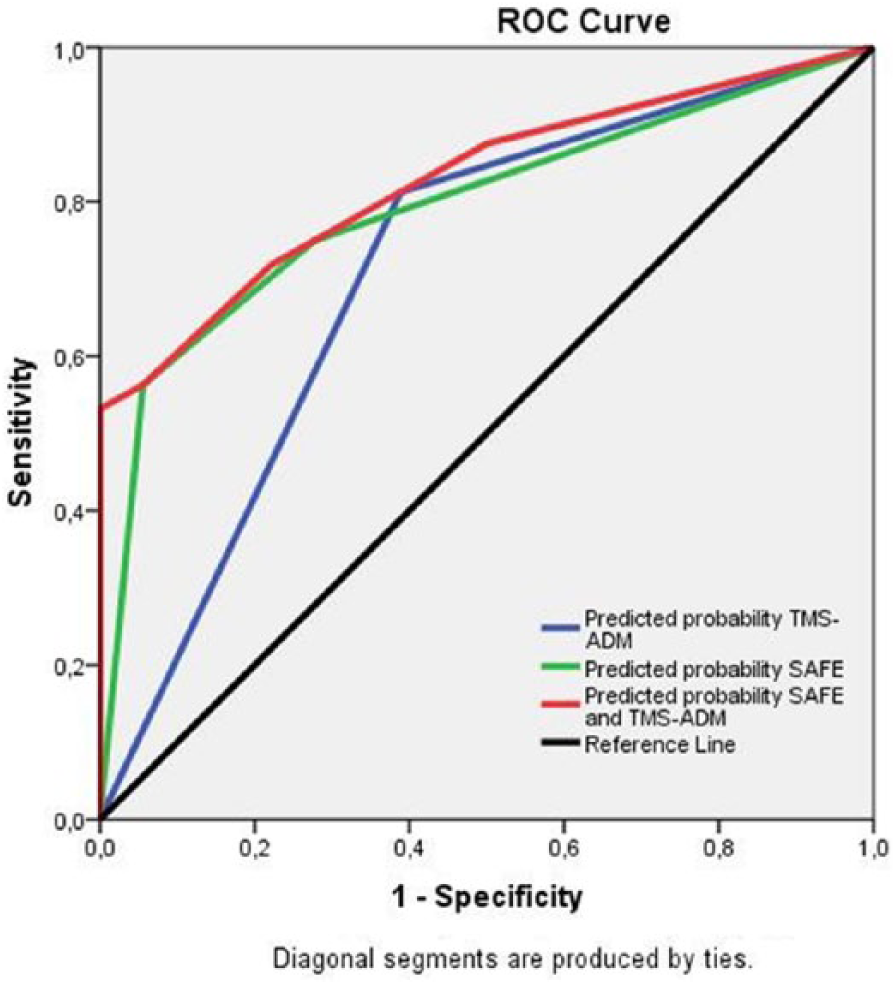
Receiver operating characteristic (ROC) curve plots for the 3 prediction models to predict upper-limb motor function within 48 hours poststroke. In the first model (blue line), the predictive value of transcranial magnetic stimulation–induced motor-evoked potentials of the adductor digiti minimi muscle (TMS-ADM) was investigated. The second model (green line) included clinical assessments alone, using voluntary shoulder abduction (SA) and finger extension (FE), whereas in the third model (red line) the variables SA, FE, and TMS-ADM were combined.
Figure 3 shows the ROC analyses of the 3 prediction models measured at 11 days poststroke. The AUC ranged from 0.880 for the SAFE model (SE = 0.051; P < .001; 95% CI = 0.780-0.980), 0.905 for the SAFE model with TMS-ADM (SE = 0.047; P < .001; 95% CI = 0.814-0.997), and 0.826 for the TMS-ADM (SE = 0.067; P < .001; 95% CI = 0.695-0.958). Comparison of the 3 ROC curves showed that the AUC was significantly different between the TMS-ADM model and the SAFE plus TMS-ADM model in favor of the SAFE and TMS-ADM model combined (z = 2.060; P = .039). No significant difference was found between the SAFE model and the TMS-ADM model (z = 0.782; P = .434) and for the SAFE model and the SAFE model combined with TMS-ADM (z = 0.821; P = .412).
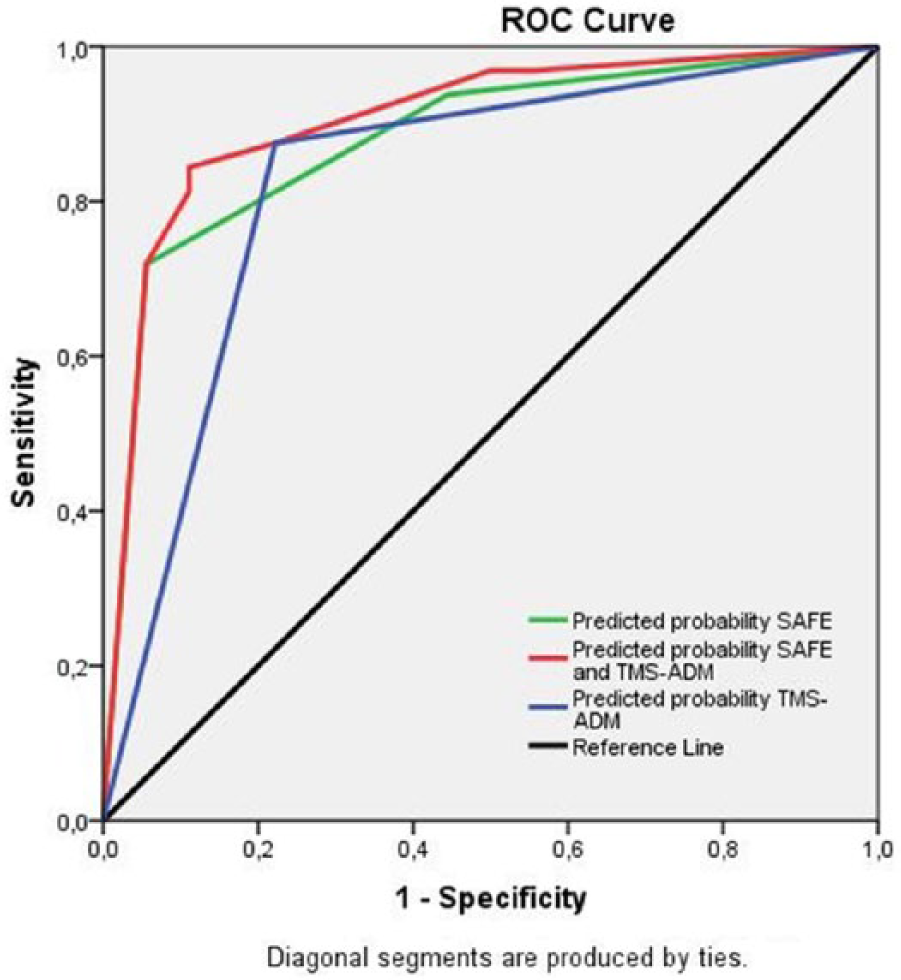
Receiver operating characteristic (ROC) curve plots for the 3 prediction models to predict upper-limb motor function at 11 days poststroke. In the first model (blue line), the predictive value of transcranial magnetic stimulation–induced motor-evoked potentials of the adductor digiti minimi muscle (TMS-ADM) was investigated. The second model (green line) included clinical assessments alone, using voluntary shoulder abduction (SA) and finger extension (FE), whereas in the third model (red line) the variables SA, FE, and TMS-ADM were combined.
Discussion
The present study aimed to demonstrate the added prognostic value of TMS-ADM to the clinical SAFE model when applied within the first 48 hours or at 11 days poststroke in an attempt to improve the accuracy of predicting upper-limb function for achieving 22 points or more on FM-UE at 6 months after severe stroke. The present study shows in a prospective cohort of stroke patients with severe motor impairment that the accuracy of predicting a favorable or unfavorable outcome was not significantly better for TMS-ADM when compared with clinical modeling based on the SAFE model 1 if applied at the same day poststroke. A slightly, even lower accuracy was observed for the TMS-ADM (P = .039), when compared with TMS-ADM combined with the clinical SAFE model at 11 days. The present study further emphasizes that the diagnostic accuracy of TMS-ADM is, like return of voluntary FE, 23 time dependent24,25 and mainly driven by poorly understood processes of spontaneous neurobiological recovery. 25 Finally, the current study shows that the added value of diagnostic TMS for predicting FM-UE should always be seen in light of the current set of powerful clinical tests available for making a valid prognosis early poststroke.1,24,25
Assuming that TMS-ADM may reflect the intactness of CST, the relatively low NPV and low specificity suggest that an initial absence of TMS-ADM may be masked by processes such as corticospinal diaschisis that suppresses the conductivity of CST very early poststroke.26-28 The time dependence of accurate prediction of outcome early poststroke1,23,25 may further clarify the seemingly conflicting results of the added value of TMS-ADM to clinical modeling, next to observed differences in patient selection, type of TMS equipment, and defining outcome.5,28 Future studies are needed to distinguish those patients who are likely to be false negatives and following the expected amount of spontaneous neurological recovery poststroke from patients who are true negatives and failed to show spontaneous neurobiological recovery. Recently, a number of prospective studies showed that about 20% to 30% of first-ever ischemic strokes do not follow the expected 70% rule of spontaneous neurobiological recovery early poststroke.29-31 Probably, this proportional recovery rule is dependent on the intactness of the ipsilesional CTS as revealed by TMS-MEP and fractional anisotropy of the posterior limbs of the internal capsule. 29 Unfortunately, the biomarkers for identifying these (almost none) spontaneously recovering stroke patients are lacking in the literature and a main target for further translational research29,32-34 to improve the underpowered designs of stroke recovery trials in the near future.33,35
This study has some limitations. First, the sample size was limited, and our model may not be applicable to patients with brainstem, hemorrhagic, or recurrent strokes. Second, although the reliability of TMS-induced MEPs of the ADM in the affected hemisphere after ischemic stroke was found to be moderate to excellent,20,28 the selection of ADM instead of other distal intrinsic muscles such as APB constitutes an arbitrary choice. Therefore, future studies should investigate if MEPs of finger extensors, which may reflect more the intactness of corticospinal control, such as the extensor indices muscle, 36 may further improve the prognostic accuracy of TMS very early poststroke. Third, the second assessment in this prospective cohort was set at 11 days poststroke, which was a pragmatic choice, related with length of hospitalization.
Future studies are needed to reveal the added value of other innovative methods such as structural29,34 and functional neuroimaging techniques early poststroke. 37 For example, diffusion tensor imaging (DTI) indexing the extent of white matter damage may have an added value to clinical modeling and TMS-ADM. 38 However, the accuracy of DTI as defined by the initial fiber number ratio at 24 and 72 hours poststroke as a surrogate marker of corticospinal tract integrity may be hindered by the fact that Wallerian degeneration also requires time to manifest itself in the first days poststroke.34,39 Finally, the review of 71 prognostic studies investigating the internal validity of neurological biomarkers, such as DTI, TMS, fMRI, and structural MRI as a predictor alone or in combination with clinical biomarkers of stroke recovery, revealed that 50 (2/3) studies suffered from insufficient robustness and poor methodological quality. 32 In particular, small sample sizes, the accompanying uncertainty about the minimal clinically important difference, and lack of cross-validation made the authors conclude that neurological biomarkers in combination with behavioral clinical measures are more accurate than models that used neurological biomarkers alone. 32
Footnotes
Acknowledgements
The authors would like to gratefully thank Johan Bisschop and Jan Middendorp from the department of clinical neurophysiology of the Isala Klinieken for performing all TMS assessments.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.