
Abstract
Acquired brain injury (ABI) is associated with a range of cognitive and motor deficits, and poses a significant personal, societal, and economic burden. Rehabilitation programs are available that target motor skills or cognitive functioning. In this review, we summarize the existing evidence that training may enhance structural neuroplasticity in patients with ABI, as assessed using structural magnetic resonance imaging (MRI)–based techniques that probe microstructure or morphology. Twenty-five research articles met key inclusion criteria. Most trials measured relevant outcomes and had treatment benefits that would justify the risk of potential harm. The rehabilitation program included a variety of task-oriented movement exercises (such as facilitation therapy, postural control training), neurorehabilitation techniques (such as constraint-induced movement therapy) or computer-assisted training programs (eg, Cogmed program). The reviewed studies describe regional alterations in white matter architecture and/or gray matter volume with training. Only weak-to-moderate correlations were observed between improved behavioral function and structural changes. While structural MRI is a powerful tool for detection of longitudinal structural changes, specific measures about the underlying biological mechanisms are lacking. Continued work in this field may potentially see structural MRI metrics used as biomarkers to help guide treatment at the individual patient level.
Introduction
Acquired brain injury (ABI) can result from a variety of causes, including trauma, stroke, tumor, substance abuse, or degenerative neurological diseases, and is considered as one of the main disability groups. 1 Although medicine has made considerable strides in reducing ABI-related mortality, many individuals develop chronic problems, often resulting in lifelong disability. The clinical outcome in ABI often includes persistent cognitive problems such as attention deficits, memory impairments, slowed processing speed, word-finding difficulties, behavioral disinhibition, and emotional lability. 2 While less obvious than in congenital disorders like cerebral palsy, motor disabilities are also evident in patients with ABI. 3 It has been hypothesized that these motor and cognitive dysfunctions arise from disturbed connectivity between different brain regions. 4
The use of structural magnetic resonance imaging (MRI) techniques, including anatomical MRI and diffusion MRI, provides insights on the relationship between structural alterations and behavioral deficits. For example, our previous voxel-based morphometry (VBM) study has revealed reduced volume in cerebellar lobules, pons and midbrain in children with brain injury due to external trauma (traumatic brain injury [TBI]), 5 which correlated with lower scores on tests of postural control. Associations were also found between neuropsychological scores and regional grey matter volumes of prefrontal, parietal, temporal, and insular cortex in multiple sclerosis. 6 Altered white matter microstructure in sensorimotor tracts and association fiber bundles have also been reported in ABI patients using diffusion MRI. 7 These studies show significant, moderate-to-high correlations between motor control, language and cognitive performance on one hand and diffusion MRI metrics on the other such that increased white matter (WM) pathology predicts poorer performance in brain injured patients. Over time, these MRI techniques have shown improved pathologic sensitivity and have highlighted the correlations among behavioral impairments and disease-modified brain structures.
The traditional view is of irreversible neural impairment in ABI; however, recent studies using functional MRI techniques have questioned this assumption by showing lifelong potential for reorganization and plasticity. More specifically, there is mounting evidence supporting the compensation hypothesis that brain-injured patients efficiently recruit additional brain regions for cognitive or motor control during task performance, approaching the performance levels of healthy controls. 8 Moreover, studies on ABI patients have demonstrated functional changes in cortical excitability, metabolic rate, or blood flow in sensorimotor regions after training. 9 During training-induced recovery, adaptation of functional systems to damage has been revealed. Functional neuroplasticity in brain-injured adults have already been described elsewhere and the interested reader is referred to a number of recent review papers on this topic.10-14
More recently, there is mounting evidence in healthy adults that improvements in movement skill and cognition through training may be the result of structural alterations within the brain. Studies in healthy adults show structural variation in brain regions that are related directly to the level of task experience, for example, in bilingual individuals. 15 There is also evidence that training over a short time period can modify brain structure in healthy adults. Working memory training, for instance, has resulted in increased fractional anisotropy (FA), an index of tissue microstructural organization, in the intraparietal sulcus and the anterior corpus callosum. 16 Evidence has accumulated over recent years to show that this structural plasticity in response to training reported in healthy adults (at least over short time periods) is also evident in people with an ABI.
The aim of this review is to assess existing evidence that motor and cognitive rehabilitation may enhance structural neuroplasticity in patients with ABI assessed using MRI techniques. The particular focus of the review is to clarify those aspects of training in ABI that best afford experience-dependent plasticity. The review includes ABI training studies that report brain structural MRI-based techniques that probe microstructure (diffusion MRI) or macrostructure (anatomical MRI). The review critically examines the existing structural MRI-based evidence to determine whether motor and cognitive rehabilitation can induce structural plasticity in the brain of patients with ABI. The conclusions will guide researchers and practitioners toward evidenced-based practice and more targeted approaches to rehabilitation.
Methods
Search Strategy and Article Selection
Two electronic databases (PubMed and Web of Science) were searched for English-language articles focusing on structural MRI studies on neuroplasticity in response to training or rehabilitation in ABI. The search was run using the following terms: “(“brain injur*” OR ABI OR TBI OR stroke* OR aphasia OR “cerebral infarction” OR “multiple sclerosis” OR huntington* OR “axonal injur*” OR parkinson* OR neurodegeneration OR “cerebellar degeneration”) AND (“structural magnetic resonance imaging” OR “structural MRI” OR “diffusion MRI” OR “diffusion tensor imag*” OR DTI OR “diffusion tensor tractography” OR “voxel-based morphometry” OR “voxel based morphometry” OR VBM OR “anatomical MRI” OR “MR imaging” OR T1* OR freesurfer) AND (rehab* OR train* OR therap* OR treat* OR physiotherap* OR “physical therap*”) AND (motor OR sensorimotor OR balance OR cognit* OR speech* OR language OR music OR physiotherap* OR “physical therap*” OR exercis* OR intervention*)”. No article type limitations or time period restrictions were applied, and the latest search was undertaken on August 22, 2017. Attempts to identify further articles were made by searching the reference lists of these studies. We were not familiar with any study currently in progress that could be considered for inclusion. Also excluded were published study protocols, conference abstracts, and articles not available in English. To fit the main purpose of this review, we excluded studies that did not include structural MRI/diffusion MRI.
Study Selection
The title and abstract of the retrieved articles were examined against all inclusion criteria (below) and the full text article was retrieved if all criteria were met. The assessment of eligibility was performed by 2 investigators (AC, KC) independently with the requirement of consensus. In case of disagreement, a third expert (PI) was consulted. In total, we identified 25 research articles (see Figure 1) that met the following four inclusion criteria: (a) the studies involved adults who sustained acquired brain injury (mean age >18 years); (b) use of a cognitive, language, and/or motor training protocol; (c) pre-post assessment of behavioral and brain-based outcomes; and (d) MRI based methods were employed to measure structural changes.
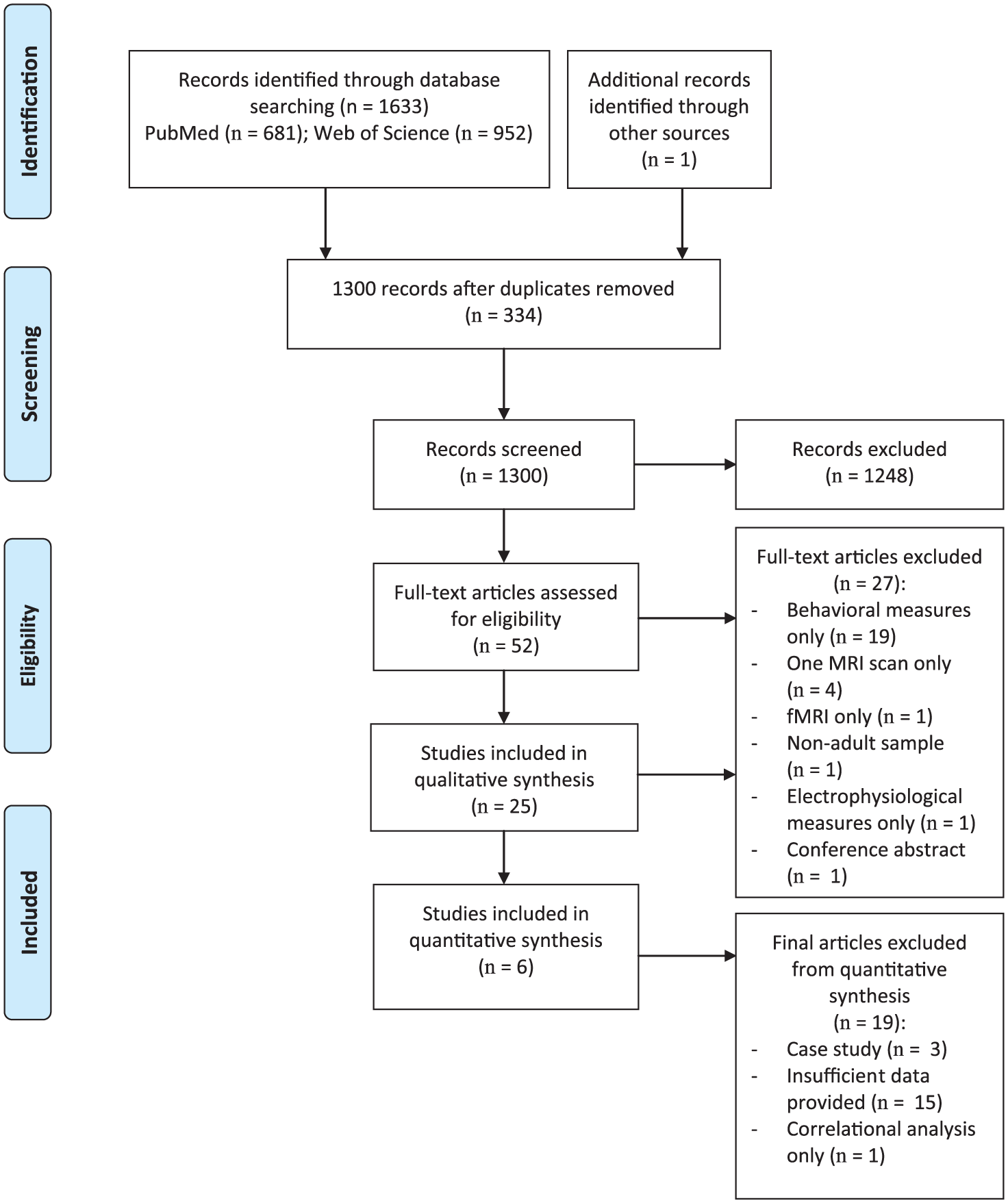
Flowchart of the conducted systematic search and study inclusion for the qualitative and quantitative syntheses.
Data Extraction and Qualitative Analysis
As shown in Figure 1, the initial search resulted in 1634 citations. After removal of the duplicates, 1300 unique articles were screened based on title and abstract. It was determined that 1248 of these studies did not meet the inclusion criteria. Fifty-two articles were withheld for further detailed screening by examining the full text. It appeared that 27 studies did not meet the inclusion criteria as described. In total, we identified and included 25 studies investigating structural neuroplasticity in response to training, including 447 patients with ABI.
Two authors (KC, AC) assessed the methodological quality of each study independently, using the 5 criteria recommended by the Cochrane Back Review Group. 17 This scale evaluates criteria relevant to training and is suitable for the evaluation of clinical trials in neurological disorders. This Clinical Relevance Scale has been used in previous systematic reviews.18-20 Presently, there are no established cutoff scores for high- and low-quality studies using this tool. Disagreements between reviewers were resolved by consensus.
Data Synthesis and Quantitative Analysis
Two independent raters (KC, AC) synthesized the data in a table, including study modality, patient characteristics, training intervention, control interventions (if present), training dosage and all outcome measures (behavioral results, main findings in structural MRI metrics), percentage change on structural brain metrics (when available), and correlations with clinical or behavioral measures (Tables 1-3).
Summary of Included Articles Investigating Structural Brain Changes in Stroke Patients After Training Using Voxel-Based Morphometry (VBM) or Diffusion Tensor MRI (DTI) Techniques.
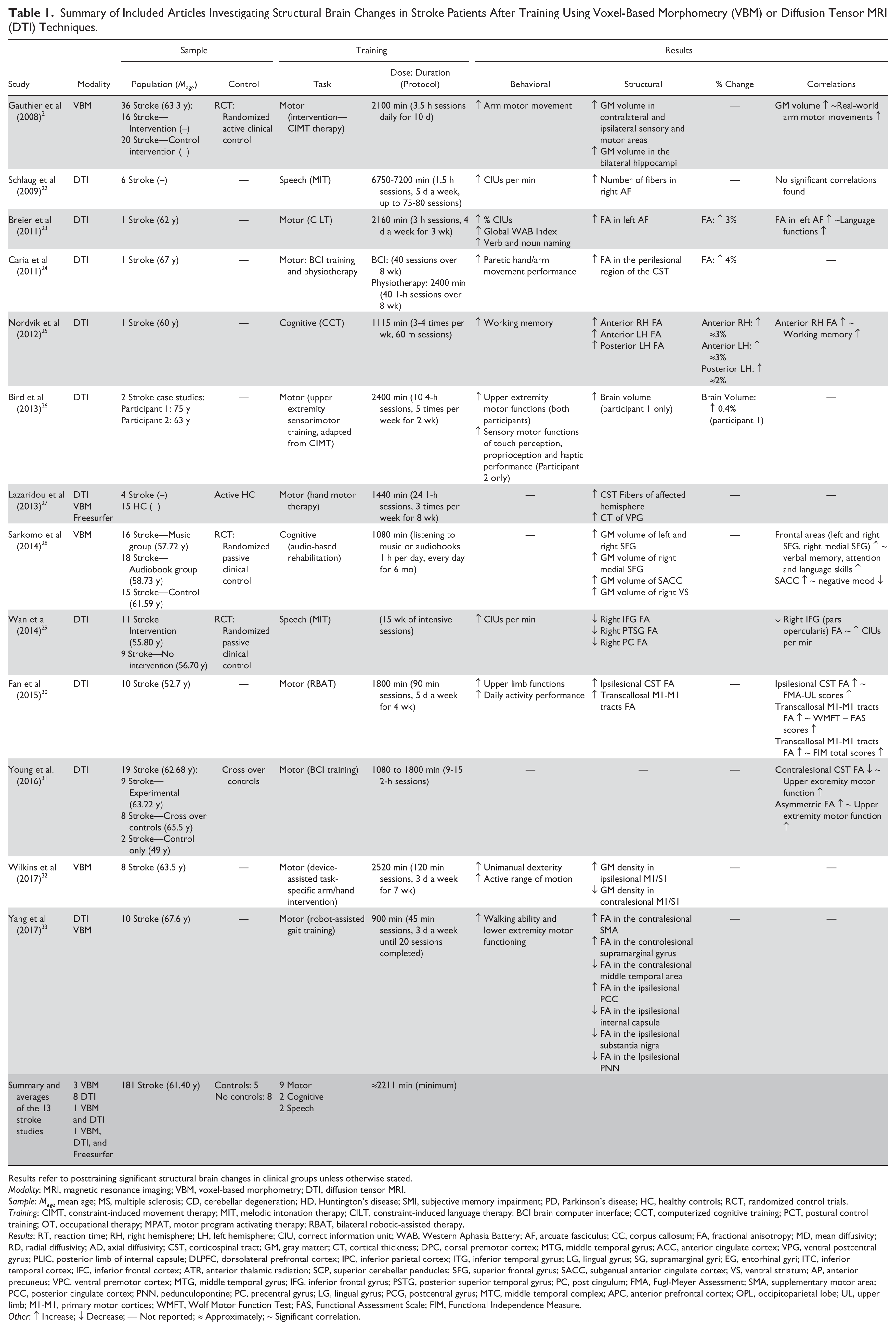
Results refer to posttraining significant structural brain changes in clinical groups unless otherwise stated.
Modality: MRI, magnetic resonance imaging; VBM, voxel-based morphometry; DTI, diffusion tensor MRI.
Sample: Mage mean age; MS, multiple sclerosis; CD, cerebellar degeneration; HD, Huntington’s disease; SMI, subjective memory impairment; PD, Parkinson’s disease; HC, healthy controls; RCT, randomized control trials.
Training: CIMT, constraint-induced movement therapy; MIT, melodic intonation therapy; CILT, constraint-induced language therapy; BCI brain computer interface; CCT, computerized cognitive training; PCT, postural control training; OT, occupational therapy; MPAT, motor program activating therapy; RBAT, bilateral robotic-assisted therapy.
Results: RT, reaction time; RH, right hemisphere; LH, left hemisphere; CIU, correct information unit; WAB, Western Aphasia Battery; AF, arcuate fasciculus; CC, corpus callosum; FA, fractional anisotropy; MD, mean diffusivity; RD, radial diffusivity; AD, axial diffusivity; CST, corticospinal tract; GM, gray matter; CT, cortical thickness; DPC, dorsal premotor cortex; MTG, middle temporal gyrus; ACC, anterior cingulate cortex; VPG, ventral postcentral gyrus; PLIC, posterior limb of internal capsule; DLPFC, dorsolateral prefrontal cortex; IPC, inferior parietal cortex; ITG, inferior temporal gyrus; LG, lingual gyrus; SG, supramarginal gyri; EG, entorhinal gyri; ITC, inferior temporal cortex; IFC, inferior frontal cortex; ATR, anterior thalamic radiation; SCP, superior cerebellar penducles; SFG, superior frontal gyrus; SACC, subgenual anterior cingulate cortex; VS, ventral striatum; AP, anterior precuneus; VPC, ventral premotor cortex; MTG, middle temporal gyrus; IFG, inferior frontal gyrus; PSTG, posterior superior temporal gyrus; PC, post cingulum; FMA, Fugl-Meyer Assessment; SMA, supplementary motor area; PCC, posterior cingulate cortex; PNN, pedunculopontine; PC, precentral gyrus; LG, lingual gyrus; PCG, postcentral gyrus; MTC, middle temporal complex; APC, anterior prefrontal cortex; OPL, occipitoparietal lobe; UL, upper limb; M1-M1, primary motor cortices; WMFT, Wolf Motor Function Test; FAS, Functional Assessment Scale; FIM, Functional Independence Measure.
Other: ↑ Increase; ↓ Decrease; — Not reported; ≈ Approximately; ~ Significant correlation.
Summary of Included Articles Investigating Structural Brain Changes in Multiple Sclerosis Patients After Training Using Voxel Based Morphometry (VBM) or Diffusion Tensor MRI (DTI) Techniques. a
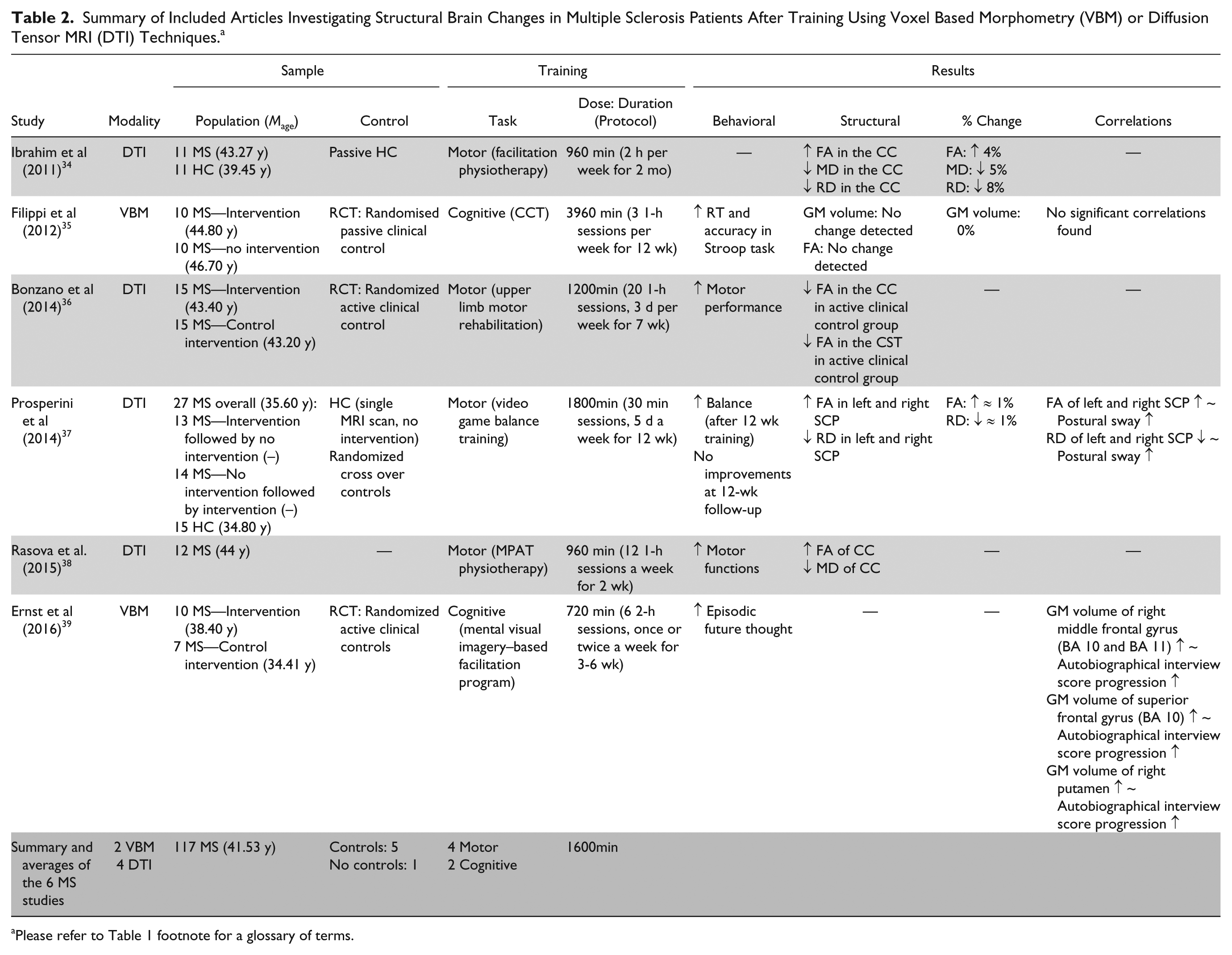
Please refer to Table 1 footnote for a glossary of terms.
Summary of Included Articles Investigating Structural Brain Changes in Huntington’s Disease (HD), Parkinson’s Disease, Cerebellar Degeneration (CD), and Traumatic Brain Injury Patients After Training Using Voxel-Based Morphometry (VBM) or Diffusion Tensor MRI (DTI) Techniques. a
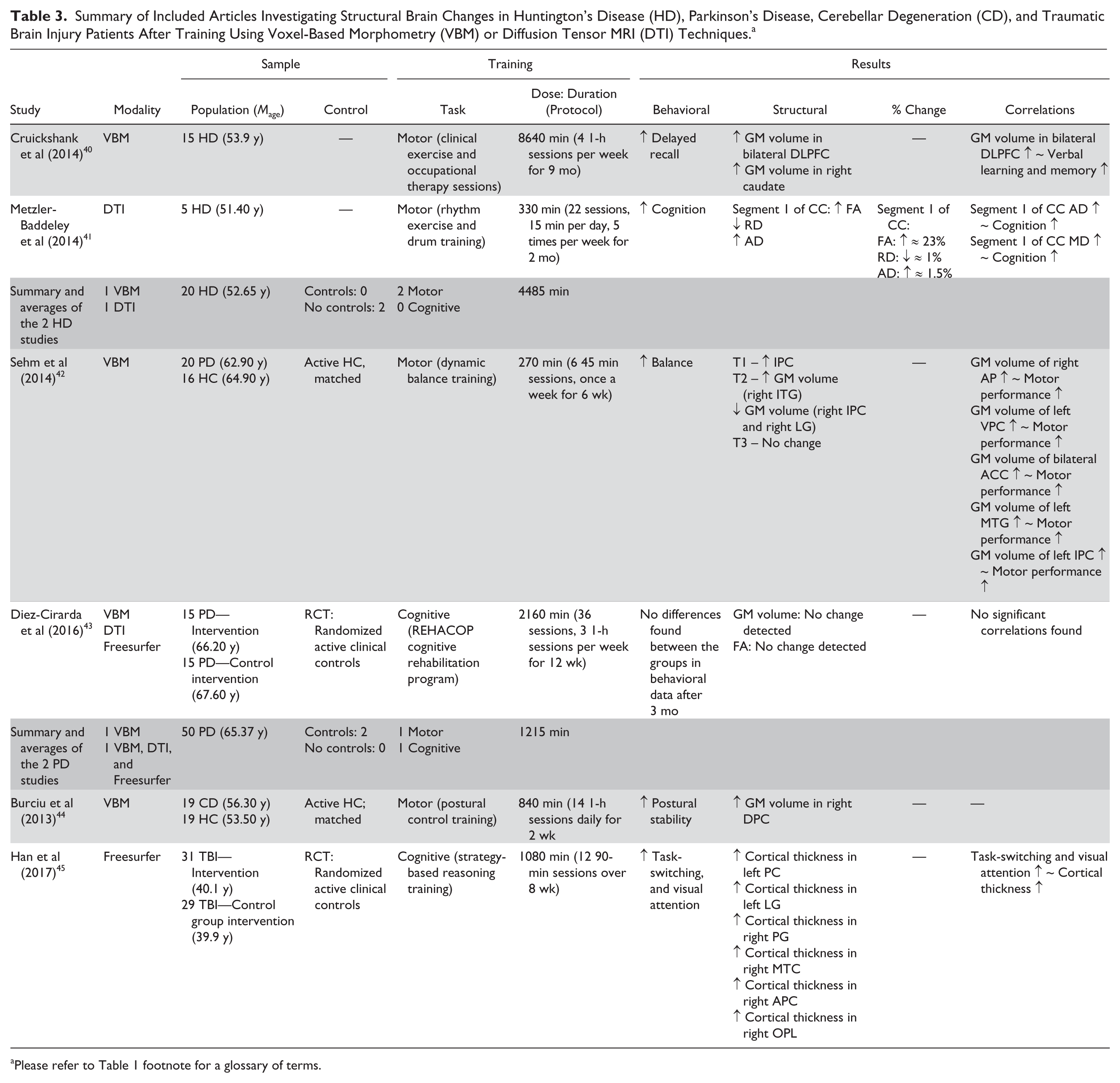
Please refer to Table 1 footnote for a glossary of terms.
Since different outcome measures were utilized as primary and secondary outcomes, we analyzed the effectiveness of different training programs on FA to better examine the results across studies. From 6 studies, mean differences and their standard deviations on FA, P values, and sample sizes for the groups were entered into Comprehensive Meta-Analysis (CMA; Biostat, Englewood, NJ, USA) version 2.2.064. A random effects model was used to compute the effect size estimate, Hedges’ g, a variation of Cohen’s d that corrects for small sample size biases. The magnitude of Hedges’ g was categorized as follows: small (≥0.2), medium (≥0.5) and large (≥0.8). 46 Pooled effect sizes were calculated by aggregating the mean effect sizes weighted by each study’s sample size, and the 95% confidence intervals (CIs) and z scores based on the overall mean and standard error. Positive effect size outcomes reflected increases in FA following the training, while negative effect size values indicated a decrease in FA following the training. Heterogeneity was formally assessed with the I2 statistic, whereby we assigned I2 value of low, moderate, and high statistical heterogeneity with corresponding I2 values of 25%, 50%, and 75%. In 2 studies,30,37 changes in FA were reported separately for different brain regions. These effect sizes were pooled to avoid violating the assumption of independence. 47
Results
There were a total of 25 studies investigating structural neuroplasticity in response to training, including 181 patients with stroke, 117 patients with multiple sclerosis, 20 patients with Huntington’s disease, 20 patients with Parkinson’s disease, 19 patients with cerebellar degeneration, and 60 patients with traumatic brain injury. Tables 1 to 3 provide a summary of the studies categorized according to disorder. A detailed summary of each article can be found in the Supplementary Material.
Quality
Table 4 summarizes the quality and clinical relevance of the trials. Most trials measured relevant outcomes and had treatment benefits that would justify the risk of potential harm. Only 3 trials accomplished clinically important effect sizes. Overall, the quality score varied from 1 to 5 points (average score: 2.84). The trial by the group of Bird et al 26 were judged more clinically relevant than the others.
Trial Ratings on the Clinical Relevance Scale. a
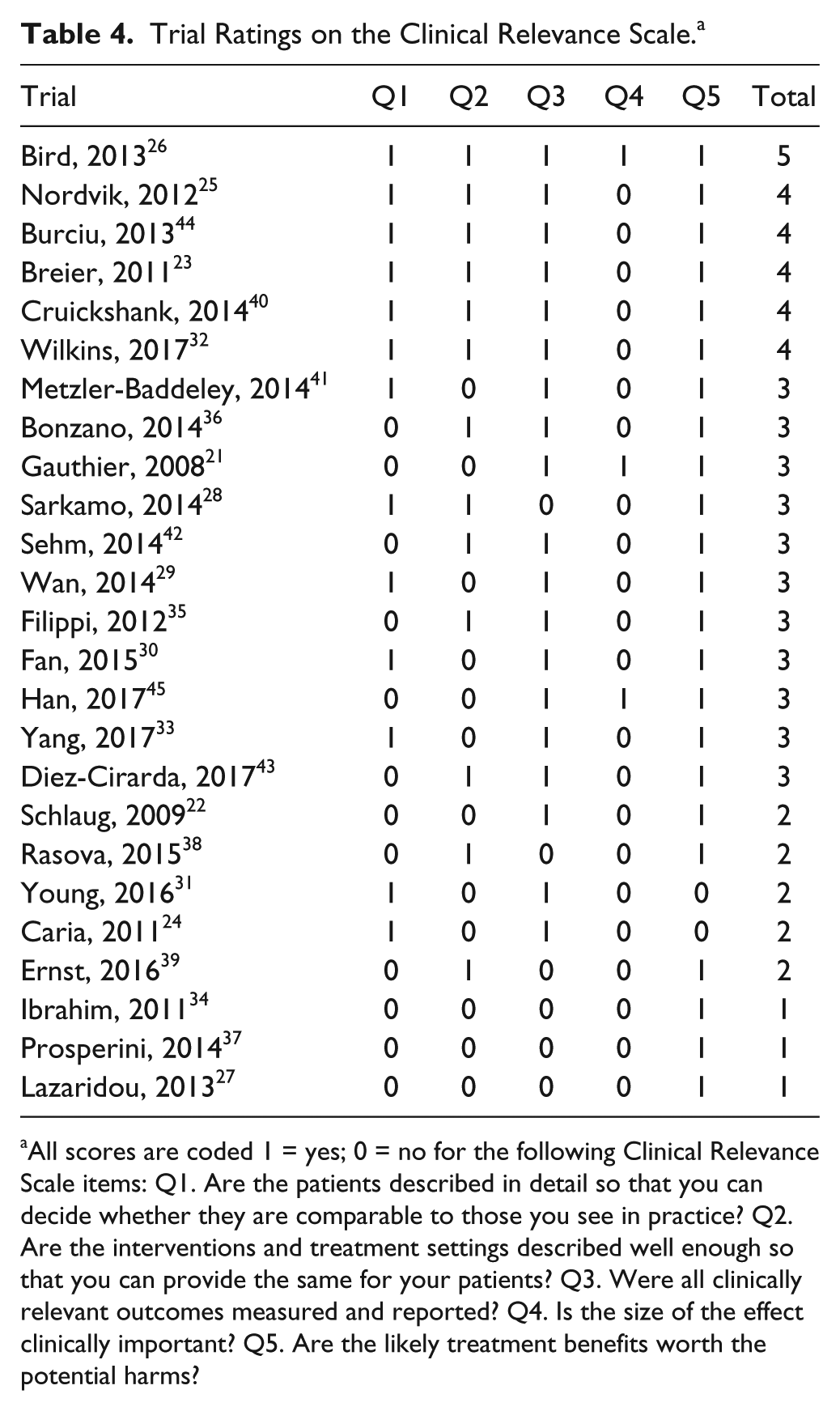
All scores are coded 1 = yes; 0 = no for the following Clinical Relevance Scale items: Q1. Are the patients described in detail so that you can decide whether they are comparable to those you see in practice? Q2. Are the interventions and treatment settings described well enough so that you can provide the same for your patients? Q3. Were all clinically relevant outcomes measured and reported? Q4. Is the size of the effect clinically important? Q5. Are the likely treatment benefits worth the potential harms?
Main Effects of Training on Fractional Anisotropy
Six studies were included in the meta-analysis. Overall, the effect of training programs on FA values was approaching significance (see Figure 2). The average effect size was medium, g = 0.62 (95% CI −0.06 to 1.3, P = .074). Apart from the study of Wan et al, 29 effect estimates were in the same direction, that is, FA increased with training. Heterogeneity between studies was significant I2 = 83.56%, Q = 30.41, P < .001, indicating definite heterogeneity across studies. Important sources of this heterogeneity are likely to be training duration and the different clinical groups and ROIs involved (see Discussion section). The low number of included studies in the quantitative analysis prevented us from further reliable subgroup meta-analyses.
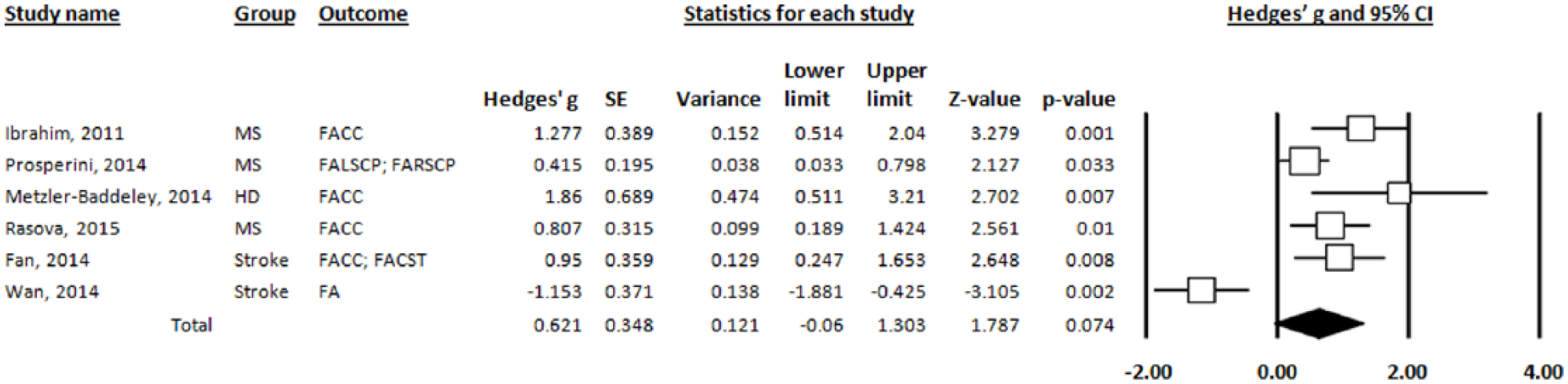
Forest plot of 6 studies that examined the effect of training programs on fractional anisotropy (FA).
Discussion
Findings from the current review suggest that training interventions have effects on behavior and brain structure in patients with ABI. Below we will examine the evidence of structural neuroplasticity from a critical view. Specifically, we will discuss the following issues: (1) Do neuroplastic changes occur after training? (2) What treatment dose is necessary to obtain MRI-detectable structural changes? (3) Do neuroplastic changes coincide with behavioral improvements? (4) Which structural brain metrics are sensitive enough to identify training-related changes?
Do Neuroplastic Changes Occur After Training?
Structural MRI findings support the notion that neuroplasticity can occur in ABI after specific task-dependent and target-selected training programs. These results also point out the role of some specific brain regions (Figure 3) as targets of neuroplasticity including the corpus callosum and cerebellum. Changes in structural MRI metrics with training tend to be small (% change of around 3%, in the main—see Tables 1-3), with values ranging between 1% and 23%. This is perhaps not surprising, since changes in brain structure within a limited duration (weeks or even months) are likely to be subtle and difficult to detect. 48 These percentage changes are more than the published error rates (in terms of reproducibility and reliability) of brain volume change (0.2%) 49 and are only slightly above the published error rate of the diffusion metrics alterations (1.7%-7.1%).50,51 Percentage change (in cases where we could calculate this) was higher than that shown by studies of healthy subjects. For example, the well-known juggling study of Scholz et al 52 reported a significant training-related increase of around 4% in gray matter density in the medial occipital and parietal lobe as well as a significant increase (~5%) in FA near the right posterior intraparietal sulcus. We tentatively suggest that structural neuroplasticity can be observed when training the motor or cognitive functions of patients with ABI and to a higher degree than that of healthy subjects.
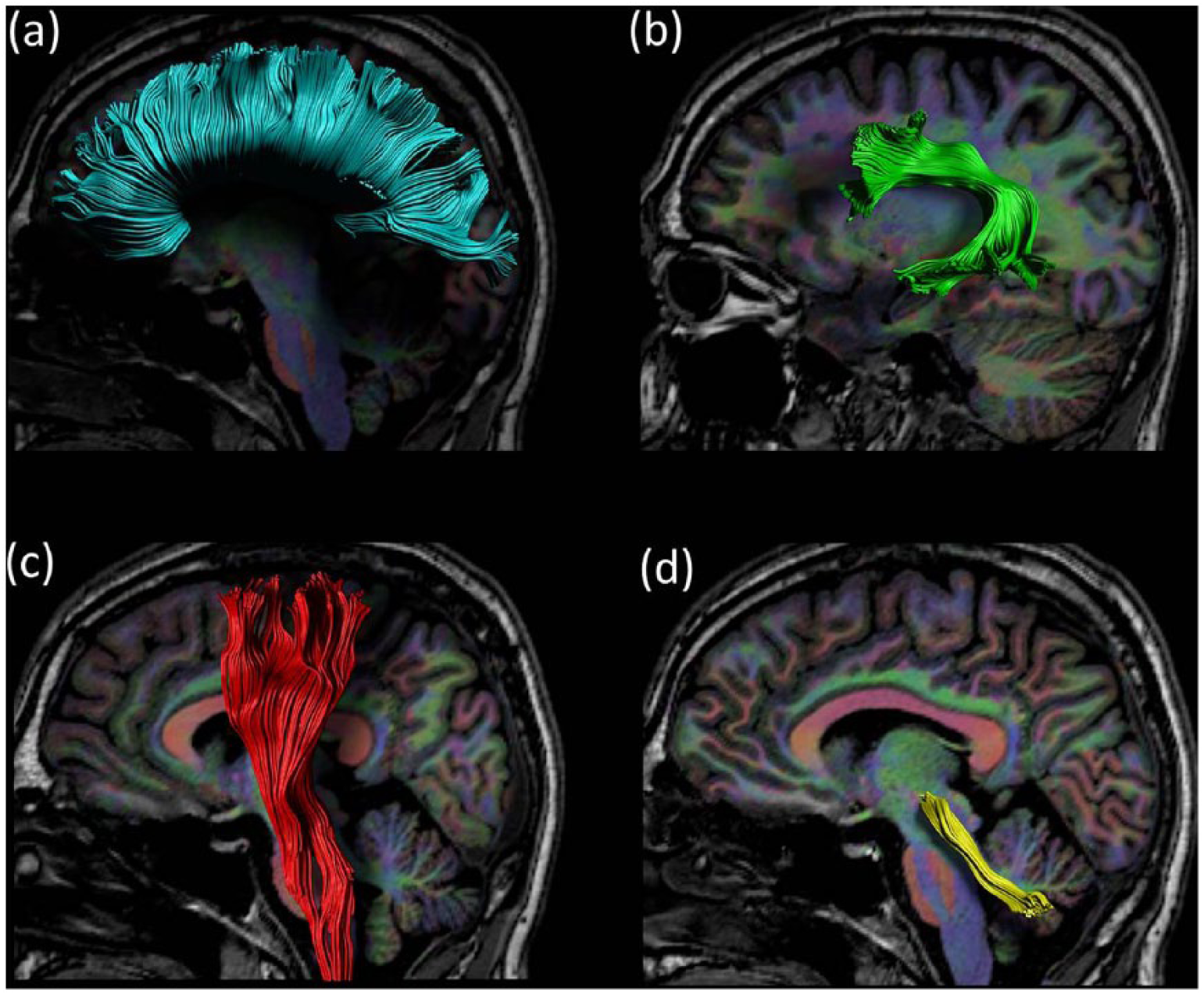
White matter tracts that show alterations with motor, language, or cognitive training in acquired brain injury (ABI) patients. Trajectories of (a) the corpus callosum, (b) arcuate fasciculus, (c) corticospinal tract, and (d) superior cerebellar peduncle as reconstructed with a diffusion magnetic resonance imaging (MRI)–based fiber tractography method.
Utilizing the Clinical Relevance Scale (see Table 4, column Q1), patients with subtle deficits were more commonly included than those with more severe deficits. For example, most training studies in multiple sclerosis have included patients with an expanded disability scale score <5,34,37,38 meaning fully ambulatory. A similar bias could be observed in studies of stroke where patients with aphasia are excluded. 26 It is likely that studies have been limited to patients with minimal functioning to overcome higher drop-out rates. For example, in Metzler-Baddeley et al 41 the two most severely impaired individuals with Huntington’s disease withdrew because the training was too demanding. However, low-functioning patients should be included in training studies to enhance generalizability of findings.
Finally, the present study did not reveal evidence for shared or distinct patterns of structural neuroplasticity with training program (cognitive, speech or motor rehabilitation) or brain injury type (stroke, multiple sclerosis, Huntington’s disease, Parkinson’s disease, cerebellar degeneration, traumatic brain injury). We suggest a clear pattern will become evident when more studies are conducted in this domain.
What Treatment Dose Is Necessary to Obtain MRI-Detectable Structural Changes?
Training regimes in the studies varied considerably in terms of total treatment time, or dose (as shown in Tables 1-3). The training duration varied from 270 minutes 42 to 8640 minutes. 40 The average training duration also varied according to type of brain injury (Tables 1-3), supporting the idea that the beneficial effects of a rehabilitation treatment are disease-dependent. Future studies including larger sample sizes with multiple brain disorders are required.
Contrary to the traditional views that structural brain changes are restricted to critical periods during early age or that they are slowly evolving processes emerging over several months, studies have recently demonstrated training-induced changes over relatively short time frames, that is, within days (in healthy adults) 53 or even hours (in animal models). 54 Taubert et al 53 reported gray matter volume increases in sensorimotor regions after 90 minutes of balance training that decreased after further training. Reduced grey matter volume was interpreted by the authors as a result of practice and acquisition of a new motor skill, suggestive of greater efficiency.
Within ABI patients, Sehm et al 42 could even identify an increase in grey matter volume in the right inferior parietal cortex after 90 minutes of training (over 2 weeks). After another training period of 90 minutes, the gray matter volume in the right inferior parietal gyrus region decreased, together with a decrease in gray matter volume in the right lingual gyrus. 42 These early and late transient changes in the inferior parietal cortex were interpreted as transient structural changes by the authors. However, these fluctuations could also be due to different positioning in the scanner and other small scan variations with time. 55
The magnitude of changes observed in micro/macrostructural metrics should be analyzed by taking into account random variance between scanning sessions. Scan-to-scan variability was tested in Schlaug et al 22 by administering two separate diffusion weighted scans before the start of the training. The results showed similar numbers of fibers across these 2 pretraining scanning sessions. By calculating a signal-to-noise ratio within the regions of interest 56 a measure of random noise of the scanner can be computed for each individual scan of each tract of interest, as computed in the study of Bonzano et al. 36 The results of Bonzano et al 36 revealed no significant change in signal to noise ratio between pre and post training in the three tracts of interest.
The majority of studies have typically evaluated the structural changes only during pre- and posttraining (apart from Sehm et al 33 and Yang et al 42 ). Although intermittent scans during the training period have rarely been acquired, the use of multiple timepoints is crucial to developing more complex statistical models (such as piecewise growth curve modeling) to best capture changes in brain structure over varying time scales. The effects of training duration can also be investigated in more detail by considering it as a continuous variable. However, there are no studies that have investigated the relationship between training duration and structural brain changes in ABI. Rather, the amount of training was held constant in a controlled environment or the authors only provided a group estimate rather than individual registrations of training time. To further investigate the effect of training load on structural brain metrics, experimental designs are required whereby different subjects are allocated to different training regimes with different dosage. This approach would disentangle how tightly aligned structural changes are to the amount of training time and to the amount of performance improvement.
To date, the variation in training regimes (eg, task, duration) across studies limit the conclusions that can be drawn about the most effective dose to elicit structural changes. Further research on dose, timing, and duration of training is necessary to generalize the motor or cognitive training protocols to the field of structural neuroplasticity. We argue that interventions emphasizing intense, active and repetitive practice will be of high value. Future studies designed to evaluate training protocols on brain structure in large clinical trials will be necessary to map the structural neuroplasticity that supports behavioral recovery in brain-injured patients.
Do Neuroplastic Changes Coincide With Behavioral Improvements?
In the field of ABI, the effects of training on behavior need to be evaluated at multiple levels; impairment, activity, and participation. The behavioral effects reported in the reviewed studies were predominantly related to the trained abilities only or related skills using measures of near transfer (ie, related task-specific skills, most often at the impairment and activity levels of the International Classification of Functioning, Disability and Health). For example, Burciu et al 44 showed a near transfer effect of balance control training to another postural control task in patients with cerebellar ataxia. Specifically, learning to shift the center of gravity on a dynamic platform to reach several target positions presented on a computer screen (using the Limits of Stability subtest of the Neurocom system) also led to a decrease of the sway length in a task where upright stance was tested under different sensory conditions (using the Sensory Organization Test of the Neurocom system).
Most surveyed studies have failed to show far transfer effects on measures of activities of daily living or clinical measures. For example, no significant changes in ataxia were observed after postural control training in cerebellar ataxia patients. 44 In contrast, far transfer effects were demonstrated in a study of chronic stroke by Gauthier et al 21 where patients receiving CIMT (experimental group) showed greater use of the more affected arm in daily life situations than the comparison therapy. Facilitating these training effects was a transfer package that prepared (the experimental group) patients for learning and task achievement in activities outside the laboratory, whereas controls received all components of CIMT except for the transfer package. Far transfer to daily life activities performance was reported in a study by Fan et al 30 as evidenced by increased total scores on the Functional Independent Measure in stroke patients after bilateral robotic training. More convincing evidence of far transfer was demonstrated by Rasova et al 38 who evaluated a targeted training approach for postural control in patients with multiple sclerosis. Their behavioral results showed significant improvements not only in gross motor functioning but also in hand function after the training. The authors explained this far transfer effect by the nonvoluntary activation of all motor functions (both postural functions and hand functioning) during this motor program activating therapy resulting in global effects on motor functioning.
The question remains whether these statistically significant far transfer effects following therapy are clinically significant. That is, it is important to investigate whether the change in behavioral scores meets the criteria for a minimal clinically important difference, on the basis of previous established behavioral studies. The evaluation of clinical significance however, has not yet been performed in most of the reviewed articles (see Table 4, Q4). In one of the few studies, Bird et al 26 showed that one patient demonstrated a change in Motor Activity Log (MAL) in response to sensorimotor training, but this change was not clinically meaningful. In contrast, the change in MAL scores in a second patient exceeded the minimal clinically important difference and could be considered as a meaningful change. In this case, the posttest score approached levels of the age-matched healthy population.
To further clarify the issue of transfer, the analysis of behavioral and brain data needs to be combined by computing relationships between improved behavioral function and MRI-measured changes. Surprisingly, the majority of the surveyed studies have not performed correlations with behavioral outcomes,34,36,38,44 as can be seen in Tables 1 to 3. Although correlations between behavioral changes and structural brain alterations do not imply causation, they do provide evidence of a relationship between pre- and post- training. 48 For example, training-induced changes in standing balance were accompanied by changes in FA of the superior cerebellar peduncles in multiple sclerosis patients (correlation coefficients, left superior cerebellar peduncle: r = 0.40, P = .038; right: r = 0.395, P = .042). 37 The magnitude of grey matter increases in the sensorimotor regions and hippocampus were significantly correlated with amount of improvement in real world arm use in chronic stroke patients receiving CIMT (rs = 0.45-0.49, Ps < .024). 21
Reminding us of the preliminary nature of this work, the reported correlations between structural changes and behavioral improvements were weak to moderate (accounting for 16%-24% of the total variance). In addition, correction for multiple comparisons was not performed in the above studies. Specifically, “uncorrected” thresholds and “trends” were often reported in relation to structural and/or behavioral changes when results did not reach statistical significance.22,28,29,44 For example, in Schlaug et al, 22 a “strong trend for a correlation” (r = 0.70, P = .10, N = 6) was reported between absolute change in the number of Correct Information Units/min produced during spontaneous speech and absolute change in number of arcuate fasciculus fibers. Although contemporary researchers and publishers are moving away from the importance of the P < .05 threshold, statistical analysis using uncorrected thresholds may lead to type I errors (false positives). Future studies should employ a more stringent threshold to ensure valid outcomes, although we acknowledge that trends could still be reported to help motivate future studies. Finally, significance tests should be accompanied by the report of effect sizes and confidence intervals.
A further important limitation is that not all studies have found relationships between specific difference scores in structural metrics and behavioral or clinical changes. In Nordvik et al, 25 microstructural changes did not correspond directly with behavioral improvements, which may have been due to nonspecific neural responses to training. The training program imposed prolonged cognitive demands that may have triggered changes in brain structure, but not necessarily in a way that covaried significantly with performance on neuropsychological tests. Negative findings may have also been due to the fact that the structural MRI metrics affected by ABI may not be the ones that cause behavioral deficits. As suggested by Thomas and Baker, 48 more advanced statistical analyses are required to reveal what may be the complex nonlinear relationships between structural and behavioral changes. Only one study so far, by Han et al, 45 assessed associations between nonmonotic changes in the brain and improvement in neuropsychological performance. Future studies are needed to determine (a) whether the observed structural brain changes are caused by or are an effect of the behavioral changes, (b) the dynamics of the interaction between these brain structures and behavior, and (c) other neural processes that may control or be rate limiting factors in neurorehabilitation.
Which Structural Brain Metrics Are Sensitive Enough to Identify Training-Related Changes?
Although the voxel-based morphometry (VBM) approach has been debated for many years,57,58 the VBM approach has been used most frequently (see Tables 1-3, 11 studies) in studies of training-induced neuroplasticity in ABI. Importantly, a change in gray matter volume essentially refers to a change in intensity of the images, not a change in the real volume of the neurons. Interpretation of these changes in VBM parameters is not straightforward, as they can reflect changes in brain morphology, brain microstructure or a combination of both. The potential underlying mechanisms for gray matter changes include axon sprouting, dendritic branching, synaptogenesis, neurogenesis, changes in glia number and morphology, and angiogenesis. 59 Moreover, the grey matter probability values used in VBM do not correlate with quantitative histological measures of neuronal density. 60
Alternative measures of cortical morphometry are cortical thickness and surface area, which can be obtained using the FreeSurfer software package. Cortical thickness and cortical surface area reflect complementary aspects of the underlying neural architecture: cortical surface area is primarily determined by the number of columns within a cortical region, whereas cortical thickness is thought to reflect the number of cells within these cortical columns. Therefore, evaluation of either or both metrics can provide additional information to better understand the mechanisms of neuroplasticity in ABI. Only 3 studies so far have evaluated changes in cortical thickness with training in ABI patients.27,43,45
Diffusion metrics should also be used carefully and interpreted cautiously. Increases in the number of reconstructed streamlines are often interpreted as new fibers appearing after training. For example, in Lazaridou et al 27 the number of fibers and the average tract length of the corticospinal tracts significantly increased after eight weeks of hand motor function training in chronic stroke patients. The authors interpreted these increases as new fibers projecting. Similarly, in response to intense speech therapy, Schlaug et al 22 interpreted an increase in number of fibers and volume of the arcuate fasciculus of the right hemisphere as a “remodelling of the right arcuate fasciculus.” However, these interpretations are presumptuous because tractography results can be heavily biased. 61 Tractography approaches based on more advanced diffusion models, such as constrained spherical deconvolution 62 may provide more accurate structural connectivity patterns in future ABI neuroplasticity studies.
In addition to these limitations, the training-induced FA increases in the reviewed articles (see Tables 1-3, Figure 2) are often interpreted as increased myelination. For example, Prosperini et al 37 state that, “The improvement of FA in both superior cerebellar peduncles after the 12-week training period was mainly due to a reduction in radial diffusivity, suggesting an enhancement of myelination-related processes driven by training-induced white matter plasticity after high-intensity, task-oriented exercises.” A more cautious interpretation is warranted because FA is modulated by many factors, such as changes in myelination, axon density/diameter and the layout of the axons within the image-voxel. 61 Taken together, FA is quite a nonspecific tool and it remains unclear what biological factors underpin training-induced FA changes. Indeed, reliance on FA can even lead to apparently counter-intuitive results. For example, a treated group of stroke patients showed a reduction in FA in the white matter underlying the right inferior frontal gyrus, which also correlated with improvements in speech fluency. 29
Future studies are required to investigate structural neuroplasticity using novel in vivo techniques to identify training-induced changes in markers believed to be more sensitive to axon density and myelin. In our recent studies,63,64 we investigated white matter plasticity in healthy adults with specific MRI scans that identified training-induced changes in axon density (with the composite and hindered model of diffusion CHARMED) 65 and myelin (with the relaxometry based mcDESPOT pipeline). 66 MRI methods with improved specificity (such as relaxometry) have not yet, to our knowledge, been used to study neuroplasticity in brain-injured patients. The field of neuroplasticity in brain-injured patients would greatly benefit from quantitative MRI scans that produce neurobiologically validated measures, providing detailed information about the cellular and molecular mechanisms.
Conclusion
This review finds supporting evidence of structural neuroplasticity in brain-injured patients. The amount of time needed for these structural changes was not entirely clear, but we suggest that training interventions culminate in robust effects if the training intervention is both intense and long term. Only a few studies have found direct relationships between neuroplastic changes and behavioral improvements. Yet, we have argued that this evidence is preliminary, does not afford strong statements on causality, and that more controlled studies are required to clarify that nature of dose effects, the specificity of training effects, and transfer. With developments in technology (eg, stronger magnets/gradients), the underlying cellular changes will become more apparent. We contend that future studies utilizing adequate control conditions, larger groups, intermittent scans and accurate registration procedures will be crucial to obtain robust evidence for the effects of training and neuroplasticity for brain injured patients. This approach combined with volumetric assessment and diffusion metrics in whole-brain network connectivity may ultimately help clinicians to improve strategies for neurorehabilitation.
Footnotes
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website, along with the online version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was facilitated by an ACURF Program grant awarded to Karen Caeyenberghs by the Australian Catholic University (ACU).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.