
Abstract
Background. Motor training alone or combined with transcranial direct current stimulation (tDCS) positioned over the motor cortex (M1) improves motor function in chronic stroke. Currently, understanding of how tDCS influences the process of motor skill learning after stroke is lacking. Objective. To assess the effects of tDCS on the stages of motor skill learning and on generalization to untrained motor function. Methods. In this randomized, sham-controlled, blinded study of 56 mildly impaired chronic stroke patients, tDCS (anode over the ipsilesional M1 and cathode on the contralesional forehead) was applied during 5 days of training on an unfamiliar, challenging fine motor skill task (sequential visual isometric pinch force task). We assessed online and offline learning during the training period and retention over the following 4 months. We additionally assessed the generalization to untrained tasks. Results. With training alone (sham tDCS group), patients acquired a novel motor skill. This skill improved online, remained stable during the offline periods and was largely retained at follow-up. When tDCS was added to training (real tDCS group), motor skill significantly increased relative to sham, mostly in the online stage. Long-term retention was not affected by tDCS. Training effects generalized to untrained tasks, but those performance gains were not enhanced further by tDCS. Conclusions. Training of an unfamiliar skill task represents a strategy to improve fine motor function in chronic stroke. tDCS augments motor skill learning, but its additive effect is restricted to the trained skill.
Introduction
Worldwide, stroke is the leading cause of persistent motor disability. Despite significant functional recovery in the first 3 to 6 months after injury,1,2 many patients remain substantially limited by chronic motor impairment that interferes with independent living,3,4 prompting a need to identify therapeutic interventions that could promote recovery well into the chronic stage.
The central tenet in stroke rehabilitation is motor training.5,6 In healthy individuals, training leads to motor skill changes that take place during practice (online learning) and in between training sessions (offline learning) and may be maintained over time (long-term retention).7-10 In patients with chronic stroke, training also improves motor skills.11-18 However, the integrity of the different learning stages over multiple training sessions has not been explored in detail after stroke.
Transcranial direct current stimulation (tDCS) modulates cortical excitability19,20 and promotes synaptic plasticity in a polarity-dependent fashion.21,22 In healthy humans, tDCS with the anode placed over the primary motor cortex improves motor skill learning.9,10,23,24 tDCS combined with physical or occupational therapy can also improve functional motor outcomes after stroke.25-28 However, clear recommendations for therapeutic use of tDCS are currently not given because of heterogeneity in outcome variables, interventions, and study populations. 29 Moreover, these previous studies did not specifically evaluate training or tDCS effects on the stages of motor skill learning during therapy or their interactions. After stroke, tDCS with the anode placed over the ipsilesional primary motor cortex also enhances skill learning within a single session,30,31 with posttraining skill levels maintained for about 1 week. However, replicability of this finding has been questioned. 32 The influence of tDCS on stages of motor skill learning over multiple days (online and offline learning and long-term retention) are unknown. This information is needed to gain insight into the mechanisms by which noninvasive brain stimulation influences motor learning after stroke and to optimize dosing and timing of interventional brain stimulation protocols in neurorehabilitation.
Here, we investigated the influence of repeated training, tDCS, and their interaction on stages of multisession motor skill learning after chronic stroke. Our primary hypothesis was that tDCS would enhance total learning. Additionally, we explored whether skill improvements generalize to untrained tasks compared with a no-training/no-tDCS group and whether generalization is affected by tDCS. Finally, we assessed patient characteristics that may affect total learning or the response to tDCS, such as lesion anatomy or the BDNF val66met polymorphism.
Methods
Patients and Experimental Design
This prospective, randomized, sham-controlled, blinded study was approved by the institutional review board at the National Institute of Neurological Disorders and Stroke (NINDS), National Institutes of Health (NIH) and the local Ethics Committee of the University of Freiburg. The study was preregistered (http://www.clinicaltrials.gov, NCT00314769) and conducted in accordance with the declaration of Helsinki. All patients gave written informed consent. Eight patients were tested at the NIH site; 48 patients were subsequently tested in Freiburg, Germany, using the same experimental setup.
Clinical Assessment
Chronic stroke patients were screened by a detailed clinical interview and exam, standardized questionnaires, and genotyping for the BDNF val66met polymorphism (DNA analysis described previously 21 ). Details are shown in Figure 1B, Table 1, and in Supplementary Methods. Inclusion criteria were the following: (1) age 18 to 80 years, (2) unilateral, first ever ischemic stroke more than 3 months before study enrollment, (3) mild to moderate hemiparesis with residual hand function sufficient for task performance, (4) clear hand preference as assessed by the Edinburgh Handedness Inventory, 33 and (5) sufficient cognitive function to comply with study requirements. Patients at the Freiburg site had structural magnetic resonance imaging (MRI) done to characterize lesion anatomy. NIH patients did not receive scans because of contraindications, personal reasons, or logistic reasons.
Patient Information, Psychophysical, and Baseline Behavioral Data. a
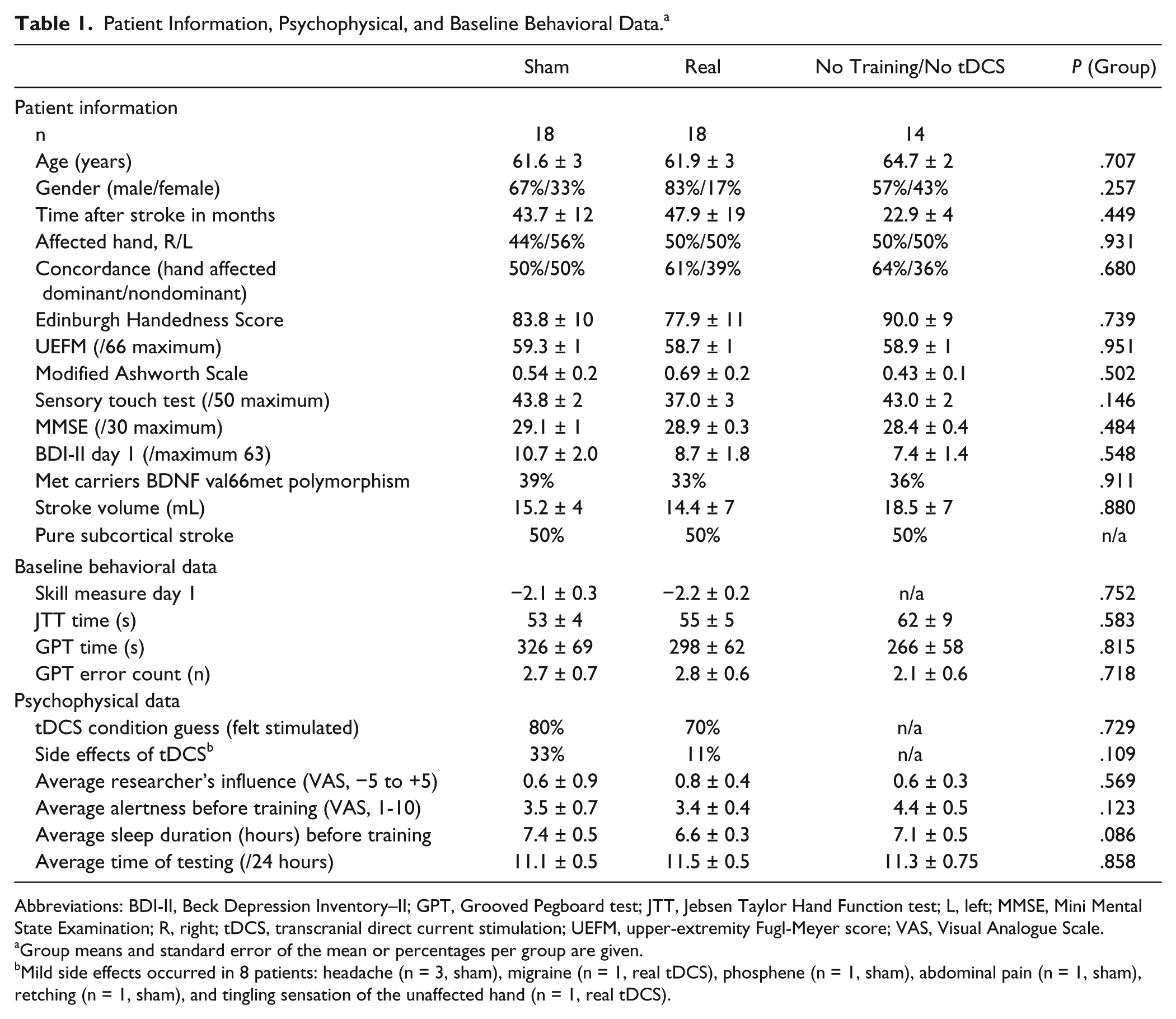
Abbreviations: BDI-II, Beck Depression Inventory–II; GPT, Grooved Pegboard test; JTT, Jebsen Taylor Hand Function test; L, left; MMSE, Mini Mental State Examination; R, right; tDCS, transcranial direct current stimulation; UEFM, upper-extremity Fugl-Meyer score; VAS, Visual Analogue Scale.
Group means and standard error of the mean or percentages per group are given.
Mild side effects occurred in 8 patients: headache (n = 3, sham), migraine (n = 1, real tDCS), phosphene (n = 1, sham), abdominal pain (n = 1, sham), retching (n = 1, sham), and tingling sensation of the unaffected hand (n = 1, real tDCS).
Study Design
The study consisted of 5 days of consecutive training and 5 follow-ups over 4 months (Figure 1A). Sessions took place between 8
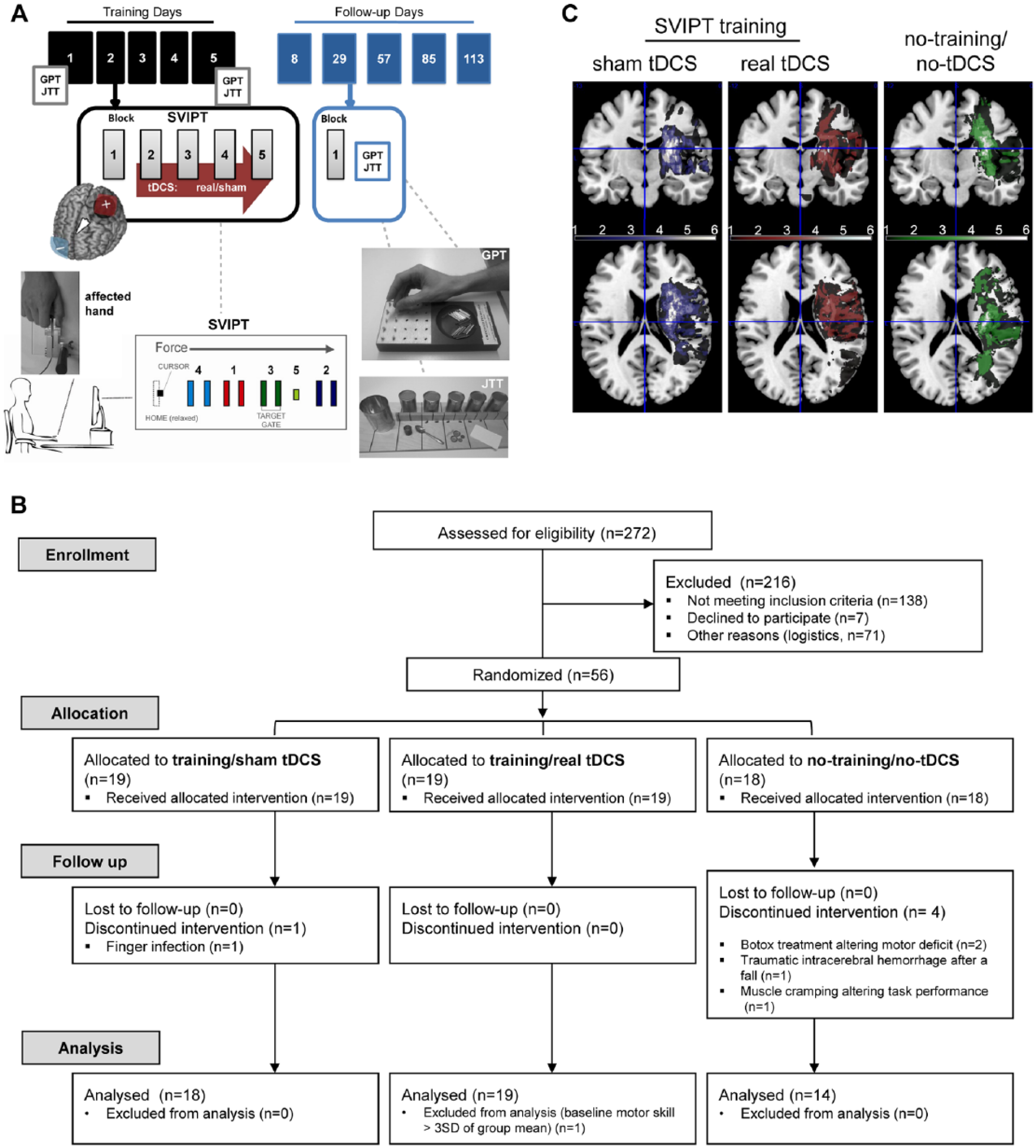
Study design: A. Patients trained for 5 consecutive days and were then subjected to 5 follow-up visits. During training, they received real (0.4 A/m2) or sham transcranial direct current stimulation (tDCS) for 20 min/d, with the anode targeting the primary motor cortex (M1) of the affected hemisphere. A training session consisted of 5 blocks of 20 trials of the sequential visual isometric pinch force task (SVIPT). At the beginning of day 1, the end of day 5, and all follow-ups, the Jebsen Taylor hand function test (JTT) and the Grooved Pegboard test (GPT) were also performed. The no-training/no-tDCS group performed only the generalization tasks without receiving training or tDCS. B. CONSORT flow diagram of the study. C. The summarized binary lesion overlay for each study group is shown: blue, sham tDCS; red, real tDCS; green, no-training/no-tDCS group. Color key (dark to bright) ranges from 1 to 6 patients. The majority of patients had an infarction mainly located along the pyramidal tract and particularly in the internal capsule. Stimulation groups were well matched for their lesion anatomy and volume. VLSM revealed no group differences.
Real and Sham tDCS Groups (n = 18 Each)
Patients practiced a modified version of the sequential visual isometric pinch force task (SVIPT 10 ; Figure 1B) with their paretic hand for approximately 45 min/d (5 × 20 trials with short breaks between blocks to avoid fatigue). As in a previous study, 10 patients squeezed a force transducer between thumb and index finger to move a cursor as quickly and accurately as possible through a fixed pattern of 5 target gates on a computer screen. Patients received visual feedback based on the cursor location, which partially allowed them to interpret their success—for example, in case a target was not hit correctly (over-/undershoots). There was no additional feedback provided by the investigators. After the first training block of each day, real or sham tDCS was applied for 20 minutes to the M1 of the affected hemisphere. Stimulation started after block 1 to keep the first training block free of online stimulation effects for the analysis of offline learning. Training outlasted the stimulation on the first day, but as patients became faster over time, training blocks were spaced to align with stimulation duration. To assess the generalization of hand motor skill learning to upper-extremity function, patients performed the Jebsen Taylor Hand Function test (JTT) and the Grooved Pegboard test (GPT; Figure 1B) at the beginning of the first and the end of the fifth training day and after SVIPT assessment at each follow-up. The JTT was performed 3 times, and the GPT was performed twice. These tests were chosen because they are both executed unimanually and require pinch and grip movement elements (the pinch showing similarity to the SVIPT), and both have been reliably used in stroke patients.34-37
No-Training/No-tDCS Group (n = 14)
Patients performed only the JTT and GPT on days 1 and 5, and at each follow-up time point. They did not undergo SVIPT training or tDCS. This group was implemented to discern repetition effects of the JTT and GPT on their performance from generalization effects of SVIPT training and tDCS.
Transcranial Direct Current Stimulation
We followed our published standard operating protocol 38 for the determination of the cortical hotspot using single-pulse transcranial magnetic stimulation (here: the M1 hotspot at which consistent motor evoked potentials (MEPs) were evoked in the contralateral (paretic) first dorsal interosseus muscle). MEPs were present in all patients. The anode (25 cm2) was centered over the ipsilesional M1 hotspot, and the cathode (25 cm2) was placed over the contralateral supraorbital area. In the real tDCS condition, 20 minutes of 1mA current was delivered (current density 0.4 A/m2, total charge 0.048 C/cm2). Sham tDCS was ramped up and then down over 30 s to induce similar scalp sensations as real stimulation. Stimulation was delivered in a single-blind manner (Phoresor II, Iomed) at the NIH site and double blinded (Neuroconn DC-Stimulator plus, with study mode) at the Freiburg site. tDCS blinding success was assessed by asking patients to guess whether they received active or inactive stimulation.
Refinement of the Mathematical Skill Model
For determination of motor skill, the speed accuracy assessment described previously 10 was refined to incorporate more fine-grained detail about force precision. Movement time (time from movement onset until reaching the fifth target) and target error rate (percentage of missed targets per training block) were combined into a single index, the skill parameter. The speed-accuracy trade-off function specific to stroke patients was obtained from an unrelated subset of patients to mathematically model skill (see supplementary data). The function generated was as follows:

where a is the skill parameter incorporating a performance’s target error rate and movement time, and 3.43 is the constant. “Skill” reflects the log-transformed skill parameter ln(a).
Analysis of Skill Learning and Generalization
Overall Training Effect
After comparing baseline skill (block 1, day 1) to ensure comparability of the groups, we assessed the success of training by evaluating time (day 1 block 1, day 5 block 5) and group differences (sham, real tDCS) in skill as well as their interaction using a repeated-measures analysis of variance (ANOVA).
Total Learning (Primary Outcome)
As before in Reis et al, 10 the primary outcome measure was total learning—that is, the sum of skill changes occurring by the end of training (last block on day 5). These skill changes were compared between groups.
Learning Stages
Online learning was defined as the sum of skill differences between the first and last block of each of the 5 training days. Offline learning was defined as the sum of skill differences between the last and first block of consecutive days. Retention was defined as the delta between the last block on day 5 and the block on day 113, and the rate of forgetting was the time-weighted slope of skill over all follow-ups after training. For all these measures, positive values correspond to a skill gain, whereas negative values express a skill loss. To relate the skill remaining at day 113 to the individual skill level achieved by the last block of day 5, retention was additionally expressed as a proportion of skill retained at day 113.
Generalization
For each patient and assessment, we averaged the overall time to complete each JTT repetition, and the time and errors to complete the GPT. For the JTT and GPT, percentage change in speed (total time to complete the task) was assessed for day 5 and each of the follow-ups (day n) as

so that a positive value implies a reduction in time and, therefore, an improvement in speed. For GPT accuracy, the absolute change (delta) in errors was calculated across time points as
Absolute accuracy change = Day 1 errors − Day n errors,
so that a positive value implies a reduction in errors and, therefore, an improvement in accuracy. We assessed GPT errors as absolute change because several patients made zero errors, precluding a relative assessment. These parameter changes were compared between the 2 stimulation groups and the no-training/no-tDCS group and across time in a multivariate model.
Online Learning on the First Day
To enable comparison with the previous literature, learning within the first training day (the skill difference between the first and last block of day 1) was analyzed.
Cumulative Learning Probability
We specifically addressed the cumulative learning probability using Kaplan-Meier analysis. A skill change of 1 was used as “time to event.” This criterion was chosen based on visual inspection of the skill changes (see Figure 2A), which corresponds to the value that sham patients clearly exceeded during training and maintained long term. A skill change of 1, thus, represents a minimum state of skilled proficiency, which all individuals did not naively have but could potentially achieve with training (disregarding a possible tDCS-related placebo effect in the sham condition). For each patient, we identified the time point (training block) at which this proficiency was achieved, and the proportion of patients per group was counted and/or censored. Censoring applied to those patients in whom the time to event could not be determined because skill remained below our threshold criterion until the end of training. A binomial effect size display (BESD 39 ) was used to describe by which percentage the likelihood to reach a skill gain >1 increases under the influence of tDCS.
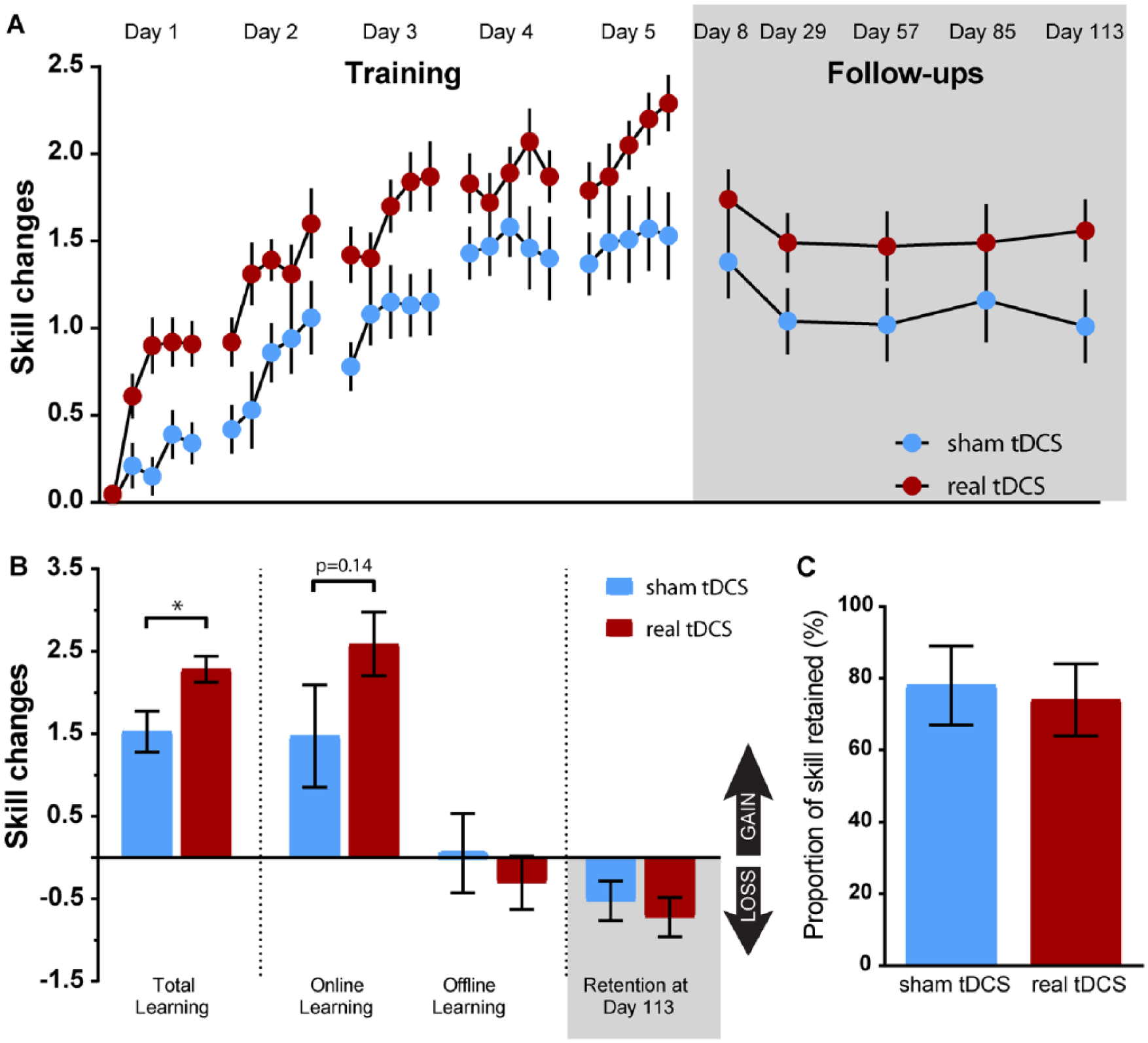
Measures of motor skill learning during the training and follow-up periods: A. Skill learning curve over 5 training days (5 blocks per day) and the follow-up period. The patients receiving real transcranial direct current stimulation (tDCS; red dots) showed significantly greater improvement of motor skill and outperformed sham stimulated patients (blue dots) at all time points. The majority of acquired skill was retained after the end of training. At day 113, the real tDCS group showed greater remaining skill compared with sham tDCS. B. Higher total learning in the real tDCS group (red) was predominantly a result of greater online (within session) learning. C. The proportion of skill retained at day 113 was similar in the 2 stimulation conditions, suggesting that real tDCS did not per se affect long-term retention. Significance: *P < .05. All data are shown as group mean ± standard error of the mean.
Relation Between Online and Offline Learning
We explored the relation between online and offline skill changes and asked whether tDCS would specifically perturb it. Correlations between online and offline skill changes were calculated per group. To discern an effect of tDCS on the online-offline relation, the 2 correlation coefficients were transformed with the Fisher’s Z-transformation, and the Z-scores were compared.
Changes in Movement Time, Target Error Rate, and Movement Smoothness
To further discern which aspects of skill had changed over training, movement time, target error rate, and movement smoothness were assessed as separate measures. Smoothness characterizes variations in the movement jerk, the third derivative of the recorded movement force profile, which is expressed as the integrated squared jerk (ISJ). 40 The normalized jerk (NJ) multiplies the ISJ, such that it results in a unitless number40,41:

Smoothness is reported as the inverse value (1/NJ). We evaluated time and group effects on each of the 3 parameters at day 1 and 5.
Correlation of Total Learning With Patient Characteristics
Baseline performance, time since stroke, stroke lesion volume, lesion location, stroke concordance (dominant hand affected), and the BDNF val66met polymorphism may conceivably influence patients’ capacity to train, learn, or respond to tDCS.1,21,32,42 We correlated the first 3 parameters with total learning to address the role of these potential confounders. For lesion location, concordance, and the BDNF val66met polymorphism, total learning was compared between subgroups of patients. Lesion location on the MRI was rated as either subcortical or combined lesion (subcortical plus cortical). The BDNF val66met polymorphism state was categorized as either BDNF val/val or as BDNF met carrier (val/met or met/met).
MRI Stroke Lesion Assessment
Lesion detection, lesion overlays (Figure 2), and voxel-based lesion symptom mapping regarding the lesion anatomy were performed as described previously 43 (see Supplementary Methods).
Psychophysical Assessment
Side effects, sleep duration, researcher’s influence (visual analogue scale [VAS] from −5 [very negative] to +5 [very positive]), and alertness (VAS from 1 to 10 [perfectly alert to extremely tired]) were recorded daily. To detect any longer-lasting mood changes, patients completed the Beck Depression Inventory (BDI) and the Positive and Negative Affect Scale on days 1, 5, and 8.
Statistical Analysis
Sample size calculation is provided in Supplementary Methods. Following the Shapiro-Wilk test for normal distribution, group differences were assessed using the 2-tailed t-test or ANOVA comparisons with Bonferroni-Holm corrected post hoc tests. The 2-sided significance level was set to P <.05. Effect size is given as Cohen’s d (<0.5 indicating a small, 0.5-0.7 a moderate, and >0.7 a strong effect). 44
The overall training effect was assessed using a repeated-measure ANOVA with factors Time (d1 block 1, d5 block 5) and Group (sham, real tDCS). The primary outcome parameter was total learning, which was assessed as group difference between real and sham tDCS groups (t-test). Further t-tests were used to assess group differences in baseline skill, online learning, offline learning, retention measures, and learning on the first day. JTT speed, GPT speed, and GPT accuracy changes were compared using 2 multivariate ANOVAs. First, we addressed time and overall group differences related to training state (training vs no training) as well as their interactions. Second, time and overall group effects related to the tDCS condition (sham vs real tDCS) as well as their interactions were assessed. Significant findings were then further analyzed in univariate models for the 3 parameters (change in JTT speed, GPT speed, and GPT accuracy). The cumulative learning probability was measured by Kaplan-Meier analysis with Mantel-Cox log rank statistics. Time-related changes in movement time, target error rate, and movement smoothness were assessed by separate repeated-measures ANOVAs. Correlations were assessed using Pearson’s r, and group differences were compared using Fisher’s z-transformation. Stroke lesion volume and concordance was compared between subgroups of patients by independent t-tests. To take the effect of the BDNF val66met polymorphism on learning into account, total learning per genotype and tDCS condition was compared using 4 planned independent t-tests (Supplementary Methods). In addition, demographic data (Table 1) were compared between groups using separate 1-way ANOVAs. Binary data were compared using the χ2 test. Changes in BDI were assessed using repeated-measure ANOVA (Table 1, Supplementary Table 1). Anatomical lesion distribution was compared between groups using the VLSM Liebermeister procedure of the MRIcron nonparametrical mapping tool. 45
Results
Demographic and Psychophysical Data
Of 272 screened patients, 56 patients were enrolled in the study (Figure 1B). Five patients did not complete the study for the following reasons: finger infection interfering with task execution (n = 1), Botox treatment during the follow-up period altering the motor deficit (n = 2), traumatic intracerebral hemorrhage after a fall (n = 1), and muscle cramping interfering with performing the tests (n = 1). One patient (baseline skill >3 SD worse than all others, UEFM 42, severe hand fatigue during training) was excluded. Consequently, data from 50 patients (n = 18 real tDCS, n = 18 sham tDCS, n = 14 no-training/no-tDCS) were analyzed. The 3 groups were comparable in terms of demographical and clinical data (Table 1, Figure 1C, and Supplementary Table 1). The voxel-wise lesion-symptom mapping analysis did not reveal a group difference in lesion anatomy (P > .01, FDR corrected). Participants tolerated the tDCS intervention well and were successfully blinded for the type of stimulation (Table 1). They rated the perceived influence of the investigator on their performance similarly neutral to slightly positive in all 3 groups. Regardless of intervention, patients displayed lower values on the BDI on day 5, suggesting a mood-enhancing effect of the study context.
Motor Skill Learning and Generalization
Sessions took place at about 11
Overall Training Effect
Across groups, skill increased significantly over time of training [F(1, 34) = 167.96; P < .0001; d = 4.45)], and the effect was catalyzed by tDCS, as indicated by a significant Group × Time interaction: F(1, 34) = 6.60; P = .015; d = 0.88. There was no effect of group: F(1, 34) = 0.56; P = .461; d = 0.25.
Total Learning (Primary Outcome)
Total learning was significantly enhanced by tDCS (2.29 ± 0.16 real tDCS vs 1.53 ± 0.25 sham tDCS group; t(34) = −2.57, P = .02, d = 0.86; Figure 2B, Supplementary Table 2). These values reflect unitless “skill” changes of the log-transformed skill parameter ln(a).
Learning Stages (Online Learning, Offline Learning, Retention, Rate of Forgetting)
Numerical values are presented in Supplementary Table 2. Compared with sham tDCS, patients showed more online learning and less offline learning when stimulated with real tDCS (Figure 2B), but no statistical differences were found: t(34) = −1.53, P = .14, d = 0.51; t(34) = 0.62, P = .54, d = 0.20, respectively. As shown in Figure 2A, most of the skill resulting from training was retained in the follow-ups, regardless of stimulation type. However, there was no specific effect of tDCS on long-term retention assessed at day 113 (Figure 2B; t(34) = 0.58, P = .56, d = 0.16). Accordingly, the time-weighted slope of forgetting over all follow-up time points was not different between groups: t(34) = 0.37; P = .71; d = 0.12. The proportion of skill retained on day 113 was similar in both conditions (78% ± 11% sham vs 74% ± 10% real tDCS; t(34) = 0.29, P = .77, d = 0.10; Figure 2C). For visual illustration of online and offline learning as well as retention on individual days, see Supplementary Figure 4.
Skill Gains Remaining at the End of the Study
Because real tDCS stimulated patients showed greater total learning, and retention was unaffected, we also found a strong trend for greater remaining skill at the end of the study compared with sham tDCS: t(34) = −1.98; P = .056; d = 0.66.
Generalization
To assess the effects of hand training and tDCS on generalization, we tested patients for improvements in untrained motor tasks (JTT, GPT). This group comparison included the no-training/no-tDCS group. Patients started with similar performances on the 2 tasks (Table 1; JTT speed: F(2, 47) = 0.55, P = .58; GPT speed: F(2, 47) = 0.21, P = .82; GPT errors: F(2, 47) = 0.33, P = .72). After training, GPT accuracy improved in the 2 training groups, whereas it was poorer in the no-training/no-tDCS group (Figure 3A). GPT speed (Figure 3B) improved in all groups. Training was also associated with greater improvements in JTT speed compared with the no-training/no-tDCS group (Figure 3C). The MANOVA (GPT accuracy, GPT speed, JTT speed) revealed a main effect of time [F(5, 30) = 6.28; P < .0001; d = 0.81] and training state [F(1, 42) = 3.203; P = .033; d = 0.58] on generalization, but no interaction (F = 0.795; P = .67; d = 0.29). Per univariate analysis, differences related to training state were present in GPT accuracy (F = 4.59; P = .038; d = 0.69) and JTT speed (F = 4.534; P = .039; d = 0.69) but not GPT speed (F = 0.145; P = .71; d = 0.12).
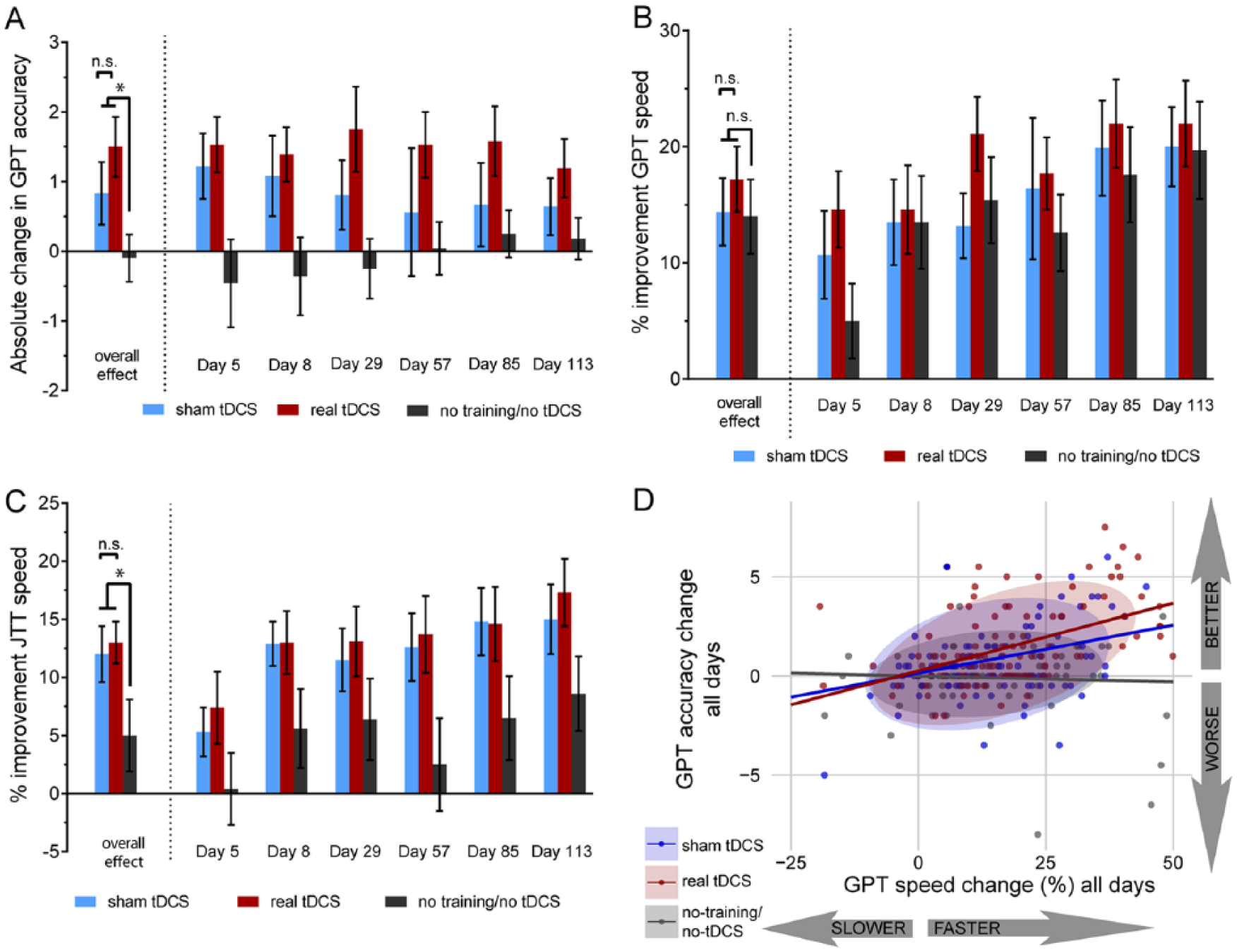
Measures of generalization after sequential visual isometric pinch force task training and during the follow-up period: A. Grooved Pegboard test, paretic hand; improvement measured by absolute change in accuracy relative to day 1. Both training groups showed increased accuracy (a reduction in number of errors is indicated by positive values) on all days, whereas the no-training/no–transcranial direct current stimulation (tDCS) group showed less accuracy (ie, trading accuracy for higher speed). The MANOVA revealed a significant effect of training compared with no training/no-tDCS, but no additional effect of real tDCS compared with sham tDCS. B. Grooved Pegboard test, paretic hand, percentage improvement in speed (total time to complete the test) relative to day 1. Both training groups and the no-training/no-tDCS group showed improvements in total time. There was no significant difference between trained and untrained patients or between sham and real tDCS stimulated patients. C. Jebsen Taylor test (JTT), paretic hand; percentage improvement in speed (total time to complete the full test) relative to day 1. The MANOVA revealed a significant effect of training compared to no- training/no-tDCS, independent of tDCS stimulation type. The no-training/no-tDCS group showed only minor improvements (repetition effects). D. The Grooved Pegboard test (GPT) accuracy change is plotted against the GPT speed change. Data from all time points were used for illustration of the lacking relationship between the 2 variables in the no-training/no-tDCS group, compared with the strong positive relationship in the 2 trained groups (indicating improvements in both variables). The real tDCS group shows the greatest improvements in accuracy for a given speed change. The ellipses indicate the 90% confidence interval per group, the lines represents the mean centered linear regression line per group. Significance: *P < .05. All data except for panel D (single subject data) are shown as group mean ± standard error of the mean.
When testing for an additive effect of tDCS, no significant differences between the 2 tDCS conditions were detected in the MANOVA: group F(1, 28) = 0.396; P = .757; d = 0.22. As expected, there was a significant effect of time [F(5, 42) = 6.42; P < .0001; d = 0.87] but no interaction (F = 1.562; P = .192; d = 0.43).
Because the separation of GPT performance into 2 parameters (speed and accuracy) may mask potential changes in the speed-accuracy trade-off, we additionally plotted speed and accuracy changes at all time points for visual inspection of their relationship. Figure 3D suggests a loss of accuracy to achieve higher speeds in the no-training/no-tDCS group, in contrast to the improvement of both parameters in the 2 trained groups.
Online Learning on the First Day
For comparison with previous studies commonly using a single session design, we also assessed learning on the first training day, which was significantly greater for real than sham tDCS: t(34) = 3.29; P = .002; d = 1.1.
Cumulative Learning Probability
A greater proportion of patients in the real tDCS group required less training amount to reach a skill gain >1 compared with sham tDCS (χ2 = 8.44, P = .004, d = 1.88, Figure 4A). In other words, proficiency was achieved significantly earlier during training in the real tDCS group. Using the BESD, these data suggest that if treated with real tDCS, the likelihood to reach this particular level of skill increases by 11.1%, corresponding to a number needed to treat of 9 patients.
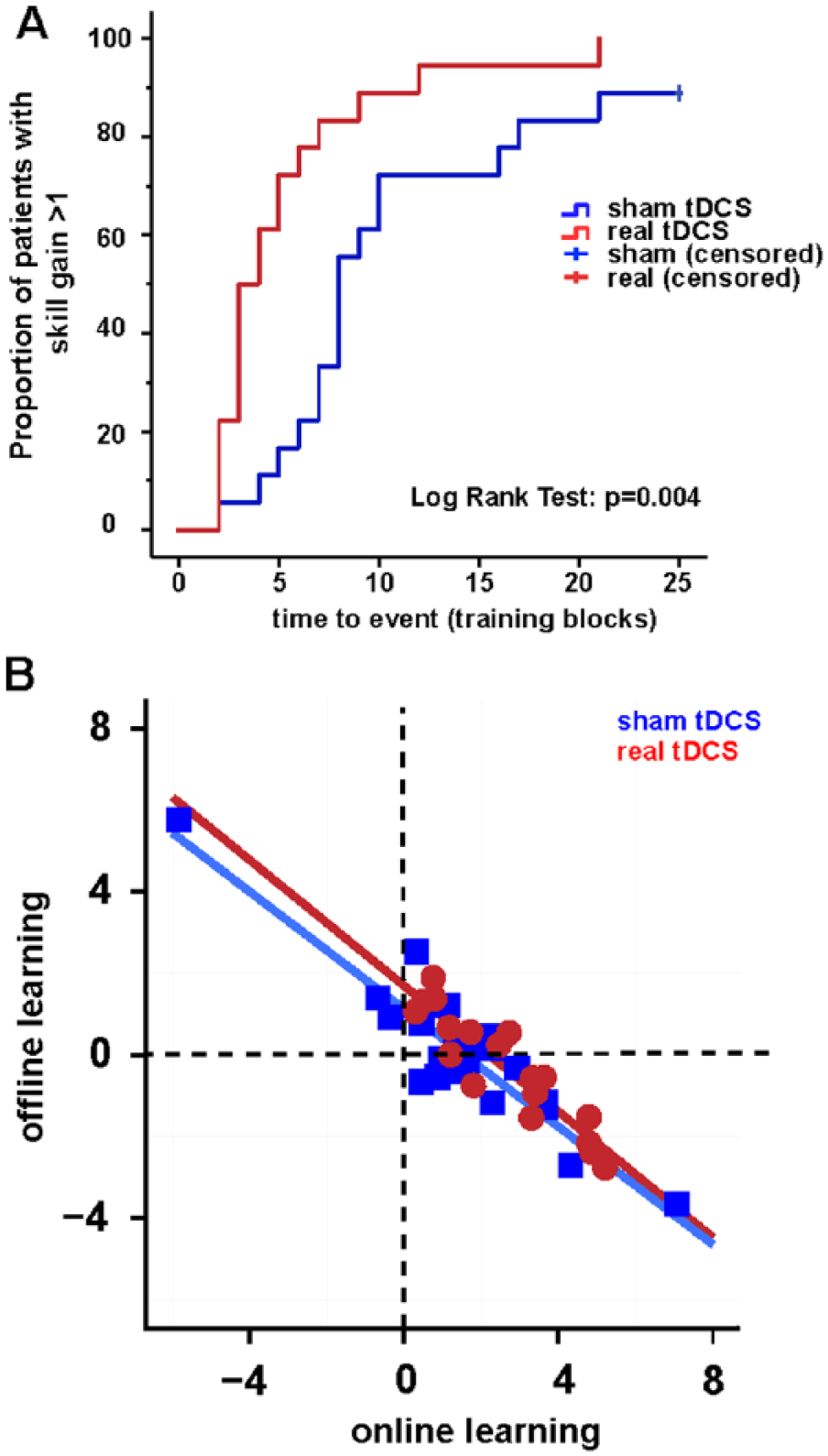
Analysis of cumulative learning probability and correlation of learning subcomponents: A. Compared with sham transcranial direct current stimulation (tDCS; blue), patients reached a minimum skill gain of 1 unit earlier, when training was combined with real tDCS (red). A skill gain of 1 unit represents the average level of skill reached by the sham tDCS group and was extrapolated from a predictive model. Note that the sham tDCS group is censored—that is, the Kaplan Meier interval for the time to event (100% of patients reaching the criterion) is not known for this particular group. This happened because few patients did not reach a skill gain of 1 within the 25 training blocks. B. There was a strong negative correlation between online and offline learning during training across groups. Real tDCS (red circles and line) shifted the set point for occurrence of offline skill loss toward higher online learning compared with sham (blue squares and line).
Relation Between Online and Offline Learning
Patients gained skill mainly by online learning and subsequently maintained skill between sessions (Figure 2B). Interestingly, those patients showing the greatest online learning also showed the least offline learning: that is, there was a strong negative correlation (r = −0.929, P < .0001; Figure 4B). Patients receiving real tDCS also showed this negative correlation (r = −0.918; P < .0001), which was not altered compared to sham (z = −0.205; P = .419). However, the set point for the occurrence of negative offline learning (forgetting) was shifted toward greater online learning (Figure 4B).
Changes in Movement Time, Target Error Rate, and Movement Smoothness
Movement time and target error rate decreased, whereas movement smoothness increased across training days [F(1, 34) = 95.433, d = 3.35; F(1, 34) = 43.931, d = 2.273; and F(1, 34) = 28.961, d = 1.846, respectively; all P < .00001, Figure 5]. The real tDCS group had significantly faster movement times across sessions compared with sham (Group × Time interaction: F(1, 34) = 8.595; P = .006; d = 1.01), whereas target error rate decreased similarly across sessions with both stimulations (Group × Time interaction: F(1, 34) = 0.178; P = .676; d = 0.145). Moreover, real tDCS increased the quality of the movement across sessions—that is, movement smoothness relative to sham (Group × Time interaction: F(1, 34) = 4.167; P = .049; d = 0.7). There were no differences for factor group.
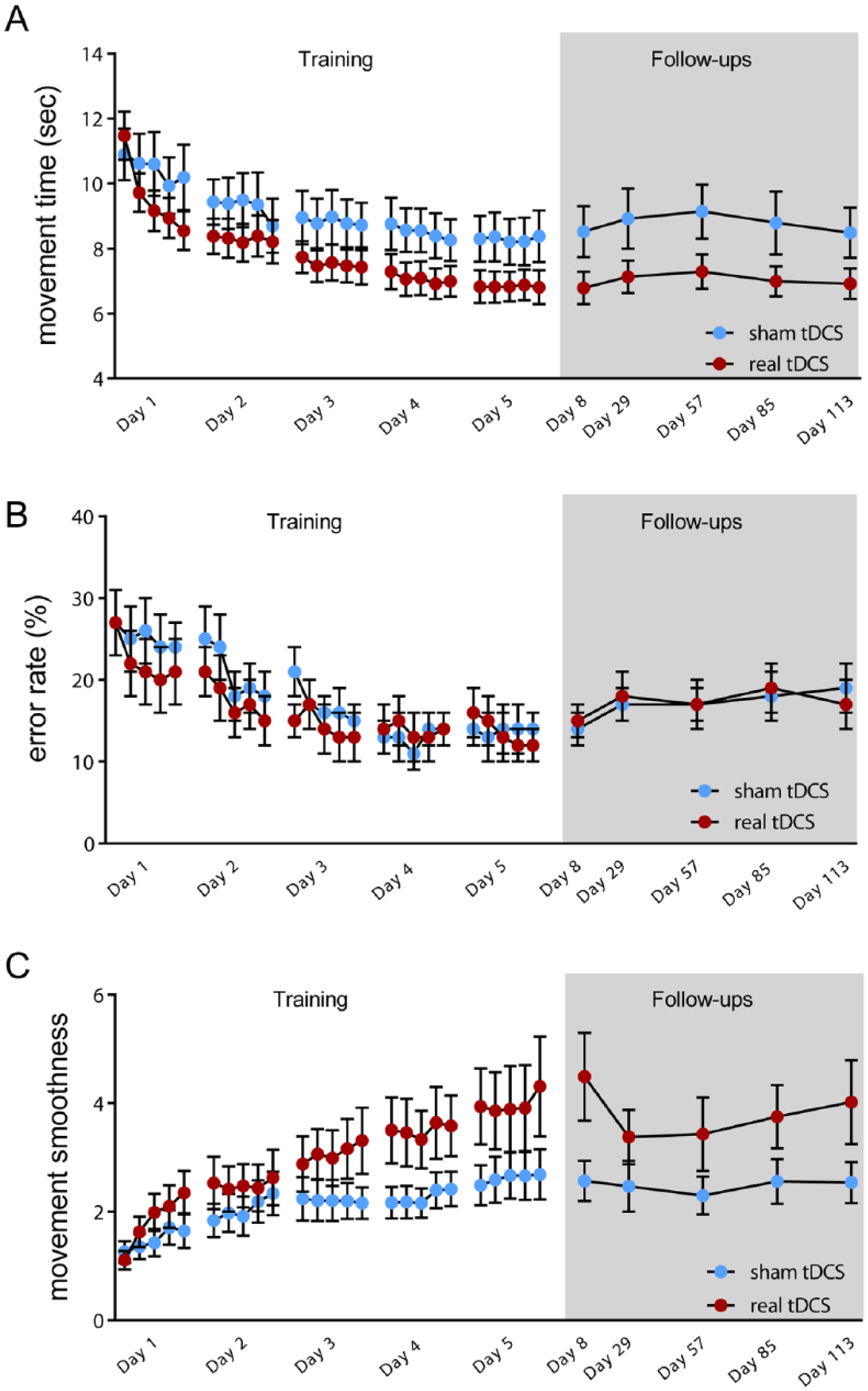
Learning curves for the 5 training days and the follow-up period for movement time, error rate, and movement smoothness: A. Movement time: both groups showed improvements in movement time; real transcranial direct current stimulation (tDCS) significantly shortened movement time across sessions compared with sham tDCS. B. Error rate: both groups reduced the error rate over 5 days; no significant differences were found between real and sham tDCS. C. Movement smoothness: real tDCS significantly enhanced movement smoothness across sessions compared with sham tDCS. All data are shown as group mean ± standard error of the mean.
Correlation of Total Learning With Patient Characteristics
Total learning was not influenced by starting performance (R2 = 0.09; P > .9), time since stroke (R2 = 0.21; P > .9), lesion volume (R2 = 0.002; P = .785), lesion location (all t < 0.51; P > .05) concordance (sham: t(16) = 0.23, P = .81; real tDCS: t(16) = 0.09, P = .93), or BDNF genotype (sham: t(16) = 0.89, P = .39; see supplementary results). Across those individuals receiving real tDCS, BDNF met carriers tended to demonstrate less total learning compared with BDNFval/val patients (t(16) = 1.93, P = .072; Supplementary Figure 5B).
Discussion
In a group of mildly impaired chronic stroke patients, we found that tDCS applied to the ipsilesional M1 during training enhanced learning of the trained skill, predominantly through an effect on the online learning stage. Training was associated with long-lasting generalization to untrained upper-extremity motor function, with no additional benefit of tDCS.
Stages of Visuomotor Learning in Stroke Patients
Chronic stroke patients displayed successful visuomotor learning over multiple days, regardless of stimulation condition. Our findings extend those of single session motor learning studies, which have shown within-session improvements and intact short-term retention of skill.11,14,17,46,47 They also affirm studies finding that patients improve in single performance variables (ie, movement time) or on speed-accuracy relationships after multisession motor training.13,15,16,18,48 Here, we specifically assessed the stages of motor learning, which had not been previously investigated. We showed that similar to healthy individuals, 10 skill was acquired mainly within session (online), and patients never returned to naïve skill levels between days, indicating motor memory consolidation (ie, offline maintenance). Interestingly, online and offline skill gains were negatively correlated—that is, offline skill loss occurred in the patients with greatest online learning. These findings suggest that there may be an intrinsic set point during the learning process—for example, by homeostatic cortical network regulation,49,50 which is difficult to exceed under physiological conditions. Similar to our findings in healthy individuals 10 and even with less-intense training (500 vs 1000 trials) and a longer follow-up period (4 vs 3 months), improved skill across patient groups was retained. Collectively, these findings suggest the integrity of the stages of motor learning in chronic stroke patients, despite disordered poststroke anatomy.
tDCS Accelerates and Enhances Visuomotor Learning in Chronic Stroke
tDCS applied to M1 enhances motor skill learning over multiple days in healthy individuals.9,10 Similar findings were observed on a first/single training day in elderly individuals 24 and chronic stroke patients.30,34 Single-session study designs hinder disambiguation between effects of tDCS on performance versus effects on the learning process.10,51,52 We, therefore, assessed multisession online learning, offline learning, and long-term retention. In keeping with our findings in healthy individuals,10,23 total learning was significantly enhanced in real tDCS-stimulated stroke patients compared with the sham group. A beneficial effect of real tDCS on online learning present on day 1 is consistent with previous studies23,30,34 but was not found for the cumulated online learning over 5 days. Because the majority of stroke patients are older adults, it is worth noting that real tDCS-stimulated elderly healthy individuals demonstrate greater day 1 online learning than sham-stimulated individuals, without an effect on offline learning assessed the next day. 24 Similarly, in the present study, offline learning over multiple days did not differ between sham and real tDCS patients. These findings are in contrast to our studies in healthy individuals, where real tDCS predominantly enhanced offline learning.10,23 Hence, there may be a mechanistic difference in how tDCS affects the learning process in the elderly or injured brain, enhancing the acquisition of a skill without augmenting its subsequent consolidation. It is conceivable that healthy individuals saturate online learning through a greater number of training trials or through more proficient learning mechanisms, and real tDCS effects cannot modify this threshold. In the stroke patients, conversely, online learning may remain unsaturated (because of poorer baseline performance, fewer training trials, or less proficient learning mechanisms), resulting in a modifiable process by real tDCS. However, we found an inverse relationship between online and offline learning regardless of stimulation, pointing to a specific set point for the capacity of the motor system to gain skill. Real tDCS slightly altered this relationship compared with sham, such that for given online gains, there was marginally less offline loss. It is, thus, tempting to speculate that offline learning processes may be secondarily influenced as a consequence of a specific effect of tDCS on online learning—for example, through metaplastic effects. 49 As in healthy individuals, 10 retention of acquired skill was not affected by real tDCS. It is, thus, important to note that any long-lasting benefit of real tDCS (ie, skill remaining at day 113) is derived from the primary effect in the training period. Although this is the only study on long-term skill retention extending several months, similar findings are visible in previous studies that suggest a lack of effect of tDCS on short-term retention.30-32,34
Training, but Not tDCS, Improves Generalization of Visuomotor Learning
To be considered a valuable interventional tool in neurorehabilitation, tDCS combined with training should ideally improve motor function beyond its augmentation of trained skills. Here, we observed generalization after SVIPT training, evidenced by enhanced accuracy on the GPT and faster execution speed in the JTT. Such improvements were not found in the nontrained, nonstimulated patients. This third group enabled us to disambiguate learning effects resulting from repetition of the probe tasks from generalization of effects from training. We found no additional benefit of tDCS on generalization compared with sham. A recent meta-analysis revealed an overall beneficial effect of tDCS in combination with various motor training/therapy concepts in subacute and chronic stroke patients. 53 This effect was evident as improved performance on either clinical scales (eg, UEFM, NIHSS) or motor-specific task improvements (9-hole peg test, visuomotor tracking). Allman et al 25 reported improved clinical scores resulting from real tDCS combined with bimanual motor training, evident for at least 3 months after training. One group has also found enhanced generalization on a pegboard task 1 week after a single session of bihemispheric tDCS and unimanual visuomotor training 30 (but findings were not replicable in a similar study design 32 ). It is difficult to interpret such improvements as motor generalization because these studies lacked nontrained and nonstimulated control groups. Our study extends these findings, showing robustness of training-related generalization for 4 months after the end of training but no additive effect of tDCS.
tDCS-Improved Skills Result From a Speed-Based Shift in the Speed-Accuracy Trade-off
The majority of previous tDCS studies in stroke patients did not specifically address the speed-accuracy trade-off.25,34,46,48 In the SVIPT, healthy individuals and chronic stroke patients (performing with the elbow flexors) typically improve skill through a reduction in movement time while also improving or maintaining a constant error rate.18,54,55 Here, our sham tDCS patients improved skill on the SVIPT through reductions in both movement time and error rate. Relative to sham, the real tDCS group further reduced movement times, without differences in error rate. Hence, tDCS led to a predominantly speed-based (leftward) shift in the speed-accuracy trade-off, extending on a similar finding following a single training session in another visuomotor task. 30 Because movement smoothness significantly increased with real tDCS, it is conceivable that better movement control contributed to the ability to perform the task at higher speeds without sacrificing accuracy. We consider this further evidence that tDCS does not solely affect a single component of movement (eg, speed) but rather changes the relation between different movement components. Depending on the task, this may be reflected differently in the speed-accuracy parameter space. Similar to the SVIPT, training-related improvements in the GPT were a result of greater accuracy changes at similar to slightly faster movement times compared with the no-training/no-tDCS group. However, tDCS did not affect this speed-accuracy trade-off, providing further evidence for the restriction of the tDCS effect to the trained skill.
Limitations and Clinical Implications
We found evidence for a task-specific training-enhancing effect of tDCS with the anode applied over the ipsilesional primary motor cortex in chronic stroke patients. Because this study was planned and powered to address cumulative effects of tDCS on total learning as well as online/offline effects across 5 days of training, we are unable to assess stimulation effects on individual training days. Given the ostensible lack of focality of tDCS, 56 we are also unable to infer which stimulated cortical areas may contribute most to learning. Because our study required that patients have sufficient hand function to execute the SVIPT, it is unclear how our results would translate to more severely affected patients. We observed long-lasting generalization to untrained upper-extremity function resulting from training but no additional benefit provided by tDCS. Whereas this limitation may relate to our choice of well-recovered patients and our focus on skill tasks, future studies could include a more impaired patient cohort and more multifaceted generalization measures to comprehensively gauge stimulation effects in the clinical context. Moreover, it is important to investigate these effects in the acute stage of stroke, when tDCS-augmented activity-dependent plasticity could positively interact with injury-induced plasticity.
Supplemental Material
Supplementary_Material – Supplemental material for Transcranial Direct Current Stimulation Enhances Motor Skill Learning but Not Generalization in Chronic Stroke
Supplemental material, Supplementary_Material for Transcranial Direct Current Stimulation Enhances Motor Skill Learning but Not Generalization in Chronic Stroke by Manuela Hamoudi, Heidi M. Schambra, Brita Fritsch, Annika Schoechlin-Marx, Cornelius Weiller, Leonardo G. Cohen, and Janine Reis in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We thank Dr Marco Curado and Dr Christoph Kaller for help with data visualization as well as Gerd Strohmeier and Frank Huethe for technical realization of the SVIPT setup.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HMS was supported by a National Institutes of Health NINDS Intramural Competitive Postdoctoral Fellowship and K23NS078052; financial support for the work at the Freiburg site is provided by the German Research Foundation (MH, AS-M, BF, JR; DFG grant number RE 2740/3-1). LGC was supported by the Intramural Research Program of the National Institutes of Health, NINDS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.