
Abstract
Background. The proportional recovery rule suggests that current rehabilitation practices may have limited ability to influence stroke recovery. However, the appropriate intensity of rehabilitation needed to achieve recovery remains unknown. Similarities between rodent and human recovery biomarkers may allow determination of rehabilitation thresholds necessary to activate endogenous biological recovery processes. Objective. We determined the relative influence that clinically relevant biomarkers of stroke recovery exert on functional outcome. These biomarkers were then used to generate an algorithm that prescribes individualized intensities of rehabilitation necessary for recovery of function. Methods. A retrospective cohort of 593 male Sprague-Dawley rats was used to identify biomarkers that best predicted poststroke change in pellet retrieval in the Montoya staircase-reaching task using multiple linear regression. Prospective manipulation of these factors using endothelin-1-induced stroke (n = 49) was used to validate the model. Results. Rehabilitation was necessary to reliably predict recovery across the continuum of stroke severity. As infarct volume and initial impairment increased, more intensive rehabilitation was required to engage recovery. In this model, we prescribed the specific dose of daily rehabilitation required for rats to achieve significant motor recovery using the biomarkers of initial poststroke impairment and infarct volume. Conclusions. Our algorithm demonstrates an individualized approach to stroke rehabilitation, wherein imaging and functional performance measures can be used to develop an optimized rehabilitation paradigm for rats, particularly those with severe impairments. Exploring this approach in human patients could lead to an increase in the proportion of individuals experiencing recovery of lost motor function poststroke.
Introduction
Optimization of rehabilitation efficacy to maximize poststroke recovery is a primary goal of preclinical and clinical stroke research. 1 Identification of biomarkers in individuals likely to obtain the most benefit from poststroke therapy is crucial to streamline health care system resources and offer the best quality of care to patients.2,3 Corticospinal tract damage beyond a certain threshold, 4 and lack of motor-evoked potentials, 5 are indicative of limited potential for poststroke recovery. Furthermore, patients who show potential for recovery inevitably plateau at ~70% of their maximum possible on a given scale.6-12 These findings, combined with the low rates of change in patients receiving outpatient stroke rehabilitation, 13 have led to the suggestion that current rehabilitation practices may not provide benefits beyond those that occur spontaneously. 14
Alternatively, a threshold intensity, or “dose,” of rehabilitation may be needed to activate endogenous recovery processes.1,15 The role of rehabilitation dose has been studied in the chronic poststroke phase, 16 although the appropriate threshold needed to achieve recovery remains unknown.15,17 However, because of the ethics of withholding treatment, determining the magnitude and efficacy of rehabilitation effects is exceedingly difficult to address in the acute poststroke phase in humans. 18
In a companion article, we demonstrated that initial poststroke impairment alone predicts recovery of upper-limb function in rats, as in humans. This cross-species homology suggests that other aspects of the stroke recovery process may also be conserved between species. Identification of additional recovery biomarkers in rodent models may enable the determination of rehabilitation thresholds necessary to activate recovery processes.19-21 Such a rehabilitation threshold could be applied using principles of personalized medicine 22 and serve as a theoretical basis for further development of human prediction and stratification algorithms for stroke recovery.23-25 This is one of the few avenues of stroke recovery research that shows real promise to improve patient outcomes 26 amid a sea of failures.27,28
The present study sought to answer 4 key questions: (1) In addition to the proportional recovery rule, do other biomarkers of human stroke recovery (ie, lesion severity) also apply to rats? (2) Can these biomarkers be used to create a predictive model of poststroke recovery that is applicable to any animal, irrespective of stroke severity, and does rehabilitation modulate this model? (3) Can the manipulation of these biomarkers influence recovery as predicted by our model? (4) By using biomarkers of recovery, can we accurately prescribe individualized intensities of rehabilitation that will generate significant recovery of function? If so, what is the accuracy of such a prescription?
Methods
As discussed in our companion article, all available raw data for experiments within the Corbett laboratory that met the following criteria were collated in a single master dataset:
Subjects: Male, Sprague-Dawley rats (age range 2.5-4 months at time of surgery)
Focal ischemia: Unilateral intracerebral endothelin-1 (ET-1) administration
Functional assessment: Pellet retrieval in the Montoya staircase-reaching task
Assessment timeline: Minimum of 3 measurements: prestroke, within 1 week poststroke, and final assessment no earlier than 3 weeks poststroke (time of terminal assessment ranged from 3 to 10 weeks)
The retrospective dataset compiled using these criteria was composed of N = 672 subjects from a number of published19,29-33 and unpublished (at the time of writing) experiments. None of the data from these experiments had been previously used to study the proportional recovery rule. The institutional animal care committees of either Memorial University of Newfoundland and Labrador or University of Ottawa approved all procedures performed on these subjects.
Retrospective Analysis/Modeling
Rats were excluded from the analysis if they did not have a measurable deficit, relative to prestroke performance, at the initial poststroke time point. This was calculated using a 95% confidence interval of each rat’s prestroke performance. If an individual animal fell outside of this confidence interval at the poststroke time point then the rat was determined to have at least a minimal level of impairment. On average, this minimal level of impairment was a decrease of at least 2.42 pellets from prestroke to poststroke. In an effort to maximize the range of rats included in the study, this minimal detectable impairment level was used as the cutoff criterion for inclusion. After excluding animals, 593 subjects remained in the final staircase analysis.
Characteristics with statistically significant differences between fitters and nonfitters of the proportional recovery rule from our companion article were advanced as variables of interest for linear regression to test their ability to predict change in pellet retrieval (PR) from the initial to terminal poststroke assessment (ΔPRObserved = PRTerminal − PRInitial). Additionally, subcharacteristics of our rehabilitation paradigm were also analyzed to determine which aspects of the treatment were likely to have the greatest impact on recovery (Supplementary Table 1). The final list of possible predictors included initial poststroke pellets retrieved, cortical and striatal infarct volume (mm3), whether an animal had significant striatal injury (>3.0 mm3), and the mean number of pellets retrieved in rehabilitation per day. Rats were only included in regression analysis if data were available for all predictors, leading to a further reduction in total N. Of the original 383 rats that did not receive rehabilitation, 151 did not have data available on infarct volume. Of the 210 rats that received rehabilitation, infarct volume data were missing from 87. This resulted in final Ns of 232 rats that did not receive rehabilitation and 123 rats that did receive rehabilitation for predictive modeling. Predictors were eliminated using backward stepwise procedures until all remaining predictors were significant at α = .05 or the adjusted R2 decreased. 6 Extra sum-of-squares F tests were used to assess model fit between rehabilitated and nonrehabilitated groups. All significant regression predictors were examined using variance inflation factor <0.1, collinearity tolerance (tolerance > 10), eigenvalue, and condition index statistics (>15) as potential indicators of multicollinearity problems. Model cross-validation was conducted by using half of the total sample (determined at random) as the training set for calculating recovery model parameters. This model was then validated against the other half of the total sample as the testing set. No indicators of multicollinearity between predictor variables were detected. This recovery model demonstrated good cross-validation with the 95% confidence intervals of all predictor Bs overlapping between the training and testing subsets.
Equation to Prescribe an Individualized Recommendation for Rehabilitation Intensity in Rats
a
.
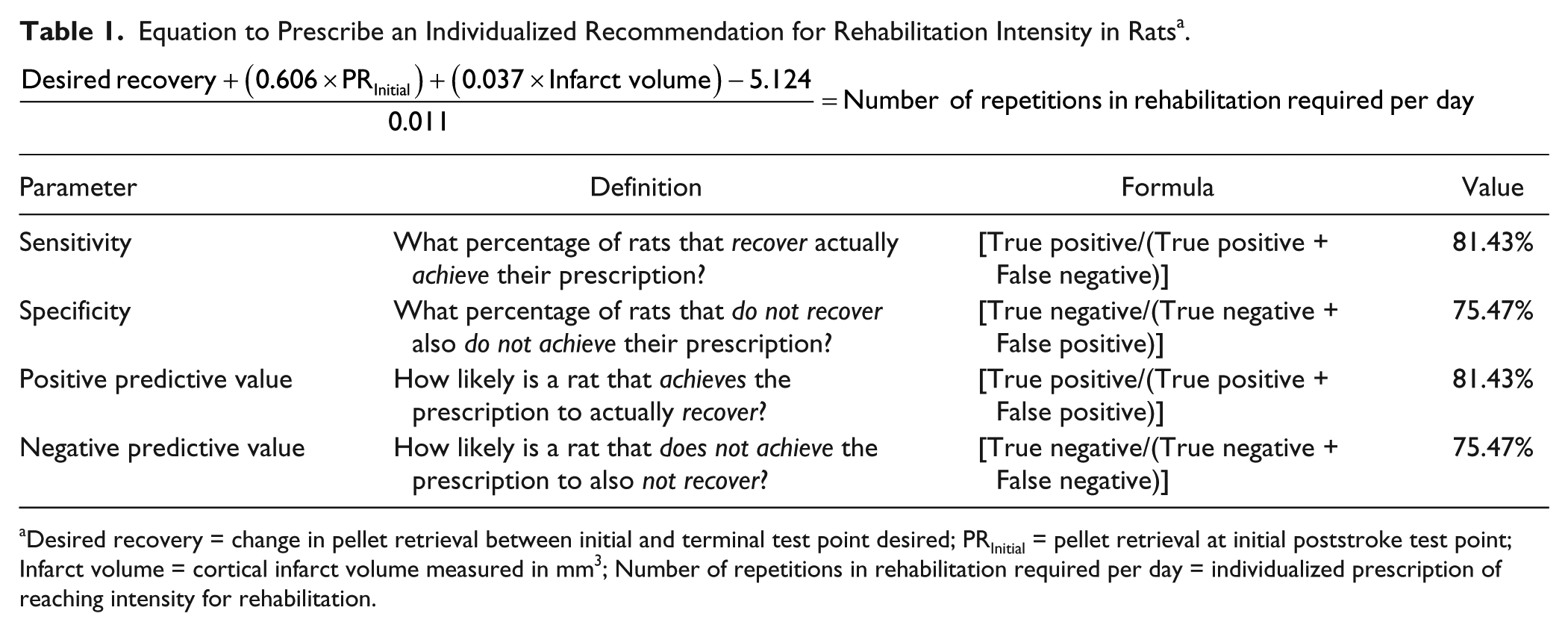
Desired recovery = change in pellet retrieval between initial and terminal test point desired; PRInitial = pellet retrieval at initial poststroke test point; Infarct volume = cortical infarct volume measured in mm3; Number of repetitions in rehabilitation required per day = individualized prescription of reaching intensity for rehabilitation.
Experimental Validations of Predictive Model
A total of 49 male Sprague-Dawley rats (experiment 1, n = 27; experiment 2, n = 22) weighing 200 to 250 g on arrival were used for these experiments. Animals were handled for ~5 minutes each for 5 days to facilitate acclimatization to the experimenters. Rats were housed in groups of 2 to 4 on a reverse 12-hour light/dark cycle (9
Stroke Induction
All subjects had focal ischemia induced via intracerebral injection of the vasoconstrictive peptide ET-1 (Abcam, ab120471), using previously published coordinates and methodologies.34,35 Rats were given strokes 1 to 2 days after the last day of baseline motor testing. Anesthesia and body temperature were maintained with 1.5% to 2% isoflurane and at 36.5°C using heating blankets, respectively. Rats were placed in a stereotaxic apparatus and a small incision was made in the scalp. Two (for cortical-only) or 3 (for cortical + striatal) small burr holes (~1.0 mm diameter) were drilled through the skull. One hundred-micrograms of ET-1 was dissolved into 100 µL of sterile water to make a 400 pmol/µL solution. Ischemic injury was produced in each rat by injection of 2 to 3 µL of the ET-1 solution using a 0.485 mm inner diameter Hamilton syringe. The injected hemisphere was contralateral to the rat’s dominant or most proficient paw in the baseline staircase test. For each injection, the needle was inserted over 30 seconds. Once the needle was introduced, ET-1 was injected (1 µL/site) after a 1-minute wait period. After injection of the ET-1, the syringe remained in place for 2 minutes to reduce backflow. The coordinates of the cortical injections were as follows: 0.0 and 2.3 mm anteroposterior (AP), ± 2.5 mm mediolateral (ML) and −1.7 mm dorsoventral (DV) relative to Bregma and the brain surface. The additional striatal injection was directed at 0.7 mm AP, ±3.8 mm ML and −7.0 mm DV relative to Bregma and the skull surface. These stereotaxic coordinates correspond to the forelimb sensorimotor cortex (for the cortical injections) and to the dorsolateral area of the striatum.
Forelimb Motor Assessment
Forelimb motor function of rats was assessed using the Montoya staircase-reaching task. 36 This involved rats performing reaching, grasping, and retrieval movements using the impaired forelimb in order to obtain food pellet rewards (45 mg TestDiet; Purified Rodent Tablet; 5TUL). Training and testing procedures followed a standardized protocol across all included experiments, as previously published.19,29-33 Rats received 2 weeks of daily training on the staircase skilled-reaching task prior to stroke. The assessment of prestroke performance occurred over the last 2 days of training. Procedures for staircase testing were identical for staircase training. Briefly, rats were placed in a reaching box for 15 minutes in which 21 pellets could be retrieved using the impaired forelimb along a 7-tiered descending staircase (Figure 1A). This apparatus allowed rats to only reach for pellets on the left with their left paw and on the right with their right paw. Rats were food restricted to 14 g per day the evening before testing to encourage reaching. Food restriction continued for the duration of each test period. Animal weights were measured once a week and maintained at ~95% to 100% of their free-feeding weight. Each day of testing consisted of two 15-minute trials separated by a period of approximately 4 hours. A test period involved 6 trials (3 days of testing, 2 trials/day) with the last 4 trials averaged to generate test point data. Testing was performed in the dark and white noise was turned on to allow the rats to acclimate and mask any distracting sounds. At the end of a trial, rats were returned to their cages and the number of pellets eaten by each animal was recorded and used to assess forepaw dexterity.
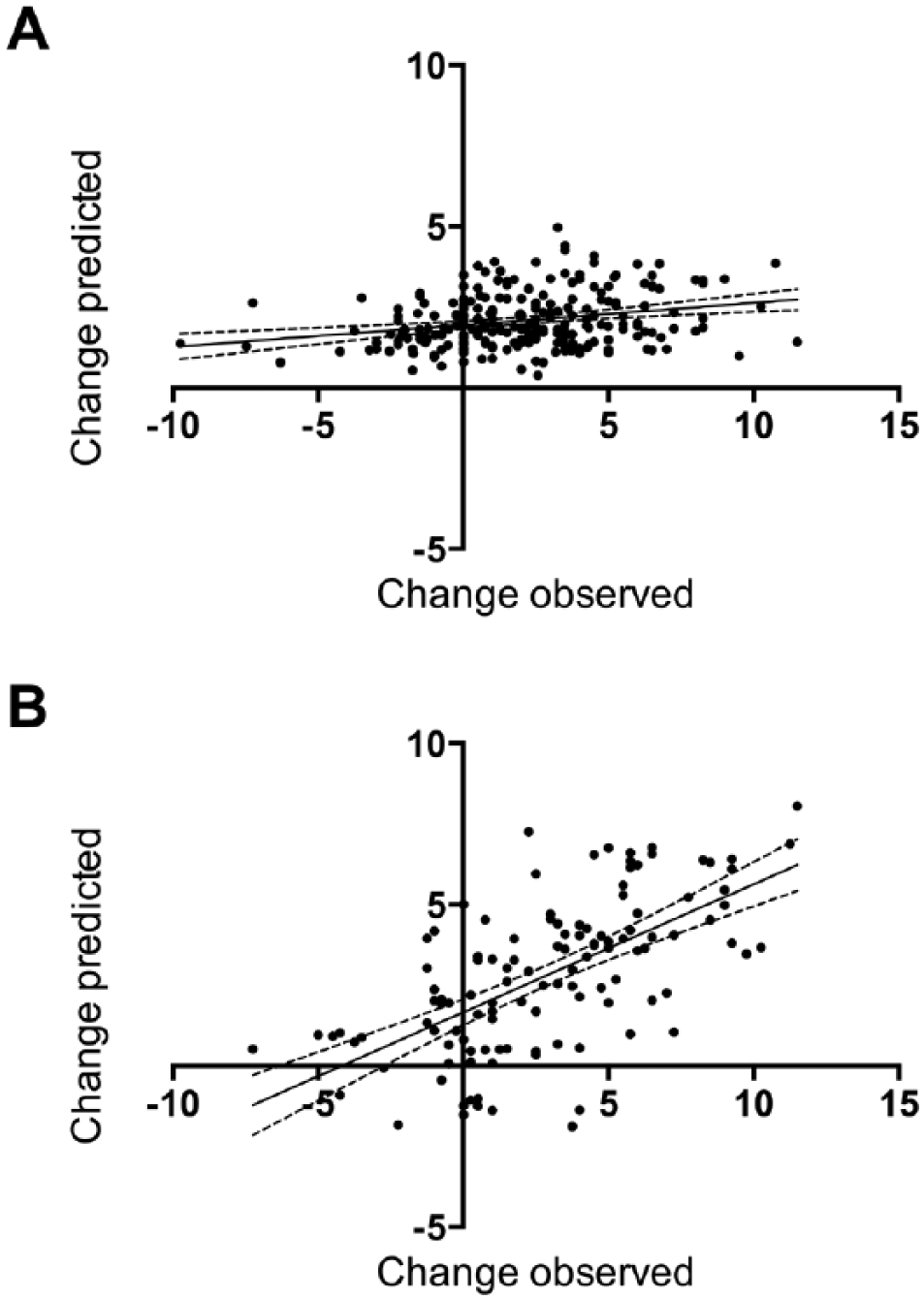
Examples of reaching chamber, environmental enrichment, and staircase task. (A) A rat reaching in the staircase task. (B) A typical environmental enrichment cage. (C) The daily reaching practice chamber used in Figure 3A-D. (D) A comparison with the voluntary access reaching practice chamber used in Figure 3E-H.
Rehabilitation Paradigm
Rehabilitation consisted of a combination of enriched environment housing (Figure 1B) and access to a modified staircase apparatus to practice task-specific reaching movements (Figure 1C), as previously described.37,38 Rats in the rehabilitation treatment group were housed in large ferret cages containing various objects that encouraged exploration and increased use of the impaired limb. Once a week, the cages were changed and made more challenging by varying the types of objects used and their placement in the cages. Rats in the nonrehabilitation group were housed in groups of 2 in Tecniplast Green Line IVC Sealsafe PLUS rat cages for the duration of the experiment and only removed during behavioral testing periods.
In conjunction with an enriched environment, rehabilitated rats were subjected to reaching practice at the beginning of the dark cycle, 5 days a week. Three times a day, rats were placed in Plexiglas reaching boxes that consisted of 2 shelves on either side of the rat separated by a central platform. The shelf beneath the impaired limb was filled with a large number of sugar pellets, and for 15 minutes, the rats were left to reach for pellets ad libitum. The 3 daily reaching sessions were separated by 45 minutes of rest, during which the rats were returned to their ferret-style cages. At first, 20 g of pellets were placed in each reaching box at the start of a reaching session, but this amount was reduced to 14 g to make the exercise more challenging once the rat had demonstrated its ability to reach at least 6 g of pellets. Nonrehabilitated rats were not subjected to daily reaching practice sessions and remained in their cages for the duration of the exercise.
In prospective experiment 1 (Figure 3A-D), a large reaching box with a closed back was used (Figure 1C). Rats were unable to leave the apparatus for the duration of the reaching session. In prospective experiment 2 (Figure 3E-H), a voluntary access reaching apparatus placed inside a regular rat cage was used. The back of the reaching box was open, which allowed the rats to enter and exit the apparatus, as they desired (Figure 1D).
Infarct Volume Quantification
Trained experimenters following standardized procedures performed analysis of infarct volume. Total hemispheric, cortical, and striatal infarct volumes were calculated using Nissl stained sections by subtracting the volume of intact tissue in the infarcted hemisphere from the volume of intact tissue in the noninfarcted hemisphere, as previously described. 19 The injury cutoff was selected as 3.0 mm3 because this is the amount of injury typically observed in ET-1 saline injection sham surgery in the Sprague-Dawley rat strain. 35
Statistical Analysis of Prospective Experiments
All statistical analysis was performed using SPSS software (v23, IBM Corp, Armonk, NY). Behavioral data across multiple time points was analyzed using repeated-measures analysis of variance. Single time-points and post hoc analysis was performed using Bonferroni-corrected t tests. Analysis of the relationship between reaching rehabilitation and staircase performance utilized nonlinear regression techniques with extra sum-of-squares F tests to determine the best fitting regression equation. Family-wise type I error was controlled to α = .05 as the significance cutoff for all tests using appropriate corrections for multiple comparisons.
Results
Initial Impairment, Infarct Volume, and Rehabilitation Intensity Predict Poststroke Recovery
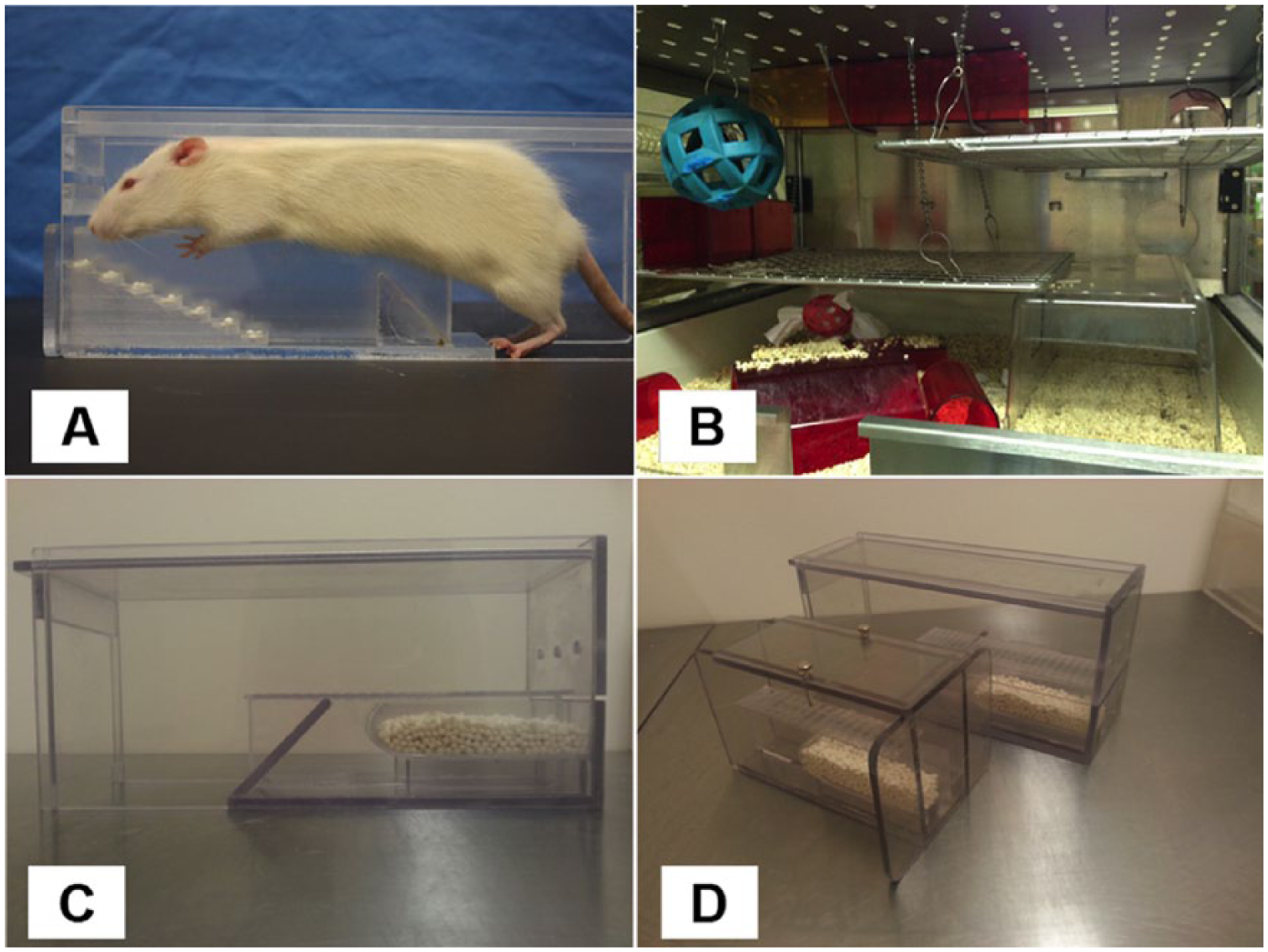
The capacity of initial poststroke pellets retrieved, cortical and striatal infarct volume (mm3), whether an animal had significant striatal injury (>3.0 mm3), and the mean number of pellets retrieved in rehabilitation per day to predict poststroke recovery was determined by linear regression. Separate analyses were conducted for rats that did and did not receive rehabilitation because of the inability to include number of reaching repetitions per day as a variable for nonrehabilitated animals. For rats tested in the staircase task without rehabilitation, initial poststroke pellet retrieval, cortical infarct volume, and presence of striatal injury were able to predict recovery. However, this model accounted for only 6.8% of the variance in recovery for these animals (Y = 0.0683X + 1.946, R2 = 0.06821, P < .0001, n = 232; Figure 2A). In strong contrast, 40% of variance in recovery (Y = 0.3973X + 1.661, R2 = 0.4036, P < .0001, n = 123; Figure 2B) was accounted for in rats that received rehabilitation based on initial pellet retrievals, cortical infarct volume, and mean reaches per day in rehabilitation. Extra sum-of-squares F test confirmed that rats that did and did not receive rehabilitation were best represented by different regression equations (F = 42.74, P < .0001). In the staircase task, rehabilitation is therefore a necessary component to accurately predict functional recovery. See Supplementary Table 2 for full regression parameters.
Goodness-of-fit for predictive models of recovery. (A) Rats in the staircase task without rehabilitation (Y = 0.0683X + 1.946, R2 = 0.06821, P < .0001, n = 232). (B) When receiving rehabilitation, an accurate prediction of recovery on the staircase task could be obtained using initial level of impairment, cortical infarct volume, and rehabilitation intensity (Y = 0.3973X + 1.661, R2 = 0.4036, P < .0001, n = 123). All graphs show regression lines with 95% confidence bands. See Supplementary Table 1 for β of predictors in each regression equation.
Manipulating Biomarkers Influences Recovery as Predicted by Our Model
We validated the ability of these biomarkers to predict recovery by performing prospective experiments in which identified biomarkers were manipulated. Varying degrees of infarct volume and presence/absence of rehabilitation were tested for their efficacy as predictors of stroke recovery (N = 27; Figure 3A-D). We used a 2 × 2 factorial design in which animals received either a cortical-only injury or a combination of cortical and striatal injury in conjunction with or without rehabilitation. All rats showed a sharp decrease in pellet retrieval on the staircase task 1 week following stroke with increases in performance by week 5 poststroke (Figure 3A, B). Large injury (ie, combination cortical and striatal stroke) resulted in poor poststroke recovery, with significantly less change in pellet retrieval between week 1 and week 5 compared with cortical-only injury (F = 6.692, P = .016; Figure 3C). Additionally, delivery of the rehabilitation paradigm resulted in significantly greater recovery than not receiving rehabilitation (F = 6.320, P = .003; Figure 3D). Descriptive characteristics for each subgroup can be found in Supplementary Table 3. These results validated our prediction that initial impairment, injury volume, and rehabilitation are important contributors to poststroke recovery.
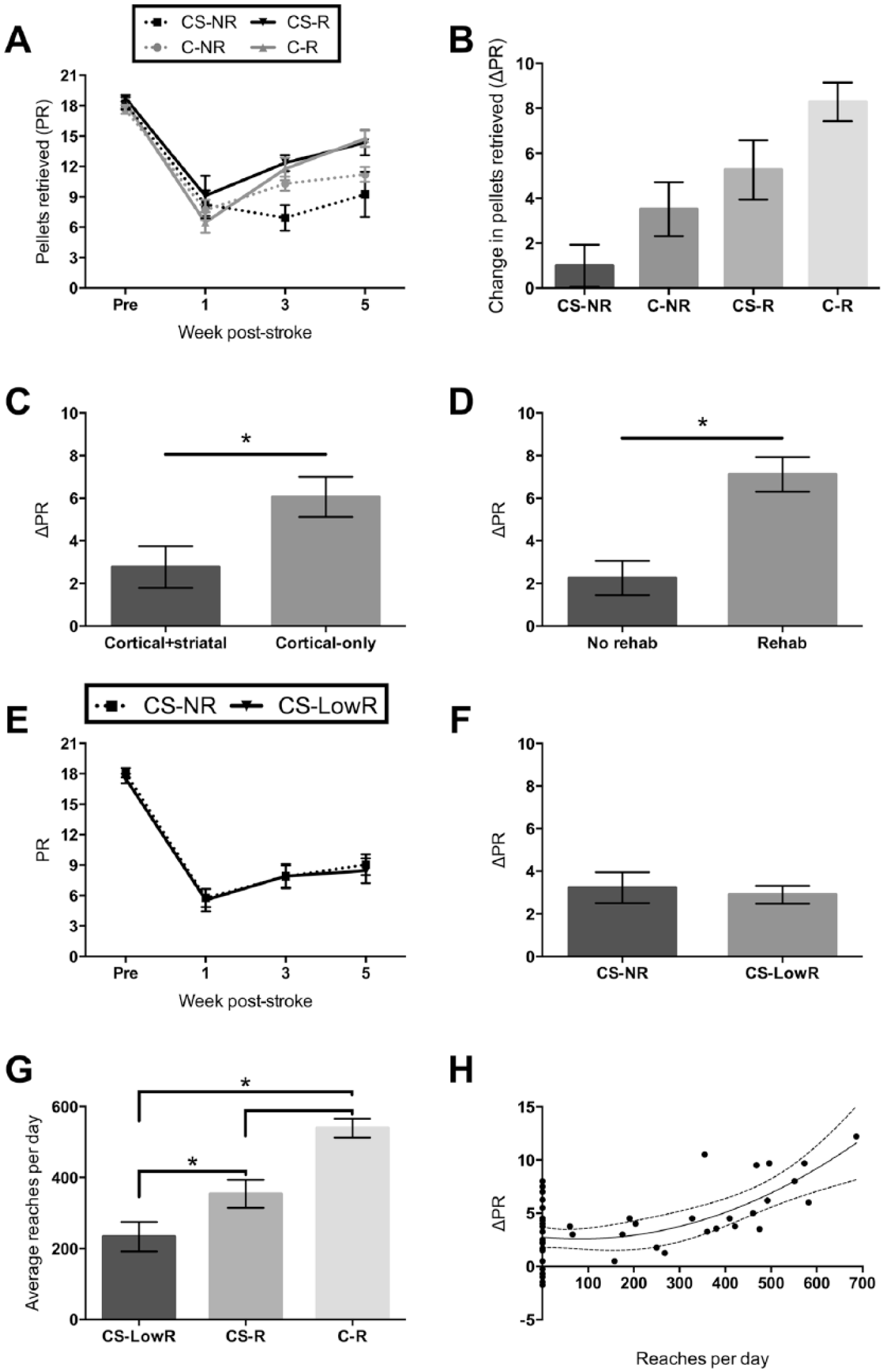
Prospective manipulation of infarct volume and rehabilitation intensity. (A, B) Pellet retrieval in the staircase task with cortical + striatal injury, no rehabilitation (CS-NR, n = 7); cortical-only injury, no rehabilitation (C-NR, n = 7); cortical + striatal injury, with rehabilitation (CS-R, n = 5); cortical-only injury, with rehabilitation (C-R, n = 8). All graphs show mean ± SEM. (C) Receiving smaller injury (F = 6.692, P = .016) and (D) rehabilitation (F = 6.320, P = .003) both result in improved recovery. (E, F) Rats that received lower intensity rehabilitation (CS-LowR, n = 10) did not significantly improve in performance relative to those that received no rehabilitation (n = 12). (G) Rats in voluntary access boxes completed fewer practice reaches per day in rehabilitation than those in closed boxes (F = 22.234, P < .001). (H) Repetitions per day in rehabilitation are nonlinearly related to recovery (Y = 0.00002466X2 − 0.004053X + 2.752, R2 = 0.3444, P < .0001, N = 49). A minimum threshold of rehabilitation intensity must be surpassed in order to realize the benefits of rehabilitation.
Next, we tested the influence of rehabilitation intensity on recovery. All rats received the large cortical-striatal injury (N = 22). Contrary to previous experiments where reaching practice was delivered in a closed reaching box, rats were provided with a voluntary-access reaching box. Rats reaching in the voluntary access box performed significantly fewer repetitions per day than rats exposed to closed-reaching boxes (F = 22.234, P < .001; Figure 3G). Consequently, this altered reaching paradigm resulted in rats not significantly improving relative to those that received no rehabilitation (Figure 3E, F). Combining data across experiments showed that mean reaches per day in rehabilitation nonlinearly predicted recovery across time (Y = 0.00002466X2 − 0.004053X + 2.752, R2 = 0.3444, P < .0001, N = 49; Figure 3H). Extra sum-of-squares F test confirmed this quadratic model to be a significantly better fit to the data than a linear model (F = 5.330, P = .0289). Intensity of rehabilitation (defined as daily number of practice reaches in rehabilitation) is therefore a necessary component of poststroke recovery. Furthermore, the quadratic relationship implies that a minimum threshold of rehabilitation exists in order to effectively “activate” recovery. 19 By generating a regression model from these prospective experiments we verified our previous findings that initial level of impairment, infarct volume, and rehabilitation intensity are important predictors of recovery (Supplementary Figure 1 and Table 4).
Prescribing Individualized Rehabilitation Intensity Using Biomarkers of Recovery
We used the predictive model from our retrospective dataset (Supplementary Table 2) to generate an equation capable of prescribing the minimum rehabilitation intensity necessary to achieve significant improvement in function in the staircase task (Table 1). Of the original 593 animals, 210 had received rehabilitation, with infarct volume data not available for 87 of these subjects. This meant that sufficient data were available from 123 rats for development of a prescriptive equation (ie, received rehabilitation with data regarding initial level of impairment, cortical infarct volume, and intensity of rehabilitation). Improvement by at least 2.2 pellets was chosen to test the performance of this equation. This value represented the upper limit of the 95% confidence interval of improvement for rats that did not receive rehabilitation. Therefore, recovery above this threshold represented a statistically significant increase in performance relative to what would spontaneously be achieved without rehabilitation. Our prescriptive equation had good performance on all parameters used clinically: sensitivity of 81%, specificity of 75%, positive predictive value of 81%, and negative predictive value of 75% (Table 1), which is similar to the accuracy of recently developed algorithms for predicting human clinical outcome after stroke. 26 The presently described algorithm represents a powerful tool for estimating the individualized minimum intensity of rehabilitation necessary to achieve significant functional recovery. Even rats with severe infarcts (up to 134.86 mm3) and initial impairments (zero pellets retrieved) were able to significantly recover if sufficient rehabilitation intensity was achieved. Nevertheless, our prescriptive equation revealed that in order to realize functional benefits in the most severe cases the required intensity of rehabilitation (ie, upwards of 600-700 repetitions per day), though clinically feasible, is outside of what is delivered in typical human rehabilitation paradigms (approximately 32).39,40
Equipped with a tool to estimate required rehabilitation intensity, we examined the relationship between prescription compliance and recovery in the classification of fitters, nonfitters, and decliners of the proportional recovery rule. We compared the clinical performance results from Table 1 to the proportional recovery clusters from our companion article. Intriguingly, rats that fit the proportional recovery rule always significantly improved regardless of whether they received the prescribed dose of rehabilitation (Figure 4A). Therefore, the intensity of rehabilitation may not be relevant for engaging recovery in rats that fit the proportional recovery rule. Decliners (~6% of sample) neither recovered nor did they ever achieve their prescribed dose of rehabilitation. Decliner rats may not have received sufficient rehabilitation intensity for a number of reasons, including possible task noncompliance or elevated anxiety during testing. The majority of nonfitters (~74%) were accurately classified by our rehabilitation prescription. Thirty percent of these rats achieved the required dose and recovered, while 44% did not meet their required dose of rehabilitation and did not recover. A small proportion of nonfitter rats (8%) recovered without meeting their prescribed dose of rehabilitation, while 18% did not recover despite achieving their prescription (Figure 4A).
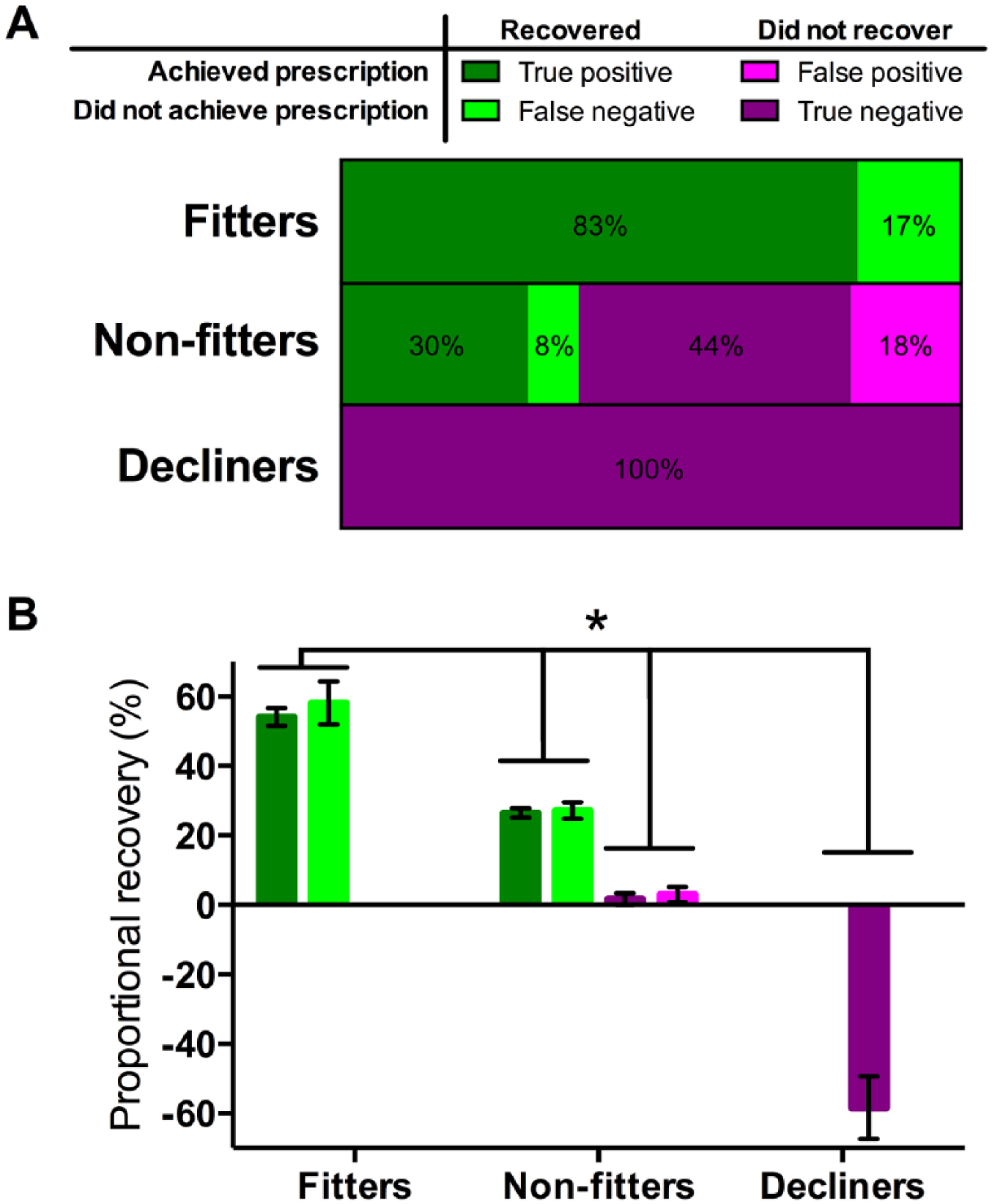
Accuracy of rehabilitation prescription for fitters, nonfitters, and decliners of the proportional recovery rule (see companion article). (A) Each bar represents the percentage of the fitter (n = 42), nonfitter (n = 73), and decliner groups (n = 8) that fell into each clinical classification. This is in respect to whether each animal achieved its prescription of rehabilitation intensity from Table 1, and also whether each animal showed significant recovery. Recovery was defined as a change in pellet retrieval of at least 2.2 pellets from their initial poststroke assessment to their terminal assessment point. (B) Rats that fit the proportional recovery rule always recovered regardless of whether they met their prescription. If nonfitters met their prescription they showed a lesser degree of proportional recovery, but if they did not meet their prescription they showed no proportional recovery at all. Decliners never met their rehabilitation intensity prescription and always deteriorated in function. All groups were significantly different (F = 234.810, P < .001) and are represented as mean proportional recovery, [ΔPRObserved/(PRPre-stroke − PRInitial)] ± SEM.
Of the subgroup of rats that had all of the required data for prescribing rehabilitation intensity (N = 123), those that were originally classified as fitters showed proportional recovery of 55 ± 15% (mean ± standard deviation). Nonfitters that recovered showed 27 ± 6% proportional recovery, while those that did not recover had a mean of 2 ± 9% proportional recovery. Decliners had a mean of −58 ± 9% proportional recovery. All of these groups were significantly different from one another (F = 234.810, P < .001; Figure 4B). We demonstrate that nonfitters of the proportional recovery rule are capable of recovery when sufficient rehabilitation intensity is achieved. However, the magnitude of this proportional recovery is smaller for nonfitters than for rats originally classified as fitters of the proportional recovery rule, regardless of whether or not the fitters achieved their prescribed intensity of rehabilitation (Supplementary Figure 3). We conclude that it is this population of nonfitters of the proportional recovery rule that benefitted the most from the intensive rehabilitation efforts in this study.
Discussion
In the present study, we identified distinguishing characteristics of fitters, nonfitters, and decliners of the proportional recovery rule to establish useful biomarkers for predicting stroke recovery. We validated the utility of these predictors in a series of experiments where we controlled for each factor and assessed the resulting impact on recovery. With this approach, we determined that initial level of impairment, infarct volume, and intensity of rehabilitation are important predictors of functional recovery for rats. Individually, these factors have also been previously identified as predictors of human recovery.4,6,17,41,42 However, the present study is the first to combine all 3 factors into a single, comprehensive predictive model. Importantly, our refined model indicated that rehabilitation was essential for promoting poststroke recovery, which has been seriously questioned since the discovery of proportional recovery principles.1,14 Whether this enhanced recovery was because of impairment resolution, or development of beneficial compensatory movement strategies is unclear. This is an avenue for further investigation in both preclinical and clinical research. Although human studies have not shown an impact of rehabilitation on proportional recovery of impairment resolution, benefits of rehabilitation may be apparent in enhancing development of compensatory strategies.
Using our novel predictive model of recovery, we generated an algorithm to prescribe a recommended intensity of reach training as a component of rehabilitation. This prescription is based on the desired level of recovery, initial level of impairment, and cortical infarct volume, representing the individualized intensity at which rehabilitation is predicted to become effective for a given rat. This algorithm has good clinical performance, accurately predicting recovery in the majority of rats (~75% to 80%), which is similar in accuracy to recently developed human predictive models (~80%). 26 Interestingly, rats that showed proportional recovery always recovered, regardless of whether they met their prescription; decliners never met their prescription and subsequently never recovered. Nonfitters of the original proportional recovery rule were the population with the greatest need of intensive rehabilitation. Indeed, a form of proportional recovery was possible in nonfitters if sufficient intensity of rehabilitation was achieved. However, the magnitude of this proportional recovery was smaller than that achieved by rats originally classified as fitters of the proportional recovery rule. The possibility of such an interaction between training and proportional recovery has been discussed in the literature, but had not been systematically tested prior to the present study. 41 Nonfitters that underperformed in rehabilitation did not recover. These findings in our rat model suggest that quantitative measures such as initial impairment and lesion volume may be useful for tailoring individualized rehabilitation programs for human patients. Implementation of this concept into clinical decision-making has the potential to increase therapist confidence, reduce inpatient length of stay, and amount to significant cost savings for chronic stroke care. 26
Before the presently described model of rehabilitation prescription can be applied clinically, a greater understanding of the magnitude of rehabilitation effects in human poststroke recovery needs to be developed. However, this is a challenging process, since clinical trials typically employ “usual care” as the control group when testing the efficacy of novel treatments, meaning that a pure estimate of the magnitude of the benefits of rehabilitation is missing in the human literature. Nonetheless, this fundamental lack of understanding of the benefits of rehabilitation has been acknowledged, leading to important new efforts to uncover the relative weight that rehabilitation has on final outcome of stroke recovery.13,17,42 In the present study, we were able to include nonrehabilitated animals (not ethically possible in humans) in our modeling, giving us a direct estimate of the magnitude of the benefits of our rehabilitation paradigm. This allowed us to demonstrate that some aspects of the recovery process (ie, proportional recovery) may generalize between humans and rats.
One caveat to this conclusion is that the task-specific performance measured by the staircase task is dissimilar from the neurological impairment measured by the Fugl-Meyer task in human studies of proportional recovery. 43 Recovery of pellet retrieval in the staircase can be achieved using compensatory body positioning, true resolution of impaired kinematics, or a combination of the two. This could be especially important in relation to our finding that even nonfitters of the original proportional rule can show a lesser degree of recovery if sufficient intensity of rehabilitation is received. It is possible that fitters and nonfitters may have achieved recovery through different mechanisms (impairment resolution vs compensatory strategies). However, the ability to perform activities via either impairment resolution or more effective compensation are both relevant to the quality of life of stroke survivors. Future studies could disentangle recovery mechanisms in fitters and nonfitters using kinematic analysis, which can be employed in both rats 44 and humans.45,46 This approach may also provide valuable information on the efficacy of rehabilitative treatments, and their contribution to either impairment resolution, or adoption of beneficial compensatory strategies. It is very encouraging that even without the superior specificity of the Fugl-Meyer task we were still able to observe the same degree of proportional recovery between rats and humans. Given that human proportional recovery has been shown to generalize to a variety of impairment types,10-12 it is possible that rat proportional recovery may be similarly robust across impairment domains.
Conclusion
Recent studies have led to the suggestion that rehabilitation may have limited efficacy in improving human poststroke recovery. The present study demonstrates that rehabilitation is crucial for predicting stroke recovery in rats. It is imperative that rehabilitation paradigms are sufficiently intense and enriching in order to provide benefits beyond those that would occur spontaneously. Consequently, we have established an algorithm to determine the individualized daily dose of rehabilitation necessary for a rat to achieve significant improvements in motor performance. This equation is solely dependent on knowledge of a subject’s initial poststroke level of impairment and cortical infarct volume. Further development of this individualized approach to treatment could represent the next major breakthrough in stroke recovery research and similar algorithms need to be pursued for the clinical setting.23-26 However, before this can occur, evidence that conventional human stroke rehabilitation practices exert a dose-dependent effect on recovery must be produced. Without a clear demonstration that current rehabilitation strategies actually improve recovery beyond that which would occur spontaneously, and the ability to calculate the magnitude of these effects in a dose-dependent manner, efforts to optimize and individualize stroke care, as we have done in rats in the present study, will not be possible.
Footnotes
Authors’ Note
The data that support the findings of this study are available from the corresponding author on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Partnership for Stroke Recovery, Canadian Institutes for Health Research (CIHR), Natural Sciences and Engineering Research Council of Canada (NSERC), Heart & Stroke Foundation of Canada and Canada Research Chairs program provided funding to DC for the studies that comprise this research. SK received fellowships from CIHR and the Ontario Graduate Scholarship (OGS) program. JA and AF received Research in Science and Engineering (RISE) Worldwide Program awards from the German Academic Exchange Service (DAAD).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.