
Abstract
Background. Perinatal stroke causes most hemiparetic cerebral palsy. Ipsilateral connections from nonlesioned hemisphere to affected hand are common. The nonlesioned primary motor cortex (M1) determines function and is a potential therapeutic target but its neurophysiology is poorly understood. Objective. We aimed to characterize the neurophysiological properties of the nonlesioned M1 in children with perinatal stroke and their relationship to clinical function. Methods. Fifty-two participants with hemiparetic cerebral palsy and magnetic resonance imaging–confirmed perinatal stroke and 40 controls aged 8 to 18 years completed the same transcranial magnetic stimulation (TMS) protocol. Single-pulse TMS to nonlesioned M1 determined rest and active motor thresholds (RMT/AMT), motor-evoked potential (MEP) latencies, and stimulus recruitment curves (SRC: 100%-150% RMT). Paired-pulse TMS evaluated short-latency intracortical inhibition (SICI) and intracortical facilitation (ICF). Ipsilateral (IP) participants (ipsilateral MEP ≥0.05 mV in ≥5/20 trials) were compared with contralateral MEP only, nonipsilateral (NI) participants. Assisting Hand and Melbourne assessments quantified clinical function. Results. Twenty-five IP were compared with 13 NI (n = 38, median age 12 years, 66% male). IP had lower motor function. SRC to unaffected hand were comparable between IP and NI while IP had smaller ipsilateral SRC. Ipsilateral MEP latencies were prolonged (23.5 ± 1.8 vs 22.2 ± 1.5 ms contra, P < .001). Contralateral SICI was different between IP (−42%) and NI (−20%). Ipsilateral SICI was reduced (−20%). Contralateral ICF was comparable between groups (+43%) and ipsilaterally (+43%). Measures correlated between contralateral and ipsilateral sides. Conclusion. Neurophysiology of nonlesioned M1 and its relationship to motor function is measureable in children with perinatal stroke. Correlation of excitability and intracortical circuitry measures between contralateral and ipsilateral sides suggests common control mechanisms.
Introduction
Perinatal stroke is a focal vascular brain injury between 20 weeks gestation and the 28th postnatal day. 1 Survivors suffer lifelong physical disability and most hemiparetic cerebral palsy is due to perinatal stroke. 2 An incidence of at least 1:2500 live births suggests that more than 75 000 North American children and families are living with consequences of perinatal stroke.3,4 Disabling motor deficits of stroke-induced hemiparetic cerebral palsy are present in more than 80% of cases5,6 and current therapeutic options are limited. Such a focal injury early in life in an otherwise healthy brain represents an ideal model of human developmental motor plasticity. 7
Combining animal studies with advanced imaging and neurophysiology studies in humans have defined models of motor system organization following early focal injury.8-10 Bilateral corticospinal projections from primary motor cortex of equal strength are demonstrable at birth using transcranial magnetic stimulation (TMS). 8 During normal early development, the vast majority of ipsilateral connections are withdrawn, resulting in motor control by the contralateral motor cortex. An early unilateral injury to the motor system alters this developmental progression, often leading to abnormal preservation of ipsilateral connections between the contralesional hemisphere and the affected limb.11-16 Relative success in competing for synapses with spinal lower motor neuron pools between contralateral and ipsilateral corticospinal projections may determine corticomotor control of the affected limb. 17 Hemiparetic children may then have relative degrees of ipsilateral connections, the extent of which has been associated with poorer motor function. 18 However, how the cortical neurophysiology of the contralesional motor cortex differs in relation to this corticospinal tract arrangement is poorly understood.
Ipsilateral projections may also dictate different elements of motor control. For example, the minor ipsilateral control found in normal subjects predominantly affects proximal muscles while in early acquired brain injury, they may preferentially control distal muscles. 17 Mirror movements (synchronized mimicry of the opposite hand during unimanual movements) provide a clinical correlate of such organization though how they reflect contralesional cortical neurophysiology is not well understood.12,13,16,19 Studies to date have also been limited by heterogenous etiologies, older populations, and modest sample sizes. The role of the contralesional motor cortex is therefore of essential importance in understanding developmental plastic reorganization following perinatal stroke.
Comparable approaches in adult stroke have advanced models with translation into clinical trials of novel therapeutic intervention.9,20 Controlled trials of noninvasive brain stimulation, including repetitive TMS (rTMS) and transcranial direct current stimulation (tDCS) can enhance motor outcomes in hemiparetic adult stroke participants, where the contralesional motor cortex is astimulation target.21-23 Recent trials have shown that neuromodulation of the contralesional motor cortex can enhance motor function in hemiparetic children.24,25
Understanding the neurophysiology of the contralesional primary motor cortex (M1) is paramount to advancing such therapeutic approaches, including optimizing targets and individualizing interventions. We performed a large, population-based, case-control study of school-aged children with perinatal stroke, applying a systematic TMS protocol to elucidate the cortical neurophysiology of the contralesional motor cortex and its relationship to clinical function.
Methods
Participants
Participants were recruited through the Alberta Perinatal Stroke Project (APSP), a population-based research cohort from southern Alberta, Canada. Inclusion criteria were (1) symptomatic hemiparetic cerebral palsy, including Pediatric Stroke Outcome Measure 26 >0.5 and Manual Ability Classification System27,28 (MACS) I-IV and both parent and child perceived functional limitations; (2) magnetic resonance imaging–confirmed perinatal arterial ischemic stroke in the middle cerebral artery (AIS-MCA) or unilateral periventricular venous infarction confirmed by 2 blinded investigators according to validated criteria 29 ; (3) age 6 to 19 years; (4) developmental maturity consistent with participation; and (5) informed consent/assent. Participants with any of the following were excluded: (1) multifocal stroke and/or other brain injury/abnormality, (2) severe hemiparesis (MACS level V), (3) severe developmental delay or inability to comply with study protocol, (4) unstable epilepsy, (5) any TMS contraindications, 30 or (6) botulinium toxin, orthopedic surgery, or other invasive therapy within the previous 6 months.
Typically developing control participants were recruited from our healthy controls research program (www.hiccupkids.ca). Children of comparable age and gender without neuropsychiatric disease or medication underwent identical procedures. Experiments were carried out with the approval of the Research Ethics Board at the University of Calgary and informed consent/assent of the participants and their guardians. Experiments were conducted at the Alberta Children’s Hospital Pediatric Non-Invasive Brain Stimulation Laboratory.
Neurophysiology Measures
Participants were brought to the laboratory with a caregiver and oriented to the procedures. Participants were seated comfortably in a chair and allowed to watch a movie of their choice during times not requiring cooperation. A pair of Ag-AgCl electrodes (Kendall; Chicopee, MA, USA, 1.5-cm radius) were used to record surface electromyogram (EMG) from first dorsal interosseous (FDI) muscles of both hands with a wrist ground band . EMG signals were amplified by 1000 and band-pass filtered from 20 to 2000 Hz and then digitized at a rate of 5000 Hz using CED 1401 hardware and Signal 6.0 software (Cambridge Electronic Design, Cambridge, UK).
Single-Pulse TMS: Motor Thresholds and Excitability
To assess corticospinal tract properties, we measured motor-evoked potentials (MEPs) in the FDI muscle with single-pulse TMS. A figure-of-eight coil (70 mm) connected to a Magstim Bistim2 stimulator (Magstim; Dyfed, UK) induced posterior-anterior currents in the contralesional motor cortex while recording FDI bilaterally. The location over M1 that produced the largest contralateral MEP (ie, hotspot) was mapped using mildly suprathreshold intensities. This hotspot for the unaffected hand was used for all subsequent stimulations. This location was landmarked for consistent coil placement and orientation on a 3-dimensional anatomical T1 MRI using neuronavigation(Brainsight 2, Rogue Research, Montreal, CA).
FDI maximum voluntary contraction (MVC) was determined by asking the participant to squeeze a stress ball as hard as they could. The full-wave EMG was rectified and smoothed (100ms time constant, Neurolog NL703EMG Integrator, Digitimer UK) using an oscilloscope (GDS-1022, GwINSTEK, Taiwan). For all active trials, the visual targets for contraction levels were set to 20% MVC with continual biofeedback and rest breaks as needed.
Rest motor threshold (RMT) was determined according to published standards as the minimum stimulator intensity (percentage of the maximum stimulator output, MSO) required to elicit >50μV FDI MEP in 5/10 consecutive trials. Similarly, active motor threshold (AMT) was the minimum intensity required to elicit >200 μV FDI MEP in 5/10 consecutive trials during 20% MVC. Participants with thresholds greater than maximum tolerated or 100% stimulator output were documented but excluded from further analysis.
To produce resting stimulus response curves (SRC), TMS intensities were delivered at 10% increments from 100% to 150% of RMT. Ten TMS stimuli were delivered at each intensity in random order. To produce active SRC, intensities were increased from 100% to 150% of AMT with the participant maintaining active contraction at 20% MVC.
Generated MEP signal files were imported into MATLAB R2011b (Mathworks, Inc, Natick MA) for offline analysis. Each tracing was visually inspected for artifacts such as baseline motor activity during rest protocols with erroneous tracings removed. A custom MATLAB script calculated peak-to-peak MEP values from un-rectified EMG by setting a time window of 15 to 80 ms from the TMS pulse.
Corticospinal tract arrangement: Ipsilateral status. Previous adult and pediatric TMS studies investigating ipsilateral pathways have not defined specific criteria so methods were developed to objectively quantify individual ipsilateral status. Interparticipant MEP variability is high and occasional ipsilateral MEP may be obtained in normal adults31-33 and children.34,35 Therefore, detection of any ipsilateral response was considered nonspecific. To objectively quantify significant ipsilateral responses, 20 TMS stimulations of nonlesioned M1 at 120% RMT were examined for ipsilateral MEP. Participants with ≥5/20 ipsilateral MEP >50 μV in amplitude were classified as ipsilateral (IP) while those without were considered nonipsilateral (NI).
Stimulus response curves (SRCs). Peak-to-peak amplitudes of 10 MEP were averaged at each stimulus intensity to produce individualized input/output curves. The SRC was also quantified by calculating the area under the curve (AUC) generated. This generated a single variable quantifying net effects of increasing stimulation strength on cortical excitability.
MEP latency. Latencies were calculated as the average time from the TMS artifact (t = 0 ms) to MEP onset at 120% RMT. MEPs were recorded at rest. Average MEP latency was calculated from 20 MEPs at 120% RMT. A MATLAB script identified MEP onset as the time point when the EMG exceeded 3 standard deviations from mean background EMG.
Paired-Pulse TMS: Intracortical Inhibition and Facilitation
Paired-pulse TMS used 2 stimulators (Bistim2 and 2002 Magstim, UK) connected by an adaptor. Paired pulses were delivered with interstimulus intervals (ISI) between an initial conditioning stimulus (CS) and subsequent test stimulus (TS). Protocols evaluated short-interval intracortical inhibition (SICI) and intracortical facilitation (ICF) in accordance with published evidence.36,37 Rest paradigms consisted of 120% RMT TS preceded by 90% AMT CS 38 at ISI of 2 ms (SICI) and 10 ms (ICF). 36 For active SICI and ICF, CS were adjusted to 70% AMT. 31 Ten unconditioned (test only) and 20 conditioned (10 at each ISI) stimulations were applied in random order. The average amplitude of the 10 conditioned MEP at both 2- and 10-ms ISIs were expressed as percentage of the average of the 10 unconditioned test MEP (<100% indicating inhibition, >100% indicating facilitation).
Intrahemispheric correlations
With both the affected and unaffected limbs controlled by the contralesional hemisphere in IP participants, correlations between each of the TMS neurophysiological parameters were sought between the 2 sides.
Clinical Outcome Measures
Motor outcomes were obtained in standardized fashion by certified pediatric occupational therapists. Assessments were completed in the same quiet environment and videotaped for validation. Motor outcomes were
Assisting Hand Assessment (AHA). The AHA is a series of bimanual, multifaceted tasks to evaluate affected hand function during bimanual performace in children with an impaired unilateral upper limb. The AHA carries the best evidence of interrater and intrarater reliability, test validity, and response sensitivity to detect change in upper extremity function in children with hemiparetic cerebral palsy. 33 Scores are expressed in AHA logit units (maximum 100).
Melbourne Assessment of Unilateral Upper Limb Function (MA). The MA is a validated measure of unilateral function in the affected extremity that considers motor function in the context of cognitive, sensory, and perceptual considerations.34-36 Scores are expressed as a percentage (maximum 100%).
Box and Block Test (BBT). This standardized, validated unimanual hand function test measures the speed of lifting, carrying and releasing blocks in a 1-minute period. 37 It affords uncapped quantification of motor function in both the affected and unaffected upper extremities. Scores are the number of blocks moved in 60 seconds.
Safety and tolerability. A standardized measure of safety and tolerability in pediatric TMS 38 was applied on days 1 and 10. This captured and quantified any adverse effects and ranked the experience relative to common childhood experiences.
Statistical Analysis
Analyses were performed using SigmaPlot (version 13.0) software. Following confirmation of a normal distribution, differences in age, AHA and MA scores between the IP and NI groups were examined with independent t tests. To compare IP, NI, and control SRC, SICI, ICF, and MEP latency between IP, NI, and controls, a 1-way analysis of variance (ANOVA) was used with post hoc t tests (Bonferroni corrected). To compare MEP amplitudes across the different TMS intensities in the SRC, a repeated measures ANOVA was used with post hoc paired t tests (Bonferroni-corrected). To compare contralateral and ipsilateral SICI, ICF, and SRC AUC within the IP group, paired t tests were used. Associations between contralateral and ipsilateral physiology, as well as between neurophysiological and clinical measures were assessed using Pearson and Spearman’s rank correlation coefficients where appropriate.
Results
Participants
Fifty-two participants potentially meeting criteria were identified and their neurophysiology data was screened. Thirty-eight had measureable MEP thresholds with 1.2 RMT being <100% of maximum stimulator output that allowed completion of the complete protocol. This final study population had a median age of 12 ± 3 years (range: 6-18 years) and was 65% male. Clinical outcome data was complete for all cases. The typically developing control population consisted of 40 participants (mean age 15 ± 3years, range 8-18 years; 48% male). Ages were comparable across the IP, NI, and control groups (all P > .2) while the average age of those excluded for unobtainable MEP or high thresholds was lower (P < .001). The study populations are summarized in Table 1. There were no serious adverse events and no dropouts. Headache associated with TMS was more common in stroke subjects (40%) compared with controls (13%) but decreased across sessions and was always mild and self-limiting. All other subjective effects were described in <3% of sessions. Average tolerability scores were rated as similar to a long car ride.
Demographic Characteristics, Stroke Information, and Clinical Measures. a
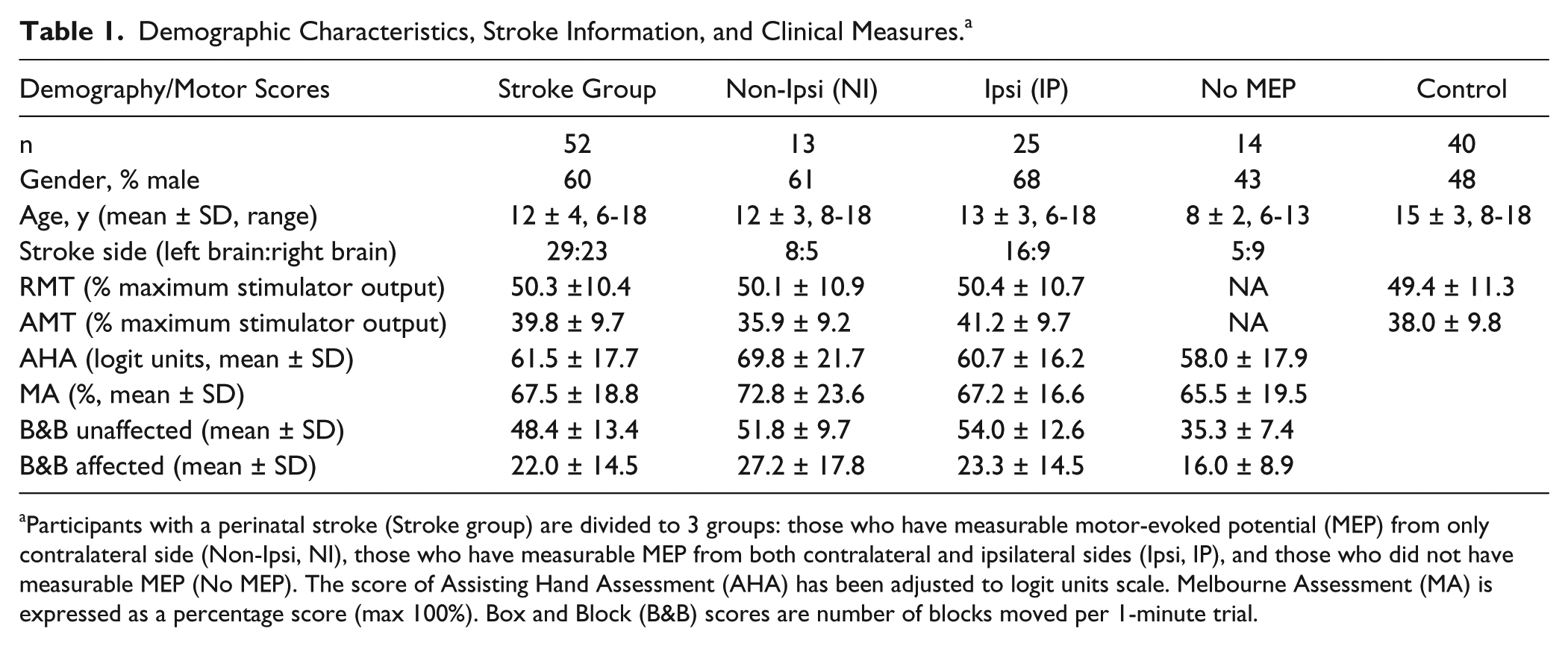
Participants with a perinatal stroke (Stroke group) are divided to 3 groups: those who have measurable motor-evoked potential (MEP) from only contralateral side (Non-Ipsi, NI), those who have measurable MEP from both contralateral and ipsilateral sides (Ipsi, IP), and those who did not have measurable MEP (No MEP). The score of Assisting Hand Assessment (AHA) has been adjusted to logit units scale. Melbourne Assessment (MA) is expressed as a percentage score (max 100%). Box and Block (B&B) scores are number of blocks moved per 1-minute trial.
Single-Pulse Neurophysiology
Corticospinal Tract Arrangement
Single pulse TMS defined corticospinal tract (CST) arrangement in all participants with obtainable responses (Figure 1). Using the ipsilateral criteria, 25 of 38 (66%) had significant bilateral MEP with stimulation of the contralesional motor cortex and were classified as IP. The remaining 13 (34%) had only contralateral MEP and were classified NI. Bilateral outcomes are therefore reported in IP participants (labeled as “contra IP” for unaffected hand and “ipsi IP” for affected hand) while NI participants only have contralateral, unaffected hand responses (contra NI).
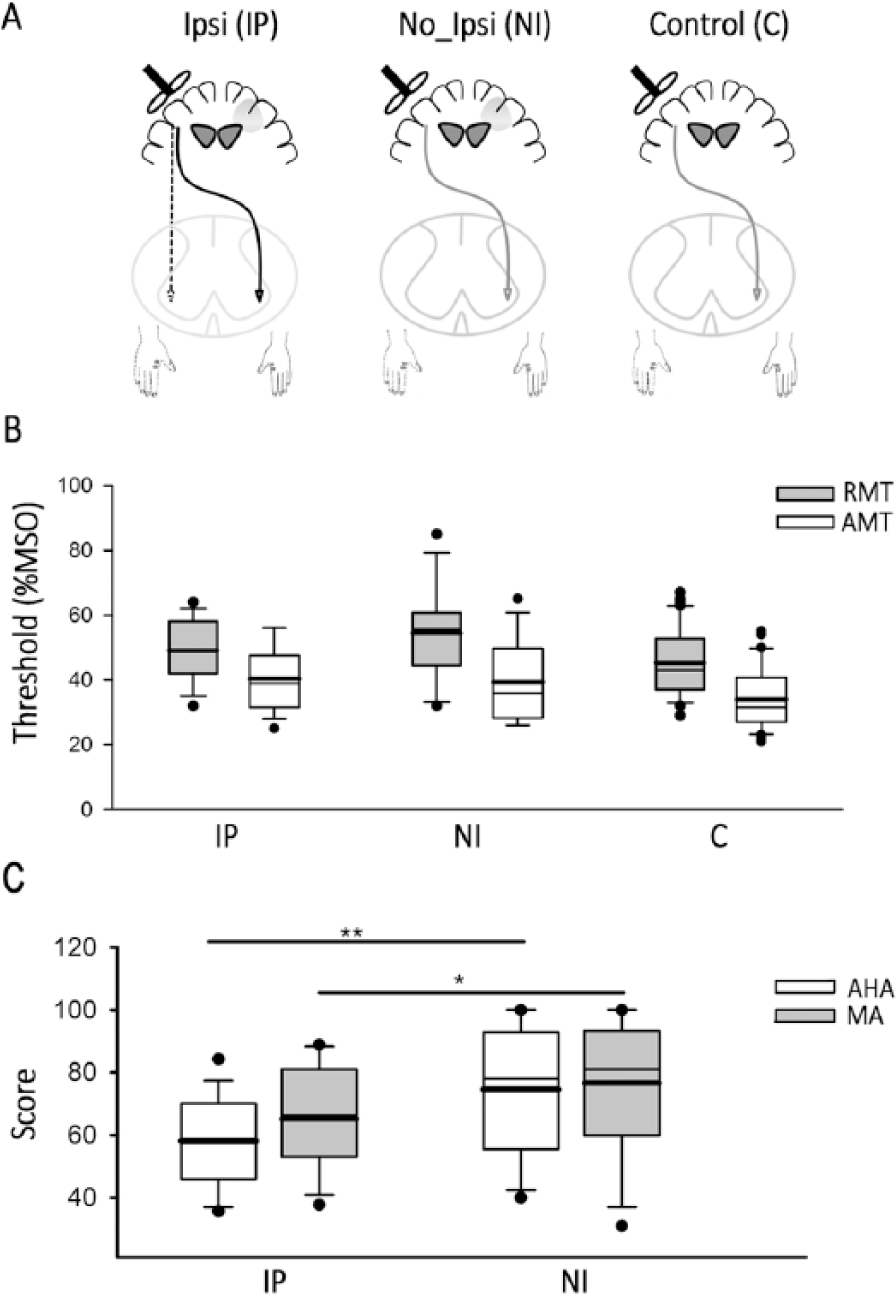
Classification of participants. (A) Sketch of motor organization of participants with left perinatal stroke who present with ipsilateral response (IP), contralateral responses only (NI), and participants who are neurologically intact (C). (B) Comparison of resting (RMT) and active (AMT) motor thresholds between IP, NI, and C groups. (C) Comparison of Assisting Hand Assessment (AHA) and Melbourne Assessment (MA) between IP and NI groups. The median and mean of the data are shown by the thinner and thicker horizontal lines, repectively, on the box plots. *P < .05 and **P < .01.
Motor Thresholds
Both RMT and AMT were elicited from the nonlesioned M1 and recorded from the unaffected FDI. As shown in Figure 1B, mean RMT and AMT were comparable across groups, with AMT being lower than RMT in all cases. There was no difference between the RMT of controls and either the IP or NI stroke participants, F(2, 58) = 1.07, P = .35. The nonlesioned AMT was also not different across the 3 groups, F(2, 58) = 1.23, P = .66. Those participants excluded due to limited measurements included 7 participants with RMT greater than 83% of maximum stimulator output (preventing suprathreshold 120% stimulation) and another 7 participants with no attainable MEP at maximum stimulation intensity (100% of maximum stimulator output).
Clinical motor function was associated with corticospinal arrangement. Mean AHA and MA scores for IP participants were lower as compared with NI participants (Figure 1C, P < .01 and P = .04, respectively). Comparable differences were seen when stroke participants were divided into arterial and periventricular venous infarction subgroups.
Stimulus-Response Curves and MEP Latency
SRCs were obtained from all IP and NI stroke participants. Representative examples of rest and active SRC tracings are shown in Figure 2. TMS of the nonlesioned motor cortex resulted in bilateral MEP in IP participants. The morphology and the responsiveness to the increase in TMS intensities were similar between the ipsilateral and contralateral MEP responses (Figure 2A). In NI participants (Figure 2B), TMS of the nonlesioned motor cortex resulted in only contralateral MEP, which were similar in shape and size to the contralateral responses of the group IP participants. Single pulse TMS also afforded a comparison between the onset latency of ipsilateral and contralateral MEP within IP participants and across groups to explore differences in pathway timing (Figure 2C and D). As shown by a representative example in Figure 2C, the onset latency of ipsilateral MEP was delayed compared with the contralateral MEP. The latency of ipsilateral MEP was an average of 1.3 ± 0.5 ms (longer than contralateral MEP; Figure 2D, P < .001). The intraparticipant comparision showed that the latency of ipsilateral MEPs were longer than contralateral MEPs within the same individual in all but one IP participant. The latency of ipsilateral responses was also longer than those of NI contralateral MEP (P = .01) and controls contralateral MEP (P < .001). There was a trend toward longer latencies of contralateral responses from IP and NI compared with controls contralateral MEP, F(2, 44) = 3.1, P = .06.
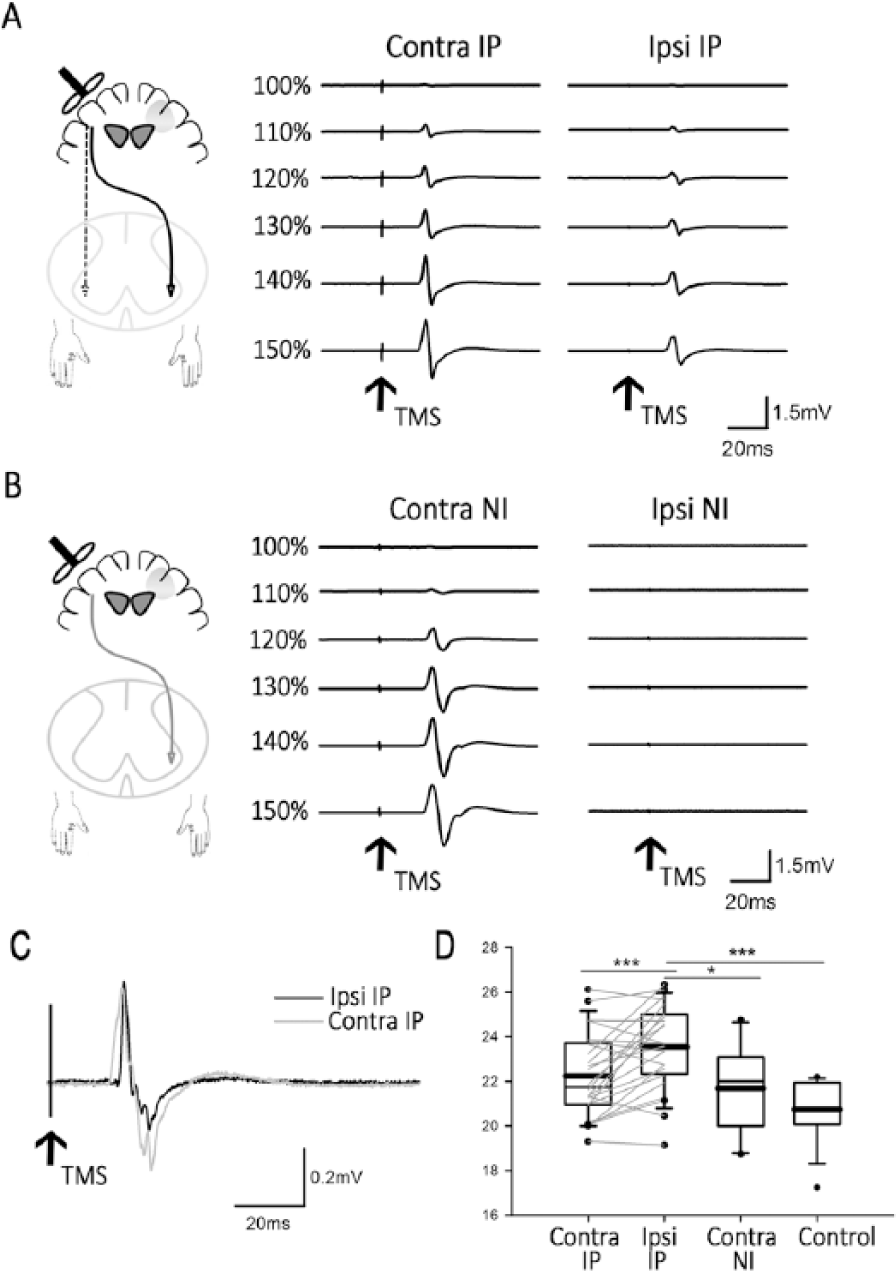
Motor-evoked potential (MEP) traces and MEP latency. (A) Average of 10 first dorsal interosseous (FDI) MEP evoked from incrementing intensities of transcranial magnetic stimulation (TMS) of nonlesioned motor cortex of (A) group IP (ipsilateral) participants, and (B) group NI (nonipsilateral) participants. Left panel: Contralateral MEP. Right panel: Ipsilateral responses. (B) Average of 10 FDI MEP evoked from incrementing intensities of TMS of non-lesioned motor cortex of (A) group IP participants and (B) group NI participants. Left panel: Contralateral MEP. Right panel: Ipsilateral responses. (C) Example contralateral and ipsilateral MEP traces from a single IP participant. (D) Average latency of contra- and ipsilateral MEP from IP participants individual changes shown by light gray lines, and contralateral MEP from NI and control participants. *P < .05 and ***P < .001.
Across all groups, responses to increased stimulation intensities demonstrated a sigmoid-shaped curve(Figure 3). SRC recorded at rest was similar between the contralateral responses from IP, NI, and control groups. However, distinct ipsilateral SRC in IP participants were significantly lower across all intensities (Figure 3A), F(1, 2) = 13.2, P < .001. The AUC in ipsilateral SRC was lower than contralateral SRC in the same participants, as well as NI participants and controls (Figure 3B, P < .001).
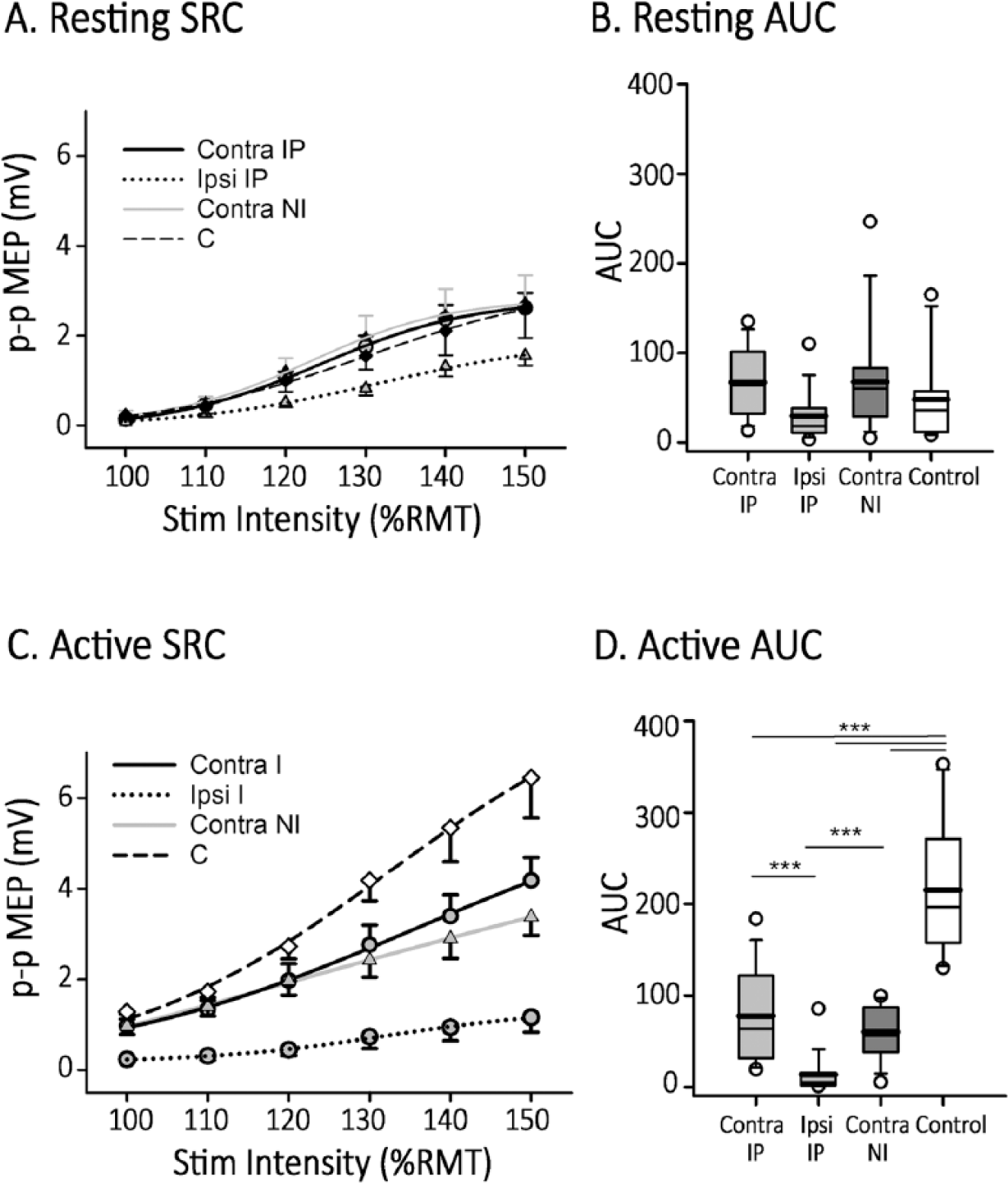
Stimulus response curves (SRC). (A) Contralateral transcranial magnetic stimulation (TMS) response curves from first dorsal interosseous (FDI) muscles of ipsilateral (IP; solid black line), nonipsilateral (NI; solid gray line), and control (dotted black line) participants, and ipsilateral SRC from IP participants (dashed black line). Each trace represents the average response of 10 stimuli at each stimulus intensity. (B) The area under the SRC curve from IP participants (light gray boxes) and the area under contralateral SRC from NI (dark gray box) and control (white box) participants. (C) Same format as in A, but SRCs were done during active FDI contraction. (D) Same format as in B, but the area of the SRCs that were done during active FDI contraction. *P < .05 and ***P < .001.
In contrast, when the SRC protocol was repeated with FDI actively contracting at 20% MVC, the SRC values and area under the curve were less than controls for all stroke participants (Figure 3D, all Ps <.001) given similar level of background EMG activity (all Ps >.11). The contralateral SRC was not different between IP and NI groups (P = .6). The ipsilateral SRC of IP participants was again significantly lower than the contralateral SRC compared to both the same participants and the NI group, F(1, 5) = 3.6, P = .03.
Paired-Pulse TMS: Intracortical Inhibition and Facilitation
For all participants, paired-pulse data was obtained from the nonlesioned motor cortex. As shown by representative tracings from both IP and NI participants (Figure 4A), test MEPs were generally inhibited by subthreshold conditioning stimuli at 2-ms ISI (SICI) and facilitated at 10-ms ISI (ICF). The inhibition and facilitation patterns and morphology of the conditioned MEP was similar between the contralateral and ipsilateral responses within the IP group. At rest, mean conditioned MEP at 2-ms ISI were significantly less than 100% for all groups (all Ps <.03, Figure 4B), suggesting SICI effects. ICF effects were present but less robust. At 10-ms ISI the conditioned MEP from the contra response of IP participants (P = .02) and controls (P < .001) were significantly greater than 100%. In contrast, there were no significant (all Ps >.3) SICI or ICF effects seen in any groups when the paired-pulse experiments were conducted during active contraction at 20% MVC (Figure 4C).
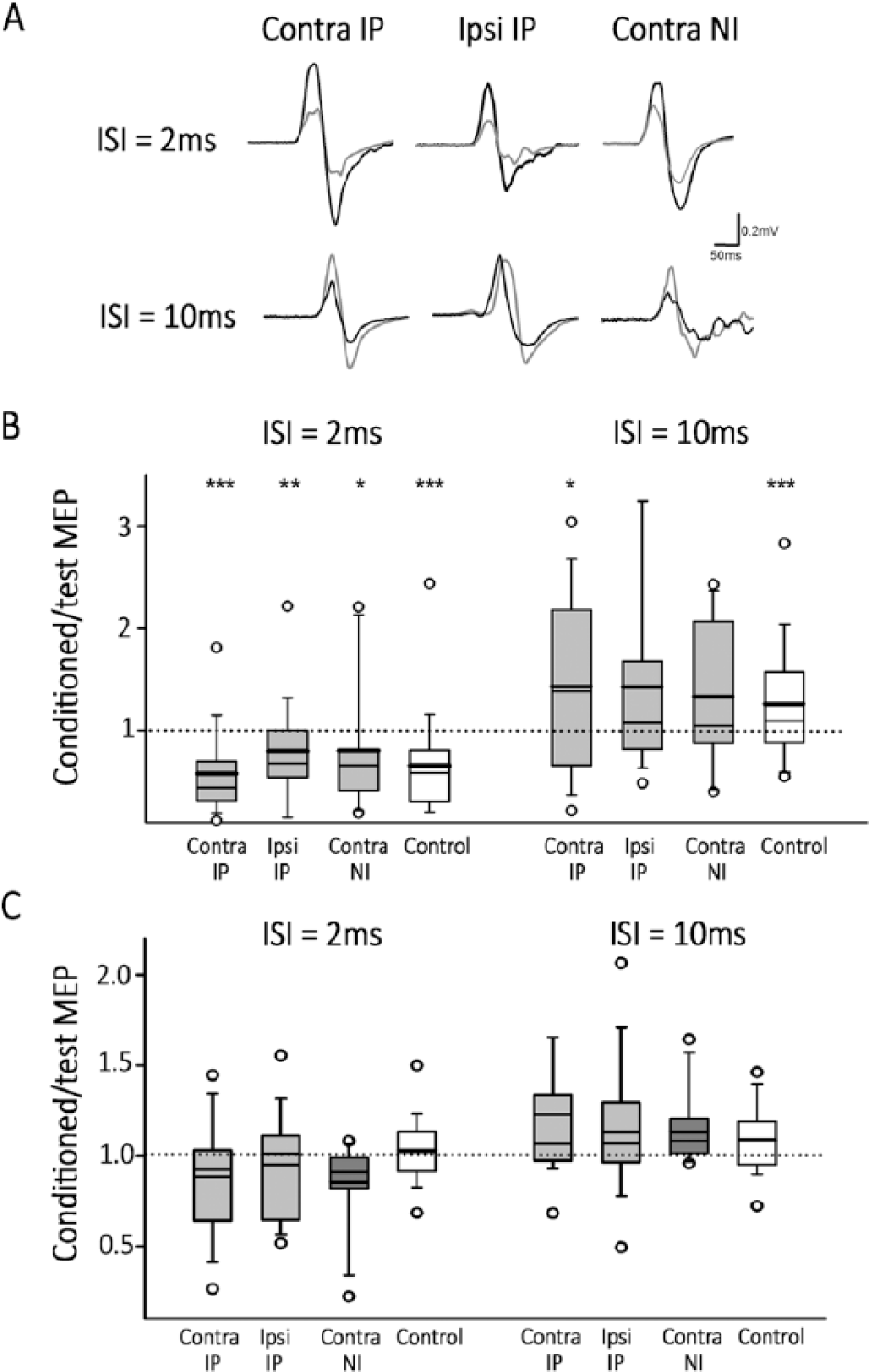
Intracortical inhibition and facilitation. (A) Average of 10 test-alone motor-evoked potential (MEP) (black trace) and 10 subthreshold transcranial magnetic stimulation (TMS) conditioned MEP (gray trace) at 2-ms interstimulus intervals (ISI; top graphs) and 10-ms ISI (bottom graphs) in a single participant from each of ipsilateral (IP) and nonipsilateral (NI) groups. (B) Ratio between average of conditioned and test-alone MEP, across all IP, NI, and control participants at 2-ms ISIs (left panel) and 10-ms (right panel) ISIs. (C) Same format as in B but during active condition. *P < .05, **P < .01, and ***P < .001.
Group analysis demonstrated comparable contralateral SICI between IP and controls (Figure 4B, P = .1) with effects of −42%, and −30% compared to test stimuli, respectively. SICI was present but reduced both contralaterally in NI participants and ipsilaterally in IP participants (−20% for both, P = .03 and P = .002, respectively). In IP participants, contralateral ICF was comparable (+43%, P = .06) and similar ipsilaterally (+43%, P = .07). When the above SICI and ICF protocols were repeated during active FDI contraction at 20%MVC, SICI and ICF effects were reduced. Neither controls nor stroke participants demonstrated significant differences from neutral (100% test response) (Figure 4C, all Ps >.2).
Correlations Between Ipsilateral and Contralateral Responses
Neurophysiological properties of contralateral and ipsilateral responses in IP participants demonstrated consistent correlations. Bivariate analysis demonstrated an association between contralateral and ipsilateral AUC in both rest (not shown, r = 0.7, P < .001) and active states (Figure 5A active: r = 0.5, P = .03). Paired-pulse measures of intracortical systems were also associated, including active SICI (Figure 5B; active: r = 0.6, P = .002) and active ICF (Figure 5C active: r = 0.7, P = .03) and resting ICF (not shown, resting: r = 0.6, P < .001). No correlation was seen between ipsilateral and contralateral resting SICI (not shown, r = 0.2, P = .2).
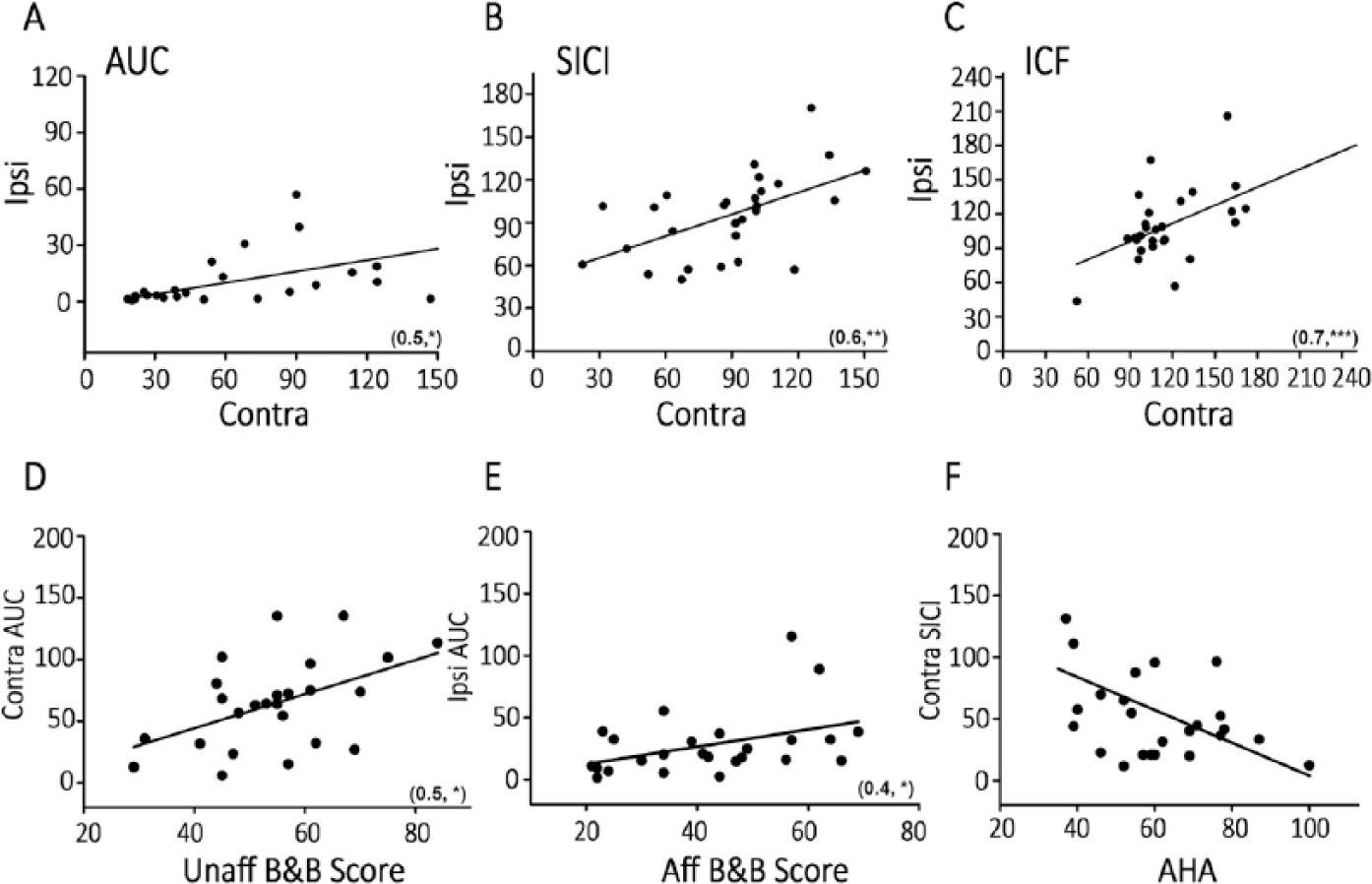
Correlation between ipsilateral and conralateral responses, and clinical and neurophysiological measures. (Top panel) A plot of contralateral against the corresponding ipsilateral (A) active area under the curve (AUC), (B) active short-latency intracortical inhibition (SICI) and (C) active intracortical facilitation (ICF). (Bottom panel) (D) A plot of contralateral AUC against unaffected(nonparetic) Box and Block (B&B) scores, (E) a plot of ipsilateral AUC against affected (paretic) hand B&B scores, and (F) a plot of contralateral SICI against Assisting Hand Assessment (AHA) scores. Each data point represents a single ipsilateral (IP) participant. *P < .05, **P < .01, and ***P < .001.
Correlation Between Neurophysiology and Motor Function
Associations were observed between contralesional motor neurophysiology and clinical motor function. Correlations between SRC AUC and motor function demonstrated specificity in IP participants; contralateral AUC was correlated with unaffected upper limb function (Figure 5D, r = 0.5, P = .01) while ipsilateral AUC correlated with affected limb function (Figure 5E, r = 0.4, P = .04) as measured by the Box and Block test. In IP participants, contralateral SICI correlated with better bimanual function as measured by the AHA while the ipsilateral association was not significant (Figure 5F, r = −0.5, P = .1). Neither contralateral nor ipsilateral ICF were correlated with clinical scores (data not shown).
Discussion
In this study, we characterized multiple neurophysiological components of the contralesional motor cortex in hemiparetic children with perinatal stroke. Our findings add to seminal previous studies by bringing focused attention to the contralesional motor cortex with application of detailed TMS measures to a large well-characterized sample of children with specific early brain injuries. Key findings are the persistence of ipsilateral projections in the majority and their association with poor motor function assessed with comprehensive, validated clinical measures. Cortical control mechanisms of the affected hand by the contralesional hemisphere have distinct qualities, including unique excitability curves, MEP latencies, and intracortical circuitry. However, these systems appear to share fundamental physiological mechanisms with how the contralesional motor cortex controls the unaffected hand. These neurophysiological measures appear to represent functional biomarkers of developmental plasticity and potential therapeutic targets.
Unilateral perinatal brain injury often results in persistence of corticomotor projections from the unlesioned hemisphere to the paretic hand. Our work complements several previous fundamental studies. Examining 4 preschool-aged children with congenital hemiplegia and prominent mirror movements with combined cortical stimulation and EMG, Farmer et al 12 described prominent input to the affected hand from the contralesional cortex. Carr et al 13 employed similar methodology in 33 congenitally hemiparetic children with comparable findings, including evidence of increased abnormal distal branching of ipsilateral inputs being associated with mirror movement intensity. Combining TMS with functional magnetic resonance imaging, Staudt et al 17 described patterns of ipsilateral reorganization in hemiparetic young people with fetal unilateral white matter lesions, the degree of which correlated with lesion size and clinical function. We observed relative proportions of approximately 2:1 of children with ipsilateral arrangements that appeared similar to these previous studies. This distcinction of subjects as “ipsilateral” or not is simple but pargamatic, including easy identification in subjects that may in turn predict responsiveness to specific therapies, 39 opening the door for personalized neurorehabilitation.
MEP characteristics can further define our understanding of developmental corticospinal reorganization following early stroke. For example, MEP morphology and the shapes of SRCs often behaved similarly between contralateral and ipsilateral sides, supporting their production by similar cortical mechanisms (see below). MEP latencies were also informative. Ipsilateral MEP latencies were significantly longer than all contralateral responses from the different groups. A case-control study of 12 participants with congenital hemiplegia described abnormally prolonged MEP latencies in both ipsilateral and contralateral directions that inversely correlated with clinic function. 40 In a seminal study of normal children by Eyre et al, 41 single pulse TMS was delivered at birth and repeated serially through the first 2 years of development. 8 Symmetrical, bilateral MEP of comparable latency and amplitude at birth gradually shifted toward dominant, larger responses from the contralateral hemisphere. Latency shortened for contralateral MEP while remaining prolonged for the diminishing ipsilateral responses. The persistence of such immature ipsilateral projections may in part explain the prolonged latencies we observed. However, this does not explain the shorter latencies in the contralateral direction and alterations in cortical and/or spinal locations may also be contributing factors.
We observed distinct differences in SRC between IP and NI participants. Reports of SRC measures in this population are limited, possibly due to the higher thresholds of young children that complicate completion of stimulation to 150% RMT. This selection bias is acknowledged in our population though we did obtain data on children as young as 6 years. Perhaps not surprisingly, ipsilateral SRC demonstrated lower slopes and areas, consistent with altered excitability. More interesting was the separation of SRC during muscle activation. While ipsilateral curves remained approximately half strength, the contralateral curves of both IP and NI participants were reduced compared to controls; an effect clearly not present at rest (Figure 3C). This identifies two potentially important considerations. One is that at least some TMS neurophysiology measures at rest carry limitations in assessing what is presumably more functionally relevant voluntary contraction. Another more novel observation is that cortical mechanisms involved in activation of the unaffected hand are clearly altered in children with perinatal stroke, regardless of how ipsilateral their developmental organization has been. This carries important functional and rehabilitation implications as patients often rely on this hand for much of their upper extremity function.
Paired-pulse paradigms were designed to investigate intracortical inhibitory and facilitory mechanisms. Such approaches have rarely been applied in this population. A case-control study of 10 participants with perinatal stroke described reduced SICI in the lesioned motor cortex but normal contralesional SICI and bilateral ICF. 42 Our results appear consistent but add additional evidence that prominent ipsilateral organization may influence SICI in the contralesional cortex. While contralateral SICI effects were comparable between IP and NI participants, SICI strength was reduced ipsilaterally. That ipsilateral and contralateral SICI effects were also highly correlated suggests similar intracortical inhibitory systems exist within contralesional motor circuits influencing both hands. Our experiments were limited to a single ISI (2 ms) though studies suggest effects diminish above this value in this population. 42 That both SICI and ICF effects were essentially abolished with muscle activation further supports the assertion that rest and active paradigms reveal distinct elements of neurophysiology in hemiparetic children.
Interpretation of TMS measures of motor cortex neurophysiology are made challenging by high inter-individual variability, age effects, and issues of lesion type and degree of functional impairment. However, the relevance of our findings appears supported by specific and consistent correlations with validated measures of clinical motor function. An example was observed with SRC where only contralateral AUC correlated with unaffected unimanual function while only ipsilateral AUC correlated with affected hand function. These are in addition to clear associations between ipsilateral status and multiple validated motor outcomes. The clinical relevance of contralesional motor neurophysiology may not be limited to those with ipsilateral projections. Small case series have demonstrated functional significance of contralesional motor network activations in participants without prominent ipsilateral projections. 43 Studies using modulatory forms of noninvasive brain stimulation such as virtual lesions or plasticity protocols may shed further light on functional relevance.
Characterizing contralesional motor neurophysiology carries therapeutic potential. Combining animal44,45 and human10,46 evidence, there are increasingly informed models of motor system development following unilateral perinatal brain injury. These in turn have generated central therapeutic targets for potential therapeutic neuromodulation. 7 Noninvasive neuromodulation with rTMS has demonstrated efficacy in many adult conditions, inlcuding stroke-induced hemiparesis where the contralateral M1 is the most common target. 23 Reorganization patterns have recently been shown to dictate responsiveness to constraint-induced movement therapy in hemiparetic subjects with perinatal brain injury. 39 A trial of contralesional inhibitory rTMS in 19 children with perinatal stroke and hemiparesis demonstrated efficacy and favourable safety. 25 A factorial, randomized controlled trial in 45 children has recently reported similar results. 24 Improved understanding of contralesional motor network physiology will facilitate target identification, patient selection, and future development of such interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Heart and Stroke Foundation of Canada and Alberta Children’s Hospital Foundation.