
Abstract
Background. The identification of deficits in interjoint coordination is important in order to better focus upper limb rehabilitative treatment after stroke. The majority of standardized clinical measures characterize endpoint performance, such as accuracy, speed, and smoothness, based on the assumption that endpoint performance reflects interjoint coordination, without measuring the underlying temporal and spatial sequences of joint recruitment directly. However, this assumption is questioned since improvements of endpoint performance can be achieved through different degrees of restitution or compensation of upper limb motor impairments based on the available kinematic redundancy of the system. Confusion about adequate measurement may stem from a lack a definition of interjoint coordination during reaching. Methods and Results. We suggest an operational definition of interjoint coordination during reaching as a goal-oriented process in which joint degrees of freedom are organized in both spatial and temporal domains such that the endpoint reaches a desired location in a context-dependent manner. Conclusions. In this point-of-view article, we consider how current approaches to laboratory and clinical measures of coordination comply with our definition. We propose future study directions and specific research strategies to develop clinical measures of interjoint coordination with better construct and content validity than those currently in use.
Introduction
Characterizing coordination during reaching is a challenge for researchers and clinicians. Upper limb (UL) motor function is impaired in around 80% of stroke survivors, 1 with motor recovery proportional to the initial level of impairment.1,2 However, we know little about how motor recovery occurs and which assessments may best capture this process. 3 To better distinguish recovery and compensatory motor processes after stroke, Levin et al 4 proposed a terminology based on 2 levels of description: endpoint displacement and joint/segment rotations/movements. Motor performance is quantified by the characteristics of endpoint displacement such that for reaching, better movement is considered to be faster, more accurate and smoother with a lower level of variability. 5 At a more analytical level, movement quality is characterized by the individual joint rotations or segment movements (ie, trunk) as well as the coordination between 2 or more joints. An underlying assumption is that smooth and precise movement at the endpoint level depends on coordinated movement at the joint or segment level. However, few clinical measures directly quantify interjoint or intersegment coordination during reaching in patients recovering from stroke. The purpose of this point of view is to identify gaps in the methods used to quantify interjoint coordination in laboratory and clinical settings, and to suggest solutions to the problem of coordination measurement in the clinic.
The Problem
With increasing recognition that basic principles of motor control and motor learning should be better understood and incorporated into rehabilitative efforts to improve movement, an examination into how we define and measure fundamental features of movement is warranted. Damage to descending pathways after stroke leads to the appearance of stereotypical UL movement patterns, referred to as abnormal synergies. 6 The term synergy has been used clinically to describe abnormal recruitment of multiple joints in a specific pattern when isolated joint movement is desired. 6 Some clinical scales of motor recovery measure synergy severity (eg, Fugl-Meyer Assessment [FMA], 7 Chedoke-McMaster Assessment [CM] 8 ). In contrast, in the motor control literature, the concept of synergy is defined as a task-specific organization of many elements aiming to stabilize one or more performance variables. 9 Specifically, reaching movement (eg, endpoint trajectory) can be accomplished by an infinite number of joint configurations (degrees of freedom [DFs] 10 ), which provide abundant movement patterns to accomplish the same motor task. 9 The “principle of abundance” implies that the numerous DFs allow the system to adapt movement to changing environmental conditions, often occurring during performance of activities of daily life. Motor abundance is reduced in patients with stroke,11,12 resulting in the system finding other solutions for task accomplishment including the incorporation of compensatory movement. For example, some patients with stroke recruit excessive trunk and/or shoulder displacement during reaching and pointing11,13,14 and can use these compensations to adapt movement in task-dependent ways. Movements of the arm-plane angle have been used to quantify shoulder compensations. 15 The arm-plane angle is greater in patients with stroke, yet can be used adaptively to increase endpoint precision in patients with mild-to-moderate stroke. 15 Evidence also suggests that the remaining variability in the task-dependent structure of UL kinematics can be used adaptively during reaching and pointing tasks in chronic stroke. 16 Therefore, measurement of interjoint coordination and task-specific variability are important for understanding reaching deficits in stroke.
As defined above, UL motor recovery after stroke is often characterized by improvements in endpoint performance during reaching in both laboratory17,18 and clinical settings.19,20 Such clinical measures as the Finger-to-Nose Test 7 and the Box and Block Test 21 characterize performance indirectly by measuring movement time (eg, time to complete 5 movements) or task completion (eg, number of blocks transferred in a box) respectively. Both these clinical measures implicitly assume that endpoint performance reflects interjoint coordination or movement quality. Although recent studies support a relationship between Finger-to-Nose Test completion time 22 or endpoint path curvature 23 with elbow-shoulder temporal coordination, the relationship between other endpoint performance measures (ie, smoothness) and interjoint coordination has not been evaluated. This illustrates that the lack of an operational definition of coordination, accounting for movement features measured in the laboratory or clinic, is a limiting factor when translating basic science evidence to clinical practice.
For the purposes of this dialog, we start by providing an unambiguous operational definition of interjoint coordination for reaching movement. We examine assumptions about the relationship between endpoint performance and interjoint coordination and identify whether and how interjoint coordination during reaching is measured clinically. We discuss the advantages and disadvantages of using kinematics to describe interjoint coordination and offer solutions to the problem of coordination measurement in the clinic. We limit our consideration to UL reaching or pointing tasks without object manipulation in an ecological sense. However, it is assumed that the principles underlying the definition and measurement of interjoint coordination for different types of UL tasks are similar.
Definition of Interjoint Coordination
Bernstein 10 defined coordination of human movement as the process of mastering redundant DFs. This definition implies that coordination is a process rather than a consequence of movement. While endpoint performance measures, such as movement error, velocity, and smoothness have been used as measures of “upper limb coordination” clinically (eg, Finger-to-Nose Test), they do not directly reflect multi-DF coordination, but emerge only as a result of this organization. Similarly, spatial and temporal endpoint variables, such as trajectory length or curvature (spatial) and movement units (temporal), are also emergent features of coordination. Because of kinematic redundancy, the same endpoint performance can be achieved by many different combinations of DFs. For example, excessive trunk recruitment is the typical compensation observed in individuals with stroke to preserve endpoint trajectory and smoothness. 11 Thus, recovery assessment based only on endpoint performance variables does not differentiate between improvement due to compensatory trunk displacement versus true recovery of active arm joint ranges and interjoint coordination. Furthermore, endpoint measures are insufficient to describe how different DFs are coordinated and/or combined to produce movement.
There is a lack of consensus about the operational definition of coordination for reaching and pointing tasks. Krasovsky and Levin 24 operationally defined locomotor coordination as: “The ability to maintain a context-dependent and phase-dependent cyclical relationship between different body segments or joints in both spatial and temporal domains.” The important insight is that both spatial and temporal aspects covary and should be measured together. However, a direct translation of knowledge gained from gait to reaching studies is limited because of differences in movement characteristics of the upper limb compared with those of the lower-limb (eg, lack of cyclicity, more possible movements and DFs 25 ). In light of these differences, we suggest an operational definition of coordination for reaching and pointing as: “A goal-oriented process in which DFs are organized in both spatial and temporal domains such that the body configuration enables the endpoint to reach to a desired location in a context dependent manner.”
Clinical Measurement of UL Reaching
Reaching is a task-dependent movement with the goal of bringing the endpoint (eg, hand) to a desired location within or beyond the arm workspace and at a desired time, considering task and environmental (eg, gravity) constraints. 9 Spatially, the endpoint trajectory usually follows a relatively straight path and is characterized temporally as having a single peak velocity. To accomplish straight line trajectories, 2 or more joints have to be recruited since rotations at single joints necessarily produce curved endpoint movement. 26 Temporally, when multiple peaks occur in the reaching velocity profile, the movement is thought to be composed of several smaller, corrective submovements.27,28 Deficits in spatial and temporal interjoint coordination during reaching in individuals with stroke can result in more curved and less smooth endpoint movements. 13
Measures of UL function are classified at the Body Functions and Structure and Activity levels of the International Classification of Functioning, Disability and Health (ICF). 29 Interjoint coordination is not specifically identified but can be included in several classifications at the Body Functions and Structure level: b760 (Control of voluntary movement functions), and subcategories b7600 (Control of simple voluntary movements), b7601 (Control of complex voluntary movements), and b7602 (Coordination of voluntary movements). Clinical measures such as the Fugl-Meyer Assessment of the Upper Limb can be listed under this classification (Table 1). Reaching activity is classified as an Activity limitation, d4452 (Reaching). Clinical measures of the ability to complete UL activities (eg, Wolf Motor Function Test [WMFT]; Table 1) can be categorized in this domain. An underlying assumption is that the ability to complete a task (eg, fold a towel, WMFT) is related to some degree of coordination between UL joint movements. However, according to the definition above, interjoint coordination is only one element needed to complete a task, in the absence of which, the task may be completed by other means. Clinical measures often infer the presence of interjoint coordination by measuring parameters of endpoint performance, such as speed, smoothness, and accuracy using both visual observation and time quantification. However, in the process of rehabilitation, these endpoint performance parameters can improve by true recovery or compensation.4,30 For example, when excessive trunk displacement assists forward hand movement, endpoint trajectory parameters may be indistinguishable from those when only shoulder and elbow displacements are used.11,31 Such a distinction is only partially captured by commonly used clinical assessments of time to task completion. 22
Summary of Psychometric Properties of Clinical Measures That Include an Upper Limb Reaching and/or a Reach-to-Grasp Movement—Organized According to Body Functions and Structure and Activity levels of the International Classification of Function.
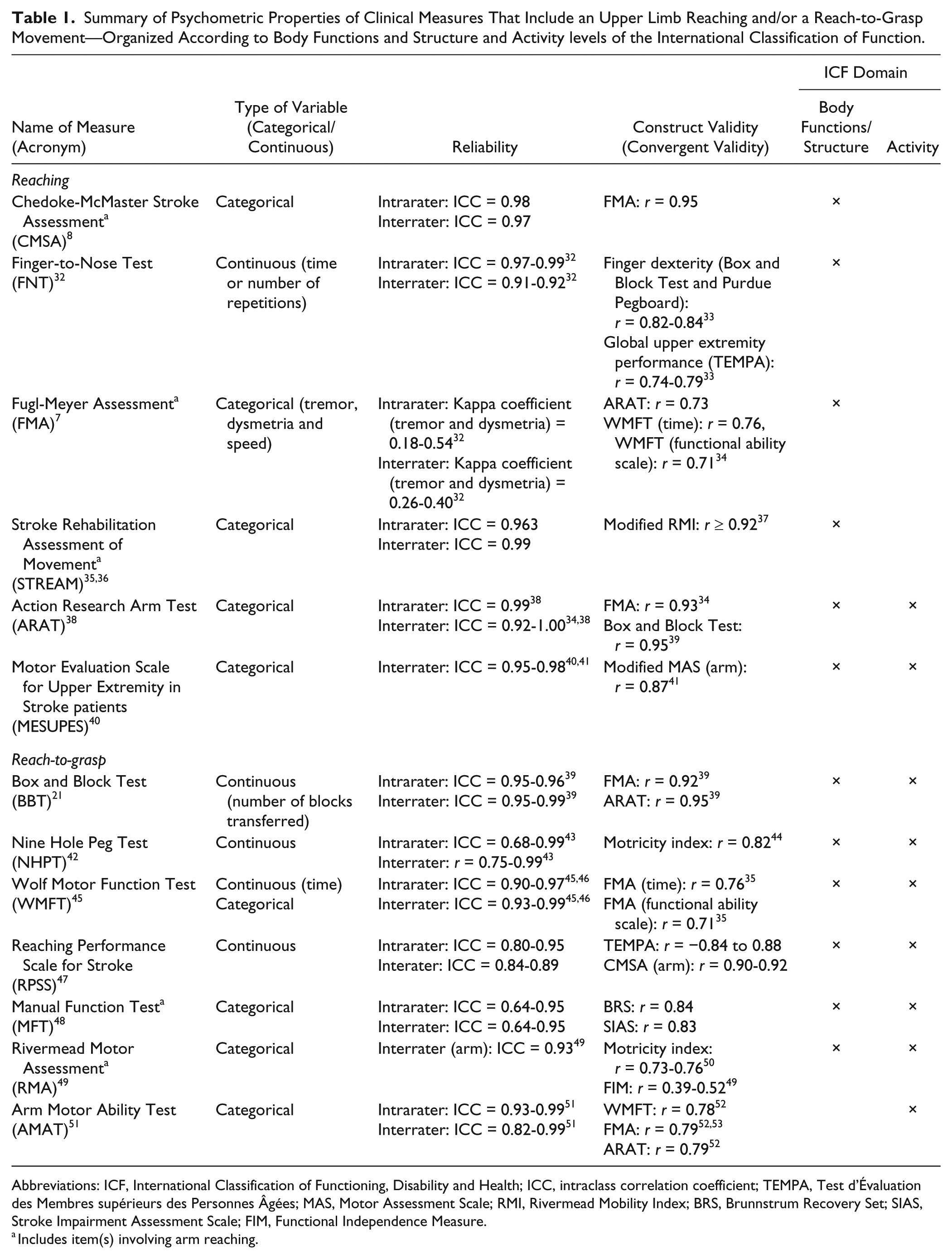
Abbreviations: ICF, International Classification of Functioning, Disability and Health; ICC, intraclass correlation coefficient; TEMPA, Test d’Évaluation des Membres supérieurs des Personnes Âgées; MAS, Motor Assessment Scale; RMI, Rivermead Mobility Index; BRS, Brunnstrum Recovery Set; SIAS, Stroke Impairment Assessment Scale; FIM, Functional Independence Measure.
Includes item(s) involving arm reaching.
Furthermore, most UL reaching functions are measured on ordinal scales describing endpoint performance (ie, 6-point rating scale in the Functional Ability scale of WMFT; Table 1) or time required for task completion without considering movement strategy or quality during performance. In addition, scales may have floor or ceiling effects, low resolution in terms of response options, low intra- and/or interrater reliability (eg, coordination item in FMA-UL; Table 1) and depend on visual observation affected by rater experience or training.
In summary, although measures of endpoint performance may allow clinicians to infer problems with interjoint coordination, no clinical scale directly measures this construct during UL tasks.
Laboratory Measurement of UL Interjoint Coordination
In keeping with our definition of interjoint coordination, we categorized laboratory measures into those that address temporal and spatial domains. We expand our definition to consider discrete and continuous measures of body segments or joint movement in each domain. Discrete measures characterize the instantaneous relationship between joints (or body segments) at a particular time point, while continuous measures characterize the dynamic relationship between the segments throughout the movement. Laboratory measures for each category are described below and their advantages and limitations are discussed. Psychometric properties of the measures are summarized in Table 2.
Summary of Psychometric Properties for Measures of Interjoint Coordination During Reaching—All at the Body Functions and Structure Level.
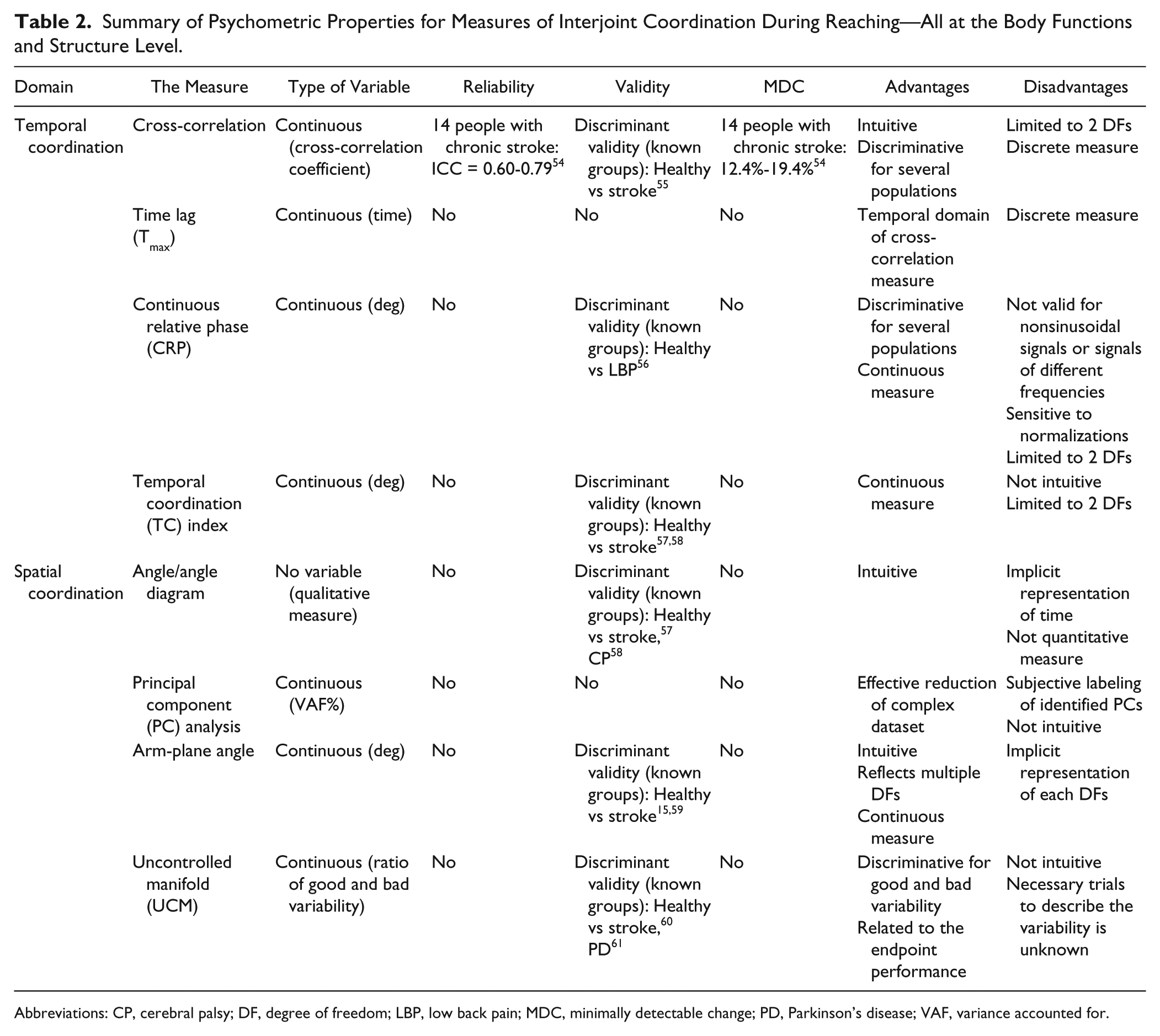
Abbreviations: CP, cerebral palsy; DF, degree of freedom; LBP, low back pain; MDC, minimally detectable change; PD, Parkinson’s disease; VAF, variance accounted for.
Temporal Measures
Discrete Temporal Measures
Cross-correlation coefficient
The cross-correlation coefficient between 2 joint movements ranges between −1 and 1 and has been used to measure temporal interjoint coupling during reaching in individuals with stroke.17,55 The time lag (τ) is the delay between movements of each joint and is measured by artificially shifting one joint profile in time until the 2 signals overlap (Figure 1A and B). Highly positive or negative cross-correlation coefficients indicate tight in-phase or anti-phase coupling, respectively. A value near zero indicates independent joint movement. 62 Test-retest reliability of the elbow-shoulder cross-correlation coefficient during the transport component of a reach-to-grasp task in individuals with chronic stroke was reported to be good, ranging from intraclass correlation coefficient (ICC) = 0.60 to 0.79 with a minimal detectable change of 12.4% to 19.4%. 54
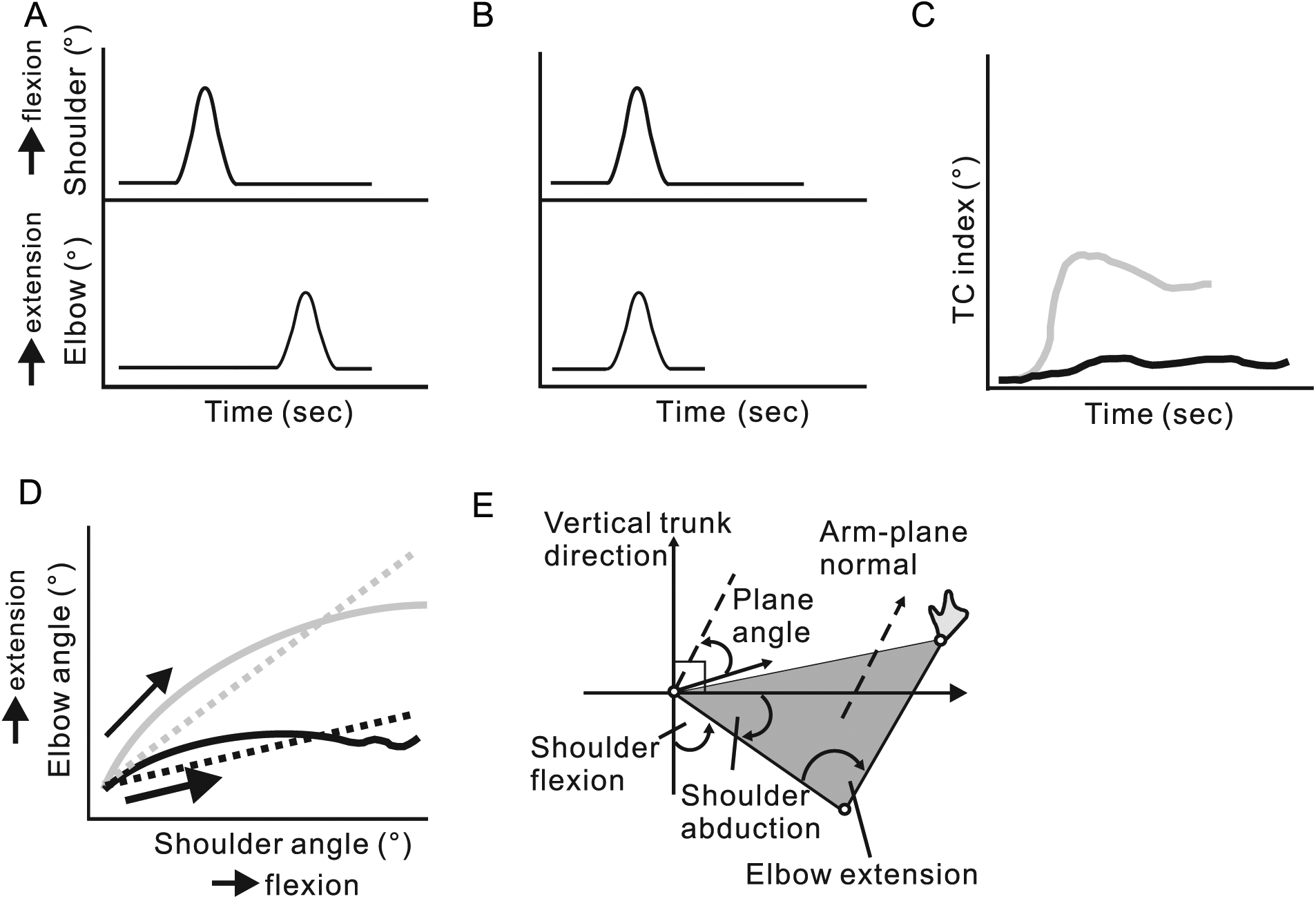
Diagrams of temporal (A, B, C) and spatial (D, E) interjoint coordination measures. (A) Examples of joint angles (shoulder, elbow) plotted as a function of time that are not coupled (cross-correlation coefficient = 0). (B) When a time lag of 1 second (τ = 1) is added to the elbow trace, interjoint coupling occurs (cross-correlation coefficient = 1, Tmax = 1 second). However, the total joint movement time is decreased by 1 second. (C) An example of the temporal coordination index (TCI) in a healthy (gray line) and stroke subject (black line) performing a 3-dimensional pointing movement to a sagittal target at shoulder height and arm’s length. 57 The different amplitude and shape of the TCI of the stroke subject indicates altered temporal interjoint coordination between shoulder and elbow joint movements. (D) Angle-angle diagram between elbow extension and shoulder flexion angles during forward reaching in healthy (solid gray line) and stroke (solid black line) subjects. Compared with the healthy subject, the diagram of the movement in the stroke subject shows less elbow extension and disruptions at the end of the movement. Straight lines show linear slopes of each angle-angle relationship (healthy, gray dotted line; stroke, black dotted line). (E) The arm-plane angle is formed by 3 markers placed on the shoulder, elbow, and wrist and is the complement of the angle between the arm-plane normal and the vertical trunk direction. In this system, a greater complement angle represents a higher elbow elevation (modified from figure 1 in Merdler et al 59 ).
Advantages
The cross-correlation coefficient indicates coupling strength between 2 joints with a time lag estimate (τ). The coefficient at zero time lag (
Limitations
The cross-correlation coefficient only provides a measure of coupling between 2 joints out of a larger number of DFs involved in the movement. In addition, since it is measured at a single time point, it does not indicate how coupling changes throughout the movement. Computationally, since the cross-correlation is calculated between two signals with the same length, the artificial time delay decreases the length of data shared by the 2 signals such that the greater the τ, the more data are eliminated from the calculation. Therefore, a cross-correlation coefficient with a large τ may not adequately represent the relationship between 2 signals. Presently, there is no established maximal value of τ. Indeed, different movements may be characterized by different time lags depending on joint movement directions and segment lengths. For example, when both joints (ie, elbow and shoulder) move in the same direction by the same amount such as when reaching upward in the sagittal plane, coupling may be high at a zero time lag, but it may be low when each joint moves differently such as during horizontal circle drawing. Thus, cross-correlation coefficients must be interpreted with respect to the movement being described. Furthermore, test-retest reliability of τ is unreported.
Continuous temporal measures
Continuous relative phase
The relative phase between movements of two joints describes the intrinsic dynamics of a 2-joint arm system.63,64 Dynamic stability has been measured by generating displacement versus velocity phase diagrams of movements of each joint or body segment. From the resulting phase plane trajectories, a phase angle φ = tan−1(velocity/displacement) is calculated for each data point throughout the entire motion. The continuous relative phase (CRP) curve of 2 joints is derived from the difference between the phase angles of the first and second joint angle at each moment throughout the movement. Two segments (eg, arms) swinging in an anti-phase manner have a CRP of 180°, while those swinging in-phase yield a CRP of 0°.
Temporal coordination index
Cirstea et al 57 introduced a temporal coordination index (TCI) to measure shoulder-elbow coupling during reaching from sitting in individuals with chronic stroke (Figure 1C). The TCI is a complex measure based on the difference between the phase angles of 2 joints. The TCI discriminated between temporal shoulder-elbow coordination patterns in individuals with mild and moderate-to-severe stroke, 57 as well as between typically developing children and children with cerebral palsy during reaching movement. 58
Advantages
CRP and TCI are continuous measures of changes in temporal coupling throughout the movement.
Limitations
CRP and TCI are computationally complex and relevant only to the description of the coupling between 2 DFs for any given movement and have mainly been applied to shoulder-elbow movement. Consequently, when more than 2 DFs are involved in a movement, the pair of DFs that is most representative of the particular movement pattern has to be selected for analysis. Furthermore, the test-retest reliability of CRP and TCI measures has not been reported.
Spatial Measures
Discrete spatial measures
Angle/angle diagrams
Angle/angle diagrams describe the instantaneous spatial relationships between 2 joints (Figure 1D). Despite the many possible joint combinations, most studies have examined shoulder flexion/abduction and elbow flexion/extension to characterize interjoint coordination during reaching or pointing in healthy subjects, 65 in adults with hemiparesis,13,60 and in children with cerebral palsy and developmental coordination disorder.62,66,67 Linear or polynomial regression slopes between 2 joints in the angle/angle diagram have been used to quantify spatial interjoint coordination. 13 For linear slope estimations, a value of 1 or −1 indicates that for each degree of movement in one joint, the adjacent joint contributes an equal degree of movement in the same or opposite direction respectively. A slope of less than or greater than 1 would indicate that one joint contributes more or less to the movement compared to the other.
Advantages
The angle/angle diagram directly represents the relationship between 2 DFs identified as being important for the movement.
Limitations
Because of the implicit representation of time, one dimension in the diagram should be transformed to represent the timing of an instantaneous event such as a change in the interjoint pattern between individuals or groups (ie, a change in slope during the movement). Although the slope of the angle/angle diagram describes the overall contribution of each joint (Figure 1D), the quality of the regression line (goodness of fit) is not routinely reported.
Principal component analysis
There are many combinations of joint angles that can be used to reach the same endpoint position in the arm workspace. 68 Principal component analysis (PCA) is a statistical method used to reduce the number of elements of a given set of mutually correlated variables (eg, adjacent arm joints) into a smaller set of elements. A correlation matrix between joint angles is generated and eigenvectors are extracted. The ratio between the first eigenvalue and all the eigenvalues gives a number between 0 and 1 (ie, PC1%). The smaller set is uncorrelated. The first few components usually account for most of the variance in the original dataset. 69 For example, van Kordelaar et al 14 investigated longitudinal changes in UL and trunk kinematics during a reach-to-grasp task in subjects using PCA. In stroke and healthy subjects, 10 PCs were identified and the first PC accounted for 82% and 87% of the variance of arm and trunk rotation, respectively. In both groups, shoulder horizontal adduction and elbow extension contributed most to the task. Similar analyses have been used in a wide range of populations, including children with cerebral palsy 66 and patients with Parkinson’s disease. 70
Advantages
PCA can effectively decrease the dimensionality of a given set of kinematic data and identify the main joint rotations used to perform a task. Although it is generally used as a discrete measure of the behavior of a large element dataset, it can also provide information about the dynamic structure of a movement when computed at multiple time points.
Limitations
Although several PCs can often be identified, only the first PC can be interpreted. 14 This highlights a common problem of PCA: after data reduction, PCs have to be individually labeled based on the experimenter’s prior knowledge, expertise or assumptions. 71 Data interpretation is subjective and clinically ambiguous, as the same result may be interpreted differently by different observers. Another problem of PCA is the subjective determination of the threshold variance above which a PC is considered meaningful. Finally, while PCA can explain global factors in the structure of a dataset, it cannot identify specific motor elements underlying reaching deficits. A more specific analysis of individual joint ranges of motion is still needed to target such factors.
Continuous spatial measures
Arm-plane angle
Covariations of multiple limb segment rotations in 3-dimenssional space during certain motor tasks fall on a plane and are thought to reflect synergistic changes between movements of multiple joints in a chain. 72 For example, the shape and orientation of lower limb joint planar covariation is related to the acquisition of stable locomotion in toddlers 73 and is similar when walking at different speeds and for different gaits (running, hopping, obstacle avoidance). 72 This measure has been used to characterize intersegmental coordination of the lower limbs in children with cerebral palsy.73-75 It has also been applied to assess UL movements during reaching. A greater arm-plane angle (shoulder, elbow and wrist) represents a higher elbow elevation. 76 The arm-plane angle has been used to analyze reaching in healthy adults and stroke subjects (Figure 1E).15,59
Advantages
The arm-plane measure characterizes multiple joint segment covariance compared with individual joint kinematics, and can be recorded with a reduced marker set (ie, only 3 markers on the whole arm replacing multiple markers to compute arm segment movements separately). Furthermore, the arm-plane angle is a continuous measure that can capture body segment covariation throughout the movement.
Limitations
Planar covariation measures have been used extensively to describe the behavior of the leg during different locomotor tasks in different populations. Only a few studies have used it to describe reaching behavior in healthy and stroke subjects. The arm-plane angle does not represent the individual joint displacements. Because the measure represents the angle between the arm-plane and the trunk vertical coordinate, there are an infinite number of combinations of elbow and shoulder joint displacements that can represent a particular arm-plane angle. Therefore, the measure is generally reported along with a description of individual joint displacements. The test-retest reliability of arm-plane angle measures has not been reported.
Spatial-Temporal Measures of Variability
Variability between movements of different joints is an important aspect of interjoint coordination. For example, a less proficient movement may be characterized by a higher degree of spatial joint coupling, demonstrating a reduction in normal movement variability, 10 and more skilled performers can use more or fewer DFs depending on the task demand. 68 Decreased spatial joint variability over repetitions is common in pathological conditions, including stroke.12,14 This is often measured as the standard error or deviation of the mean of one or more joint displacements. However, standard deviation measures do not describe the structure of the variability, which is important for assessing whether and how spatial variability contributes to a desired outcome, such as movement accuracy. In contrast, the uncontrolled manifold (UCM) approach was designed to specifically measure task-related variability. UCM is based on the idea that the central nervous system organizes elemental motor variables (eg, muscles, joint angles, forces) that are important to ensure the stability of motor performance with regard to a particular performance variable (eg, endpoint position in reaching). For a reaching task, displacements of multiple UL DFs are quantified at each time point between movement beginning and end. A constraint of this approach is that the endpoint position and whole arm configuration has to be identical at the beginning of each movement trial. Then, the variability of individual joint rotations across repetitions is separated into 2 components (Figure 2). The component that reflects combinations of joint rotations leading to endpoint progression toward the target is called “good” variability or VUCM. The component reflecting joint rotations moving the endpoint away (orthogonal) from the target is called “bad” variability or VORT.77,78 Stable movements are those in which VUCM is greater than VORT through all movement phases.
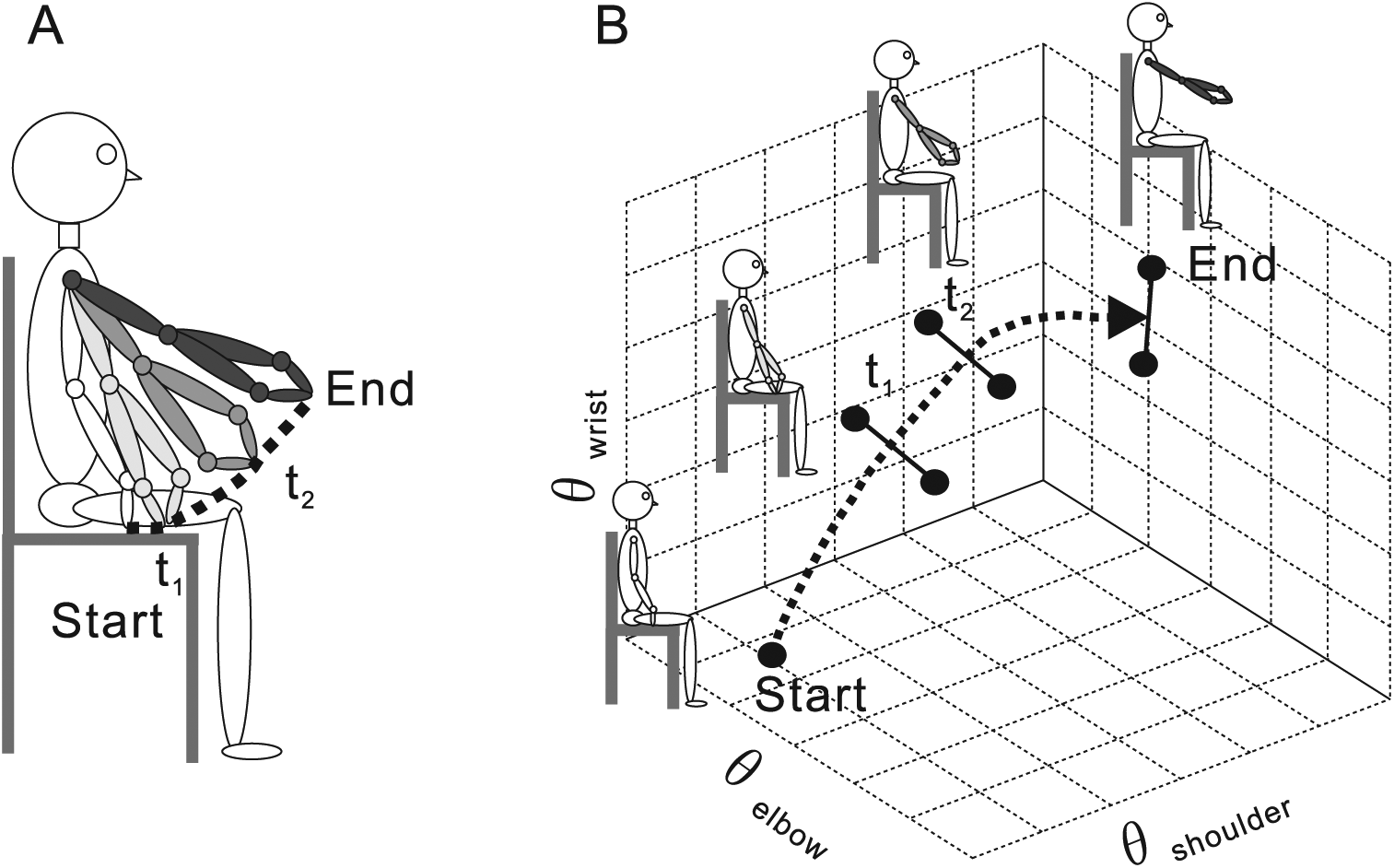
Uncontrolled manifold (UCM) analysis of a seated reaching task. (A) A subject performing a reaching movement in sitting. The initial body configuration is shown in white. Joint configurations at 4 different time points (start, t1, t2, and end) are shown. Because of kinematic redundancy, the same endpoint trajectory (dashed line) can be accomplished by different combinations of joint movements at the shoulder, elbow, and wrist. (B) Elbow, shoulder, and wrist interjoint coordination plotted in 3-dimensional space. Black circles indicate the 3 joint interjoint coordination at 4 time points for 2 trials. A line connecting the black circles at each time point indicates a UCM space, where different interjoint coordination stabilize the endpoint position. The estimation of the UCM space becomes more accurate as the number of repetition becomes greater.
Advantages
The standard error or deviation of joint displacement is a straightforward measure and can be easily calculated. When the UCM is expressed at each time point during the movement, it provides a continuous (temporal) measure of variability structure in joint space with respect to the performance variable.
Limitations
The UCM analysis has several limitations. First, test-retest reliability and minimally detectable change during reaching have not been reported. Second, UCM analysis requires the collection of kinematic data during the performance of multiple trials of a task set up with specific constraints,77,78 making its interpretation relative to tasks measured in the clinic questionable. Presently, the minimal number of repetitions needed for the analysis has not been validated. Third, as for PCA, UCM analysis also requires an accurate representation of multiple DFs and a subjective choice of elemental and performance variables.
The Solution
Our operational definition emphasizes that interjoint coordination is a process underlying the accomplishment of a certain task goal such as reaching. Most clinical scales of UL motor function or activity assume that good interjoint coordination underlies good endpoint performance, often characterized by movement precision, speed, and smoothness. This notion is supported by the classification of coordination and reaching in different ICF domains, suggesting that these 2 elements can influence each other, while they have different constructs.
To measure interjoint coordination, angle-angle diagrams (Figure 1D) may be the simplest and most intuitive quantitative approach. However, such measures may be difficult to obtain in the clinical setting due to the low precision of current clinical motion analysis systems (ie, Kinect). Thus, we propose the implementation and uptake of measurement systems providing more easily obtainable endpoint measures once their validity with respect to assessing interjoint coordination for various tasks has been established. In terms of endpoint performance, laboratory studies have characterized movement smoothness using various metrics such as number of movement units, 79 normalized jerk, 79 and path curvature 80 (Figure 3A-C). While assessment of such performance characteristics may allow clinicians to infer some degree of interjoint coordination, the validity of this assumption has not been established for different UL tasks and activities included in common clinical scales. Future studies should address the construct and content validity of kinematics describing endpoint movement as measures of interjoint coordination for different actions or tasks assessed in clinical UL scales. In addition, endpoint kinematics need to be evaluated in the context of the presence or absence of undesirable compensatory movements, to determine the extent to which compensatory movement may be occurring as a result of altered interjoint coordination.
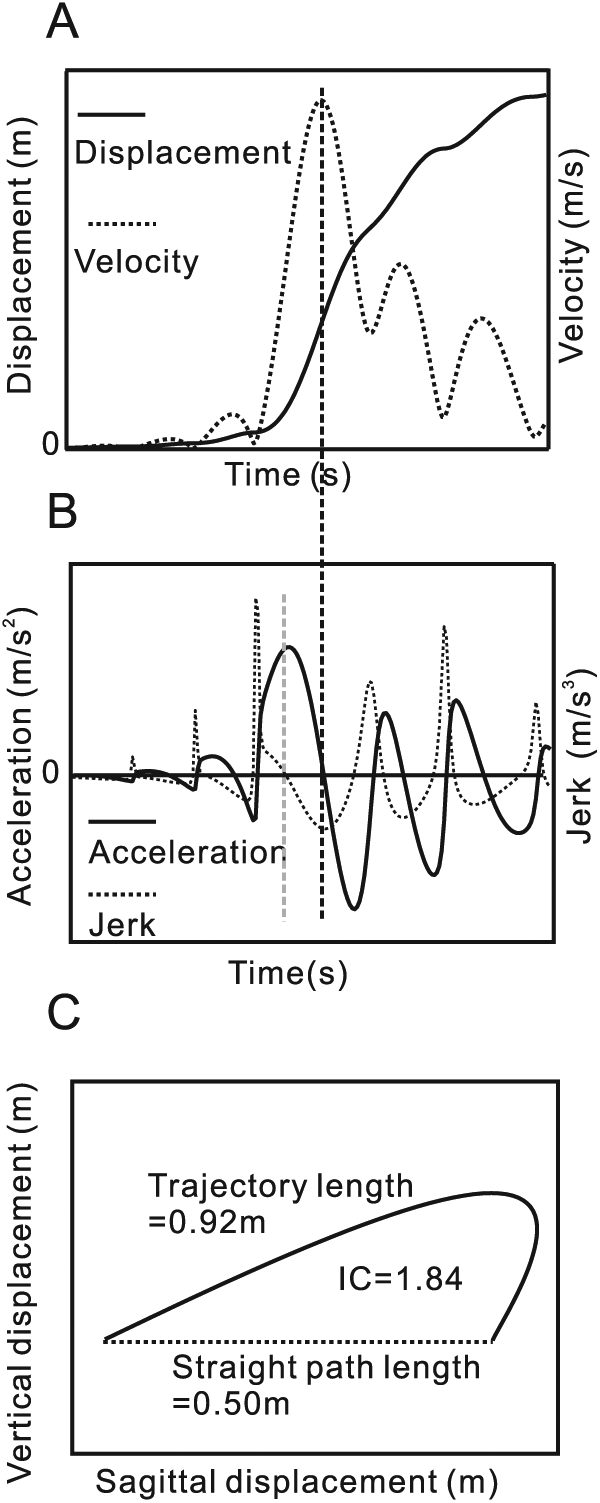
Endpoint performance variables during forward reaching. (A) Endpoint displacement (solid line) and its first derivative, velocity (dotted line), when a stroke subject performed forward reaching. The endpoint velocity has multiple peaks (4 movement units). (B) Acceleration (second derivative of displacement; solid line) and jerk (third derivative; dotted line) during the same movement as panel A. The velocity peak in A corresponds to the acceleration zero-crossing point in B (vertical dashed black line). Similarly, the acceleration peak in B corresponds to the jerk zero-crossing in B (vertical gray dashed line). (C) Two-dimensional illustration of an actual endpoint trajectory (solid line) and a hypothetical straight line connecting initial and final endpoint positions (dotted line). Index of curvature (IC = 1.84) is calculated as the ratio of the actual endpoint trajectory length (0.92 m) and the straight path length (0.50 m).
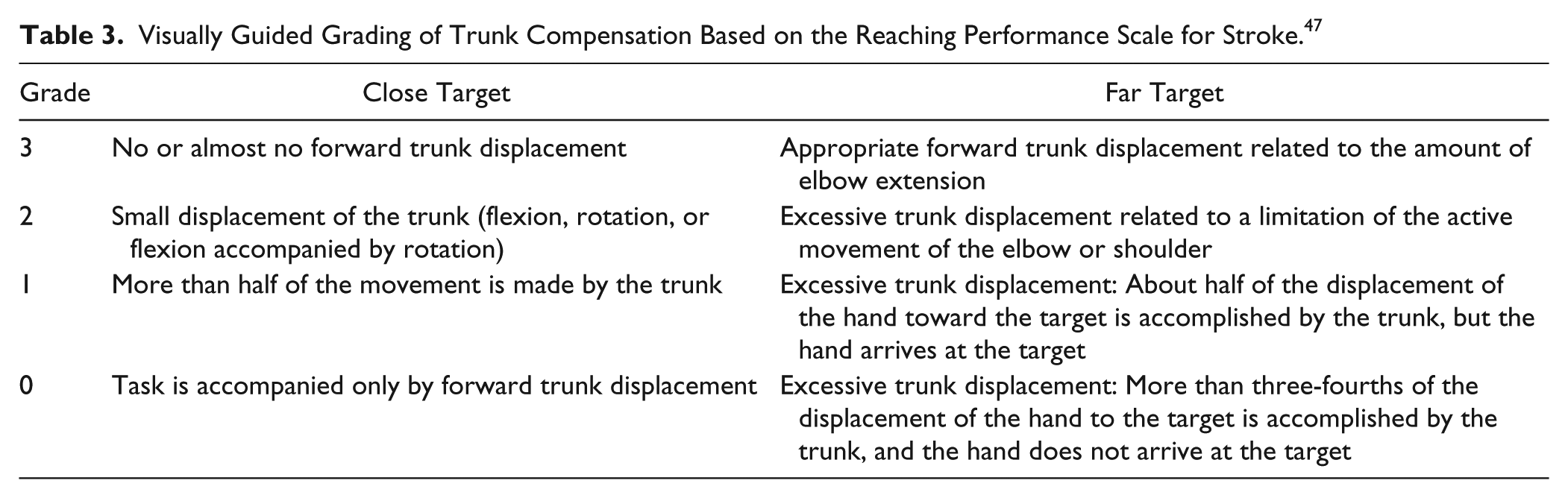
One clinical scale, the Reaching Performance Scale for Stroke (RPSS), uses observational kinematics to assess compensatory movement during reaching by rating how much individual UL joints and the trunk segment contribute to the task. 69 Interjoint coordination is scored indirectly as the degree of endpoint smoothness, while accounting for movements of the UL segments and trunk in the same scale. While the RPSS is the only clinical scale that exclusively quantifies movement quality during reaching by evaluating the degree of compensation, once validated, clinicians may include similar assessments of compensatory strategies for tasks assessed in existing clinical scales. For example, during the timing of the Finger-to-Nose Test, clinicians could visually quantify the degree to which the trunk contributes to each movement phase (Table 3).
Visually Guided Grading of Trunk Compensation Based on the Reaching Performance Scale for Stroke. 47
In lieu of recording movement kinematics with expensive motion tracking technology, low-cost devices may provide more accessible solutions. The advent of software platforms such as Nintendo Wii (Kyoto, Japan), webcam camera tracking, Microsoft Kinect (Redmond, WA, USA), and portable sensors such as accelerometers and gyroscopes have ushered in a promising new era of clinically accessible motion tracking. These technologies have been used as measurement tools as well as training tools for movements practiced in virtual reality environments. 81 Furthermore, interjoint coordination can be measured in many different environments and task conditions using these platforms due to the ease of manipulation of task conditions and training environments. Thus, low-cost devices can offer solutions for translating laboratory-based evidence of interjoint coordination measures to clinical settings. However, current camera-based tracking technology is not as precise as laboratory-based systems, with reportedly large tracking errors for shoulder movements made in different directions and distances from the camera. 82 Imprecise camera-based motion tracking also has implications for the validity of movements made in virtual reality compared to real-world environments. 83 Future research should establish the extent to which movement analysis and retraining are affected by low-quality tracking and the limits of precision tolerance.
Nevertheless, despite their limitations, low-cost tracking systems for clinical motion analysis can be improved by providing clinicians with turnkey software that automatically analyzes and scores key kinematic features of endpoint performance and movement quality during targeted tasks. An example of such a commercialized system is the NeuroCom Smart EquiTest for sensory organization. Given the wide range of possible UL tasks, the software should be sufficiently flexible for clinicians to evaluate different task-relevant kinematics such as the angle/angle profiles of different joint pairs. For current systems, however, clinicians should interpret these results with caution given the large tracking errors of these devices.
Conclusions
One of the assumptions about motor recovery is that it depends on the acquisition of the ability to coordinate movement between 2 or more joints. Thus, assessment of interjoint coordination is an important element for identifying motor recovery in stroke rehabilitation. Although many clinical scales assessing UL motor function may capture endpoint performance, a clear distinction is made between measurement of endpoint performance and coordination since their constructs are different. Future studies should address the validity of current clinical scales as interjoint coordination measures by investigating their relationship with laboratory measures. Further development of low-cost motion tracking devices, including sensors and data analysis platforms, can increase the feasibility of kinematic measurement for interjoint coordination in clinical settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Y.T. and M.R.M.R. were supported by the Richard and Edith Strauss Musculoskeletal Doctoral Fellowship awarded by McGill University. M.F.L. holds a Tier 1 Canada Research Chair in Motor Recovery and Rehabilitation.