
Abstract
Background. Many physical interventions can improve locomotor function in individuals with motor incomplete spinal cord injury (iSCI), although the training parameters that maximize recovery are not clear. Previous studies in individuals with other neurologic injuries suggest the intensity of locomotor training (LT) may positively influence walking outcomes. However, the effects of intensity during training of individuals with iSCI have not been tested. Objective. The purpose of this pilot, blinded-assessor randomized trial was to evaluate the effects of LT intensity on walking outcomes in individuals with iSCI. Methods. Using a crossover design, ambulatory participants with iSCI >1 year duration performed either high- or low-intensity LT for ≤20 sessions over 4 to 6 weeks. Four weeks following completion, the training interventions were alternated. Targeted intensities focused on achieving specific ranges of heart rate (HR) or ratings of perceived exertion (RPE), with intensity manipulated by increasing speeds or applying loads. Results. Significantly greater increases in peak treadmill speeds (0.18 vs 0.02 m/s) and secondary measures of metabolic function and overground speed were observed following high- versus low-intensity training, with no effects of intervention order. Moderate to high correlations were observed between differences in walking speed or distances and differences in HRs or RPEs during high- versus low-intensity training. Conclusion. This pilot study provides the first evidence that the intensity of stepping practice may be an important determinant of LT outcomes in individuals with iSCI. Whether such training is feasible in larger patient populations and contributes to improved locomotor outcomes deserves further consideration.
Introduction
Approximately half of those with spinal cord injury (SCI) are classified as motor incomplete (iSCI), indicating partial preservation of descending supraspinal pathways. 1 The extent of lower extremity movement in patients with iSCI may provide some potential for recovery of independent ambulation,2,3 although strategies that maximize walking function are unclear. Previous basic and applied studies have suggested specific physical training parameters may augment plastic changes in neuromuscular and cardiopulmonary systems that can influence locomotor performance following neurological injury.4-6 For example, in animal models of SCI, provision of large amounts of stepping (ie, walking) practice can facilitate greater locomotor recovery as compared to less stepping practice or practice of other tasks.7-9 In individuals with subacute or chronic SCI, the efficacy of specific stepping, or locomotor training (LT) strategies varies,10-12 although some studies suggest practice of walking-related tasks elicits greater improvements in locomotor function than nonwalking activities.13,14
While the amount of stepping practice may be important, other training variables could also influence locomotor recovery. Specifically, the intensity of exercise has been shown to influence locomotor performance in able-bodied individuals 15 and in patients with cardiovascular 16 or neurological disorders.17,18 Despite inconsistent definitions in the literature,19-22 “intensity” is defined here as workload or power output, consistent with definitions used in exercise physiology. 23 Locomotor intensity is readily manipulated by altering movement (ie, walking) speeds or loads carried, and estimated indirectly using cardiopulmonary or subjective measures, such as heart rate (HR) or ratings of perceived exertion (RPE). Mechanisms underlying gains in locomotor function following high-intensity training across populations may include increased metabolic capacity15,24-26 through changes in cardiopulmonary capacity 25 and efficiency, 26 muscular metabolic alterations,27,28 and increased synthesis and release of neurotrophic factors29,30 that may underlie plastic changes in supraspinal or spinal circuits. 31
Despite these potential gains, the contribution of high-intensity training to locomotor recovery following iSCI is unknown. In patients with other acute-onset neurological injuries (ie, patients poststroke), LT performed at moderate to high intensities (ie, up to 85% of maximum HR) has been shown to improve walking function as compared with lower intensity interventions,32,33 even when the amount of practice is controlled.17,18 While gains in cardiopulmonary capacity have been observed with such training, 26 improvements in neuromuscular impairments 34 and walking function35,36 have also been demonstrated.
Few studies have attempted to investigate the specific effects of exercise intensity during LT in individuals with iSCI.11,14,37 Gorman and colleagues 14 recently reported higher peak oxygen consumption (VO2peak) following robotic-assisted LT versus a conventional training program. However, the specific effects of locomotor exercise intensity were not clear, as treatments varied in both the amount and types of practice, and robotic-assisted LT is typically performed at lower intensities.38,39 Another study by Yang et al 11 comparing skilled walking training versus massed stepping practice (endurance training) on a treadmill found the latter to result in significantly greater improvements in selected locomotor outcomes. However, the primary emphasis in this trial was on differences in types of training rather than exercise intensity. While selected recent studies indicate positive influences of high-intensity LT on locomotor function, neurotrophin synthesis, and metabolic capacity, 30 no studies have demonstrated whether higher versus lower intensity LT can elicit greater improvements in walking outcomes following iSCI.
The goal of this study was to evaluate the effects of high- versus low-intensity LT in subjects with iSCI on clinical and metabolic measures of gait performance. Using a randomized crossover design with blinded assessments, the effects of high- versus low-intensity training focused only on stepping was assessed in individuals >1 year following iSCI. Consistent with previous studies, we hypothesized that measures of locomotor function would improve to a greater extent following high-intensity LT. Such information may provide further rationale for employing high-intensity training during the rehabilitation of patients with iSCI.
Methods
Study Sample and Design
Individuals were recruited if they presented with a motor iSCI (classified as C or D using the American Spinal Injury Association Impairment Scale) at neurological injury level of T10 or above for >1 year duration. Additional inclusion criteria were the follwoing: 18 to 75 years old; overground self-selected walking speed <1.0 m/s without physical assistance but with assistive devices and bracing below the knee as needed; intact quadriceps and plantarflexor tendon reflexes; and medical clearance to participate. Exclusion criteria included severe lower extremity contractures; osteoporosis; cardiovascular or metabolic instability; unhealed decubiti or existing infection; active heterotrophic ossification; previous history of other central nervous system injury; and inability to adhere to study requirements. Participants could not be enrolled in physical therapy during training. The project was approved by the Northwestern University Institutional Review Board and all participants provided written informed consent.
Using a repeated-measures crossover design, participants were randomized to receive up to 20 sessions of either a high- or low-intensity LT over 4 to 6 weeks, followed by a 4-week wash-out, after which participants received the other training paradigm (Figure 1). Given the potential limitations and difficulties of traditional randomized trials, 40 the crossover deign was used to increase the efficiency of the sample size used. A previous study suggested 12 individuals poststroke were necessary to demonstrate significant between-group differences following high- versus low-intensity LT for primary outcomes, 17 and 16 to 18 total subjects were targeted to accommodate for differences in patient populations, including greater impairments (ie, less volitional control bilaterally). Subjects were stratified by gait speed (<0.5 m/s and 0.5-1.0 m/s) and block-randomized (4 per block) into high- or low-intensity LT first.
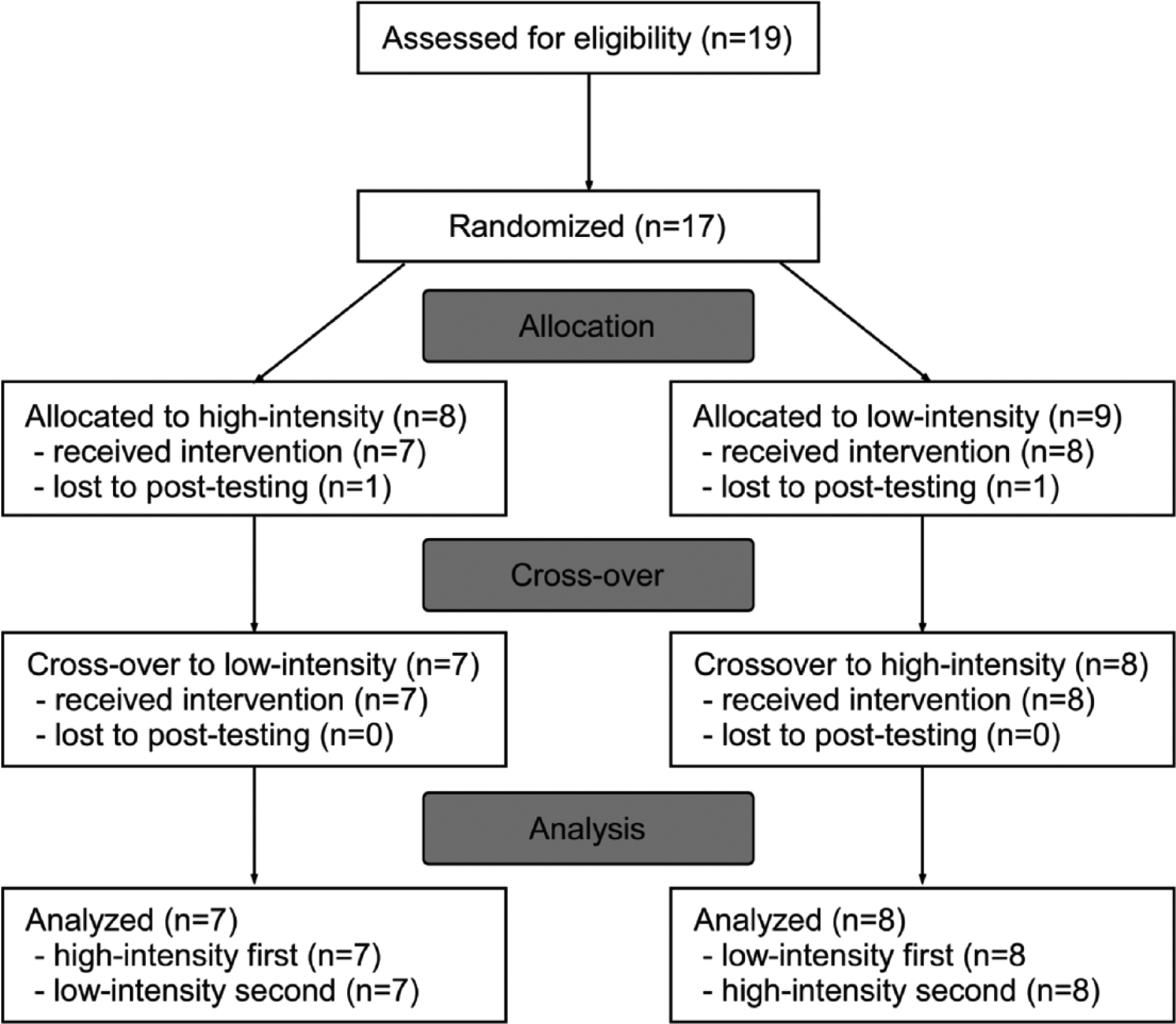
CONSORT (Consolidated Standards of Reporting Trials) flow diagram of randomized crossover design.
Intervention
Both high- and low-intensity LT consisted of up to 20 one-hour sessions at a frequency of 3 to 5 days/week over ≤6 weeks. To ensure consistency of training sessions using the crossover design, the number of sessions for the second training protocol was matched to the first protocol. The goals of LT sessions were to achieve 40 minutes of stepping practice while maintaining the desired HRs or RPEs. The use of assistive devices and therapist assistance varied according to each subject’s capability and safety. The primary measure of intensity was training HRs, which was monitored continuously using pulse-oximetry, and correlates well with oxygen consumption in intact and impaired individuals. With determination of maximum age-predicted HR (208 − (0.7 × age)), the goal of high-intensity LT was to maintain HRs within 70% to 85% of predicted maximum HR (HRmax)35,36 while low-intensity training targeted 50% to 65% HRmax; these HR ranges approximate those observed during conventional physical therapy.35,41 If targeted HR zones could not be achieved during training, the rating of perceived exertion (RPE) scale42,43 was also used as a secondary measure of intensity, with targeted ratings of 15 to 17 (“hard” to “very hard”) for the high-intensity LT protocol and 11 to 13 (below “somewhat hard”) for low-intensity LT protocol.17,26,35
The primary goals of stepping practice during both high- and low-intensity LT included (1) maximizing successful stepping practice in a specific direction (eg, forward, backward, sideways), (2) achieving specific aerobic intensities (high or low), and (3) increasing difficulty of skilled walking tasks as tolerated. Each session was composed of 4 different stepping tasks practiced over ~10 minutes per session, including speed-dependent treadmill training, skill-dependent treadmill training, overground training, and stair climbing (also see appendix in Holleran et al 36 ). Speed-dependent treadmill training was focused on walking forward on a treadmill while maintaining targeted HR or RPE ranges. Limb swing assistance, body weight support, and nylon straps stabilizing the pelvis were provided only as needed to ensure successful stepping, characterized by positive step lengths, lack of stance-phase limb collapse, and sagittal/frontal plane stability. Skill-dependent treadmill training was performed by applying perturbations to challenge postural stability, propulsion, and limb swing during treadmill walking, and included stepping in multiple directions, over inclines and obstacles, with limited handrail use as tolerated. Additional loads (weighted vest or leg weights) or resistance (posterior elastic forces at the trunk or thighs) we applied as necessary to reach the targeted intensities while focusing on specific biomechanical gait components (stability, propulsion, limb swing). Perturbations were applied such that 2 to 5 different stepping tasks were repeated every 10 minutes. Overground training focused on speed- or skill-dependent locomotor activities similar to those described above, with use of a gait belt or overhead suspension system for safety. Additional stepping activities included walking over uneven or narrow surfaces and stepping around obstacles. Stair climbing was performed over static or rotating stairs (Stairmaster, Vancouver, WA) with attempts to use reciprocal gait patterns and progression to higher speeds and reduced hand rail use as able. If the HR/RPE was outside the targeted range, the loads carried or walking speeds were manipulated to alter the neuromuscular demands of walking. Stepping activity during each session was measured using accelerometers on the ankle of the more impaired limb (StepWatch, Modus, Washington DC).
Outcomes
Participants were assessed prior to and following each 4- to 6-week training paradigm. Primary measures included the 6-minute walk test (6MWT) distance and peak treadmill (TM) speed, 44 with simultaneous collection of cardiorespiratory function using a portable indirect calorimetry system (K4b2, CosMed, Chicago, IL). The 6MWT has previously been shown to be sensitive to the effects of aerobic training in patients poststroke. 33 In addition, peak TM speed often improves with high-intensity activities in both stroke and iSCI.30,32 The 6MWT was performed by blinded assessors, with instructions to “cover as much ground as possible.” Bracing and use of assistive devices were consistent with participants’ preferences during community mobility and were identical at all assessments. Peak TM speed was evaluated during a modified graded TM test, during which individuals began walking on a motorized TM at 0.1 m/s for 1 minute with speed increased by 0.1 m/s every minute until the subject experienced significant gait instability, could not continue walking at that speed, or requested to stop. Patients wore a safety harness during training, and cardiorespiratory data were collected during testing. Specific measures included the rate of O2 consumption (VO2, mL O2/kg/min), which was collected on a breath-by-breath basis, with HRs evaluated throughout and documented each minute, and blood pressure measured immediately prior to and following testing. All participants wore a safety harness without weight support. Peak TM speed was the highest speed achieved for 1 minute.
Secondary blinded clinical measures included: walking speed over short distances at self-selected speeds (SSS) and fastest-possible speeds (FS; GaitMat, Equitest Inc, Chalfont, PA); the Berg Balance Scale (BBS); and, the Lower Extremity Motor Score (LEMS). Secondary metabolic measures were not blinded and included measures of VO2 during the graded TM test and 6MWT. Peak metabolic capacity (VO2peak) was calculated as the average VO2 achieved over the last 30 seconds of the peak TM speed. Gait efficiency was estimated by comparing VO2 at the highest matched treadmill speeds from pre- to posttesting (VO2 match). In addition, comparisons of VO2peak and VO2match at posttesting (VO2peak-match) were calculated as a more precise estimate of combined changes in metabolic capacity and efficiency that may be better correlated with walking outcomes. 26 For overground measures, gait economy, or the cost of transport (O2cost, ml O2/kg/m), was evaluated during the 6MWT, and calculated by averaging data from the last 3 minutes of the 6MWT; this measure reflects the rate of O2 consumption per unit distance, and has been shown to improve under certain training conditions.32,45
Analysis
Training parameters collected included total number of sessions and average steps/session, with measures of training intensity (ie, RPE and HR) documented every 5 minutes. The average peak HR/session (reported as %HRmax), and average peak RPE/session were specific measures of intensity during each session.
For statistical analysis, data were analyzed on-protocol versus intent-to-treat to evaluate the specific effects of manipulating LT intensity. Data are presented as mean ± standard deviation in the text with standard error in the figures. One-sample Kolmogorov-Smirnov tests were used to determine normality for primary and secondary outcomes, with all measures with normal distributions except O2cost. Outcomes assessed immediately prior to and following each training intervention were of primary interest to understand the relative contribution of LT intensity to observed changes in locomotor dysfunction. Statistical analysis of primary outcomes (peak TM speed, 6MWT) for the crossover investigation were performed using a mixed-model analysis of variance (ANOVA), with primary main effects of time (prior to and following each LT period, repeated), order (high-intensity first or second), and LT intensity (high or low, repeated). We were specifically interested in the significant main effects of time (pre- vs post-LT) and interaction effects of time × intensity, and time × intensity × order. Bonferroni corrections were made for multiple comparisons for the primary measures of 6MWT and peak TM speed (adjusted α = 0.025). Considering the potential carry-over effects of the crossover design, we also performed a separate analysis of the initial parallel-group randomization, evaluating differences in outcomes following the first training intervention, without the second training epoch considered. These latter analyses also used a mixed-model ANOVA with primary main effects of time (pre-LT vs post-LT, repeated) and training intensity (high vs low). All outcomes of the second training period are presented in Table 2, although outcomes that were significant for the initial 3-way ANOVA are highlighted in the text.
Similar analyses were performed for secondary clinical measures, with Bonferroni corrections determined separately for the 4 clinical measures (SSS, FS, BBS and LEMS; adjusted α = 0.0125). Additional differences for secondary metabolic measures included, VO2peak, VO2match, VO2peak-match and gait economy (O2cost) during the 6MWT, with similar Bonferroni corrections.
Potential associations between the ability to achieve targeted intensities were compared with demographics or baseline assessment, and to changes in locomotor outcomes were evaluated using Pearson and Spearman’s correlation analyses as appropriate. Specific differences in training intensities were calculated by subtracting the average peak HR or RPE throughout high- vs low-intensity training (ie, ΔHR = average HR during high-intensity LT vs average HR during low-intensity LT) with differences in changes in outcomes following each training paradigm (ie, the differences in the change scores for specific outcomes following high- vs low-intensity LT; eg, Δ6MWT prior to and following high-intensity – Δ6MWT prior to and following low-intensity). In addition, specific changes in secondary metabolic or non-walking measures were compared with changes in primary or secondary locomotor outcomes to evaluate potential mechanisms underlying the results.
Results
Seventeen of 19 individuals initially consented for the study fulfilled inclusion criteria and were randomized, although only 15 individuals were able to complete all training; 1 individual terminated his participation due to increased back pain during low-intensity training, and another did not tolerate high-intensity LT. Seven subjects who completed training were randomized into the high-intensity LT protocol first (8 into low-intensity first). No significant adverse events were noted in subjects who completed both training paradigms. The flow diagram for patients enrolled is provided in Figure 1, with demographic and clinical characteristics of those who completed both training protocols provided in Table 1.
Demographics and Baseline Characteristics (C, cervical; T, thoracic).
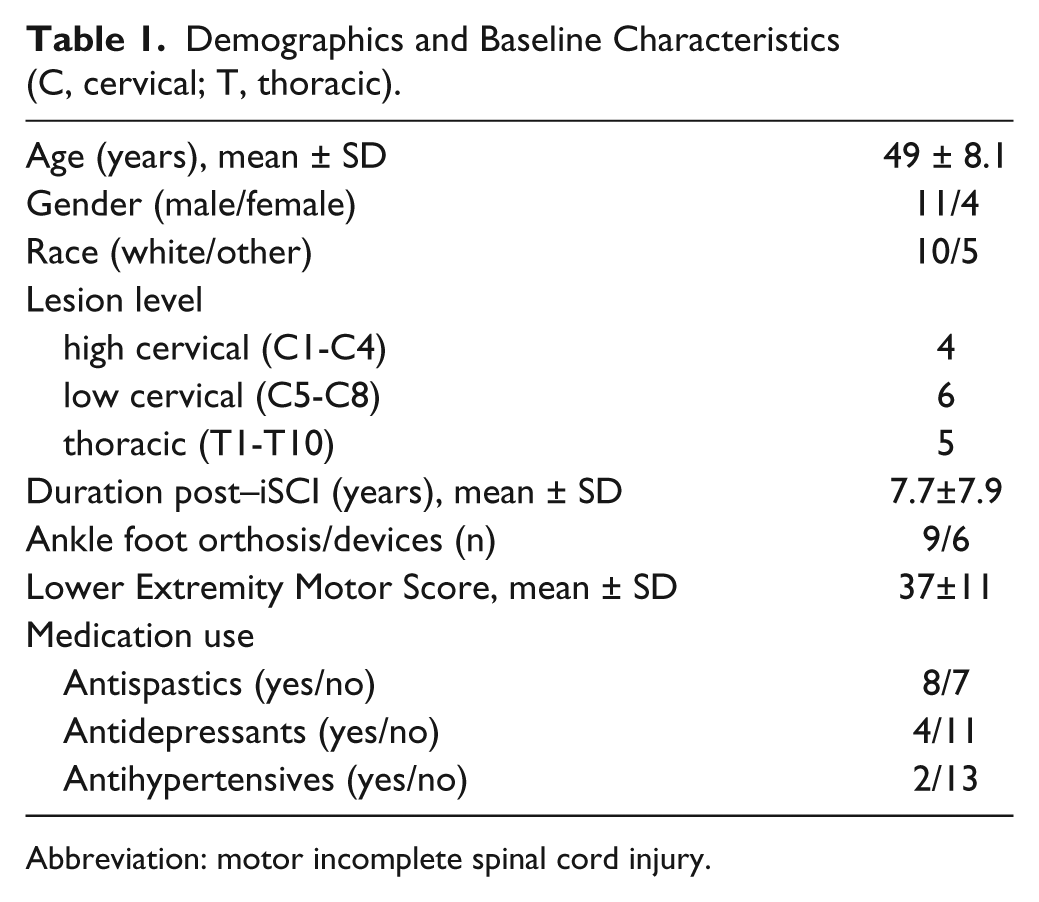
Abbreviation: motor incomplete spinal cord injury.
Training Parameters
The average number of sessions completed (19 ± 2.3 vs 18 ± 2.5 sessions, P = .91) and number of steps within sessions (2143 ± 1052 vs 1797 ± 722 steps/session, P = .12) were not significantly different between high- versus low-intensity training. Average peak HRs achieved during each session were different between groups, with high-intensity training achieving average HRs of 70% ± 12% HRmax and low-intensity LT reaching 60% ± 11% HRmax (10% ± 6% HRmax difference; P < .01). Despite these differences, the targeted intensities were difficult to achieve in selected patients; 5 subjects were unable to reach within 5% of the targeted high-intensity HR range (range: 48%-65%) and 3 subjects achieved higher HRs during low-intensity training than desired (72%-80%HRmax). For the former group unable to achieve high-intensity ranges, increases in speed or added resistance/assistance failed to increase HR sufficiently to reach the target zones. In the latter group with higher HRs greater than the targeted low-intensity range, reducing speed or providing assistance did not lower HR responses, and stepping was continued at a substantially decreased speed. Nonetheless, average RPEs during high- versus low-intensity LT were 16 ± 1.4 and 13 ± 1.1 (P < .01), respectively, and within targeted ranges. In addition, there was a low but significant correlation between HRs and RPEs (r = 0.48, P = .02), although measures of intensity were not significantly correlated to demographic variables or baseline clinical measures. However, those with HRs higher than the targeted ranges were more impaired subjects (LEMS range, 9-32; BBS range, 5-14), while those with blunted HR responses all presented with iSCI above C5 levels.
Primary and Secondary Outcomes
Assessment of primary outcomes revealed significant differences following high- versus low-intensity LT. Significant main effects of time (P < .01) but not time × intensity interactions were observed for 6MWT (changes following high- vs low-intensity LT: 26 ± 27 vs 14 ± 30 m; P = .16; Figure 2A and Table 2). For peak TM speed, however, main effects of both time and time × intensity interactions were significant (0.18 ± 0.14 vs 0.02 ± 0.02 m/s, P = .02 and P < .01, respectively; Figure 2B). No significant interaction effects of order were observed for either measure (both Ps > .30). Statistical analysis of the initial parallel-group only (ie, excluding the crossover training) revealed significantly greater gains in peak TM speed following high- vs low-intensity training performed first (0.21 ± 0.13 vs 0.00 ± 0.12 m/s, P < .01; Table 2) with similar gains following the second training period (0.15 ± 0.14 vs 0.03 ± 0.10 m/s). There were no significant differences between changes in 6MWT following lower vs high intensity training performed first (Table 2).
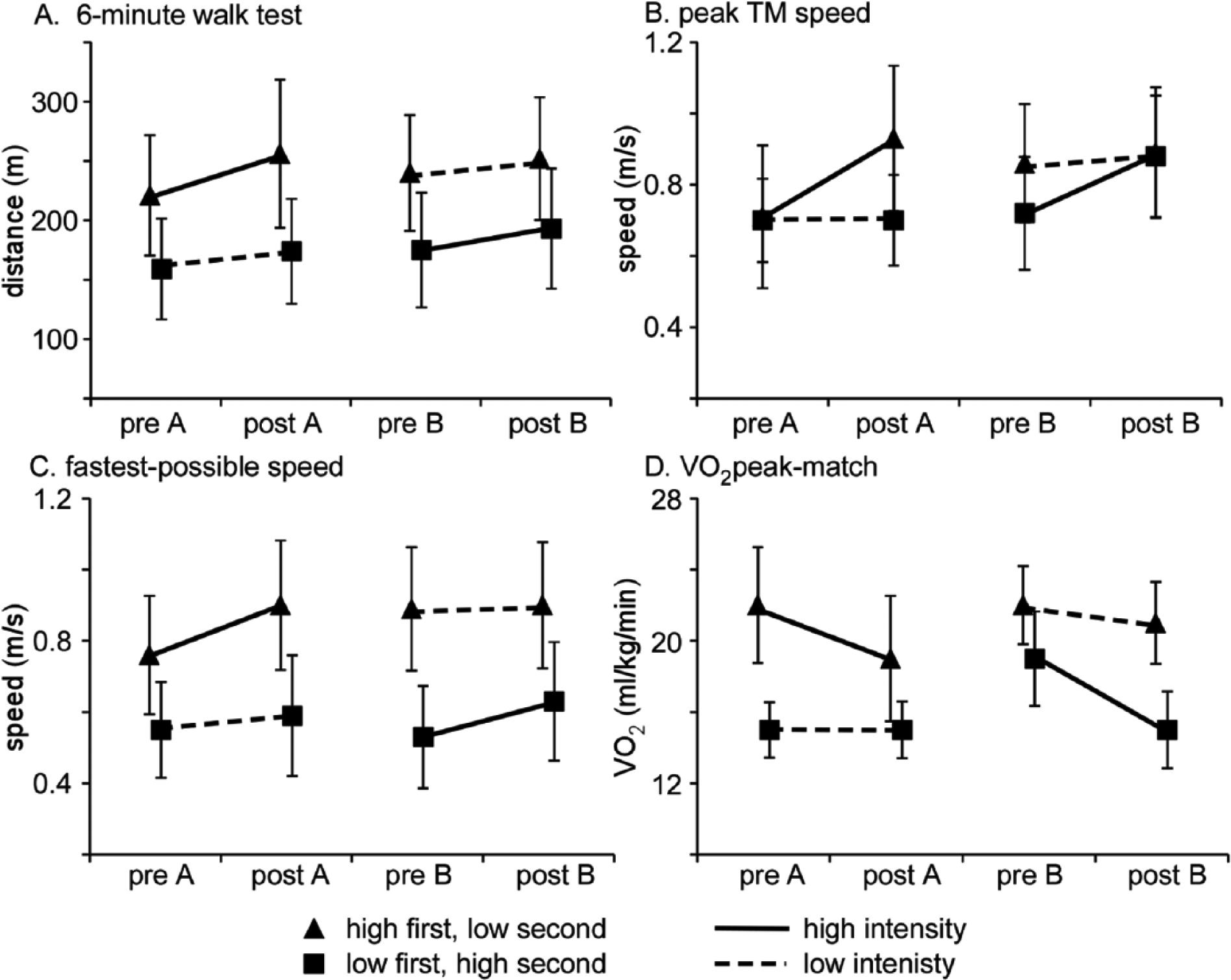
Differences in primary locomotor outcomes of (A) 6-minute walk test (6MWT), (B) peak treadmill (TM) speed, and secondary outcomes of (C) self-selected speed (SSS) and (D) fastest-possible speed (FS); pre-A and post-A indicated pre- and post-training performed first; pre-B and post-B indicated second training conditions; dark lines indicate high-intensity training, dashed lines indicate low-intensity training, triangle symbols denote high-intensity training performed first, low-intensity second; squares denote low-intensity first, high-intensity second.
Pretraining and Posttraining data for High- Versus Low-Intensity Training. a
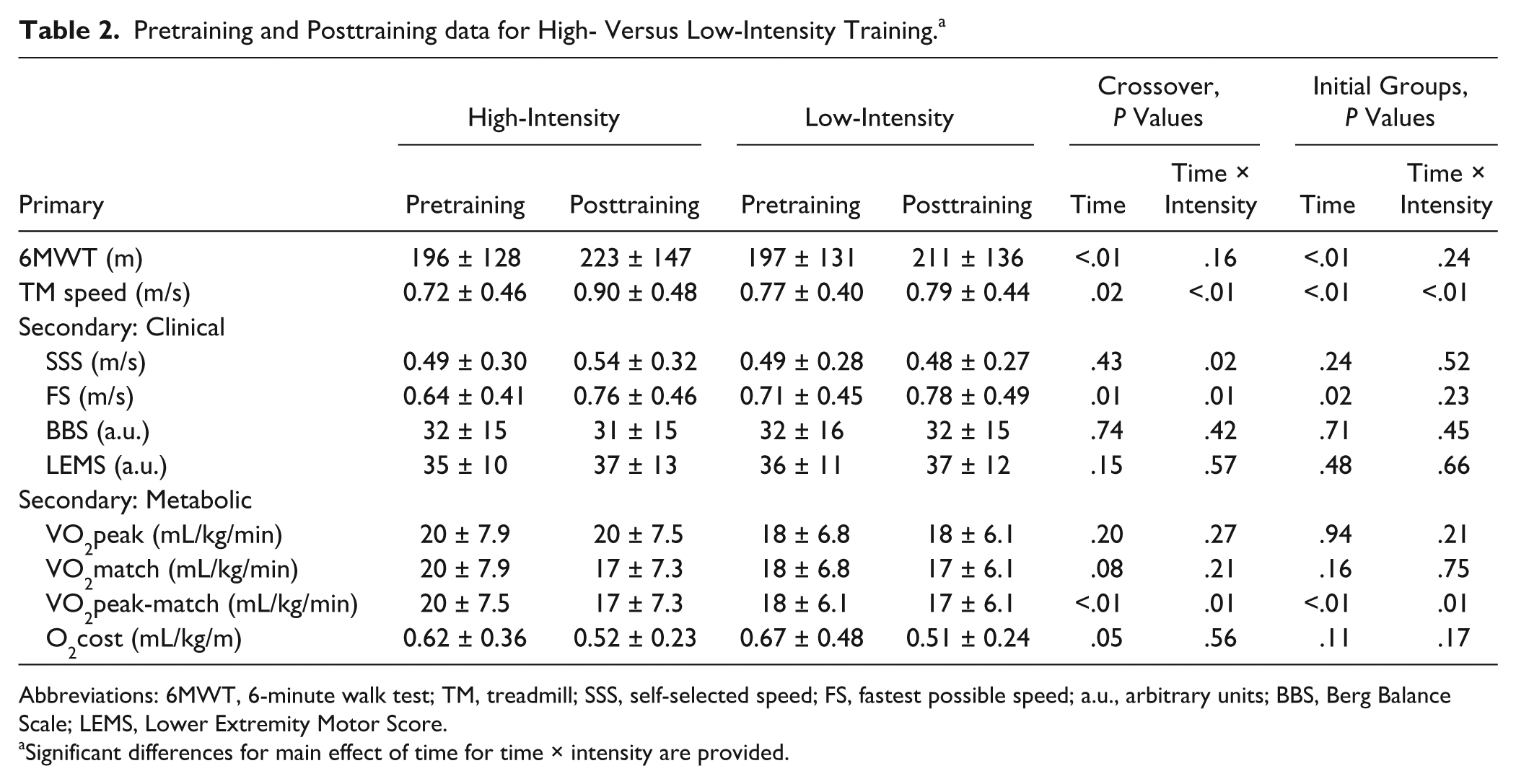
Abbreviations: 6MWT, 6-minute walk test; TM, treadmill; SSS, self-selected speed; FS, fastest possible speed; a.u., arbitrary units; BBS, Berg Balance Scale; LEMS, Lower Extremity Motor Score.
Significant differences for main effect of time for time × intensity are provided.
For secondary clinical outcomes, significant main effects of time and time × intensity interactions were observed for FS (Figure 2C; 0.12 ± 0.10 vs 0.03 ± 0.13 m/s, P = .01; Table 2), with a trend for significant time × intensity interactions for SSS (0.04 ± 0.08 vs −0.01 ± 0.07 m/s; P = .02). No significant main or interaction effects were observed for BBS or LEMS. Analysis of secondary clinical measures for the initial training groups reveal no significant time × intensity interactions for FS (0.14 ± 0.11 vs 0.05 ± 0.14 m/s, P = .23), or SSS (0.04 ± 0.10 vs 0.01 ± 0.05 m/s, P = .52). For both measures, however, similar changes were observed following the second training period (FS, 0.10 ± 0.09 vs 0.02 ± 0.12 m/s and SSS, 0.05 ± 0.07 vs −0.03 ± 0.09 m/s).
Analysis of secondary metabolic outcomes revealed no significant differences for VO2peak or O2cost for the time × intensity interaction, although main effects of time for VO2match and O2cost approached significance (P = .08 and .05). However, combined changes of both changes in peak metabolic capacity and efficiency (ie, VO2peak-match; Figure 2D) revealed significant main effects of time (P < .01) and time × intensity interactions (P = .01) favoring high- versus low-intensity training (2.2 ± 1.9 vs 0.37 ± 2.0 mL O2/kg/min). Analysis of the initial training conditions without the crossover also revealed significant between-group differences (2.6 ± 1.7 vs −0.22 ± 2.0 mL O2/kg/min, P = .01), although smaller differences were observed in changes in VO2peak-match during the second training period (1.9 ± 2.1 vs 1.1 ± 1.8 mL O2/kg/min). No significant interaction effects of order were observed for any secondary measure.
Correlation Analyses
Correlation analyses were performed to compare differences in HR and RPE during high- vs low-intensity training (eg, average %HR max during high-intensity − average %HR max during low-intensity; or ΔHR) to differences in outcomes during each training condition (eg, Δ6MWT following high-intensity – low-intensity). For primary outcomes, Figure 3A demonstrates the significant correlation between differences in Δ6MWT following high- and low-intensity training and Δ%HR during each training episode (P = .03), whereas similar correlations were not significant for peak TM speed (Figure 3B). Secondary locomotor measures of ΔSSS (P < .01) and ΔFS (P = .03) were also significant (Figure 3C and D). In addition, significant associations were observed between ΔRPE versus Δ6MWT (r = 0.53, P = .03) and versus ΔFS (r = 0.85, P < .01).
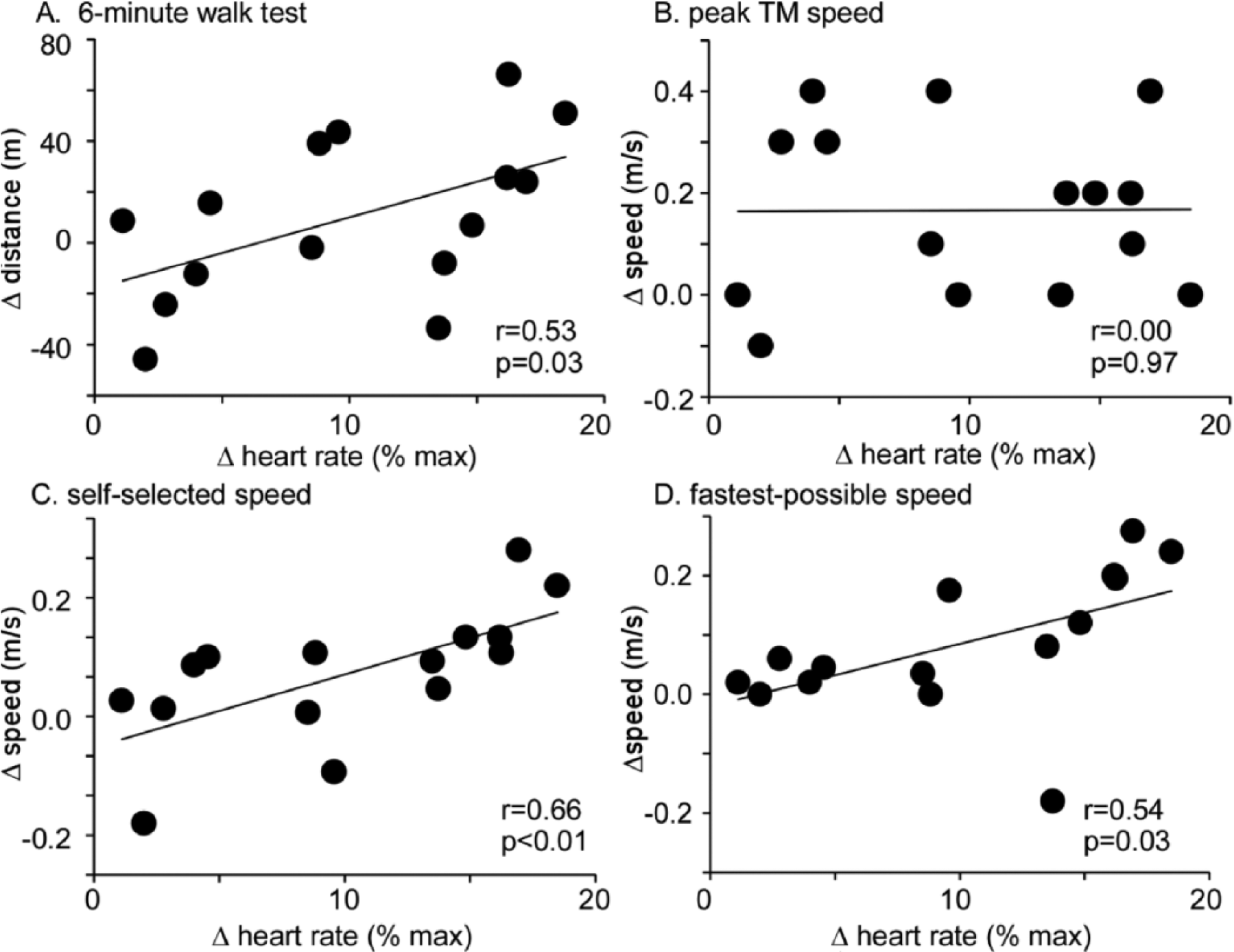
Correlations between differences in changes (Δ) for selected outcome measures (ie, Δ6MWT indicates differences in changes observed following high-intensity LT versus changes following low-intensity LT, change in 6MWT) versus differences in training intensity (%HRmax) between high- and low-intensity conditions: (A) Δ6MWT, (B) Δpeak TM speed, (C) ΔSSS, and (D) ΔFS during high- versus low-intensity training. Significant differences were observed for Δ6MWT, ΔSSS, and ΔFS (all Ps < .05). 6MWT, 6-minute walk test; LT, locomotor training; TM, treadmill; HR, heart rate; SSS, self-selected speed; FS, fastest possible speed.
Gains in locomotor outcomes were also compared to changes in primary impairments (strength, balance, metabolic function). Changes in BBS and LEMS were unrelated to gains in primary or secondary locomotor outcomes (all rs< 0.30, P > .05). While most measures of changes inVO2peak and VO2match were also not related to gains in locomotor function, a significant negative correlation was observed between differences in ΔSSS and ΔVO2match (r = −0.40; P = .03). In addition, ΔVO2peak-match demonstrated significant correlations between ΔSSS (r = 0.42; P = .02) and Δpeak TM speed (r = 0.62; P < .01).
Discussion
The primary findings of this study indicate high-intensity LT elicited greater gains in selected locomotor and metabolic outcomes than low-intensity LT in individuals with chronic iSCI. Significantly greater improvements in peak TM speed, FS, and VO2peak-match were observed following high-intensity training, while changes in SSS and 6MWT approached significance. In addition, moderate to strong correlations were observed between differences of the observed changes in 6MWT, SSS, and FS following high- versus low-intensity protocols and differences in LT intensities (HR and RPE). The combined data suggest the intensity of stepping protocols may influence walking function in patients with chronic iSCI, without differences in stepping amount or number of sessions.
The present findings are consistent with previous studies in patients poststroke that evaluated the effects of intensity of stepping exercise on walking outcomes.17,18 In those studies, high-intensity stepping training limited to forward treadmill and overground walking elicited greater gains in 6MWT than lower intensity LT even with attempts to match total workload (distance) or amount of stepping practice. In the present study, the duration and number of training sessions were similar between groups, although differences in measures of intensity were different. Previous studies in patients with iSCI have not attempted to evaluate the specific effects of LT intensity while controlling for the type and duration of task practice. Rather, most investigations focus on manipulating the type of walking interventions provided,10,12-14 with limited information on amount and intensity of training (see, however, Alexeeva et al 46 ). An important exception is a recent study by Yang and colleagues 11 that measured stepping activity and intensity during endurance (ie, treadmill) versus variable (skilled) LT. In that study, the authors reported ~3-fold greater stepping amounts and higher HRs during endurance versus variable training, which may have contributed to greater gains in 6MWT observed. The present study further supports the contributions of LT intensity as a substantial contributor to improved locomotor outcomes.
Despite the potential influence of LT intensity on the observed outcomes, the mean difference in stepping amounts and %HRs were smaller than expected. For stepping activity, smaller differences between training groups could be due to increased loads or resistance applied to the trunk or limbs to increase HRs. For stepping intensity, however, peak HRs were separated by ~10% predicted HR (70 vs 60% during high- vs low-intensity LT), whereas previous studies manipulating LT intensity in patients poststroke revealed greater HR differences (18 %HR differences). 35 The relatively smaller difference was highlighted by blunted HR responses in selected participants regardless of training intensity, and by others with greater HRs than the targeted low-intensity range. Altered HR responses may be due to factors related to the injury (ie, altered autonomic function), lack of mobility and deconditioning following injury, or individual variations that existed prior to the iSCI. Caution may be warranted in specific patients when targeted HR levels may not be attainable, and use of surrogate measures (RPE) may be appropriate. For example, specific differences between changes following high- and low-intensity training were associated with differences in RPE, and measures of either HR or RPE may be warranted to help differentiate LT intensity in patients with iSCI.
Considering the limitations in intensity measures, the statistically significant differences between training groups were not as large as expected. Specifically, changes in gait speed and endurance (6MWT) were below minimal detectable changes (MDCs) according to selected research, although other data suggest that the changes in SSS or FS were above minimally clinically important differences (MCIDS) for patients with neurological injury 47 (≥0.05 m/s for SSS or FS and ≥20 m for 6MWT). The lack of expected differences may be due to the chronicity or degree of injury of this patient population, or potentially the lack of ability to elicit greater differences in HR/RPE responses during high- versus low-intensity stepping. However, the present data nonetheless provide further evidence for the utility of intensity of stepping practice, consistent with previous studies involving patients poststroke.17,18
Potential mechanisms underlying the changes in locomotor performance following high- versus low-intensity LT are not clear but are likely multifactorial. Previous data suggest that high-intensity LT in individuals with stroke24,33 results in gains in VO2peak, which may contribute to improved walking function. In the present study, greater changes in VO2match vs VO2peak were observed following high- versus low-intensity LT, although was neither significant nor related to walking function. As in previous work, however, the combined gains in metabolic capacity and efficiency 26 (VO2peak-match) compensated for individual variations and demonstrated stronger associations with walking outcomes.
Given the larger changes in metabolic efficiency versus capacity, mechanisms underlying improved locomotor function in this study could be due to neuromuscular factors. Potential changes include improved neuromuscular coordination, which can be achieved through altered kinematic37,45 and/or muscle activation strategies48,49 (ie, reduced co-activation) to achieve faster speeds without large increases in VO2peak. However, previous training studies in patients with stroke48,49 and iSCI 37 suggest improved speeds without altered co-activation strategies, and alterations in gait kinematics may be a more likely contributor. Mechanisms underlying improved kinematic coordination deserves further study, but suggests altered neural strategies underlie the observed changes. Indeed, stepping training has been shown to elicit increases in supraspinal 50 and spinal circuits 51 that may contribute to locomotor improvements. These changes may be enhanced with high-intensity training, which can result in the synthesis and release of various trophic factors (eg, brain-derived neurotrophic factors, or BDNF; for review, please see Huang et al 52 and Knaepen et al 53 ) that may facilitate neuroplastic alterations. 30 Many other neuromuscular factors could contribute to the observed changes, included altered muscle metabolism, and are of interest in future studies.
Limitations of this pilot study include the small sample size and lack of blinded assessors for the graded TM and metabolic testing, although future trials can use these findings to understand potential effect sizes observed with these interventions. In addition, the potential carryover effect of high-intensity training necessitated analysis of only the initial training groups, which revealed consistent significant differences in peak TM speed and VO2peak-VO2match. Despite significant changes in selected locomotor outcomes (peak TM speed and FS), effect sizes for differences in SSS (Cohen’s d = 0.67) and 6MWT (d = 0.36) indicate greater subject numbers (21 and 63 subjects, respectively) would be sufficient to obtain significant differences. The sample sizes required to obtain significant differences in some of these outcomes were larger for FS and SSS than those observed in the data from Yang and colleagues, 11 although our relative changes in 6MWT were certainly smaller. More work is required to evaluate the effects of training intensity in iSCI.
Conclusions
In summary, the present study details an initial to delineate the effects of intensity of locomotor practice in patients with motor iSCI, revealing significantly greater improvements following high- versus low-intensity training in individuals in selected locomotor variables and combined metabolic capacity and efficiency. More directly, stepping practice at lower intensities without substantial demands to neuromuscular and cardiopulmonary systems results in smaller changes in locomotor function. In the clinical setting, intensity of stepping exercise can be readily manipulated and indirectly monitored using cardiopulmonary and subjective measures, and may be recommended with further research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by National Institute of Health (R01-NS079751) and National Institute of Disability and Rehabilitation Research (H133N110014).