
Abstract
Background. About 75% of persons with ASIA (American Spinal Injury Association) Impairment Scale C and D incomplete spinal cord injury (SCI) achieve walking ability. Objective. To compare a walking reeducation program using Lokomat with conventional overground training among individuals with incomplete SCI of both traumatic and nontraumatic etiology. Methods. A total of 80 participants from 3 to 6 months after onset admitted to 1 site for rehabilitation were included in a single-blind randomized clinical trial of 2 parallel groups, with blind evaluation by independent observers. Patients received 40 walking reeducation sessions of equal time using a Lokomat program with overground practice or overground mobility therapy alone. Primary measurements of outcome were walking speed and the Walking Index for Spinal Cord Injury (WISCI II). Secondary outcomes were the 6-minute walk test, locomotor section of the Functional Independence Measure, Lower Extremity Motor Score (LEMS), Ashworth Scale, and Visual Analog Scale for pain. Results. No significant differences were found at entry between treatment groups. Walking speed for Lokomat (0.4m/s [0.6-0.2]) and overground therapy (0.3m/s [0.5-0.2]) groups did not differ. The WISCI II for the Lokomat group (16 [8.5-19]) was better than for overground therapy (9 [8-16]). The 6-minute walk test and LEMS displayed significant differences in favor of Lokomat therapy but were not corrected for multiple comparisons. Conclusions. Robotic-assisted training was equivalent to conventional walk training in patients with a variety of nonprogressive spinal cord pathologies for walking speed, but the need for orthotics and assistive devices was reduced, perhaps because of greater leg strength in the robotic group.
Keywords
Introduction
About 53% of traumatic spinal cord injuries (SCIs) are incomplete, and one of the principal goals for rehabilitation is recovery of walking ability.1,2 Approximately 25% of persons with incomplete traumatic SCI fail to become ambulatory.3-5 Manual and robotic-assisted body weight–supported treadmill training (BWSTT) is based on optimizing sensory inputs relevant to step training, repeated practice, and possible optimization of neuroplasticity. In uncontrolled studies by Werning et al 6 and Wirz et al 4 on acute and chronic individuals, within-subject improvements were found in walking ability using these techniques. Further studies with active control interventions versus manual 7 and robotic-assisted BWSTT 8 and BWSTT with electric functional stimulation9,10 were equivalent or inferior to overground practice. BWSTT for other neurological diseases has also not been better than conventional therapy.11,12 A Cochrane Library review 2 suggested insufficient evidence to decide whether one of these treatments for SCI is better than conventional interventions.
To address the ongoing uncertainty, we compared a walking reeducation program using the Lokomat system (mechanically assisted BWSTT) with conventional overground training. We hypothesized that (1) in incomplete recent SCIs, training with the Lokomat will yield greater functional recovery in terms of gait speed and pattern than does conventional training; and (2) walking reeducation programs using robotic-assisted BWSTT will yield improvements in physical condition in terms of walking endurance, greater muscular strengthening, and functional independence for walking than conventional overground training.
Methods
We conducted a clinical trial with a randomized, single-blind, parallel-group design. The assessors were blinded for treatment allocation and familiar with the test battery. This study was undertaken at the National Paraplegics Hospital (Hospital Nacional de Parapléjicos), a 210-bed, specialist SCI center. Prior approval for the study was obtained from the ethics and research committees.
Of all patients admitted from November 2006 to September 2008, we selected those who met the inclusion criteria outlined in Table 1. After the study participants had been selected and their demographic data and injury characteristics recorded (level, ASIA [American Spinal Injury Association] grade, 13 etiology, and time course), they were randomized to the Lokomat and conventional overground groups using a proper allocation concealment process by a centralized computer program. Baseline measurements of the outcome variables were taken before they underwent the intervention corresponding to the group to which they had been allocated. Patients were assessed on reaching 20 sessions, as representing the midpoint of the study, so that they could be evaluated on an intention-to-treat basis if they were unable to complete the training and on participating in the full 40 sessions of the treatment program. All outcome measures were evaluated by a person external to the study.
Inclusion and Exclusion Criteria
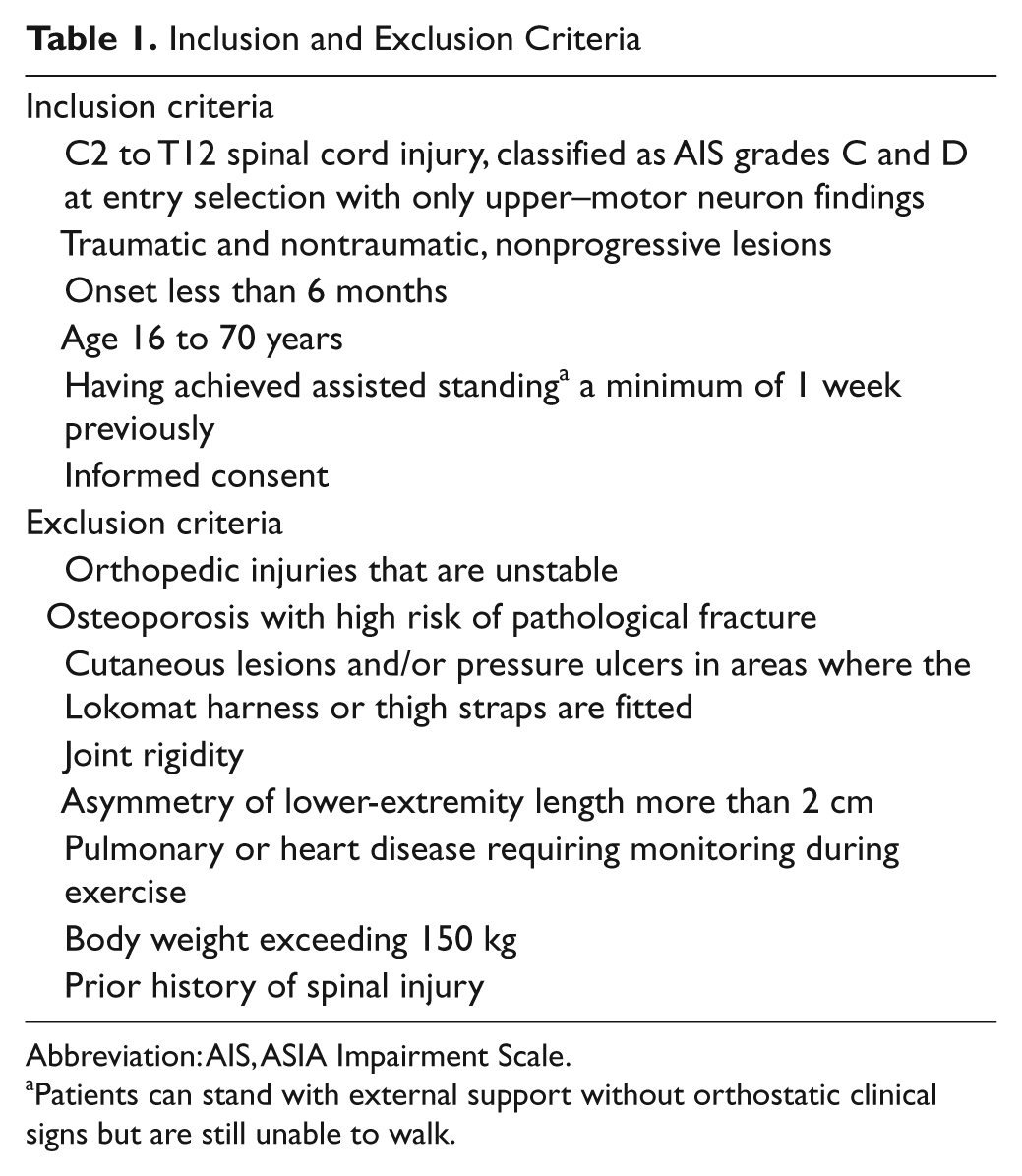
Abbreviation: AIS, ASIA Impairment Scale.
Patients can stand with external support without orthostatic clinical signs but are still unable to walk.
Intervention
All participants underwent the standard physical treatment program, based on daily sessions of joint mobilization below the level of the spinal injury, strengthening of supralesional musculature and remaining motor functions, muscle stretching and postural relaxation techniques to treat spasticity, and trunk stabilization and rotation work, and practice of self-care skills. Within this routine, the main component of their mobility training was 40 sessions (8 weeks) of either Lokomat or overground therapy for walking. They did not receive any formal training for walking other than during these sessions. The necessary orthoses were prescribed in accordance with the patient’s injury level and remaining motor functions and used to work on balance in bipedal locomotion, weight shift, and finally, body transfer. In both groups, the study patients underwent 40 walking training sessions of 1 hour duration; the Lokomat group completed 30-minute sessions with the Lokomat in each walking session. Before the intervention, none of the participants had trained with the Lokomat.
For treatment with the Lokomat system, the amount of body weight supported was initially set at 60% of each individual’s weight and then decreased in accordance with load tolerance, but not less than 25% support was provided. The speed selected was the one at which the patient worked most comfortably. Treatment sessions were in all cases conducted under the supervision of a trained physiotherapist.
Outcome Measures
The principal outcome variables were walking speed measured with the 10-meter walking test14,15 and type of gait support per the Walking Index for Spinal Cord Injury (WISCI II) Scale. 16 Of the various possibilities of undergoing the 10-m walking test, 14 exactly 10 m were taken into account for study purposes and were incorporated into the measurement of the acceleration and deceleration times that occurred at the extremes. When performing the test, each individual was allowed to use the necessary orthoses and technical aids and was asked to walk in a straight line at a comfortable pace to cover the distance. Individuals without walking ability were allocated a speed value of 0 m/s. The WISCI II scale is the revised version of the WISCI scale, 17 developed and validated for specific use in SCIs. Using this scale, patients were scored from 0 to 20, in accordance with the technical aids, orthoses, and assistance necessary for walking 10 m.
Among the secondary measures, we included walking endurance measured with the 6-minute walk test14,15; the walking and stairs tasks of the Functional Independence Measure Locomotor section (FIM-L),18,19 scored from 2 to 14; muscular strength of the lower limbs measured with the ASIA13,20 Lower Extremity Motor Score (LEMS) subscale (0-50); presence of spasticity measured with the Ashworth Scale (0-4) 21 ; and existence of pain measured with a Visual Analog Scale scored from 0 to 10.
Statistical Analysis
Walking speed was used as the outcome to estimate the statistical power of the present trial. Our pilot study showed a precision of ±2.79 s (95% CI) for difference between group means. Therefore, with 40 individuals per group, the trial has a statistical power of 80.1% for detecting statistical significance in the main outcome.
The associations between qualitative variables were assessed by using the χ2 or Fisher exact test, in the event that more than 25% of the expected values might be less than 5. Comparisons of means were performed using the Student t test for independent groups, applied if data were normally distributed. For nonnormally distributed ordinal scale outcomes, the medians between 2 arms of the study were tested by the median test. For determining the normality of the distribution, the Kolmogorov-Smirnov goodness-of-fit test was used. A significance value of 5% was accepted for all tests. We did not adjust for multiple comparisons in analyzing the secondary outcomes because we believe that the measurements are not independent. An explanatory logistic regression model was constructed, taking the intervention (training with the Lokomat system or conventional training) as the independent variable. We calculated the odds ratios of nonimprovement with the independent variable, conventional treatment, adjusted for the initial potential confounding variables, WISCI II, FIM-L, and LEMS.
Results
Flow Chart
All acute patients admitted to the National Paraplegics Hospital from November 2006 to September 2008 (n = 297) were assessed for eligibility (Figure 1). They had both traumatic and what were considered to be nonprogressive spinal cord lesions.

Flow char.
Randomization
Demographic and injury-related characteristics are shown in Table 2, along with the baseline results. No significant differences were detected in age, sex, injury level, ASIA grade, time course, or baseline measurements of results. The study groups were thus comparable.
Participant Baseline Characteristics a
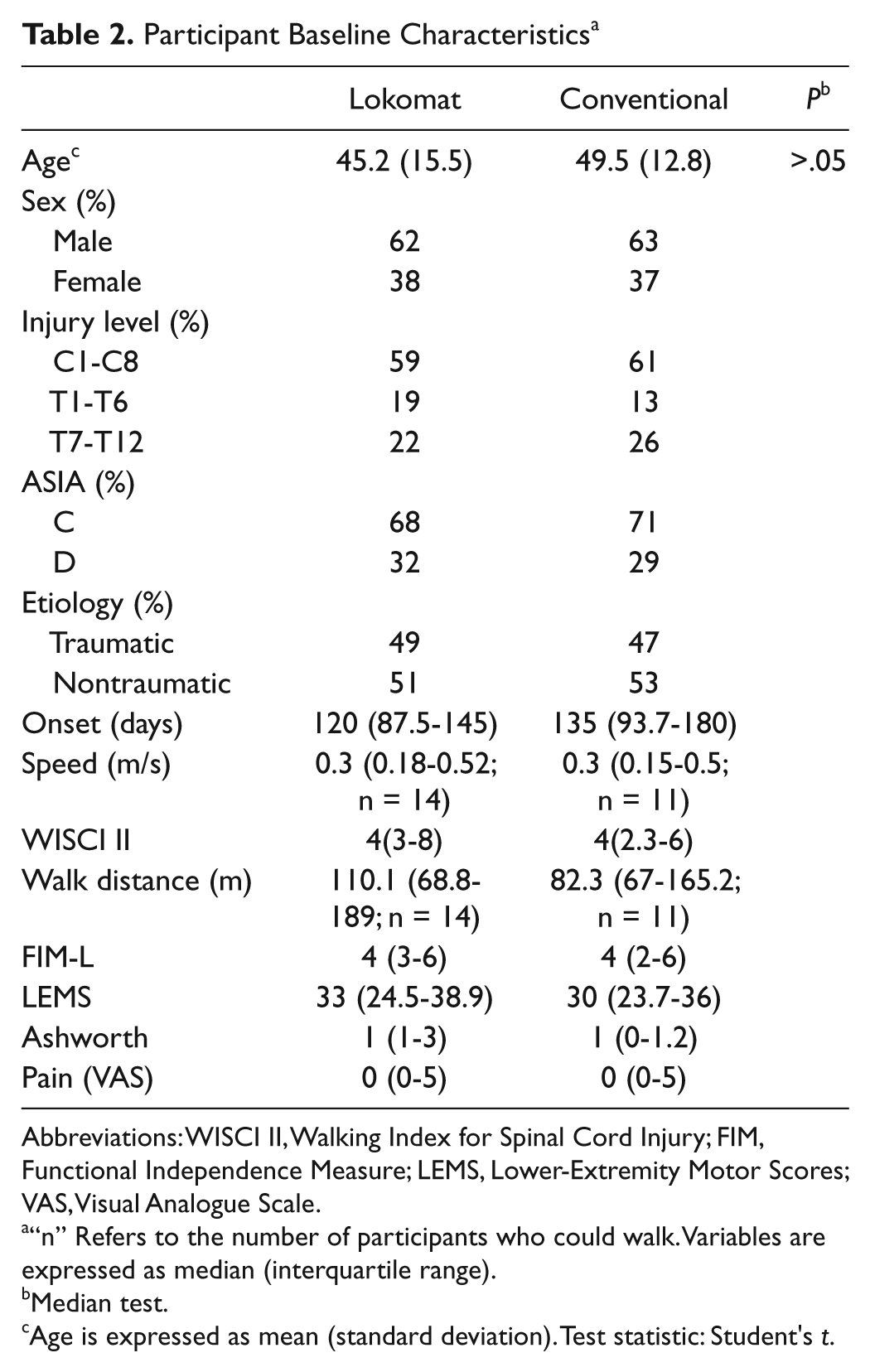
Abbreviations: WISCI II, Walking Index for Spinal Cord Injury; FIM, Functional Independence Measure; LEMS, Lower-Extremity Motor Scores; VAS, Visual Analogue Scale.
“n” Refers to the number of participants who could walk. Variables are expressed as median (interquartile range).
Median test.
Age is expressed as mean (standard deviation). Test statistic: Student's t.
Primary Outcomes
No statistically significant differences were found between the 2 groups for walking speed. For the WISCI II, however, a significant (P < .05) difference was found in favor of walking reeducation with the Lokomat (Table 3).
Comparative Analysis of Lokomat and Conventional Groups a
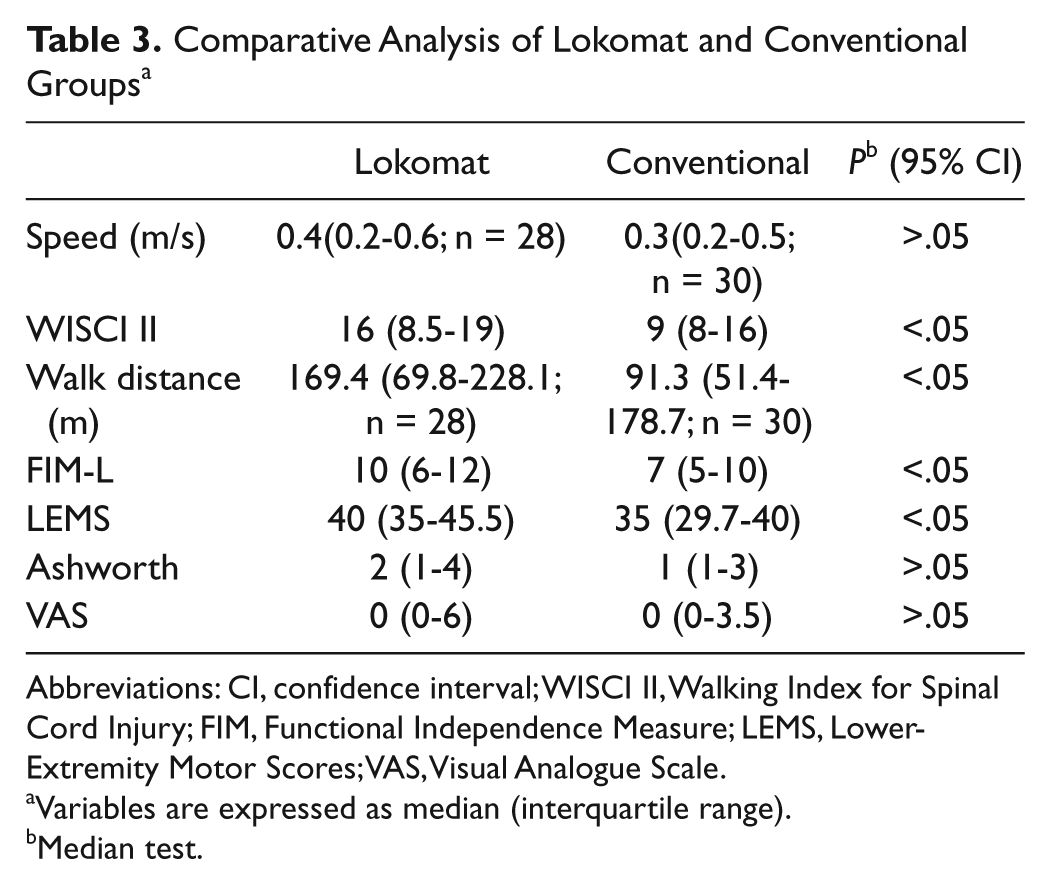
Abbreviations: CI, confidence interval; WISCI II, Walking Index for Spinal Cord Injury; FIM, Functional Independence Measure; LEMS, Lower-Extremity Motor Scores; VAS, Visual Analogue Scale.
Variables are expressed as median (interquartile range).
Median test.
Secondary Outcomes
The results for the secondary variables are in Table 3. Participants assigned to the Lokomat improved in the 6-minute endurance test, the FIM-L, and lower-limb strength.
Logistic Regression Analysis
Risk of nonimprovement with conventional overground treatment was significantly higher for the LEMS, but not the WISCI II and FIM. Tables 4 and 5 list the odds ratios and significance results for the LEMS and WISCI II.
Odds Ratios of Conventional Treatment in Nonimprovement of LEMS, Adjusting for Confounding Variables
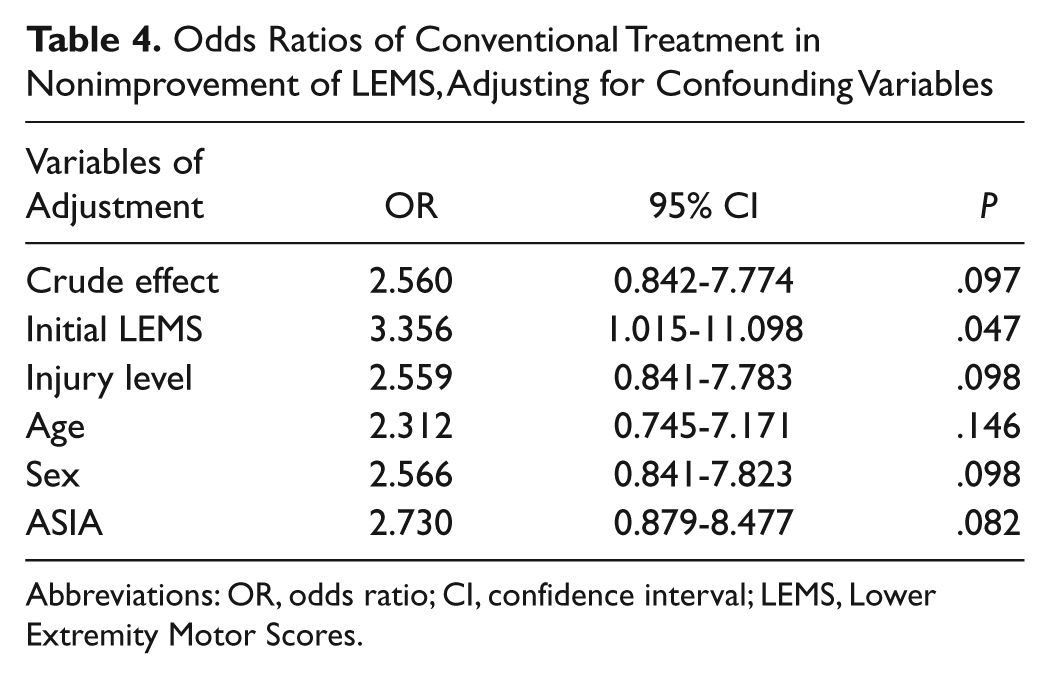
Abbreviations: OR, odds ratio; CI, confidence interval; LEMS, Lower Extremity Motor Scores.
Odd Ratios of Conventional Treatment in Nonimprovement of WISCI II, Adjusting for Confounding Variables
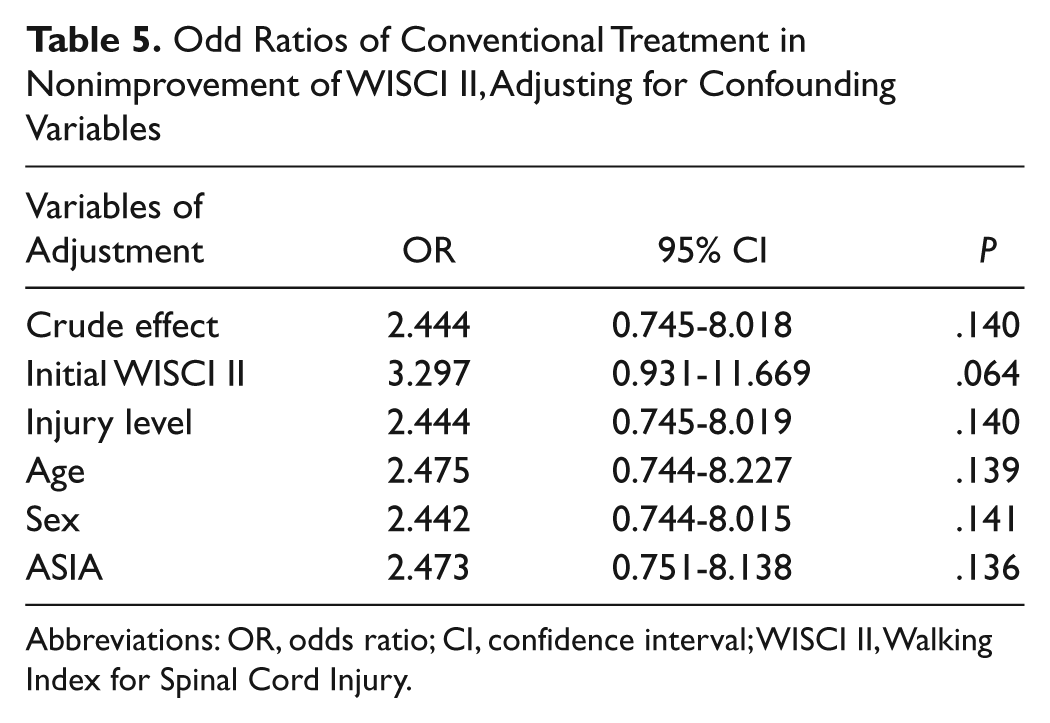
Abbreviations: OR, odds ratio; CI, confidence interval; WISCI II, Walking Index for Spinal Cord Injury.
Discussion
The study participants were selected from patients admitted to the National Paraplegics Hospital, a specialist SCI center. To conduct the research work, 2 groups were randomly constituted. The initial descriptive analysis of the demographic and injury-related characteristics and the baseline results of the principal and secondary study variables displayed no statistically significant differences, thereby confirming the success of the randomization and, by extension, the fact that the 2 groups were comparable.
Based on the WISCI II, 6 minute endurance test, FIM-L, and lower-limb strength as per the LEMS subscale, analysis of the results shows statistically significant differences in favor of walking reeducation with the Lokomat system. For the remaining variables—namely, speed measured with the 10-m walking test, spasticity assessed by the Ashworth scale, and pain assessed by the Visual Analog Scale—no differences were observed. The characteristics of the study sample made it necessary to use nonparametric tests with a lower statistical power as test statistics. This means that one cannot altogether rule out the possibility that the statistically significant differences found might have been caused by the existence of small nonsignificant differences between the 2 groups from the commencement of treatment. Consequently, the statistical work was completed with a logistic regression analysis, in which only the difference observed for the LEMS could be confirmed as significant and a trend toward significance was seen for the WISCI II. Lokomat training gains seems to be based on an increase of strength obtained with this kind of training.
In our study, ASIA Impairment Scale B and caudal lower motor neuron lesions were not included. Participants had traumatic and nontraumatic, nonprogressive lesions, so the sample differs from those of traumatic SCI, which may make it more representative of the incomplete myelopathy population for external validity. The average time since onset—more than 3 months—may suggest that spontaneous gains played a lesser role than training did.
In conclusion, although training with the Lokomat system improves walking ability in the case of incomplete motor SCIs of less than 6 months’ duration, the functional results achieved in terms of speed and quality of walking cannot be said to be better than those produced by a conventional overground training program. In our study, however, use of the Lokomat system yielded greater endurance for walking and better results in terms of lower-limb strength than did conventional reeducation. Our results do not afford a basis on which we can claim that this kind of training is better than traditional techniques. Variations in results found in the literature for robotic-assisted training are probably a result of factors such as differences in the patient population (type and severity of lesion, time of onset to entry, LEMS, etc), the devices used, application of the interventions, outcome measurements, and control interventions. Further well-designed trials with present and future robotic devices seem to be indicated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by a grant from FISCAM (Fondo para la Investigación Sanitaria en Castilla la Mancha) - AN/2006/27.