
Abstract
Background. A cardiac arrest can lead to hypoxic brain injury, which can affect all levels of functioning. Objective. To investigate 1-year outcome and the pattern of recovery after surviving a cardiac arrest. Methods. This was a multicenter, prospective longitudinal cohort study with 1 year of follow-up (measurements 2 weeks, 3 months, 1 year). On function level, physical/cardiac function (New York Heart Association Classification), cognition (Cognitive Log [Cog-log], Cognitive Failures Questionnaire), emotional functioning (Hospital Anxiety and Depression Scale, Impact of Event Scale), and fatigue (Fatigue Severity Scale) were assessed. In addition, level of activities (Frenchay Activities Index, FAI), participation (Community Integration Questionnaire [CIQ] and return to work), and quality of life (EuroQol 5D, EuroQol Visual Analogue Scale, SF-36, Quality of Life after Brain Injury) were measured. Results. In this cohort, 141 cardiac arrest survivors were included. At 1 year, 14 (13%) survivors scored below cutoff on the Cog-log. Both anxiety and depression were present in 16 (15%) survivors, 29 (28%) experienced posttraumatic stress symptoms and 55 (52%), severe fatigue. Scores on the FAI and the CIQ were, on average, respectively 96% and 92% of the prearrest scores. Of those previously working, 41 (72%) had returned to work. Most recovery of cognitive function and quality of life occurred within the first 3 months, with further improvement on some domains of quality of life up to 12 months. Conclusions. Overall, long-term outcome in terms of activities, participation, and quality of life after cardiac arrest is reassuring. Nevertheless, fatigue is common; problems with cognition and emotions occur; and return to work can be at risk.
Introduction
There is concern that the increasing success of cardiac resuscitation in the community, secondary to lay people’s involvement (bystander CPR) and the use of automated external defibrillators (AEDs), may be associated with increasing numbers of people left with hypoxic brain damage.1-4 Although recent studies have shown that global neurological outcome appears to be good in the majority of survivors, the validity and sensitivity of the commonly used Cerebral Performance Categories can be questioned.5-7 In fact, many studies using more specific instruments have found a high prevalence of problems after cardiac arrest, including cognitive impairments,8,9 emotional problems, 10 and/or fatigue 11 —problems that are probably related to the hypoxic brain damage that arises from disrupted cerebral circulation. 4 In addition, daily functioning and participation in society, including return to work, are also adversely affected.12,13 In contrast to these reported problems, a systematic review on quality of life described that most survivors experience a relatively good quality of life. 14
The interpretation of the various studies is complicated by the wide variation in investigated domains of functioning, measurement instruments used, and study designs. An integrated view on overall outcome after cardiac arrest, which takes all aspects of functioning into account, is lacking.
The main goal of this study was to investigate outcome at all levels of functioning during the first year after survival of a cardiac arrest. In this project, the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization was used as a framework to describe outcome after cardiac arrest, complemented by the concept of quality of life.15,16 We expected that problems could occur on all domains of functioning, but that the ICF levels of functions (cognition, emotions, and fatigue) and participation would be most frequently affected.9-13
Second, we analyzed the pattern of recovery after cardiac arrest and examined whether there were improvements throughout the first year. Most of the recovery was expected to occur within the first months because this is the common pattern of recovery after nonprogressive neurological diseases such as stroke. 17
Methods
Design
This study was part of a larger project, “Activity and Life after Survival of a Cardiac Arrest” (ALASCA; ISRCTN74835019). 18 The ALASCA project consisted of a multicenter prospective longitudinal cohort study (n = 238) with a nested randomized controlled trial (RCT, n = 185). In the RCT, we evaluated the effect of a new nursing intervention and found it to be effective.18,19 As the goal of the current analysis was to examine natural recovery after a cardiac arrest, we excluded patients who were randomized into the intervention group of the RCT (n = 97) from the analysis of the current cohort study. This resulted in the current cohort of 141 patients (=238 − 97), who received usual care only, best reflecting natural recovery after cardiac arrest.
For the project as a whole, the percentage of patients who refused to participate was 29%, and the main reasons for refusing were lack of time/too much burden, lack of interest, and medical problems.
Setting
Patients were recruited from the coronary care units and intensive care units of 7 hospitals in the southern part of the Netherlands between April 2007 and December 2010. The participating hospitals serve approximately 1 million inhabitants. All the hospitals had protocols for care of resuscitation patients in line with international guidelines and performed induced hypothermia and pacemaker implantations. 20
Participants
Inclusion criteria for registration were the following: survival more than 2 weeks after an in-hospital or out-of-hospital cardiac arrest, living within 50 km of one of the participating hospitals, age 18 years or older, and sufficient knowledge of the Dutch language. Patients with a life expectancy of less than 3 months as a result of another medical condition, as estimated by their treating physician, were excluded from the register.
Procedure
Newly admitted survivors of cardiac arrest were assessed for eligibility, and potential participants were approached between 3 and 10 days after their cardiac arrest. Patients who decided to participate signed an informed consent form. If the patient did not have the capacity to consent, the caregiver was asked for provisional consent until the patient had the capacity to decide. Baseline measurements were planned 2 weeks after the cardiac arrest, with follow-up at 3 and 12 months. Research assistants visited the patients at their homes to perform the measurements. There were no procedural differences between the hospitals.
This study complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Maastricht University Medical Centre, the Netherlands.
Outcome Measures
Medical variables were registered during hospital admission, and sociodemographic data were collected at the initial assessment. Figure 1 presents the ICF model, which describes the impact of a health condition on 3 levels of functioning—(1) functions, (2) activities, and (3) participation—as well as the measurement instruments used to assess these different levels of functioning. We added quality of life to the ICF model to complete the overall view on outcome. 16 Quality of life can be affected by all levels of the ICF model and is considered the person’s own assessment of his or her situation.
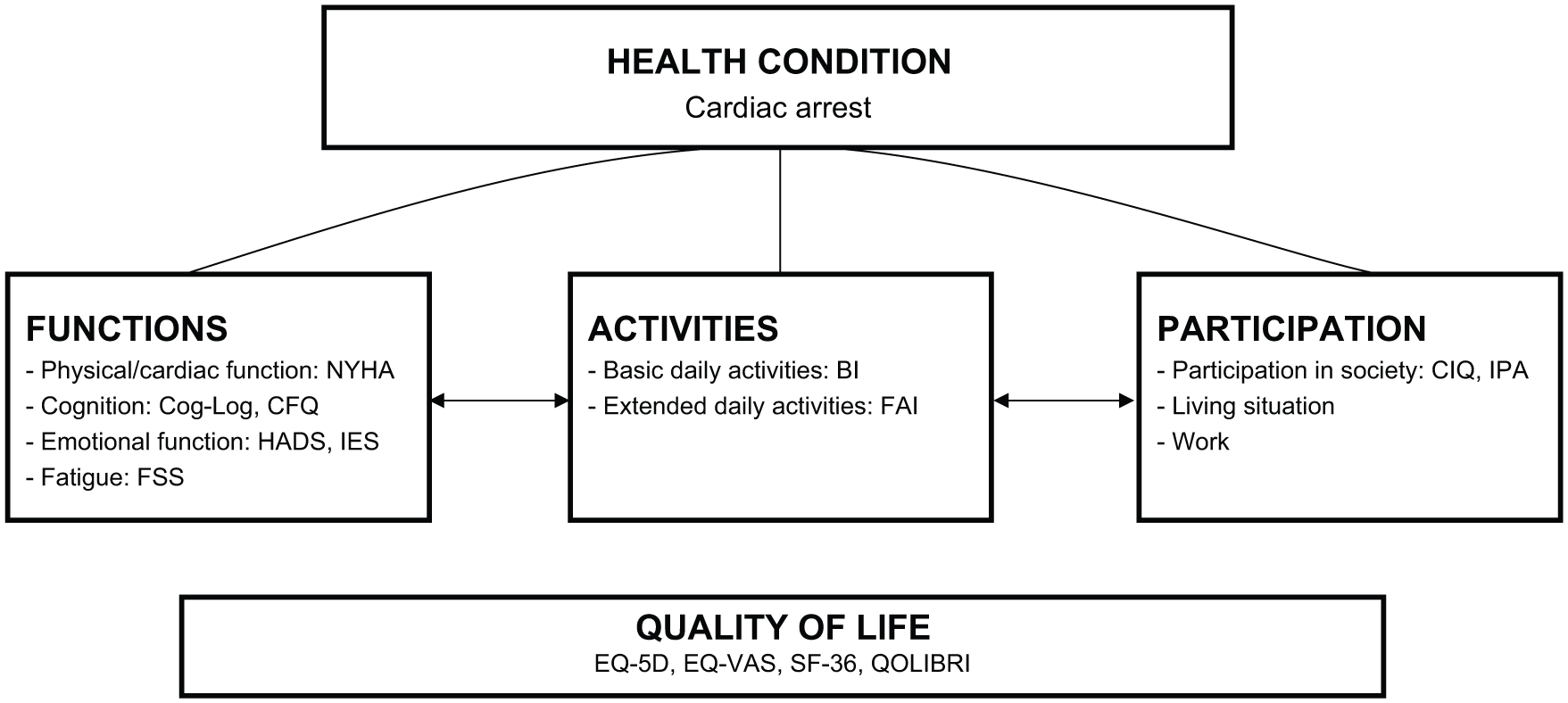
ICF model and measurement instruments used.
Function Level
The New York Heart Association Classification (NYHA classification) is a functional classification system that divides cardiac patients into 4 classes depending on their limitation in physical activities. 21 Higher scores indicate more limitations. A score NYHA ≥3 was considered abnormal.
The Cognitive Log (Cog-Log) is a 10-item cognitive screening instrument. It measures higher neurocognitive processes, including orientation, memory, concentration, and executive skills. Scores can range from 0 to 30, with higher scores representing better cognitive function; scores <25 were considered impaired. 22 The Cognitive Failures Questionnaire (CFQ) is a 25-item questionnaire on self-reported cognitive failures, resulting in a score between 0 and 100. Higher scores indicate that the participant experiences more cognitive complaints. Cognitive complaints were regarded as high in cases where scores were ≥26. 23
The Hospital Anxiety and Depression Scale (HADS) is a commonly used questionnaire, which was designed to detect the presence of mild degrees of mood disorders in nonpsychiatric hospital outpatients. The HADS consists of 14 items, and has 2 subscales—namely, depression and anxiety. The scores on both subscales range from 0 to 21, with higher scores representing more emotional problems. Scores ≥9 on the subscales were considered abnormal. 24
The Impact of Event Scale (IES) measures psychological reactions that can take place after a traumatic event. 25 The IES has 15 items and explores the level of posttraumatic stress. Scores can range from 0 to 75, with higher scores indicating a higher level of posttraumatic stress. A score ≥26 was used as a cutoff. 26
The Fatigue Severity Scale (FSS) is a 9-item questionnaire that measures experienced severity of fatigue symptoms in daily activities. The total scale ranges from 0 (no fatigue) to 7 (severe fatigue); scores ≥4 were regarded abnormal. 27
Activity Level
The Barthel Index is a widely used instrument that measures basic (personal) activities of daily living. The instrument consists of 10 items and measures to what extent a person can perform basic ADL activities independently. 28 The total scores range from 0 to 20, with higher scores indicating a higher level of independence. The Barthel Index was only assessed at baseline because a ceiling effect was expected for this population.
The Frenchay Activities Index (FAI) is an accepted measure for extended activities of daily living that reports on 15 daily-life activities, resulting in a score ranging from 0 to 45. 29
Participation Level
The Community Integration Questionnaire (CIQ) is a 15-item questionnaire that assesses the level of participation in society. 30 Scores range from 0 to 29, with higher scores indicating a higher level of participation.
The Impact on Participation and Autonomy (IPA) is a 32-item questionnaire, using a 5-point scale (0 = very good, 1 = good, 2 = fair, 3 = poor, 4 = very poor). The IPA distinguishes 5 domains of participation—namely, autonomy indoors, family role, autonomy outdoors, social relations, and work and education. Mean item scores for each domain are presented. Higher scores indicate that there are more problems in participation and autonomy. 31
To measure living situation, participants were asked to respond to written questions concerning their current residence and whether they were living independently or needed help from others. Return to work was defined as partial or complete return to a paid job.
Quality of Life
The EuroQol 5D (EQ-5D-3L) is a generic quality-of-life measure consisting of 5 items (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each with 3 answer possibilities (no problems, some problems, severe problems). To report outcome on the EQ-5D, scores were analyzed using the overall index score as well as on an item level.32,33 The EuroQol VAS (EQ-VAS) is a Visual Analogue Scale from 0 to 100, on which participants are asked to give a general rating of their current health state. 32
The Medical Outcomes Study 36-item Short Form Health Survey (SF-36/RAND 36-item Health Survey) is a 36-item generic quality-of-life questionnaire that measures 8 domains of perceived health. 34 Reference values for the general Dutch population are available and are as follows for the age group 55 to 64 years: physical functioning = 73 (SD = 24), social functioning = 87 (SD = 21), role physical = 77 (SD = 38), role emotional = 90 (SD = 25), mental health = 77 (SD = 19), vitality = 67 (SD = 21), bodily pain = 75 (SD = 25), and general health = 64 (SD = 22). 35
The Quality of Life after Brain Injury questionnaire (QOLIBRI) is a brain injury–specific quality-of-life measure. The QOLIBRI consists of 37 items, and total scores are converted to a total score that ranges from 0 to 100. 36
Measurement instruments were administered at 3 measurement moments (2 weeks, 3 months, and 12 months after the cardiac arrest). The FSS and the QOLIBRI were administered at 3 and 12 months only because at baseline, patients were often still in hospital. The IPA was only administered at 12 months.
The patient’s level of daily functioning (FAI) and participation in society (CIQ) was measured at 3 and 12 months, but we also retrospectively assessed the level of functioning prior to the cardiac arrest in order to be able to compare postarrest functioning with prearrest functioning. This retrospective assessment was done during the first meeting by asking the patient to think back to their situation prior to the cardiac arrest and, if necessary, with help of the caregiver.
Statistical Analysis
To check for selection bias, we examined the differences between participants who completed the study and those who dropped out during the study in terms of the following baseline characteristics: age, gender, location of the cardiac arrest, initial overall cognitive status (Cog-Log), and level of basic daily activities (Barthel Index). Descriptive statistics were used to describe baseline sociodemographic and medical variables.
Outcomes on the measurement instruments are presented using descriptive statistics. Means (SDs) or medians (ranges) are reported depending on whether data had a normal or a nonparametric distribution. Established cutoff scores were used (where available) to calculate the percentage of patients with abnormal scores on each domain. For measures with a prearrest score available (FAI and CIQ), the postarrest score was also presented as a percentage of the prearrest score.
Changes over time were investigated using Friedman’s ANOVA. In case a significant (P ≤ .05) difference between the 3 moments in time was found, additional post hoc analyses were performed using a Wilcoxon signed-rank test to determine where the changes over time had occurred. The significance level for these analyses was set at P ≤ .0167, based on a Bonferroni correction (α/number of comparisons). For the instruments that had been administered twice (FSS and QOLIBRI), only the Wilcoxon signed-rank test was used. We did not impute any missing data. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0.
Results
Participants
Figure 2 presents the flow of participants through the study. Overall, 141 patients were included in the study, of whom 110 (78%) were followed up to 12 months after the cardiac arrest. There were no significant differences between participants who dropped out during the study and those who completed it regarding age (62 vs 60 years, P = .242), male gender (81% vs 86%, P = .515), location of the cardiac arrest (out of hospital 74% vs 81%, P = .414), and level of initial basic daily activities (median 19 vs 20, P = .119). In contrast, those who dropped out during the study had a lower initial score on the cognitive screening (median 24.5 vs 27.0, P = .001).
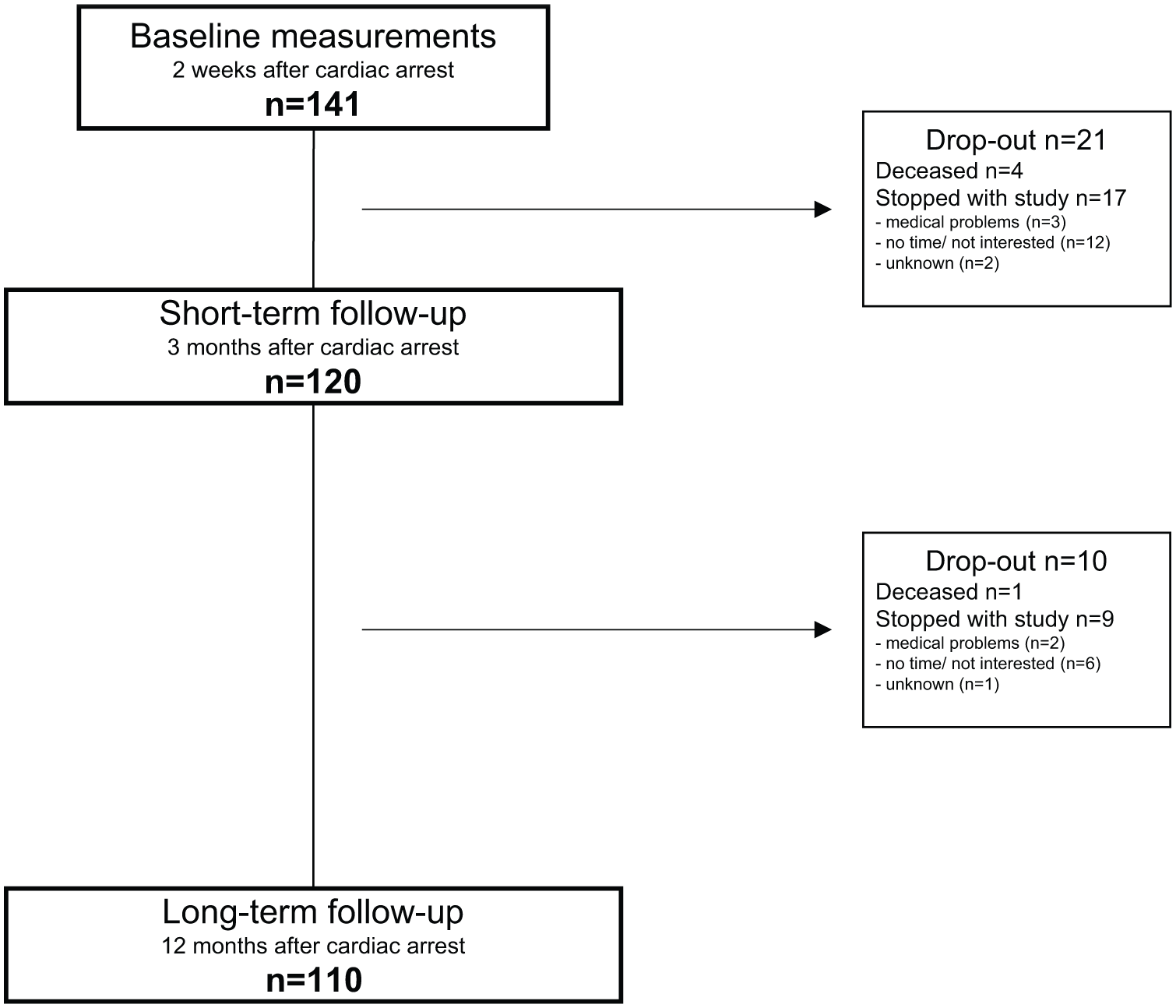
Flow of participants through the study.
Baseline assessments were performed on average after 24 days (SD = 11), with 3- and 12-month follow-up assessments on average after 98 days (SD = 15) and 374 days (SD = 15), respectively. Table 1 shows the patients’ sociodemographic and medical characteristics. Of the participants, 112 (79%) had survived an out-of-hospital cardiac arrest and 29 (21%) an in-hospital cardiac arrest.
Sociodemographic and Medical Characteristics.
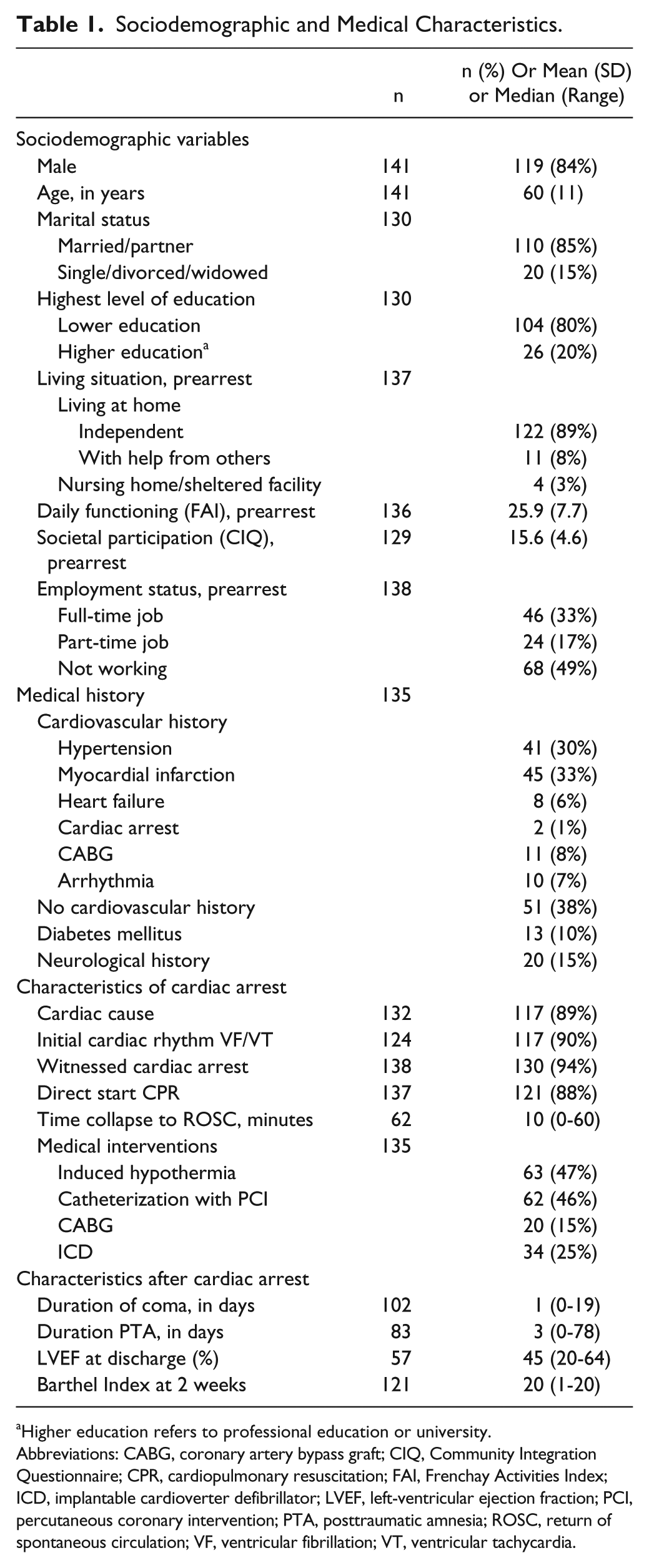
Higher education refers to professional education or university.
Abbreviations: CABG, coronary artery bypass graft; CIQ, Community Integration Questionnaire; CPR, cardiopulmonary resuscitation; FAI, Frenchay Activities Index; ICD, implantable cardioverter defibrillator; LVEF, left-ventricular ejection fraction; PCI, percutaneous coronary intervention; PTA, posttraumatic amnesia; ROSC, return of spontaneous circulation; VF, ventricular fibrillation; VT, ventricular tachycardia.
Outcome After Cardiac Arrest
Function Level
Table 2 presents the patients’ outcome at the level of function. One year after the cardiac arrest, cognitive functioning was below cutoff in 14 (13%) survivors, and 14 (14%) also experienced cognitive complaints. Both anxiety and depression were present in 16 (15%) survivors, and 29 (28%) experienced symptoms of posttraumatic stress. Fatigue was the most common problem and occurred in 55 (52%) survivors.
Outcome on Function Level During the First Year After Cardiac Arrest.
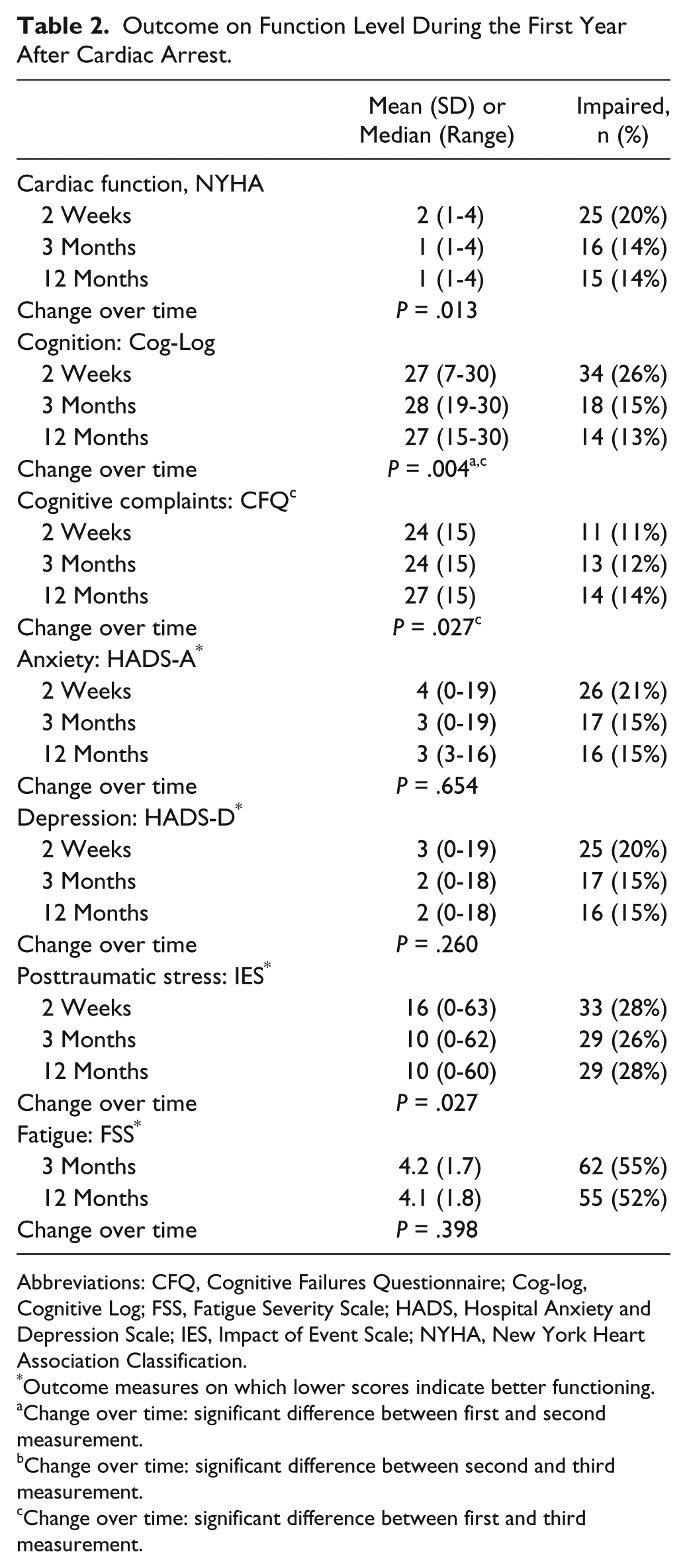
Abbreviations: CFQ, Cognitive Failures Questionnaire; Cog-log, Cognitive Log; FSS, Fatigue Severity Scale; HADS, Hospital Anxiety and Depression Scale; IES, Impact of Event Scale; NYHA, New York Heart Association Classification.
Outcome measures on which lower scores indicate better functioning.
Change over time: significant difference between first and second measurement.
Change over time: significant difference between second and third measurement.
Change over time: significant difference between first and third measurement.
Activities and Participation
Table 3 shows the results on the level of activities and participation.
Outcome on Activities and Participation During the First Year After Cardiac Arrest.
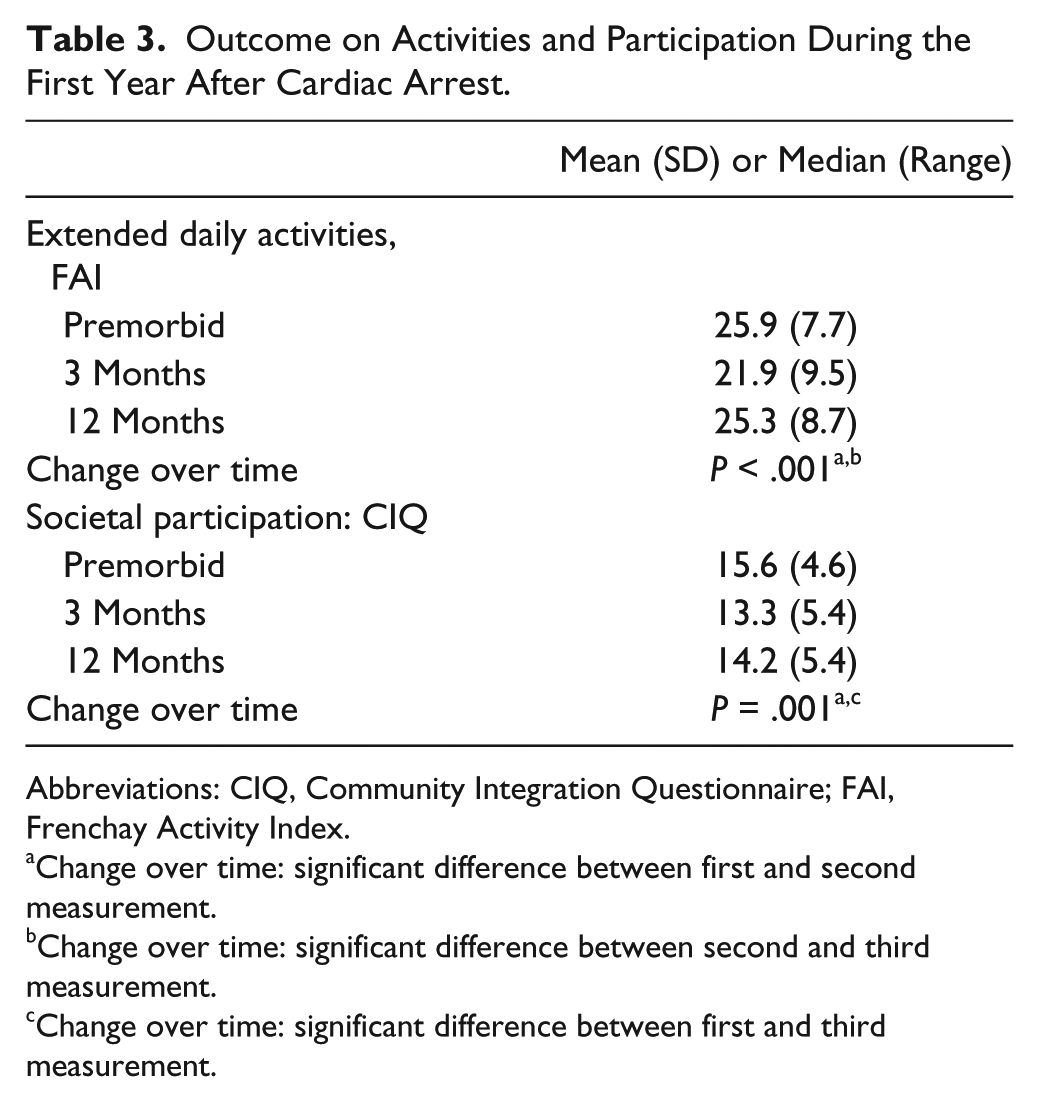
Abbreviations: CIQ, Community Integration Questionnaire; FAI, Frenchay Activity Index.
Change over time: significant difference between first and second measurement.
Change over time: significant difference between second and third measurement.
Change over time: significant difference between first and third measurement.
In addition, scores on 2 measures (FAI and CIQ) could be compared with prearrest levels of functioning. With regard to extended daily activities (FAI), patients scored on average 82% of their prearrest level at 3 months, with an increase up to 96% at 12 months. Overall, scores on FAI at 1 year were not significantly (P = .066) different compared with prearrest levels.
On the level of participation in society (CIQ), at 3 months, patients scored on average 88% of their prearrest score, increasing up to 92% at 12 months. The CIQ scores at 1 year were significantly (P = .001) lower than the prearrest scores, although the difference in mean scores was limited (1.4 points).
Scores on the subdomains of the IPA at 1 year were as follows: median = 0.3 (range = 0-2.6) for autonomy indoors, 1.0 (0-3.4) for family role, 1.0 (0-3.4) for autonomy outdoors, and 1.0 (0-3.1) for social relations, all indicating “good” outcome on these domains. Most problems were experienced on the domain of work and education (median = 1.8; range = 0-3.7).
As regards the living situation of the survivors at 1 year, 104 survivors (99%) lived at home, of whom 20 persons (19%) needed some help from others. One person (1%) was living in a nursing home. Half of the survivors (51%) had still been working at the time of their cardiac arrest. At 3 months, 13 (24%) were back at work. At 1 year, 41 (72%) had returned to work, although 18 (44%) of them had reduced their number of working hours as compared with their prearrest working hours.
Quality of Life
Table 4 describes the results for quality of life. The median index score of the EQ-5D increased from 0.8 at 2 weeks to 0.9 at 1 year.
Quality of Life During the First Year After Cardiac Arrest.
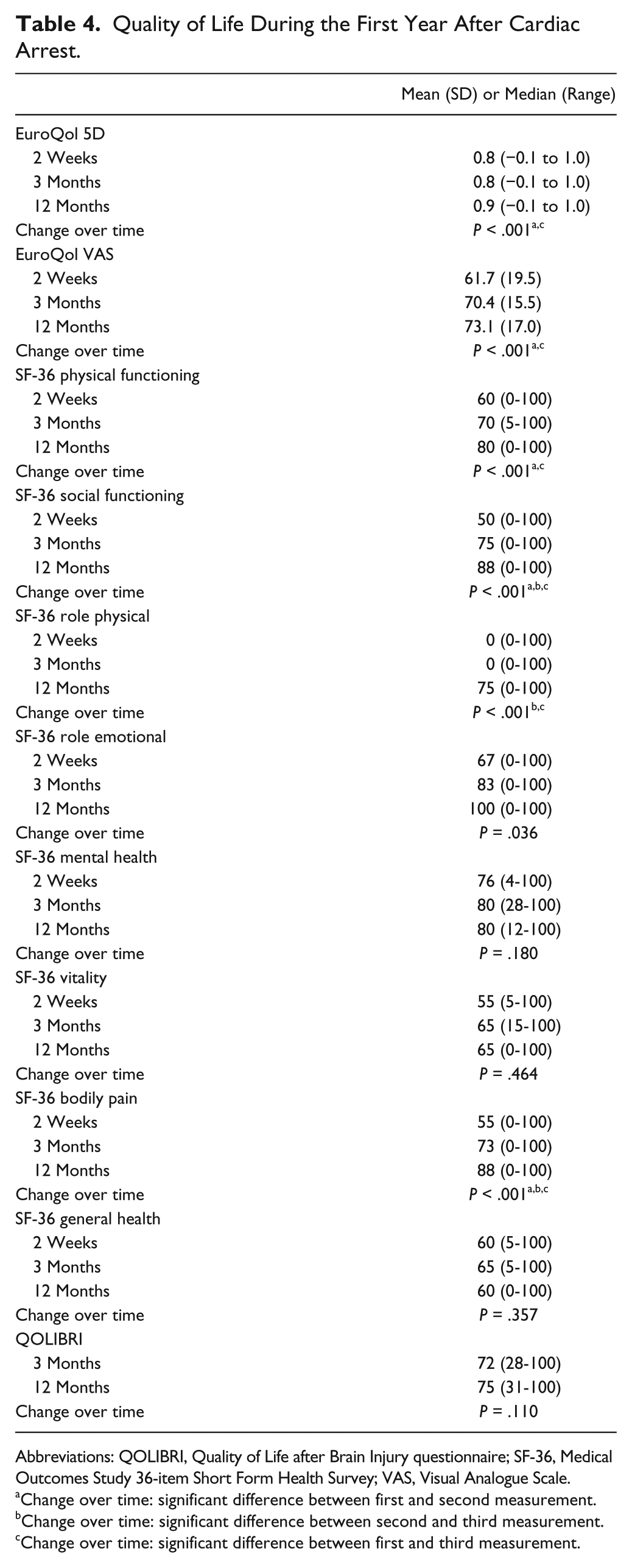
Abbreviations: QOLIBRI, Quality of Life after Brain Injury questionnaire; SF-36, Medical Outcomes Study 36-item Short Form Health Survey; VAS, Visual Analogue Scale.
Change over time: significant difference between first and second measurement.
Change over time: significant difference between second and third measurement.
Change over time: significant difference between first and third measurement.
In addition, scores on the 5 individual items of the EQ-5D at 1 year were as reported: survivors experienced some to severe problems in mobility in 35 (35%) of the cases, 9 (9%) with self-care, 42 (42%) with usual activities, 39 (39%) in pain/discomfort, and 26 (26%) on anxiety/depression. EuroQol VAS scores rose from 61.7 at 2 weeks to 73.1 at 1 year. The SF-36 scores at 1 year were close to the reference values for a comparable age group of the general Dutch population.
Differences Over Time
The cardiac arrest survivors showed significant improvements between 2 weeks and 3 months (Tables 2, 3, and 4) on cognitive function (Cog-Log) and several measures of quality of life (EQ-5D, EQ-VAS, and the SF-36 domains Physical Functioning, Social Functioning, and Bodily Pain). There were further improvements between 3 months and 12 months on the SF-36 domains social functioning, bodily pain, and role physical. Cognitive complaints were more frequently present at 1 year compared with 2 weeks. In addition, there were significant positive overall effects of time on the cardiac function (NYHA), symptoms of posttraumatic stress (IES), and SF-36 domain role emotional on Friedman’s ANOVA test, but the post hoc analyses using Bonferroni correction were not significant.
Discussion
In this study on problems seen 12 months after a cardiac arrest, we found that the main residual problems occur on the ICF function level, with emotional problems in 25% of the survivors and fatigue in more than half. In contrast, we have shown that functioning on the levels of activity and participation approaches prearrest levels. In addition, return to work, in those who had been working at the moment of their cardiac arrest, was relatively high (72%). Also, the outcomes on quality-of-life measures present a positive picture of long-term outcome after cardiac arrest.
This study showed that most recovery of cognitive function and quality of life occurs within the first 3 months, with (further) improvement on some domains of quality of life (SF-36 domains social functioning, bodily pain, and role physical) seen up to 12 months. This is in line with the pattern of recovery seen in other nonprogressive neurological diseases. 17 However, the amount of recovery during the first year on the levels of activities and participation is higher than in stroke patients.37-39
Our results indicate that for the establishment of long-term outcome after cardiac arrest, follow-up should extend beyond 3 months because we found multiple and significant improvements between 3 and 12 months. But because we did not perform any measurements between 3 and 12 months, future research should investigate at what point in time maximum recovery is most commonly reached and whether follow-up beyond 1 year should be recommended.
Recently, Raina et al 40 published one of the first studies on long-term outcome after cardiac arrest with measures also covering aspects of all 3 ICF domains and quality of life. During the first year, recovery was reported on global measures (Cerebral Performance Category and Modified Rankin Scale), whereas depressive symptoms did not seem to improve. The levels of activities and participation were more reduced, when compared with our study. However, this study included 29 patients only. The results of the current study make an important contribution to the growing body of evidence on this topic.
Based on earlier studies, we expected cognitive impairments and complaints to be higher than was eventually found.8,9 This discrepancy could be a result of a suboptimal sensitivity of the Cog-log in this population. A surprising finding was that the amount of subjective cognitive complaints increased over time. A potential explanation is that survivors only become aware of their cognitive limitations when they are faced with more complex and demanding activities, such as return to (volunteer) work. Therefore, long-term follow-up of cognitive functioning is recommended. This is in line with a recent study, which showed the importance of addressing cognitive functioning, even in survivors with rapid recovery, because cognitive impairments (especially memory and psychomotor functioning) had a negative effect on quality of life in a cohort of survivors with good outcome. 41
The current study confirmed that fatigue is a common problem after cardiac arrest. 11 Fatigue also has a very high prevalence after other neurological conditions such as stroke and aneurysmal subarachnoid hemorrhage.42,43 Because fatigue is a complex and multifactorial concept, more research is needed to disentangle the causes and explore potential remedies for this problem. Future research should also address the interrelationships between the different domains of functioning to discover whether there are certain clusters of problems.
An interesting finding is that although the number of problems on the function level is relatively high, this is not reflected by poor outcomes in activities, participation, or quality of life. This could be attributed to good coping styles or might be explained by the experience of a “second chance” after such a life-threatening condition, which might lead to reattribution of values or a more proactive lifestyle. 44
This study showed that although the majority (72%) of those who had still been working were able to return to work, almost half of them had had to reduce their working hours. We do not have any data on productivity of those who returned to work, but it is highly possible that this was affected, especially because cognitive problems and fatigue were still common. This shows that return to work should be carefully monitored and that more research on this topic is required.
This study has some limitations. First, most outcome measures, except the cognitive tests, were based on questionnaires, which imply a potential risk of overestimation or underestimation caused by self-report. However, the instruments we used are also commonly used in brain injured populations and found to be valid.
Second, being part of a cohort study might also have had some influence on natural recovery because patients might have become more aware of their limitations and may have searched for help themselves. Indeed, there is no real natural recovery, in that all patients would probably have received advice or other input from health care professionals seen as part of general (usual) health care.
Third, there may be some selection bias in this study. It is possible that relatives of patients who were still critically ill at the moment of inclusion might have refused participation, which might also explain why there were no patients in a vegetative state in this cohort. In addition, survivors who dropped out during the study had a lower initial score on the cognitive screening, which could be an indication of more neurological damage. The outcomes presented in this article may, therefore, have some bias toward overestimation of functioning. However, the generalizability of this study is relatively high because we targeted to include all cardiac arrest survivors and did not exclude any patients based on location of cardiac arrest, cause of the arrest, age, or poor prognosis, as is often the case in other studies.
Finally, data collection took place between 2007 and 2010, and the question can be raised whether these findings are still representative for the present situation. However, in the study region, induced hypothermia was already applied before the start of this study and also the presence and use of AEDs was already high. To the best of our knowledge, there have been no major changes in clinical care after cardiac arrest in the meantime that could have had a significant impact on outcome.
Implications
This project has several practical implications. Although long-term outcome is, on average, fortunately reassuring on the levels of activity, participation, and quality of life, long-term follow-up care after cardiac arrest is needed and should, at least, include screening on cognitive and emotional problems and fatigue. We have also shown that a concise nursing intervention after discharge can further improve emotional well-being and quality of life. 19 In case of severe emotional problems, referral for further psychological care is recommended, especially because these problems tend to remain and are risk factors for new cardiac events.40,45,46 Future research should also address determination of prognostic factors, so that persons at risk for long-term problems can be detected earlier and referred to specialized (rehabilitation) care more swiftly.
Footnotes
Acknowledgements
We would like to acknowledge all patients for their participation in this study. All participating hospitals, involved staff members, and research assistants are thanked for their cooperation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Netherlands Organisation for Health Research and Development (ZonMw 920-03-373); Fonds Nuts Ohra (0602-069); and Stichting Elisabeth Strouven. The funding agencies were not involved in the design, performance, or interpretation of the study.