
Abstract
Background. Despite the fact that social participation is considered a pivotal outcome of a successful recovery after stroke, there has been little attention on the impact of activities and services on this important domain. Objective. To present a systematic review and meta-analysis from randomized controlled trials (RCTs) on the effects of rehabilitation interventions on social participation after stroke. Methods. A total of 8 electronic databases were searched for relevant RCTs that evaluated the effects of an intervention on the outcome of social participation after stroke. Reference lists of selected articles were hand searched to identify further relevant studies. The methodological quality of the studies was assessed using the Physiotherapy Evidence Database Scale. Standardized mean differences (SMDs) and confidence intervals (CIs) were estimated using fixed- and random-effect models. Results. In all, 24 RCTs involving 2042 stroke survivors were identified and reviewed, and 21 were included in the meta-analysis. There was a small beneficial effect of interventions that utilized exercise on social participation (10 studies; SMD = 0.43; 95% CI = 0.09, 0.78; P = .01) immediately after the program ended. Exercise in combination with other interventions (13 studies; SMD = 0.34; 95% CI = 0.10, 0.58; P = .006) also resulted in beneficial effects. No significant effect was observed for interventions that involved support services over 9 studies (SMD = 0.09 [95% CI = −0.04, 0.21]; I2 = 0%; P = .16). Conclusions. The included studies provide evidence that rehabilitation interventions may be effective in improving social participation after stroke, especially if exercise is one of the components.
Introduction
A World Health Organization 1 report revealed that stroke results in the greatest burden of disease among all neurological disorders (including Alzheimer’s and dementias). There is an increasing number of strokes because the North American population is aging, and a greater proportion of people than before are surviving stroke. Unfortunately, not all patients are getting access to the care and rehabilitation they need to have the best possible outcome. 2
Recovery of function in stroke patients is a complex process, which may be spontaneous and involve the effects of therapeutic interventions.3,4 Knowledge about interventions that promote the best outcomes on recovery may help optimize health care services. Successful recovery from a stroke should result in a quality of life and degree of participation in the community similar to that prior to the stroke event. There has been increasing criticism of the lack of services and research on the long-term consequences after stroke. A BMJ commentary summarized this sentiment: “Comprehensive national audits of stroke care show alarming levels of neglect in terms of chronic disease management and seem to indicate a collective nihilism about the potential for altering function and well-being after the early treatment of stroke” (p 461). 5 However, there is little consensus about the effects of rehabilitation services for stroke survivors once they have left the hospital and are living in the community. Social participation is considered one of the most relevant and pivotal outcomes of a successful recovery. 6 Individuals have been shown to be dissatisfied with their ability to engage in numerous aspects of participation, including socializing, outings, and travel, at 3 months after sustaining a stroke. 7 The provision of rehabilitation services after hospital discharge may be particularly relevant because it aims to promote patients’ independence and reintegration into the community.
The International Classification of Functioning, Disability and Health (ICF) defines participation as “involvement in a life situation” 8 or as “the lived experience” of people in the actual context in which they live. Participation is a treatment goal in the context of recovering from stroke and is known to correlate with domains related to quality of life. 9 Using a content analysis involving 43 studies, Levasseur et al 10 defined social participation “as a person’s involvement in activities that provide interaction with others in society or the community” (p 2148). Similarly, the Disability Creation Process conceptual model defines social participation as a means of carrying out one’s life habits in one’s environment (eg, school, work place, neighborhood). 11
Despite the fact that social participation is critical to the success of community reintegration, the literature in this area has not been systematically collated and synthesized previously, to our knowledge. Therefore, we performed a systematic review and meta-analysis to determine if rehabilitation interventions improve social participation among stroke survivors based on the evidence from randomized controlled trials (RCTs).
Methods
Search Strategy, Eligibility Criteria, and Data Retrieval
An electronic database search was done up to April 2015 using 8 databases. MEDLINE (OvidSP), Embase (OvidSP), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials (CENTRAL), Physiotherapy Evidence Database (PEDro), PsycINFO, ProQuest ERIC, and NIH Clinical Trials Databases were searched using the MeSH and keywords stroke, cerebrovascular disease, cerebrovascular disorder, cerebral infarction, and brain infarction in conjunction with rehabilitation, social participation, quality of life, and activities of daily living. We did not limit the search to any language or date. Considering the different terms that can be used for social participation, we did not restrict the review to any specific outcome measure.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 12 was followed. Peer-reviewed publications were included if they were RCTs of any nonpharmacological and nonsurgical community-based intervention for community-dwelling stroke survivors, where social participation was an outcome. Further inclusion criteria were the following: (1) participants >18 years of age; (2) a baseline data point and a postintervention data point or follow-up (ie, retention of effects) assessing social participation using a validated scale; (3) intervention and control group treatments clearly defined; and (4) intervention carried out for at least 4 weeks to have sufficient duration for benefits to accrue. Studies that included other populations were included if data for the stroke group were available. A social participation outcome required measurement of one or more of the following 3 characteristics: social contact, contributing to society (eg, volunteer work), or receiving from society (eg, receiving a visit from a friend). 13 Studies were excluded if the full research document was not located, if the type of intervention could not be identified or detail of intervention was not provided, and if the data were derived from a conference proceeding or abstract. Interventions that involved electrotherapeutics or electromechanics (eg, electrical stimulation, vibration) were excluded because they are not typically considered community-based programs.
All citations obtained were exported to RefWorks bibliography management software. After duplicates were deleted, the titles and abstracts of studies identified were screened, and full articles of abstracts that appeared relevant were retrieved. The reference lists of the full-text articles were searched by hand to identify additional relevant research articles. At this point, any article that did not meet the inclusion/exclusion criteria was discarded. The remaining articles were assessed for quality of evidence and risk of bias using the Physiotherapy Evidence Database (PEDro) Scale (maximum score of 10). 14 When available, we utilized the official scores posted on the PEDro Web site because these have been verified by 2 trained experts. If the median and range were reported, we converted them to the mean and standard deviation. 15 If an interquartile range was reported, we converted it to a standard deviation. 16 The reviewers assessed eligibility based on the full-text articles and conducted data extraction independently using a standard form. The study selection process along with excluded articles at the full-text level was presented via a PRISMA study flow diagram.
Statistical Analysis
An analysis was undertaken for (1) immediate postintervention (differences between the baseline and postintervention) and (2) follow-up (differences between the baseline and last follow-up point, ie, months after the intervention ended) for interventions that were reasonably homogeneous. Given the outcome of social participation, we expected that programs providing support services would be a typical intervention found within this search. Thus, we planned to undertake an analysis of support service interventions, defined as those programs or services offered to assist individuals and their families in handling the myriad physical, emotional, social, and practical problems that follow a stroke diagnosis and its subsequent treatment. 17 We also expected that exercise programs would be another intervention found within the search because better mobility and endurance may be associated with the ability to participate in everyday activities.18,19 Thus, we planned to undertake an analysis of exercise as an intervention, defined as a physical activity that is planned, structured, repetitive, and purposive, with the objective of improvement or maintenance of physical fitness and function. 20 A standardized mean difference (SMD) was calculated for all outcomes. Heterogeneity was assessed by the I2 value. Random-effect models were used if statistical heterogeneity observed in the groups was high (I2 > 25%) 21 ; else, fixed-effect models were used. All statistical analyses were performed with Review Manager 5.3 (the Nordic Cochrane Centre, Copenhagen). Statistical significance was considered as a P value <.05.
Results
Included Studies
A total of 24 studies22-45 met the inclusion criteria (Figure 1), with a total of 2042 individuals with stroke. Two studies30,34 did not have immediate postintervention data but reported outcomes 6 months 30 and 9 months 34 after the intervention ended. Four studies required conversion of the data to mean and standard deviation; 1 each reported median and interquartile ranges 27 and median and range values, 33 and 2 reported mean and confidence interval (CI) values28,42 The ages of the stroke survivors ranged from 30 to 91 years. The length of the intervention ranged from 4 weeks 44 to 12 months,35,37 with the duration of most of the studies (22/24) being 4 weeks 44 to 6 months.39,41,43 Individual study details are included in Table 1 and present 7 support service studies, 11 exercise studies, 3 mixed studies (support service and exercise), and 3 other studies that did not involve exercise or support service.
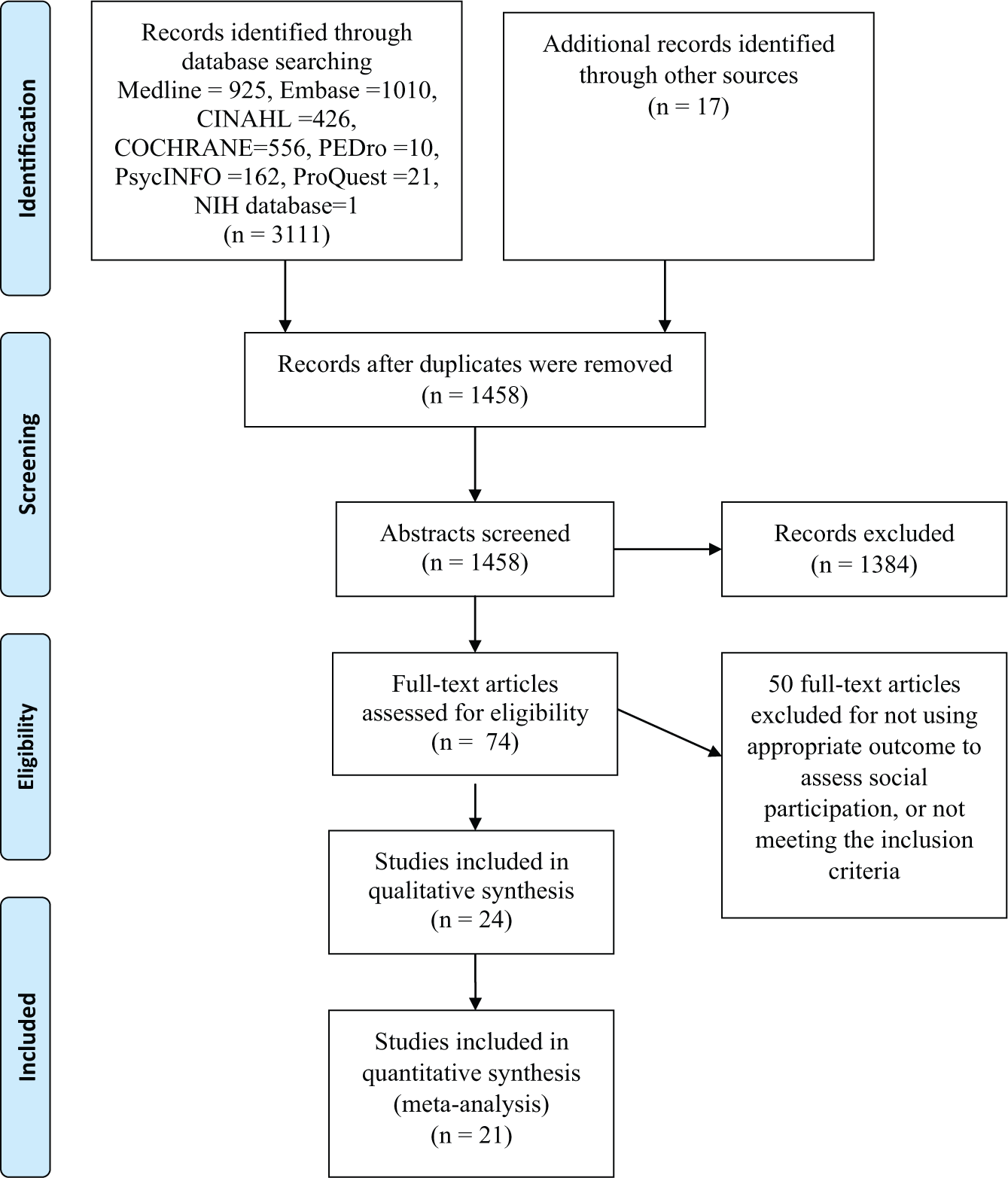
PRISMA study selection flow diagram.
Characteristics of Included Studies. a
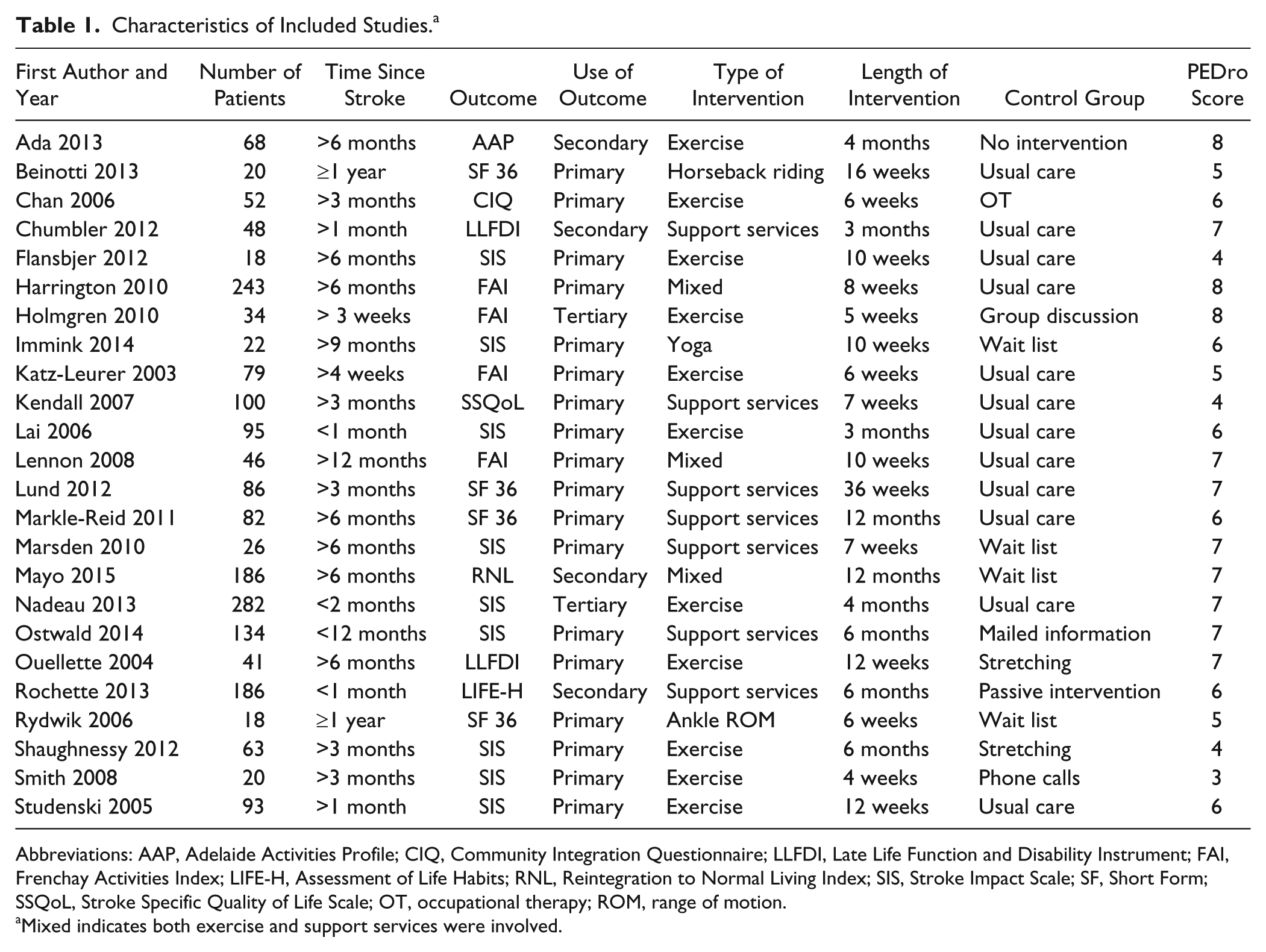
Abbreviations: AAP, Adelaide Activities Profile; CIQ, Community Integration Questionnaire; LLFDI, Late Life Function and Disability Instrument; FAI, Frenchay Activities Index; LIFE-H, Assessment of Life Habits; RNL, Reintegration to Normal Living Index; SIS, Stroke Impact Scale; SF, Short Form; SSQoL, Stroke Specific Quality of Life Scale; OT, occupational therapy; ROM, range of motion.
Mixed indicates both exercise and support services were involved.
Studies utilizing support services included telephone calls,25,41 home visits,35,39 educational courses,31,34 mailed educational information, 39 and group discussions. 36 Studies utilizing support services as an intervention or in combination with other interventions25,27,31,33-37,39,41 had a frequency of at least one session per month for 8 weeks. Studies utilizing exercise included treadmill training,22,38,43,44 cycling,30,33 group exercise, 37 and progressive resistance exercise.28,32 Studies utilizing exercise had a frequency of at least 2 sessions per week.
Outcome Measures of Social Participation
Most of the studies (18/24) assessed social participation as a primary outcome,23,24,26,27,29-36,39,40,42-45 and 9 studies26,29,32,36,38,39,43-45 used the social participation subscale of the Stroke Impact Scale. Two studies27,37 used both a subscale and full scale to assess social participation. In these instances, complete scales used to assess social participation were chosen over subscales.
Quality of Evidence
The PEDro scores ranged from three 44 to eight.22,27,28 One study 41 did not have a confirmed PEDro score, and it was calculated independently by 2 authors; disagreements were resolved by discussion. In all, 11 studies23,24,26,29-31,34,42-45 did not perform an intention-to-treat analysis. More than 15% of loss to follow-up occurred in 4 studies.31,35,40,41 Two exercise studies recorded adverse events,38,40 whereas one 28 only reported falls. One study each reported that no adverse events 25 and no serious adverse events occurred. 37 Also, 17 studies,22-24,26,27,29-36,39,43-45 including 10 with exercise components, did not state whether any adverse events occurred or not.
Quantitative Analysis
Analysis of the 10 studies that used exercise alone (n = 764) produced a significant model immediately after the intervention ended (SMD = 0.43 [95% CI = 0.09, 0.78]; I2 = 78%; P = .01; Figure 2A). Because some studies have multiple components, restricting the analysis to 13 studies that involved at least an exercise program (n = 1239) also produced a significant model (SMD = 0.34 [95% CI = 0.10, 0.58]; I2 = 73%; P = .006; Figure 2B). After removing 2 studies considered as outliers because their SMDs were greater than 1.4 (ie, very strong effect of exercise),24,40 whereas all others were less than 0.7, the model remained significant (SMD = 0.14 [95% CI = 0.02, 0.25]; I2 = 0%; P = .02). Removing the only study 44 that was considered of poor methodological quality following risk-of-bias assessment (PEDro score ≤ 3) still produced significant models for studies that involved exercise alone (SMD = 0.42 [95% CI = 0.06, 0.78]; I2 = 80%; P = .02) or at least an exercise program (SMD = 0.32 [95% CI = 0.07, 0.57]; I2 = 75%; P = .01). There was no statistically significant effect of exercise for the follow-up period of 6 studies that used exercise alone or 7 studies that used exercise in conjunction with other components.
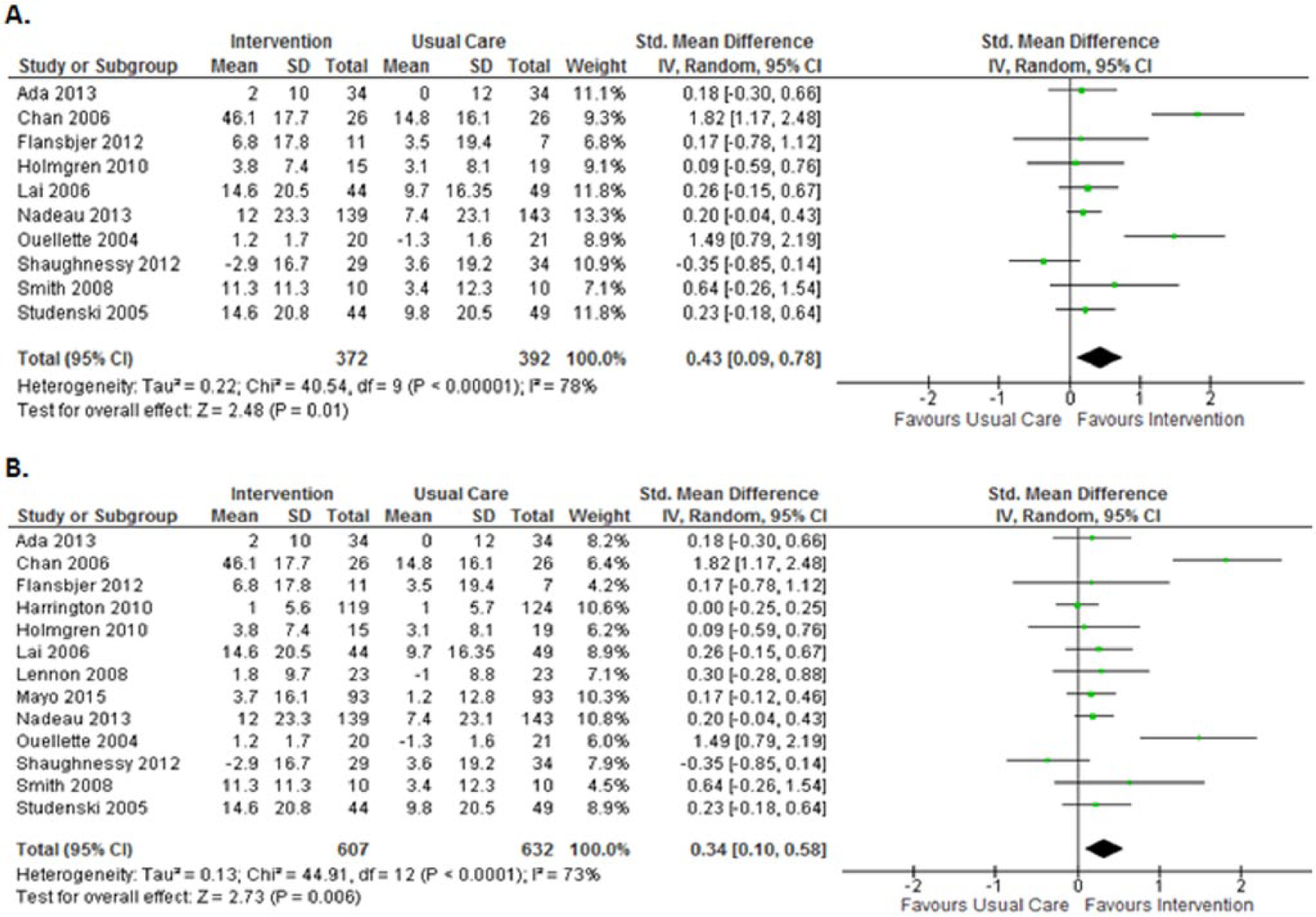
Postintervention forest plot of interventions involving (A) exercise alone or (B) at least exercise.
No significant difference was observed for interventions that involved support services over 9 studies (SMD = 0.09 [95% CI = −0.04, 0.21]; I2 = 0%; P = .16; Figure 3). Removing the only study 41 that did not involve face-to-face contact or require the participant to leave the home resulted in a near significant effect (SMD = 0.13 [95% CI = −0.00, 0.27]; I2 = 0%; P = .05). There was no statistically significant effect of support services for the follow-up period of 4 studies that used support services alone or 5 studies that used support services in conjunction with other components. Of the 3 studies that did not involve support service or exercise as defined in the study, 1 study reported significant improvement on social participation using passive and active ankle range of motion 42 (SMD = 3.13 [95% CI = 1.65, 4.61]), and 2 reported no significant impact using yoga 29 (SMD = 0.65 [95% CI = −0.21, 1.51]) or horseback riding 23 (SMD = −0.05 [95% CI = −0.93, 0.83]).
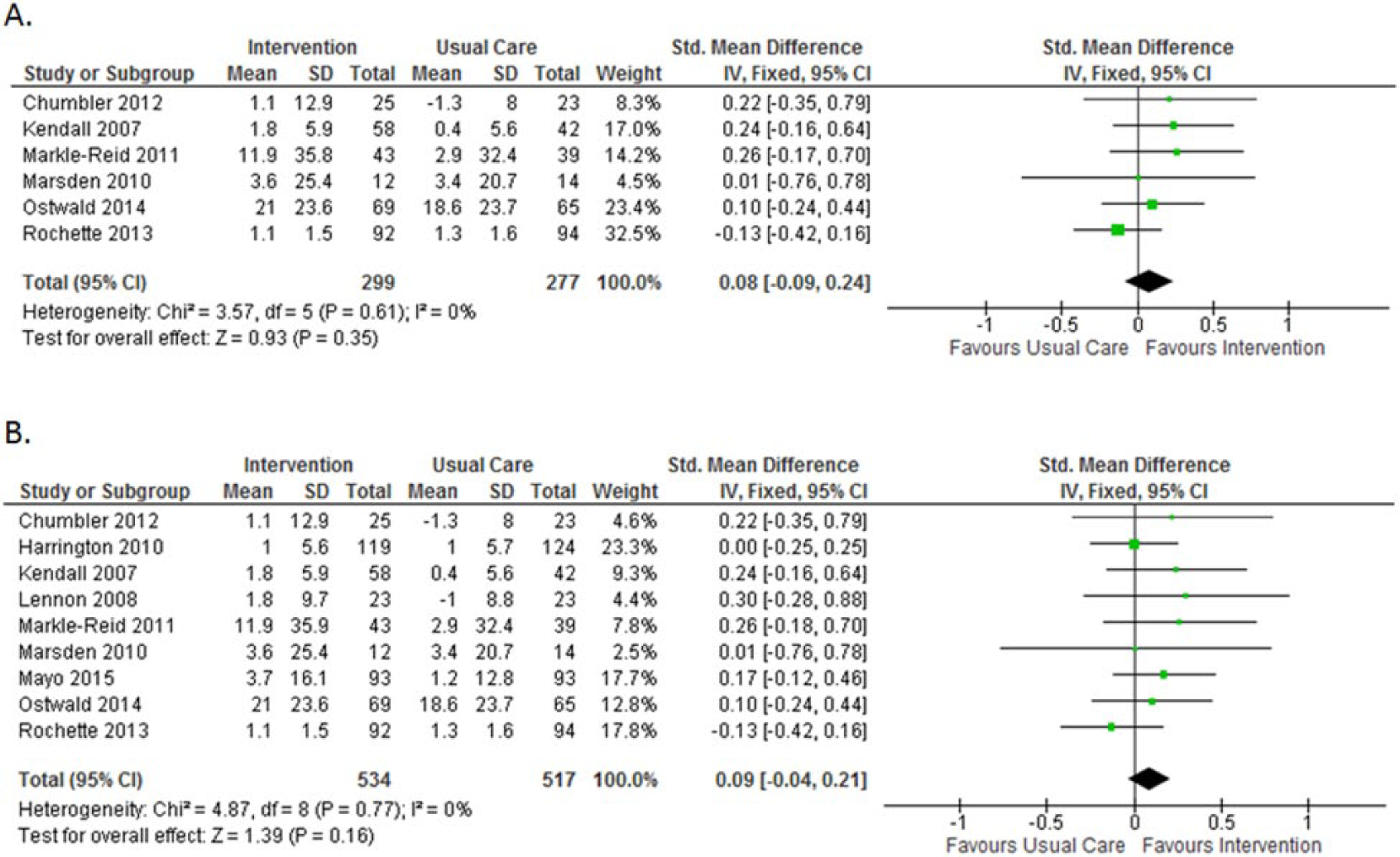
Postintervention forest plot of interventions involving (A) support services alone or (B) at least support services.
Discussion
Social participation is one of the most important end points of recovery from a stroke, and it is usually the ultimate goal of rehabilitation. In a recent metaethnographic review of the experiences and views of community-dwelling stroke survivors, 46 most studies reported that stroke disrupts the lives of participants, leading to a change in their social lives and loss of autonomy and independence. The findings in our study showed that it is possible to improve social participation with certain rehabilitation interventions. In particular, interventions that involved exercises (in part or alone) were effective. The prominence of studies focusing on the impact of exercise is not surprising given the long-held clinical belief in the value of active exercise in stroke rehabilitation. 47
There are a number of mechanisms that may explain the impact of exercise on social participation. Exercise can improve mobility, 48 balance, fatigue, and endurance after stroke, 49 which may enable the stroke survivor to engage in activities. Physical activity is also known to improve a number of the secondary effects of stroke, which may be a barrier to social participation. For example, exercise can prevent or reduce depressive symptoms after stroke, 50 which may lead to greater willingness to engage in activities. Hence, exercise has a very real protective function, helping to increase physical independence and improving quality of life.
All but two32,45 of the studies that involved exercise had the intervention carried out in either a community setting22,27,37 or rehabilitation center.24,26,28,30,33,38,40,44 Because these venues are different from their homes, they provide a form of social participation. Exercise provided in groups may also provide an additive benefit that has an element of social participation in socially engaging settings with participants experiencing similar health issues. 51 The support provided by the exercise instructors (eg, external encouragement, qualified personnel) has been identified as a facilitator in participating in exercise. 52 Group exercise can also increase levels of participation in physical activity as social support from other group members provides encouragement to attempt new exercises and challenge negative perception of ability. 53 Stroke-specific exercise groups are viewed as enabling social support, increasing confidence, improving mood and motivation, and providing an opportunity for knowledge acquisition. 54 Exercise appeared to have been beneficial in stroke, but the effects were not retained after the intervention ended. Being physically active on a regular basis is recommended by all exercise guidelines.
It is possible that the act of getting out of the home to engage with other people is the critical element of the exercise programs, which resulted in improved social participation. However, some of the exercise studies required both the experimental and control groups to participate in a community group program, which would account for attention, engaging with others and getting out of the home. In fact, some of the exercise studies which utilized attention controls had the largest effect sizes,24,40 suggesting that it is the exercise itself that is effective. Some of the studies requested that participants exclude their outings because of the exercise itself when estimating their social participation, 37 which provides additional evidence that it is the act of exercise that is beneficial for improving social participation.
Over the long term, a stroke survivor’s focus on recovery shifts from physical concerns to social concerns, where there is a desire to participate in the social world and integrate into lives and relationships. 55 Although it may seem logical that providing services to support community integration would enhance social participation, the meta-analysis showed that the effect of support services on social participation is questionable. Of interest, removing the only study 41 that did not involve face-to-face contact resulted in a near significant effect, suggesting that the act of leaving the house and interacting in person with others may need to be an active ingredient of a social participation intervention. It is important to note that participants only received usual care (and not an attention control) in 4 studies25,31,33,35 out of 5 that showed that support service was more beneficial, and thus, it is not possible to disentangle the effects of attention versus support.
In this present meta-analysis, only 1 study 37 developed the intervention with the intention of enhancing participation after stroke. In addition to exercise, these participants explored local community resources and opportunities and were encouraged to engage in community-based activities to meet leisure and life goals. The authors noted that their strongest effects were demonstrated at the end of the intervention (at 12 months) and at follow-up (3 months later) versus midintervention (6 months), and they suggested that gains in participation take time. Other studies may be limited by their short duration. It is possible that the efficacy of support service interventions may have also been affected by the treatment frequency. Most of the support service interventions had less treatment frequency (typically once a week) compared with interventions that utilized a component of exercise (frequency of 2 to 5 times a week). Duration and intensity are important factors in the effectiveness of rehabilitation. 56
It is difficult to draw conclusions about the interventions that did not involve support services or exercise because there was only one study for each. In the study by Rydwik et al 42 involving passive and active range-of-motion training, the authors attributed a large effect on social participation to attention, potentially from the health care providers, because the control group received no intervention, and these effects were not accompanied by any physiological changes. We did not categorize horseback riding or yoga as exercise according to our definition and found that neither had an effect on social participation, despite the additional attention provided over the usual care control group. Although some forms of horseback riding and yoga can be considered exercise, the one study with horseback riding utilized it mostly as an educational form of therapy, including touching different parts of the horse, 23 and the one yoga study included some physical aspects and also mental imagery when the exercises were too challenging. 29
This systematic review has some limitations. There was heterogeneity in the studies, especially with variability in interventions and outcomes. Although interventions that involved exercise may be beneficial for community-dwelling stroke survivors, the specific type of exercise with most benefit and the effects of duration are unclear. Given the lack of effect from support service interventions, we would suggest that future studies target their interventions to improve specific aspects of social participation, including the individual’s involvement in activities that provide interaction with the community and society. In addition, outcome measures that measure multiple characteristics of social participation such as social contacts as well as contributions to society should be used. Studies are needed to determine the optimal rehabilitation strategy for improving social participation. Future research should follow individuals for a longer period postintervention (eg, 6- to 12-month follow-up) to elucidate the effects of duration on improvements. In addition, the use of control groups matched for attention will help in understanding the impact of these interventions on social participation. This will ultimately advance knowledge about the rehabilitation strategy for promoting social participation in individuals with stroke.
Conclusion
The included studies provide evidence that rehabilitation interventions may be effective in improving social participation in individuals with stroke, especially if exercise is one of the components.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant support from the Canadian Institutes of Health Research (CIHR) (MOP-136965) and Social Sciences and Humanities Research Council (895-2013-1021), as well as fellowship support to A. Obembe from CIHR and the Michael Smith Foundation of Health Research.