
Abstract
Background. Stroke patients with mild-moderate upper extremity motor impairments and minimal sensory and cognitive deficits provide a useful model to study recovery and improve rehabilitation. Laboratory-based investigators use lesioning techniques for similar goals. Objective. To determine whether stroke lesions in an upper extremity rehabilitation trial cohort match lesions from the preclinical stroke recovery models used to drive translational research. Methods. Clinical neuroimages from 297 participants enrolled in the Interdisciplinary Comprehensive Arm Rehabilitation Evaluation (ICARE) study were reviewed. Images were characterized based on lesion type (ischemic or hemorrhagic), volume, vascular territory, depth (cortical gray matter, cortical white matter, subcortical), old strokes, and leukoaraiosis. Lesions were compared with those of preclinical stroke models commonly used to study upper limb recovery. Results. Among the ischemic stroke participants, median infarct volume was 1.8 mL, with most lesions confined to subcortical structures (61%) including the anterior choroidal artery territory (30%) and the pons (23%). Of ICARE participants, <1% had lesions resembling proximal middle cerebral artery or surface vessel occlusion models. Preclinical models of subcortical white matter injury best resembled the ICARE population (33%). Intracranial hemorrhage participants had small (median 12.5 mL) lesions that best matched the capsular hematoma preclinical model. Conclusions. ICARE subjects are not representative of all stroke patients, but they represent a clinically and scientifically important subgroup. Compared with lesions in general stroke populations and widely studied animal models of recovery, ICARE participants had smaller, more subcortically based strokes. Improved preclinical-clinical translational efforts may require better alignment of lesions between preclinical and human stroke recovery models.
Keywords
Introduction
Motor rehabilitation investigators typically select participants based on neurological impairments, not stroke lesion characteristics.1,2 These investigators typically enroll stroke patients with mild-moderate hemiparesis and few other neurologic deficits; this subgroup represents about 2% to 6% of the general stroke population.2-4 This reductionist approach of focusing on upper extremity motor impairment decreases heterogeneity and thus increases statistical power and precision. Investigators have identified these individuals as being particularly promising for motor recovery interventions, and likely to provide useful mechanistic information.
Investigators studying preclinical stroke recovery also focus on motor impairment, but in addition strive to create lesions that are highly reproducible with regard to size and location. The most studied ischemic stroke models include focal cortical injury with photocoagulation5-7 or injection of vasoconstricting substances8,9 and middle cerebral artery occlusion (MCAO).10,11 The most common intracranial hemorrhage (ICH) model12-18 produces hematomas in the striatum. Lesions in these preclinical models do not align perfectly with the general stroke population, 19 but do capture some of the main stroke syndromes. For example, half of all strokes in the general population are in the MCA territory,20-22 and MCAO models helped lead to successful development of acute therapies for stroke.23,24 What remains unclear is how well the lesions in these preclinical models mimic the lesions in participants recruited into stroke motor recovery trials. Major lesion differences between preclinical and clinical motor recovery studies could potentially hinder translational efforts.
There is a long-standing but unproven theory that lesion location and size are determinants of recovery and response to rehabilitation therapy. 25 Evidence in support of this theory comes from recent stroke recovery studies in humans suggesting that deep white matter lesions affecting the corticospinal tract (CST) cause much of the hemiparesis following stroke.26,27 This evidence was somewhat corroborated by neuroimaging data from patients with lower extremity weakness enrolled in a recent multicenter trial that showed high rates of lacunar infarction. 28 Lesion size may affect motor outcome in those with subcortical stroke. 29 It follows that if lesion size and location are truly important for recovery, then lesion differences between clinical trial samples and animal models may lead to discordant findings and impair translational efforts.
The stroke lesion attributes from large multicenter trials of upper extremity motor recovery have never previously been characterized, possibly because of the cost and complexity of adding research-quality imaging to phase 3 rehabilitation trials. We developed a method to overcome this challenge by using images obtained during routine clinical care to characterize the stroke lesions in participants enrolled in the Interdisciplinary Comprehensive Arm Rehabilitation Evaluation (ICARE) study. We then matched the stroke lesions from participants in ICARE to the animal stroke models most commonly used to study motor recovery of the upper limb. We theorized that a population selected for primarily motor impairments and few cognitive deficits would have small stroke lesions largely confined to subcortical locations, and therefore, not align well with common preclinical models of motor recovery.
Methods
Participants
Clinical poststroke neuroimages from participants prospectively enrolled in ICARE were collected and analyzed retrospectively. ICARE was a multicenter, single-blind, controlled trial that randomized participants with mild stroke and moderate upper extremity impairment to 1 of 3 outpatient rehabilitation therapy programs at 14 to 106 days poststroke. 3 The study was approved by the institutional review board at each site and all participants provided written informed consent. The ICARE population was 56% male and 42% African American; mean age was 60.7 years, with a mean upper extremity Fugl-Meyer score 42/66 (range 19-58) and a mean National Institutes of Health Stroke Scale Score 3.6 (SD 1.8). All had some ability to release a grasp on the affected side and no significant neglect, aphasia, or other cognitive impairments. The ICARE participants were representative of participants enrolled into other upper limb rehabilitation trials based on severity of upper extremity impairment and exclusion of cognitive deficits.2,4,30 The primary outcome measure was the change in the log-transformed Wolf Motor Function Test (WMFT) time score 1 year postrandomization. Mean improvement in motor performance score was substantial (54%), but ICARE found no significant differences in the primary outcome measure between groups at 1 year. 3
Neuroimaging/Clinical Lesion Characterization
Participants were enrolled in ICARE from 7 rehabilitation hospitals in the greater metropolitan area of Los Angeles, Atlanta, and the District of Columbia; these participants came from 55 acute care hospitals. Images were uploaded into the ICARE Neuroimaging Viewer, 31 a custom web-based system allowing the user to view multiple imaging sequences, draw regions of interest (ROIs), calculate lesion volumes, overlay lesion location templates (see below), and store lesion characteristics in an electronic database. Lesion characterization was performed by 2 vascular neurologists, M.A.E. who read all scans and A.W.D. who independently read 25 randomly chosen scans for interrater reliability. One imaging study was analyzed for each participant. Ischemic stroke lesions were identified on diffusion-weighted imaging (DWI) if ≤7 days from stroke onset, fluid-attenuated inversion recovery (FLAIR) if >7 days, or computed tomography (CT) when DWI or FLAIR was unavailable. Primary ICH were identified on CT; gradient echo (GRE) sequences were used when CT was not available. Lesion volume was estimated using the ABC/2 method 32 and by manually drawing ROIs on each axial slice to determine planimetric volume. Intraventricular hemorrhage was not included in ICH volume determinations. Stroke lesions were characterized as involving the cortical gray matter (first 2-4 mm along the cortical surface), cortical white matter (deep to cortical gray matter, superficial to basal ganglia), subcortical region, or a combination of these structures. Because of the heterogeneity of imaging studies, including the need for the same method to characterize both magnetic resonance imaging (MRI) and CT, lesion location analysis was performed using templates established for CT localization.33,34 The templates were slightly modified to combine smaller template subdivisions into larger divisions and to include the basilar and vertebral artery vascular territories in the posterior circulation using MIPAV software and anatomical maps 35 (see Supplementary Figures 1-5 online). Figure 1 provides a description of template analysis procedures. The predominant area was chosen to reflect the template subdivision located in the 3-dimensional center of the stroke lesion. To further localize posterior circulation lesions, we determined whether lesions were centered in the midbrain, pons, medulla, cerebellar hemisphere, or cerebellar vermis. Old strokes >1 cm in diameter were identified on FLAIR or CT. Leukoaraiosis severity was determined using the age-related white matter changes (ARWMC) scale. 36 To capture typical vascular neurology nomenclature, clinical vascular territory analysis was also performed separate from the template localization only for the ischemic strokes.
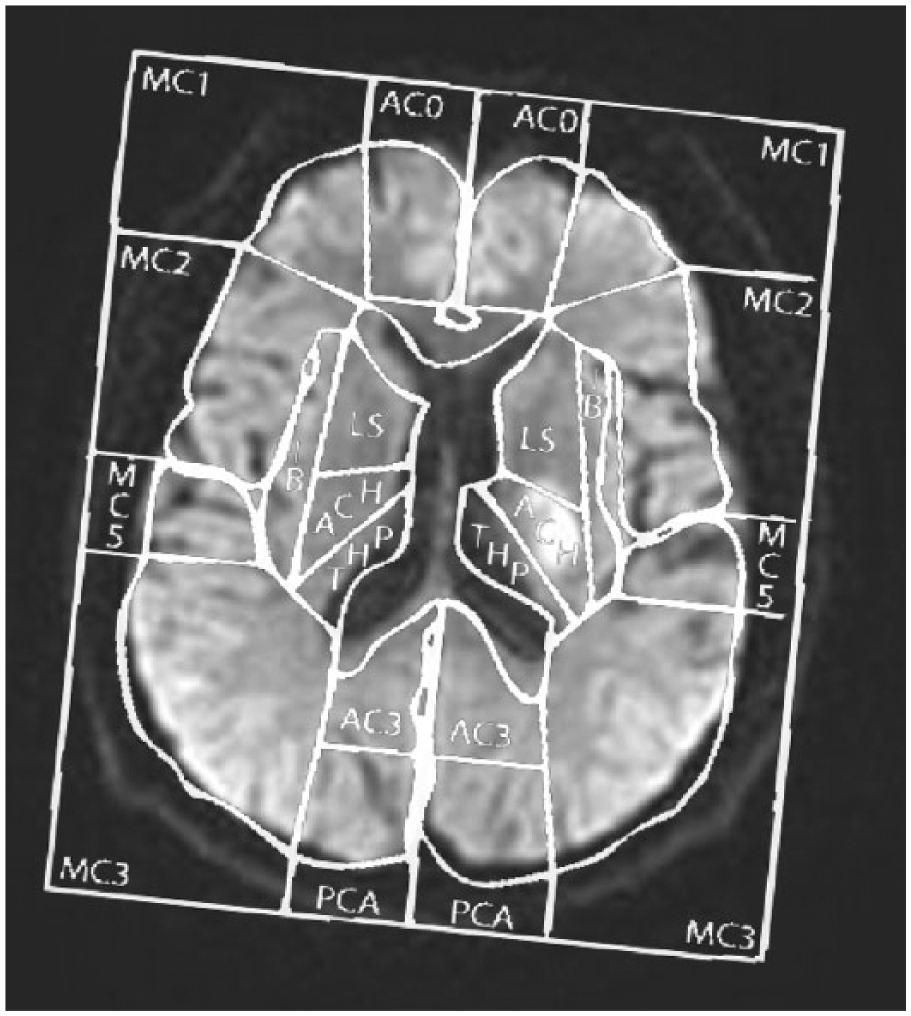
Template analysis using the ICARE (Interdisciplinary Comprehensive Arm Rehabilitation Evaluation) Neuroimaging Viewer. After identifying the group of templates corresponding to the angle at which the head was scanned, the template that best matched the axial slice was chosen and overlaid on top of the diffusion-weighted image (DWI) image. The template was rotated clockwise and enlarged to match the outer border of the brain. This process was repeated for each axial slice to be sure the predominant area captured the template subdivision in the 3-dimensional center of the lesion. In this example, the predominant area was scored as anterior choroidal (ACH). AC0/AC3, anterior cerebral artery subdivisions; MC1/MC2/MC3/MC5, middle cerebral artery subdivisions; PCA, posterior cerebral artery; IB, insular branches; LS, lenticulostriates; THP, thalamoperforating.
Preclinical Model Comparisons
To estimate the percentage of the ICARE population reflected by preclinical ischemic stroke models, we selected the preclinical models most commonly used to study upper limb recovery. For ischemic stroke, this entailed selection of models from all forelimb training studies in a recent meta-analysis 37 with the exception of the temporary MCAO models.38,39 The wide variability in lesion size in temporary MCAO models depending on occlusion time did not facilitate direct comparisons with our clinical population. For ICH, we included models from all the studies in a recent meta-analysis 40 that assessed forelimb recovery and measured hematoma volumes 3 days after stroke. In addition to the preclinical models included from the meta-analyses above, we added subcortical ischemic41-45 and hemorrhagic 46 stroke models that create lesions localized to subcortical areas controlling the forelimb. These capsular stroke models were mostly developed later than the models in the above-cited meta-analyses and were felt to be particularly relevant given the large percentage of subcortical strokes discovered in the ICARE population. All preclinical studies used for comparison, including the capsular models, were of intermediate or high quality according to the methods of Schmidt et al. 37
We then matched the preclinical and clinical lesions based on relative size and location. For lesion size comparisons, total MCA infarct volume in humans was estimated at 300 mL. 47 The total hemispheric brain volume was estimated at 200 mm3 for mice, 48 500 mm3 for rats, 49 and 600 mm3 for humans. 50 Relative lesion size in the mouse and rat were therefore estimated at 1/3000 and 5/6000 the lesion size in humans, respectively. Location comparisons were performed as follows. Because preclinical models using electrocautery of surface vessels produce isolated cortical gray matter infarction, 51 they were matched to the number of ICARE participants with isolated cortical gray matter lesions. Although there is some heterogeneity in lesion size depending on technique, preclinical models that cause focal injury to sensorimotor cortex via injection of vasoconstricting substances52,53 or photocoagulation54,55 most often create a large cortical lesion that spares subcortical structures; they were matched to the number of participants with both cortical gray and cortical white matter injury. To match the lesions from animal models causing focal ischemia to the subcortical white matter controlling the forelimb41-45 we chose the number of participants with stroke confined to subcortical structures that also overlap the anterior choroidal subtemplate area, which contains the motor fibers passing through the posterior limb of the internal capsule (PLIC). For ICH, the most widely used model—injection of collagenase into the striatum12-18—was compared to the number of ICH participants with hematomas centered in the lenticulostriate region. The lesser used ICH model of collagenase injection into the internal capsule 46 was compared with the number of ICH participants with hematomas centered in the anterior choroidal template region.
Statistical Analysis
Means and standard deviations for normally distributed continuous variables, and median and interquartile ranges for nonnormally distributed continuous variables were computed. The percentages described in lesion comparisons are descriptive in nature. Interrater reliability was assessed using the weighted kappa statistic for the categorical variables, and Spearman’s correlation and Bland-Altman limits of agreement for continuous variables. Weighted kappa calculations were performed using R version 3.1.2; all other analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Results
Eighty-two percent of the ICARE participants had interpretable neuroimaging with stroke lesions identified. A total of 258 ischemic strokes (186 DWI/53 CT/19 FLAIR) and 39 primary ICHs (31 CT/8 GRE) were analyzed. Median infarct volume was small for both the ischemic stroke (1.8 mL) and ICH (12.5 mL) participants. Lacunar infarcts made up 46% of the ischemic stroke population based on a strict definition for which the stroke diameter could not exceed 20 mm in axial diameter. 56 There was high correlation between the 2 raters for planimetric volume (Spearman = 0.98, P < .001), template predominant area (K = 0.98) and clinical vascular territory (K = 0.95). Figure 2 shows the predominant area incidence map, representing the percentage of ischemic stroke and ICH participants with lesions centered in each of the template subdivisions. For the ischemic stroke participants, lesions were centered in the anterior choroidal (35%), basilar (25%), MCA (22%), anterior cerebral artery (ACA; 7%), lenticulostriate (3%), insular branch (3%), vertebral (2%), thalamoperforating (2%), and posterior cerebral artery (PCA; 1%) template subdivisions; most of the posterior circulation lesions were in the pons (84%). For the ICH participants, lesions were centered in the anterior choroidal (46%), thalamoperforating (26%), lenticulostriate (13%), basilar (5%), ACA (5%), MCA (3%), and insular branch (3%) template subdivisions.
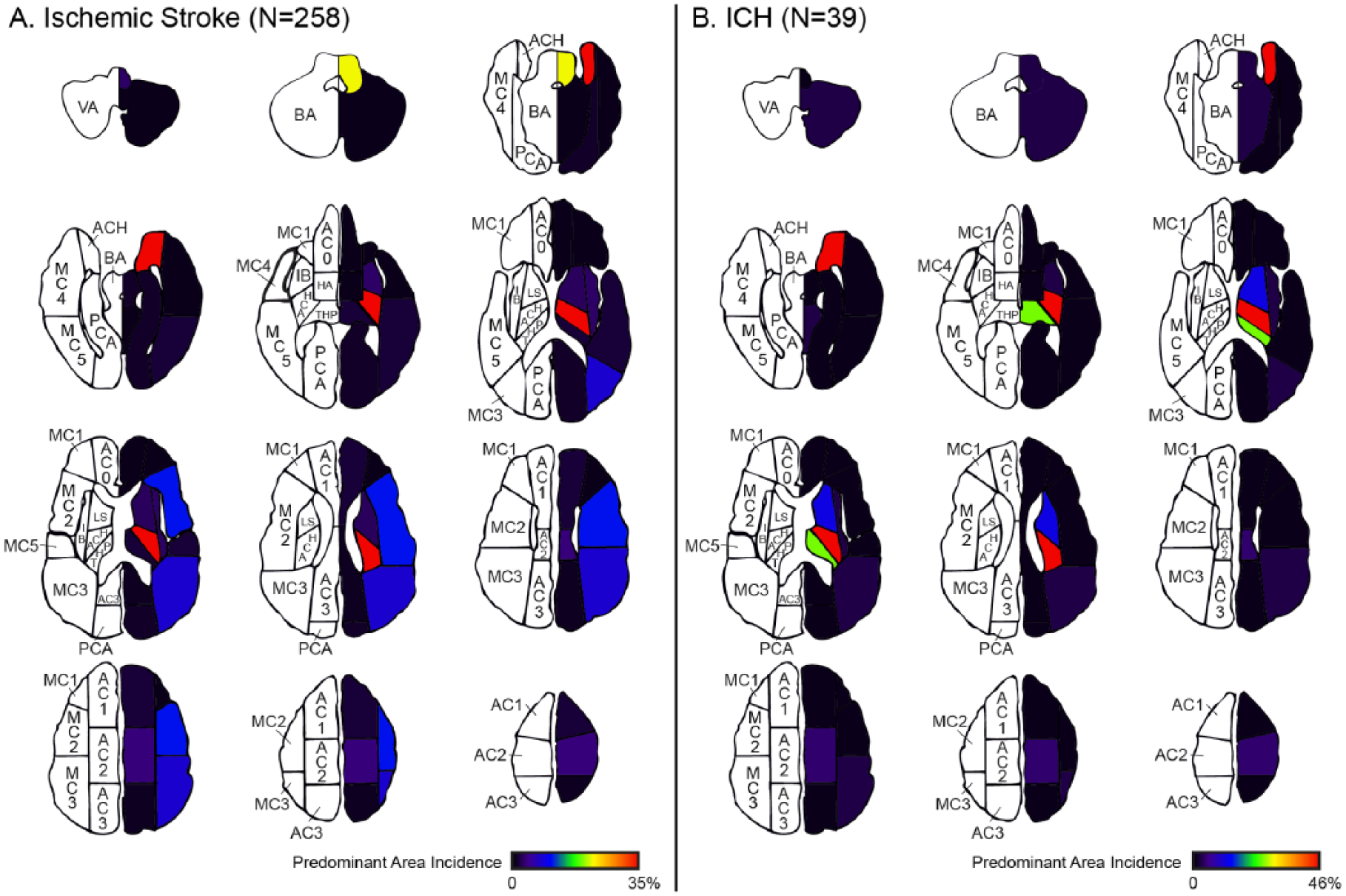
Map displaying the incidence of stroke lesions centered in each template subdivision (predominant area) for (A) Ischemic stroke participants and (B) intracranial hemorrhage (ICH) participants. The incidence was normalized to the template subdivision with the highest incidence, which was the anterior choroidal (ACH) for both ischemic stroke and ICH. To better delineate lesion involvement in the posterior circulation, the vascular territory data from the template analysis was replaced by the predominant area analysis for the brainstem/cerebellum. Note that the ACH vascular distribution extends into the anteromedial region of the temporal horns, but the vast majority of ACH involvement was confined to the internal capsule/basal ganglia. AC0/AC1/AC2/AC3, anterior cerebral artery subdivisions; MC1/MC2/MC3/MC4/MC5, middle cerebral artery subdivisions; PCA, posterior cerebral artery; HA, Heubner’s artery; IB, insular branches; LS, lenticulostriates; THP, thalamoperforating; BA, basilar artery; VA, vertebral artery.
We used lesion size and location data (Tables 1 and 2) to estimate the percentage of ischemic stroke and ICH participants that align with various preclinical stroke models (Table 3). With regard to lesion size, only 1 participant had a stroke lesion approaching the volume of a complete MCA infarct (Figure 3). The median volume for ischemic stroke in the ICARE human cohort corresponds to a 0.8 mm3 lesion in the mouse and a 1.5 mm3 lesion in the rat; the median ICH volume corresponds to a 4.2 mm3 lesion in the mouse and a 10.4 mm3 lesion in the rat. For frame of reference, preclinical ICH volume from the control groups of the 7 striatal models12-18 and the capsular model 46 was 21 mm3 and 7.1 mm3, respectively (note that all of these studies were in rats).
Lesion Characteristics.
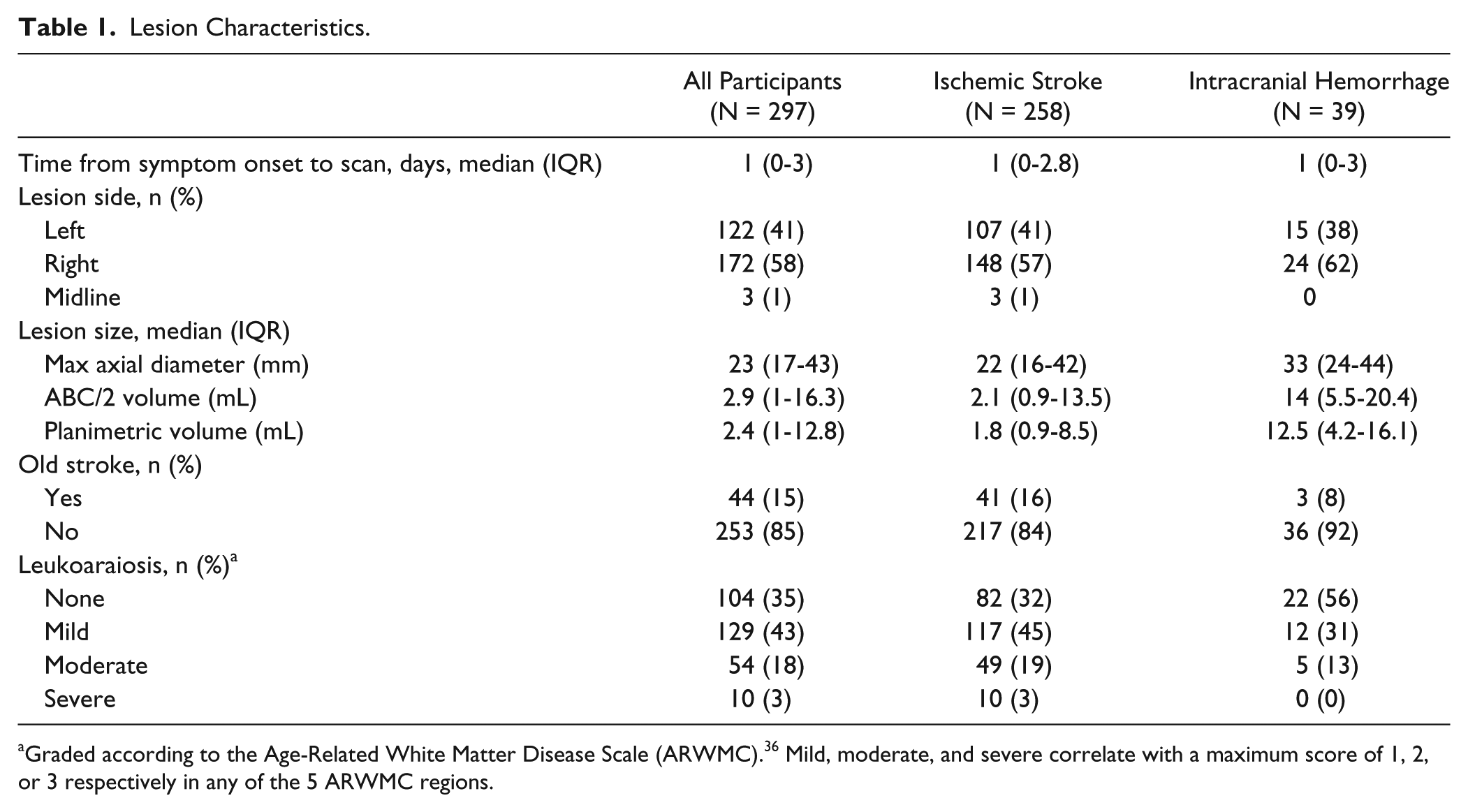
Graded according to the Age-Related White Matter Disease Scale (ARWMC). 36 Mild, moderate, and severe correlate with a maximum score of 1, 2, or 3 respectively in any of the 5 ARWMC regions.
Stroke Lesion Vascular Template Predominant Area, Depth, and Clinical Vascular Territory.
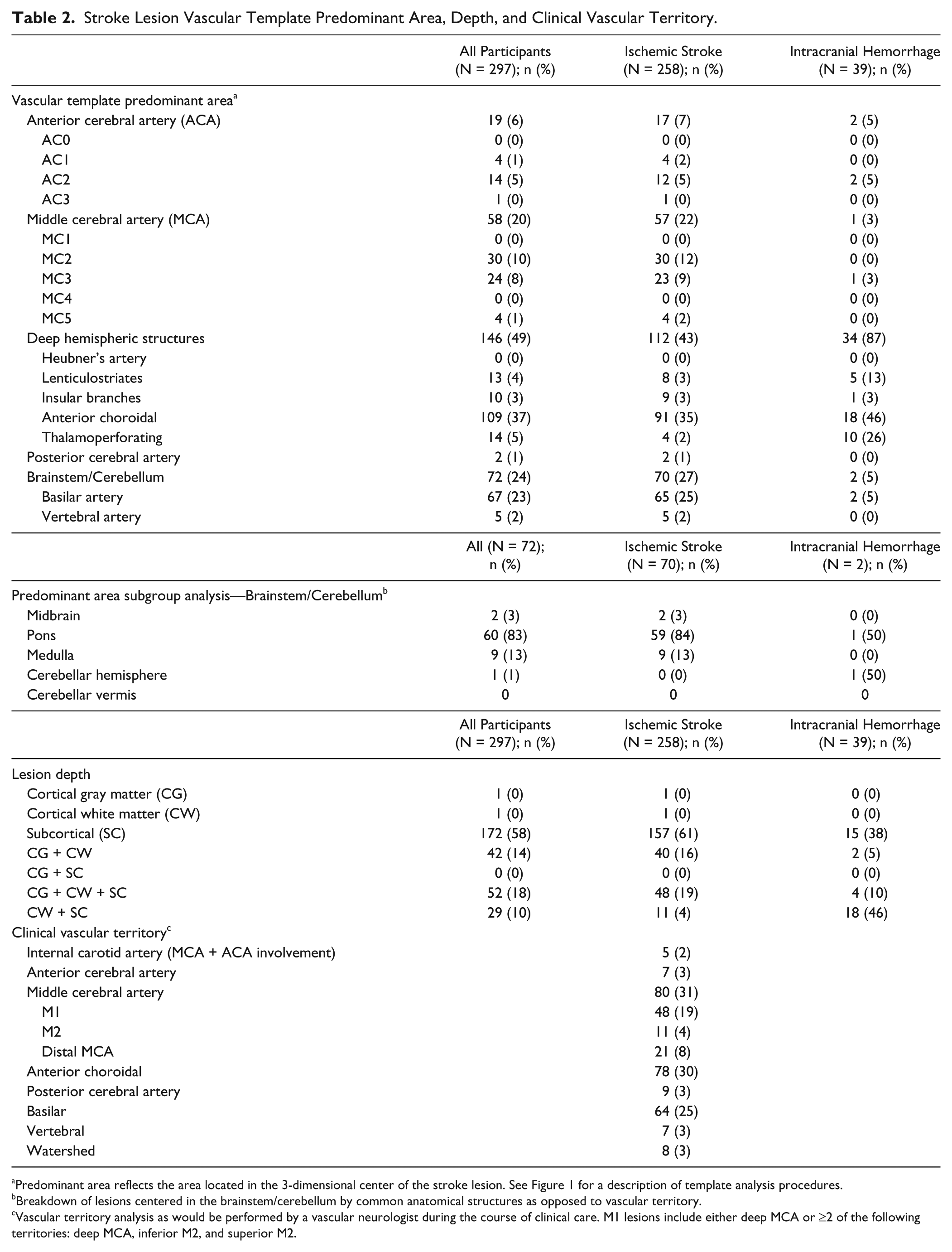
Predominant area reflects the area located in the 3-dimensional center of the stroke lesion. See Figure 1 for a description of template analysis procedures.
Breakdown of lesions centered in the brainstem/cerebellum by common anatomical structures as opposed to vascular territory.
Vascular territory analysis as would be performed by a vascular neurologist during the course of clinical care. M1 lesions include either deep MCA or ≥2 of the following territories: deep MCA, inferior M2, and superior M2.
Estimation of How Animal Models of Stroke Align With ICARE Population.
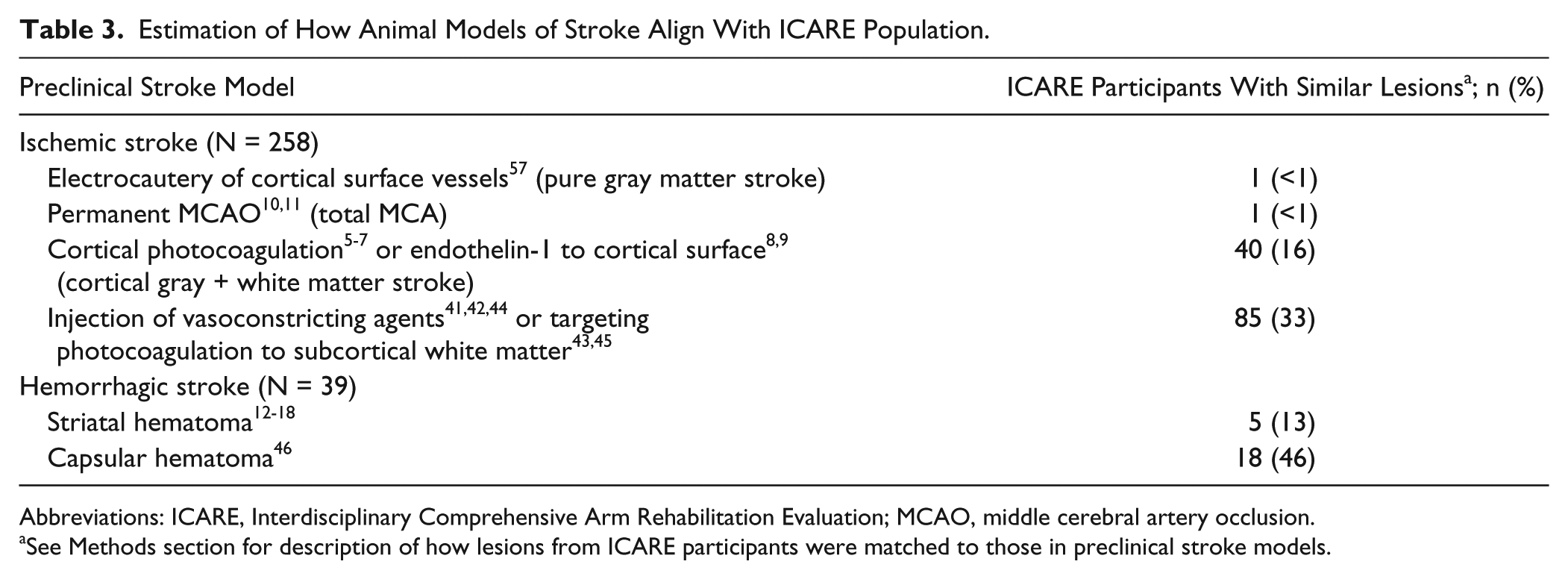
Abbreviations: ICARE, Interdisciplinary Comprehensive Arm Rehabilitation Evaluation; MCAO, middle cerebral artery occlusion.
See Methods section for description of how lesions from ICARE participants were matched to those in preclinical stroke models.
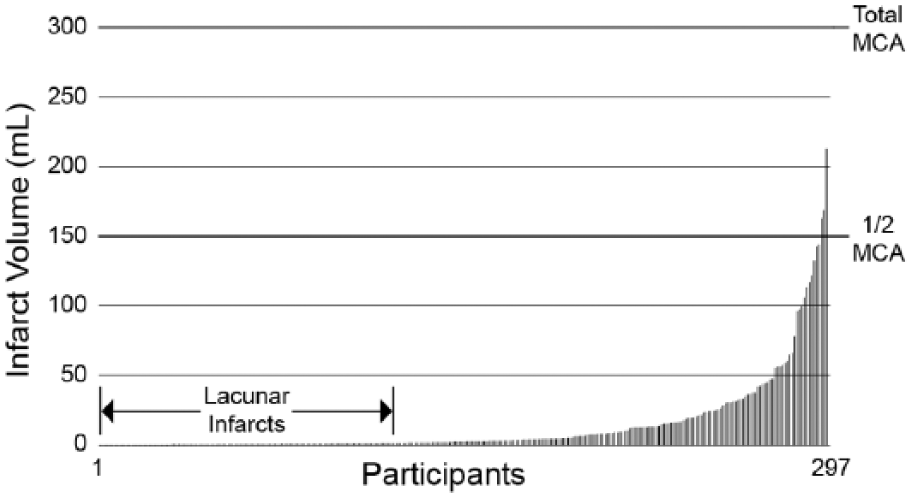
Stroke lesion planimetric volumes for ICARE (Interdisciplinary Comprehensive Arm Rehabilitation Evaluation) participants (n = 297). The y-axis on the right denotes the approximate volume of the middle cerebral artery (MCA) territory in humans.
For ischemic stroke lesion location, only 1 participant had a lesion confined to the cortical gray matter, suggesting that models employing electrocautery of surface vessels 51 reflect <1% of the ICARE population. Two preclinical models that have come into widespread use in recovery studies, photocoagulation5-7 or endothelin-1 injection8,9 to sensorimotor cortex, capture a modest subset of the ICARE population—40 participants (16%). Preclinical models that inject vasocontricting agents or target photocoagulation at the subcortical white matter controlling the forelimb41-45 best reflected the ICARE cohort. This subcortical stroke model would capture 85 of the ICARE participants (33%). For ICH location, the striatum injection model12-18 reflected 13% of the ICARE population, whereas the lesser used capsular injection model 46 matched 46% of the ICARE sample. In summary, more recent subcortical models of ischemic and hemorrhagic stroke best matched our clinical trial population with regard to lesion size and location.
Discussion
The relationships between brain lesion characteristics, recovery, and response to rehabilitation intervention remain controversial. One path toward resolution of the controversies is to study both animal and human models of stroke recovery, often in analogous interspecies studies. 58 This approach may be strengthened by aligning the models as much as possible to resolve whether lesion location, size, timing, and other variables are determinants of recovery or treatment response. Since many clinical investigators choose to study stroke patients with relatively isolated upper extremity motor impairments, we asked to what extent the lesions in this human sample resemble and differ from the animal models. We argue that this information is useful in translating the results of preclinical modeling into human studies, and to translate results from clinical trials back to the bench. To the extent that lesion location and size drive mammalian brain recovery and response to rehabilitation, misaligned animal and human models risk yielding incorrect or imprecise translation of findings between species. Should future studies show that lesion location and size do not drive clinical stroke recovery, then preclinical investigators interested in studying motor recovery can simply focus on motor phenotype with less regard for lesion characteristics.
First, while differences in lesion characteristics between this mild-to-moderately impaired subgroup from the general stroke population were expected, the extent of these differences is striking. Compared with the general stroke population, lesion volume was much smaller for both ischemic stroke (1.8 vs 9-35 mL)59,60 and ICH (12.5 vs 27 mL)61,62 participants. There was a higher percentage of lacunar infarction than typically seen in general stroke samples, (46% vs 13%-25%).20,63,64 Most of the strokes in ICARE were subcortical, and there was approximately half the incidence of MCA stroke reported in population-based studies (31% vs 45%-65%).20-22 ICARE participants had a much higher incidence of ischemic stroke in the anterior choroidal artery territory (30% vs 2%-8%)65-67 and the pons (23% vs 5%-11%),20,21,66,68 which corroborates reports that strokes causing motor impairment commonly overlap the CST.26,27 Note that there is a large literature of prior studies not cited above assessing lesion volumes in general stroke populations,32,69-73 but methodological concerns hindered proper comparison with our patient cohort. Though these prior studies all showed larger stroke volumes than the lesions seen in ICARE, they had inclusion/exclusion criteria that would select for larger or smaller strokes and were therefore not true population-based samples. Our findings demonstrate that participants recruited into upper extremity motor rehabilitation trials are markedly different with respect to lesion size and location than those in true general stroke populations, skewed toward those with small subcortical infarcts.
Second, we found that the lesions in the ICARE population rarely resembled the most common preclinical stroke models. Thus, to the extent that lesion location and size matter, animal model–based generalization about mammalian motor recovery may not apply to the typical human candidates currently enrolled in upper extremity motor recovery intervention trials. Permanent MCAO in rodents creates lesions that are proportionally orders of magnitude larger than the majority of the lesions seen in ICARE participants.10,11 Models employing more focal lesions, such as the classic motor plasticity studies in squirrel monkeys 51 or photocoagulation of sensorimotor cortex in rodents,5-7 are the right size; however, unlike the strokes in ICARE, the lesions are primarily confined to the cortex. For ICH, the striatum injection model typically creates hematomas that are larger and more anterolateral than those typical for ICARE participants.12-18 The discrepancies in infarct size and location described above may have significant consequences, similar to those discussed in the current STAIR committee guidelines, which outline methods to improve preclinical stroke studies in an effort to improve translation. 19
If lesion characteristics drive recovery and response to therapies, then more effort to converge the clinical trial samples and animal models would be needed. One approach could be to devote greater efforts to developing subcortical preclinical stroke models—particularly those targeting white matter tracts that control the forelimb. This important endeavor has begun. 74 A rodent model of anterior choroidal artery infarction exists, 75 but is complicated by variable infarct size and concurrent hypothalamic injury. The structures supplied by the anterior choroidal artery in humans include the medial temporal lobe, posterior putamen, PLIC, lateral thalamus, periventricular tail of the caudate nucleus, optic radiations, lateral geniculate nucleus, and the cerebral peduncle. 65 Injecting vasoconstricting agents41,42 or targeting photocoagulation43,45 directly at structures supplied by the anterior choroidal artery that contain the white matter tracts controlling the forelimb such as the PLIC may be the most straightforward approach to recreating ICARE-like ischemic stroke lesions in animals. There is also a preclinical model for ICH that targets the internal capsule. 46 This capsular injection model in the rat produces motor weakness with hematoma volumes (~10 mm3) similar to the relative lesion volume in the ICARE cohort and may therefore be preferred over the striatal model for testing motor rehabilitation strategies.
In developing these subcortical models, differences in brain and behavior between rodents and humans must be considered. Rodent brains contain 15% white matter by volume compared with 50% for humans. 76 In addition, rodents do not rely on the CST to control skilled forelimb movements, but rather the corticoreticulospinal tract (CRST) which runs parallel to the CST through the internal capsule.77,78 Capsular rodent models therefore explore a different cellular environment with behavioral measures that reflect disynaptic (CRST) rather than monosynaptic (CST) control pathways. As a result, subcortical models may require either larger lesions by volume or more sensitive measures of motor function to effectively study motor recovery. One might argue that creating pure lesions of the motor tracts more distal to the PLIC, such as with pyramidotomy 79 might effectively mimic the lesions seen in ICARE. We do not favor this approach, however, because brain ischemia itself induces endogenous repair mechanisms 80 that might be lost with such a model.
Other preclinical models also warrant consideration. Temporary MCAO models could capture a significant fraction of the lesions in our clinical trial population. Direct comparison between published studies and the ICARE cohort was made difficult, however, by the wide variability in lesion size depending on occlusion time. For ICARE, 31% of our participants had MCA strokes. Temporary MCAO models would not capture this entire fraction, however, because this technique does not create the small cortical lesions that one sees with distal MCA strokes in humans. Short occlusion times for temporary MCAO may best match the relative lesion volumes from the ICARE sample. We also acknowledge that other preclinical stroke models that do not represent a large proportion of lesions in rehabilitation trial participants remain important for studying particular aspects of motor recovery physiology. For example, cortical lesioning in squirrel monkeys 57 and the mouse 81 led to evidence of vicarious function in other cortical areas following recovery from injury. There may be cases, therefore, where preclinical investigators wish to closely match a clinical trial sample and others where motor physiology is the primary concern.
As an alternative to turning toward subcortical preclinical models, clinical rehabilitation investigators could instead perform trials that enroll participants with lesions that more closely resemble those found in the most common preclinical models. Preclinical models of MCAO eventually proved quite valuable in the general stroke population as evidenced by the remarkable efficacy shown in endovascular trials.23,82 Yet most large recovery trials in humans to date failed to show any improvement in the primary outcome measure when compared with usual and customary care.3,83,84 While some have argued these failures were a result of insufficient dose or timing of therapy, 85 perhaps recruitment of participants with infarct characteristics matching those of the supporting preclinical studies would allow the gains shown in preclinical models to be realized in humans. Developing clinical rehabilitation trials based on preclinical studies is challenging, but can be accomplished by mitigating some of the limitations inherent in studying human participants. 58 In this case, the challenge of selecting study participants by stroke lesions would need to be offset by enrolling persons with a wider range and combination of neurological impairments than is current practice. New outcome measures would need to be developed along with alternative statistical methods that embrace the multidimensional nature of rehabilitation and recovery. 86
Finally, while rigorous and detailed lesion data about stroke rehabilitation trial samples would be ideal to characterize the stroke lesions that lead to motor impairment, such data are not always necessary or feasible to collect. Additionally, there are few, if any high-quality large-sample human imaging databases that include detailed motor outcomes to inform stroke rehabilitation researchers. We demonstrated a new method for stroke lesion characterization, using vascular territory templates overlaid on routinely ordered clinical images that may be adequate for studies in which research-quality MRI is unavailable or unnecessary. This method has the advantage of accommodating clinical neuroimaging obtained at different centers and times from stroke onset without adding significant study-related cost or complexity. There are, of course, limitations to this approach. In the current study, for example, we suspect ICARE participants had a high incidence of lesion overlap with the CST, but cannot carefully quantify this possibility without diffusion tensor tractography. 27 In addition, these templates may not be accurate for participants with large variation in ventricular size or displacement due to cerebral edema. On the other hand, few large stroke motor rehabilitation trials have attempted any lesion characterization, and our method provides a straightforward approach to usefully classify stroke lesion features.
Conclusions
Participants enrolled between 14 and 106 days after stroke in a large upper extremity motor restoration trial have a higher incidence of small, subcortical strokes than the general stroke population. These lesion characteristics only rarely resemble the lesions in the most common preclinical stroke models, which are either too large or too superficial. If future studies prove that lesion characteristics drive recovery and response to treatment then greater efforts will need to be made to match the stroke lesions in preclinical and clinical study populations, perhaps by further developing subcortical stroke models.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Interdisciplinary Comprehensive Arm Rehabilitation Evaluation (ICARE) trial was funded jointly by the National Institutes of Health, National Institute of Neurological Disorders and Stroke (primary) and the National Center for Medical Rehabilitation Research of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (U01NS056256).
Supplementary material is available for this article online on the Neurorehabilitation & Neural Repair website.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.