
Abstract
Objective. Stroke survivors with motor deficits often have pyramidal tract atrophy caused by degeneration of corticospinal fibers. The authors hypothesized that the degree of atrophy correlates with severity of motor impairment in patients with chronic stroke and predicts the response to rehabilitation training. Methods. They performed a post hoc analysis of 42 hemiparetic patients (>6 months) who had been randomized to either 6 weeks of bilateral arm training with rhythmic auditory cueing (BATRAC) or dose-matched therapeutic exercise (DMTE). Arm function was measured using the Fugl-Meyer (FM) and modified Wolf Motor Function Test (WMFT). Structural MRI and diffusion tensor imaging (DTI) on the pontine level measured corticospinal tract (CST) atrophy by planimetric measurement of the mesencephalon (mesencephalic atrophy ratio) and fractional anisotropy (FA), respectively. Voxel-based lesion symptom mapping (VLSM) was used to determine the lesions associated with highest degrees of atrophy. The predictive value of CST atrophy for impairment and training response was analyzed. Results. CST atrophy predicted baseline motor arm function measured by the FM and WMFT. The authors found only a trend for the correlation with FA. No measure of atrophy predicted response to either BATRAC or DMTE. CST atrophy was higher with larger lesions and those that affected the CST. VLSM identified internal capsule lesions as being associated with highest CST atrophy. Conclusion. Larger lesions, internal capsule lesions, and those overlapping the pyramidal tract are associated with greater CST atrophy. CST atrophy explains in part the variability of baseline deficits but does not seem to predict the response to BATRAC or unilateral arm training on upper-extremity function.
Introduction
Several rehabilitation techniques for the upper extremity have proven effective in patients with hemiparetic stroke when initiated 6 or more months after onset. 1-4 Because therapeutic responsiveness varies, measures that can predict the likelihood of an individual’s response would be useful. Bilateral arm training with rhythmic auditory cueing (BATRAC) is one of the interventions that may improve arm function in some, but not all patients, with chronic upper-extremity motor impairment. 2,5-7
Atrophy and morphological changes of the cerebral peduncles caused by Wallerian and transsynaptic degeneration of pyramidal tract fibers are often observed in chronic stroke patients. 8-12 Wallerian degeneration is characterized by progressive degeneration of the distal portion of the injured axon and consecutively by degeneration of the myelin sheath and removal of myelin debris. Whereas Wallerian degeneration occurs fast in the peripheral nervous system (PNS; within days to weeks), it is very slow (months to years) and incomplete in the central nervous system (CNS) of mammals. Rapid clearance of myelin seems to result in an extracellular environment that promotes axon regeneration in the PNS, whereas in the CNS, the prolonged presence of myelin-associated inhibitors likely contributes to the failure of CNS axons to regenerate and consecutively leads to atrophy. 13 This process may lead to a slow progressive deterioration of function even long after a stroke. Preventing this decline is an important therapeutic target.
Magnetic resonance imaging (MRI) can be used to determine the degree of atrophy and the structural integrity of the corticospinal tract (CST). A recent study showed that the degree of mesencephalic pyramidal tract atrophy is a function of the extent of CST injury in the lesioned hemisphere. 10 Similarly, Warabi et al 14 had observed a positive relationship between descending motor tract injury and the mesencephalic CST atrophy in chronic stroke. The same investigators later found evidence that patients with CST atrophy greater than 60% showed limited recovery of hand function. 15 But reports on the relationship between CST atrophy and the response to rehabilitation or the severity of paresis remain controversial. 16-21
Diffusion tensor imaging (DTI) is an MRI technique often used to evaluate CST integrity by measuring the amount of directional diffusion of protons along white matter tracts (fractional anisotropy, FA). Two studies showed a correlation between DTI measures of CST atrophy, motor-evoked potentials (MEPs) as a measure of functional CST integrity, and arm function in those with chronic stroke. 20,22 Additionally, Stinear and colleagues 20 and others 22 reported poor improvements after a 30-day upper-extremity rehabilitation program in patients who had a high degree of CST damage on DTI (FA asymmetry index > 0.25) and absent MEPs.
We combined several neuroimaging methods to assess the relationship between CST atrophy, motor deficits at baseline, and response to bilateral arm training (BATRAC) and unilateral arm training (dose-matched therapeutic exercise [DMTE]). Voxel-based lesion symptom mapping (VLSM) was used to identify lesions that are associated with severe CST atrophy. 23 CST atrophy and integrity was determined by DTI and morphologically by measuring midbrain symmetry on axial MRI sections. 14
Materials and Methods
Study Participants
This report presents a post hoc analysis of a single-center, randomized controlled trial comparing BATRAC and DMTE (unilateral arm training based on conventional physiotherapy) in their effects on arm function (J.W. et al, unpublished data, 2010). We analyzed 42 patients who had undergone MRI scanning at baseline; 17 were in the BATRAC and 17 in the DMTE group. In all, 8 participants dropped out during training after receiving baseline assessments and MRI scanning. Reasons for dropping out were medical complications, personal or social issues, and difficulty with transportation to the training site. Whereas all participants received anatomical MRI scans, DTI was acquired in 23. The remaining participants did not tolerate the additional scan time of DTI. Two DTI scans had to be excluded from the analysis because of movement artifacts.
Patients were enrolled in the trial if they had residual upper-extremity hemiparesis following a single ischemic stroke 6 months or earlier prior to enrollment. All patients had the ability to initiate antigravity shoulder/elbow movement in flexion and extension in the transverse plane such that at least 3 inches of forward movement occurred. All participants had completed 3 to 6 months of conventional rehabilitation therapy. Inclusion criteria included adequate language and cognitive function to understand instructions. Patients with multiple clinical strokes, a history of other neurological disease, chronic pain, or emotional disorders were excluded. The study was conducted as part of the University of Maryland School of Medicine, National Institute on Aging—Claude D. Pepper Older Americans Independence Center in collaboration with the Division of Brain Injury Outcomes, Johns Hopkins University. All study participants provided written informed consent. The study was approved by the ethics committees of the participating institutions (the University of Maryland School of Medicine, the Baltimore Veterans Affairs Medical Center, and the Johns Hopkins University School of Medicine).
BATRAC Training
BATRAC training consisted of hour-long therapy sessions (four 5-minute movement periods interspersed with 10-minute rest periods) 3 times per week for 6 weeks. On receiving auditory cues at individually determined preferred rates of 0.67 to 0.97 Hz, participants pushed and pulled bilaterally, in synchrony or alternation, 2 T-bar handles sliding in the transverse plane. The control group received dose-matched unilateral therapeutic exercise (DMTE) for the upper extremities over the same time period. DMTE involved 4 exercises based on neurodevelopmental principles, 24 including thoracic spine mobilization, scapular mobilization, weight bearing with the paretic arm, and opening the hand with finger extension performed on the same 5-minute schedule as BATRAC. This treatment emphasizes handling techniques that facilitate body and limbs to assume “normal” positions. Participants were encouraged to actively move while performing the exercises. They were aware of the treatment differences but did not know that DMTE was a control intervention; thus, they reasonably expected an improvement regardless of group.
Assessments of Impairment and Function
Upper-extremity motor function was measured with the upper-extremity portion of the Fugl-Meyer Motor Performance Test (FM) 25 and the modified Wolf Motor Function Test 26 (WMFT). The mean time, which was required to perform the 14 tasks of the WMFT with the paretic arm and hand, was used in statistical analyses. Maximum time allowed for each task was 120 s. Assessments were conducted at a location separate from the training site and carried out by a tester (same person each time) blinded to group assignment.
MRI Data Acquisition and Analysis
MRI scanning was performed with a 1.5 T scanner (Philips, Eindhoven, Netherlands) at the Kirby Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, Maryland. Scanning was performed within 2 weeks before the start of training.
A T1-weighted sequence (3D-MPRAGE sequence; resolution 1 × 1 × 1 mm3, whole brain coverage) was used to measure the mesencephalic asymmetry ratio (MAR) and to characterize lesion location and size. The MAR was used to quantify CST atrophy at the level of the mesencephalon. The sizes of the left and right mesencephalon were measured planimetrically on an axial slice. The axial slice was parallel to the plane through the mamillary body and the posterior commissure. The axial slice was positioned midway between the mamillary body and upper rim of the pons. Planimetric measurements were conducted using Medical Image Processing, Analysis and Visualization software (MIPAV, Version 3.1.6) 27 MAR was defined as the ratio for the affected to the unaffected side.
Voxel-Based Lesion-Symptom Mapping (VLSM)
For Voxel-Based Lesion-Symptom Mapping (VLSM), 23 T1-weighted images were transformed into Talairach space 28 by rotation and scaling using Brain Voyager QX software (Brain Innovation BV, Maastricht, Netherlands). Binary lesion masks were produced based on T1-weighted scans by manually segmenting the lesion area. Areas of CSF intensity and hypodense regions at the boundary were combined to define the lesion. Lesion size was derived from the lesion mask by multiplying the number of voxels with voxel volume (1 mm3). Manual segmentation was performed using MRIcro (Chris Rorden, University of Nottingham, Great Britain). Masks with right-hemisphere lesions were flipped so that the lesion was always on the left. The binary lesion masks of each participant were entered into the VLSM software (http://crl.ucsd.edu/vlsm, based on Matlab, Mathworks Inc, Natick, MA). For each of these voxels, participants were divided into 2 groups, whether or not that voxel was included in the lesion mask. To keep the number of participants in those groups sufficient for statistical comparisons, only voxels that were part of 3 or more lesion masks were considered. The MAR values for both groups were then compared using t tests, resulting in a t value for each voxel. The color-coded map of the t values of all voxels was then overlaid onto a healthy brain template using a threshold of P ≤ .05. Brain regions with significant t values were localized using the Talairach daemon. 29
Assessment of Direct CST Injury
To measure the degree of CST injury, the overlap of each stroke lesion with the CST was determined counting the number of common voxels in the lesion mask and a CST region of interest (ROI). The CST ROI was obtained from a DTI-based fiber tract atlas in Talairach space. 30 In addition to the absolute number of common voxels, the percentage overlap was calculated as the quotient between common voxel number and the number of all voxels in the CST ROI.
Diffusion Tensor Imaging
DTI data were acquired using a single-shot, echo-planar imaging sequence with sensitivity encoding (SENSE, parallel-imaging factor of 2.5 31 ). The imaging matrix was 96 × 96 with a field of view of 240 × 240 mm2 (nominal resolution, 2.5 mm), zero-filled to 256 × 256 pixels. Transverse sections of thickness 2.5 mm were acquired parallel to the anterior commissure to posterior commissure line. A total of 50 to 55 sections covered the entire brain and brainstem without gaps. Diffusion weighting was encoded along 30 independent orientations, 32 and the b value was 700 s/mm2. Five additional images with minimal diffusion weighting (b ≈ 33 s/mm2) were also acquired. To enhance the signal-to-noise ratio, this protocol was repeated 3 times. Fractional anisotropy (FA) of pontine CST fibers was measured to assess CST integrity, as described in detail elsewhere. 33 The FA ratio was built between FA of unlesioned and lesioned CST. To allow comparison with other studies (eg, reference 20), lateralization indices were also calculated for FA: difference over the sum (FA unlesioned − FA lesioned)/(FA unlesioned + FA lesioned).
Statistical Analyses
To assess therapy response, general linear models were used to predict the change in outcome variables (FM, WMFT) across time (difference post-pre), one for each variable. Independent variables included group (comparison BATRAC vs DMTE) and the baseline value of the respective dependent variable. Additionally, within-group comparisons (paired t test; difference in test performance: posttraining − pretraining) were conducted for each group. General linear modeling was used to determine lesion parameters associated with CST atrophy and to analyze the predictive value of lesion and atrophy parameters for baseline deficit and therapy response. Separate models were computed for each dependent variable, CST atrophy, baseline WMFT, baseline FM, change in WMFT, and change in FM over the training period. Independent variables were CST atrophy (MAR, for baseline deficit and therapy response models), lesion size, lesion location (cortical vs subcortical), time since stroke, age, and CST damage (overlap between lesion and CST). Separate models were computed to test the influence of FA on the dependent variables because DTI data were only available in a subset of patients. Independent variables were entered and removed from the models in a stepwise fashion using P < .25 as entry and then P > .05 as a criterion for removal. Interactions were included in the model and removed if insignificant. Data are expressed as mean ± standard deviation. A 2-tailed P < .05 was considered significant.
Results
The results of the parent randomized-controlled trial about the efficacy of BATRAC therapy versus DMTE will be reported. Briefly, significant improvements in FM and modified WMFT were shown for both groups without between-group differences. Basic demographic and clinical characteristics of the study participants are provided in Table 1. Whereas all patients included here underwent FM testing (n = 42), WMFT scores were only available in 36 patients. In the present sample of 34 patients (BATRAC/DMTE = 17/17) in whom MRI scans as well as baseline and posttraining functional data were available, there was a significant improvement in WMFT in the BATRAC group (−2.9 ± 2.4 s; range, +3.6 to −12.9 s; t = 2.79; degrees of freedom (df) = 16; P = .01) and a trend of improved function in FM score for BATRAC (+0.94 ± 2.9 points; range, −2 to +5; t = −1.36; df = 16; P = .19) and in both FM and WMFT in DMTE (+1.3 ± 3; range, −3 to 5; t = −1.77; df = 16; P = .1, respectively, −3.0 ± 5.3 s; range, +1.8 to 13.0 s; t = −1.9; df = 10; P = .1). Repeated-measures ANOVA revealed no significant time-by-group interactions for both measures (FM: F(1, 32) = 0.12, P = .73; WMFT: F(1, 26) = 0.001, P = .98). See Table 1.
Baseline Characteristics and Therapy Response
Abbreviations: BATRAC, bilateral arm training with rhythmic auditory cueing; DMTE, dose-matched therapeutic exercise; MAR, mesencephalic asymmetry ratio; FM, Fugl-Meyer; WMFT, Wolf Motor Function Test.
Between-group comparison (t test; BATRAC vs DMTE).
Fisher Exact Test.
N = 23.
Functional change = therapy response as defined by the difference of scores: posttraining − pretraining.
MANOVA (time × group interaction; BATRAC vs DMTE)
Within-group comparison (paired t) significant by P < .05.
Lesion Profiles Predicting CST Atrophy
In addition to a correlation between CST damage (overlap CST-lesion) and lesion size (cortical: r = 0.73, P = .0001; subcortical: r = 0.89, P < .0001), both variables independently predicted CST atrophy—that is, MAR (size: r = −0.50, P = .035; CST overlap: r = −0.49, P = .038, Figure 1). Both factors together explained 31% of the variability of MAR. Interactions between lesion size, CST damage, and lesion location (cortical vs subcortical) were insignificant and were removed from the model. Lesion location, age, and time since stroke did not explain the variability of MAR. For those in whom DTI was available, the FA ratio did not correlate significantly with MAR (r = 0.1).
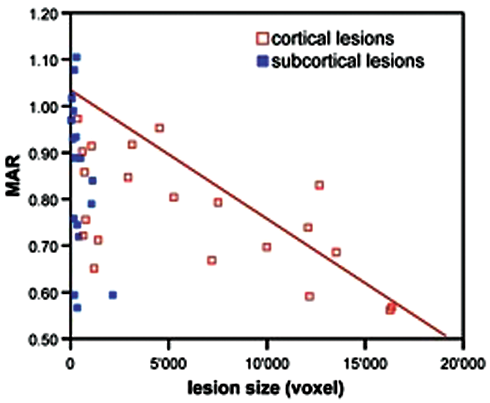
Relationship between lesion size and mesencephalic atrophy ratio (MAR) for cortical and subcortical lesions in all participants (n = 42): lower MAR values indicate higher degrees of atrophy
VLSM analysis was used to identify lesion patterns that were associated with CST atrophy (n = 42). VLSM can only identify those brain regions that are lesioned in 3 or more participants in the sample. Within this compound brain area (Figure 2A), lesions in the internal capsule were statistically related to higher degree of ipsilesional CST atrophy (t = 2.522; P < .01); see Figure 2B.
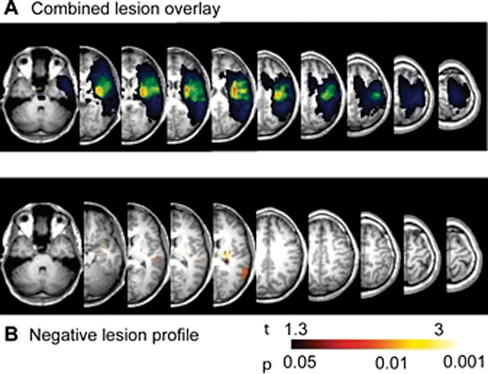
Overlay of all lesions included in the sample (n = 42). B. Voxels predicting high degrees of corticospinal tract atrophy (P < .01)
CST Atrophy, Baseline Function, and Therapy Response
High CST atrophy predicted low arm function (baseline FM score: r = 0.39, P = .014; WMFT time: r = −0.35, P = .042; Figure 3). FA was not significantly related to baseline arm function, but trends were noted for both baseline FM score (ratio: r = 0.4, P = .06; lateralization index: r = −0.41, P = .051) and baseline WMFT (ratio: r = −0.43, P = .09; lateralization index: r = 0.46, P = .08). No parameter that characterized lesion morphology (size, location, CST overlap) and atrophy (MAR, FA) predicted therapy response in the BATRAC or DMTE groups or in all participants combined.
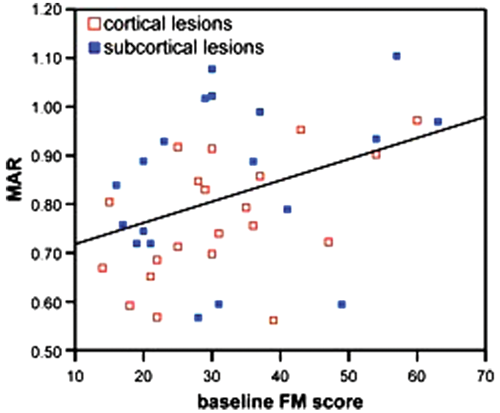
Correlation between arm function and corticospinal tract atrophy in all participants (n = 42). Lower mesencephalic asymmetry ratio (MAR) values—that is, higher atrophy—are associated with lower Fugl-Meyer (FM) scores—that is, lower arm function
Discussion
CST atrophy measured at the level of the mesencephalon occurs with larger cortical or subcortical lesions affecting the CST. Although chronic upper-extremity motor deficits are associated with high degrees of CST atrophy, atrophy does not influence response to BATRAC or DMTE in chronic stroke survivors.
Warabi et al 14 reported an association between lesion size and location and mesencephalic atrophy in 89 chronic stroke survivors. Mark et al, 10 however, did not find infarct size to predict atrophy in their sample of 34 chronic stroke survivors but reported that CST atrophy was related to the degree of overlap CST damage (CST-lesion overlap) as we observed in our sample. Consistent with this observation is the VLSM analysis that identified lesions in the internal capsule, that is, subcortical lesions strategically affecting the CST, to be specifically prone to produce CST atrophy. Our data also show a relationship between the size of cortical strokes and CST atrophy (Figure 2A) indicating that large cortical lesions also cause atrophy. One limitation of planimetric measurement of mesencephalic peduncular atrophy is that it does not encompass the CST exclusively, and results might be influenced by degeneration of other corticofugal tracts as well.
Larger lesions themselves seem to be associated with more severe deficits in the acute phase as well as 3 months after stroke. 34-38 Some reports, including ours in chronic stroke, however, have not found this relationship. 39,40 Certainly, lesion location influences the size–deficit relationship. Direct correlations may only exist as long as lesions within the same functional brain system are compared. 15,36,38,41 For example, even larger lesions affecting or extending into frontal areas may be clinically silent, at least if patients do not undergo neuropsychological testing for impairments. Therefore, the combination of size and location (“lesion profile”) may be required to determine impairments and prognosis. 35,37
Although the lesion profile did not predict impairment severity here, CST atrophy did. This observation is in accordance with the results of 2 recent studies. 20,22 However, the conclusion that atrophy causes arm impairment is premature because disuse of the arm as a consequence of the initial deficit may have contributed to CST atrophy.
No lesion or atrophy parameter predicted responsiveness to BATRAC or DMTE. One previous report showed less benefit from a 30-day unilateral upper-extremity training program in patients with chronic stroke who had greater CST damage, which was determined by DTI and transcranial magnetic stimulation. 20 Differences in clinical baseline impairment and the degree of CST disintegration—patients in the study by Stinear et al 20 had markedly lower baseline FM scores (16 ± 7.3 vs 31.9 ± 12.5) and greater CST damage than our patients—may explain contrasting results. Stinear et al reported predictive effects only for patients in whom no MEPs were evoked by transcranial magnetic stimulation. Those patients showed an FA lateralization index >0.25 and did not improve at all. We cannot rule out that a similar association exists in a subset of our patients because we have no MEP data, and only 3 patients (13%) had an FA index >0.25. Thus, it may be that only severe atrophy may negatively affect therapy responsiveness. The benefit of rehabilitation therapies may additionally be determined by the ability of the nonlesioned brain to undergo functional reorganization or neuroplasticity. 5 Consequently, factors predicting therapy response may be found in the unaffected rather than in the lesioned brain at least for bilateral training. Alternatively, reorganization may involve cortical and subcortical networks that exclude the mesencephalon.
FA showed only a trend toward an association with motor deficits. This may either be the consequence of low statistical power as a result of a small sample or may reflect methodological limitations, for example, DTI being very sensitive to motion artifacts.
In conclusion, this study suggests that larger lesions and those that affect the CST are associated with severe CST atrophy at the level of the mesencephalon. CST atrophy predicts motor impairment severity in chronic stroke survivors. CST atrophy, however, had no negative impact on the effectiveness of bilateral or unilateral rehabilitation training.
Footnotes
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the France-Merrick Foundation, the Eleanor Naylor Dana Charitable Trust and the Robert-Bosch Foundation (Forschungskolleg Geriatrie).