
Abstract
Background. Enhancement of sensory input in the form of repetitive peripheral sensory stimulation (RPSS) can enhance excitability of the motor cortex and upper limb performance. Objective. To perform a systematic review and meta-analysis of effects of RPSS compared with control stimulation on improvement of motor outcomes in the upper limb of subjects with stroke. Methods. We searched studies published between 1948 and December 2017 and selected 5 studies that provided individual data and applied a specific paradigm of stimulation (trains of 1-ms pulses at 10 Hz, delivered at 1 Hz). Continuous data were analyzed with means and standard deviations of differences in performance before and after active or control interventions. Adverse events were also assessed. Results. There was a statistically significant beneficial effect of RPSS on motor performance (standard mean difference between active and control RPSS, 0.67; 95% CI, 0.09-1.24; I2 = 65%). Only 1 study included subjects in the subacute phase after stroke. Subgroup analysis of studies that only included subjects in the chronic phase showed a significant effect (1.04; 95% CI, 0.66-1.42) with no heterogeneity. Significant results were obtained for outcomes of body structure and function as well as for outcomes of activity limitation according to the International Classification of Function, Disability and Health, when only studies that included subjects in the chronic phase were analyzed. No serious adverse events were reported. Conclusions. RPSS is a safe intervention with potential to become an adjuvant tool for upper extremity paresis rehabilitation in subjects with stroke in the chronic phase.
Introduction
Stroke is a leading cause of disability worldwide.1,2 Upper limb paresis is observed in 87% of stroke survivors, 3 but the quality of the evidence for interventions to improve upper limb motor function is controversial.4,5
Strategies to enhance motor performance by augmentation of afferent information from the paretic upper limb are based on the key role of sensory input on motor performance and on findings of worse recovery of hemiparesis in subjects with sensory impairment.6,7 Increased afferent input is provided during motor performance of the paretic limb in rehabilitation strategies such as constraint-induced movement therapy and robot-assisted training,4,5 or in the absence of overt movements in interventions such as electrical peripheral nerve stimulation, muscle tendon vibration and cutaneous stimulation.
The terms transcutaneous electrical stimulation and neuromuscular stimulation are often used to designate a variety of techniques in which electrical stimuli are noninvasively applied to the skin or also to muscles and nerves. The goals of electrical peripheral nerve stimulation, muscle tendon vibration or cutaneous stimulation are to facilitate motor performance or learning 6 by offering intensification of sensory input from the paretic limb.
In repetitive peripheral sensory stimulation (RPSS), in particular, trains of electric pulses are delivered to peripheral nerves by surface electrodes at an intensity that evokes paresthesias but minimal or no motor responses. The duration of each pulse is 1 ms, the duty cycle, 1 second (500 ms on, 500 ms off) and the frequency of pulses within the trains, 10 Hz. Stimulation is delivered for 2 hours. 8 These parameters were initially chosen to optimally activate proprioceptive and large cutaneous sensory fibers 9 and increase excitability of the contralateral motor cortex to transcranial magnetic stimulation (TMS) in healthy subjects.8,10 Later, it was demonstrated that this paradigm of stimulation enhances cortical excitability of motor representations from the stimulated body part in rats 11 and in human subjects with stroke. 12 Also, when associated with motor training over 2 weeks, RPSS decreases gamma event-related desynchronizations in the precentral gyrus of the hemisphere affected by stroke in humans. 13
These results encouraged research about the usefulness of RPSS to decrease motor impairments or improve function in subjects with stroke. The RPSS technique is inexpensive and straightforward but until now, the evidence-base of this intervention in subjects with stroke had not been thoroughly assessed. The aim of this systematic review and meta-analysis was to evaluate the evidence of benefit of RPSS on improvement of motor performance of the paretic upper limb in subjects with stroke. A previous systematic review of sensory transcutaneous electrical stimulation included not only RPSS studies but also studies involving other techniques of peripheral electrical stimulation. 14 Because of the variability between studies and of insufficient data, a meta-analysis could not be performed. Another systematic review addressed parameters of peripheral electrical stimulation able to induce cortical plasticity. Again, studies that used various parameters of stimulation were evaluated and the authors concluded that more research was required to determine optimal paradigms. 15 To avoid the inability to reach conclusions by analyzing results of studies that applied different parameters of stimulation, and because there was a firm physiological construct supporting the RPSS paradigm initially described by Ridding et al, 8 we opted to focus on studies that applied this paradigm.
Methods
Literature Review
We searched studies published between 1948 and July 2016. The articles were manually searched on Medline (1948 to July 2016), the Cochrane Register of Controlled Trials (CENTRAL—2015, Issue 9), the Latin American and Caribbean Health Sciences Literature (LILACS—1982 to July 2016), and the Database Research in Stroke (DORIS), by 3 reviewers. We also searched for trials registered on Clinicaltrials.gov. Shortly before submitting the manuscript, a new search was made for articles published between August 2016 and December 2017. The index terms were: evoked potentials, somatosensory, stroke, cerebrovascular disease. The systematic review was registered with PROSPERO under CRD42016046013.
Selection Criteria
We searched for crossover, randomized controlled trials (RCTs), and quasi-randomized trials testing the hypothesis that RPSS can improve motor performance of the paretic hand of patients with stroke if compared with other treatments, whether administered in isolation or as an add-on therapy prior to motor training. We included studies that evaluated (1) men and women aged ⩾18 years; (2) with history of single or recurrent, ischemic or hemorrhagic stroke; (3) assessed upper limb motor outcomes such as the Jebsen-Taylor Test (JTT),16,17 and the Upper Limb Fugl-Meyer Assessment of Motor Recovery After Stroke (FMA) 18 ; (4) applied RPSS, either alone or before motor training, to the median, ulnar, or radial nerves using noninvasive electrodes placed on the skin with the parameters described by Ridding et al 8 ; (5) compared effects of active RPSS with those of a control intervention; (6) provided individual data, either in the manuscript or after requests sent to authors. We excluded studies that lacked behavioral motor outcomes (for instance, studies that only evaluated cortical excitability).
For studies that applied RPSS alone or with other types of treatment such as TMS or transcranial direct current stimulation (tDCS), only the results of the intervention “RPSS alone” were analyzed. For crossover studies, only results of the first session of treatment were analyzed.
Data Extraction
Three authors (AAS, SMA, and JC) independently verified the title and abstracts of the studies. Duplicate articles were removed. Inclusion of the trials was made by agreement between the reviewers, and a fourth author (ABC) was called in case of conflicts, to reach a final decision.
A data extraction form was prepared for evaluation of the articles using the selection criteria. The forms were completed independently and encompassed the following items: participants, interventions, comparisons, outcomes, study design (PICOS); methodology; follow-up period; and adverse events. Authors of the studies were contacted and unpublished results that could be relevant to this systematic review were requested.
Data Analysis
The risk of bias (methodological quality assessment) of studies included in the review was assessed by the Cochrane Collaboration’s tool. This tool assesses 6 domains (generation of the allocation sequence, concealment of the allocation sequence, blinding, incomplete outcome data, selective outcome reporting and other biases). 19
The data extracted from the selected trials were analyzed in Cochrane’s software (RevMan 5.3). Continuous data were analyzed with means and standard deviations of differences in performance before and after active or control interventions. We only included studies that provided individual data so that we could calculate standardized mean differences for different outcomes. Standardized mean differences allow conversion of all outcomes to a common scale so that studies that use different assessment tools can be compared by other authors.5,20,21
We used a random-effects model to provide a conservative estimate of the effect of individual treatments on motor outcomes, regardless of the level of heterogeneity. The heterogeneity was verified using the heterogeneity test (I2) to calculate and compare the results considering different sample sizes, study design, and outcome results. For studies with more than one outcome, we analyzed measures related to activity limitation or to body function and structure according to the World Health Organization International Classification of Function, Disability, and Health (ICF). 4 First, we analyzed outcomes of body structure and function together with outcomes of activity limitation, in studies that included subjects in the subacute and chronic phases after stroke. We also intended to perform subgroup analyses according to the type of outcome (activity limitation or body function and structure), the number of stimulated nerves (one or more than one), phase after stroke (subacute or chronic) 22 and performance or not of RPSS as an add-on therapy to motor training.
Results
Selection of Studies
From the 14 papers selected for full-text reading, 9 (64.3%) were excluded (Figure 1). This review selected 5 studies that provided all the individual data needed to conduct the meta-analysis, considering the information reported in the articles and the answers to e-mails requesting the data. The reasons for exclusion of 9 of 14 manuscripts are listed in Supplementary Table 1.
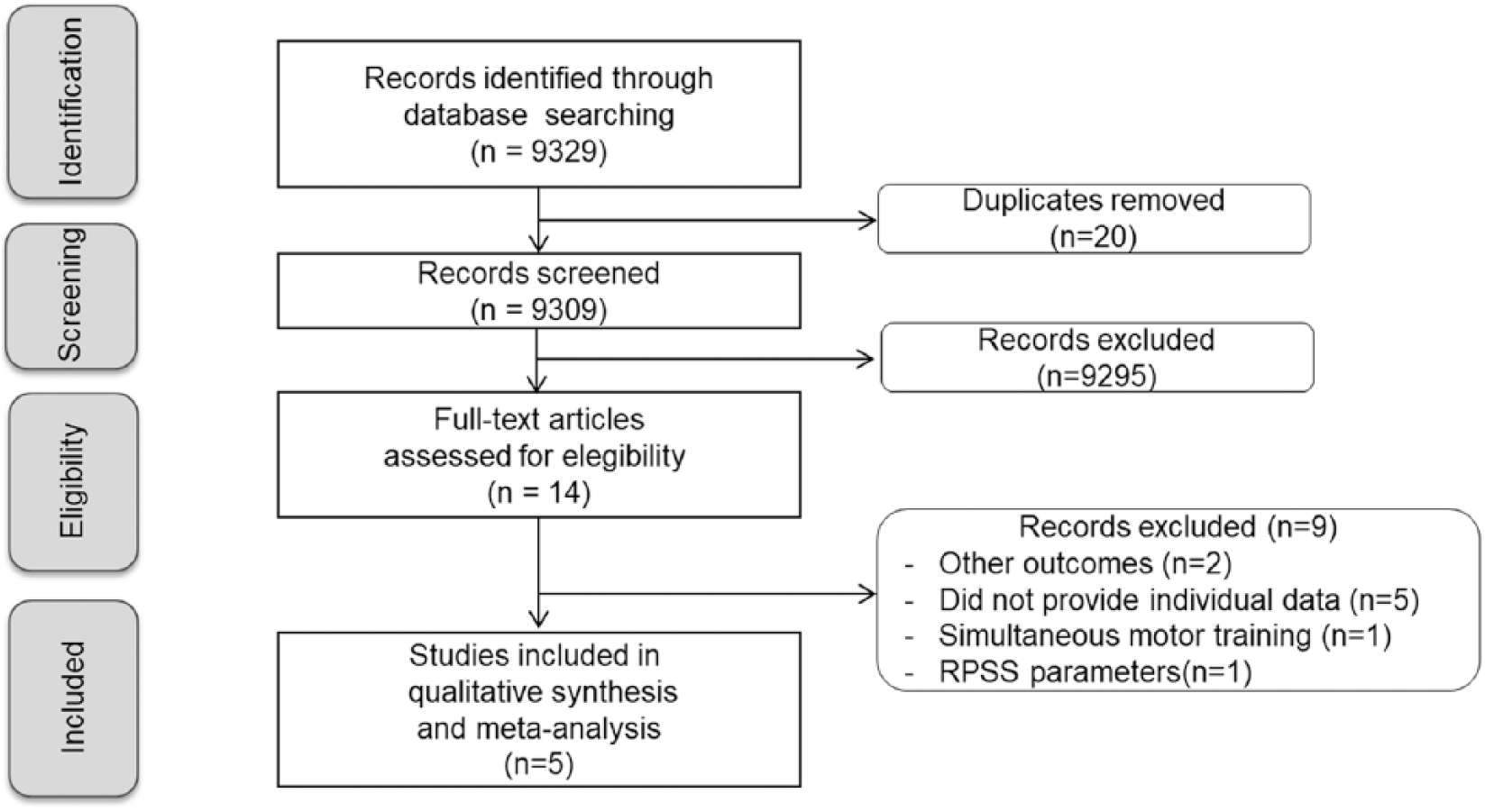
Flow diagram of search.
Characteristics of the Participants
A total of 95 subjects were included in the selected studies (Table 1). The median number of participants per study was 19 (range, 8-36) and about 45.7% were women. The mean age (± SD) was 56.9 ± 10.1 years.
Characteristics of the Participants Included in the Selected Studies. a
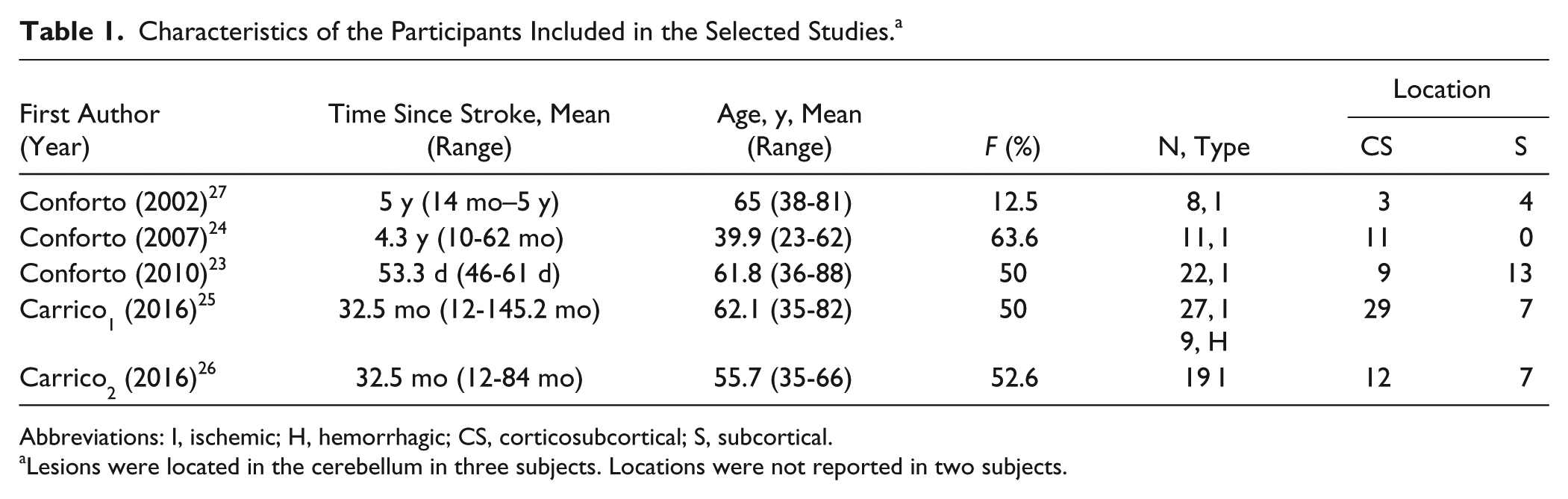
Abbreviations: I, ischemic; H, hemorrhagic; CS, corticosubcortical; S, subcortical.
Lesions were located in the cerebellum in three subjects. Locations were not reported in two subjects.
Most (4/5) studies included participants in the chronic phase, after at least 6 months from stroke (mean 3.0 ± 1.9 years). Only 1 study 23 included patients with less than 3 months after stroke (Table 1).
As shown in Table 1, all studies described locations of strokes. Most of the participants had corticosubcortical or subcortical lesions presumably involving the corticospinal tract. No subgroup comparisons were performed to investigate if particular lesion sites were associated with better outcomes because data were not always available.
Four studies described motor eligibility criteria: upper limb paresis with ability to complete the JTT23,24; at least 10° of active range of motion (ROM) of interphalangeal and metacarpophalangeal joints, and 20° of active wrist extension.25,26
Outcomes
Motor outcomes are shown in Table 2. The studies used a variety of metrics to assess hand force,24,27 upper limb motor impairment (FMA),25,26 performance of activities of daily living (JTT),23,24 Action Research Arm Test (ARAT),25,26 and the Wolf Motor Function Test (WMFT).25,26 According to the ICF, hand force and the FMA are measures of body structure and function, while the JTT, the WMFT, and the ARAT are measures of activity limitation.4,28
Outcomes in the Selected Studies. a
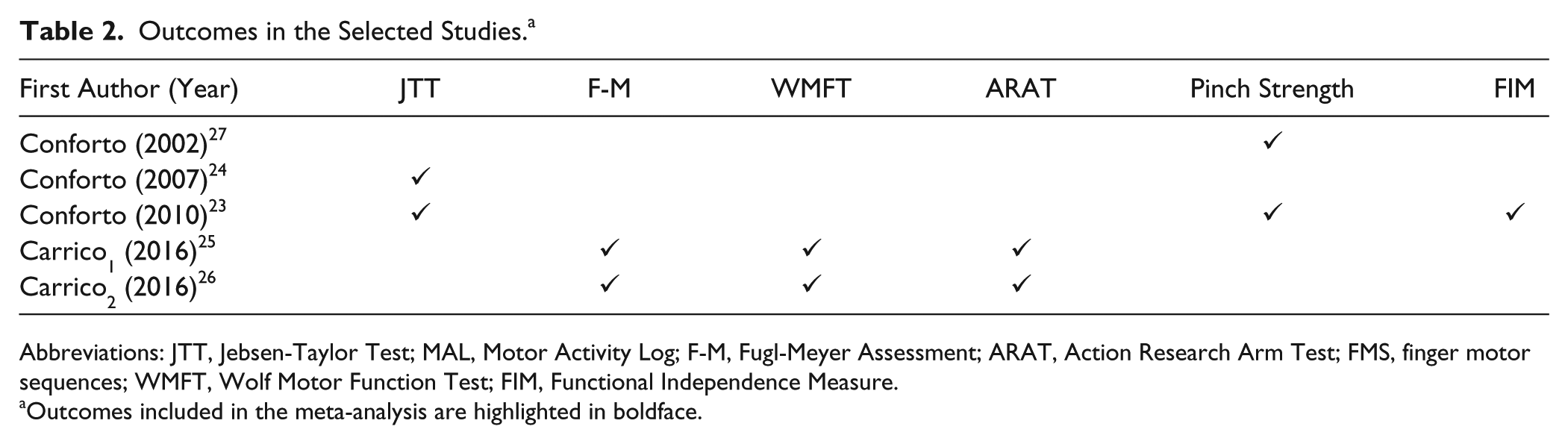
Abbreviations: JTT, Jebsen-Taylor Test; MAL, Motor Activity Log; F-M, Fugl-Meyer Assessment; ARAT, Action Research Arm Test; FMS, finger motor sequences; WMFT, Wolf Motor Function Test; FIM, Functional Independence Measure.
Outcomes included in the meta-analysis are highlighted in boldface.
RPSS Paradigms and Risk of Bias
Table 3 summarizes RPSS paradigms. All studies applied the same duration of RPSS (120 minutes) based on the first published paradigms in healthy subjects 8 and in individuals with stroke. 27 Also, the cathode was positioned proximally, as initially described in studies in healthy subjects.8,10 In all studies, RPSS was delivered at rest. In 2 studies, a single session of RPSS was applied24,27 and in three, multiple sessions were administered.23,25,26
Paradigms of Stimulation and Motor Training in the Selected Studies.
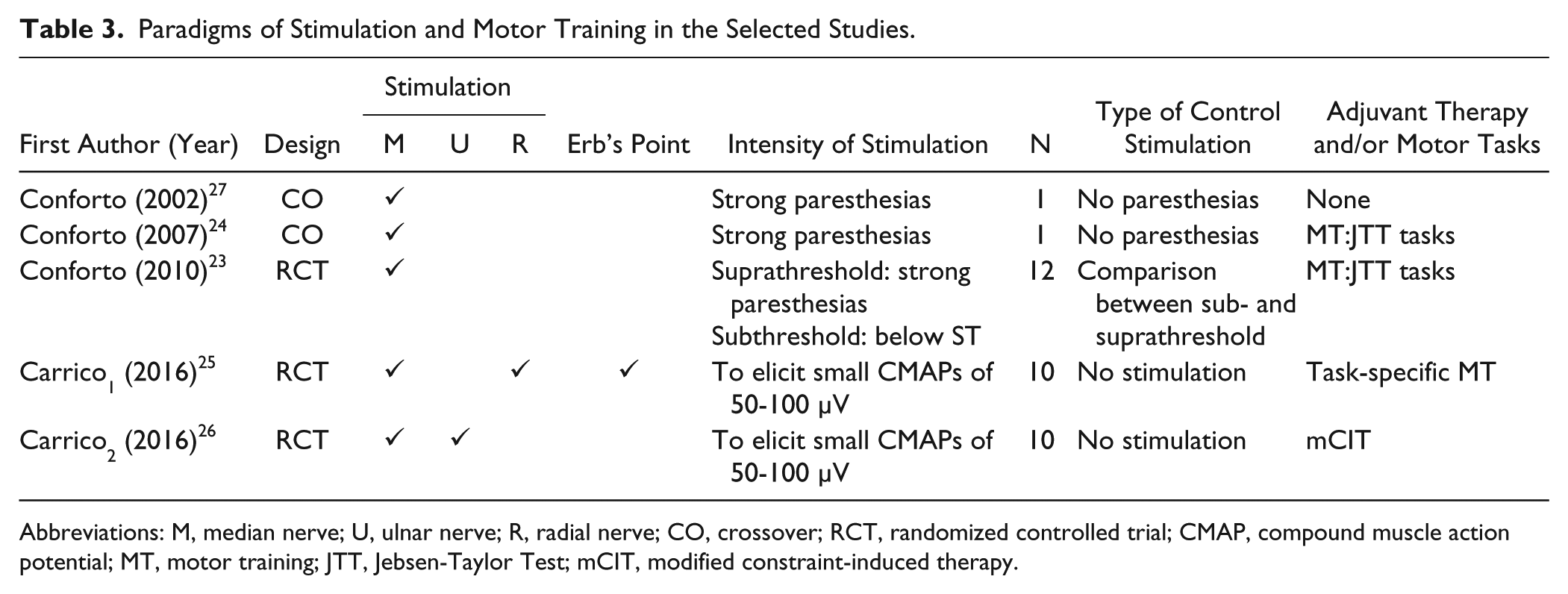
Abbreviations: M, median nerve; U, ulnar nerve; R, radial nerve; CO, crossover; RCT, randomized controlled trial; CMAP, compound muscle action potential; MT, motor training; JTT, Jebsen-Taylor Test; mCIT, modified constraint-induced therapy.
The median nerve was stimulated in all studies.23-27 The ulnar nerve was stimulated in 1 study 26 and the radial nerve, in another one. 25 In the latter, the brachial plexus was also stimulated. 25
Active RPSS was applied at intensities able to induce strong paresthesias in the territory of the stimulated nerve(s) in 3 studies.23,24,27 In 2 studies, subjects reported mild paresthesias and stimulus intensity was adjusted to elicit small compound muscle action potentials of 50 to 100 µV amplitudes.25,26 The aim of RPSS was to provide sensory stimulation with minimal or no motor stimulation.
Effects of RPSS alone on motor performance were evaluated in two studies.24,27 In four, RPSS was administered prior to motor training.23-26 Tasks that are part of the JTT,23,24 task-oriented training, 25 shaping and use of a restriction device comprising a modified constraint-induced therapy (mCIT) protocol 26 were included in the training paradigms (Table 3).
Control stimulation consisted of subthreshold stimulation23,24,27 or no stimulation.25,26 Four studies reported that patients were blind to the type and order of stimulation (control or active)23-26 but only 1 study 24 reported that participants were blinded to the hypotheses. In the 2 studies with crossover designs, subjects experienced active and control RPSS. None of them debriefed participants’ guesses about the types of interventions received. There is a risk of bias in blinding (Supplementary Figure 1) because active RPSS elicits paresthesias in the territory of the target sensory or mixed upper limb nerve and the different types of control stimulation do not.
Effect of RPSS on Motor Function
We opted to analyze results of the ARAT rather than the WMFT for studies in which both scales were evaluated, because the ARAT was selected as the outcome of choice for assessment of activity limitation in different stages after stroke according to Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. 28
Table 4 and Figure 2 summarize the results. When data from the JTT, ARAT, FMA, and hand force were analyzed, there was a statistically significant effect of RPSS on improvement of motor outcomes, but the confidence interval was wide (standard mean difference 0.67; 95% CI, 0.09-1.24) and heterogeneity, substantial (I2 = 65%) (Figure 2A). The total number of subjects in Figure 2A (172) does not reflect the total number of subjects in the analysis (95) because the ARAT and Fugl-Meyer data were collected from the same subjects.25,26 The same applies to JTT and pinch force data. 23
Summary of Results According to Outcomes and Phases After Stroke. a
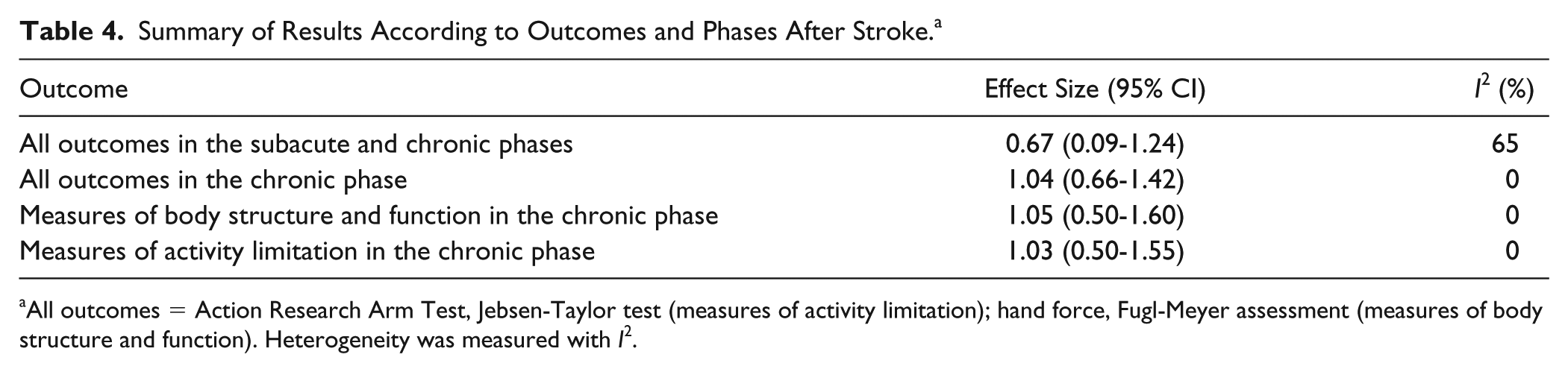
All outcomes = Action Research Arm Test, Jebsen-Taylor test (measures of activity limitation); hand force, Fugl-Meyer assessment (measures of body structure and function). Heterogeneity was measured with I2.
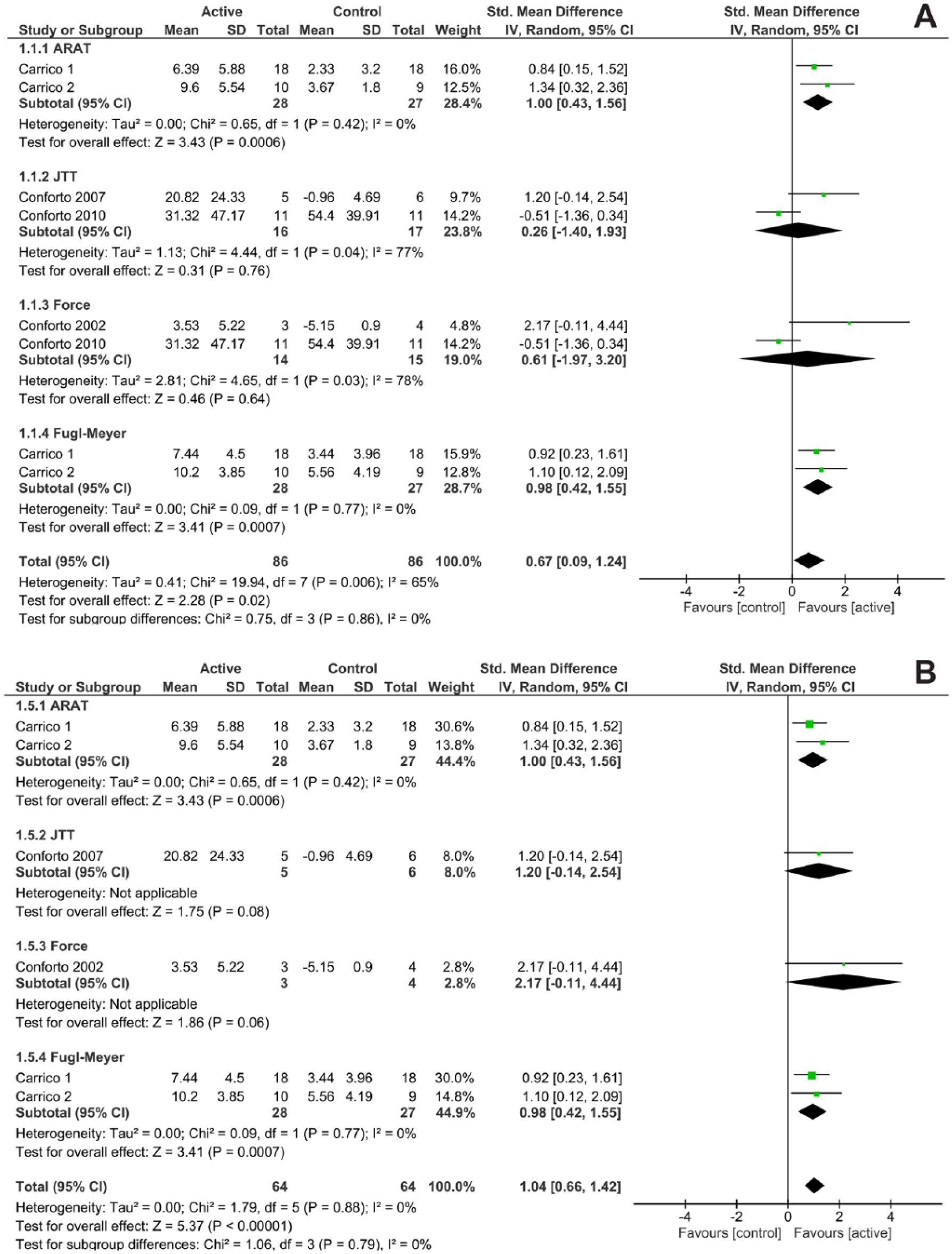
Meta-analysis plots of the effects of repetitive peripheral sensory stimulation on motor outcomes of the paretic limb in subjects with stroke. Each line and square represents an individual effect size. The black diamond indicates a standardized effect size. (A) Outcomes from 5 studies in which subjects in the subacute or chronic phase were included. (B) Outcomes from 4 studies in which only subjects in the chronic phase were included.
RPSS had a statistically significant benefit on the ARAT (standard mean difference 1.00; 95% CI, 0.43-1.56) as well as on the FMA (standard mean difference 0.98; 95% CI, 0.42-1.55) with no heterogeneity (Figure 2A). The effect on the JTT was not significant and heterogeneity was high (77%). This probably occurred because 1 of the 2 studies that assessed effects of RPSS on the JTT 23 showed a greater benefit of the sham intervention (subthreshold stimulation) than the active treatment. This was the only study that included subjects at the subacute phase after stroke. Also, effects on pinch force were not statistically significant (Figure 2A).
We then restricted the analysis to the 4 studies that only included patients in the chronic phase (Figure 2B). When all outcomes were combined, effects of RPSS were statistically significant with no heterogeneity (standard mean difference 1.04; 95% CI, 0.66-1.42). Subgroup analysis according to the type of outcome in the chronic phase showed that RPSS had significant effects with no heterogeneity when measures of body structure and function (Supplementary Figure 2) or activity limitation (Supplementary Figure 3) were analyzed separately.
Duration of the Effects
One study reported that the beneficial effect of a single session of RPSS on motor performance can last for at least 24 hours 27 but in only 1 study, motor outcomes were assessed beyond this period. 24 In this study, retention of effects of motor training combined with RPSS on JTT performance were observed for at least 30 days in the active, but not in the sham group. Likewise, a study that applied 10 sessions of RPSS to subjects in the chronic phase after stroke noted retention of performance in the FMA, WMFT, and ARAT in the active group at 1 month after treatment. 25
On the other hand, in the study that randomized patients within the first 2 months after stroke, 23 JTT improved significantly more in the group that received subsensory RPSS intensity than in the group that received suprasensory RPSS, immediately after end of treatment. After a period of 2 to 3 months later, the between-group difference was no longer statistically significant.
Dose-Response and Target-Response Relations
One study 27 described direct correlations between RPSS intensity and the magnitude of motor improvement. The higher the stimulation above sensory threshold, the greater the change observed in lateral pinch force. However, the number of subjects submitted to stimulation of one nerve was small (n = 18) compared with the number of subjects submitted to stimulation of more than one nerve (n = 55). Different outcomes were assessed in studies in which one23,24,27 or more than one nerve were stimulated.25,26 Therefore, subgroup analysis according to the number of stimulated nerves was not performed.
In only 1 study, motor training was not administered after RPSS (Table 3). Therefore, subgroup analysis according to administration of training was not performed.
Safety
No serious adverse events were reported in any of the studies, and no adverse events at all were reported in 3 studies.23,25,26
Discussion
The main finding of this study was that RPSS has statistically significant effects compared with control stimulation on improvement of upper limb motor outcomes in subjects in the chronic phase (>6 months) after stroke, with no heterogeneity. Subgroup analysis showed benefits for measures of activity limitation as well as for measures of body structure and function in the chronic phase. One study described a dose-response relation 27 suggesting that “more RPSS is better.” No serious adverse events were reported.
In the only study that included subjects less than 3 months poststroke, subsensory RPSS, intended to be a control intervention, was associated with greater enhancement of motor performance than suprasensory stimulation. 23 Levels of neuronal activity or excitability can vary according to time from stroke and it is plausible that a given intervention may have different effects at subacute or chronic stages.29,30 For instance, constraint-induced movement therapy can enhance motor function when delivered within 3 to 9 months poststroke 31 but is not superior to traditional therapy within the first 28 days. 32 It remains to be confirmed whether effects of RPSS also vary according to time from stroke.
As expected considering our inclusion criteria, all studies applied similar RPSS parameters based on the seminal paradigm of Ridding et al 8 in healthy subjects. RPSS was always applied to the median nerve but the ulnar 26 or radial nerves 25 were also stimulated in some protocols, and the brachial plexus was stimulated in one. 25 The optimal “dose” of RPSS is still uncertain.
The severity of motor impairments at baseline may be relevant to effects of RPSS. In the studies included in this review, improvements were reported not only in subjects with mild to moderate upper limb motor impairments but also in more severely affected participants.25,26 Larger studies, with a wider range of baseline levels of motor impairments, are necessary in order to determine if there is a difference in effects of RPSS according to severity.
The retention of the results of RPSS 30 days after a single 24 or multiple 25 sessions of RPSS suggest that this intervention may have long-lasting effects when administered in the chronic phase after stroke. The duration of RPSS (2 hours) may limit its applicability in clinical practice, especially when combined with intensive motor training. Whether shorter durations can have comparable effects, or whether the association of several sessions of RPSS and other neuromodulation tools such as tDCS 33 can allow shortening of the period of peripheral stimulation and lead to similar results, remains to be tested.
This study has some limitations. First, because we only included studies that applied a specific paradigm of nerve stimulation, it is not possible to clarify whether other paradigms of afferent stimulation lead to similar positive effects on motor outcomes. Second, because paresthesias are conscious perceptions, the choice of the best control intervention to RPSS is a challenge. The risk of bias in unblinding of participants was considered high in all the included studies. Further work should include debriefing to assess participants’ experience of RPSS.
The number of subjects included in the 5 trials selected for this meta-analysis of RPSS was small (n = 95), compared with the numbers included in meta-analysis of effects of other neuromodulation interventions such as rTMS or tDCS to improve upper limb motor outcomes in stroke. On the other hand, all studies included in the meta-analysis provided individual data, a major strength considering the heterogeneous outcomes and the need to calculate mean standard differences.
When our results are compared with those of meta-analyses of rTMS or tDCS in the chronic phase poststroke, the effect size of RPSS is higher (1.4; 95% CI, 0.66-1.42; I2 = 0%) than the effect size of tDCS (0.45; 95% CI, 0.09-0.80; I2 = 0%). 21 Some meta-analyses reported similar effect sizes for tDCS (0.58; 0.44-0.79) or rTMS (0.55; 0.37-0.72) 34 while others did not reveal significant beneficial effects of these interventions.35,36
Heterogeneity in choice of outcomes, sample sizes, criteria for selection of studies and statistical approaches can explain these discrepancies.
Conclusions
The results of our systematic review and meta-analysis suggest that RPSS, despite less frequently assessed than other interventions such as tDCS or rTMS, may be beneficial in subjects in the chronic phase after stroke and that its effect size is at least comparable to those of these neuromodulation strategies. Optimal RPSS paradigms leading to long-term improvements in motor performance or function, as well as whether or not this intervention may also benefit subjects within the first weeks or months poststroke, remain to be determined. The lack of relevant adverse events, the simplicity, low costs of RPSS and the improvements in motor performance should encourage multicenter studies with a greater number of subjects to define the role of this intervention on improvement of motor function of the upper limb.
Supplemental Material
Supplemental_Figures – Supplemental material for Repetitive Peripheral Sensory Stimulation and Upper Limb Performance in Stroke: A Systematic Review and Meta-analysis
Supplemental material, Supplemental_Figures for Repetitive Peripheral Sensory Stimulation and Upper Limb Performance in Stroke: A Systematic Review and Meta-analysis by Adriana Bastos Conforto, Sarah Monteiro dos Anjos, Wanderley Marques Bernardo, Arnaldo Alves da Silva, Juliana Conti, André G. Machado and Leonardo G. Cohen in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr André Machado declares, in addition to receiving funding from the National Institutes of Health (grant not related to this work), personal fees from St Jude and distribution rights related to IP (intellectual property) from Enspire, ATI, and Cardionomics. The other Authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This investigation was supported by the Fogarty International Center of the National Institutes of Health under the NCD-LIFESPAN (GRANT D71TW009132-01). Sarah Monteiro dos Anjos, Juliana Conti, and Adriana Bastos Conforto received funding from the National Institutes of Neurological Disorders and Stroke (R01NS076348).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.