
Abstract
Background. Insulin-like growth factor-1 (IGF-1) is neuroprotective after stroke and is regulated by insulin-like binding protein-3 (IGFBP-3). In healthy individuals, exercise and improved aerobic fitness (peak oxygen uptake; peak VO2) increases IGF-1 in circulation. Understanding the relationship between estimated prestroke aerobic fitness and IGF-1 and IGFBP-3 after stroke may provide insight into the benefits of exercise and aerobic fitness on stroke recovery. Objective. The purpose of this study was to determine the relationship of IGF-1 and IGFBP-3 to estimated prestroke peak VO2 in individuals with acute stroke. We hypothesized that (1) estimated prestroke peak VO2 would be related to IGF-1 and IGFBP-3 and (2) individuals with higher than median IGF-1 levels will have higher estimated prestroke peak VO2 compared to those with lower than median levels. Methods. Fifteen individuals with acute stroke had blood sampled within 72 hours of hospital admission. Prestroke peak VO2 was estimated using a nonexercise prediction equation. IGF-1 and IGFBP-3 levels were quantified using enzyme-linked immunoassay. Results. Estimated prestroke peak VO2 was significantly related to circulating IGF-1 levels (r = .60; P = .02) but not IGFBP-3. Individuals with higher than median IGF-1 (117.9 ng/mL) had significantly better estimated aerobic fitness (32.4 ± 6.9 mL kg−1 min−1) than those with lower than median IGF-1 (20.7 ± 7.8 mL kg−1 min−1; P = .03). Conclusions. Improving aerobic fitness prior to stroke may be beneficial by increasing baseline IGF-1 levels. These results set the groundwork for future clinical trials to determine whether high IGF-1 and aerobic fitness are beneficial to stroke recovery by providing neuroprotection and improving function.
Introduction
Insulin-like growth factor-1 (IGF-1) is known to be neuroprotective after middle cerebral artery occlusion in animals1-4 and may even act as a neuronal rescue agent when given through intranasal delivery.2,5 When administered through intranasal delivery, core lesion size can be reduced up to 94% 2 while also improving functional status compared to vehicle controls. 4 In humans, those with high circulating levels of IGF-1 early after stroke have greater survival rates and fewer impairments, tested by the National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS), at 3 and 24 months poststroke compared to those with low IGF-1 levels.6-8 This suggests that IGF-1 may also have a neuroprotective effect in humans. Furthermore, the molar ratio of IGF-1 and insulin-like growth factor binding protein-3 (IGFBP-3), IGF-1’s primary regulatory protein, has also been observed to be related to stroke recovery. 7 Individuals with a high molar ratio of IGF-1 to IGFBP-3 exhibited better stroke outcomes at 3 months poststroke, indicating that having low IGFBP-3 levels may also be beneficial to stroke recovery. Therefore, it is important to understand what may influence levels of IGF-1 and IGFBP-3 in individuals with stroke.
In healthy individuals, both circulating levels of IGF-1 and IGFBP-3 can be influenced by physical activity and aerobic fitness (peak oxygen consumption, peak VO2).9-13 Prior work has demonstrated that people who are more physically fit have better white matter integrity, 14 regional brain volume, 15 and brain blood flow. 16 Therefore, aerobic fitness prior to a stroke may not only benefit overall brain health but also provide some level of neuroprotection via circulating IGF-1, which has been shown to improve stroke outcomes.6-8 However, even though these studies have demonstrated that higher than median levels of circulating IGF-1 improve outcomes after stroke, there is lack of information regarding the relationship of prestroke aerobic fitness, IGF-1, and IGFBP-3 in individuals with acute stroke.
Assessing peak VO2 during the acute stroke hospital stay via a maximal exercise test and direct measurement of expired gases could be difficult if the person has unstable blood pressure, activity restrictions, or time constraints due to other standard of care testing. However, one potential alternative method for assessing prestroke aerobic fitness is through the use of a nonexercise prediction equation to estimate peak VO2. Current literature has shown that nonexercise equations to predict peak VO2 can be easily administered and provide useful alternatives to exercise testing in healthy adults and older adults.17,18 Furthermore, we recently demonstrated the use of a nonexercise prediction equation 18 to estimate prestroke peak VO2 during the acute stroke hospital stay. 19 Quick, nonexercise prediction equations would feasibly allow for the study of prestroke aerobic fitness (peak VO2) and its relationship to IGF-1 and IGFBP-3.
Therefore, the purpose of this study was to determine the relationship of IGF-1 and IGFBP-3 to estimated prestroke aerobic fitness (peak VO2) in individuals with acute stroke. We hypothesized that (1) estimated prestroke peak VO2 would be significantly and positively correlated to IGF-1 and inversely correlated to IGFBP-3 and (2) individuals with higher than median circulating IGF-1 levels would have significantly higher estimated prestroke peak VO2 compared to those with lower than median levels.
Methods
Study Design
Institution approval from the Human Subjects Committee at the University of Kansas (KU) Medical Center was obtained before beginning the study (HSC#00000972). Written informed consent was obtained from every individual or their surrogate decision maker prior to study participation.
Participants
Individuals were a part of a larger, parent study and were therefore eligible to participate if they met the parent study requirements. Individuals were eligible to be included if they had a confirmed diagnosis of acute ischemic or hemorrhagic stroke, were admitted to the certified comprehensive stroke units at the KU Hospital, and were between the ages of 25 and 85 years. Individuals were excluded from the study if they (1) were not able to consent and begin data collection within 72 of admission; (2) had a diagnosis of bilateral stroke; (3) could not consent due to sedation, aphasia, and no surrogate consent present; (4) could not return for follow-up visit for the parent study; (5) could not position their arm for testing of the parent study; (6) had a diagnosis of acute renal failure; (7) had a history of ischemic or hemorrhagic stroke, ischemic cardiovascular event, or coronary artery bypass graft surgery less than 3 months prior to their current hospital admission; and (8) congestive heart failure; or (9) severe peripheral artery disease. Figure 1 describes the number of participants screened and the reasons for nonenrollment.
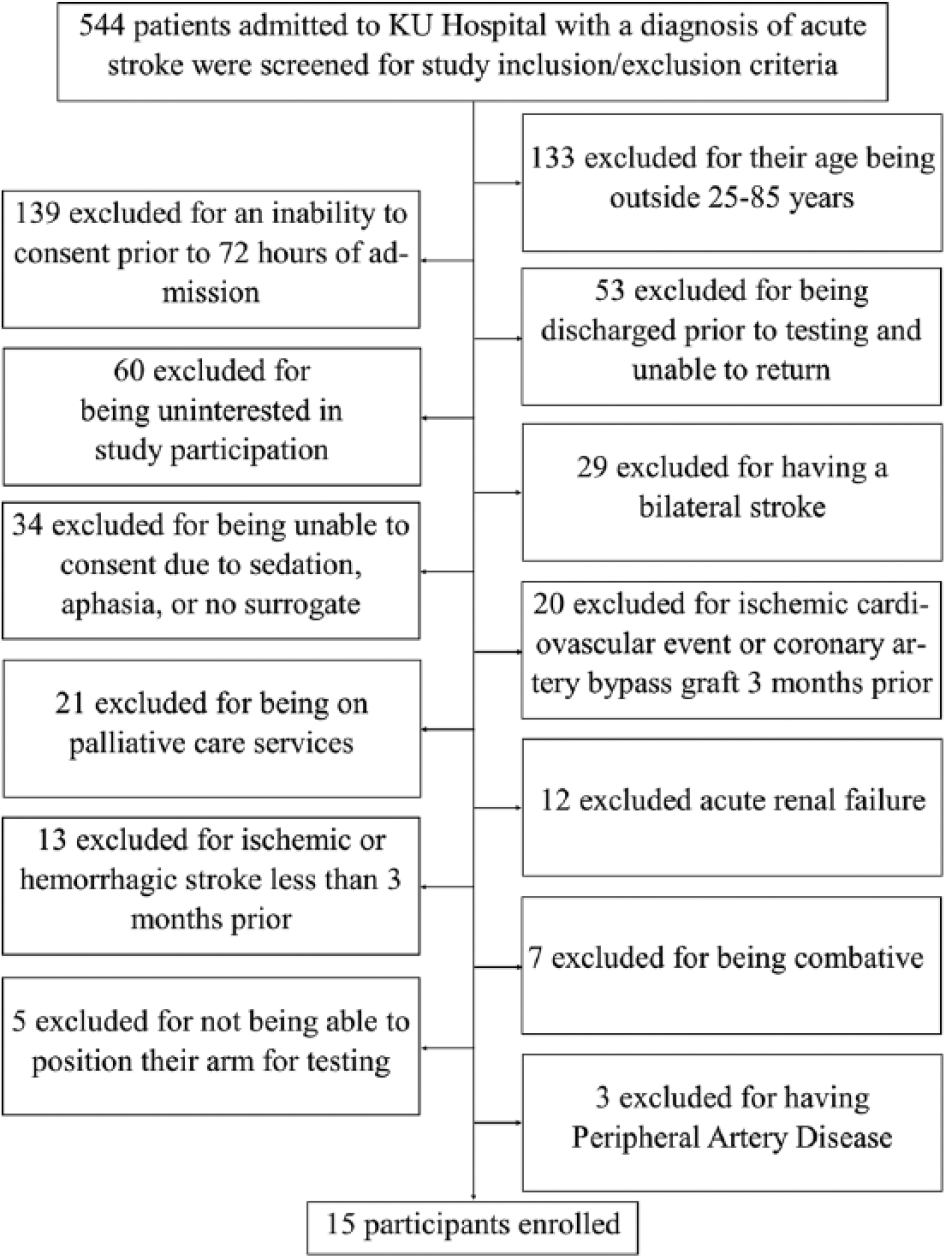
Subject exclusion chart.
Estimated Prestroke Peak VO2
Prestroke peak VO2 was estimated using the Jurca prediction equation.
18
The Jurca prediction equation uses the following variables: sex, age, body mass index
Quantification of Biomarkers
Blood for quantification of IGF-1 and IGFBP-3 was obtained after an overnight fast, between 7:30
After all samples were collected, total IGF-1 (Alpco; Salem, NJ; Cat# 22-IGFHU-E01) and IGBP-3 (Alpco; Cat#22-BP3HU-E01) were quantified using enzyme-linked immunoassays (ELISAs). To avoid protein shock, samples were slowly thawed to room temperature with ice prior to assaying. Procedures for assaying were performed exactly to the recommendations of the manufacturer in the manual provided with the ELISA kits.
Stroke Severity and Lesion Size
NIHSS was obtained by the admitting stroke physician and taken from the patients’ electronic medical records. A radiologist, and study team member, measured and calculated lesion volume from structural magnetic resonance imaging performed on admission to the hospital. Established, standardized techniques of neuroimaging using an ellipsoidal assumption of lesion shape was used.20,21 When multiple lesions were present, the largest lesion volume (cm3) was reported and used for analysis.
Data Analysis
Shapiro-Wilk tests were performed to determine whether estimated prestroke peak VO2 and IGF-1 levels were normally distributed. Pearson correlations were performed to determine the relationship of proteins (IGF-1 and IGFBP-3) to estimated prestroke peak VO2. Median levels of IGF-1 and IGFBP-3 were determined using descriptive statistics. T tests were performed to determine the difference in estimated prestroke peak VO2 between above and below median values for both IGF-1 and IGFBP-3. All statistical tests were considered significant at the α level of .05 and were performed using IBM SPSS, Version 22 (SPSS, Inc, Chicago, IL). Pearson correlations were also performed to determine the association of lesion volume, stroke severity, and BMI to circulating IGF-1 and IGFBP-3 levels.
Results
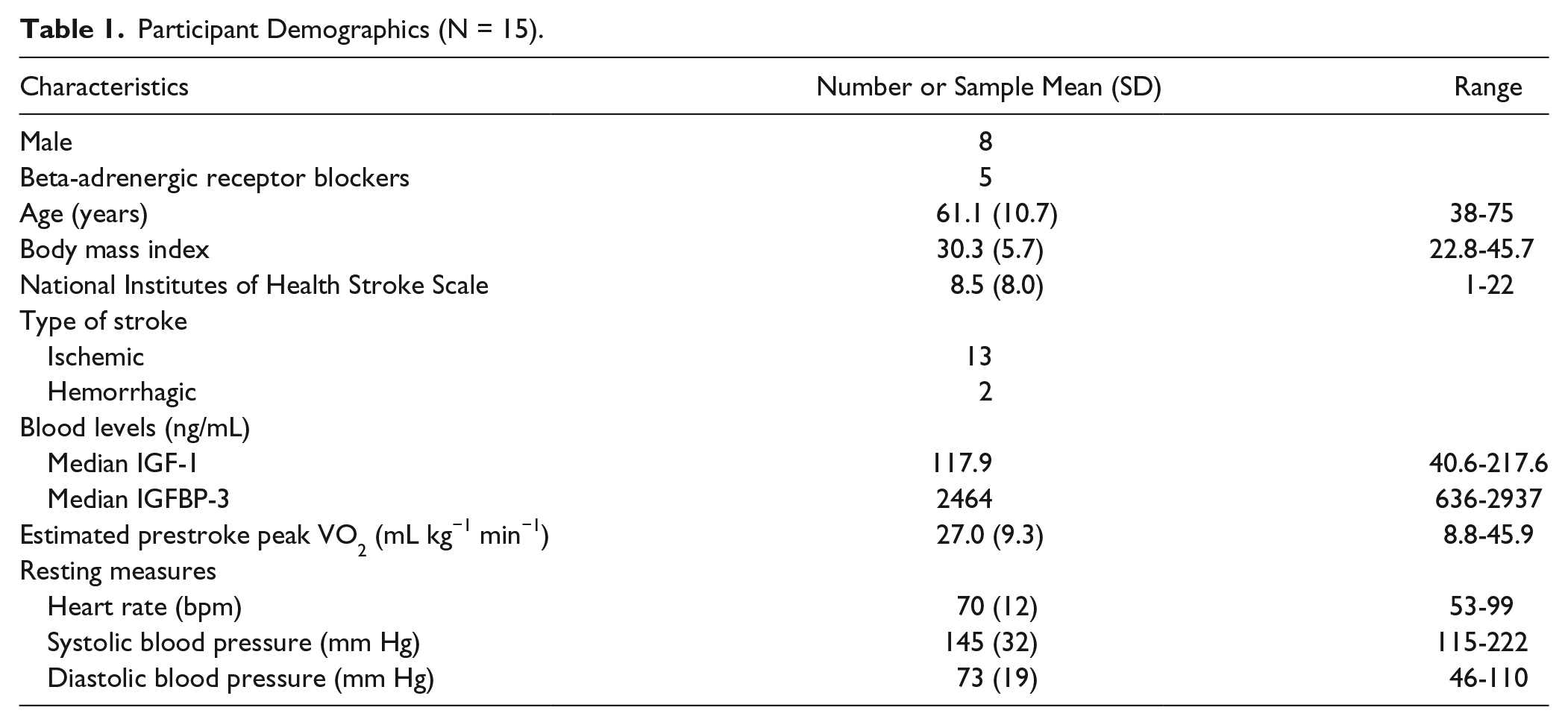
Fifteen individuals with acute stroke (8 males, 61.1 ± 10.7 years) were enrolled into the study and completed data collection within 72 hours of hospital admission. Thirteen individuals completed data collection within 48 hours of admission. Table 1 describes the demographics of all participants, mean levels of IGF-1 and IGFBP-3, and the results of the nonexercise prestroke peak VO2 estimation equation.
Participant Demographics (N = 15).
Shapiro-Wilk tests revealed that estimated prestroke peak VO2 (P = .93) and IGF-1 levels (P = .40) were both normally distributed. Estimated prestroke peak VO2 was significantly and positively related to IGF-1 levels sampled within 72 hours of stroke (r = .60; P = .02; Figure 2), but not significantly related to IGFBP-3 (r = −.09; P = .75). Median level of IGF-1 and IGFBP-3 was 117.9 and 2464 ng/mL, respectively. Individuals with higher than median levels of IGF-1 during acute stroke had significantly better estimated peak VO2 (n = 8; 32.4 ± 6.9 mL kg−1 min−1) compared to individuals with lower than median IGF-1 levels (n = 7; 20.7 ± 7.8 mL kg−1 min−1; P = .03). There were no significant differences in estimated peak VO2 between higher (n = 8; 29.7 ± 8.0 mL kg−1 min−1) and lower than median (n = 7; 23.8 ± 10.3 mL kg−1 min−1; P = .24) levels of IGFBP-3.
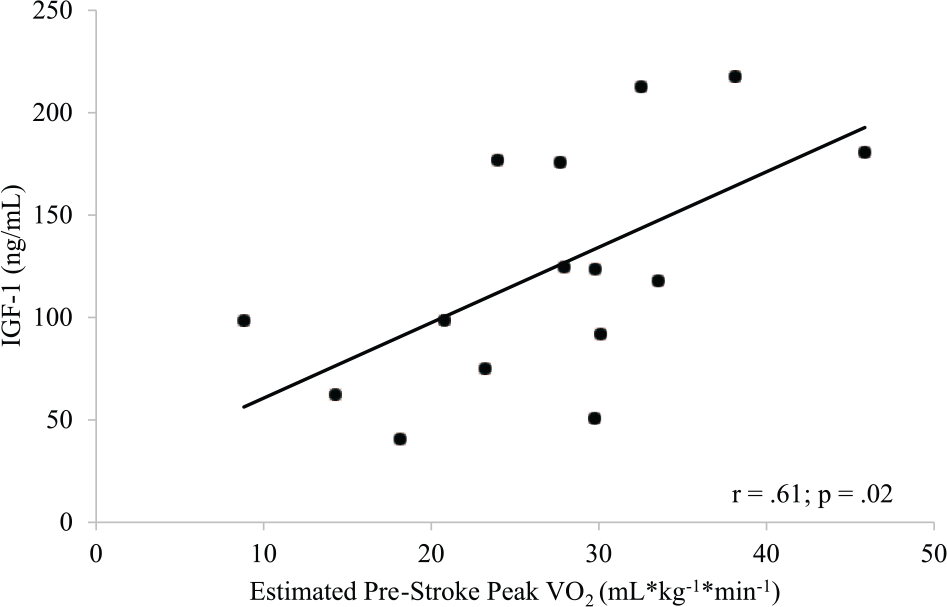
Relationship of circulating IGF-1 and estimated prestroke peak VO2.
Finally, circulating IGF-1 levels were not significantly related to lesion volume (r = −.15; P = .6), admitting NIHSS (r = −.36; P = .19), or BMI (r = .02; P = .95). Circulating IGFBP-3 levels were also not significantly related to lesion volume (r = −.10; P = .74), admitting NIHSS (r = −.41; P = .13), or BMI (r = .36; P = .18).
Discussion
Our hypotheses were partially supported in that estimated prestroke peak VO2 was related to circulating levels of IGF-1 early after stroke, but not to levels of IGFBP-3. Furthermore, we found that individuals with higher than median levels of IGF-1 had greater estimated aerobic fitness (peak VO2) when compared to individuals with lower than median levels. The results of this work have important implications for future studies to investigate whether circulating IGF-1 levels and aerobic fitness are related to functional recovery following a stroke. These studies would be important for further development of future rehabilitation techniques to improve functional recovery in individuals with stroke.
Neuroprotection
IGF-1 is known to be neuroprotective after stroke.1-4 In humans, individuals with higher than median levels of IGF-1 during the early phase of stroke have higher survival rates and less severe impairments at 3, 6, and 24 months poststroke compared to those with lower than median IGF-1 levels.6-8 Denti and colleagues examined IGF-1 and IGFBP-3 levels in 85 acute stroke participants. 8 Stroke severity was assessed by the Barthel Index at 3 and 6 months poststroke. Individuals with acute stroke who had IGF-1 levels less than 60 ng/mL had higher stroke severity and lower survival rates at 3 and 6 months poststroke. 8 De Smedt et al further demonstrated the neuroprotective quality of baseline IGF-1 by examining IGF-1 and IGFBP-3 levels and stroke severity with the NIHSS and mRS. 7 The results showed that even when controlling for cardiac risk factors, such as hypertension, diabetes, atrial fibrillation, coronary artery disease, heart failure, smoking, and previous stroke, lower than median IGF-1 levels were related to increased stroke severity and lower survival rates at 3 and 6 months poststroke when compared to those with higher than median levels of IGF-1. 7 There were no associations between IGFBP-3 levels and stroke severity. However, individuals with higher molar ratios of IGF-1 to IGFBP-3 had better stroke outcomes at 3 months poststroke, 7 indicating that IGFBP-3 may not directly be related to stroke recovery but plays a role in regulating the availability of IGF-1 and is therefore important to consider. The studies by De Smedt and Denti and colleagues have demonstrated that higher than median circulating IGF-1 improves outcomes after stroke and, along with IGFBP-3, is important to stroke recovery. However, there is lack of knowledge regarding the potential influence of factors such as prestroke peak VO2 and its relationship to IGF-1 and IGFBP-3 in individuals with acute stroke.
Aerobic Fitness
Aerobic fitness, tested by peak aerobic capacity (peak VO2), has been directly related to circulating IGF-1 levels in 846 healthy men. 13 Blood was collected in the morning after an overnight fast for the quantification of IGF-1. Individuals then underwent a graded maximal exercise test on a cycle ergometer with direct gas analysis to obtain peak VO2. A repeated squats test was also performed to assess leg strength. Individuals with higher peak VO2 exhibited higher levels of circulating baseline IGF-1. Furthermore, better aerobic fitness was associated with increased performance on the repeated squats test, indicating a greater functional performance in the lower extremities. 13 Nindl and colleagues’ study in healthy men could potentially have very large implications for individuals poststroke. However, the relationship of exercise performance, specifically, aerobic fitness, to IGF-1 levels had not yet been tested in individuals with stroke prior to the current study, but gives important insight for which future studies could be based.
Testing aerobic fitness in individuals with stroke can be extremely difficult due to neuromotor limitations in the lower extremities. In the acute setting, it is particularly challenging because of various factors such as time constraints for standard of care diagnostic assessments, lack of trained professionals and specialized equipment, and extreme fatigue of the participant. However, our previous work displays feasibility of the use of a nonexercise prediction equation to estimate prestroke peak VO2 in individuals admitted to the hospital with a diagnosis of acute stroke. 19 Our work showed that estimated prestroke peak VO2 was easily administered. The results of the current study corroborates these findings but also show that this easily administered tool to estimate prestroke aerobic fitness may also influence IGF-1 levels in individuals with acute stroke.
The results of the current study are novel and important as we found a strong and significant relationship between estimated prestroke aerobic fitness (peak VO2) and IGF-1. Although this requires further exploration, it is plausible that prestroke aerobic fitness may have a potential benefit following stroke. In healthy men, those with higher peak VO2 and greater lower extremity functional ability had higher levels of circulating baseline IGF-1. 13 In our study, we also report that individuals with higher estimated prestroke peak VO2 have above median levels of IGF-1 when compared to individuals with lower than median levels of IGF-1. However, the current study does not answer questions regarding IGF-1 levels and functional performance of the lower extremity but provides strong rationale for further investigation. Furthermore, we did not observe a significant relationship between estimated prestroke peak VO2 and circulating IGFBP-3 levels. The lack of the hypothesized relationship could be due to many factors. In the study by De Smedt and colleagues, IGFBP-3 was not directly related to stroke outcomes, but the ratio of IGF-1 to IGFBP-3 was. 7 It is possible that IGFBP-3 can be influenced by exercise short term, but baseline levels may not be directly related to aerobic fitness. Furthermore, changes in IGFBP-3 circulating levels may depend on the type or duration of exercise. 22
Limitations
We must acknowledge that the participants, or their surrogate decision makers, may report higher or lower activity levels and thereby influence the estimated prestroke peak VO2 estimation. From our prior work using the Jurca nonexercise estimation equation in acute stroke 19 and others using the equation in community-dwelling adults and older adults with several cardiovascular risk factors,18,23 we believe this is a feasible and safe alternative in individuals who are within 72 hours of stroke.
Furthermore, the current study was limited by a small sample size and the results should be interpreted with caution. Despite this, we believe the results of our study give rise to further questions regarding estimated prestroke aerobic fitness, IGF-1, and functional recovery. Future work should address whether prestroke aerobic fitness and IGF-1 in acute stroke influence functional recovery and stroke outcomes.
Another potential limitation of the study was that lesion volume may be associated with circulating IGF-1 and IGFB-3 levels. However, in our sample, we did not see any significant relationships between IGF-1 and IGFBP-3 to lesion volume or stroke severity. Furthermore, dietary intake, BMI, percent body fat, and body fat distribution could be related to circulating IGF-1 and IGFBP-3 levels. However, while we did not control for dietary intake or percent body fat/body fat distribution, our results showed no relationship between BMI and IGF-1 levels or IGFBP-3 levels. Additionally, a study by Cappon and colleagues showed that increases in IGF-1 after a short bout of exercise was not significantly different after drinking a high-fat meal, high-glucose meal, or a noncaloric placebo meal. 10
Finally, blood was sampled, on average, within 48 hours of stroke admission. The sampling window used was more narrow than one study that sampled blood anywhere between 1 and 10 days poststroke. 6 Although we sampled blood within at most 72 hours, our time window for sampling blood was wider than previous studies examining IGF-1 and stroke outcomes.7,8 However, we believe that this would have minimal effect on our study as there is no suggested optimal time to obtain blood for the quantification of IGF-1 and IGFBP3.
Conclusion
This study investigated the relationship between IGF-1 and IGFBP-3 levels and prestroke estimated peak VO2 in individuals with acute stroke. We hypothesized that (1) prestroke estimated peak VO2 would be positively and significantly related to IGF-1 and negatively related to IGFBP-3 and (2) individuals with higher than median circulating IGF-1 levels would have significantly better estimated prestroke peak VO2 compared to individuals with lower than median levels of IGF-1. Our results partially supported this hypothesis in that we observed a significant, positive relationship between prestroke peak VO2 and circulating IGF-1 levels, but a nonsignificant relationship with IGFBP-3. Furthermore, our second hypothesis was supported and demonstrated that individuals with higher than median levels of IGF-1 had higher prestroke estimated peak VO2, while individuals with lower than median levels of IGF-1 had a lower prestroke estimated peak VO2. The results of this study are novel and significant to the field in that they provide support for future studies for examining how aerobic fitness, IGF-1, and IGFBP-3 levels are related to recovery and physical function after stroke.
Footnotes
Acknowledgements
The authors would also like to thank the KU hospital stroke unit for their support and the participants and their families for their time and dedication to this study.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health and Human Development nor American Heart Association, the funding agencies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SAB was supported in part by K01HD067318 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. AEM was supported in part by T32HD0577850 from the National Institutes of Health and in part by award number 14PRE20040026 from the American Heart Association. The Georgia Holland Research in Exercise and Cardiovascular Health (REACH) laboratory space was supported by the Georgia Holland Endowment Fund.