
Abstract
Background and purpose. This study compared the effect of cyclic neuromuscular electrical stimulation (NMES), electromyographically (EMG)-triggered NMES, and sensory stimulation on motor impairment and activity limitations in patients with upper-limb hemiplegia. Methods. This was a multicenter, single-blind, multiarm parallel-group study of nonhospitalized hemiplegic stroke survivors within 6 months of stroke. A total of 122 individuals were randomized to receive either cyclic NMES, EMG-triggered NMES, or sensory stimulation twice every weekday in 40-minute sessions, over an 8 week-period. Patients were followed for 6 months after treatment concluded. Results. There were significant increases in the Fugl-Meyer Assessment [F(1, 111) = 92.6, P < .001], FMA Wrist and Hand [F(1, 111) = 66.7, P < .001], and modified Arm Motor Ability Test [mAMAT; time effect: F(1, 111) = 91.0, P < .001] for all 3 groups. There was no significant difference in the improvement among groups in the FMA [F(2, 384) = 0.2, P = .83], FMA Wrist and Hand [F(2, 384) = 0.4, P = .70], or the mAMAT [F(2, 379) = 1.2, P = .31]. Conclusions. All groups exhibited significant improvement of impairment and functional limitation with electrical stimulation therapy applied within 6 months of stroke. Improvements were likely a result of spontaneous recovery. There was no difference based on the type of electrical stimulation that was administered.
Introduction
There is growing evidence that motor recovery after stroke is activity dependent. Studies have suggested that repetitive movement therapy mediated by surface (ie, transcutaneous) neuromuscular electrical stimulation (NMES) facilitates motor control in upper-limb hemiparesis.1-6 Cyclic NMES, electromyographically (EMG)-triggered NMES, and sensory stimulation are commercially available surface NMES modalities that may be used as adjuncts to therapy offered by allied health professionals to improve function after stroke. The treatment methods for these types of NMES differ in many ways that may influence their efficacy in reducing impairment and functional limitation. There is little data on which to base decisions regarding which devices should be purchased or which modalities to offer.
Theoretically, the different methods of NMES engage the stroke survivor in different ways that could potentially affect outcome. Cyclic NMES activates the paretic muscles according to preset timing and intensities to provide extension at the wrist and/or fingers.7,8 The participant is passive; no cognitive input or attempt to assist cyclic NMES is required from the participant. EMG-triggered NMES is similar to cyclic NMES, except that a cognitive element is introduced by triggering the NMES with the participant’s own volitionally activated EMG signal.6,9,10 Thus, the NMES provides wrist and/or finger extension time-locked to the cognitive intent to actively extend the wrist and open the hand. Sensory stimulation without motor stimulation provides a lesser amount of afferent input than NMES because there is no muscle activation or joint movement resulting from stimulation, although it may have some therapeutic benefit.11-13 Thus, in this study, sensory stimulation serves as a conservative control group.
Clinicians, faced with a growing number of commercially available NMES devices and modalities, have little data on which to base decisions regarding which devices should be purchased or which modalities to offer to patients. Very few, and only small, studies have compared the efficacy of NMES modalities.14,15 This trial was undertaken to compare the efficacy of cyclic NMES, EMG-triggered NMES, and sensory stimulation on impairment and functional limitation in stroke patients with upper-limb hemiparesis. To the best of the authors’ knowledge, this study represents the largest clinical trial comparing EMG-triggered and cyclic NMES in the subacute stroke population. It was hypothesized that the cognitive input related to EMG-triggered NMES would result in significantly larger impairment reductions than cyclic NMES and that sensory stimulation would produce the smallest motor impairment reduction.
Methods
This was a multicenter, balanced randomization, single-blind, multiarm parallel-group study conducted in the United States at 3 medical centers. The study protocol was approved by the institutional review boards at each location. This trial was registered at ClinicalTrials.gov (NCT00142792).
Participants
Inclusion criteria were the following: (1) medically stable; (2) nonhospitalized adults within 6 months of stroke; (3) age 21 to 89 years; (4) required to have intact skin on the hemiparetic arm; (5) adequate cognition to participate (follow 3-step commands, recall 2 of 3 items at 30 minutes); (6) full passive range of motion of the wrist, thumb, index, and long finger metacarpophalangeal joints of the affected limb; (7) less than full strength of the affected limb; (8) a score less than 12 out of 14 points on the hand portion of the upper-extremity section of the Fugl-Meyer Assessment (FMA); (9) detectable, volitionally activated EMG signals from the wrist or finger extensors (extensor carpi radialis [ECR] or extensor digitorum communis [EDC] muscles); (10) the ability to tolerate NMES for wrist and finger extension; and (11) the ability to set up and operate the assigned NMES device independently or with assistance.
Exclusion criteria were the following: (1) insensate affected arm; (2) uncompensated hemineglect, as measured by testing for extinction on double simultaneous stimulation (visual or tactile) or by drawing a clock face; (3) history of cardiac arrhythmia with hemodynamic instability; (4) premorbid upper motor neuron lesion affecting the hemiparetic arm; (5) uncontrolled seizure disorder; (6) metacarpophalangeal joint or wrist pain to palpation or with extension; (7) implanted stimulator (such as cardiac pacemaker); and (8) pregnancy.
Randomization
Following consent, the nurse coordinator and the blinded assessor at each site determined eligibility using the above screening criteria. Participants who satisfied study criteria underwent baseline assessment prior to randomization. Once the candidate enrolled and completed baseline assessment, the treating therapist, who was not blinded, assigned participants to treatment groups via a computer-generated random, permuted, blocked randomization sequence (in blocks of 6) for each of the sites.
Interventions
Participants were randomized to receive either cyclic NMES, EMG-triggered NMES, or sensory stimulation (control) administered twice every weekday in 40-minute sessions, over an 8-week period. The treatment occupational therapist ensured that enrolled participants were able to demonstrate correct use of the device. Participants took the device home to complete the 8-week treatment protocol. Adherence visits were at least once weekly, occurring either at the participants’ homes or following the prescribed outcome visits on-site.
Cyclic NMES
Two 2-inch diameter surface electrodes attached to a commercially available stimulator (NeuroMove NM900, Zynex Medical, Lone Tree, CO) were placed over the motor points of the ECR and the EDC. When stimulation occurred, this configuration produced paretic wrist and finger extension. Stimulation intensity (pulse amplitude) was set to produce maximum finger and wrist extension without discomfort. Participants were instructed to “relax” during the treatment and not assist the NMES. Because simultaneous activation of the contralateral wrist and fingers may affect motor relearning, 10 participants were instructed to refrain from movement of the contralateral limb during treatment. Thus, the treatment provided muscle and joint proprioceptive feedback of the affected limb without a cognitive intent to extend the fingers and wrist.
Stimulation was delivered via a biphasic waveform, with a pulse duration of 300 µs. Pulse frequency was adjusted to participant comfort but kept between a range of 20 and 40 Hz. The duty cycle was initially set at 5 s on, 20 s off. The off time was decreased approximately every 3 days by 5 s, until the duty cycle was 5 s on and 5 s off. The internal memory in the stimulator was interrogated weekly to monitor adherence. Participants were also asked to maintain a diary documenting the treatment sessions.
EMG-Triggered NMES
Surface electrodes were placed in a manner identical to the Cyclic NMES group, with the goal of producing contraction of the ECR and EDC; however, stimulation was delivered only when the participant initiated wrist and or finger extension that generated an EMG signal from either muscle of sufficient magnitude to exceed a preset threshold of 10% of the maximum EMG signal during maximum contraction of the wrist and finger extensors. During the treatment, the participants were instructed to attempt to extend the wrist and fingers of the affected limb in response to an audio/visual cue issued from and displayed on the stimulator. Once the stimulation was successfully triggered, the participants were asked to relax and not assist the stimulation. Thus, the treatment provided muscle and joint proprioceptive feedback of the affected limb, coupled with a cognitive intent to extend the fingers and wrist. The rationale to relax during stimulation was 2-fold: (1) to isolate the effect of cognitive input that is required for EMG-triggered NMES and (2) to prevent the potential interference of voluntary contraction on electrical stimulation that can reduce the force of muscle contraction.16,17 The duty cycle, daily dose, and duration of treatment were identical to that in the cyclic NMES group. Stimulation intensity and frequency were set in the same manner. Thus, the only variable that was manipulated was the type of stimulation, per the study purpose.
Sensory Stimulation (Control)
Surface electrodes were placed in a manner identical to the cyclic and EMG-triggered NMES groups; however, the stimulation intensity was set above sensory threshold but below motor threshold. Thus, the treatment provided cutaneous afferent feedback but without muscle and joint proprioceptive feedback and without cognitive intent. The duty cycle, daily dose, and duration of treatment were identical to that in the cyclic and EMG-triggered NMES groups. Stimulation frequency was set at 30 Hz.
Outcomes
Outcomes assessments were completed at each site by a blinded occupational therapist at baseline, midtreatment, end of treatment, and 1, 3, and 6 months after completion of treatment. The primary outcome measure was the upper-extremity section of the FMA. Volitional movement of the upper limb (shoulder, elbow, forearm, wrist, and hand) is examined in and out of synergies. Each item is graded on a 0 to 2 ordinal scale and summed to provide a maximum score of 66. A post hoc outcome of the FMA limited to the wrist and hand subscales was undertaken because the interventions were limited to the wrist and hand, with a maximum score of 24.
A secondary outcome was the ability of a hemiparetic upper limb to execute specific activities and was assessed with the functional ability component of the Arm Motor Ability Test (AMAT). 18 The time component was excluded because of a significant floor and ceiling effect with respect to FMA, 19 and the number of compound tasks was reduced to reduce redundancy. The modified AMAT (mAMAT) consisted of 9 compound tasks excluding those tasks reliant on ambulatory skills. The tasks were scored on a 0 to 5 ordinal scale, with higher numbers signifying greater function of the hemiparetic limb. The scores across the 9 tasks were averaged to produce a final score with a maximum of 5.
The phase of spontaneous neurological recovery is important to consider when evaluating outcomes of treatment intervention. Studies have observed that the fastest pace of recovery tends to occur immediately after the stroke, with a slower pace as time passes.20-24 Furthermore, recovery tends to reach a plateau at approximately 12 weeks after stroke.21,23,24 In this study, participants were divided into those who were 6 weeks or less after stroke, and thus would receive half of the treatment intervention within the first 12 weeks, and those who were longer than 6 weeks from their stroke.
Concurrent Therapies
Many subacute stroke survivors exhibit multiple sequelae requiring additional rehabilitation therapy interventions; however, concurrent therapy can bias outcomes. But limiting provision of concurrent therapies in a subacute population would be unethical. Thus, the total number of hours of physical and occupational therapy sessions were monitored during the entire study period. In addition, other interventions such as botulinum toxin injections, intrathecal baclofen, shoulder corticosteroid injections, use of a shoulder sling, and use of a resting hand splint were monitored throughout the study.
Data Analyses
Power
This study was powered to detect differences in upper-extremity FMA scores of a minimum effect size of 0.8 at a significance level of .01, the smallest effect size difference anticipated between cyclic NMES and sensory stimulation, based on prior studies.7,9 A minimum of 50 participants per group was required to detect differences between groups with a power of 90%. The sample sizes were sufficient to detect the lower estimate of 4.25 points for the minimum clinically important difference (MCID) 25 between the EMG-triggered NMES and each of the other groups at all follow-up time points. A significance level of .01 in the power analysis was taken because for each measurement occasion, 3 post hoc tests are needed. In addition, to account for an anticipated drop-out rate of 20%, the minimum number of participants required to enroll per group was increased to 63 for a total of 189 participants for the entire study.
Outcome Analyses
The effect of treatment group over time was analyzed using a linear mixed model for repeated measures for each outcome measure, with SAS software, version 9.3 (SAS Institute Inc, Cary, NC). A random intercept for each participant with a first-order antedependent covariance structure was used because it is reasonable to assume that for each individual, there is a greater correlation between assessments that are closer together in time and that variance might be different at different assessments. Preliminary statistical testing rejected the hypothesis of equality of slopes among the sites; thus, a fixed effect for site was added to the model. Missing data were handled by a maximum likelihood algorithm under the assumption that the missingness was random. The analyses were conducted by the available-case, intention-to-treat method; that is, all data were included in the analysis, and the data were analyzed with all participants remaining in the treatment group in which they were initially randomized.
Post hoc analyses to control for phase of spontaneous neurological recovery were completed. The linear mixed model as described above was analyzed with the addition of fixed effects for phase of recovery (within 6 weeks of stroke at baseline), the interaction with treatment assignment, the interaction with time, and the interaction with treatment assignment and time.
Post hoc analyses to estimate the FMA, the FMA wrist and hand subscales, and the mAMAT outcomes at the end of treatment and at 3 and 6 months after the end of treatment were completed to improve interpretation of the results because the recruitment goal was not met. The same linear mixed model analyses as previously described were performed with 6 discrete time points (at baseline, midtreatment, end of treatment, and 1 month, 3 months, and 6 months after completion of treatment). Least-squares means point estimates and 95% CIs for each group were computed from the model in an intention-to-treat manner using all available data.
To characterize the magnitude of change over time, the effect sizes of the cyclic and EMG-triggered NMES groups compared with the sensory stimulation group were calculated. The mean difference scores were calculated by subtracting the mean estimated change from baseline to the end of treatment (EOT), 3-month, and 6-month follow-up assessments for the cyclic and EMG-triggered NMES groups, from the mean estimated change from baseline to follow-up for the sensory stimulation group. Predicted values from the mixed linear regression analysis with discrete time points generated the difference scores. The Cohen’s d treatment effect sizes were calculated by dividing the mean difference scores by the baseline standard deviation of the sensory stimulation group. Cohen’s d values of 0.2, 0.5, and 0.8 represent small, moderate, and large effect sizes, respectively. 26
Between-group comparisons for treatment adherence, diary completion, and concurrent therapies were analyzed with a Kruskal-Wallis test for continuous variables and a χ2 test for dichotomous variables.
Results
Participant Demographics
Out of a total of 1197 stroke survivors who were prescreened for eligibility, 122 met study criteria, agreed to participate and were randomized (Figure 1). Time from stroke at enrollment ranged from 12 days to 6.0 months. 109 (89.3%) participants completed the treatment interventions as assigned, and 83 (68.0%) completed all outcomes assessments. The demographic characteristics were similar among the treatment groups (Table 1). The impairments did not consistently differ in such a way that a single group was consistently more severely affected than the others. One participant in the EMG-triggered NMES group delayed the 1-, 3-, and 6-month follow-up outcome assessments because of difficulty with transportation and scheduling, which resulted in the final assessment being at 9 months. These data were included in the analysis.
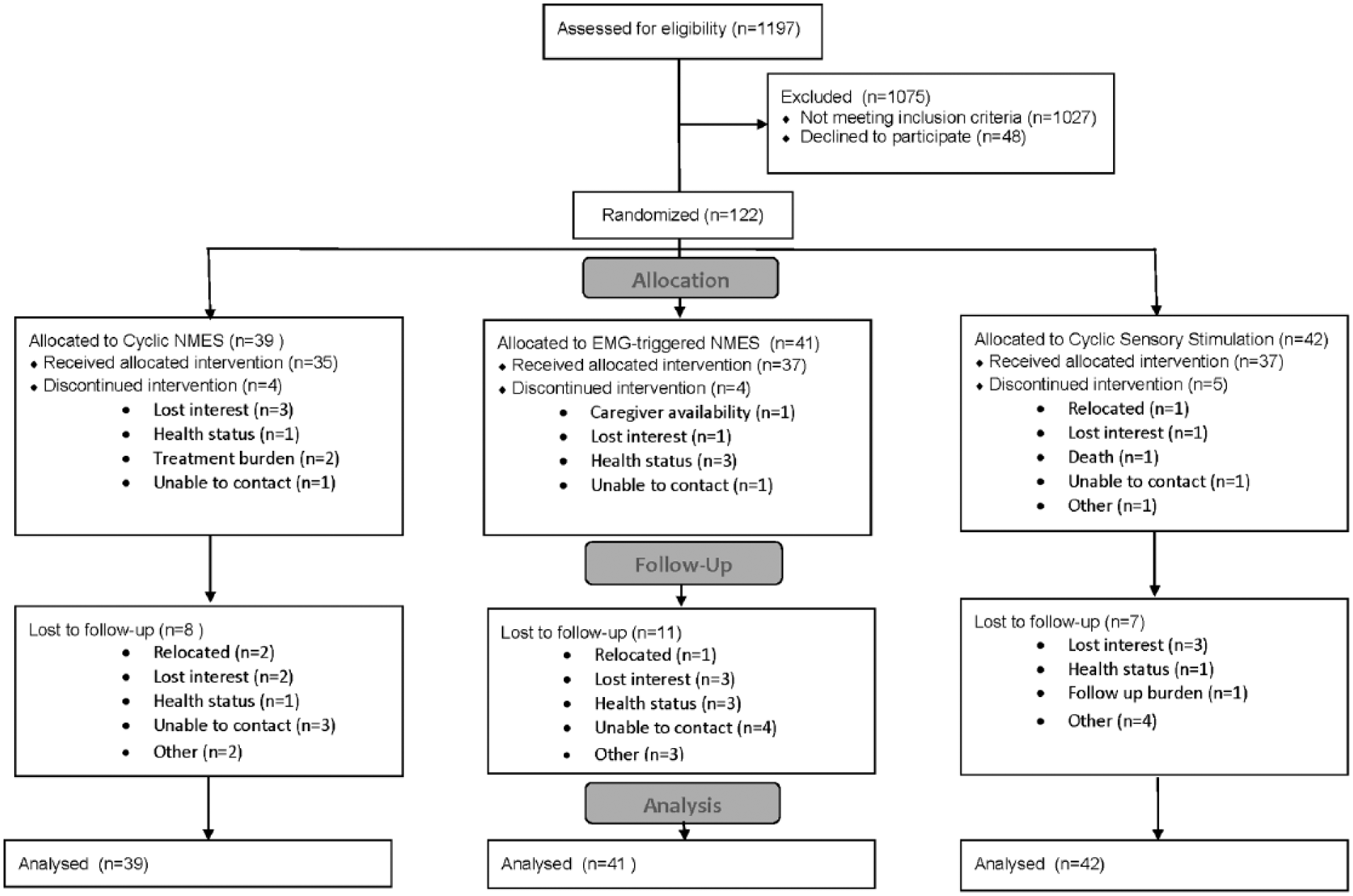
Participant flow diagram.
Demographic Characteristics.
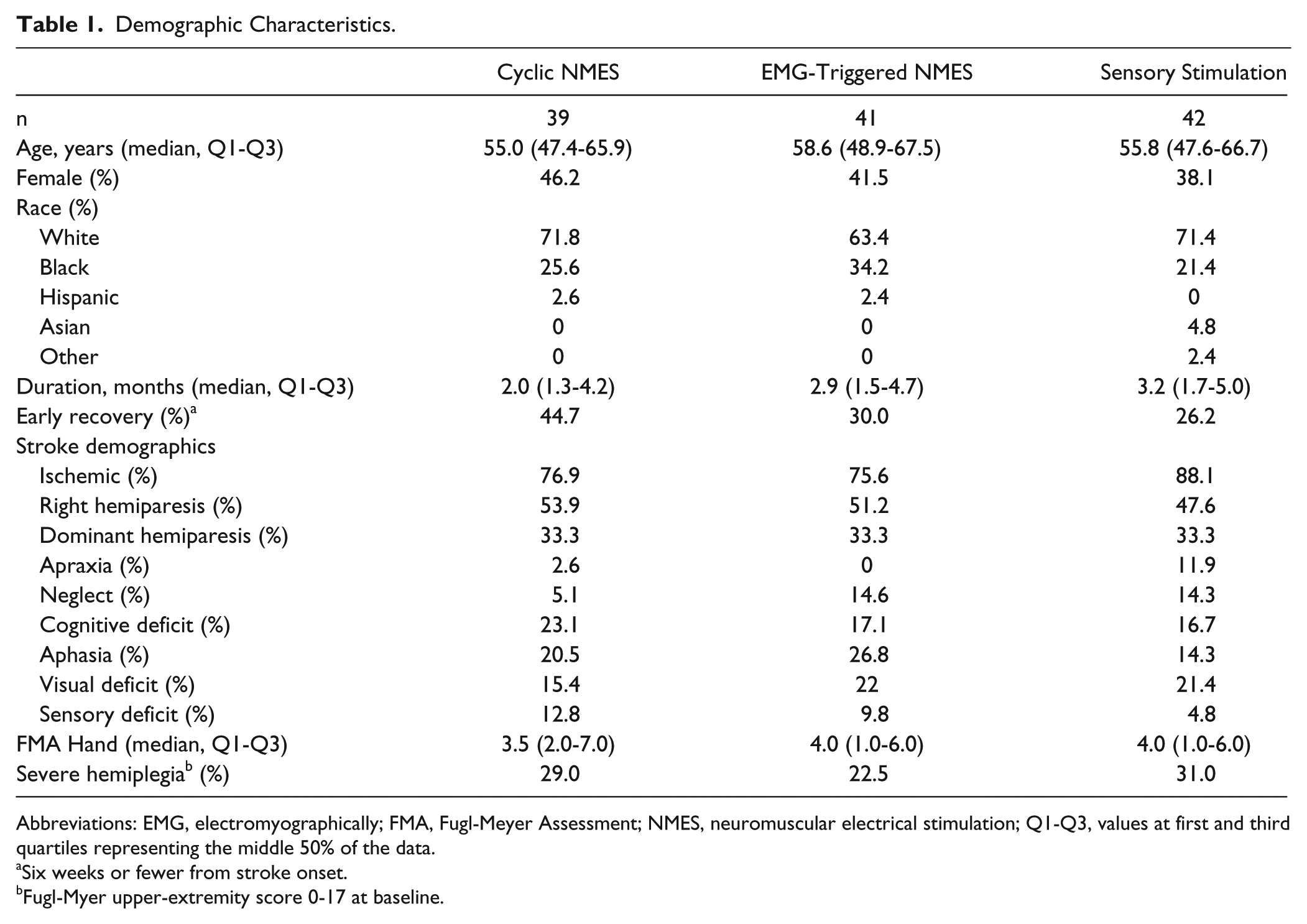
Abbreviations: EMG, electromyographically; FMA, Fugl-Meyer Assessment; NMES, neuromuscular electrical stimulation; Q1-Q3, values at first and third quartiles representing the middle 50% of the data.
Six weeks or fewer from stroke onset.
Fugl-Myer upper-extremity score 0-17 at baseline.
Fugl-Meyer Assessment Outcomes
No differences were observed (Figure 2) in magnitude of change in FMA score among treatment groups [Time × Group interaction effect: F(2, 384) = 0.2, P = .83], although there was a significant score increase with treatment [time effect: F(1, 111) = 92.6, P < .001]. Cohen’s effect size values for EMG-triggered NMES (d = 0.03, −0.01, and 0.08) and cyclic NMES (d = −0.12, −0.08, and −0.09) at EOT, 3 months, and 6 months, respectively, suggest low clinical significance in FMA. No differences were observed in magnitude of change in FMA wrist and hand subscales among treatment groups [Time × Group interaction effect: F(2, 384) = 0.4, P = .70], although there was a significant score increase with treatment [time effect: F(1, 111) = 66.7, P < .001]. Cohen’s effect size values for EMG-triggered NMES (d = −0.08, −0.02, and 0.20) and cyclic NMES (d = −0.07, −0.08, and −0.08) at EOT, 3 months, and 6 months, respectively, suggest low clinical significance in FMA wrist and hand. The estimates of the FMA outcomes assessments, adjusted for site, are available in Table 2.
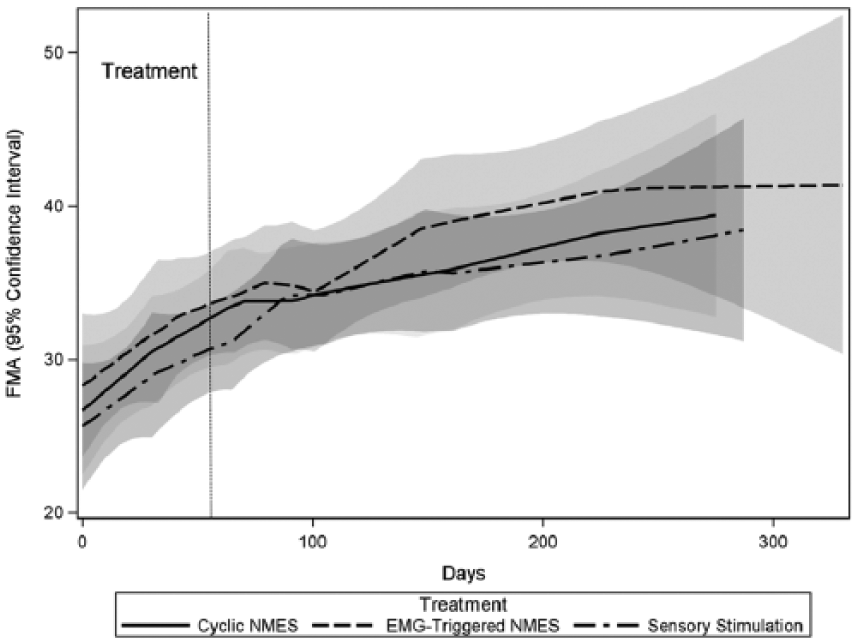
FMA Upper Limb for each treatment group over the course of the study. The shaded areas indicate the 95% CI of the group mean.
Outcomes Assessments. a
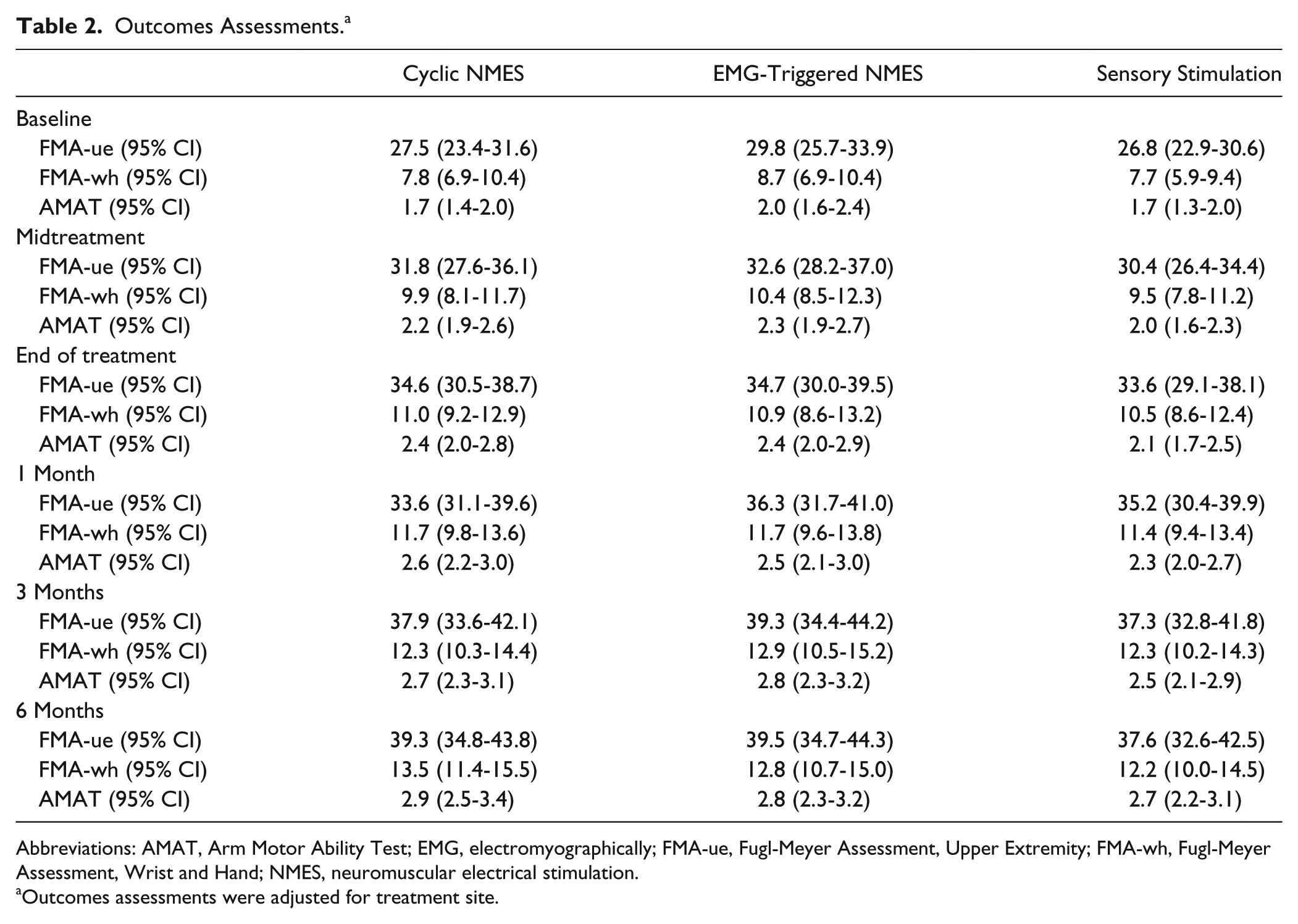
Abbreviations: AMAT, Arm Motor Ability Test; EMG, electromyographically; FMA-ue, Fugl-Meyer Assessment, Upper Extremity; FMA-wh, Fugl-Meyer Assessment, Wrist and Hand; NMES, neuromuscular electrical stimulation.
Outcomes assessments were adjusted for treatment site.
Modified Arm Motor Ability Test Outcomes
No differences were observed (Figure 3) in magnitude of change in mAMAT scores among treatment groups [Time × Group interaction effect: F(2, 379) = 1.2, P = .31], although there was a significant improvement with treatment [time effect: F(1, 111) = 91.0, P < .001]. Cohen’s effect size values for EMG-triggered NMES (d = 0.22, 0.18, and 0.19) and cyclic NMES (d = 0.04, −0.02, and −0.18) at EOT, 3 months, and 6 months, respectively, suggest low clinical significance. The estimates of the mAMAT outcomes assessments, adjusted for site, are available in Table 2.
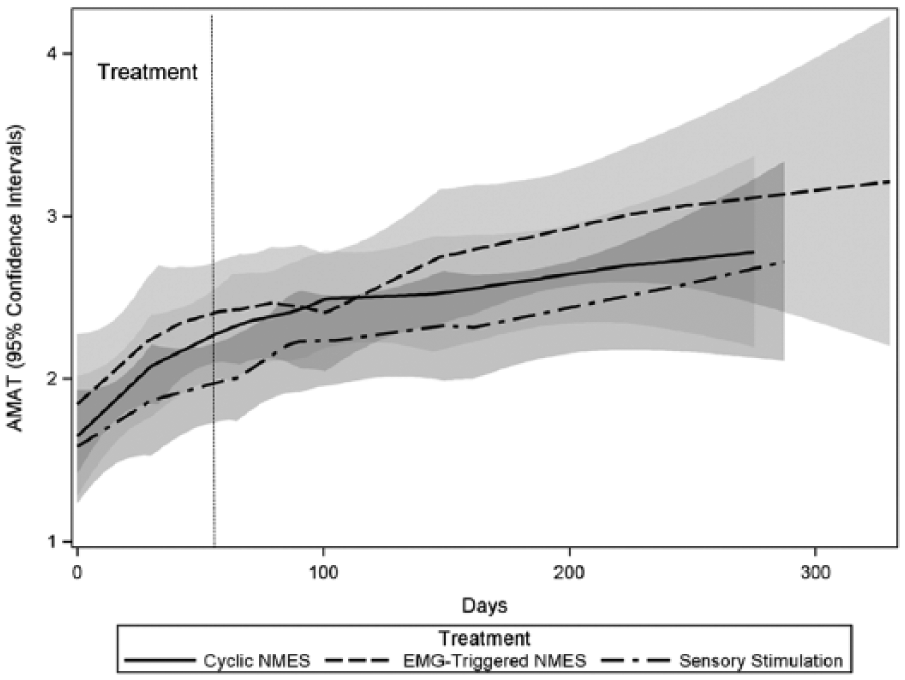
AMAT for each treatment group over the course of the study: the shaded areas indicate the 95% CI of the group mean.
Adherence and Provision of Concurrent Therapies
There was a significant difference in adherence to the prescribed stimulation dose when comparing the proportion of prescribed minutes completed each week among the groups (H = 9.4, P = .008; Table 3), with the adherence of the EMG-triggered NMES group being lower than that of the other 2 groups. There were no significant differences between groups in regard to the amount of exposure to concurrent therapies. To control for the difference in stimulation adherence, the models were analyzed with the addition of mean adherence for each individual over the treatment period added as a fixed effect. With the addition of adherence to the models, there was still no significant difference among treatment groups for either FMA (Time × Group interaction effect: F(2, 366) = 0.4, P = .66) or mAMAT [Time × Group interaction effect: F(2, 367) = 1.4, P = .25].
Treatment Adherence and Concurrent Therapies.
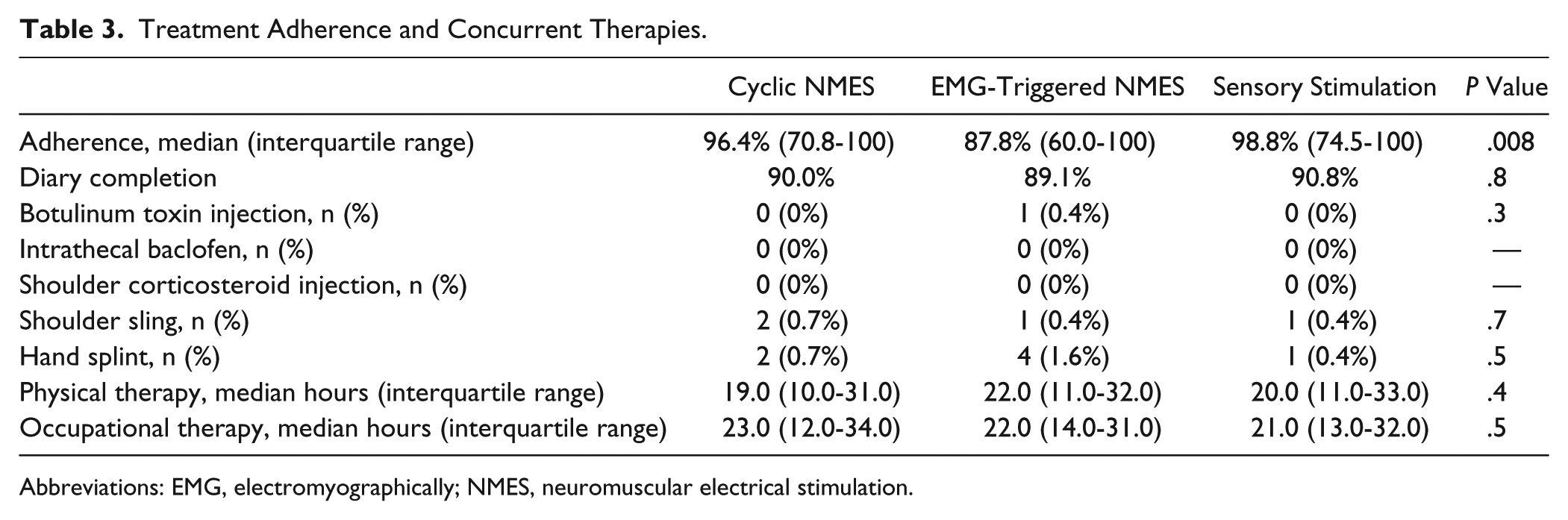
Abbreviations: EMG, electromyographically; NMES, neuromuscular electrical stimulation.
Discussion
This multisite, randomized controlled trial (RCT) compared the effect of cyclic NMES, EMG-triggered NMES, and sensory stimulation on paretic upper-extremity impairment and activity limitations in stroke survivors with subacute upper-limb hemiparesis. The expectation that, as a result of spontaneous recovery, all groups would exhibit score increases on motor impairment measures and functional ability relative to baseline 27 was supported by the data; however, the hypothesis that participants treated with NMES would exhibit larger score increases compared with participants treated with sensory stimulation was not supported. Furthermore, the hypothesis that participants treated with EMG-triggered NMES would exhibit greater score increases on the FMA, which measures neurological recovery within the context of the motor system, 28 and mAMAT, which measures hand-dependent functional tasks, 28 compared with participants treated with cyclic NMES was not supported. When considering the effect size of the outcomes, it is apparent that treatment with either NMES paradigm did not cause meaningful change in any of the outcomes measures. Analysis of the FMA wrist and hand subscales, which focused on movements that the NMES intervention groups practiced, also failed to detect a difference between groups. Adjusting for phase of spontaneous recovery20-24 did not alter the results.
It has been proposed that improvement of motor function associated with repetitive movements is mediated by afferent input to the central nervous system.29-32 Thus, motor stimulation, which provides cutaneous and proprioceptive afferent feedback, was hypothesized to be more effective in motor relearning than sensory stimulation alone, which is limited to cutaneous feedback. It is also believed that intention-driven movement, with close temporal association of motor intention (central neural activity) and stimulated motor response (peripheral neural activity) is important for electrical stimulation–based motor relearning therapies. It is not clear why, in this study, differences in motor impairment and function were not found to be associated with the different treatment paradigms. However, the lack of functional task practice may have contributed to the study results.
The results of this study are consistent with the results of smaller trials comparing EMG-triggered NMES and cyclic NMES. A RCT of 31 individuals with subacute stroke that compared a 3-week treatment of EMG-triggered NMES with cyclic NMES found that both were superior to sham stimulation, though without significant differences between the 2 treatments. 14 Another RCT of 22 individuals with subacute stroke that compared a 6-week treatment of EMG-triggered and cyclic NMES showed improvements in both groups without finding a difference between them. 15 That this study, which included a larger sample size (n = 109) and a longer treatment duration (8 weeks), also failed to detect a difference between EMG-triggered and cyclic NMES treatment protocols provides the strongest evidence that one treatment method should not be chosen over the other.
It is possible that EMG-triggered NMES, as used in this study, did not incorporate an adequate level of cognitive input (ie, motor intention) to improve motor relearning when compared with the other modalities. Motor intention was required to trigger electrical stimulation that produced wrist and finger extension; however, participants were then asked to relax once the stimulation commenced. Relaxation during stimulated muscle contraction effectively unpaired the motor intention and peripheral neural activity, which might have reduced the effectiveness of the intervention and its contrast with cyclic NMES. 33 That is, EMG-triggered stimulation may not have created a close enough temporal association of motor intention and stimulated motor response.
There are limitations with this study that are relevant to interpretation of the results. First, the estimated sample size needed to reach 90% power to detect clinically meaningful differences within the groups was not met because of slow recruitment. The lower power creates the possibility that a type II error was made. Table 4 shows that, at the extremes of the 95% CIs, the differences in the outcomes for FMA could exceed the lower estimate of the MCID. The MCIDs for the FMA wrist and hand and the mAMAT have not been established. Second, it is not clear if the improvements all 3 groups experienced are a result of the treatments they received in this study or a result of spontaneous recovery and whatever concomitant therapy they received. This study did not limit by intact corticomotor function, necessary for capacity for spontaneous recovery, 34 or by type of stroke. As such, it is not possible to know if differences in efficacy between the treatment paradigms would have emerged with application of alternative participant selection criteria. Third, because sensory stimulation can reduce motor impairment, 35 it was not a true placebo group. Therefore, it is possible that all 3 groups improved more than they would have if they had not received the interventions tested in this study. Nevertheless, what this study does make clear is that merely triggering NMES is not enough to improve on the outcomes achieved with cyclic NMES in subacute patients. It is also possible that important impairments were not equally represented in participants between treatment assignments. There were differences in proportions of participants in the early phase of recovery, with severe hemiplegia, with compensated neglect, and with sensory, cognitive, communicative, and visual impairments; however, the differences in impairments did not affect one group in particular. Finally, although the outcomes assessor was blinded, participants and treatment therapists were not, and thus, bias is still possible.
Between-Group Differences in Outcomes Assessments. a
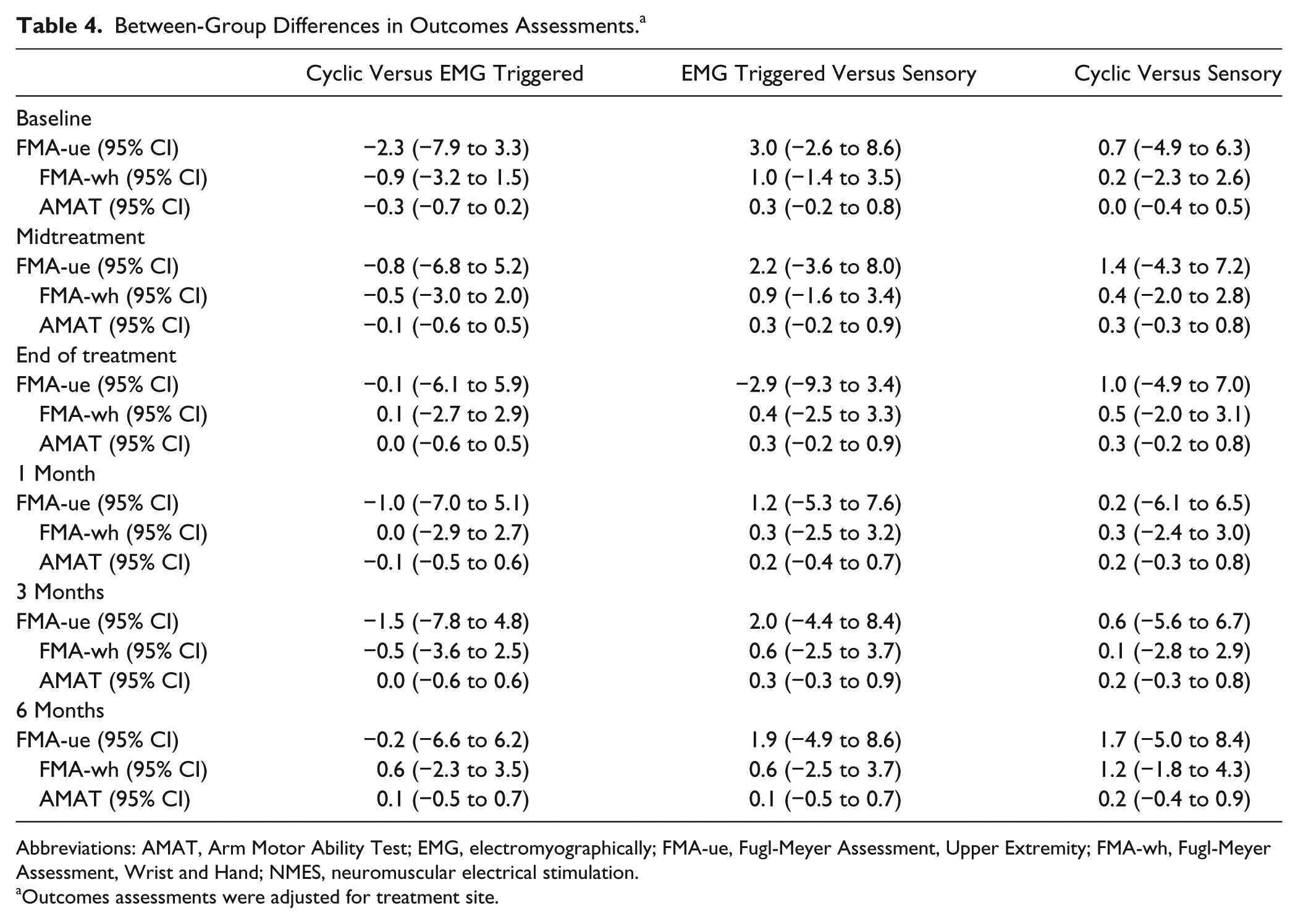
Abbreviations: AMAT, Arm Motor Ability Test; EMG, electromyographically; FMA-ue, Fugl-Meyer Assessment, Upper Extremity; FMA-wh, Fugl-Meyer Assessment, Wrist and Hand; NMES, neuromuscular electrical stimulation.
Outcomes assessments were adjusted for treatment site.
Conclusion
This multisite RCT demonstrated equal, statistically significant increases in upper-extremity motor impairment in subacute stroke survivors with upper-limb hemiparesis, with an 8-week treatment with cyclic NMES, EMG-triggered NMES, and sensory stimulation. There was no difference between groups based on the stimulation treatment paradigm, and treatment effects were negligible. Merely triggering NMES with EMG signal is not enough to improve on the outcomes achieved with nontriggered cyclic NMES or sensory stimulation. There was no evidence that time poststroke influenced response to treatment.
Footnotes
Authors’ Note
ClinicalTrials registration: https://clinicaltrials.gov/ct2/show/NCT00142792?term=NCT00142792&rank=1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01HD049777).