
Abstract
Background. The effect of levodopa on postural motor learning in people with Parkinson’s disease is poorly understood. In particular, it is unknown whether levodopa affects improvement in protective postural responses after external perturbations such as a slip or trip, a critical aspect of fall prevention. Objective. Determine the effect of levodopa on postural motor learning in people with Parkinson’s disease. Methods. We assessed improvement in protective postural responses in people with Parkinson’s disease over short-term (1 day) perturbation training on and off levodopa. We also assessed retention and generalization of improvement. Participants were 22 individuals with Parkinson’s disease. The primary outcome was total center of mass (COM) displacement after perturbation. Secondary outcomes assessed first step performance and included margin of stability at first foot contact. Results. People with Parkinson’s disease improved COM displacement (P = .011) and margin of stability (P = .016) over training. Improvements in these outcomes were more pronounced after training while on levodopa than off levodopa. Levodopa State × Training interactions were not observed for other step performance variables (eg, step latency, length, total number of steps). Improvements were retained for 24 hours, and for margin of stability, retention was more pronounced while on levodopa than off (P = .018). Conclusions. Individuals with Parkinson’s disease are able to improve protective postural responses through short-term perturbation training, and improvements were more pronounced when on levodopa for some variables. Perturbation training may be more effective if completed while optimally medicated with levodopa.
Introduction
Falls in people with Parkinson’s disease (PD) lead to frailty, depression, reduced quality of life, and mortality. 1 Postural dysfunction is the most common reason for falls in PD.2-7 Automatic postural responses after external perturbations, such as a trip or a slip, are critical for fall prevention8,9 and are dysfunctional in people with PD. In particular, protective steps that occur in response to external perturbations are often later and smaller in people with PD, likely contributing to imbalance and falls.10,11
Perturbation training (ie, repeated exposure to perturbations that elicit a protective step) improve postural responses in healthy older adults9,12 and people with PD. 2 Jobges et al 2 showed that 2 weeks of exposure to external perturbations (via shoulder tugs) resulted in improved protective movements. Critically, these improvements were retained for 2 months. However, this study was carried out in the on levodopa state—that is, during optimal dopaminergic treatment. Motor learning, which is the basis of rehabilitation, may be affected by dopamine.13,14 In fact, upper-extremity motor learning studies show that levodopa may have negative effects on learning.15-18 Kwak and colleagues demonstrated that improvements during the acquisition phase of explicit sequence learning were impaired while on levodopa, possibly because of levodopa “overdosing” of the ventral striatum.13,14,17
Several recent reports suggest that motor learning of posture and gait tasks may be either unaffected19,20 or improved 21 with the use of levodopa. Anderson et al 19 investigated the effect of levodopa on the center of mass (COM) velocity while voluntarily leaning toward a target. Results showed that although levodopa improved performance (faster velocity), it did not affect the amount of improvement over the course of training. Similarly, Hayes et al 20 demonstrated that postural sequence learning was unaffected by levodopa in people with PD. Roemmich et al 21 investigated the effects of levodopa on adaptation of symmetry of step length after split-belt treadmill manipulations. Results showed (as in the study by Anderson and colleagues) that people with PD adapted to split-belt conditions similarly on and off medications. However, the storage or aftereffects were more pronounced on levodopa compared with off.
Together, these findings suggest that the effects of levodopa on learning are mixed. Importantly, no investigations have studied the effects of levodopa on improvement of protective postural responses, including stepping, in response to external perturbations. Given the importance of postural responses in fall prevention8,9,12 and the small, slow protective steps commonly observed in people with PD,10,11 a better understanding of how levodopa effects improvements in protective postural responses via perturbation training can inform neurorehabilitation. Specifically, these results can help inform whether balance rehabilitation is most effective on or off levodopa.
Thus, we investigated how anti-Parkinson’s medication (levodopa) alters postural motor learning in people with PD. Specifically, we investigated how levodopa affects (1) improvement of postural performance over 1 day of perturbation training, (2) retention of improvements, and (3) generalization of improvement to a nontrained perturbation task.
Methods
Participants
Participant characteristics are presented in Table 1. In all, 22 individuals with confirmed idiopathic PD participated. Inclusion criteria were the following: currently taking levodopa, ability to stand without aid for >1 hour, no neurological diagnoses other than PD, and no orthopedic injuries in the previous 6 months that interfered with gait or balance. Participants exhibited worse motor signs (Movement Disorders Society Unified Parkinson’s Disease Rating Scale Part III) and balance (Mini Balance Evaluation Systems Test) when off levodopa with respect to on (Table 1).
Participant Characteristics.
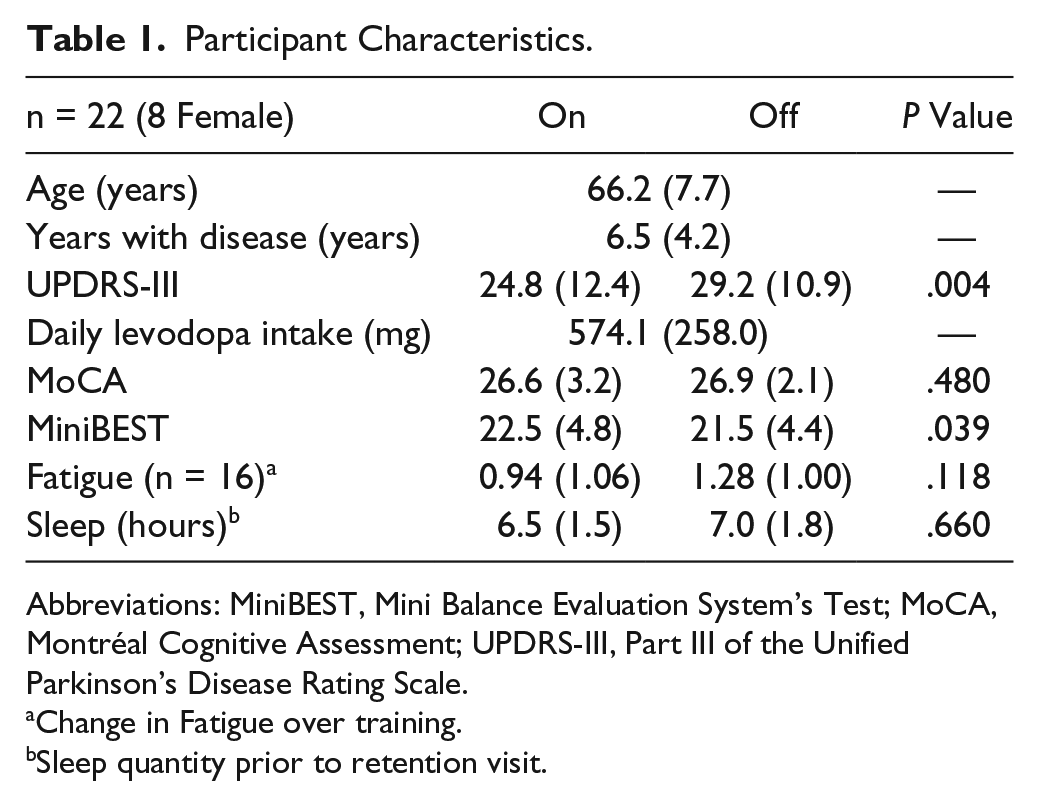
Abbreviations: MiniBEST, Mini Balance Evaluation System’s Test; MoCA, Montréal Cognitive Assessment; UPDRS-III, Part III of the Unified Parkinson’s Disease Rating Scale.
Change in Fatigue over training.
Sleep quantity prior to retention visit.
Fatigue was captured on a subset of participants (n = 16). Participants rated their physical fatigue as 1 to 10 (1 = no fatigue; 10 = most fatigue) throughout the testing session. Average fatigue during on and off training sessions was low (2.5 ± 1.5 and 3.15 ± 1.9, respectively), although this difference was significantly different (P = .018; Table 1). However, the change in fatigue from the beginning of the session to the end of the session was not different across levodopa states (Table 1). Given the importance of sleep in learning, we recorded self-reported hours of sleep between testing and retention visits. No differences were observed on or off levodopa (Table 1). All participants provided informed consent, and the research protocol was approved by the Oregon Health and Science University Institutional Review Board.
Experimental Design
Protocol Outline
Improvements in protective postural responses were assessed on and off levodopa in the same participants (Figure 1A). Participants first completed a training/retention assessment over 2 consecutive days. The same participant then repeated this 2-day assessment after a washout period (described below). Assessments were exactly the same, except that participants withdrew from levodopa use for 1 of the 2 assessments. For the off levodopa assessments, participants withdrew from all anti-Parkinson medication (levodopa and dopamine agonists) for 12 hours before arrival. Assessments were separated by a washout period of >6 weeks (mean ± SD = 9.47 ± 3.79 weeks) to minimize the carryover of improvement between the first and second training/retention assessments. To further account for the possibility of carryover of training, the order of medication testing was randomized such that 12 of the 22 participants were tested in the on state first, and 10 participants were tested in the off state first.
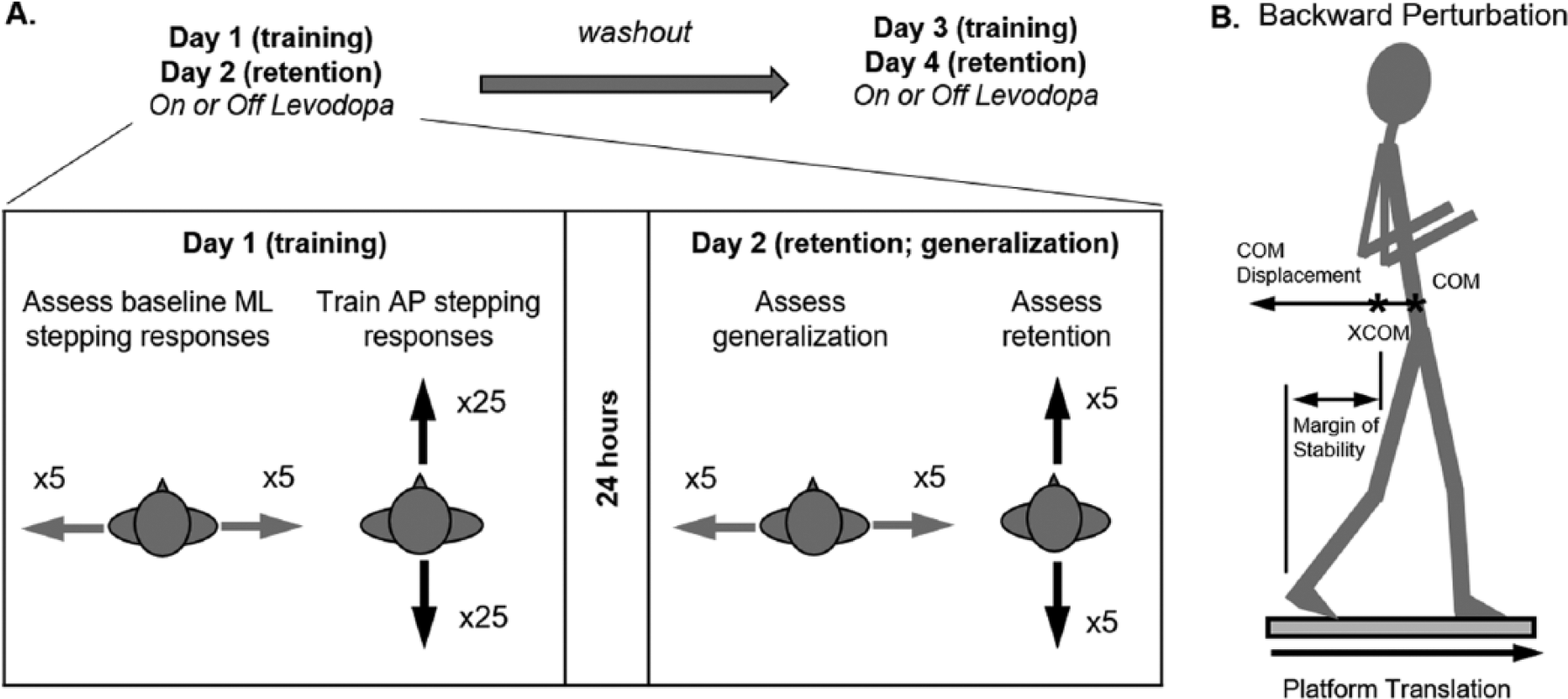
(A) Schematic of data collection protocol (day 1 [training] and day 2 [retention]) conducted both in the on state and in the off state. Among the participants, 12 completed testing on first, whereas the other 10 completed testing off first. Perturbations within each block (anterior-posterior [AP] or mediolateral [ML]) are randomized. (B) Schematic of primary outcome variables, including center of mass (COM) and margin of stability, which is calculated using the extrapolated center of mass (XCOM). See text for further details.
Description of Support Surface Perturbations
Participants stood on computer-driven moveable force plates. They underwent a series of perturbations in the anterior-posterior (AP) and medial-lateral (ML) directions. Throughout the article, perturbation direction will refer to the direction of postural sway induced by the surface translation. Thus, a backward perturbation refers to forward movement of the support surface inducing backward body sway and stepping (Figure 1B). Perturbations were delivered via surface translations, a reliable way to examine compensatory stepping responses. 22 For all perturbations, participants stood with feet together, arms crossed across their chest, and eyes open. Starting foot position was held constant across trials and participants. Participants were instructed to “not anticipate upcoming perturbations and to react naturally to the perturbation when trying to keep balance.” Open-ended instructions were provided to avoid altering participants’ natural protective postural responses. Participants wore a safety harness that was attached to the ceiling but did not provide body weight support. Timing of perturbation onset was randomized between 2 and 10 s.
Training and Retention Assessment
Day 1 (training)
Reflective markers were placed on boney landmarks of the torso and lower limbs. Then, participants underwent 3 perturbation stages: perturbation familiarization, generalization testing, and training protocol. Participants were notified when they moved through each stage.
Perturbation familiarization (AP and ML perturbations). Participants first underwent 3 familiarization perturbations consisting of forward (9 cm, 18 cm/s) and left (9 cm, 14.6 cm/s) translation and a toes-up rotation (4°, 20°/s). They were then exposed to 12 perturbations (3 per direction; forward, backward, left, and right). These perturbations started small (forward and backward: 9 cm, 18 cm/s; left and right: 9 cm, 14 cm/s) and increased to a large amplitude and velocity (forward and backward: 15 cm, 56 cm/s; left and right: 15 cm, 21 cm/s).
Generalization testing (ML perturbations). To obtain a baseline measure of ML protective stepping responses, participants were exposed to 5 leftward and 5 rightward translations. Perturbation direction was randomized to prevent anticipatory biomechanical changes such as leaning.
Training protocol (AP perturbations). Participants were then exposed to 25 forward and 25 backward perturbations. Perturbations were randomly ordered and separated into blocks of 10 (5 forward and 5 backward). Perturbations for 20 of 22 participants were 15 cm and 56 cm/s. Two participants required smaller perturbation sizes (9 cm, 18 cm/s). For all individuals, perturbation size and speed was consistent across assessments.
Day 2 (Retention/Generalization)
Participants returned to assess retention and generalization 24 hours after day 1. Familiarization and generalization stages were completed exactly as on day 1. Then, participants completed 10 AP perturbations (5 per direction, random order) to assess retention of improvements on the trained task.
As noted above, the order of perturbations was randomized. However, the same sequence was used for all participants. Furthermore, the sequence of the 10 AP perturbations on day 2 was the same as the first 10 AP perturbations used on day 1. Similarly, the sequence of the 10 ML perturbations were the same on days 1 and 2. The same sequences were used at both training and retention assessments (before and after washout).
Data Analysis and Variables of Interest
The primary variable of interest was total displacement of the whole-body COM after perturbations because it has previously been used as a global measure of performance after perturbations.23-25 The position of whole-body COM was derived from the weighted sum of the individual limb COM locations using a custom-designed MATLAB program (Mathworks, Natick, MA), segment kinematics, and anthropometric data.26,27 Marker data were captured at 120 Hz via a motion analysis system (Motion Analysis Corporation, Santa Rosa, CA). Data were filtered with a fourth-order Butterworth low-pass filter at a frequency of 5 Hz. COM displacement was then calculated as the AP distance traveled by the whole-body COM with respect to its position at perturbation onset.
The first protective step after a perturbation is critical for preventing falls. Thus, secondary variables focused on characteristics of the first step and included margin of stability, step length, step latency, and number of steps. Margin of stability was identified as the distance between the boundary of support and the extrapolated COM (XCOM) at first foot contact. 28 For example, during a backward stepping perturbation, margin of stability was the distance between the XCOM and heel of the stepping foot when that foot touches down (Figure 1B). XCOM is defined as follows:
where x is the position of the vertical projection of the COM to the ground, Vx is the AP velocity of the COM, and
Statistical Analysis
We assessed the effects of levodopa on (1) improvement of protective postural responses over the course of training, (2) retention of improvement over 24 hours, and (3) generalization to nontrained perturbation tasks.
Improvement Over the Course of Training
Data were tested for skewness using the Shapiro-Wilk test. If small or modest skewness was observed (P > .01; Shapiro-Wilk test), parametric tests were used. Repeated measures were used for all analyses. Repeated-measures ANOVAs with repeated effects on dopamine status (on vs off) and time (day 1, blocks 1-5) assessed improvement across training and medication state as well as Medication × Training interactions.
If skewness was observed (P < .01; Shapiro-Wilk test), nonparametric statistical assessments were used. Training effects (collapsed across medication state) and medication effects (collapsed across time) were assessed via Wilcoxon signed-rank tests. To assess interaction effects between training and medication (ie, whether improvement in performance differed on and off levodopa), we first calculated performance improvement in each medication state separately by taking the difference between day 1, block 1 and day 1, block 5. This difference score was compared across medication states via Wilcoxon signed-rank tests. If a significant Training × Medication interaction was observed, post hoc across-time paired-sample t tests or Wilcoxon signed-rank tests were run separately for each medication state.
Retention
Retention was assessed only in variables that exhibited significant training effects. Similar to the training assessment described above, repeated-measures ANOVAs or Wilcoxon signed-rank tests assessed whether day 2 performance was different from baseline performance (day 1, block 1) and whether improvements were retained similarly on and off levodopa. This analysis determined if variables measured at day 2 remained significantly different from the beginning of day 1.
Generalization
To assess generalization, COM displacement after ML perturbations were compared before and after AP perturbation training. A mixed-model ANOVA assessed generalization effects (across time), medication effects, and Generalization × Medication interactions. We also assessed, via a paired-sample t test, whether baseline performance (at block 1) was similar across medication states. Significance level (α) was set to .05 for all analyses.
Results
Training and Retention
Stepping performance and statistics for all outcome variables after backward and forward perturbations are shown in Table 2.
Forward and Backward Protective Stepping Performance Across Training in People With PD On and Off Levodopa. a
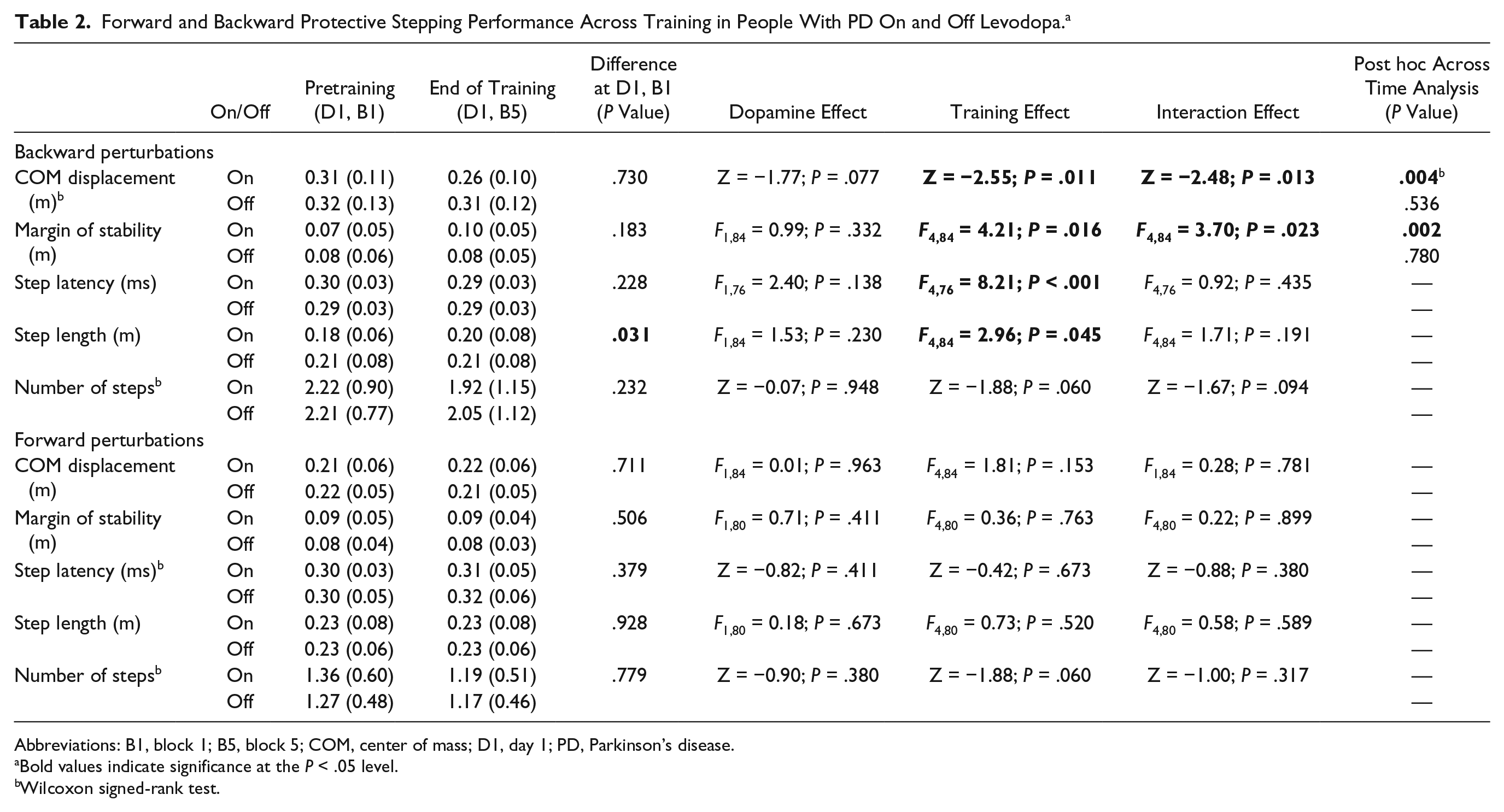
Abbreviations: B1, block 1; B5, block 5; COM, center of mass; D1, day 1; PD, Parkinson’s disease.
Bold values indicate significance at the P < .05 level.
Wilcoxon signed-rank test.
Backward Perturbations
COM displacement
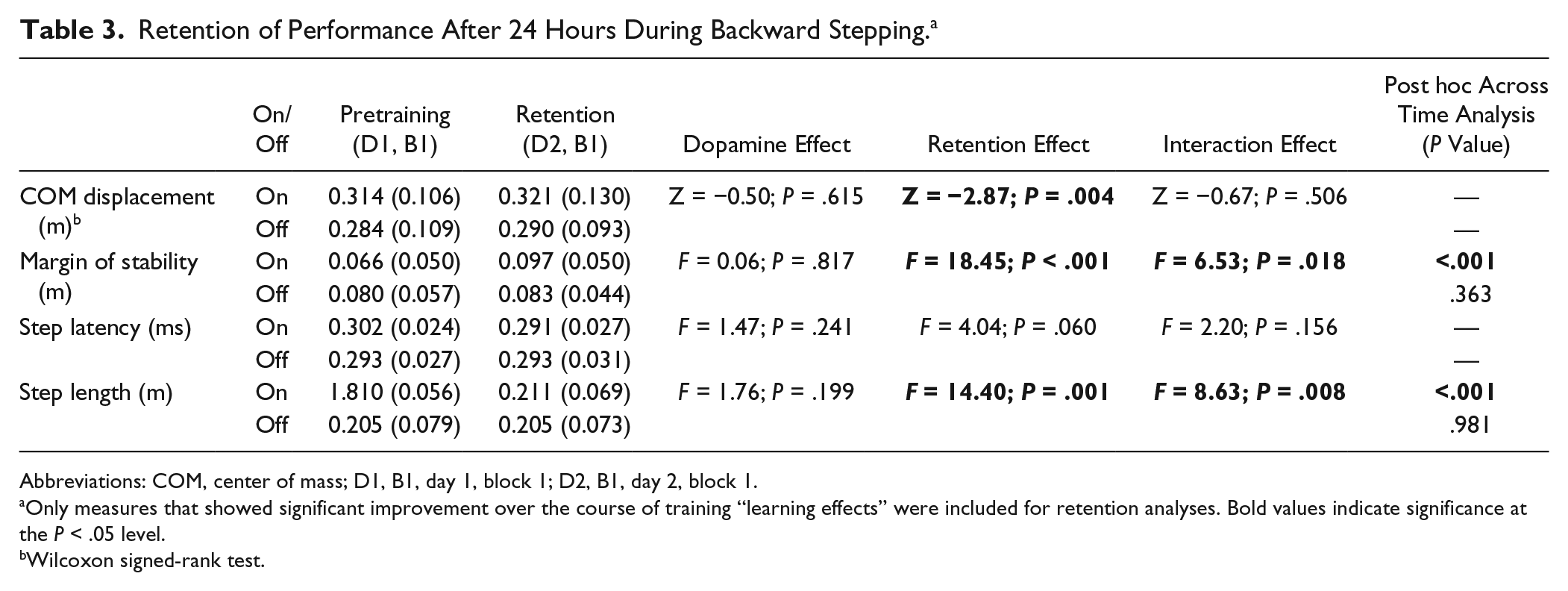
COM displacement after surface translations was significantly reduced over training (Table 2). A significant interaction effect was a result of more pronounced reduction in COM displacement on levodopa compared with off. Post hoc analyses confirmed this interaction effect because there was a significant improvement in COM displacement from the beginning to the end of training on, but not off, levodopa (Table 2, Figure 2). Improvements were retained the day after training, but no differences were observed across medication state in the degree of retention (Table 3).
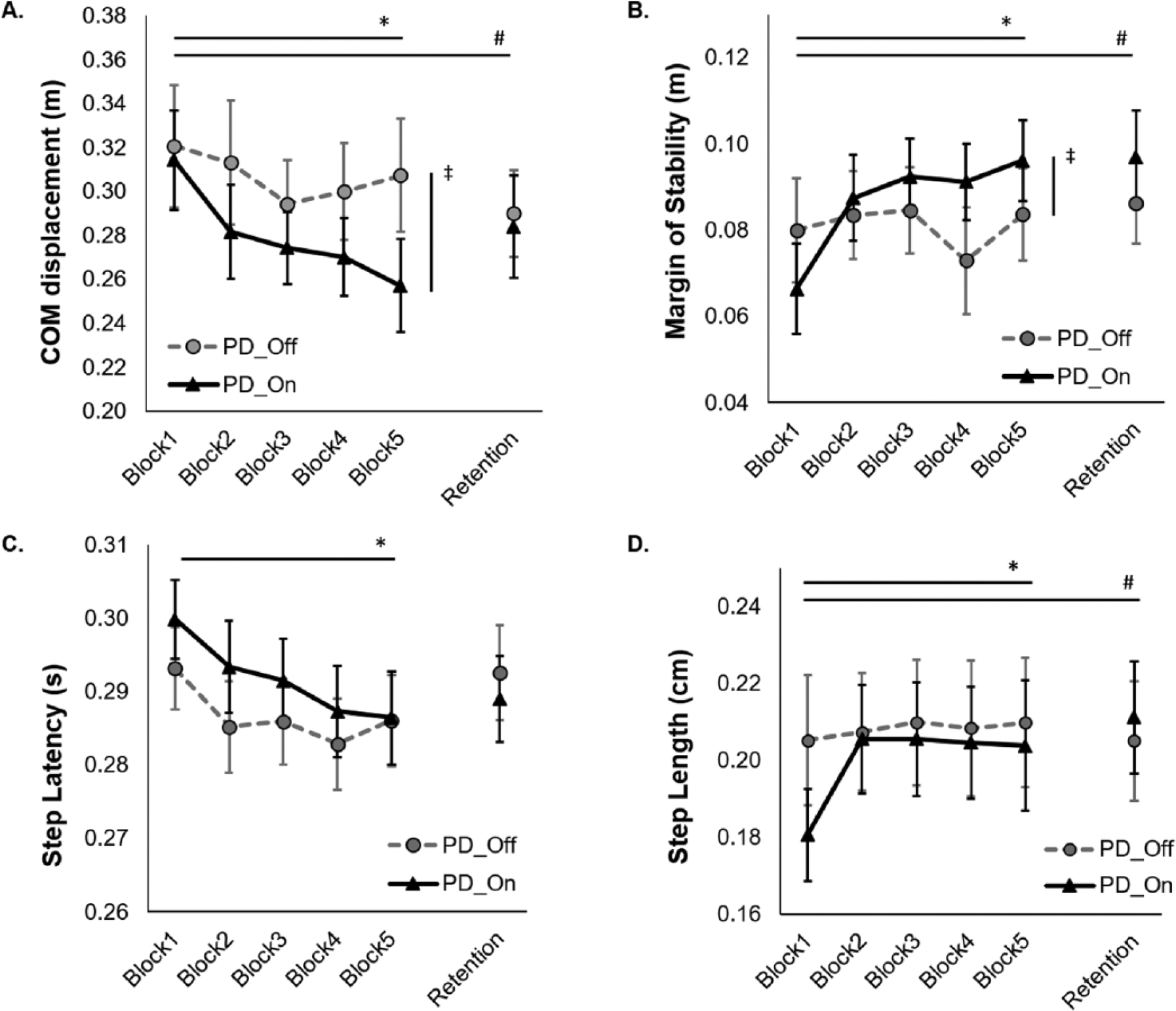
Backward protective stepping performance: (A) Center of mass (COM) displacement, (B) margin of stability, (C) step latency, and (D) step length. Participants demonstrated significant improvement in performance. Improvement was mediated by levodopa state in COM displacement and margin of stability, such that people with Parkinson’s disease (PD) exhibited more learning on levodopa than off levodopa.
Retention of Performance After 24 Hours During Backward Stepping. a
Abbreviations: COM, center of mass; D1, B1, day 1, block 1; D2, B1, day 2, block 1.
Only measures that showed significant improvement over the course of training “learning effects” were included for retention analyses. Bold values indicate significance at the P < .05 level.
Wilcoxon signed-rank test.
Margin of stability
Margin of stability, a measure of the relative location of the XCOM and base of support at first foot contact, was significantly increased (improved) through training. Similar to COM displacement, there was a significant interaction effect as a result of more pronounced increase in on levodopa compared with off. Post hoc analyses confirmed this interaction effect because there was a significant improvement in margin of stability through training on, but not off, levodopa (Table 2, Figure 2). Improvements in margin of stability were retained over 24 hours. An interaction effect was observed such that margin of stability improvements were retained better while on levodopa than off levodopa (P < .001 and P = .36, respectively; Table 3).
Step latency
Step latency was significantly reduced over training. No interaction effect was noted, suggesting similar reduction in on and off medication states (Figure 2, Table 2).
Step length
At baseline, individuals off levodopa took longer steps than when on levodopa at baseline. Step length was significantly increased over training. No interaction effect was observed (Figure 2, Table 2). Improvements in step length were retained for 24 hours. An interaction effect was observed, such that step length improvements were retained better on (P < .001) than off (P = .98) levodopa (Table 3).
Number of steps
No change in number of steps in response to the surface translation was observed across training or across medication state.
Forward Perturbations
During forward perturbations, no variables of interest exhibited significant changes across time or across medication state, and no interaction effects were observed.
Generalization
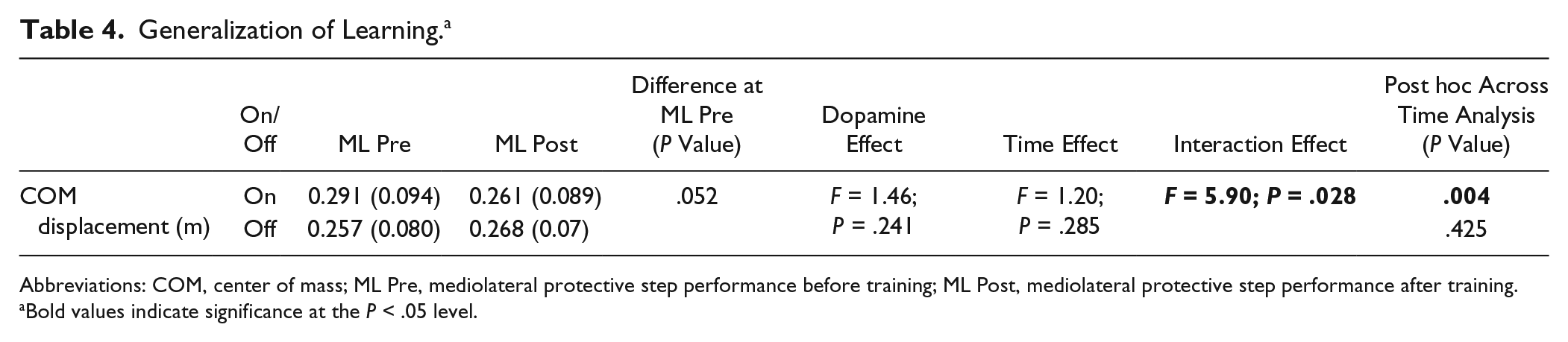
A Time × Levodopa interaction effect was noted, suggesting more pronounced generalization on than off levodopa. Post hoc analyses demonstrated improvements in the untrained ML responses while on levodopa but not while off levodopa (Table 4).
Generalization of Learning. a
Abbreviations: COM, center of mass; ML Pre, mediolateral protective step performance before training; ML Post, mediolateral protective step performance after training.
Bold values indicate significance at the P < .05 level.
Discussion
People with PD improved protective postural responses after 1 day of perturbation training. Furthermore, total COM displacement after perturbation (a measure of global protective response performance) and margin of stability at first foot contact (a measure of first step effectiveness) were improved more while on levodopa than off. Thus, unlike recent upper-extremity motor learning experiments, postural motor learning was not worse on levodopa with respect to off. Improvements in most measures were retained over 24 hours, and for margin of stability, this retention was more pronounced when on levodopa than off. Generalization to an untrained, protective stepping task was more pronounced in people with PD on levodopa than off, but this may have been related to worse initial performance while on levodopa, lessening confidence in this finding. Improvements were more pronounced during backward protective stepping than forward protective stepping, likely as a result of more severe backward disequilibrium in patients with PD. 30
Our results are consistent with work by Roemmich et al, 21 which suggests that some aspects of lower-limb adaptive learning (ie, aftereffects on gait asymmetry after split belt adaptation) may be improved by levodopa. However, our results are not consistent with upper-extremity motor learning studies, which show subtle, but significant, negative effects of levodopa on motor learning.15-18 A close examination of this literature shows that upper-extremity learning is not uniformly affected by levodopa.15,17 These investigations suggest that early acquisition of learning may be negatively affected; however, longer-term learning is not. Furthermore, the most pronounced negative effects of levodopa were observed during explicit learning tasks as opposed to implicit tasks. 15 In the current study, participants were instructed to “react naturally to the perturbation when trying to keep balance.” Although it is difficult to classify improvement in protective stepping as entirely “implicit” or “explicit,” the instructions provided may have resulted in improvement in protective stepping to occur primarily via implicit learning, partially accounting for differing observations between current findings and upper-extremity learning studies.
We observed similar baseline postural responses across levodopa states. The finding of unresponsiveness of protective postural responses to levodopa is consistent with previous reports11,31 and supports the relative unresponsiveness of postural dysfunction in general to levodopa. 32 This lack of improvement of postural control with common interventions further underscores the importance of novel balance interventions, including, perhaps, perturbation training, to improve protective postural responses.2,12
Individuals with PD on levodopa, but not off levodopa, demonstrated a subtle but significant improvement in untrained, lateral postural responses after AP perturbation training. This suggests that people with PD were able to generalize improvements in postural responses while on levodopa. However, while on levodopa, people with PD demonstrated a trend toward higher (worse) baseline COM displacement during ML stepping than while off levodopa. After training, they improved to a similar level as individuals with PD off levodopa. Thus, the statistical finding that people with PD generalized learning more on levodopa than off levodopa may be related to their worse baseline performance. The worse baseline performance in PD in the on state may be related to less rigidity, allowing for more lateral movement. Additional research is necessary to understand whether perturbation training generalizes across protective postural tasks and whether levodopa affects this process.
A strength of this study is the within-subject design, assessing learning on and off levodopa in the same participants. This protocol removes the variability and possible confounds of age, mobility status, and cognitive status when contrasting the effects of dopamine on learning. This protocol does, however, raise the possibility of carryover of learning from one testing session to another. Indeed, previous reports have shown long-term retention of improvements in protective stepping movements. 33 To assess the possibility of carryover, post hoc analyses were carried out to determine whether performance improved across visits (irrespective of dopamine status). The primary variable of interest, COM displacement, showed a nonsignificant (P = .10) improvement at follow-up visit. Interestingly, margin of stability was significantly improved at the follow-up visit with respect to the initial visit (P = .006). These findings suggest that improvements from the first visit may have partially carried over to the second visit. However, we managed this carryover effect by randomizing the order of testing, with 10 participants completing on testing first and 12 completing off testing first. Therefore, this mild to moderate carryover likely had little impact on our primary analysis: the effect of levodopa on postural learning.
Despite the observed improvement in backward responses, forward postural responses were not altered over training. The reason for this lack of improvement is unclear; however, it may be because people with PD exhibit less dysfunction in forward recovery after perturbations with respect to backward perturbations,30,34 predisposing patients to falls in the backward direction. 35 These findings suggest that improvement in backward protective step performance is particularly relevant when attempting to reduce falls in people with PD via perturbation training. 2
Limitations
Several limitations should be noted. First, previous investigations have shown that responses to external perturbations habituate and reduce in amplitude after 3 to 7 perturbation exposures.36,37 Thus, it is possible that the early improvements are not “learning” per se but, rather, are related to habituation to external perturbations. However, all participants were exposed to >10 perturbations prior to the training protocol to reduce habituation effects. Furthermore, although it is possible that improvement seen between blocks 1 and 2 may be related to habituation, it is unlikely that the continued improvement observed across time (particularly COM displacement while on levodopa) is a result of habituation. Second, COM displacement was chosen as the primary outcome because it has been previously used as a global performance outcome after perturbations.23-25 However, it is possible that COM displacement may be increased as a result of unnecessary (and possibly voluntary) steps. Thus, we included several secondary variables focused on the first step, including margin of stability, a measure related to the effectiveness of the first step. 28 Indeed, results of COM displacement and margin of stability were similar, as we observed improvement in performance of both variables. Furthermore, a Training × Medication interaction was noted for both variables, such that people on medication improved performance more than people off levodopa. Third, it is possible that fatigue across training masked improvements in stepping while participants were off levodopa. However, we feel that this is unlikely for 2 reasons. First, we did not observe larger increase in fatigue over the course of training in PD off levodopa compared with on. Second, although the overall level of fatigue was higher in PD off with respect to on, it was low in both medication states. It should, however, be noted that fatigue data were only collected in a subset (16) of the 22 participants included in this study. Fourth, although we made attempts to be consistent with washout periods, participant availability resulted in moderate variability in the time between first and second visits. This likely resulted in additional variability in findings. Fifth, we only measured retention over 24 hours. Additional, longer follow-up is necessary to understand whether improvements are retained over a more functional timescale. In addition, it is possible that longer-term follow-up may identify additional “off-line gains” following consolidation of learning. 38 Finally, comparing assessments on medications (before and after training) with those off medications (before and after training) could potentially introduce bias. However, similarly to previous studies, we observed that postural responses were similar on compared with off medication prior to training. The relative lack of impact of levodopa on postural response performance, therefore, increases our confidence in the current approach.
Conclusions
Protective postural responses to avoid a backward fall, a task critical for fall prevention, may be improved to a larger extent when people are on levodopa than off. Furthermore, people with PD retain improvements in protective stepping over 24 hours, and for some variables, retention was more pronounced while on levodopa. This work suggests that improvements via perturbation training are not negatively affected by levodopa and in fact may be more pronounced while on levodopa than off. Although further research is necessary to assess the effects of perturbation training, our work and that of others2,12 suggest that protective step training is a promising tool to improve protective movements in people with PD. Finally, additional work is also necessary to understand the degree to which postural improvements in the laboratory transfer to real-world fall prevention in people with PD.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Horak and Oregon Health and Science University (OHSU) have an equity/interest in APDM, a company that may have a commercial interest in the results of the study. This potential conflict of interest has been reviewed and managed by the Research and Development Committee at the Portland VA Medical Center and OHSU. No other authors declare any conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the United States Department of Veteran’s Affairs Rehabilitation Research and Development Service (Career Development Award-1 #I01BX007080, PI: DSP) & VA Merit Award (E1075-R, PI: FH), the National Institutes of Health (R01 AG006457 29, PI: FH), and the Medical Research Foundation of Oregon (Early Investigator Award, PI: DSP). The contents do not represent the views of the US Department of Veterans Affairs or the United States Government.