
Abstract
Background. Approximately 60% of patients suffering from acute spinal cord injury (SCI) develop pain within days to weeks after injury, which ultimately persists into chronic stages. To date, the consequences of pain after SCI have been largely examined in terms of interfering with quality of life. Objective. The objective of this study was to examine the effects of pain and pain management on neurological recovery after SCI. Methods. We analyzed clinical data in a prospective multicenter observational cohort study in patients with SCI. Using mixed effects regression techniques, total motor and sensory scores were modelled at 1, 3, 6, and 12 months postinjury. Results. A total of 225 individuals were included in the study (mean age: 45.8 ± 18 years, 80% male). At 1 month postinjury, 28% of individuals with SCI reported at- or below-level neuropathic pain. While pain classification showed no effect on neurological outcomes, individuals administered anticonvulsant medications at 1 month postinjury showed significant reductions in pain intensity (2 points over 1 year; P < .05) and greater recovery in total motor scores (7.3 points over 1 year; P < .05). This drug effect on motor recovery remained significant after adjustment for injury level and injury severity, pain classification, and pain intensity. Conclusion. While initial pain classification and intensity did not reveal an effect on motor recovery following acute SCI, anticonvulsants conferred a significant beneficial effect on motor outcomes. Early intervention with anticonvulsants may have effects beyond pain management and warrant further studies to evaluate the therapeutic effectiveness in human SCI.
Introduction
Approximately 60% of patients suffering from acute spinal cord injury (SCI) develop pain within days to weeks after injury, which ultimately persists into chronic stages.1-3 To date, the consequences of pain after SCI have been largely examined in terms of interfering with quality of life. 4 However, preclinical studies indicate that pain and management of pain with different classes of medications may also impact neurological outcomes. More specifically, the neuromodulatory properties of pain and almost every class of pain medication have been demonstrated in animal models of CNS injury, including SCI.5-8
The primary aim of this study was to examine the hypothesis that pain characteristics (classification and intensity), as well as pain management (medications), affect the course of neurological recovery after human SCI. This is an important line of investigation given that both pain and neurological function strongly influence quality of life among individuals with SCI.9,10 The effects of 2 different drug classes were specifically examined: medications typically administered to manage neuropathic pain (ie, anticonvulsants), and medications more generally administered for the management of nociceptive pain (ie, nonsteroidal anti-inflammatory drugs [NSAIDs]). To address our hypothesis, neurological outcomes (sensory and motor scores from the International Standards for the Neurological Classification of SCI, ISNCSCI) and pain data from the European Multi-centre Study about SCI (EMSCI) were examined.
Methods
Data Source and Study Design: European Multi-centre Study about Spinal Cord Injury
This was a longitudinal prospective (observational) cohort study of individuals in the EMSCI. Comprised of 19 participating trauma and rehabilitation centers from across Europe, neurological and functional outcomes are comprehensively tracked in individuals with SCI at fixed time points over the first year of injury. All individuals in the EMSCI receive standards of rehabilitation care. To be included in EMSCI, individuals must have met the following criteria: the patient was capable and willing to give written informed consent, the first EMSCI assessment was possible within the first 6 weeks following injury, and the injury was a single event (traumatic or ischemic paraplegia or tetraplegia). Exclusion criteria were: other nontraumatic paraplegia or tetraplegia, dementia or severe reduction of intelligence leading to reduced capabilities of cooperation or giving consent, polyneuropathy, and relevant brain injury. Although EMSCI was designed to facilitate data collection for clinical trials, the current study does not represent the results of an experimental/clinical trial, or the secondary analysis of clinical trial data (ie, subjects are not randomized to therapies). All patients gave their written informed consent before being included in the database. This study was approved by all responsible institutional review boards.
Pain Questionnaire
Initiated in 2007, seven member centers of the EMSCI participated in the collection of pain questionnaire data. Briefly, the structured interview comprised a comprehensive assessment of pain features. Pain was classified as nociceptive or neuropathic by trained examiners based on patient description (eg, burning, stabbing, electric, or shooting), location of pain relative to neurological level of injury, aggravating and alleviating factors (eg, musculoskeletal pain associated with movement), as well as key patient signs (eg, alloydnia and hyperalgesia associated with neuropathic pain). Neuropathic pain comprised at- and below-level symptoms. 11 According to the International SCI Pain Classification, symptoms located diffusely 3 levels or more caudal to the neurological level of the SCI were defined as “below-level” neuropathic pain. The questionnaire was repeated for up to 3 different types of pain. For the purpose of analysis, subjects were examined according to their predominant (most intense) pain. Major pain medications, including the use of antidepressants, anticonvulsants (gabapentin, pregabalin, carbamazepine, valproic acid, and lamotrigine), NSAIDS, and opioids, were also recorded. Pain intensity was determined for the average and maximum over a 1-week period using a Numeric Rating Scale.
Outcome and Exposure Assessments
Individuals were examined at 4 fixed time points: 1, 3, 6, and 12 months postinjury. Total sensory and motor scores (maximum value = 112 and 100, respectively) were the primary outcome variables, assessed separately at each of the 4 time points, and examined according to the established ISNCSCI. Trained examiners performed the ISNCSCI and classifications were verified by computational analysis. 12 Upper extremity motor score (UEMS) and lower extremity motor score (LEMS), both of which combine to form the total motor score (each with a maximum value of 50), were also examined in a post hoc analysis (see unbiased recursive partitioning below). Three pain-related variables collected at 1 month were used as primary explanatory variables: (1) pain classification (none, neuropathic, or nociceptive), (2) pain intensity (average or maximum over the past week; scale from 0 = no pain to 10 = most pain imaginable), and (3) pain drug classification, (NSAID) and anticonvulsant use. Also from the motor and sensory scores, the American Spinal Injury Association (ASIA) Impairment Scale (AIS) was determined as a measure of injury severity. A secondary analysis was performed on pain intensity (ie, where intensity was the outcome), modeling the effects of 1-month anticonvulsant use on pain intensity (ie, drug efficacy).
Statistics
For demographics and baseline characteristics, study groups were compared using t tests for continuous variables, and chi-square tests for categorical variables (or their nonparametric alternatives). To take into account the longitudinal nature of the data, to adjust for potential confounders, as well as to handle missing data, the primary analysis comprised the use of mixed effects regression models. To build the statistical models, the individual trajectories over the 4 time points were visually examined using “spaghetti” plots. Akaike information criterion and the likelihood ratio test were used to statistically compare nonnested models and nested models, respectively. As our primary interest was the rate of recovery, we examined if covariates affected the trajectory of sensory and motor recovery using formal testing of interaction terms (ie, covariate-time interactions). P < .05 was regarded as statistical significance. Bonferonni corrections were made for adjustment for multiple comparisons. R statistical software version 2.15.3 was used for all analyses.
Unbiased Recursive Partitioning
In addition to using mixed effects models to examine changes over time in the recovery of motor function, we were also interested in addressing if pain factors (ie, classification and medications) had specific effects within different cohorts. To this end, we employed “unbiased recursive partitioning” (URP)—a technique using conditional inference trees. URP is a tree-structured regression model based on sequential tests of independence between predictors and a specified clinical endpoint (ie, future outcome). More detailed information can be found elsewhere. 13 In brief, URP divides an initial heterogeneous population into successively disjoint and more homogeneous pairs of subgroups with regard to the clinical endpoint of interest, and thus creates an algorithm for predicting future outcomes within more homogeneous subgroups.
Results
Study Cohort Description
Table 1 shows basic demographics and other characteristics of the study sample (n = 225; 80% male; 96% traumatic injury etiology) at all time points after injury. One-month baseline subject and injury characteristics based on medication classification are shown in Table 2.
Cohort Description. a
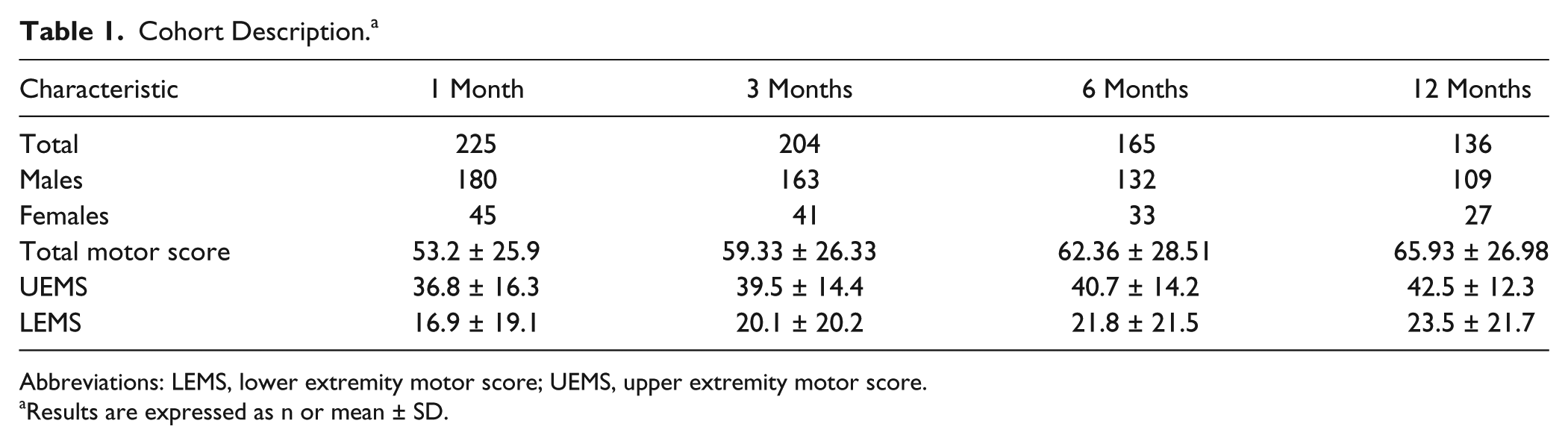
Abbreviations: LEMS, lower extremity motor score; UEMS, upper extremity motor score.
Results are expressed as n or mean ± SD.
Cohort Description by Drug Status at First Time Point. a
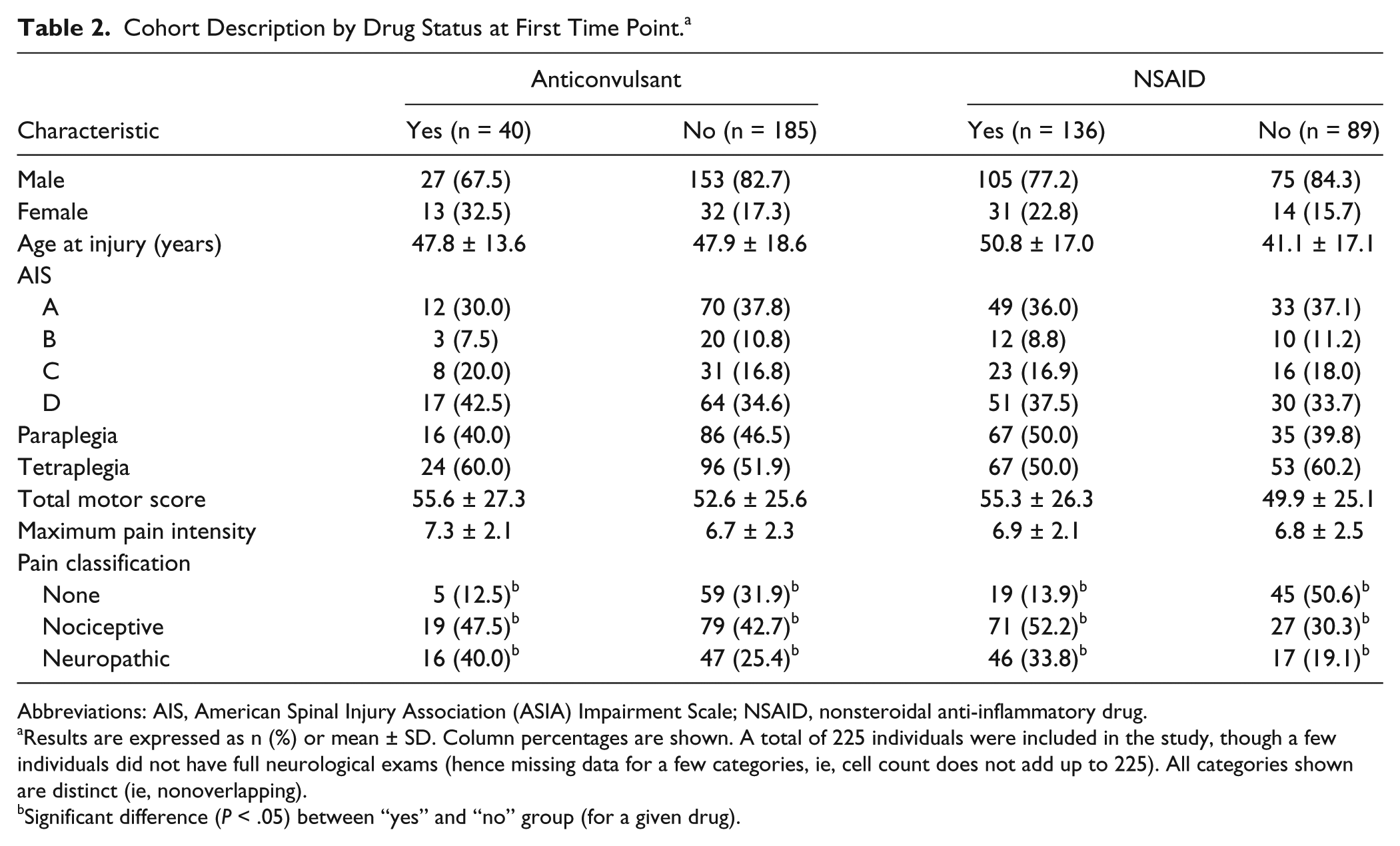
Abbreviations: AIS, American Spinal Injury Association (ASIA) Impairment Scale; NSAID, nonsteroidal anti-inflammatory drug.
Results are expressed as n (%) or mean ± SD. Column percentages are shown. A total of 225 individuals were included in the study, though a few individuals did not have full neurological exams (hence missing data for a few categories, ie, cell count does not add up to 225). All categories shown are distinct (ie, nonoverlapping).
Significant difference (P < .05) between “yes” and “no” group (for a given drug).
Effect of Pain on Motor Recovery
Supplementary Tables 1 and 2 show the output from the mixed effects analysis: unadjusted and AIS-adjusted models. In each of these models (and subsequent tables), we were interested in comparing the rates of recovery between each group (ie, the interaction term indicated in the table). We found that regardless of how pain classification was modelled, there was no significant effect of pain on the rate of motor recovery (Supplementary Tables 1 and 2; P > .05 for interaction terms).
Effect of Pain Medication on Sensory and Motor Recovery
Supplementary Table 3 shows the relationship between anticonvulsant use at 1 month and total motor score recovery. In the unadjusted model (model 1), the use of anticonvulsants at 1-month postinjury significantly affected neurological recovery (drug × time interaction: P = .031). According to this mixed-effects model, individuals who were treated at this early time point with anticonvulsant drugs recovered an average of 7.3 motor points greater over the first year (ie, 0.02 points per day) compared with those untreated with anticonvulsants (Figure 1A and C, Supplementary Table 3). In the models, the main effect for drug was not significant; however, the significant interaction term indicates a faster rate of motor recovery in those administered anticonvulsants at 1 month. Importantly, the effect of anticonvulsants persisted after adjusting for initial AIS grade (P = .039 for 7.3 motor points over 1 year; model 2 in Supplementary Table 3). Moreover, when examined separately, LEMS recovered significantly more than UEMS in the anticonvulsant group (P < .05).
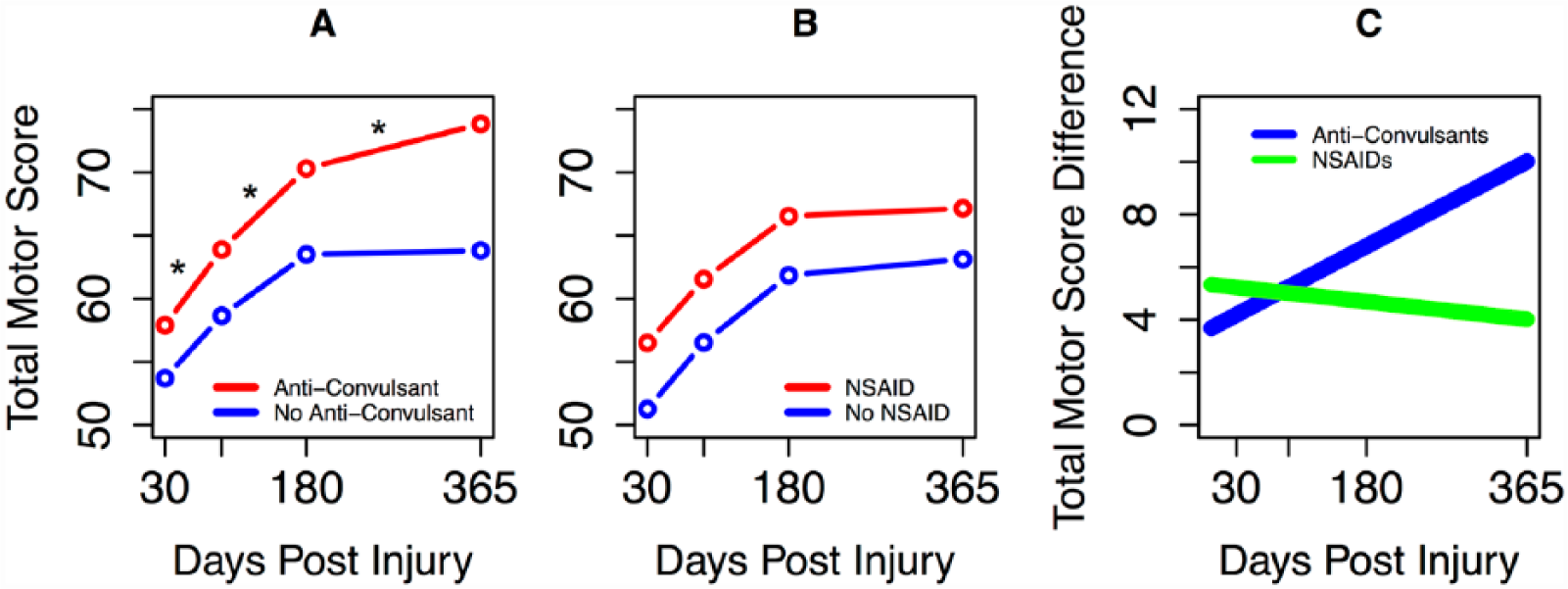
Effect of pain medications on motor recovery following spinal cord injury. (A) Effect of anticonvulsants on motor recovery following spinal cord injury. Fitted curves derived from mixed-effects models: red, anticonvulsant users; blue, nonanticonvulsant users. *P = .031 for interaction effect. (B) Effect of nonsteroidal anti-inflammatory drug (NSAID) use on motor recovery following spinal cord injury. Fitted curves derived from mixed-effects models: red, NSAID users; blue, non-NSAID users. (C) Difference between motor scores (fitted values) at each time point between anticonvulsant users and nonusers (blue) and between NSAID users and nonusers (green).
We also examined whether the effect of anticonvulsants on motor recovery was confounded by initial pain intensity (ie, 1 week maximum or 1 week average), initial pain classification (ie, neuropathic vs nonneuropathic), injury etiology (ie, traumatic vs nontraumatic), other pain-related medications administered at the first time point (ie, opioids [n = 63 at 1 month] and antidepressants [n = 46 at 1 month]), as well as injury level (ie, quadriplegia vs paraplegia). After adjusting the model for each of these factors, the effect of anticonvulsants on motor recovery remained (ie, approximately 7-point improvement over 1 year, P < .05 for interaction term).
By contrast, NSAID use at 1-month postinjury had no significant effect on motor recovery (drug × time interaction: P = .586 and P = .593, unadjusted and adjusted for AIS-grade, respectively; Figure 1B and C and Supplementary Table 4). Neither NSAIDS nor anticonvulsants conferred any effects on sensory recovery.
Effect of Anticonvulsants on Pain Intensity
In addition to influencing neurological recovery, the use of anticonvulsants significantly reduced maximum pain intensity in individuals initially classified with nociceptive or neuropathic pain (P = .04 for time × drug interaction; Figure 2; Table 3). The effect of anticonvulsants on maximum pain intensity persisted after adjusting for initial pain classification (nociceptive vs neuropathic, P = .03 for interaction term).
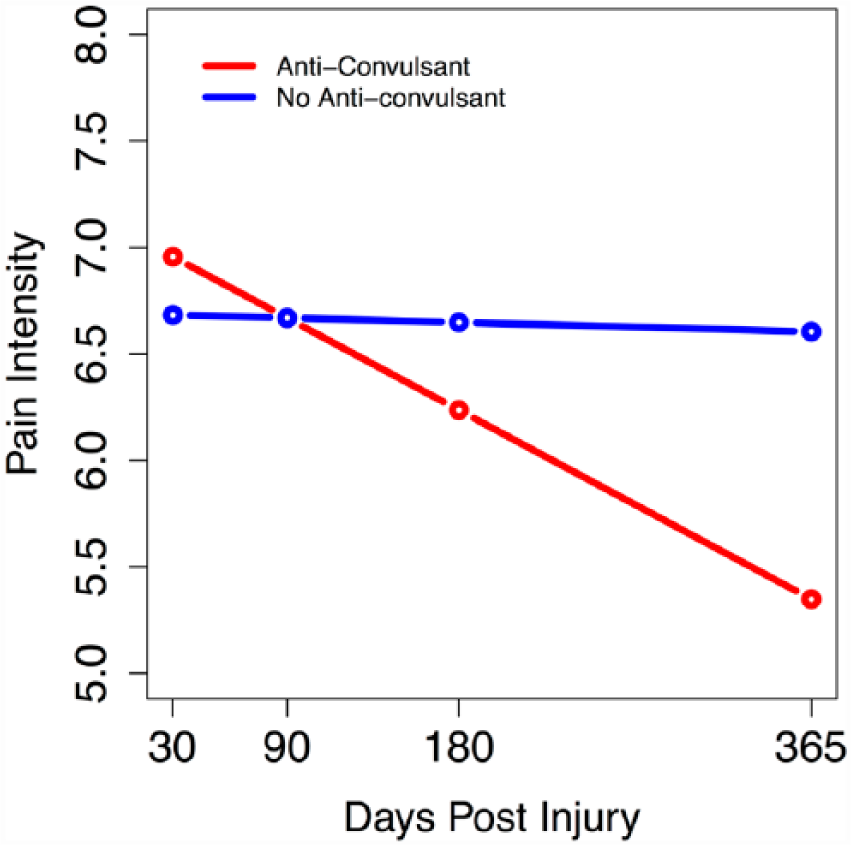
Effect of anticonvulsant use on pain intensity following spinal cord injury. Fitted curves derived from linear mixed-effects models: red, anticonvulsant users; blue, no anticonvulsant.
Pain Intensity: Maximum Pain Intensity at Each Time Point (0-10 Scale). a

Results are expressed as mean ± SD.
Predicting Motor Recovery
Unbiased recursive partitioning focused on changes in motor scores between 1 and 6 months. Initial motor scores at 1 month and whether they were administered anticonvulsants and NSAIDs were included as explanatory variables. Only those explanatory variables that are significant predictors of outcome (ie, motor recovery between 1 and 6 months) are present in the trees; furthermore, the cutoffs indicated in the tree are automatically determined by the algorithm to yield the highest heterogeneity between groups. Figure 3 shows that anticonvulsants are indeed significant predictors of changes in UEMS, notably among those with a baseline UEMS of <40. Also, in the lower extremities, there was a significant effect of anticonvulsants on changes in LEMS, but this did not depend on initial LEMS (results not shown). NSAIDs, by contrast, were not significant predictors of changes in upper or lower extremities.
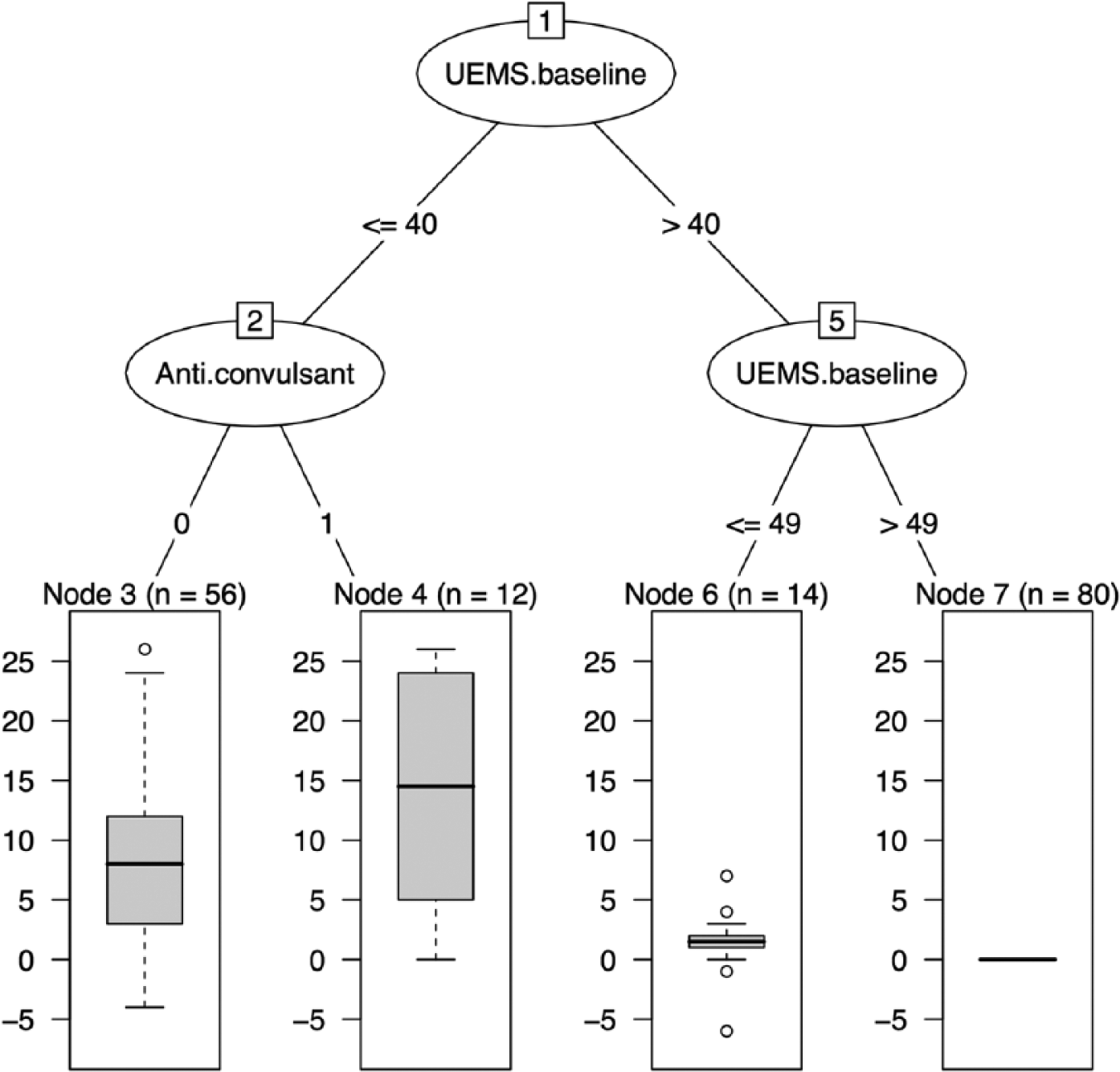
Result tree of unbiased recursive partitioning. Outcome: change in upper extremity motor score (UEMS) from 1 to 6 months post injury. Each node (homogenous group) contains a box plot (dark horizontal line is the median value) for UEMS in each group. The cutoffs indicated in the tree branches (eg. baseline UEMS >40) are automatically determined by the algorithm to yield the highest heterogeneity between groups. The analysis was run on all study subjects.
Discussion
Recovery of Motor Outcomes After Spinal Cord Injury
The transition to chronic injury is characterized by an inherent but limited capacity for neurological recovery. A central goal of rehabilitation is to capitalize on this recovery, translating neurological changes into functional improvements. Documented in several large-scale observational studies, significant recovery of muscle strength in upper and lower limbs is expected during the transition from acute to chronic injury.14-16 According to international standards, residual sensory and motor sparing below the neurological level of SCI, reflecting the initial severity or “completeness” of damage in the spinal cord, is the single most important predictor of the magnitude of recovery. 14 However, a high degree of variability remains even after considering these injury characteristics. Seemingly identical injuries recover across a broad range, suggesting that other factors are needed to explain this variability.
The present findings are the first to demonstrate that acute management of neuropathic pain may have beneficial effects over the first year postinjury. Specifically, individuals treated with anticonvulsants demonstrated greater recovery of muscle function compared with individuals not treated with anticonvulsants. Importantly, the effect of anticonvulsants was observed independently of injury related characteristics, such as the injury severity and level of injury, and other pain medications. Moreover, findings from the mixed effects modelling were supported by URP, which revealed that anticonvulsants had a beneficial effect in both the upper and lower extremities. In addition to motor recovery, anticonvulsants significantly reduced maximum pain intensity during the transition from acute to chronic stages.
Motor Recovery and Clinical Trials in Spinal Cord Injury
To measure efficacy, changes in muscle strength greater than achieved due to spontaneous recovery have been examined in past clinical trials aimed at neuroprotection17-19 and neuroregeneration.20-22 Employing motor scores, recent studies have reported preliminary efficacy for minocycline23,24 and riluzole25,26—2 drugs that have been repurposed as potential neuroprotective agents in SCI. Based on our findings, we have identified a significant effect (approximately 7 motor points) of acute anticonvulsant treatment on motor scores after SCI. To put this recovery into context, 7 motor points is comparable to that reported in a landmark clinical trial examining the effects of acutely administered methylprednisolone (NASCIS Trial), 27 and a recent observational study demonstrating the efficacy of early surgical intervention. 28
While statistically significant, an important question to address is whether 7-point motor recovery represents a clinically meaningful change. Several factors potentially impact clinical significance, including where in relation to the neurological level of injury motor recovery occurs. 29 For example, motor recovery in cervical spinal segments adjacent to the level of injury may have a substantial impact on functional outcomes, caudally shifting motor level and improving function related to self-care. 30 In contrast, the recovery of muscle strength across a larger number of spinal segments without reaching a functional threshold (ie, motor score ≥3 or muscle strength against gravity) may be less clinically meaningful. From a pragmatic perspective, other important factors to consider include the invasiveness of the intervention, associated side effects, and financial costs.
Anticonvulsants and Spinal Cord Injury: Mechanisms of Action
In terms of mechanisms, greater neurological recovery in individuals administered anticonvulsants could be a result of improved pain outcomes, that is, reductions in pain during transition from acute to chronic SCI. Along similar lines, anticonvulsants have also demonstrated effectiveness to reduce spasticity.31,32 In turn, reductions in pain and spasticity may indirectly improve motor outcomes through, among several potential mechanisms, increased participation in rehabilitation. However, our findings do not support this hypothesis (at least with respect to initial pain classification).
Other potential mechanisms may relate to neuroprotection and neuroplasticity. The “therapeutic window” for neuroprotection purportedly ranges from hours to days after injury. 33 Depending on the anticonvulsant medication administered, neuroprotection could be mediated through blockade of calcium and/or sodium channels, which in turn reduces the deleterious consequences of several well-known secondary injury mechanisms such as free radical generation, glutamate release, and lipid peroxidation. 34 Although preclinical SCI studies have demonstrated the neuroprotective effects of anticonvulsants,6,7 administration may be required in a very narrow time window (ie, minutes to hours). Whereas medications for nociceptive pain (eg, NSAIDs and opioids) would expectedly be administered in this time frame (eg, as part of the perisurgical pain management), the neuroprotective window may be closed when neuropathic pain develops and anticonvulsant use is initiated.
An interesting alternative to consider is that anticonvulsants may affect endogenous neuroplasticity, such as sprouting. Proposed to mediate spontaneous repair in preclinical models of SCI, 35 sprouting is considered a major therapeutic target for the recovery of neurological function. In line with known mechanisms, anticonvulsants may attenuate aberrant plasticity through a reduction in hyperexcitability. 36 While mechanisms are poorly understood, aberrant neuroplasticity and hyperexcitability in the cord have been suggested as potential underlying substrates of neuropathic pain. 37 Similarly, through the attenuation of aberrant plasticity and hyperexcitability, anticonvulsants administered early after SCI in individuals with neuropathic pain may “redirect” or unmask potential for neurological recovery.
While NSAIDs have also been attributed neuroprotective properties in animal models of SCI,8,33,38 we could not discern beneficial effects in terms of neurological recovery in this study. Several factors may explain the lack of a statistical effect, including that dosing for pain relief may have been suboptimal to achieve anti-inflammatory properties (ie, mechanism of neuroprotection). 39
Limitations and Future Directions
To investigate if anticonvulsants are a viable candidate to enhance neurological and functional outcomes, further studies are obviously warranted. In particular, information regarding different types of anticonvulsants (eg, gabapentin, pregabalin, carbamazepine, and valproic acid), as well as dosing and timing of administration are essential. A study proposing to acutely administer anticonvulsants would also need to consider potential side effects, such as fatigue, 40 and their impact on neurological outcomes. Side effects may be particularly problematic in individuals who do not have pain, and thus are not “benefiting” from reduced pain intensity associated with the use of anticonvulsants prescribed for other reasons. In terms of designing clinical trials, there are several advantages to repurposing anticonvulsants to promote neurological recovery, including that the safety profile in SCI is already well established. 41
Future studies involving a greater number of subjects should further consider the impact of different types of neuropathic pain (ie, at and below level) on neurological recovery. It is particularly intriguing to consider that below level neuropathic pain may confer a benefit among individuals with sensorimotor complete SCI, as a potential surrogate of afferent sparing. 42 Outside the scope of this analysis, we did not examine the relationship between changes in pain factors and injury characteristics with the recovery of motor function. This requires that time-varying covariates be included in longitudinal models (ie, changes in pain occurring in conjunction with motor recovery), which adds considerable complexity to the interpretation of results.
Patient dropout, inherent in all longitudinal cohort studies, may present a problem. In an observational cohort study, at 6 and 12 months after SCI, typically around the time patients are discharged from rehabilitation centers, this may be of particular concern. Another notable limitation of this observational study is that subjects were not randomized to different medications, and other factors related to the individual or their acute management, not captured in the EMSCI, may explain better the impact of anticonvulsants on neurological outcomes (ie, confounders, such as surgical intervention).28,43,44 Related to the use of motor scores, the current study may also have limited sensitivity to detect changes in neurological function. Future studies may benefit from the addition of different outcome measures, including kinematics, electrophysiology, and neuroimaging.
Conclusion
In addition to the management of neuropathic pain, the present study reveals for the first time that the administration of anticonvulsants has the potential to improve motor recovery after acute SCI. While additional studies are needed, these seminal findings highlight that acute standards of care (ie, treatment with pain medications) can impact neurological outcomes.
Footnotes
Acknowledgements
The authors would like to thank all sites participating in the EMSCI.
Authors’ Note
Authors Armin Curt and John K. Kramer have shared last authorship. Armin Curt is also an author on behalf of the European Multi-centre Study on Spinal Cord injury (EMSCI) Study Group.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JJC is an ALS Canada Tim E. Noël Postdoctoral Fellow and is supported by the Michael Smith Foundation for Health Research. JKK is a Michael Smith Foundation for Health Research and Rick Hansen Institute Scholar and is also supported by the North American Spine Society. JH is a Craig H. Neilsen Scholar. The project was supported by the Clinical Research Priority Program in Neurorehabilitation of the University of Zurich, Switzerland.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.