
Abstract
Background and Objectives. The onset of pervasive sleep-wake disturbances associated with traumatic brain injury (TBI) is poorly understood. This study aimed to (a) determine the feasibility of using polysomnography in patients in the acute, hospitalized stage of severe TBI and (b) explore sleep quality and sleep architecture during this stage of recovery, compared to patients with other traumatic injuries. Methods. A cross-sectional case-control design was used. We examined the sleep of 7 patients with severe TBI (17-47 years; 20.3 ± 15.0 days postinjury) and 6 patients with orthopedic and/or spinal cord injuries (OSCI; 19-58 years; 16.9 ± 4.9 days postinjury). One night of ambulatory polysomnography was performed at bedside. Results. Compared to OSCI patients, TBI patients showed a significantly longer duration of nocturnal sleep and earlier nighttime sleep onset. Sleep efficiency was low and comparable in both groups. All sleep stages were observed in both groups with normal proportions according to age. Conclusion. Patients in the acute stage of severe TBI exhibit increased sleep duration and earlier sleep onset, suggesting that the injured brain enhances sleep need and/or decreases the ability to maintain wakefulness. As poor sleep efficiency could compromise brain recovery, further studies should investigate whether strategies known to optimize sleep in healthy individuals are efficacious in acute TBI. While there are several inherent challenges, polysomnography is a useful means of examining sleep in the early stage of recovery in patients with severe TBI.
Introduction
Sleep-wake disturbances are common across the continuum of recovery following traumatic brain injury (TBI)1-3; however, their onset is still poorly understood. Using actigraphy in an acute care setting, we have shown that these disturbances emerge in the early stage after moderate-severe TBI, evidenced by nonconsolidated daytime activity and nighttime rest. 4 Rest fragmentation and prolonged rest duration were also identified using actigraphy among mild to severe TBI patients within 24 hours of being admitted to a neurosurgical ward. 5
In addition to the effects of the hospital environment on sleep, and considering the major structural, biochemical, and pathophysiological changes that occur during the acute phase of severe TBI, including diffuse axonal injury, focal lesions, elevated intracranial pressure, hypoxemia, reduced metabolism, apoptosis, and inflammation, 6 we predict that significant modifications to sleep stages and architecture may occur. In accordance with this hypothesis, recent rodent models of TBI have reported an increase in the amount of sleep, reduction in wakefulness, and more transitions between sleep and wakefulness in the first hours postinjury.7-10 However, no alterations in the amount of rapid eye movement (REM) or non-REM (NREM) sleep were observed, suggesting that acute TBI decreases the ability to maintain prolonged wakefulness rather than altering the proportion of each sleep stage.
While several studies have investigated sleep using polysomnography (PSG) in the chronic stages of TBI, to our knowledge, no prior study has utilized PSG with electroencephalography (EEG), electrooculography (EOG), and chin electromyography (EMG) to examine sleep stages and architecture during the acute stage of severe TBI in nonsedated patients. This may be due to the challenges of performing PSG recordings in this population, when most patients are confused and agitated. However, contrary to other methods used to assess sleep in hospital settings, namely, actigraphy and nurse assessment, PSG leads to more accurate measurements of sleep quality and is the only method to identify sleep stages.11,12 Thus, PSG recording in acute TBI would allow for an improved understanding of the emergence of sleep-wake disturbances.
In the present study, we conducted bedside PSG in 7 nonsedated patients hospitalized with acute (<45 days postinjury), severe TBI and 6 patients with severe orthopedic or spinal cord injuries (OSCI) without TBI to compare the sleep of patients hospitalized with similar medical condition severity, within a similar environment. We utilized EEG, EOG, and chin EMG to objectively measure sleep stages and architecture at bedside.
The aim of this research was to determine the feasibility of using PSG recordings with this acute patient population and to explore sleep quality and sleep macroarchitecture via PSG, in the acute, hospitalized stage of severe TBI. We also aimed to explore associations between injury characteristics and PSG variables. Based on animal studies and our previous actigraphy study, 4 we hypothesized that in comparison to those with OSCI, severe TBI patients would have an increased amount of sleep, reductions in wakefulness, and greater fragmentation of their sleep during the night.
Methods
Participants
A cross-sectional case-control design was used. The present study was performed in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement for case-control studies. 13 Potential TBI participants and their families were approached in the intensive care unit (ICU) of the Hôpital du Sacré-Cœur de Montreal, a tertiary trauma center, from June 2009 to January 2014. Seven patients with severe TBI (range = 17-47 years; 4 males) were recruited (see Figure 1 for flow diagram) and compared to 6 patients with severe OSCI (range = 19-58 years; 3 males). Five TBI patients in the present study were included in a previous study reporting actigraphy data only. 4 TBI was defined as an alteration in brain function, or other evidence of brain pathology, caused by an external force. 14 TBI severity was assessed on emergency room admission using the Glasgow Coma Scale (GCS) 15 and reassessed 30 minutes later to provide a post-reanimation score. Patients in the TBI group were included if they had a GCS score of 3 to 8 on both assessments. See Table 1 for demographic and injury characteristics.
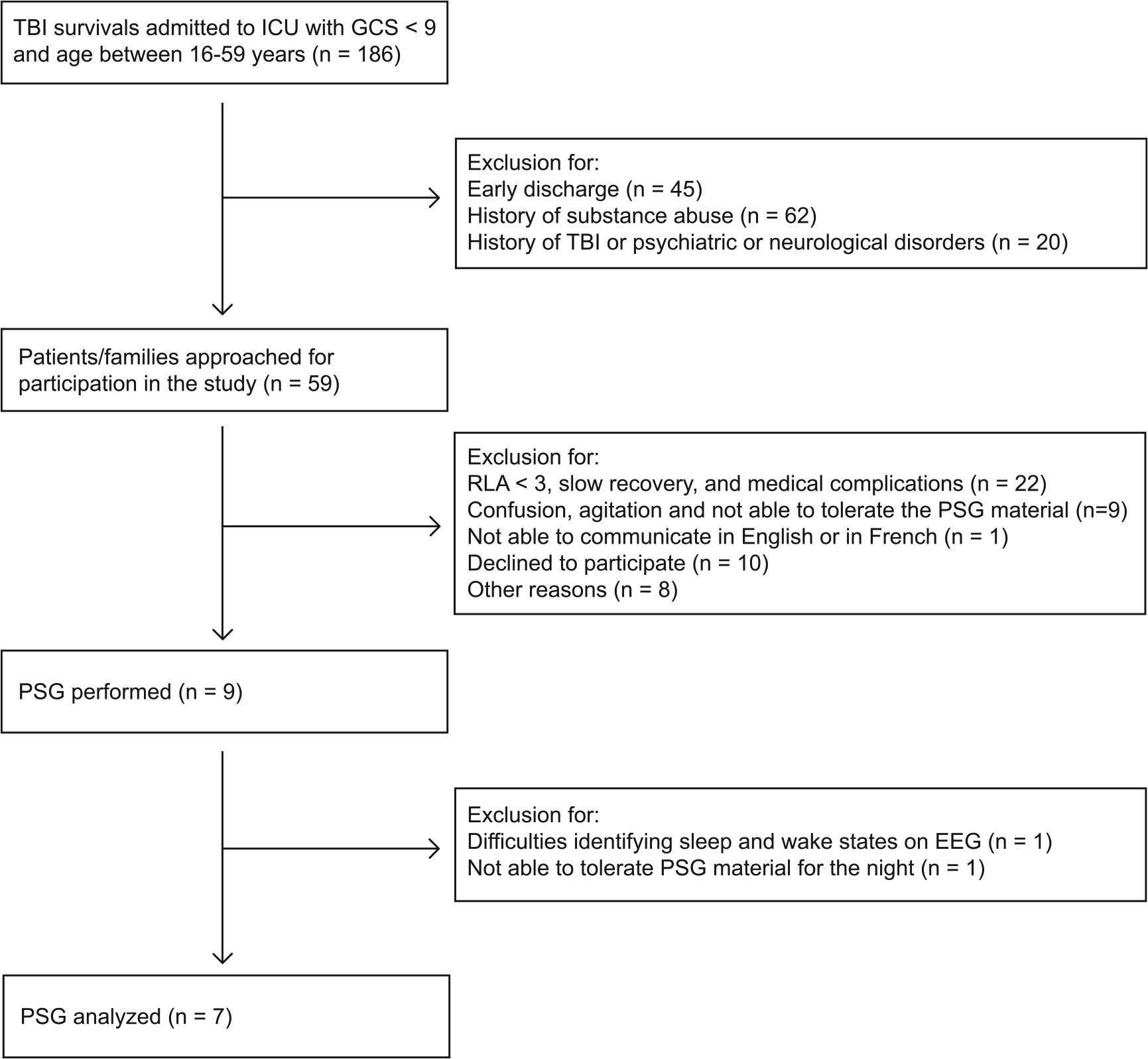
Flow diagram representing TBI patient recruitment.
Demographic and Clinical Characteristics for Patients With Moderate-Severe Traumatic Brain Injury (TBI Group) and Patients With Orthopedic or Spinal Cord Injuries (OSCI Group).
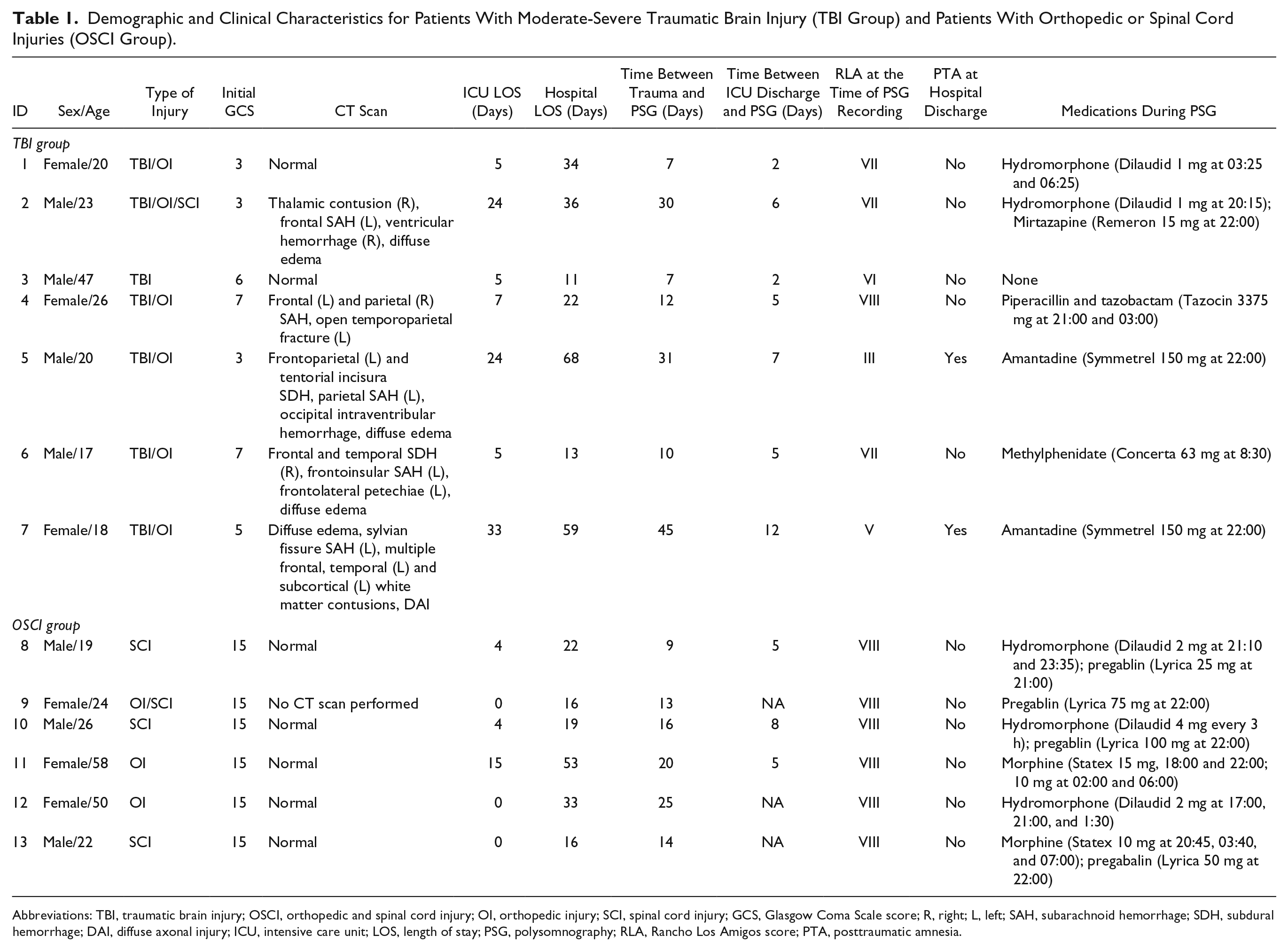
Abbreviations: TBI, traumatic brain injury; OSCI, orthopedic and spinal cord injury; OI, orthopedic injury; SCI, spinal cord injury; GCS, Glasgow Coma Scale score; R, right; L, left; SAH, subarachnoid hemorrhage; SDH, subdural hemorrhage; DAI, diffuse axonal injury; ICU, intensive care unit; LOS, length of stay; PSG, polysomnography; RLA, Rancho Los Amigos score; PTA, posttraumatic amnesia.
Inclusion Criteria
Age 16 to 59 years; extubated, normal intracranial pressure and no active or suspected infection at time of data collection; continuous intravenous sedation and analgesia discontinued for a minimum of 48 hours; remaining in the tertiary trauma center long enough to complete the study.
Exclusion Criteria (Both Groups)
Preinjury history of diagnosed psychiatric or neurologic disorders (including previous TBI), sleep disorders, substance abuse, or disease known to affect sleep and/or circadian rhythms; pregnancy; severe eye injuries that would modify perceived light; inability to tolerate research materials; temporary skull bone flap removal. Because of a periocular laceration, one OSCI patient was initially suspected of having a mild TBI; however, he did not reach the criteria for a diagnosis of mild TBI, as he had a normal brain computed tomography (CT) scan, no confusion or disorientation was observed, and he had an initial GCS score of 15 and was, therefore, not excluded.
The study received ethics approval from the hospital ethics committee. Consent to participate was provided by the patients’ family member in all TBI cases. Patients who eventually became cognitively able to provide informed consent for themselves during data collection were asked to sign a consent form for study protocol to continue. OSCI participants were able to provide their own consent.
Study Protocol and Data Analyses
Clinical Variables
We documented GCS, brain CT scan results, length of ICU stay, hospital length of stay, and Marshall score. 16 CT scans were interpreted by a neuroradiologist (DG). Cumulative administered dose of sedative and analgesic medication (lorazepam, midazolam, propofol, morphine, and fentanyl) in ICU was calculated according to the previously described method. 17 As per standard clinical protocol, daily assessments of cognitive function were performed by occupational therapists using the Rancho Los Amigos (RLA) scale. 18 Posttraumatic amnesia (PTA) at discharge was evaluated with the Galveston Orientation and Amnesia Test (GOAT). 19
Polysomnography
PSGs were recorded for at least 16 continuous hours, starting between 13:14 and 18:46, using a 32-channel Siesta system (Compumedics Limited, Charlotte, NC). PSGs for both groups were performed in regular neurologic or orthopedic units following discharge from ICU. Electrode installation was done at bedside by 2 experienced and registered medical electrophysiology technologists. PSG comprised at least 3 EEG leads (C3, C4, O2) with a mastoid (M1) reference, left and right EOG, and chin EMG. Participants were able to move around when able, since the PSG recording system was ambulatory. A trained research assistant stayed next to the patient room throughout the recording to observe the online PSG, and a registered medical electrophysiology technologist was on call and available in the hospital during the PSG to replace electrodes if needed.
Since no restrictions were placed on when patients were permitted to sleep, the sleep period was thus defined as the longest period of sleep during the night. Visual inspection of PSG data revealed that all participants began their first period of continuous nocturnal sleep (>10 minutes) between 20:11 and 00:19, and the end of their sleep period occurred between 06:22 and 08:47 (see Table 2). Any period of sleep that occurred following an awakening longer than 15 minutes, and later than 06:30, was considered a nap and thus not included within the nighttime sleep period.
Polysomnographic Results for Patients With Severe TBI and Patients With OSCI.
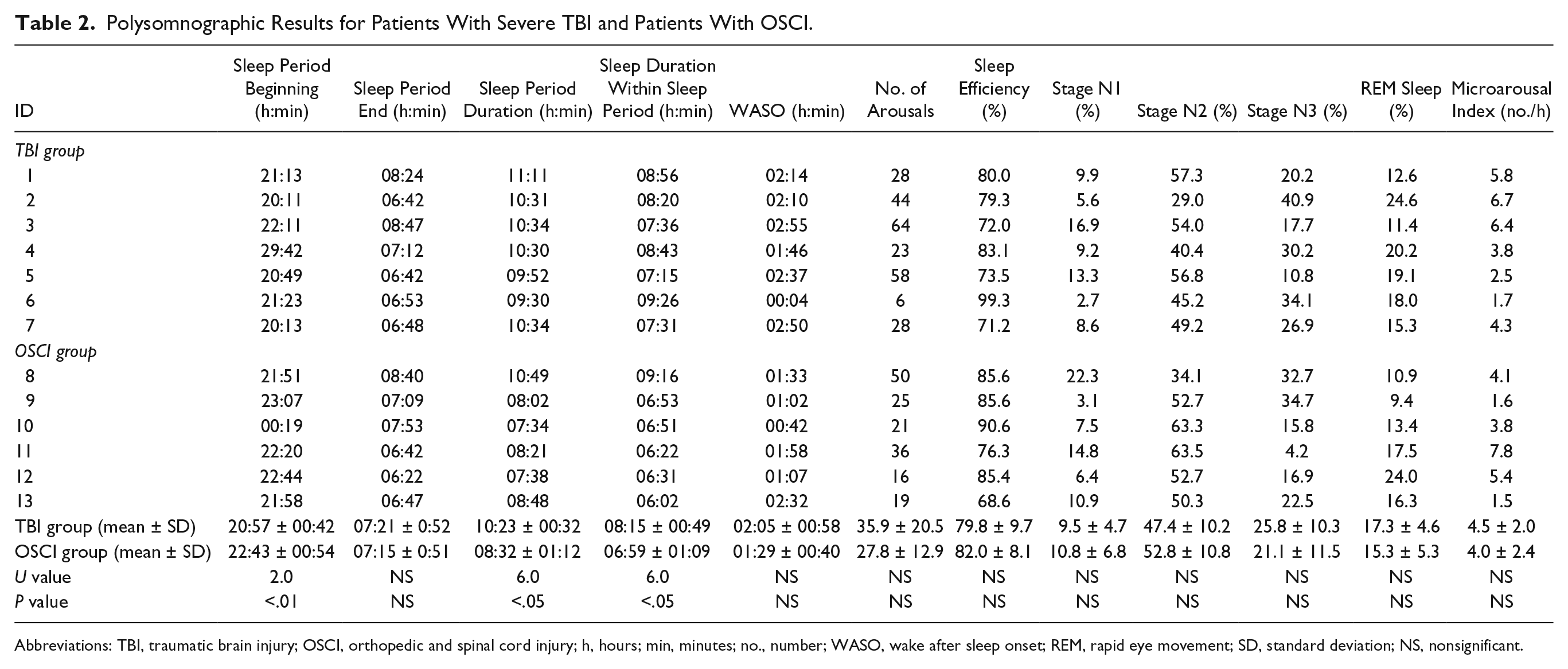
Abbreviations: TBI, traumatic brain injury; OSCI, orthopedic and spinal cord injury; h, hours; min, minutes; no., number; WASO, wake after sleep onset; REM, rapid eye movement; SD, standard deviation; NS, nonsignificant.
All PSG recordings were reviewed by a neurologist with specific training in sleep medicine and with several years of experience in a sleep clinic (AD). Sleep stages and events were scored according to the American Academy of Sleep Medicine Manual 20 by a trained medical electrophysiology technologist with a strong expertise in sleep. The following variables were derived: sleep period duration, beginning and end of the sleep period, total sleep time, sleep efficiency (percentage of time asleep during the sleep period), amount of wake after sleep onset, number of awakenings, microarousal index (number of microarousals/hour), minutes and percentages of each sleep stage, and REM sleep latency. Sleep variables were calculated for the nocturnal sleep period.
Statistical Analyses
All results are reported with descriptive statistics using means, standard deviations, and medians. Given our small sample, nonparametric tests were used. Mann-Whitney U tests were performed to compare the groups for clinical and sleep variables. Additionally, Spearman correlations were run between PSG variables and clinical characteristics. Correlations were conducted on data from all participants (TBI and OSCI), except for variables specific to TBI (eg, GCS, RLA). Significance was set at P < .05.
Results
Clinical Characteristics of Our Sample
Demographic and clinical characteristics of the TBI and OSCI groups are presented in Table 1. The TBI group included 7 patients (3 females; 24.4 ± 10.4 years old, median = 20 years) and the OSCI group comprised 6 patients (3 females; 33.2 ± 16.5 years, median = 25 years). No significant group difference was found for age and sex. The average initial GCS in the TBI group was 4.9 ± 1.9 (median = 5, range = 3-7) at the emergency room, which corresponds to severe TBI criteria. Among the 7 TBI patients, 6 also had severe orthopedic injuries. Although pain was not operationally evaluated during the PSG recording, 2 TBI patients and all OSCI patients were taking analgesic medication. Brain CT scan findings were classified according to Marshall score, 16 with 2 TBI patients having a score of I (no visible pathology) and 5 having a score ranging from II (diffuse injury) to IV (any lesion surgically evacuated; detailed neuroimaging findings are presented in Table 1). RLA scores at the time of PSG are presented in Table 1 in order to provide a gross measure of cognitive function for the TBI group. The RLA levels ranged from III (Localized response only: patient responds specifically and inconsistently with delays to stimuli, but may follow simple commands for motor action) to VIII (Purposeful, appropriate response: patient oriented, responds to environment but abstract reasoning abilities decreased). No group difference was found for the time between injury and PSG recording (TBI: 20.3 ± 15.0 days, median = 12 days; OSCI: 16.0 ± 5.0 days, median = 15.5 days), time between ICU discharge and PSG (TBI: 5.6 ± 3.4, median = 5 days; OSCI: 5.5 ± 5.9, median = 5 days) or hospital length of stay (TBI: 34.7 ± 22.0, median = 34 days; OSCI: 26.5 ± 14.4, median = 20.5 days).
Polysomnography
Table 2 presents individual PSG results. The duration of sleep periods was longer in the TBI group compared to the OSCI group (TBI: 10:23 ± 00:32, median = 10:31; OSCI: 08:32 ± 01:12, median = 08:11, U[11] = 6.0, Z = 2.07, P < .05), with an earlier sleep onset for the TBI than the OSCI group (TBI: 20:57 ± 00:42, median = 20:49, OSCI: 22:43 ± 00:54, median = 22:32, U[11] = 2.0, Z = −2.7, P < .01). However, the end of their sleep periods occurred at a similar time. Within the sleep period, TBI patients had a longer sleep duration than OSCI patients (TBI: 08:15 ± 00:49, median = 08:20; OSCI: 06:59 ± 01:09, median = 06:41, U[11] = 6.0, Z = 2.07, P < .05). Long duration of awakening after sleep onset and poor sleep efficiency were observed for both groups with no significant group differences. No group difference was found for arousal variables or microarousal index. All sleep stages were present in all patients from both groups and we were able to identify all elements of sleep, such as sleep spindles, k-complexes, and sleep stages in all participants. When the percentage of each sleep stage was considered, very similar sleep architecture was observed between the 2 groups for N1, N2, N3, and REM sleep.
Variables Associated With Polysomnographic Characteristics
No significant correlation was found between clinical characteristics (eg, initial GCS, ICU length of stay, delay between injury, and PSG) and sleep variables. Cumulative dose of analgesic and sedative medication received during the ICU stay was also not associated with any PSG variables.
Discussion
This study demonstrates the feasibility of measuring sleep via PSG in acute severe TBI patients. Although the findings of this study must be considered as preliminary, we observed that, in comparison to a control group of OSCI patients without moderate-severe TBI, patients with severe TBI had longer nocturnal sleep duration and earlier nighttime sleep onset during their hospital stay.
Feasibility and Usefulness of PSG in Acute Care
The small sample within the present study is representative of the challenges of performing PSG in acute TBI patients. Some patients are unable to tolerate the materials, and/or may be confused or agitated, which limits the feasibility of PSG in the acute stage. On the other hand, patients with a more rapid recovery are better able to tolerate the study materials; however, their fast recovery is then associated with a much smaller window of time between the cessation of continuous sedation and hospital discharge, making it very difficult to conduct a 24-hour PSG.
However, despite these challenges, the use of PSG during the acute phase of severe TBI is feasible, and has been able to provide new information regarding sleep during this very early stage after injury. In fact, we found that despite their fragmented sleep, TBI patients had normal elements of sleep, such as sleep spindles, k-complexes, and normal proportions of each sleep stages. These findings contrast with previous sleep studies performed in sedated non-TBI patients in whom up to 96% of total sleep was spent in stages N1 and N2. The present study also allowed for documentation of the exact amount of sleep in TBI patients, which was higher than that of OSCI patients. Although other techniques such as actigraphy and nurse assessment can give an approximation of sleep duration, only PSG can document exact sleep duration, particularly when sleep is fragmented. It would also have been of interest to evaluate sleep with PSG in the confused/agitated state, during which an absence of rest-activity cycle consolidation was documented by actigraphy. 4 However, PSG is not feasible during this stage, due to posttraumatic agitation and intolerance to the materials. Thus, for the stage of very early recovery, actigraphy remains the best tool to study sleep-wake patterns.
Excessive Sleep Need or an Inability to Maintain Wakefulness?
It is possible that the preliminary finding of an earlier sleep onset and an increased sleep duration in acute TBI can be explained by an enhanced sleep need secondary to the brain injury. Consistent with this hypothesis, a recent rodent model reported an acute increase in sleep duration immediately following TBI. 8 Findings among humans also show that excessive sleep need is observed in approximately 22% of mild to severe TBI patients reporting chronic sleep-wake disturbances 21 ; however, an excessive sleep need has not previously been documented among acute TBI patients. The role of sleep in neuroplasticity and neurogenesis is well recognized,22,23 and it is possible that some aspects of sleep may be critical for brain recovery following TBI and thus may be driving an increased need for sleep. This warrants further investigation.
Conversely, it is also possible that the increased sleep duration and early sleep onset observed in the present study may be reflective of an inability to maintain wakefulness rather than an excessive sleep need. This interpretation has been proposed among several animal models of TBI,7,10,24 and a decrease in hypocretin-1 (orexin) neuron activation, a neuropeptide involved in the arousal system, has been reported in mice 1 month after injury.7,24 In humans, a large decrease in cerebrospinal fluid levels of hypocretin-1 25 and a loss of histaminergic neurons in the tuberomammillary nucleus, a major arousal-promoting nucleus located in the posterior hypothalamus, has also been found following severe TBI. 26 These observations suggest that impaired neurotransmitter signaling may be a contributing factor to a decreased ability to maintain wakefulness, resulting in increased sleep duration and earlier sleep onset among our patients.
Sleep Deprivation Hypothesis
Factors other than the brain injury itself may explain the hypothetical increased sleep need or the inability to maintain wakefulness. The hospital environment (eg, noise, light, activities) in of itself may explain in part the poor sleep efficiency we observed for both TBI and OSCI patients. Severe sleep abnormalities have been reported in critically ill non-TBI patients in the ICU,27-29 with up to 96% of actual sleep time spent in the lighter stages of sleep. Moreover, the previous actigraphy study conducted by our group showed an absence of well-consolidated rest periods among TBI patients hospitalized in the ICU. 4 Thus, a significant sleep debt is likely to have accumulated while our patients were in the ICU, which may be one contributing factor to our finding. However, the average interval between ICU discharge and PSG recording was similar across the 2 groups of subjects. It is possible that the TBI patients experienced greater sleep deprivation during their stay in ICU than those with OSCI and thus may have accumulated a greater sleep debt; however, this was not measured in the current study.
Medications
Almost all patients were being administered medications that are reported to cause varying degrees of sleep modifications in healthy subjects, 30 including analgesics. Some of these medications (amantadine, piperacillin and tazobactam, and hydromorphone) have been reported to cause insomnia, while mirtazapine is known to increase total sleep time, and pregabalin and mirtazapine decrease number of awakenings in healthy subjects. Morphine is reported to decrease N3 sleep and increase N2, though it is not reported to modify total sleep time. 31 Opioid medication is known to influence sleep with suppression of REM sleep and slow wave sleep followed by a subsequent rebound.32,33 It is difficult to specifically delineate sleep modifications that may be related to or a result of medication in our sample. However, the increased sleep duration observed in the TBI patients cannot be explained by mirtazapine, as only one patient was taking this medication.
Limitations of the Study
Given the specific nature of this study, the challenges of recruiting among severely injured patients and thus our small sample size, our findings are preliminary, and further research is needed with larger samples in order to generalize these results to those patients with severe TBI in the acute postagitation stage.
There may also be some limitations regarding the use of OSCI patients as the comparison group. This group differed from the TBI group in terms of pain and analgesic medications administered during the PSG. Moreover, severe orthopedic injury or SCI may lead to acute sleep-wake disturbances. Nevertheless, OSCI patients likely remain the best control group for TBI patients, as both groups include young adults who were healthy prior to their injury, which is not the case for most critically ill patients.
Finally, we recognize the possible and likely confound of pain among both groups in relation to sleep. The OSCI group received more pain medication than the TBI group, most likely due to higher levels of cognitive functioning and awareness. Given the length of our PSG and the terminal half-life analgesic (eg, 2.3 hour for hydromorphone), we recognize that pain levels likely would have fluctuated throughout the PSG recordings. Future studies would benefit from the addition of a simple visual analog pain scale for those patients able to complete it.
Conclusion
Consistent with our hypothesis, sleep was fragmented with low sleep efficiency indicative of poor-sleep quality. Similar results were also found among the comparison group of OSCI patients and likely reflect nonspecific factors associated with the traumatic experience and the hospital environment. However, the results of this preliminary study demonstrate that an earlier sleep onset and increased sleep duration for those patients with severe TBI are the primary differences in sleep identified between the 2 groups.
A possible interpretation may be that the brain damage associated with severe TBI results in either an increased sleep need or a difficulty maintaining wakefulness. This interpretation is consistent with high levels of sleepiness frequently reported among TBI patients. 34 Improving sleep quality during the acute stage of TBI with consideration of pharmacological and environmental factors may optimize recovery of the brain itself and improve the ability to maintain optimal levels of arousal and wakefulness for cognitive recovery.
Footnotes
Acknowledgements
The authors are grateful to Ms Bridget Gibson, clinical coordinator, Ms Elyse Laflamme, occupational therapist, and staff of the traumatology program, neurological unit, and orthopaedic unit, of Hôpital du Sacré-Coeur de Montréal for their collaboration with the patients’ recruitment and evaluation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Canadian Institutes of Health Research (grant to NG and scholarship to CD), by the Fonds pour la recherche du Québec–Santé (grant to NG), by the Réseau provincial de recherche en adaptation-réadaptation (fellowship to CWH), by the Consortium pour la recherche en traumatologie du Québec (grant to NG), and by the Fondation Neurotrauma Marie-Robert (scholarship to CD).