
Abstract
Keywords
Introduction
Sleep-wake disturbances occur across the spectrum of traumatic brain injury (TBI) severity. 1 Those with TBI often report subjective sleep complaints such as difficulties with sleep initiation and sleep maintenance, and overall poorer sleep quality2,3 and show objective sleep alterations, characterized by reduced total sleep time, increased nocturnal awakenings, and changes to sleep architecture.4-6 Sleep disorders such as insomnia, circadian rhythm sleep disorders, and sleep apnea also frequently occur in TBI, 1 which may lead to reduced quality of life and impede rehabilitation outcomes. 7 Although insult to brain regions involved in sleep-wakefulness may contribute to sleep disturbances in TBI, the precise mechanisms are poorly understood.
Melatonin is a hormone secreted by the pineal gland during the biological night and is intricately involved in the regulation of the daily sleep-wake cycle. 8 We recently showed that individuals with moderate to severe TBI had lower evening melatonin production than healthy individuals, suggesting that TBI may disrupt the melatonin synthesis pathway, leading to altered sleep-wake cycles. 4 Because our previous study only measured melatonin in the evening, it is unclear whether total night-time melatonin production is attenuated. Examining melatonin profiles following TBI may provide insight into the biological underpinnings of sleep disturbances and inform appropriate treatments for sleep disturbances in TBI patients. The current study characterized the circadian melatonin rhythm (including total melatonin production and timing) in TBI patients compared with healthy volunteers.
Methods
Human Participants
TBI patients were recruited from rehabilitation centers as part of an ongoing clinical trial (ACTRN#12611000734965). Controls were recruited via online advertisements. This study was conducted in accordance with the Declaration of Helsinki and approved by the local Hospital and University ethic committees, respectively.
TBI patients had sustained blunt head trauma with no preinjury history of neurological or psychiatric illness or sleep/fatigue disturbance. All TBI patients included in the study were community dwelling, living independently, and unemployed. TBI severity was determined by length of posttraumatic amnesia (PTA), calculated using the Westmead PTA scale, administered by neuropsychologists and trained nurses. All TBI patients were diagnosed with chronic insomnia by a sleep physician according to current international diagnostic criteria. 9 Control participants had no history of TBI, or poor sleep quality, corroborated by Pittsburgh Sleep Quality Index (PSQI) scores less than 5. 10 Controls demonstrated a regular sleep-wake routine, with sleep duration ranging from 6 to 9.5 hours.
Participants were excluded if deemed at high risk of obstructive sleep apnea as determined by the Berlin Sleep Questionnaire. 11 Participants did not engage in night shift and had not undertaken transmeridian travel across 1 time zone in the preceding 6 weeks. Benzodiazepines, hypnotics, and over-the-counter sleep medications were not permitted 6 weeks prior.
Melatonin Rhythm
The primary outcome was total overnight melatonin production. Circadian phase, measured by dim light melatonin onset (DLMO) and melatonin synthesis onset (SynOn) and offset (SynOff) were secondary outcomes. DLMO is a common method to assess circadian phase, defined as the interpolated time at which melatonin levels exceed 2.3 pg/mL for 2 consecutive samples. Melatonin SynOn and SynOff were calculated by fitting a modified physiologically based mathematical model to the melatonin profiles using Isqnonlin in MATLAB 2014b (MathWorks, Inc, Natick, MS). 12 Melatonin synthesis duration was determined by subtracting SynOff from SynOn. The area under the melatonin curve (AUC) during the synthesis period was calculated using the trapezoidal method. The AUC, between SynOn and SynOff, was used to indicate total overnight melatonin production. The temporal relationship between the onset of melatonin synthesis and habitual bedtime was examined to investigate the circadian regulation of sleep-wakefulness.
Other secondary outcomes included the PSQI and Epworth Sleepiness Scale (ESS) as measures of sleep quality and daytime sleepiness, respectively. Global PSQI scores greater than 5 are indicative of poor sleepers. 13 Global PSQI scores greater than 8 have been shown to have high specificity and sensitivity for a diagnosis of insomnia in patients with TBI. 14 ESS scores from 11 to 16 indicate mild to moderate daytime sleepiness, and scores of 16 and above indicate severe daytime sleepiness. 15
Procedure
One week prior to the laboratory visit, bedtimes and wake times were determined via phone calls made by the participant to a time-stamped answering machine. Participants were asked to maintain their self-reported regular sleep-wake cycle in the lead up to the assessment. Bed and wake times were self-selected and averaged over the previous week.
On the day of assessment, participants abstained from caffeine and arrived at the laboratory 7 hours prior to habitual bedtime from the previous week. The laboratory consisted of a sound-attenuated, light-proof, and temperature-controlled suite with en suite. Saliva samples were collected hourly (Salivette, Sarstedt, Germany), 6 hours before bedtime until 2 hours after waking. Participants were permitted to sleep in between saliva collections during their habitual sleep period. Immediately after collection, samples were centrifuged, frozen (−20°C), and analyzed for melatonin via radioimmunoassay, as previously described. 4
Food, activity, and light intensity level (<10 lux during wake, <1 lux during sleep) were controlled. A standardized caloric evening and morning meal were provided 5 hours prior to habitual bedtime and 1 hour after habitual wake time, respectively. Participants maintained a semirecumbent posture during the wake period and were frequently monitored by direct observation. They were instructed to remain seated, and the consumption of food and beverages was prohibited 20 minutes prior to each saliva collection. During this entire study, participants were instructed to minimize movement, and the consumption of food and beverages were restricted to preallocated time slots. During the wake period, participants were permitted to read, engage in quiet tasks, and view films. The television screen was dimmed and placed ~4 m from the participant’s eyes. Hourly light recordings were taken on a horizontal plane at the participant’s eye level to ensure ambient light levels were maintained at <10 lux, and hourly light assessments were taken on a vertical plane. The use of mobile phones was not permitted throughout the study. During the sleep episode, participants were transferred to a hospital bed.
Statistics
Statistical analysis was conducted with IBM SPSS Statistics 20.0 (SPSS Inc, Chicago, IL). Paired sample t-tests (2-tailed) were performed for group differences.
Results
Participant Characteristics
A total of 10 patients with TBI and 10 age- and gender-matched healthy volunteers completed the protocol. Duration of PTA indicated that the majority of patients had severe TBI. All ESS scores for controls fell within normal limits (ie, ESS ranged from 1 to 7). For the TBI group, scores from 7 participants fell within normal limits, 2 showed mild to moderate sleepiness, and 1 showed severe daytime sleepiness. All global PSQI scores for controls fell within normal limits, ranging from 1 to 4. Of the TBI patients, PSQI scores for 1 participant fell in the upper end of the normal range; 1 had a score of 7, and the remaining 8 participants scored from 8 to 17. Melatonin rhythm could not be ascertained for 1 TBI patient because there was no rise in melatonin levels beyond the threshold we used for melatonin onset, leaving a final sample of 9 participants in each group (Table 1).
TBI and Control Participant Characteristics, and Subjective Sleep and Melatonin Parameters. a
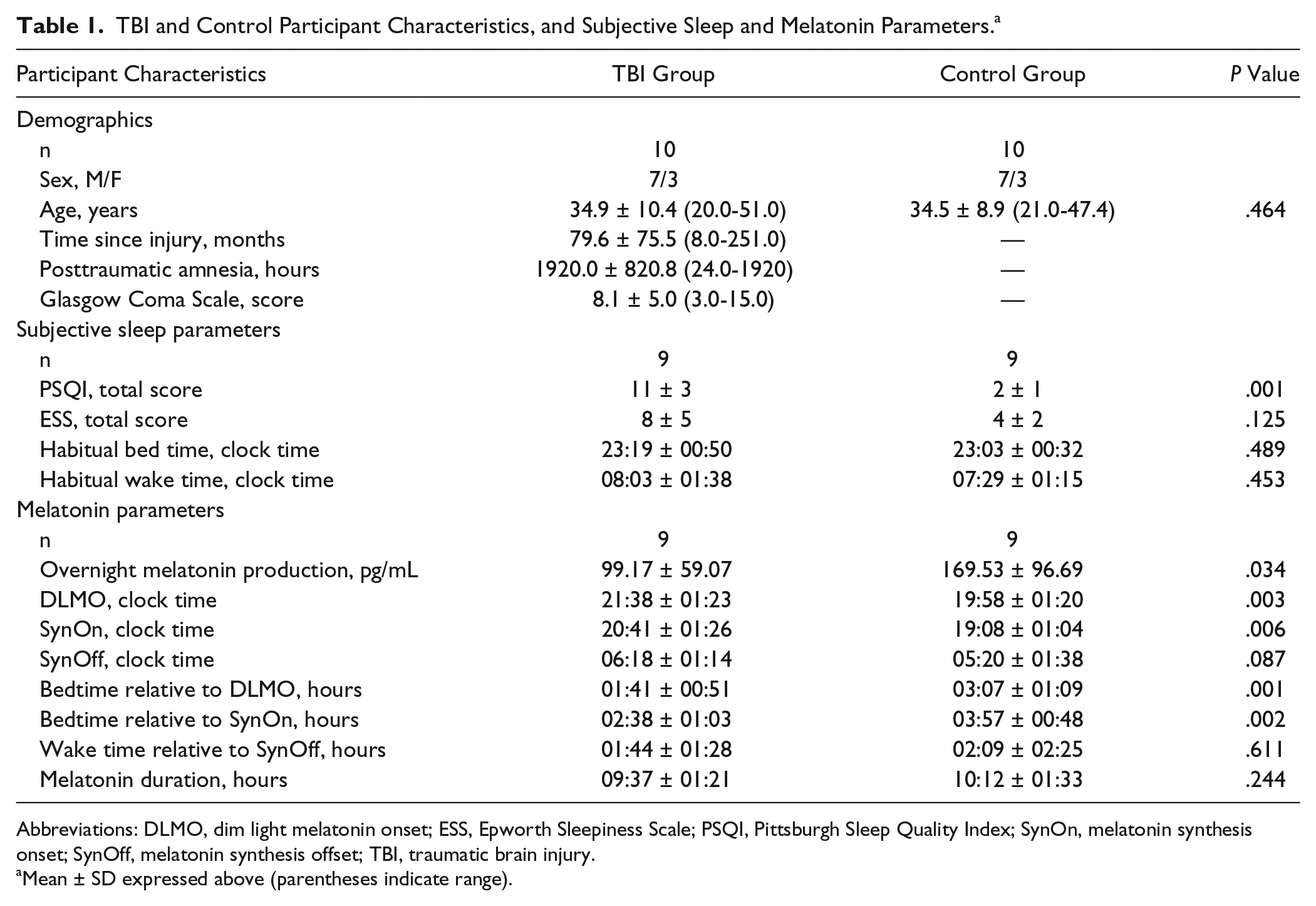
Abbreviations: DLMO, dim light melatonin onset; ESS, Epworth Sleepiness Scale; PSQI, Pittsburgh Sleep Quality Index; SynOn, melatonin synthesis onset; SynOff, melatonin synthesis offset; TBI, traumatic brain injury.
Mean ± SD expressed above (parentheses indicate range).
Melatonin Rhythm
Overnight melatonin production (AUC) was 42% lower in TBI patients as compared with controls: t(8) = −2.56; P = .034; d = 0.87 (Figure 1A).
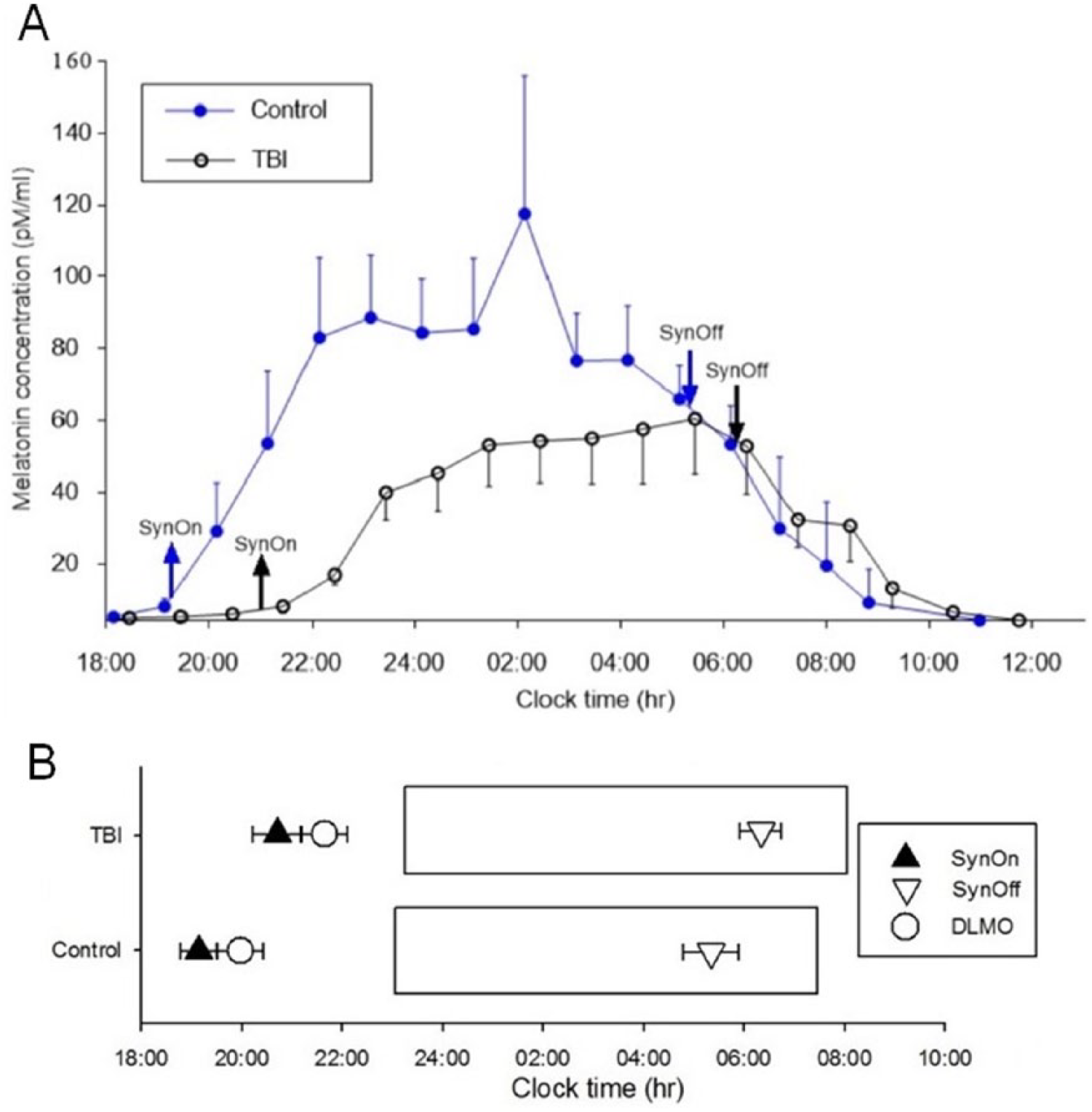
Overnight salivary melatonin profiles and melatonin onset relative to sleep schedule in patients with TBI and controls. Average overnight (±SE) salivary melatonin levels relative to habitual bedtime for patients with TBI and controls (Figure 1A). The control group had higher melatonin production during the synthesis period than the TBI group (P = .034). Figure 1B illustrates timing of melatonin onset relative to sleep timing in TBI and control participants. Rectangles indicate average habitual sleep duration in patients with TBI (upper) and controls (lower). Upward triangles indicate average (±SE) SynOn. Circles represent average DLMO (±SE). Downward triangles indicate average (±SE) SynOff. In the TBI group, melatonin onset was delayed, and the temporal relationship between habitual bedtime relative to melatonin onset was shorter for both DLMO and SynOn respectively.
The timing of melatonin synthesis, measured by both DLMO [t(8) = 4.13; P = .003; d = 1.23] and SynOn [t(8) = 3.76; P = .006; d = 1.23], was significantly later (ie, delayed) in TBI patients relative to controls. The temporal relationship between bedtime and DLMO was significantly different between the groups; DLMO occurred 01:41 hours before bedtime in TBI patients and 03:07 hours before bedtime in controls: t(8) = −4.85; P = .001; d = 1.42 (Figure 1B).
Subjective Sleep Parameters
No differences were observed in ESS scores between the TBI patients and controls (P > .05). The TBI group reported higher PSQI scores than controls: t(8) = 8.37; P = .000; d = 4.17. This was expected, given that we selected a control group with normal PSQI scores.
Discussion
This study showed that patients with severe TBI diagnosed with chronic insomnia produced 42% less melatonin overnight compared with controls, suggesting disruption to the circadian regulation of melatonin synthesis. Furthermore, melatonin synthesis (DLMO) was delayed by 1.5 hours in TBI patients relative to controls. Despite both groups reporting similar bedtimes, onset of melatonin synthesis occurred closer to habitual bedtime in those with TBI.
Our previous work demonstrated that TBI patients had lower levels of melatonin in the evening. 4 The present study extends this finding in a separate sample, demonstrating that melatonin production remains attenuated in TBI patients throughout the night. In the acute phase of injury, nocturnal light exposure in the intensive care unit environment may suppress melatonin. 16 In our study, patients were on average 6 years postinjury, suggesting that attenuated melatonin levels are an enduring consequence of TBI.
Attenuated melatonin synthesis in TBI may be underpinned by primary and secondary pathophysiological alterations, which may impair regions of the brain involved in the regulation of melatonin. TBI may cause microscopic lesions to the retinohypothalamic tract and to the neuronal pathway extending from the suprachiasmatic nucleus to the pineal gland, which is the primary site of melatonin production. 17 This may alter melatonin synthesis and disrupt circadian rhythms, potentially leading to sleep disturbance. 18 Changes in circadian phase, as observed in the current study, may be underpinned by external factors such as lifestyle changes, which result in altered light-dark exposure patterns, thereby altering the timing of the circadian pacemaker. 19 Such extrinsic factors may play a role, given that all TBI patients featured in the current study were unemployed. All patients with TBI included in the current study were diagnosed with insomnia, which in itself has been associated with alterations in circadian phase and, potentially, also thermoregulatory processes. 20 Although those with TBI displayed disrupted circadian melatonin profiles, the extent to which this contributes to poorer sleep quality is unknown. We did not have sufficient power to examine the relationships between melatonin parameters and subjective sleep scores in the TBI group.
Melatonin is thought to be involved in the circadian regulation of the sleep-wake cycle, with exogenous melatonin exhibiting both phase-shifting and sleep-promoting properties. 21 In patients with tetraplegia, abolished endogenous melatonin rhythms are associated with reduced sleep efficiency and quality. 22 In older individuals, some reports suggest that insomnia is associated with reduced melatonin, and melatonin supplementation is efficacious in improving sleep quality in patients with attenuated melatonin profiles. 23 Future work is required to demonstrate that altered melatonin profiles are associated with poorer sleep quality in TBI.
There is some evidence that diurnal cortisol profiles are attenuated during the acute phase of TBI, indicating disruption of the hypothalamic-pituitary-adrenal axis. 24 Like melatonin, cortisol exhibits a strong circadian rhythm that is regulated by the suprachiasmatic nucleus. 25 Attenuation of the diurnal cortisol profile was predictive of the development of excessive daytime sleepiness. 24 In light of these findings and our study showing that the melatonin rhythm is attenuated in TBI patients, the significance of dampened circadian signaling in sleep-wake, cognitive, and mood disturbances in TBI patients should be examined.
A limitation of the present study was that melatonin was not assessed before and after the TBI event; therefore, we cannot infer causation. Furthermore, because sleep was disrupted hourly for saliva sample collection, we did not assess sleep during the laboratory visit. The absence of actigraphy prior to the circadian phase assessment prevented us from verifying each participant’s sleep-wake schedule and light-dark exposure history prior to the laboratory visit, which likely would have contributed to altered timing of melatonin secretion. Similarly, because we did not measure environmental, lifestyle, or comorbid factors such as activity, pain, or mood, we are unable to determine specific factors associated with lower melatonin levels. Finally, our sample comprised patients with severe TBI, who were not taking sleep medications. Therefore, it is unclear whether the results generalize across the spectrum of TBI severity and to TBI patients taking medications.
The present results suggest that patients with severe TBI and insomnia display disruption to the circadian regulation and timing of melatonin synthesis. Our findings establish a basis for future studies examining chronobiological treatment approaches for sleep-wake disturbances in TBI patients.
Footnotes
Acknowledgements
The authors acknowledge Professor David Kennaway and Mark Salkeld for expertise with melatonin analysis. The authors thank Dr Matthew Pase, Dr Sean Cain, and Dr Tracey Sletten for their critical review of the manuscript. We thank Dr Suzanne Ftouni for assistance with preparation of the figures and Ms Jade Murray for assistance with implementation of the study protocol.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NAG, JLP, MAStH, and DM report no disclosures. SMR reports that he has served as scientific consultant, through his institution, to Vanda Pharmaceuticals and Philips Respironics. He is a program leader in the Cooperative Research Centre for Alertness, Safety and Productivity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding of the study was supported by an Australian National Health and Medical Research Council project grant (#1028733). NAG was funded by an Australian Postgraduate Award.