
Abstract
Objective. To examine the efficacy of the modified Story Memory Technique (mSMT) to improve learning (ie, acquisition) and memory in participants with TBI. The mSMT is a behavioral intervention that teaches context and imagery to facilitate learning within 10 sessions over 5 weeks. Methods. A total of 69 participants with moderate-severe Traumatic Brain Injury (TBI), 35 in the treatment group and 34 in the placebo control group, completed this double-blind, placebo-controlled randomized clinical trial. A baseline neuropsychological assessment was administered, including questionnaires assessing everyday memory. Repeat assessments were conducted immediately posttreatment and 6 months following treatment. Participants in the treatment group were randomly assigned to a booster session or a non–booster session group after completion of treatment with the mSMT to examine the efficacy of monthly booster sessions in facilitating the treatment effect over time. Results. The treatment group demonstrated significant improvement on a prose memory task relative to the placebo group posttreatment (η2 = 0.064 medium effect). Similar results were noted on objective measures of everyday memory, specifically prospective memory (Cohen’s w = 0.43, medium effect), and family report of disinhibition in daily life (η2 = 0.046, medium effect). Conclusion. The mSMT is effective for improving learning and memory in TBI. Classification of evidence. Based on widely accepted classification systems for treatment study design, this study provides class I evidence that the mSMT behavioral intervention improves both objective memory and everyday memory in persons with TBI over 5 weeks. Thus, this study extends the evidence for efficacy of the treatment protocol to a sample of persons with TBI.
Approximately 1.6 million Americans sustain a TBI each year, 1 with cognitive impairment being a common concomitant. 2 Cognitive dysfunction may affect attention, 3 information processing abilities, 4 language skills, executive functions, learning and memory.4,5 Memory is one of the most frequently impaired functions identified in this population,2,6 -8 with current prevalence rates ranging from 54% to 84%. 4 Such deficits have been shown to exert a significant negative impact on multiple aspects of everyday life, including occupational, emotional, and social functioning, and is a major cause of disability among these individuals.9,10 In fact, deficits in learning and memory functioning are a major factor in one’s ability to maintain meaningful employment after TBI. 4 As a result, virtually all intensive TBI rehabilitation programs include some form of cognitive intervention to minimize the impact of these deficits on daily life.9,11
Despite the fact that previous studies have examined the efficacy of cognitive rehabilitation, much of this research is lacking in methodological rigor. Specifically, Cicerone and colleagues have conducted several critical reviews of the literature,9,11,12 only reporting 10 prospective, randomized clinical trials for memory rehabilitation. These studies examined protocols utilizing external assistive devices/aids,13 -15 memory strategy applications,16 -18 mnemonics, rehearsal and visual imagery training,19,20 and computer-based memory software.21,22 Although modest treatment effects were reported, the magnitude of the treatment effects observed and the long-term efficacy of the treatment were difficult to determine.
Memory deficits may be a result of difficulty in multiple aspects of the memory process.6,23 -25 Previous research in our laboratory has shown that individuals with TBI have difficulty learning, that is, acquiring new information (defined as encoding + consolidation). Specifically, participants with TBI require significantly more learning trials than healthy participants to learn the same amount of information. However, once equated on the amount of information initially learned, individuals with TBI do not demonstrate deficits in recall or recognition. 24 Given that the memory deficit in TBI is primarily one of learning new information, an effective cognitive remediation program must target new learning abilities.
Context and imagery have been demonstrated to be effective in improving learning and memory in healthy controls26,27 and samples of TBI patients.20,28 -30 The current study was designed to extend the evidence for efficacy of the modified Story Memory Technique (mSMT31,32) to a sample of people with TBI. This treatment protocol was specifically designed to remedy deficits in new learning and memory functioning utilizing the strategies of context and imagery. The mSMT is a 10-session behavioral treatment protocol designed to teach the patient to use context and imagery to facilitate learning. Several studies now demonstrate the efficacy of the mSMT in other neurological populations. For example, research from our lab has demonstrated that the mSMT improves new learning and memory abilities, as determined by a neuropsychological evaluation, as well as everyday life activity in persons with multiple sclerosis (MS).31,32 In addition, work from our lab has demonstrated that relative to placebo controls, MS participants in the treatment group showed increased cerebral activation 33 and increased connectivity 34 while performing a memory task posttreatment using fMRI within a widespread cortical network involving frontal, parietal, precuneus, and parahippocampal regions. The increased activation seen likely reflects increased application of strategies taught during the mSMT when learning new information. 33
The current study was designed to examine the efficacy of the mSMT in a large sample of persons with TBI. The primary hypothesis was that participants with TBI in the treatment group with documented learning and memory impairment will demonstrate significant improvement on standardized neuropsychological (NP) memory tasks following the 10-session memory retraining with the mSMT relative to placebo controls. Secondary hypotheses were the following: (1) Improvement in learning and memory functioning in the treatment group will also be noted on objective measures of everyday memory, specifically the Rivermead Behavioural Memory Test (RBMT); such changes will not be evident in the TBI placebo control group; (2) compared with persons in the placebo-control group, persons in the treatment group will show decreased cognitive symptoms in daily life on the self-report and family report of the Frontal Systems Behavior Scale (FrSBe); and (3) based on previous work demonstrating an improvement in emotional symptomatology following cognitive rehabilitation in multiple neurological populations,35 -41 we hypothesized that depression and anxiety levels will decrease following participation in the mSMT in the treatment group but not the placebo control group. It was additionally expected that participants with TBI will continue to demonstrate improvement in their new learning abilities up to 6 months following treatment and that booster sessions would result in significantly better long-term treatment effects.
Method
Participants
A total of 69 participants (treatment, n = 35; control, n = 34) were recruited from local TBI clinics, study advertisements published in consumer newsletters and distributed at support groups, through the Northern NJ TBI Model System, and through the Kessler Foundation database of research participants. There were no significant differences between the groups in age, gender, estimated premorbid verbal IQ, baseline learning ability, or time since injury (Table 1). The control group had significantly greater years of education: t(63) = 2.68; P < .01. The groups performed similarly on tests of NP functioning prior to treatment as well as reports of both depression and anxiety (Table 2). Verification of health status, date of injury, and duration of loss of consciousness was achieved via medical record review.
Demographic and Disease Characteristics by Treatment Group.
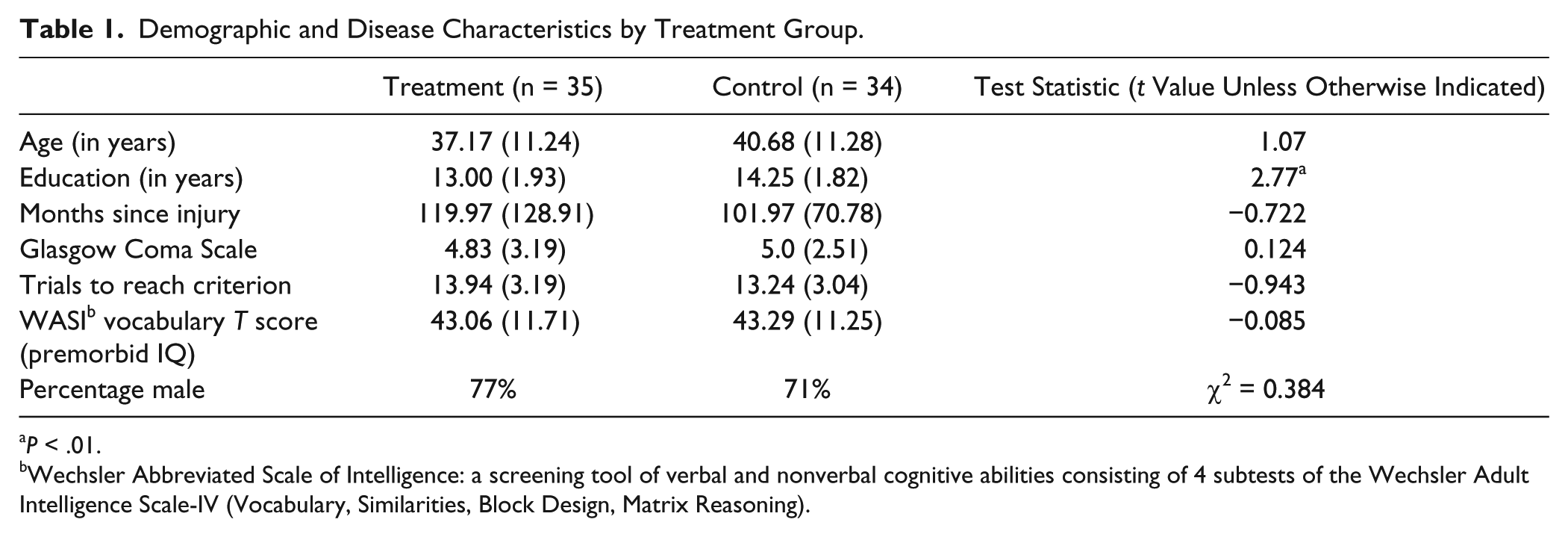
P < .01.
Wechsler Abbreviated Scale of Intelligence: a screening tool of verbal and nonverbal cognitive abilities consisting of 4 subtests of the Wechsler Adult Intelligence Scale-IV (Vocabulary, Similarities, Block Design, Matrix Reasoning).
Neuropsychological Test Performance by Treatment Group at Baseline.
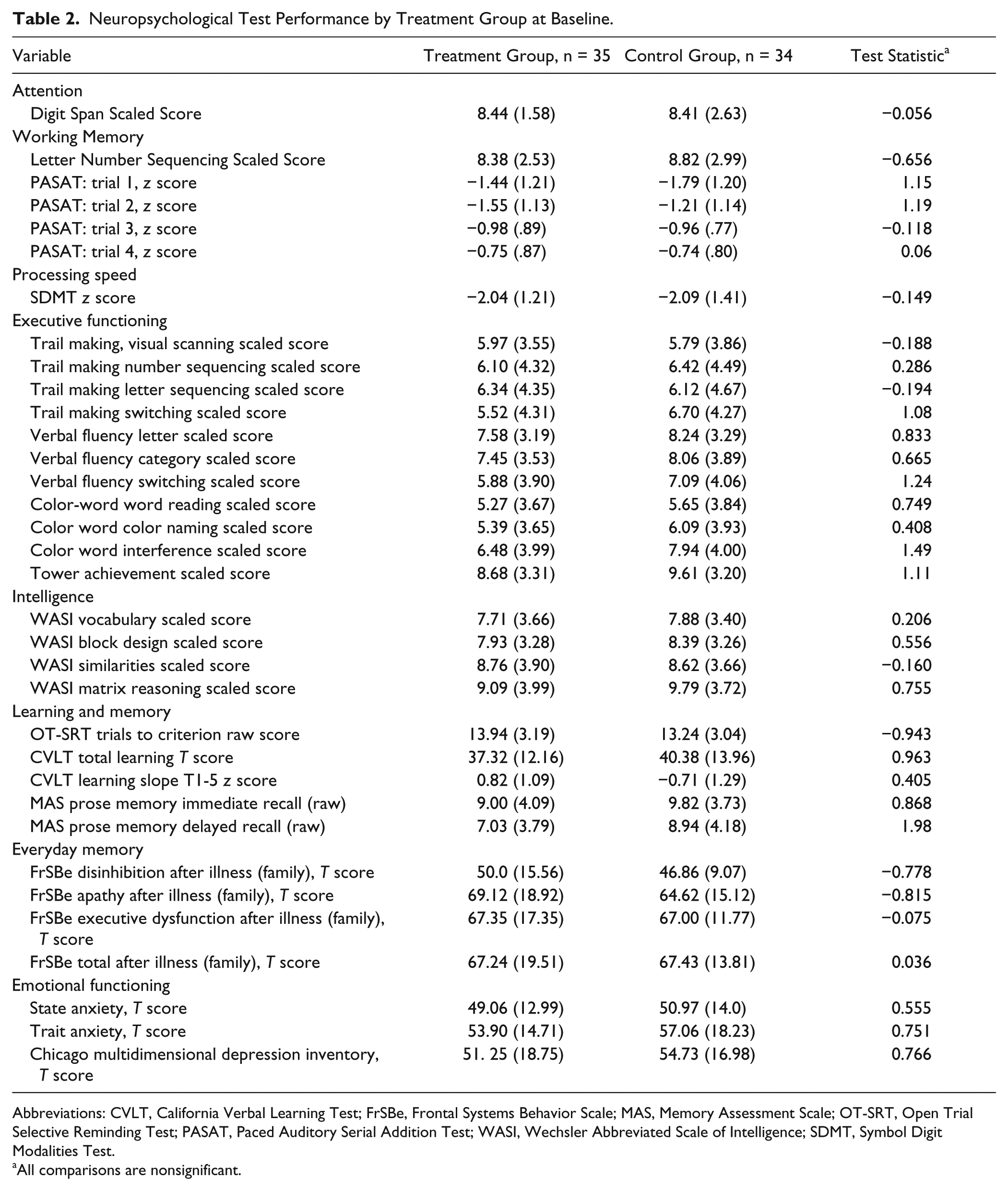
Abbreviations: CVLT, California Verbal Learning Test; FrSBe, Frontal Systems Behavior Scale; MAS, Memory Assessment Scale; OT-SRT, Open Trial Selective Reminding Test; PASAT, Paced Auditory Serial Addition Test; WASI, Wechsler Abbreviated Scale of Intelligence; SDMT, Symbol Digit Modalities Test.
All comparisons are nonsignificant.
Inclusion Criteria
Objective evidence of impaired new learning (ie, acquisition) and memory was required for participation, defined as performance 1.5 standard deviations or greater below the mean of a healthy group on the Open Trial Selective Reminding Test (OT-SRT 42 ). The OT-SRT is a list learning task in which the examiner reads a list of 10 semantically related words on trial 1, and the participant recalls as many words as possible. On the remaining trials, the examiner reminds the participants of only the words he or she did not recall on the previous trial. This procedure continues until all 10 words have been recalled correctly on 2 consecutive trials or a maximum of 15 learning trials were completed. Only individuals requiring 8 or more trials to reach the learning criterion were included. Participants were 18 to 59 years of age, 1 year postinjury and demonstrated ability to follow 1, 2, and 3 step commands on the Token Test. 43
Exclusion Criteria
Potential participants were excluded if they had (1) neurological history besides TBI; (2) uncontrolled seizures; (3) hydrocephalus; (4) current steroid and/or benzodiazepine use (medications reflecting standard of care in TBI were not excluded; however, dosages were monitored for stability throughout participation); (5) history of diagnosed major depressive disorder, schizophrenia, bipolar disorder; (6) history of a diagnosed substance use or dependence disorder (including alcohol); (7) evidence of significant vision impairment from diplopia, nystagmus, or scotomas on testing (corrected vision in worse eye >20/60).
Power
Based on our pilot study of the mSMT in MS, 31 we expected a 10% increase in performance on a verbal learning test following treatment in a sample with moderately impaired new learning. This is a modest estimation of effect size when applying the technique to a sample of TBI patients, given that a previous study 40 found a large effect size with a similar cognitive intervention in TBI. A repeated-measures design was used in which both the experimental and control groups were assessed 3 times on the California Verbal Learning Test (CVLT), a 16-item list learning test commonly used in neuropsychological assessment, with alternate forms: baseline, postintervention, and follow-up. Given previous research on this measure in TBI, we expect the mean CVLT total learning to be roughly T = 36 (SD = 10) 44 in our sample of TBI patients. With analysis of covariance (ANCOVA) as the primary method for examining group differences following treatment, a hypothesized 10% increase in CVLT from baseline to immediate follow-up, and significance set at .05 for a nondirectional test, only 30 participants per group were needed to achieve power of 0.80.
Design
This RCT used a 5-week, double-blind, parallel-groups design. Potential participants underwent a 2-part screening prior to enrollment, consisting of an initial telephone screen for age, injury type and date, neurological history, and current medications and an in-person screening for psychiatric and substance abuse history, visual acuity, language comprehension, and learning and memory.
The groups were assigned via 1:1 randomization using a computerized random number generator. Treatment allocation was concealed. The individual responsible for group assignment was not otherwise involved in data collection, and group assignment was verified by a second individual via a duplicate copy of the randomization table generated before the initiation of data collection. Only the person administering treatment was aware of group assignment. All other study personnel were blinded, which was ensured through several mechanisms. First, therapists and evaluators were always different. Second, therapists and evaluators were not able to communicate directly about participants; all communication occurred through the study coordinator. Participants were blinded to group assignment and consented to participate in a study examining the impact of mental exercises on memory. Participants were informed that they had a 50% chance of being assigned to the treatment or control groups. To evaluate the integrity of blinding, participants completed a questionnaire following participation, with 48% responding with the correct group assignment (chance response rate).
Once qualifying for participation, participants underwent baseline evaluation, including NP assessment and questionnaires assessing the impact of cognition on daily life. The NP was performed in one session, and tests were administered in a standard order for all participants.
Within 1 week of completing treatment, participants completed the same evaluation procedures with alternate forms (immediate follow-up). The treatment group was further randomized into active- or placebo-booster session groups to examine the efficacy of monthly booster sessions to increase maintenance of treatment over time. The randomization method was exactly the same as for treatment group assignment; 1:1 randomization was utilized via a computerized random number generator. Long-term follow-up was then conducted with all participants 6 months following treatment completion. The same evaluator conducted baseline, immediate, and long-term follow-up evaluations wherever possible. All evaluators completed a comprehensive training program prior to receiving approval to conduct NP assessments. This training is standard procedure in our lab and consists of one-on-one training with the lab research coordinator, who has 15 years of experience with NP assessment and cognitive rehabilitation. Training consists of initial presentation of each test individually, guided practice, individual practice with mock participants, and evaluation by the research coordinator. Once approved for testing by the research coordinator, the evaluator must receive a second level of approval from a PhD-level neuropsychologist.
Treatment Protocol
As with assessment procedures, the person administering the treatment protocol was always different from the person conducting the evaluations, to maintain blinding. Training procedures in conducting both treatment and control sessions are tightly based on training procedures for NP testing, consisting of initial presentation of each treatment session, guided practice, individual practice with mock participants, and evaluation by the research coordinator. Again, once approved for testing by the research coordinator, the evaluator must receive a second level of approval from a PhD level Neuropsychologist.
Treatment Group
The mSMT 31 consists of 10 one-on-one treatment sessions occurring twice per week for 5 weeks, lasting 45 to 60 minutes each. Two skills were trained. (1) In sessions 1 to 4, participants were taught to utilize imagery to facilitate learning. This was accomplished through the participants reading stories for which they were instructed to remember the target words and taught to utilize mental imagery to increase their memory for this information. (2) In sessions 5 to 8, participants learned to utilize context to facilitate learning. This was done through the use of word lists, for which the participant was taught to first create a highly visualizable story from the list of words and then apply their newly acquired imagery skills to visualize that story. Sessions 9 to 10 focused on generalization to everyday life; participants were taught to apply the mSMT to real-world memory-demanding tasks, utilizing both context and imagery to remember the information. The treatment is highly manualized, and scripts are provided for the therapist to follow.
Placebo Control
The placebo condition controlled for professional contact and the impact of being in a treatment program. Participants met individually with the therapist at the same frequency as the treatment group, engaging in non–training-oriented tasks. Non–training-oriented tasks consisted of reading the same stories that the treatment groups read and answering questions about their content. The placebo and treatment groups were matched for duration of contact with the examiner and computer presentation of all material. Only the treatment group received the active ingredients of the training (imagery and context).
Booster Sessions
Participants assigned to the booster session condition received monthly sessions similar to training sessions 9 to 10, focused on applying the mSMT to real-world situations. The booster session control group completed the control sessions from the treatment arm of the study. That is, they completed non–training-oriented tasks that consisted of reading the same stories that the treatment groups read and answering questions about their content. Thus, the active and control booster session groups were comparable in everything except for the active ingredients of context and imagery.
Outcome Measures
Coprimary outcomes consisted of 2 NP memory tests: (1) Memory Assessment Scales, Prose Memory (MAS-PM) 45 and (2) the CVLT-II learning slope. 46 MAS-PM examines the ability to learn preorganized verbal information. This test presents a 60-word story about a robbery for immediate and delayed free recall. A parallel form was used for the immediate follow-up. MAS-PM is a valid and reliable measure with excellent test-retest reliability (r = 0.89-0.91). 45 This test was administered to examine changes in paragraph memory from before to after treatment, which would presumably improve with increased visual imagery applied to learning.
The CVLT examines the ability to learn unorganized verbal information. Administration consists of learning a list of 16 words from 4 semantic categories presented orally over 5 trials. Two alternate forms minimize carryover between testing sessions. The CVLT I was used as the third form at long-term follow-up. The CVLT I and II are highly correlated. 46 The dependent variable was the CVLT learning slope across the 5 learning trials. This measure was selected because of its ability to capture the rate of learning over 5 repetitions of the word list. It is this learning ability that the mSMT targets through the application of context and imagery to learn new verbal information, including both lists of words and paragraphs.
Secondary outcomes consisted of (1) an objective evaluation of everyday memory (RBMT), (2) participants’ subjective report of overall functioning and behavioral symptoms associated with cognitive changes in neurological injuries, and (3) significant others’ report of the same cognitive and functional changes.
The RBMT includes memory tasks directly related to everyday aspects of memory functioning, such as practical tasks of remembering a name-photograph association, a hidden belonging, an appointment, a story, faces, and a novel route. Four parallel forms are available; forms A to C were utilized in consecutive order. The RBMT demonstrates good internal consistency, reliability, 47 and construct validity. 48 The RBMT was administered to provide a measure of memory performance on daily life activities.
The FrSBE assesses behaviors associated with neurological illness/injury, with an emphasis on those symptoms associated with the frontal lobes. 49 It consists of 46 items rated on a 5-point scale for 2 time points, before and after the injury, during the 2 weeks prior to testing. Three subscale scores (apathy, disinhibition, and executive dysfunction) comprise the total score. Patient and informant ratings are obtained. Dependent variables were the 4 indices after the injury for self-report and informant report. We chose to administer the FrSBe for several reasons. First, the FrSBe is a measure that has been recommended for use as an outcome measure in TBI research. 50 Second, Karzmark et al 51 reported that the informant version of the FrSBe is a better predictor of daily life functioning than using neuropsychological tests alone in a mixed neurological sample, including individuals with TBI. Reid-Arndt et al 52 further noted that the FrSBe more strongly correlated with measurement of community reentry than neuropsychological tests of executive functioning. Additionally, despite the fact that it was designed as an assessment of executive functioning, it queries the patient and informant about many aspects of daily life that require everyday memory skills (eg, mix up a sequence, get confused when doing several things in a row; make the same mistakes over and over, do not learn from past experience; forget to do things but then remember when prompted or when it is too late; use strategies to remember important things). Finally, the FrSBe is included in the NIHI Common Data Elements and is thus recommended as an outcome measure in clinical trials. 53
The State Trait Anxiety Inventory and Chicago Multi-dimensional Depression Inventory examined changes in emotional functioning following treatment. Changes in emotional functioning have been noted previously following cognitive rehabilitation.35 -41
Statistical Analyses
All participants were included in the analysis per the intend-to-treat design. Data imputation was done via carryover of the most recent testing results. Specifically, 4 participants discontinued participation during the treatment phase (2 treatment and 2 control). Thus, their baseline scores were carried forward to the immediate and long-term follow-up assessments, conservatively estimating no change from baseline scores. Between the immediate and long-term follow-up, 12 participants discontinued participation. Thus, their scores from the immediate follow-up were carried forward to the long-term follow-up. A follow-up sensitivity analysis, utilizing the mean of all participants as the imputed value for each dependent variable (DV), demonstrated similar results.
Analysis examining treatment effects utilized an ANCOVA, with baseline performance and education serving as the covariate in each analysis. All analyses were conducted using raw scores. Data were analyzed with 1-tailed tests because our hypotheses were unidirectional, with no reason to expect that participants would show a decline in performance within a 5-week trial. This approach has been recommended by Ludbrook, 54 who stated that unidirectional tests are preferred to test directional hypotheses when H1 is specified a priori. Because of the designation of coprimary outcome measures, α was reduced to .025 for these analyses. Repeated-measures ANOVA were used to examine long-term treatment effects. Analyses were performed with SPSS version 18 software. No interim data analyses were performed.
Ethics and Registration
All procedures were approved by an institutional review board, and all participants provided written informed consent. The RCT is registered with clinicaltrials.gov (NCT01207375).
Results
Recruitment ran from September 2007 to September 2013, with follow-ups completed in June 2014. The trial ended with completion of external funding. A total of 69 participants with documented moderate to severe TBI were randomly assigned to the treatment (n = 35) or placebo-control group (n = 34). Four participants dropped out of the study between baseline and immediate follow-up (2 from the treatment group and 2 from the control group; 6% attrition). Also, 12 more participants dropped out of the study between immediate and long-term follow-up (9 from the treatment group and 3 from the control group), resulting in a slightly higher attrition rate at this stage (19%). Participants discontinued treatment because of the time commitment and moving out of the geographical region. Analysis was based on an intend-to-treat population (Figure 1), as described in the analyses section.
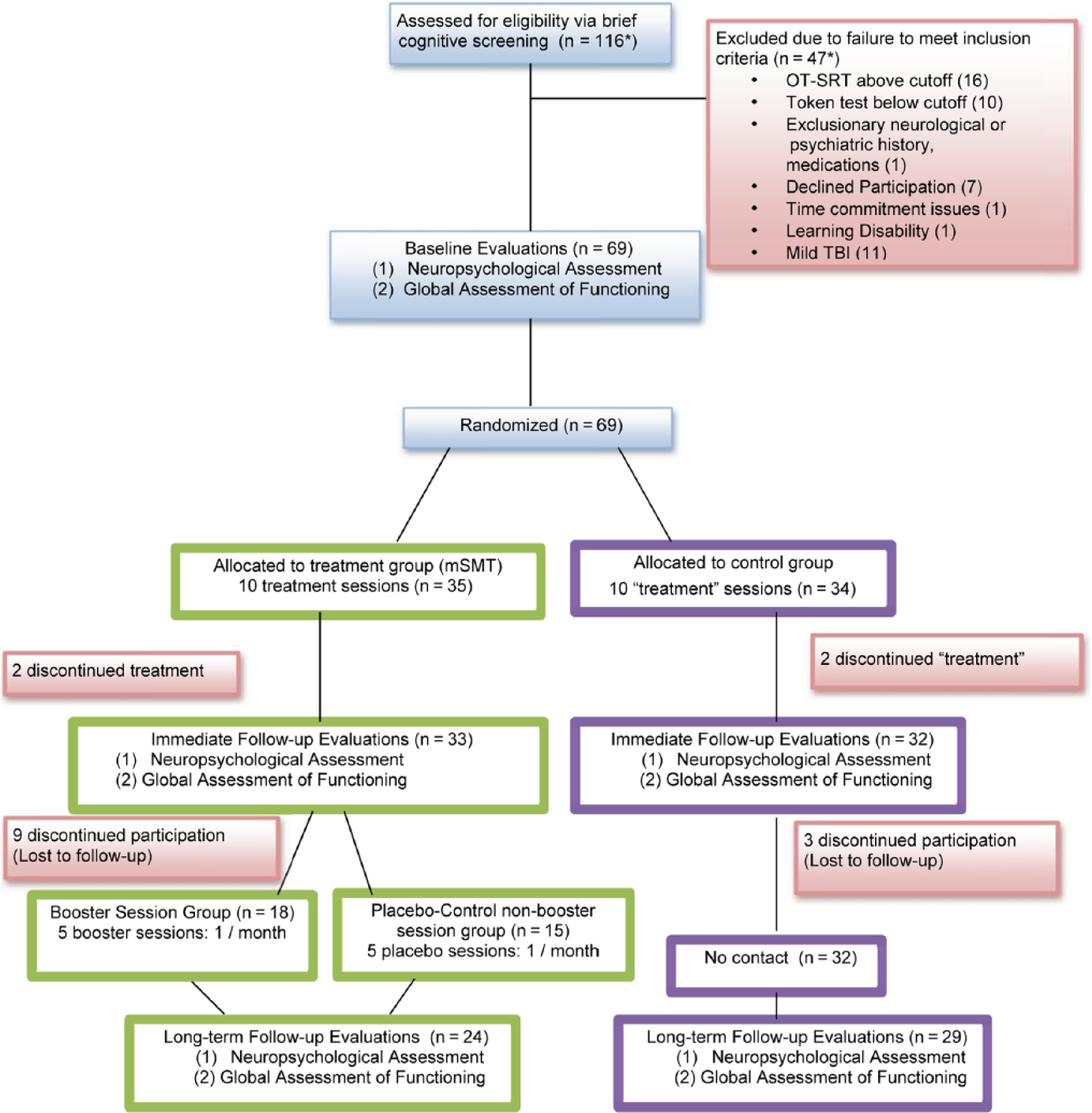
Participant flow.
Treatment Efficacy
Objective NP Performance
There were no significant differences between the groups at baseline on any of the neuropsychological tasks (Table 2).
After controlling for the variance associated with baseline performance on MAS-PM—delayed as well as education—the treatment group showed a significant improvement in prose recall from baseline to follow-up in comparison to the placebo group: F(1, 69) = 4.45, P < .025 1-tailed, partial η2 = 0.064 medium effect; CI = −1.71 to −0.047; Figure 2. The MAS-PM-delayed at baseline [F(1, 69) = 37.28; P < .001; partial η2 = 0.365 large effect] was a significant covariate in the model, whereas education was not [F(1, 69) = 0.046; NS; partial η2 = 0.001 small effect]. No significant treatment effect was noted on the CVLT learning slope [F(1, 69) = 0.686, NS, η2 = 0.011 small effect; CI = −0.154 to 0.373].
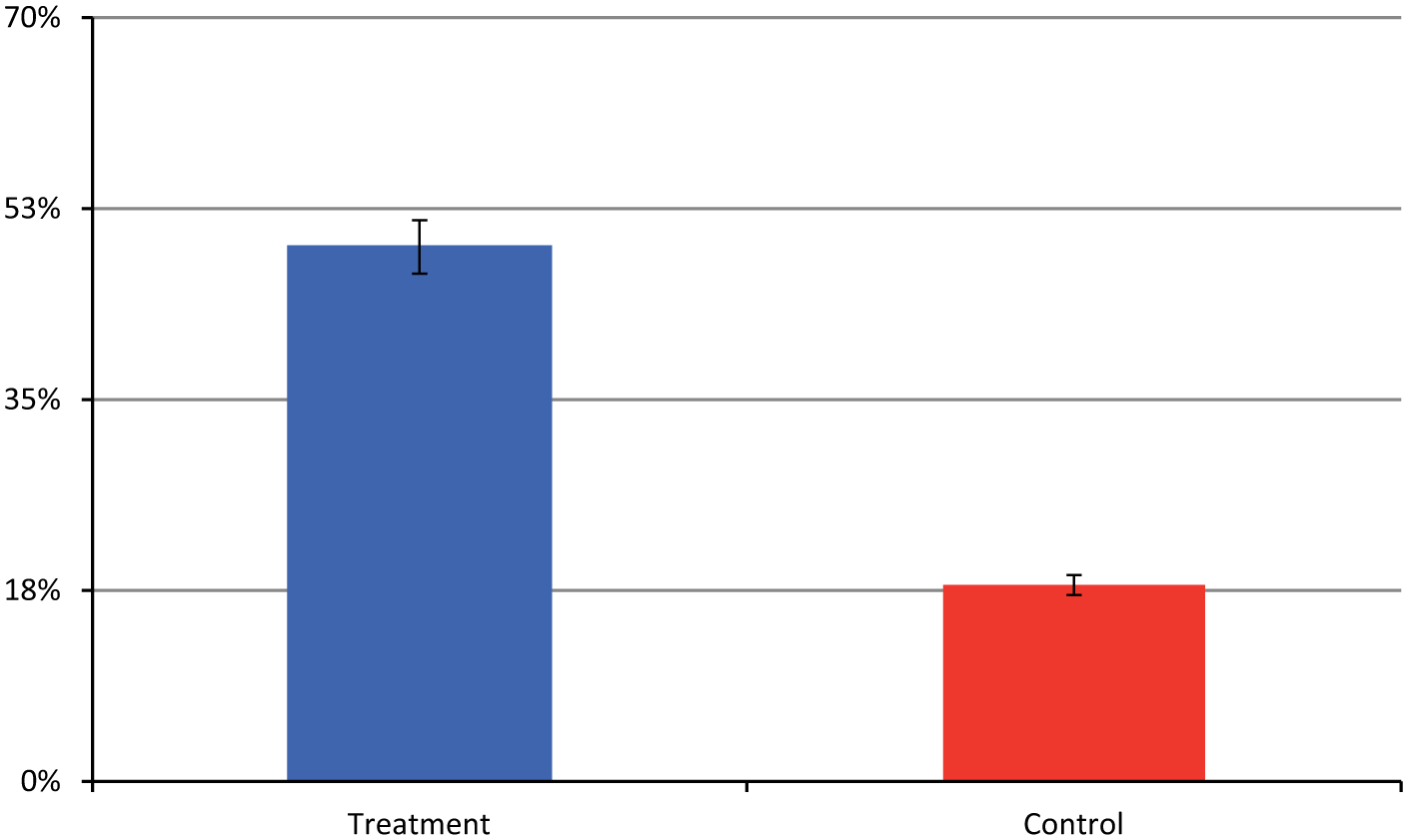
Percentage of participants who improve on Prose Memory Immediate from pretreatment to posttreatment, by group. Error bars are 1 standard error. p=.006
To examine the percentages of participants who benefitted from treatment versus those who did not, a χ2 analysis was conducted. With benefit defined as a 10% or greater improvement on the MAS-PM from baseline to immediate follow-up (consistent with studies of pharmacological agents determined to improve cognition in neurological samples 55 ), 49% of participants in the treatment group showed an improvement compared with only 18% of the control group: χ2(1) = 7.42, P = .006, Cohen’s w = 0.33, medium effect; Figure 2). We also computed the reliable change index using the Jacobson-Truax 56 formula and a 0.90 confidence interval (a 95% chance of true improvement for participants surpassing this threshold) to determine the percentage of participants in the treatment group who positively benefited 57 from treatment. In all, 23% of the treatment group showed a reliable positive change following treatment, compared with only 9% of the control group.
Objective Everyday Memory
A greater percentage of participants in the treatment group demonstrated improvement on the RBMT hidden belonging task at immediate follow-up versus the placebo group: χ2(2) = 7.36, P = .025, Cohen’s w = 0.43; Figure 3. No other significant differences were noted on the RBMT.
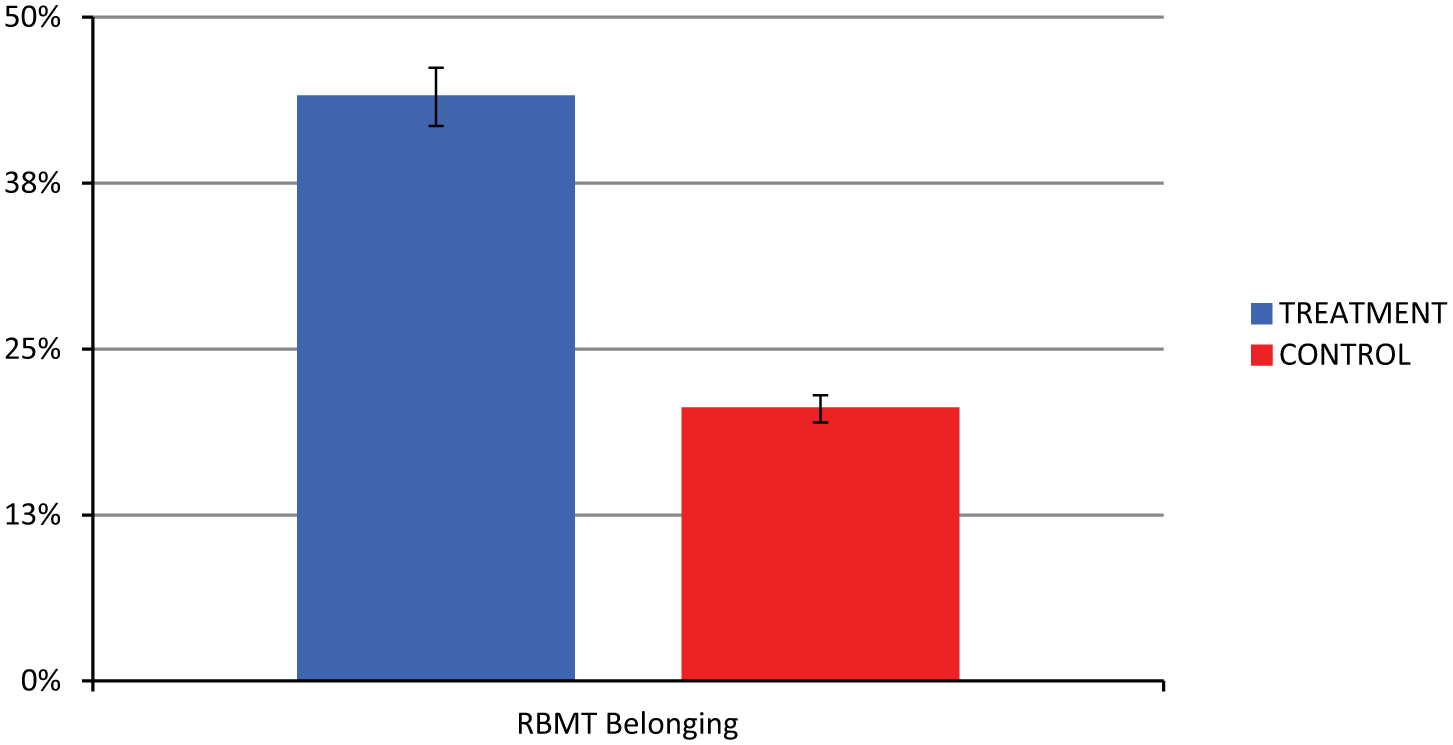
Percentage of participants showing improvement on Rivermead Behavioural Memory Test (RBMT) hidden belonging task posttreatment, by group. p=.025
Subjective Everyday Cognition and Emotion
On the FrSBe, informants reported an improvement in disinhibition from before to after treatment in the treatment group, with no difference noted in the placebo group: ANCOVA F(1, 31) = 6.86, P < .05; η2 = 0.046, medium effect; CI = 0.738 to 6.04). There was no significant difference between the groups at baseline (Table 2). No significant differences were noted from pretreatment to posttreatment between groups on the patient report forms.
There were no significant differences between the groups for depression [F(1, 61) = 0.024; P = NS; η2 = 0, no effect; CI = −12.62 to 14.72] or anxiety [F(1, 57) = .075, P = NS; η2 = 0, no effect; CI = −4.63 to 4.86] from before to after treatment.
Long-Term Effects
Long-term maintenance of treatment for MAS-PM Delayed was analyzed by a 2 (Group: treatment vs control) × 2 (Follow-up: immediate vs 6 months) Repeated Measures (RM) ANOVA with baseline and education included as covariates. The main effects of Group [F(1, 65) = 1.85, P = NS; partial η2 = 0.028] and Follow-up [F(1, 65) = 0.33, P = NS; η2 = 0.005] were not significant. The interaction Group × Follow-up, however, was significant [F(1, 65) = 3.924, P = .052; η2 = 0.057], indicating that the 2 groups performed similarly again after the passage of 6 months.
The 6-month follow-up data for the FrSBe could not be analyzed because of the fact that only 30 participants returned the FrSBe informant form at the 6-month follow-up.
Booster Sessions
Booster session efficacy was analyzed by a 2 (Group: booster vs nonbooster) × 2 (Follow-up interval: immediate vs 6 months) RM ANOVA. On the MAS-PM Delayed Recall, neither the main effects of Group [F(1, 31) = 0.047; P = NS; partial η2 = 0.002] nor Follow-up [F(1, 31) = 0.186; P = NS; partial η2 = 0.006] nor the interaction Group × Follow-up [F(1, 31) = 0.428; P = NS; partial η2 = 0.014] were significant. No adverse or unintended effects of the treatment were noted in any participant.
Discussion
This study provides class I evidence supporting the efficacy of a behavioral memory rehabilitation program for TBI patients, the mSMT. The present trial was based on the finding that impaired memory performance in TBI is primarily a result of impaired initial learning (ie, acquisition). 24 Rehabilitation interventions should, thus, focus on improving the learning deficit to achieve maximal benefit. Evidence has accumulated supporting the efficacy of context and imagery to strengthen learning/acquisition (learning includes the memory processes of encoding and consolidation), resulting in significantly improved retention.30,38 -41,58,59 The current results increase that evidence, demonstrating that training in context and imagery results in significant improvements in verbal learning. Behavioral interventions that specifically target strengthening the acquisition (ie, encoding and consolidation) of information during initial learning can significantly improve memory performance in TBI patients.
Treatment with the mSMT had a positive impact on NP memory tests and measures of everyday functioning. The impact of treatment on the memory tests revealed improvement on the paragraph memory task but not on the list learning task. These 2 tests likely rely on different cognitive processes. That is, to-be-remembered information in the paragraph learning task was preorganized for the participant, whereas to-be-remembered information on the list learning task was disorganized. The list learning task thus requires the participant to organize the information as an initial step during learning. The critical difference between these 2 memory tasks is this requirement of organizational skills. The treatment effect was observed only on the task that did not require organization. The mSMT teaches participants to apply context (or organization) and imagery techniques to facilitate stronger and deeper memory acquisition and improve learning. The divergent pattern of results implies that participants with TBI in the current study successfully applied the imagery component of the mSMT to learn the preorganized paragraph task, but they did not successfully apply context learned in the mSMT to effectively learn the disorganized list. This pattern of results differs from that observed in MS samples 32 where participants were able to utilize both imagery and context to facilitate the acquisition of new information into memory. It is important to note that those with severe learning difficulties in TBI12,24 and other populations, including those with stroke, 60 frontotemporal dementia, 61 and amnesia, 62 often show related deficits in executive control (including organizational abilities). Others have shown that the presence of significant executive dysfunction limits the effectiveness of interventions for severe memory deficits. 12
It is important to note that the treatment effect observed on the NP learning and memory tests extended to an objective test of everyday memory (RBMT) and informant-reported improvements in disinhibition in daily life. The improvements in cognition resulting from treatment with the mSMT are thus associated with improvements in everyday function, truly affecting the patient’s daily life. Of note, the RBMT has multiple subscales, including general orientation questions and facial recognition. The positive effect of treatment was not notable on all subscales of the RBMT. Given the nature of the mSMT instructions, it may be unreasonable to expect treatment to benefit all aspects of everyday memory. It will be necessary for future work to continue to demonstrate how the mSMT treatment generalizes to different tests of everyday memory and how these tests relate to functioning in daily life. Interestingly, the change in daily life reported by informants was noted on the informant disinhibition subtest of the FrSBe. Although one would not have instinctively expected to detect such a change on a disinhibition measure, recent literature points to the relationship between the Informant Disinhibition Scale of the FrSBe and daily life functioning. Specifically, Karzmark et al 51 noted that whereas all the subscales correlated with daily activities, the correlation between the informant FrSBe, Disinhibition Scale, and the Functional Activities Questionnaire was higher (r = 0.36; P < .05). Furthermore, when the FrSBe Informant Disinhibition Scale was included in a regression predicting the Functional Activities Questionnaire, the informant Disinhibition subscale accounted for 7% variance over and above that which was accounted for by neuropsychological assessment. It is, thus, likely that the FrSBe Informant Disinhibition Scale is tapping into an aspect of everyday functioning that is uniquely affected by this mSMT and particularly salient to the informants.
At the 6-month follow-up, the 2 groups were found to again perform similarly on the paragraph learning task. Despite the fact that booster sessions were incorporated into the study protocol to help maintain the treatment effect over time, no effect of booster sessions in maintaining the treatment effect over time was noted. This contrasts with previous work in normal aging demonstrating that booster sessions can be effective in maintaining a treatment effect over time. 63 Potential explanations for this include small sample size (underpowered for this analysis) and less-than-optimal frequency, intensity, or content of the booster sessions. For example, effective booster sessions might focus on the actual skills taught in treatment, with refreshers provided on context and imagery, rather than the practice of applying context and imagery to daily life. The ideal content of and frequency of booster sessions is an important topic for future investigations in an effort to facilitate the maintenance of posttreatment gains in memory abilities over time.
Increasing efforts have been directed toward developing effective memory rehabilitation treatments in TBI.9,11,12,64 These treatments can be classified as either compensatory or restorative. 12 The accumulating evidence seems to support the efficacy of compensatory strategies over restorative strategies, 64 although additional research into the efficacy of restorative strategies is necessary before making absolute claims about the effectiveness of such treatments. Compensatory approaches can be further decomposed into internal and external memory training strategies, that is, utilizing new mnemonic techniques or utilizing peripheral memory aids (eg, a notebook), respectively. 65 Compensatory strategy training has been recommended as a clinical practice standard for treating memory impairment in TBI. 12 The present evidence suggests that the mSMT is a valuable compensatory-internal memory rehabilitation strategy that should be incorporated into the clinical practice standards for treating memory impairment associated with TBI. Furthermore, using internal compensatory treatment strategies may be advantageous over external memory aids. This is because the internal strategy modifies the patient’s approach to acquiring new information and does not require that the patient transports and/or updates an external device.
There are limitations to the current study worth mentioning. First, everyday life cognitive functioning either focused primarily on self-report or encompassed a limited representation of daily life tasks (ie, RBMT). Future studies should focus more on actual everyday life activities. Unfortunately, this limitation exists in much of the cognitive rehabilitation work to date. Second, the sample size for the booster session analyses was small and underpowered and deserves increased attention in future research. In addition, prior history of substance use and to a lesser extent psychiatric history is characteristic of TBI. The current sample, however, had no such history. Thus, the efficacy of the mSMT may be different in a sample with a substance abuse and/or psychiatric history. Additional research might address whether the intervention remains effective with a broader, less-restrictive sample of participants with TBI characteristic of the clinical population. Given the heterogeneity of TBI, future research will also benefit from identifying the role that individual differences play in how patients respond to memory rehabilitation, leading to an individualized approach to cognitive rehabilitation. 66
Based on widely accepted classification systems for treatment study design,67 -69 the present results provide class I evidence supporting the efficacy of the mSMT to improve learning and memory in TBI patients with impaired learning. A treatment effect was documented on standardized NP tests of memory ability, tests of everyday memory abilities, and informant report of everyday cognitive difficulties. Thus, this study extends the evidence for efficacy of the treatment protocol to a sample of people with TBI. Future research should examine the optimal methodology for increasing the maintenance of the treatment effect over time and development of new treatment protocols that can be similarly successful in TBI patients.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Chiaravalloti reports no disclosures. Dr Sandry reports no disclosures. Ms Moore reports no disclosures. Dr DeLuca has served as a consultant for Biogen and Novartis Pharmaceuticals. He also is a journal club speaker for EMD Serono.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this article were developed under the NIDRR Grant H133A070037. However, these contents do not necessarily represent the policy of the Department of Education, and endorsement by the Federal Government should not be assumed.