
Abstract
Poststroke fatigue and limb heaviness are 2 perceptual problems that commonly occur after stroke. Previous work suggests that poststroke fatigue may be related to altered sensorimotor processing whereas limb heaviness is often considered an association of muscle weakness. To address the hypothesis that the perception of limb heaviness may also be a problem of altered sensorimotor control, we investigated whether it was more closely related to poststroke fatigue or muscle weakness. In 69 chronic stroke survivors, we found that those with high perceived limb heaviness (31 individuals) also reported significantly higher levels of fatigue (4.8/7) than those with no perceived limb heaviness (38 individuals, fatigue score = 2.68/7), but there was no difference in weakness between the 2 groups. This intriguing finding is discussed in relation to effort perception and sensory processing. The association between limb heaviness and poststroke fatigue and a dissociation from muscle weakness gives rise to the hypothesis that limb heaviness maybe a centrally arising sensorimotor disorder.
Non–exercise-related, chronic, perceptual fatigue is one of the most commonly reported symptoms after stroke 1 and can be defined as “fatigue is a feeling arising from difficulty in initiation of or sustaining voluntary effort.” It can persist for years, but little is known about its origins. Our recent work showed that those with high poststroke fatigue exhibited low motor cortex excitability 2 and slowed movement times in the affected upper limb. 3 The behavioral deficits associated with fatigue were confined to the affected side. This unilateral rather than generalized slowing of movement supports the idea that the perceptual phenomenon of poststroke fatigue results from focal abnormalities of sensorimotor processing and function. Here, we focus on another perceptual phenomenon commonly reported by stroke survivors—a sense of increased limb heaviness. In healthy individuals, peripheral muscle weakness leads to an overestimation of weight perception. 4 However, here, we hypothesize that limb heaviness after stroke is a problem of central nervous system sensorimotor control and so will be more closely linked to fatigue rather than peripheral muscle weakness. This would argue for both fatigue and sense of limb heaviness after stroke as perceptual manifestations of sensorimotor dysfunction.
Following written informed consent (ethics approval by Riverside Research Ethics Committee 12/LO/1474), 69 stroke survivors (60.36 ± 12.4 years, 20 women, and 56.81 ± 63 months poststroke) with a first-time ischemic or hemorrhagic stroke were recruited via Thames and South East Stroke Research Networks. Stroke survivors on antidepressants or other centrally active drugs, with high levels of motor and/or cognitive impairment, and with high Hospital Anxiety and Depression Scale score (>11) were excluded from the study. High motor impairment was defined as having <60% of the unaffected limb score in more than one of the following measures: (a) Nine Hole Peg Test, (b) Action Research Arm Test, and (c) grip strength. High cognitive impairment was defined as a score of more than 5 on Sustained Attention Index and Symbol Digit Modalities Test. The tests were administered as previously described. 2 As previously used, 2 a motor impairment score was obtained from a principal component analysis of the 3 motor scores. Fatigue was measured using the Fatigue Severity Scale–7 (FSS-7), and limb heaviness was measured by asking participants to either agree/strongly agree or disagree/strongly disagree with the statement, “My limbs can become very heavy.” Participants were instructed to answer the question based on how they felt in the past 2 weeks. A between-group t test was performed on FSS-7 scores and the motor impairment score. The 2 groups were those who agreed/strongly agreed with the statement and those who disagreed/strongly disagreed with the statement. Of the 69 participants, 38 disagreed with the statement, whereas the remaining 31 agreed with the statement (all patients reported heaviness with respect to the affected limb). The average FSS-7 score of those who disagreed with the statement was 2.68 ± 1.54 (mean ± SD) and those who agreed was 4.8 ± 1.53. There was a statistically significant difference between the FSS-7 scores of the 2 groups (P < .001; Figure 1A). There was no significant difference between the motor impairment scores of the 2 groups (Figure 1B).
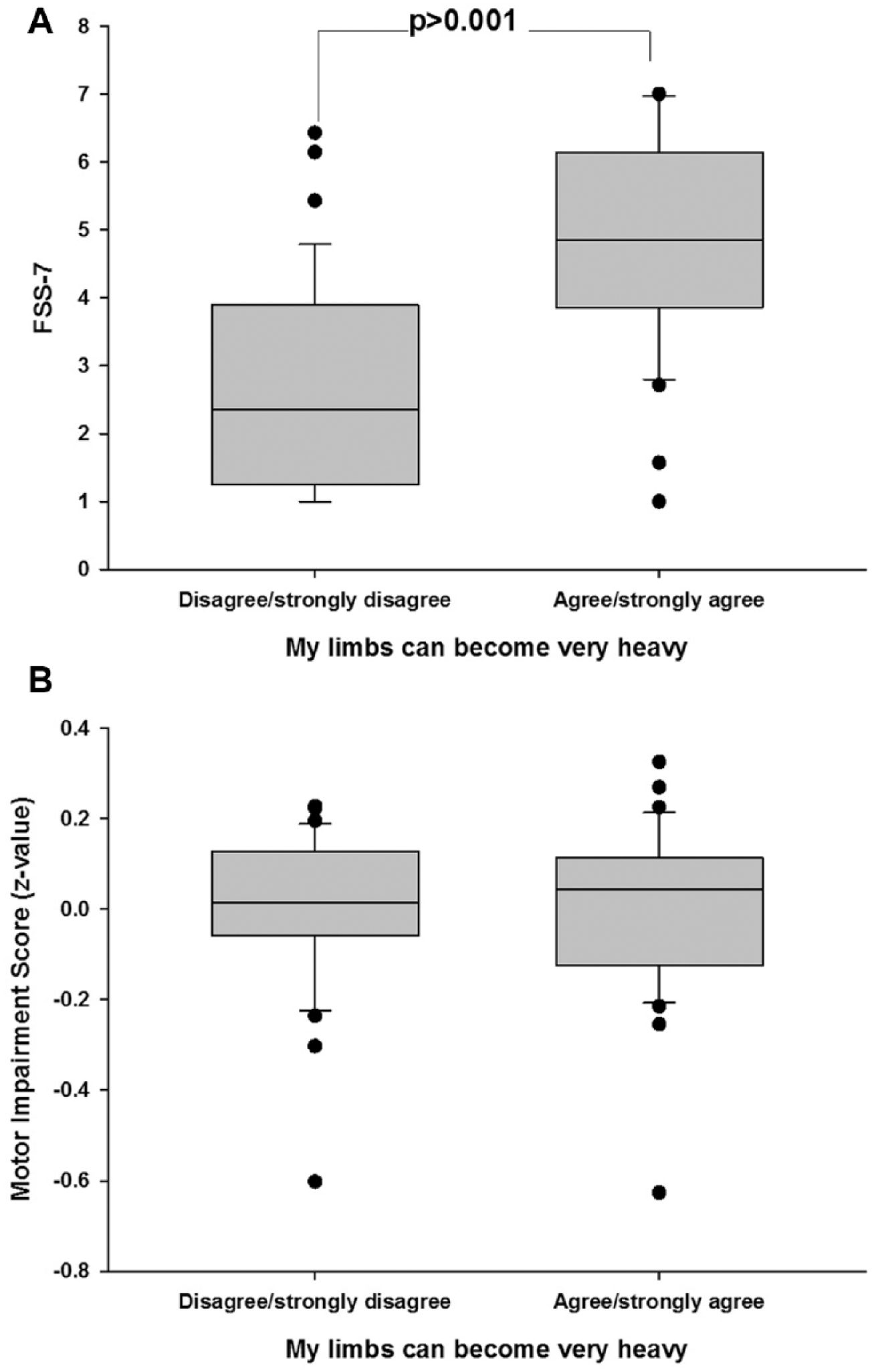
These box and whisker plots show the average fatigue scores (Fatigue Severity Scale [FSS]-7: y-axis) of the 2 groups (1A) and the z-value of the Motor Impairment Score (1B) for the group that disagrees with the statement about limb heaviness and the group that agrees with the statement about limb heaviness.
The main finding of this study is that those who report high fatigue also experience increased limb heaviness. It is important to note that the average motor impairment score, which included both muscle strength and dexterity, was not different between groups. Although limb heaviness is a common complaint of stroke survivors, this is the first study to associate limb heaviness with self-reported fatigue in stroke survivors and dissociate limb heaviness from motor impairment.
Limb heaviness in stroke is commonly thought of as a manifestation of muscle weakness, an idea that emerges from experimental studies in healthy humans. 4 In healthy humans, perceived heaviness of an object placed on a limb is thought to arise from the reafferent activity from the muscle spindles in the contracting muscle fibers. Following repeated contractions or administration of neuromuscular blocks, the peripheral muscle weakens, and more muscle fibers contract when an object is placed on the limb when compared with the preweakened state. This results in increased reafferent activity from the weakened muscles as more muscle fibers are recruited and the individual perceives an object placed on that limb as being heavier. 5 In the current study, although our patients were generally mild to moderately impaired, there was still a range of limb weakness and, therefore, of reafferent activity during maintenance of arm position. However, limb weakness, and therefore presumably reafferent activity, was not related to perceived heaviness. Therefore, one possible explanation for the relationship between fatigue and perception of limb heaviness is that central processing of normal reafferent activity from the peripheral musculature may be altered in those with high poststroke fatigue.
How might limb heaviness be related to effort perception? Effort perception is the ability to assess self-generated force and is thought to arise predominantly from central sensorimotor processing. 6 Effort perception and perceived heaviness can be thought of as 2 sides of the same coin because the former is an assessment of exerted force, whereas the latter is an assessment of experienced force. In this context, it is plausible that the perception of limb heaviness can also be predominantly mediated by central processing and not by afferent information arising from the peripheral musculature.
In summary, we show that limb heaviness, a common symptom after stroke (a) is not related to muscle weakness and (b) is closely related to poststroke fatigue
Poststroke fatigue is commonly looked on as a neuropsychiatric symptom, 7 yet pharmacological interventions have proved futile,8,9 and there are no definitive treatments for fatigue. 10 The present work taken together with our previous work2,3 suggests that changes within the sensorimotor system are more closely linked to development of non–exercise-related poststroke fatigue than previously thought. We also propose a novel mechanism of poststroke fatigue, which requires further testing.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stroke Association TSA SRTF 2012/01.