
Abstract
Objective. To determine which single or combined upper limb muscles as defined by the International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI); upper extremity motor score (UEMS) and the Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP), best predict upper limb function and independence in activities of daily living (ADLs) and to assess the predictive value of qualitative grasp movements (QlG) on upper limb function in individuals with acute tetraplegia. Method. As part of a Europe-wide, prospective, longitudinal, multicenter study ISNCSCI, GRASSP, and Spinal Cord Independence Measure (SCIM III) scores were recorded at 1 and 6 months after SCI. For prediction of upper limb function and ADLs, a logistic regression model and unbiased recursive partitioning conditional inference tree (URP-CTREE) were used. Results. Logistic regression and URP-CTREE revealed that a combination of ISNCSCI and GRASSP muscles (to a maximum of 4) demonstrated the best prediction (specificity and sensitivity ranged from 81.8% to 96.0%) of upper limb function and identified homogenous outcome cohorts at 6 months. The URP-CTREE model with the QlG predictors for upper limb function showed similar results. Conclusion. Prediction of upper limb function can be achieved through a combination of defined, specific upper limb muscles assessed in the ISNCSCI and GRASSP. A combination of a limited number of proximal and distal muscles along with an assessment of grasping movements can be applied for clinical decision making for rehabilitation interventions and clinical trials.
Keywords
Introduction
The neurological examination of individuals with spinal cord injury (SCI) is usually performed according to the International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI), 1 which is considered the gold standard to determine the levels of injury and to classify the severity of injury. The upper extremity motor score (UEMS, Table 1), a component of the ISNCSCI, is often used in clinical research to examine the course of spontaneous neurological recovery.2-5 However, the UEMS is limited to the assessment of only 5 key muscle groups for each upper limb in cervical SCI. Furthermore, individuals with cervical SCI show a high variability in motor recovery4,6-8 following acute injury. Therefore, the sensitivity of the UEMS is limited for both the prediction and measurement of a therapeutic benefit (ie, suffering from floor and ceiling effects). Accordingly, the ISNCSCI worksheet was recently updated 9 with the description of additional nonkey muscle functions for the upper and lower extremities although their sensitivity of prediction and responsiveness has not yet been analyzed.
Abbreviations.
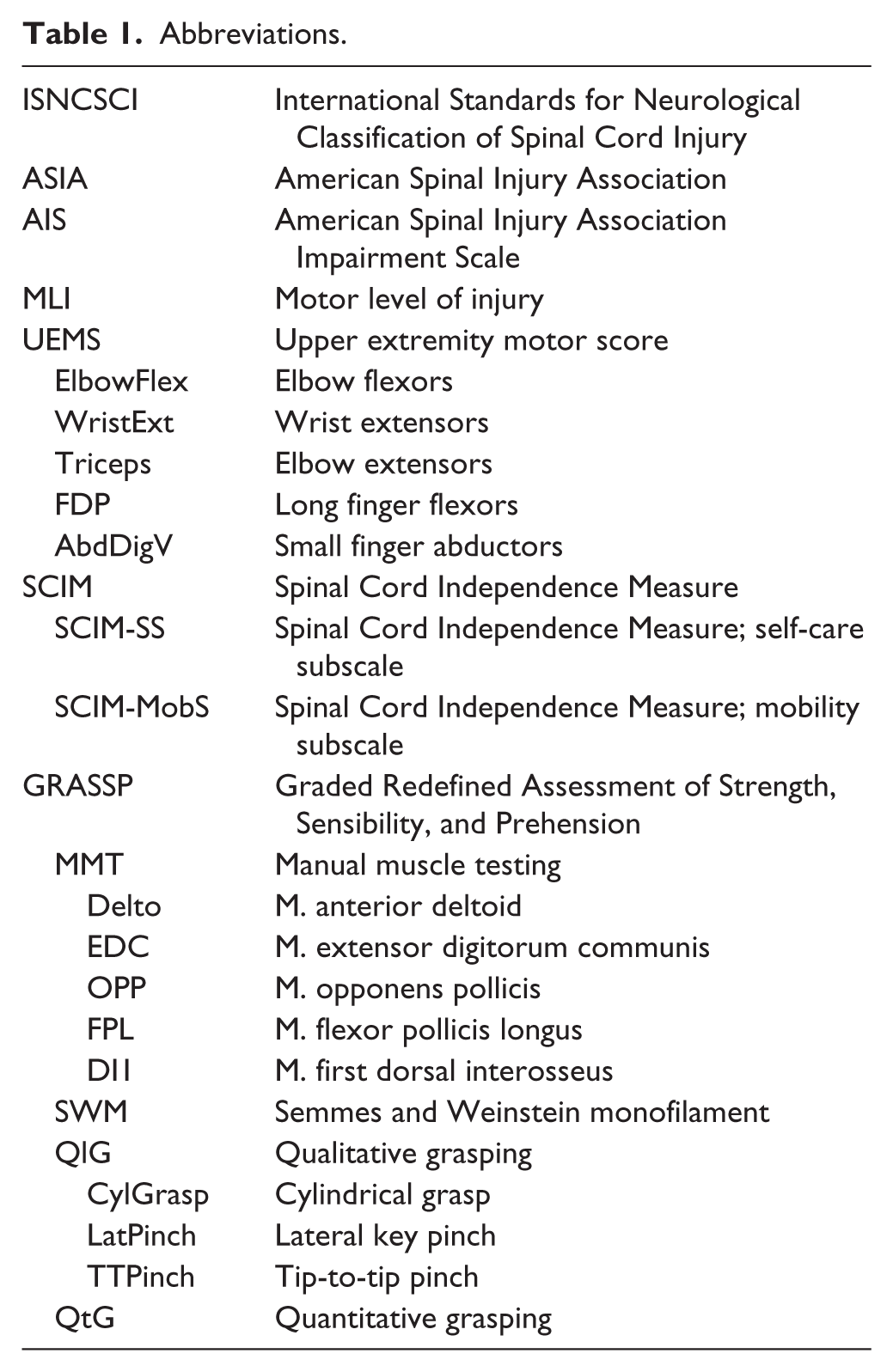
With the intention of providing more sensitive and accurate assessments of upper limb recovery in cervical SCI, the Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) was developed by an international research group. 10 The GRASSP has strong potential to improve the current clinical assessments of upper limb function6,11 since it consists of different comprehensive subtests (ie, assesses an increased number of upper limb muscles) and has demonstrated excellent psychometric properties.6,12
In recent years, there have been several investigations into the prediction of functional outcomes after SCI,13-16 increasing our knowledge of recovery and prediction of upper limb function and self-care after cervical SCI.6,7,17,18 The GRASSP allows the precise identification of recovery profiles 6 and accurately predicts upper limb function and self-care in acute tetraplegia. 7
The GRASSP strength subtest assesses 10 muscles, of which 5 are also measured in ISNCSCI-UEMS (please see Table 2). The number of muscles to be tested should be kept to a minimum and should only include muscles that are useful in the clinical setting and for research in order to optimize time resources. However, there is insufficient evidence regarding the influence of each individual muscle or muscle group on the prediction of upper limb function and activities of daily living (ADLs). Furthermore, the significance of specific grasp movements presenting early after injury and their potential predictive value for functional outcomes has not been studied so far. These specific grasp movements represent complex outcomes (ie, combined sensory and motor outputs) that may classify impairment and neurological deficit of the hand more comprehensively than isolated motor and sensory scores. This prospective study on acute cervical SCI up to 6 months thus addressed 2 aims; first, to determine which single or combined upper limb muscles as defined by the ISNCSCI-UEMS and the GRASSP, best predict upper limb function and independence in ADLs, and second, to assess the predictive value of qualitative grasp movements (QlG) on upper limb function.
Key Muscle Groups or Muscles of ISNCSCI and GRASSP. a
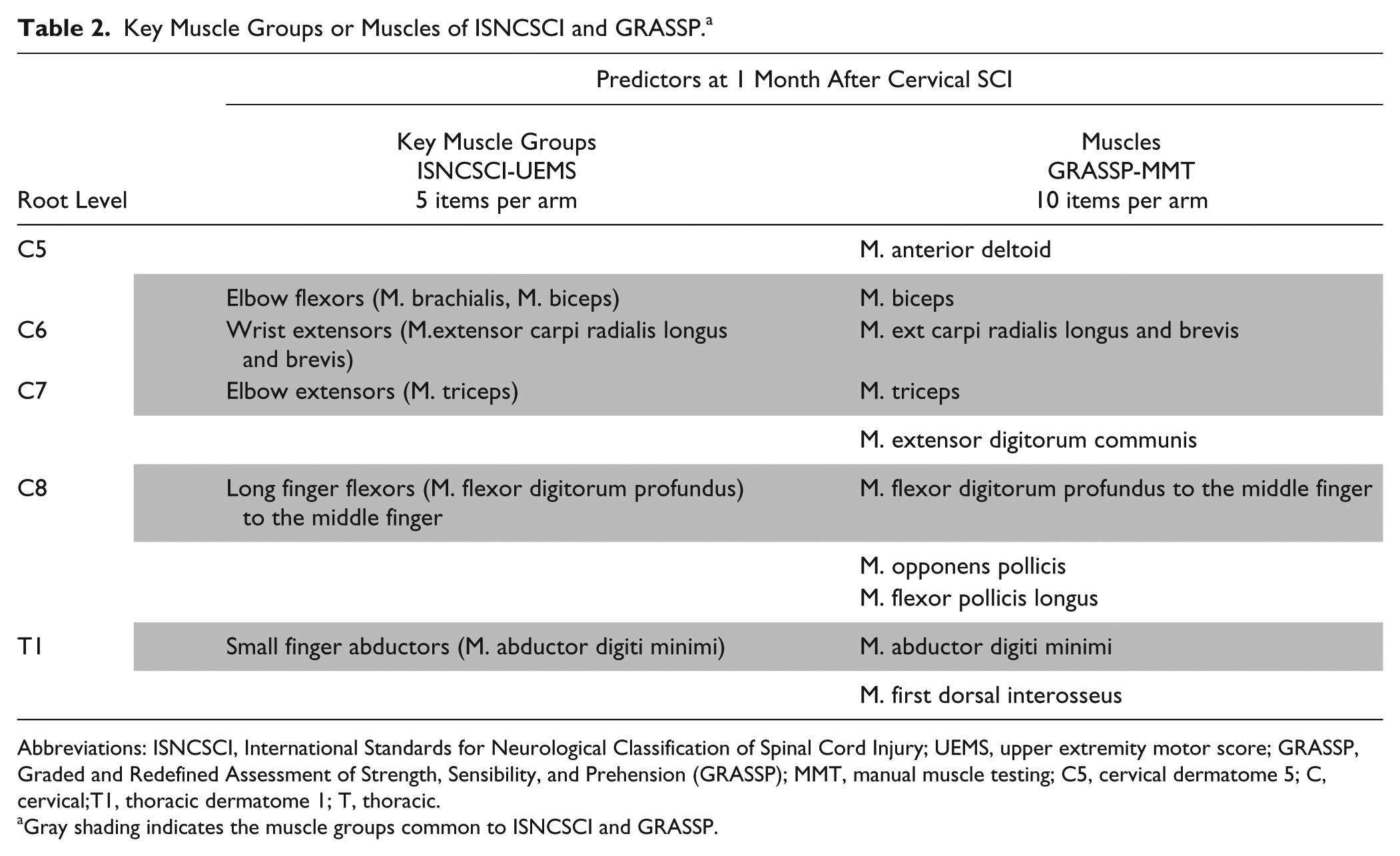
Abbreviations: ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; UEMS, upper extremity motor score; GRASSP, Graded and Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP); MMT, manual muscle testing; C5, cervical dermatome 5; C, cervical;T1, thoracic dermatome 1; T, thoracic.
Gray shading indicates the muscle groups common to ISNCSCI and GRASSP.
Methods
Study Design
This is a European prospective longitudinal multicenter study.
Study Population
Individuals with acute tetraplegia were prospectively enrolled in 5 European SCI centers from 2009 to 2012. Individuals were included if they had sustained a traumatic or nontraumatic acute (16-40 days after injury) cervical SCI as defined by the protocol of the American Spinal Injury Association (ASIA) 1 and suffered from any Impairment Scale (AIS) grade of A, B, C, or D. Participants with high cervical lesions, continuous complete ventilator dependency and complete loss of upper limb control were excluded. Participants were also excluded if they had any accompanying severe neurological disorder (eg, traumatic brain injury), any additional cause of upper limb impairment or were younger than 16 years. The study was approved by relevant authorities at all sites and written informed consent was obtained from all participants.
Clinical Assessments and Procedures
The main clinical measures included the ISNCSCI, GRASSP and the Spinal Cord Independence Measure (SCIM).
The clinical neurological examination was performed according to the ISNCSCI protocol, 1 which is the gold standard to determine the levels of injury and to classify the severity of the injury. This article focuses on subcomponents of the ISNCSCI, the UEMS, the motor level of injury (MLI) and AIS.
The GRASSP is a comprehensive measure of upper limb function with motor (manual muscle testing [MMT]), sensory (Semmes and Weinstein monofilament [SWM]), qualitative grasping (QlG) and quantitative grasping (QtG) subtests. The right and left sides are tested separately. The subtests and items within subtests can be evaluated separately or as summed scores. The GRASSP is a relatively new tool, which is being used more and more commonly in clinical research of cervical SCI. and has excellent psychometric properties.6,12 More details about the GRASSP version 1.0 are described elsewhere.6,7
The SCIM III is a global measure of function which assesses independence in fundamental daily activities specific to individuals with SCI. 19 The SCIM III consists of 3 subcategories: (a) self-care (SCIM-SS), (b) respiration and sphincter management, and (c) mobility (SCIM-MobS). The SCIM III has been shown to perform well under psychometric testing.20-22
Rehabilitation physicians trained on the ISNCSCI protocol performed the neurological examination and occupational therapists conducted the GRASSP at 1 month (range = 16-40 days) and 6 months (range = 150-186 days) after cervical SCI. All occupational therapists involved in data collection had at least 1 year of experience in working with individuals with SCI and had successfully completed competency training on how to perform the outcome measure assessments. Experienced physical therapists, nurses, and occupational therapists obtained SCIM III data at 6 months (range = 150-186 days) after cervical SCI. In addition, a standard protocol, outlining in detail how the assessments should be performed, was provided for each outcome measure with standardised recording techniques and materials across all centers.
Predictor Variables
The following baseline variables (assessed between day 16 and 40 after cervical SCI) were selected as predictors: INSCSCI-AIS, INSCSCI-MLI, ISNCSCI–UEMS, GRASSP–MMT and GRASSP-QlG.
ISNCSCI-UEMS
The ISNCSCI upper limb strength measurement consists of five key muscle groups. Each muscle group is scored from 0 (completely paralysed muscle) to 5 (active movement and a full range of movement against maximum resistance) for each arm.
GRASSP-MMT
GRASSP strength measurement consists of ten muscles. Each muscle is scored from 0 (completely paralyzed muscle) to 5 (active movement and a full range of movement against maximum resistance) for each arm. For this study, the five muscles which are also assessed in the UEMS were excluded from analysis. The five remaining muscles were selected as predictors. For more details regarding the ISNCSCI and GRASSP predictor variables, please see Table 2.
GRASSP-QlG
The ability to perform movements of the hand and fingers as they relate to a cylindrical grasp (CylGrasp), lateral key pinch (LatPinch), and tip-to-tip pinch (TTpinch) is assessed for each hand separately. Each grasp is scored from 0 (no voluntary control of wrist and digits when grasping) to 4 (normal voluntary movement control of wrist and digits when generating the grasp).
INSCSCI-AIS and INSCSCI-MLI
The AIS classifications were calculated using a computer algorithm 23 in accordance with the definitions in the ISNCSCI. 1 As described in the ISNCSCI, the motor level is defined as the most caudal spinal segment, as indexed by the key muscle group for that segment, having a muscle strength score of at least 3/5 (full range contraction against gravity alone) while all the more rostral key muscles are normal (5/5). The MLI was split in 3 subgroups: (a) C1-C4, (b) C5-C6, and (c) C7-T1.
Outcome Variables
The appreciation of upper limb function was distinguished into different domains like the quantitative capacity of each single hand to accomplish defined grasping tasks (QtG) and defined measures of independence in activities of daily life (SCIM items). All the outcome variables were assessed at 6 months (range = 150-186 days) after injury.
GRASSP-QtG
The GRASSP subtest QtG reflects upper limb function based on quantitative measures of grasp performance. Six prehension tasks were performed in a standardised way. Each task is graded from 0 (the task cannot be conducted at all) to 5 (the task is conducted without difficulties using the expected grasping pattern and upper limb function is unaffected) for each arm according to the grasp used and completeness of the task within 75 seconds. The scores of the 6 tasks were added, giving a maximum possible QtG subtest score of 30 points for each side. The scoring was performed according to the GRASSP protocol.
SCIM III
The SCIM-SS and SCIM-MobS were selected as outcome variables because these subcategories have items predominantly related to the use of the upper limb (transfers, wheelchair mobility, grooming etc.) and reflect upper limb performance. 24 The sum of the SCIM-SS ranges from 0 to 20 points. The SCIM-MobS is the sum of the SCIM mobility subcategory minus the score for the “stair” item. The sum of this SCIM-MobS therefore ranges from 0 to 37 points.
Data Analyses
Descriptive statistics were used to determine the frequency, mean, and range of the study individuals’ characteristics including AIS grade, motor level, gender, and age.
Backward multiple binary logistic regression was performed to identify the muscle and muscle group variables that show the greatest effect on the prediction of the dichotomized outcomes QtG, SCIM-SS and SCIM-MobS. The following 5 ISNCSCI-UEMS muscle group predictors were investigated for each arm: elbow flexors (ElbowFlex), wrist extensors (WristExt), elbow extensors (Triceps), long finger flexors (FDP), and small finger abductors (AbdDigV). The five GRASSP single muscle predictors that are not included in the UEMS muscle groups were investigated in this study: M. anterior deltoid (Delto), M. extensor digitorum communis (EDC), M. opponens pollicis (Opp), M. flexor pollicis longus (FPL) and M. first dorsal intersosseus (DI1) (please see Table 1. and Table 2. for details). Ten muscles or muscle group predictor variables were therefore included in the model and were subsequently eliminated in a backward stepwise regression method using the likelihood ratio test.
Sensitivity and specificity were calculated from classification tables with 95% confidence intervals (CIs), to investigate the predictive accuracy of the full and reduced model.
Dichotomization of the QtG and SCIM-SS was based on known cutoff values described elsewhere. 7 Briefly, for the unilateral QtG outcome, individuals were allocated to the success group (19-30 points) if they were able to complete the task using the standard grasp, irrespective of any difficulties while performing the task. All other individuals with scores less than 19 points were allocated to the failure group. A cutoff SCIM-SS score of 12 was applied, with scores of 0 to 12 points defined as dependent (failure), and scores from 13 to 20 as independent (success). Dichotomization of the SCIM-MobS was based on those items that characterized that individuals would need total or partial assistance and/or adaptive devices in mobility activities and are referred to as dependent in mobility (failure) while the other group consisted of individuals that are referred to as independent (success) in mobility. A SCIM-MobS score from 0 to 12 points was therefore defined as failure, and a score from 13 to 37 was defined as success.
Furthermore, we based our analysis on a flexible tree-structured regression model from the family of unbiased recursive partitioning methods called conditional inference tree (URP-CTREE), 25 which is an unbiased technique to directly identify homogenous subgroups without compromising prediction accuracy in SCI.7,26 We generated classification trees for the outcomes QtG, SCIM-SS, and SCIM-MobS at 6 months using the same 10 muscle and muscle group predictors as described under the logistic regression section, assessed at 1 month after cervical SCI. In addition to the 10 muscle predictors the 2 ISNCSCI predictors AIS and MLI were entered in the model. URP-CTREE does not assume linear dependence between predictors and outcomes, and it specifically puts the modelling focus on interactions between predictors. Each decision in the classification tree is based on the singular most significant predictor, and the splits are set as to maximize discrepancy between the groups subsequently formed. The tree stops growing when there is no longer any significant predictor. The same statistics were performed for each hand with the three QlG predictors: CylGrasp, LatPinch, and TTpinch.
For the unilateral QtG (30 points maximum sum score) outcome variable, the unilateral predictor variable scores (ordinal range from 0 to 5 for strength and 0 to 4 for QlG) were used in the analysis. For the SCIM-SS (20 points maximum summed score) and SCIM-MobS (maximum summed score 37 points) outcome variables, the right and left predictor variables were combined, giving a bilateral predictor variable score (10 points maximum sum score).
All data were analyzed using SPSS (IBM Corp) version 18.0 for Windows and the computing environment R 27 version 2.14.0 for Windows, which is based on the package “party: a laboratory for recursive partitioning.” 28
Results
Study Population
A total of 61 individuals with cervical SCI were enrolled in the study. For 4 individuals, no QtG data was available at 6 months and therefore a total of 57 individuals (n = 114 arms) were included for the GRASSP outcome QtG and 61 individuals for the SCIM-SS and SCIM-MobS outcomes. The mean ± SD age of the included participants was 47 ± 19 years (range 18-81 years) and 45 (73.8%) of the individuals were male. Detailed cohort characteristics are presented in Table 3.
Demographic and Clinical Characteristics of Participants (n = 61).
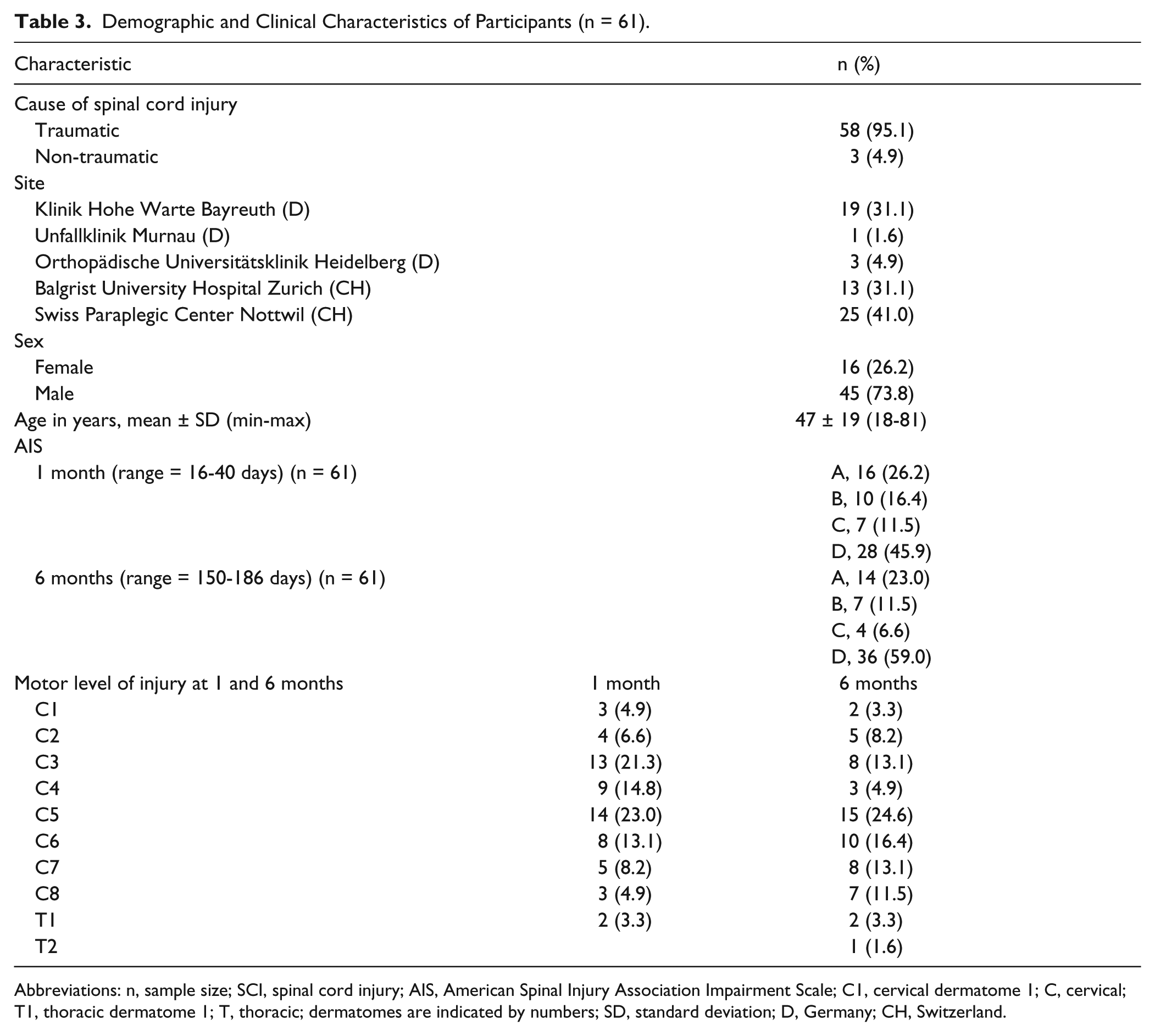
Abbreviations: n, sample size; SCI, spinal cord injury; AIS, American Spinal Injury Association Impairment Scale; C1, cervical dermatome 1; C, cervical; T1, thoracic dermatome 1; T, thoracic; dermatomes are indicated by numbers; SD, standard deviation; D, Germany; CH, Switzerland.
Logistic Regression
Completion of logistic regression analyses based on the previous defined binary outcome variables (see Methods section) in general revealed that the best statistical models did not reduce prediction accuracy (represented by the high sensitivity and specificity levels) compared with the full model with 10 muscle predictors included. The observed predictions for the full and reduced models are presented in Table 4.
Classification Table Logistic Regression. a
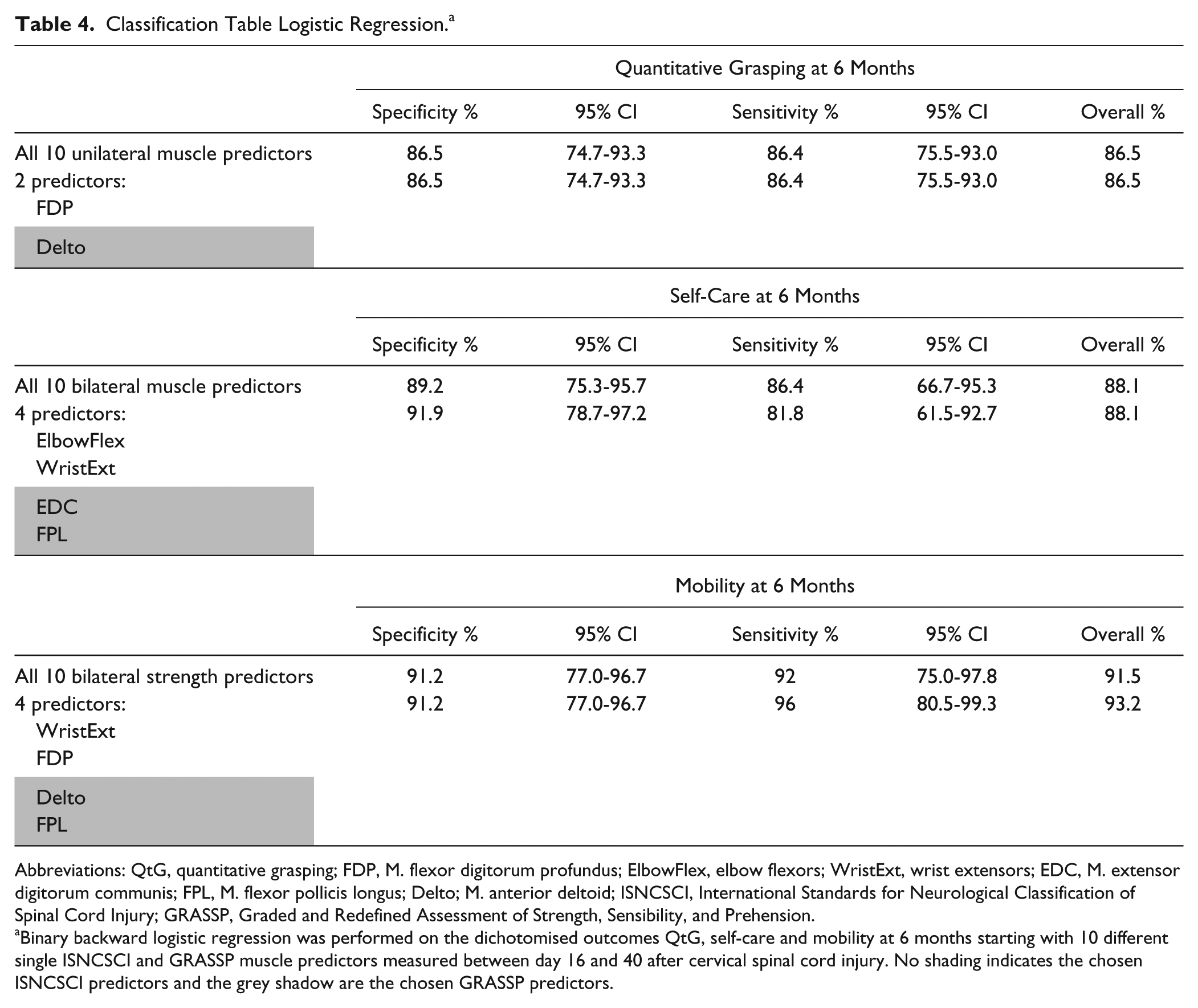
Abbreviations: QtG, quantitative grasping; FDP, M. flexor digitorum profundus; ElbowFlex, elbow flexors; WristExt, wrist extensors; EDC, M. extensor digitorum communis; FPL, M. flexor pollicis longus; Delto; M. anterior deltoid; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; GRASSP, Graded and Redefined Assessment of Strength, Sensibility, and Prehension.
Binary backward logistic regression was performed on the dichotomised outcomes QtG, self-care and mobility at 6 months starting with 10 different single ISNCSCI and GRASSP muscle predictors measured between day 16 and 40 after cervical spinal cord injury. No shading indicates the chosen ISNCSCI predictors and the grey shadow are the chosen GRASSP predictors.
Backward logistic regression identified the combination of ISNCSCI-FDP (P < .0001) and GRASSP-Delto (P < .014) as the best statistical model for binary outcome in QtG. For the prediction of the SCIM-SS in categorizing individuals as dependent or independent in self-care, the combination of 2 ISNCSCI muscle predictors (ElbowFlex, P < .0001; WristExt, P < .027) and 2 GRASSP muscle predictors (EDC, P < .028; FPL, P < .001) was found as the most accurate prediction model. The combination of 2 ISNCSCI muscle predictors (WristExt, P < .047; FDP, P < .065) and 2 GRASSP muscle predictors (Delto, P < .006; FPL, P < .008) resulted in the best model for binary outcome in SCIM-MobS.
URP-CTREE
Figure 1A and 1B and Figures 2 and 3 show the results of the URP-CTREE for the outcomes QtG, SCIM-SS, and SCIM-MobS at 6 months after cervical SCI.
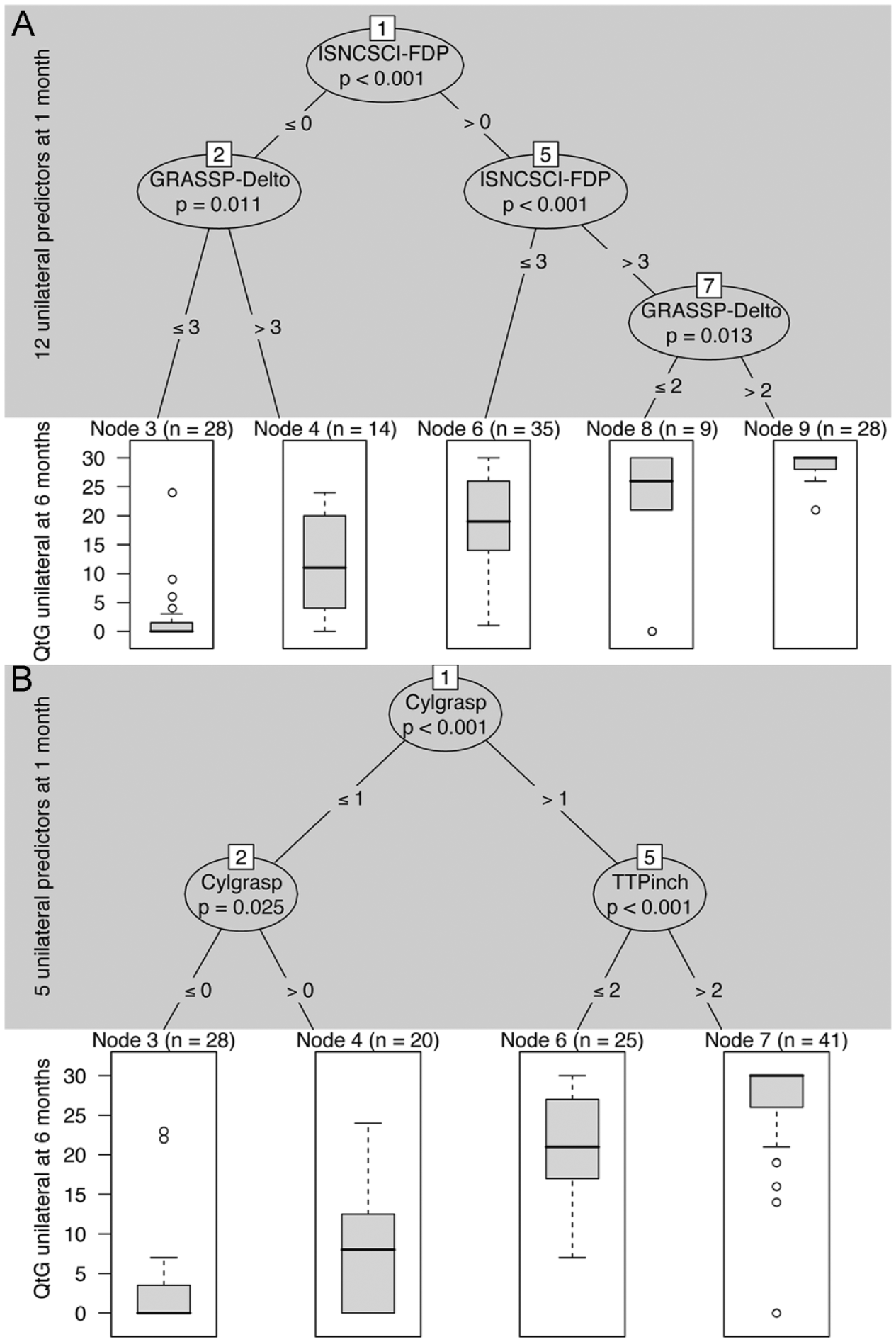
(A) Unbiased recursive partitioning conditional inference tree (URP-CTREE) for quantitative grasping (QtG) at 6 months starting with 10 different single unilateral ISNCSCI and GRASSP muscle predictors and 2 unilateral ISNCSCI predictors AIS and MLI measured between day 16 and day 40 after cervical spinal cord injury. (A) The algorithm led to a partition of the initial cervical SCI cohort into 5 subgroups, which are represented as terminal nodes. Node size (number of arms) is indicated above each terminal node. From left to right, the terminal nodes represent subgroups from low (least favorable) to high (most favorable) quantitative grasping outcome at 6 months. The ISNCSCI-FDP was selected as the first unilateral predictor variable (P < .001) and split the cohort into 2 newly formed subgroups. The initial ISNCSCI-FDP cutoff values ≤0 or >0 are indicated at the “branches.” At each branch, a multiple-testing-adjusted P value is given, which describes the strength of the statistical association between predictor and outcome variable. Further separation is achieved by GRASSP-Delto for participants with ≤0 ISNCSCI-FDP and by ISNCSCI-FDP and GRASSP-Opp for participants with >0 ISNCSCI-FDP. (B) Unbiased recursive partitioning conditional inference tree (URP-CTREE) for quantitative grasping (QtG) at 6 months starting with 3 single unilateral GRASSP qualitative grasping (QlG) predictors and 2 unilateral ISNCSCI predictors AIS and MLI measured between day 16 and day 40 after cervical spinal cord injury. (B) As the interpretations of Figure 1A and 1B are analogous, we refer readers to the explanatory notes for “A” for more details. QtG, quantitative grasping; QlG, qualitative grasping; n, arms; P, significance level; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; AIS, American Spinal Injury Association Impairment Scale; MLI, motor level of injury; GRASSP, Graded and Redefined Assessment of Strength, Sensibility, and Prehension; FDP, M. flexor digitorum profundus; Delto, M. anterior deltoid; Opp, M. opponens pollicis; QualCyl, cylindrical grasp; TTpinch, tip-to-tip pinch.
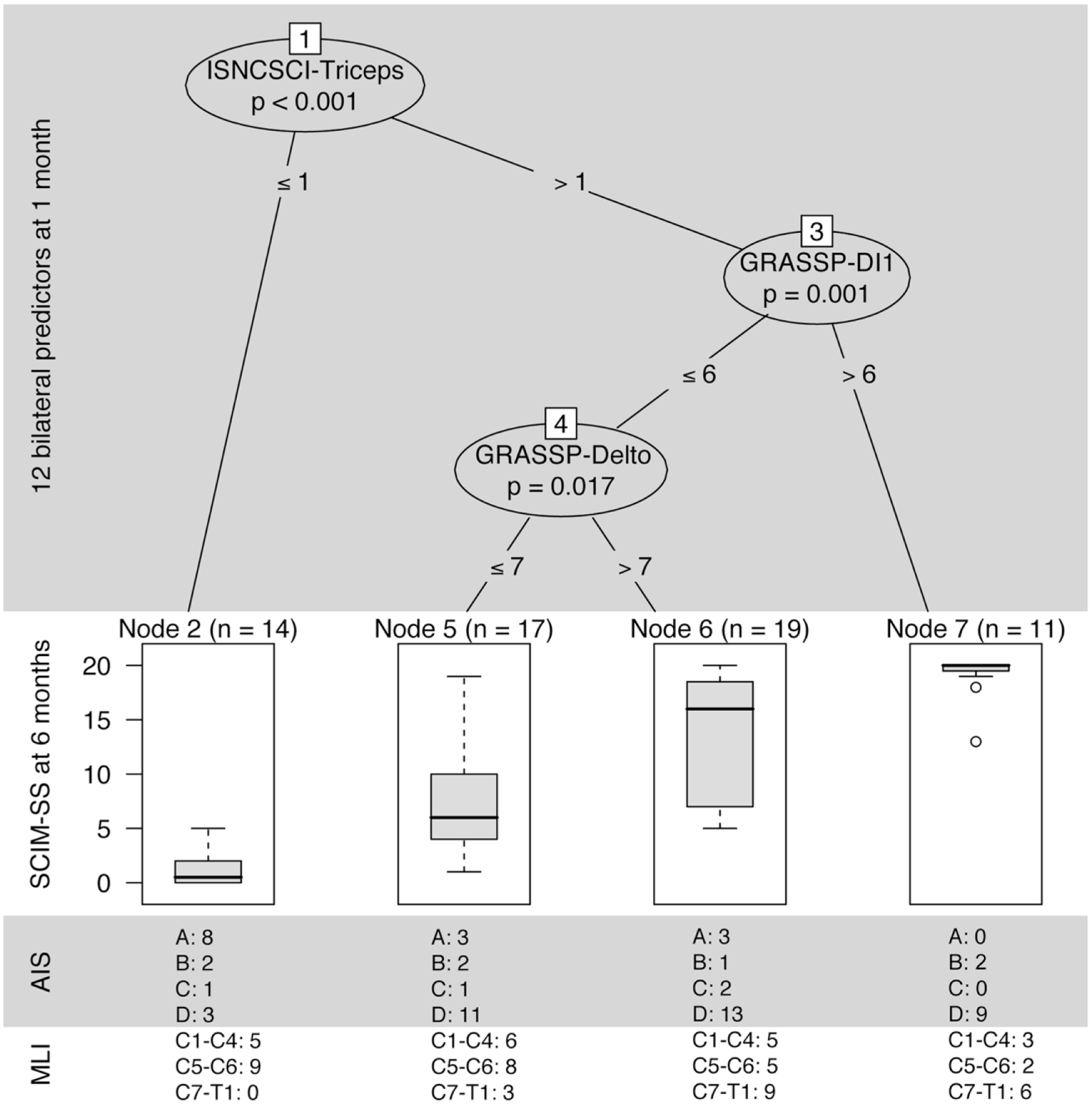
Unbiased recursive partitioning conditional inference tree (URP-CTREE) for self-care at 6 months starting with 10 different single bilateral ISNCSCI and GRASSP muscle predictors and 2 bilateral ISNCSCI predictors AIS and MLI measured between day 16 and day 40 after cervical spinal cord injury. The algorithm led to a partition of the initial cervical SCI cohort into 4 subgroups, which are represented as terminal nodes. Node size (subgroups sample size) is indicated above each terminal node. From left to right, the terminal nodes represent subgroups from low (least favorable) to high (most favorable) self-care outcome at 6 months. The ISNCSCI-Triceps was selected as the first bilateral predictor variable (P < .001) and split the cohort into one newly formed subgroup. The initial ISNCSCI-Triceps cutoff values ≤1 or >1 are indicated at the “branches.” At each branch, a multiple-testing-adjusted P value is given, which describes the strength of the statistical association between predictor and outcome variable. Below the ISNCSCI-Triceps cutoff ≤1, no further separation is achieved, and the next separation is achieved by GRASSP-DI1 and GRASSP-Delto for participants with >1 ISNCSCI-Triceps. n, sample size; P, significance level; SCIM-SS, spinal cord independence measure: self-care subscale; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; AIS, American Spinal Injury Association Impairment Scale; MLI, motor level of injury; GRASSP, Graded and Redefined Assessment of Strength, Sensibility, and Prehension; DI1, M. first dorsal interosseous; Delto, M. anterior deltoid; C, cervical dermatome; T, thoracic dermatome.
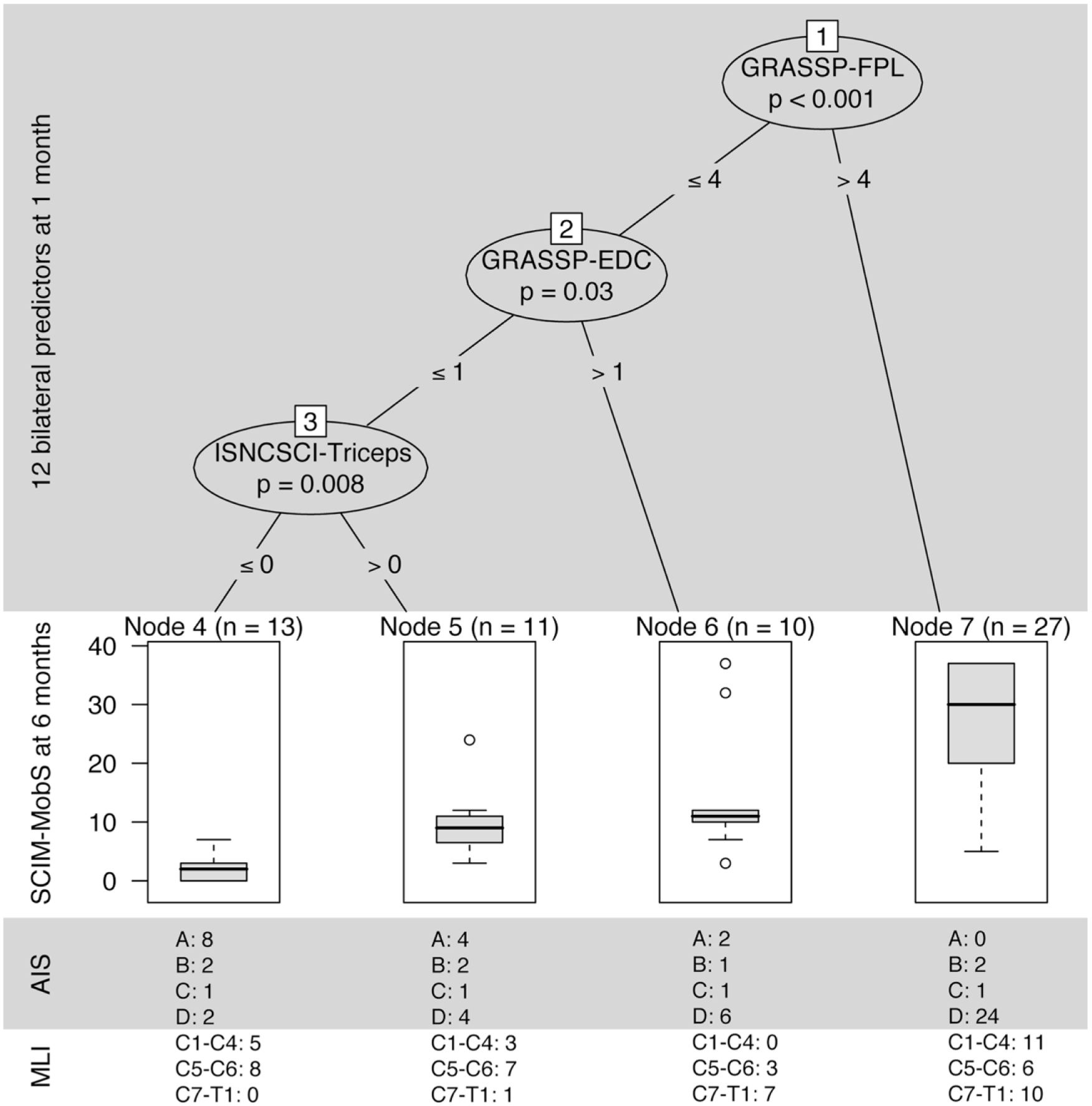
Unbiased recursive partitioning conditional inference tree (URP-CTREE) for mobility at 6 months starting with 10 different single bilateral ISNCSCI and GRASSP muscle predictors and 2 bilateral ISNCSCI predictors AIS and MLI measured between day 16 and day 40 after cervical spinal cord injury. As the interpretations of Figures 2 and 3 are analogous, we refer readers to the explanatory notes for “Figure 2” for more details. n, sample size; p, significance level; SCIM-MobS, Spinal Cord Independence Measure: mobility subscale; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; AIS, American Spinal Injury Association Impairment Scale; MLI, motor level of injury; GRASSP, Graded and Redefined Assessment of Strength, Sensibility, and Prehension; FPL, M. flexor pollicis longus; EDC, M. extensor digitorum communis; C, cervical dermatome; T, thoracic dermatome.
The URP-CTREE revealed that a combination of 3 significant single muscle predictor variables are sufficient to predict a range of different outcomes in QtG, SCIM-SS, and SCIM-MobS and identify homogenous subgroups from the cohort of cervical SCI individuals. For the QtG outcome, the URP-CTREE model with the QlG predictors (Figure 1B) showed similar results (medians and group formation) compared with the URP-CTREE model with the muscle predictor variables (Figure 1A).
As the interpretations of Figure 1A and 1B and Figures 2 and 3 are analogous, the more detailed interpretation of the URP-CTREE results will be limited to Figure 2 with the URP-CTREE for self-care at 6 months. The algorithm resulted in a partition of the initial cervical SCI cohort (n = 57) into 4 subgroups, which are represented as final nodes, based on 3 significant muscle predictor variables (bilateral) at 1 month. The final nodes represent subgroups with different outcomes ranging from low (least favorable) to high (most favorable) values for SCIM-SS at 6 months. The ISNCSCI-Triceps was selected as the first predictor variable (P < .001) and separates the population into 2 newly formed subgroups. The ISNCSCI-Triceps cutoff values ≤1 or >1 are indicated at the “branches.” At each branch, a multiple-testing-adjusted P value is given, which describes the strength of the statistical association between predictor and outcome variable. Below the ISNCSCI-Triceps cutoff ≤1, no further separation was achieved (node 2: n = 14, least favorable outcome). Proceeding from the ISNCSCI-Triceps cutoff >1 subgroup (n = 47), the next separation was achieved with the DI1 cutoff at 6 points (P = .001). Proceeding from the GRASSP-DI1 cutoff ≤6 subgroup (n = 36), the last separation was performed with the GRASSP-Delto (P = .017), identifying 2 subgroups with the GRASSP-Delto cutoff ≤7 (node 5: n = 17) and GRASSP-Delto cutoff >7 (node 6: n = 19) subgroups. Below the GRASSP-DI1 cutoff >6, no further subdividing was achieved (node 7: n = 11, most favorable outcome).
Discussion
The aims of this study were to investigate which single or combined upper limb muscles as defined by ISNCSCI-UEMS and GRASSP best predict upper limb function and independence in ADLs and to assess the predictive value of QlG on upper limb function in individuals with acute tetraplegia. The study reveals that the early assessment of motor strength of specific upper limb muscles is of high predictive value for the recovery of upper limb function and independence in ADLs at 6 months after cervical SCI. The combination of proximal and distal upper limb muscles as well as the early ability to initiate simplified grasp movements (ie, CylGrasp, LatPinch, and TTPinch), predicted upper limb function very well. Statistical methods allowed not only the elucidation of the distribution of outcomes following acute cervical SCI but also the prediction of specific cohorts of outcomes that may be specifically targeted for clinical intervention.
Logistic Regression
Correlations between baseline predictors (ie, upper limb strength) and functional outcomes following acute SCI have been shown in previous studies.7,12,29 Here, logistic regression was applied to reveal the best constellation of shared predictors on defined upper limb outcomes. Not unexpectedly, a combination of standard ISNCSCI muscle groups, that is, FDP, ElbowFlex and WristExt, and additional GRASSP muscles, that is, FPL, EDC, and Delto, showed the best predictive value for the targeted outcomes QtG, SCIM-SS, and SCIM-MobS. Specifically, including a proximal shoulder muscle, in this case M. deltoid, improved prediction as this muscle contributes greatly to daily activities like transferring from bed, toilet, or a car to the wheelchair, dressing the upper body or pouring water from a bottle into a cup. If the proximal shoulder and arm cannot be actively positioned and controlled as needed, the ability to use the hand for functional activities will be severely limited. Our refinement in including additional distal key muscles of the hand and fingers also contributed to improved prediction. Activities such as feeding, buttoning a shirt, inserting a key into a lock and turning it depend also on fine hand, finger and thumb movements, that is, WristExt, FDP, EDC, and to a major extent, FPL. Our data are comparable to findings in a prior cross-sectional study on upper limb function in cervical SCI, 24 in which a combination of distal muscle groups was proven especially useful in predicting self-care independence.
By performing a likelihood ratio test, we demonstrated that the reduced model displays a greater predictive capacity than a logistic model containing all 10 muscle predictors—an unexpected finding. A combination of a reduced number of proximal and distal muscles provided the same accuracy as the full model. This information is lost when using summed scores because in this case it is still unclear which single muscles contribute to outcome improvement. Moreover, in clinical settings and for research, the muscles to be tested should only include those of which that are useful in predicting functional outcome. The use of a combination of single predictors to enable more reliable prediction of long-term functional outcomes after SCI is in accordance with findings reported in previous longitudinal studies,7,14,16 although they have, in contrast, focused on total maximum summed scores combined with other predictor variables, making comparisons potentially unreliable.
URP-CTREE
Applying unbiased recursive partitioning resulted in the selection of a combination of proximal and distal muscles (ie,Triceps and Delto, and FDP, EDC, DI1, FPL, and Opp) as the best significant predictor variables for the outcomes QtG, SCIM-SS, and SCIM-MobS. The advantage of URP-CTREE lies in the provision of a decision tree with specific threshold values (eg, muscle strength scored from 0 to 5) for all outcomes. Our results demonstrated that a combination of a maximum of 3 significant muscle predictor variables are sufficient to predict a range of different outcomes (least favorable to most favorable) in QtG, SCIM-SS, and SCIM-MobS and can reliably identify homogeneous subgroups from the cohort of cervical SCI individuals.
The AIS and MLI predictor variables were not chosen in the URP-CTREE model, indicating that AIS and MLI do not improve prediction accuracy. The combination ISNCSCI-UEMS and GRASSP muscle predictors with threshold values above the branches (URP-CTREE) are therefore excellent indices for the stratification of patient groups and a good proxy for least and most favorable outcome irrespective of AIS and MLI. The AIS and motor level shown in the terminal nodes of Figures 2 and 3 demonstrate the high heterogeneity across all nodes at 6 months.
The URP-CTREE finding that GRASSP-QlG items predicted upper limb function accurately is exciting because QlG can be quickly and easily assessed at the bedside in almost all clinical settings and highlights the importance of including this relative simply measure in standard clinical evaluations.
Clinical and Research Implications
The high variability in neurological recovery requires reliable and sensitive prognostic tools for cervical SCI outcomes if we are to improve the design and conduct of clinical trials. This includes the stratification and enrollment of the most suitable patients (eg, avoiding the enrollment of patients who will recover well irrespective of treatment) and to provide information regarding meaningful clinical outcome thresholds. Simplified, visually informative yet sensitive prediction models like URP-CTREE are of great value in the clinical trial setting. The magnitude of recovery and expected functional outcome is also of great importance for future rehabilitation interventions and to provide early prognostic information to patients and their families.
Most interestingly, the testing of QlG may be a promising assessment tool as it can be applied easily in individuals with acute tetraplegia. QlG requires little time and can complement the standard assessment of muscle strength.
Limitations
The findings presented here are based on assessments at 1 month (range = 16-40 days) after injury and cannot be easily applied to studies performed within the first days following SCI. The effect of different time intervals on the prediction models following SCI needs to be evaluated in more detail. Validation of an independent data set (ie, external validation) will also be required to prove to what extent our findings can be generalized.
Conclusion
Our data show that prediction of upper limb function and independence in ADLs at 6 months can be accurately achieved through a combination of a limited number of single proximal and distal muscle strength tests as provided by the ISNCSCI-UEMS and GRASSP standards in individuals with acute cervical SCI. Furthermore, the combination of ISNCSCI-UEMS and GRASSP muscle predictors are ideal indices for stratifying patient groups and a good proxy for favorable and unfavorable outcomes irrespective of AIS and MLI. Qualitative grasping, a simple test with minimal time demands, predicted upper limb function very well. In summary, the predictive value of standard ISNCSCI-UEMS for upper limb function can be significantly improved with the addition of single GRASSP predictors.
Footnotes
Acknowledgements
We are grateful to the individuals with SCI who participated in this study and the cooperating centers, especially to those occupational therapists who recruited and tested the participants: Spinal Cord Injury Center, Hohe Warte, Bayreuth, Germany, Orthopädische Universitätsklinik Heidelberg, Germany, Unfallklinik Murnau, Germany, Balgrist University Hospital, Zurich, Switzerland, and the Swiss Paraplegic Center Nottwil, Switzerland. Furthermore, we thank Dr Aurelio Tobon (Nottwil) for performing the clinical neurological examinations and Mr Tim Killeen (Balgrist) for reviewing the article and his invaluable assistance with English language editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Swiss Paraplegic Center, Nottwil, Switzerland, and funded by the Clinical Research Priority Program NeuroRehab of the University of Zurich, Switzerland.