
Abstract
Background. There is inherent heterogeneity within individuals suffering from cervical spinal cord injury (SCI), and early prediction of upper limb function and self-care is challenging. As a result, considerable uncertainty exists regarding the prediction of functional outcome following cervical SCI within 1 year of injury. Objective. To evaluate the value of Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) in predicting upper limb function and self-care outcomes in individuals with cervical SCI. Method. A prospective longitudinal multicenter study was performed. Data from the GRASSP, the Spinal Cord Independence Measure (SCIM III), and the American Spinal Injury Association (ASIA) Impairment Scale were recorded at 1, 6, and 12 months after cervical SCI. For prediction of functional outcome at 6 and 12 months, a logistic regression model, receiver operating characteristics (ROC), and unbiased recursive partitioning conditional inference tree (URP-CTREE) were used with 8 different predictor variables. Results. Logistic regression analysis, ROC analysis, and URP-CTREE all revealed that the strength subtest within GRASSP is the strongest predictor for upper limb function and self-care outcomes. URP-CTREE provides useful information on the distribution of different outcomes in acute cervical SCI and can be used to predict cohorts with homogeneous outcomes. Conclusion. The GRASSP at 1 month can accurately predict upper limb function and self-care outcomes even in a heterogeneous group of individuals across a wide spectrum of neurological recovery. The application of URP-CTREE can reveal the distribution of outcome categories and, based on this, inform trial protocols with respect to outcomes analysis and patient stratification.
Keywords
Introduction
Individuals with cervical spinal cord injury (SCI) suffer from a broad spectrum of upper limb impairments. They may experience loss of strength, sensation, and movements, as well as limited ability to perform activities of daily living (ADLs). This ultimately leads to decreased independence and restricted participation as well as quality of life. Indeed, individuals with cervical SCI report a strong desire to regain arm and hand function and that such a gain would improve their independence and quality of life.1,2 Therefore, reliable prediction of future upper limb function and self-care at an early stage after cervical SCI has become increasingly important for several reasons: clinically it would help in treatment planning and goal setting, in a research context it would permit evaluation of novel interventions and patient stratification,3-6 and from a socioeconomic perspective, it would be of benefit in predicting the likely degree of capacity for independent living and required level of caregiver support. After a lesion of the cervical spinal cord, arm and hand function outcomes vary significantly and are not only dependent on the level and completeness of the lesion but also on the degree of recovery, motivation, and occupational performance of the individual. This inherent heterogeneity within individuals following cervical SCI7,8 renders early prediction of upper limb function and self-care challenging. 9
Although several outcome measures of upper limb function are available, 10 only a few have been specifically developed for SCI, and psychometric testing of these measures has revealed deficits.10,11 The predictive validity of quantitative measures has not yet been established, 12 while the aforementioned cohort heterogeneity in cervical SCI makes identifying appropriate outcome measures difficult.7,13 To overcome this limitation, the Graded and Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) was developed as a quantitative outcome measure specific to upper limb function in cervical SCI. Most important, GRASSP covers different aspects of upper limb function to evaluate changes within the motor and sensory systems and how changes in the level of impairment contribute to complex upper limb functional tasks. 14 In individuals with chronic cervical SCI (ie, more than 6 months postinjury), the GRASSP has shown high validity and excellent overall inter- and intrarater reliability, 15 while analysis of responsiveness is still pending.
Little has been published on prediction of functional outcome in general following SCI,16-19 and in particular, data on prediction and stratification of upper limb function and self-care after incomplete cervical SCI is lacking. 8 The aim of the study, therefore, was to evaluate the predictive value of GRASSP for upper limb function and self-care outcome at 6 and 12 months postinjury in individuals with acute cervical SCI.
Methods
Study Design
The study was designed as a prospective longitudinal multicenter study.
Study Population
Participants were recruited from 5 European SCI centers specialized in the rehabilitation of individuals with SCI. Participants were recruited between January 2009 and May 2011. Inclusion criteria consisted of traumatic or nontraumatic, acute (16-40 days after injury) tetraplegia with an American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade of A, B, C, or D. 20 Patients were included if their injury was between C3 and T1 in the case of ASIA A patients and C1-T1 in those with incomplete injuries. Excluded were those individuals with any accompanying severe neurological (eg, traumatic brain injury) or medical disorders or aged less than 16 years. Participants were recruited after providing written informed consent, and the study was approved by the relevant local ethics committees.
Procedures
Assessors (physicians and occupational therapists) with at least 1 year of experience in working with individuals with SCI performed the measurements. To ensure high-quality examinations and to reduce interobserver variability, 21 assessors received training in how to perform all outcome measure assessments. A unified protocol, outlining in detail how the assessments should be performed, was followed for each outcome measure, with recording techniques and materials standardized across all centers. A quiet room, free of distractions was used for all assessments. For ASIA testing, participants lay in a comfortable supine position while for GRASSP testing they were seated. The Spinal Cord Independence Measure (SCIM III) was scored by trained and experienced physical therapists, nurses, and occupational therapists. Assessments were performed at 1 month (range = 16-40 days), 6 months (range = 150-186 days), and 12 months (range = 300-400 days) after cervical SCI.
The AIS classifications were calculated by a computer algorithm, 22 in accordance with definitions in the International Standards for Neurological Classification of Spinal Cord Injury. 20
Predictor Variables
The GRASSP is an upper limb outcome measure for individuals with tetraplegia that includes manual muscle testing (MMT), Semmes and Weinstein monofilament (SWM) testing, adoption of 3 prehensile positions (qualitative grasping [QlG]) and performance of 6 task-oriented prehension skills (quantitative grasping [QtG]). The subtests within GRASSP, assessed between days 16 and 40 after cervical SCI, were selected as baseline predictor variables.
Manual Muscle Testing (MMT)
Strength was assessed for both arms using the MMT 23 in 10 muscles of the upper limb (3 in the arm, 7 in the hand). Each item (muscle) was given a score varying from 0 (response absent) to 5 (normal power). The sum of the MMT subtest score for both sites therefore ranges from 0 to 100 points, and the sum of the distal (hand) muscle group of the MMT subtest score for both sites ranges from 0 to 70 points.
Semmes and Weinstein Monofilament (SWM)
The tactile cutaneous sensation threshold was assessed with the pocket version of SWM 24 (North Coast Medical, Inc, Campbell, CA) with 4 probes on 3 dorsal and palmar sensory test locations in each hand as described in the instructions of the SWM mini-kit 24 and the GRASSP manual. The pressure applied was recorded on an ordinal scale corresponding to numeric values varying from 0 (absent) to 4 (normal). The sum of the dorsal or palmar sensation subtest score for both sites therefore ranges from 0 to 24 points.
Qualitative Grasping (QlG)
The ability of the participant to perform a cylindrical grasp, lateral key pinch, and tip-to-tip pinch was assessed for both hands. Each grasp was given a score varying from 0 (no voluntary control of wrist and digits when grasping) to 4 (normal voluntary control of wrist and digits when generating the grasp). The sum of the grasping quality subtest score for both upper limbs thus ranges from 0 to 24 points.
Quantitative Grasping (QtG)
The ability of the participant to perform 6 prehension tasks for each arm separately (like grasping or moving a coin) was assessed in a standardized way. The tasks were scored between 0 and 5 according to the grasp used. One minute and 15 seconds were allowed for the completion of each task, and if the individual was unable to perform the task within this time period, the individual was asked to move on to the next task. 25 The maximum possible sum of the quantitative subtest score was 60 for both sites.
The SCIM III assesses independence in fundamental daily activities and is useful for measuring the status of, or improvement in, everyday functions relevant to individuals with SCI. 26 The SCIM III has been shown to perform well under psychometric testing,27-29 and the self-care subcategory (SCIM-SS) is particularly notable for its high interrater reliability and internal consistency. 27 The SCIM III consists of 3 subcategories: (a) Self-care (SCIM-SS), (b) respiration and sphincter management, and (c) mobility. In our study, the SCIM III-SS was selected as a predictor variable. The sum of the SCIM-SS ranges from 0 to 20 points.
Clinical neurological examination was performed according to the ISNCSCI protocol. 20 Injury characteristics were classified according to the neurological level of injury (NLI) and the overall AIS grade. The Upper Extremity Motor Score (UEMS) of ASIA was selected as predictor variable. Strength in 5 key muscle groups of the upper limb in both arms (2 muscles in the arm, 3 in the hand) were scored between 0 (absent response) and 5 (normal power). The sum value of this score ranges from 0 and 100 for both sides.
Outcome Measures
For the purpose of this article, upper limb function is defined as the capacity to use the upper limb for skilled actions, such as reaching, grasping, and manipulation of objects used in daily life. The GRASSP subtest QtG is therefore taken as reflecting upper limb function. QtG and the SCIM-SS (for details, see above) were used as anchor outcome measures of upper limb function and self-care at 6 and 12 months after cervical SCI.
Statistical Analysis
Descriptive statistics were used to determine the frequency, median, and range of the study participants’ characteristics including AIS grade, lesion level and lateralization, sex, and age.
We dichotomized the 2 outcomes for the logistic regression analysis to assign patients into a failure or success group. For QtG, individuals were allocated to the failure group (0-36 points) if they met any of the following 3 conditions: (a) not able to perform the task at all, (b) not able to complete the task, and (c) able to complete the task only by using an alternative (ie, compensatory) grasp (not able to perform standard grasps). All individuals who were able to complete the task using the standard grasp were allocated to the success group (37-60 points), irrespective of any difficulties while performing the task. To distinguish between individuals who were dependent or independent with respect to self-care with or without devices, a cutoff SCIM-SS score of 12 was applied, with scores of 0 to 12 points defined as dependent (failure), and scores of 13 to 20 as independent (success), irrespective of supplementary device usage.
Binary logistic regression was performed on the dichotomized outcomes QtG and self-care with the goal to predict upper limb function and self-care at 6 and 12 months using predictors gathered between days 16 and 40 after cervical SCI. The number of predictors was minimized in line with the goal of producing the simplest possible model suitable for subsequent deployment in clinical practice as a simple bedside test used by rehabilitation staff within 6 weeks after cervical SCI. We did not use stepwise statistical variable selection procedures, such as forward inclusion or backward elimination, because this may result in biased estimates of regression coefficients and exaggeration of variable P values.30-32 Two different single predictors were investigated: MMT subtest strength total score and SWM sensation subtest total score (with the palmar and dorsal components combined). A correlation analysis using Spearman’s correlation coefficient was performed between the predictor and outcome variables of the logistic regression (rs) to determine the relationships between them. The level of significance was set at .05. Correlations in the range of 0 to .25 were interpreted as none to poor, .26 to .50 as fair, .51 to .75 as moderate to good, and .76 to 1.0 as very good to excellent.
The performance of each model was assessed by calculating receiver operating characteristics (ROC) curves. The area under the curve (AUC) is a measure for quantifying the discriminative ability of the model. 33 Values between .90 and 1.00 indicate excellent predictive discrimination.
Unbiased recursive partitioning is a flexible statistical model used for a variety of regression problems. A regression tool from the family of unbiased recursive partitioning methods called conditional inference tree (URP-CTREE) 34 was used to produce classification trees for the outcomes QtG and self-care at 6 and 12 months, using predictors assessed between days 16 and 40 after cervical SCI. Eight different predictors were investigated: MMT strength subtest total score, MMT distal strength subtest total score, SWM (palmar and dorsal components combined) sensation subtest total score, SWM palmar sensation subtest total score, QlG subtest total score, QtG subtest total score, SCIM-SS, and UEMS subtest total score. URP-CTREE creates decision rules, which divide the initial, heterogeneous patient population into increasingly homogeneous subgroups (with respect to outcome). Each rule in the classification tree is based on the singular most significant predictor, and the splits are set as to maximize discrepancy between the subsequently formed groups. The tree stops growing when there is no longer any significant predictor. The decision rules allow prediction of the response variable and, at the same time, can be used as a stratification tool.
All data were analyzed using SPSS version 18.0 for Windows and R version 2.14.0 for Windows.
Results
Study Population
Of the 61 participants included, 56 had a traumatic and 5 a nontraumatic SCI. Some data were missing for 4 patients at the 6-month assessment and for 5 patients at the 12-month assessment. Injury severity and lesion level were variable. Detailed cohort characteristics are presented in Table 1.
Demographic and Clinical Characteristics of Participants (n = 61).
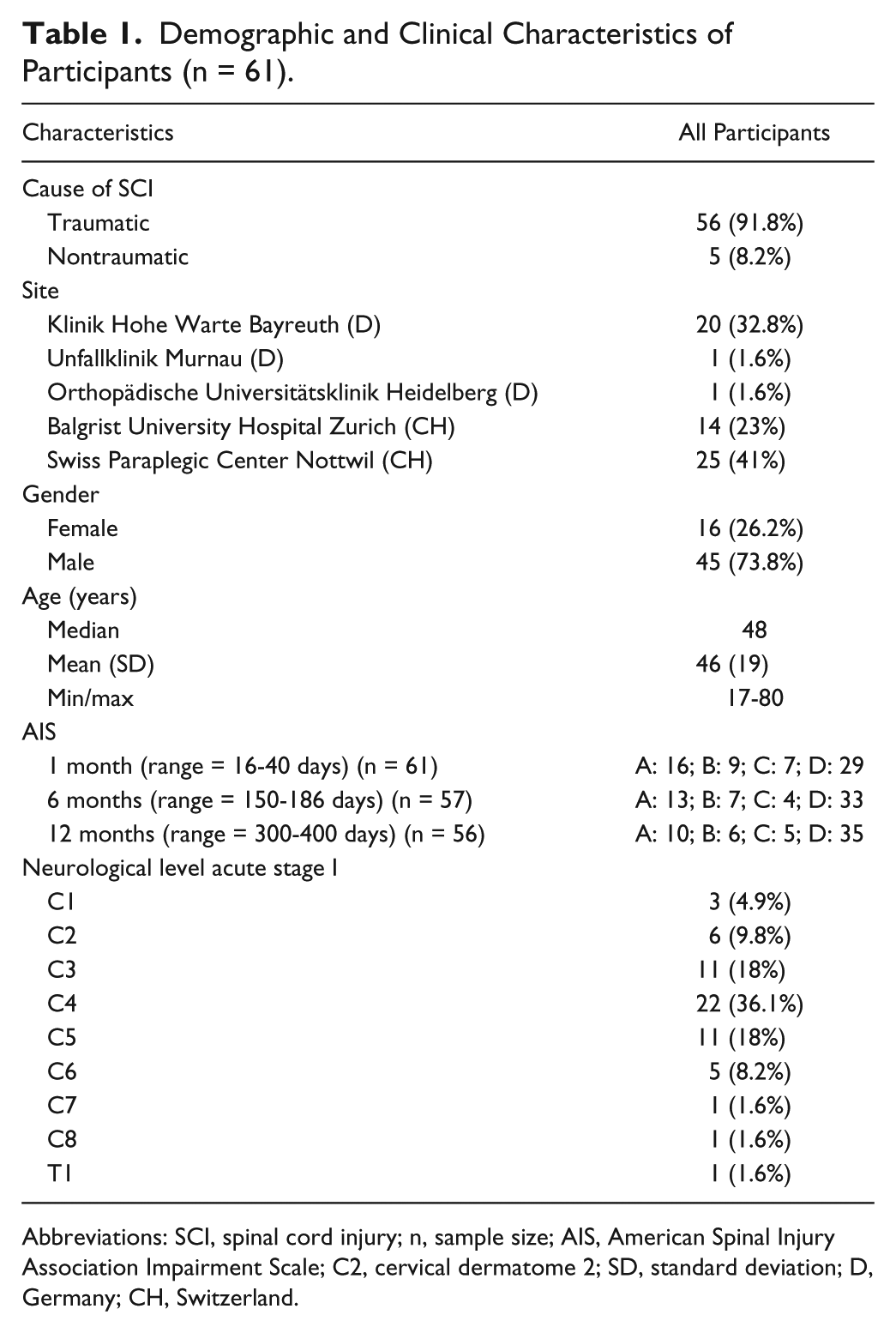
Abbreviations: SCI, spinal cord injury; n, sample size; AIS, American Spinal Injury Association Impairment Scale; C2, cervical dermatome 2; SD, standard deviation; D, Germany; CH, Switzerland.
Spearman Correlations
The correlation between MMT total score with the outcome variables QtG and self-care at 6 and 12 months was excellent (QtG, 6 months, r = .885, P < .001; 12 months, r = .904, P < .001; self-care, 6 months, r = .821, P < .001; 12 months, r = .820, P < .001). There was a moderate to good correlation between SWM total score and the outcome variables QtG and self-care at 6 and 12 months (QtG, 6 months, r = .651, P < .001; 12 months, r = .639, P < .001; self-care, 6 months, r = .781, P < .001; 12 months, r = .643, P < .001).
Logistic Regression
For prediction of QtG and self-care outcome at 6 and 12 months based on MMT total score at 1 month, specificity ranged between 72.4% and 92.1%. Sensitivity of MMT total score at 1 month ranged from 81.8% to 90.9% for the 2 outcomes at 6 and 12 months. In contrast, the SWM total score at 1 month performed less well with predictive specificity ranging from 69.6% to 78.9% and sensitivity from 68.2% to 84.4% at 6 and 12 months for QtG and self-care. Detailed results of the logistic regression analysis are presented in Table 2.
Classification Table a .
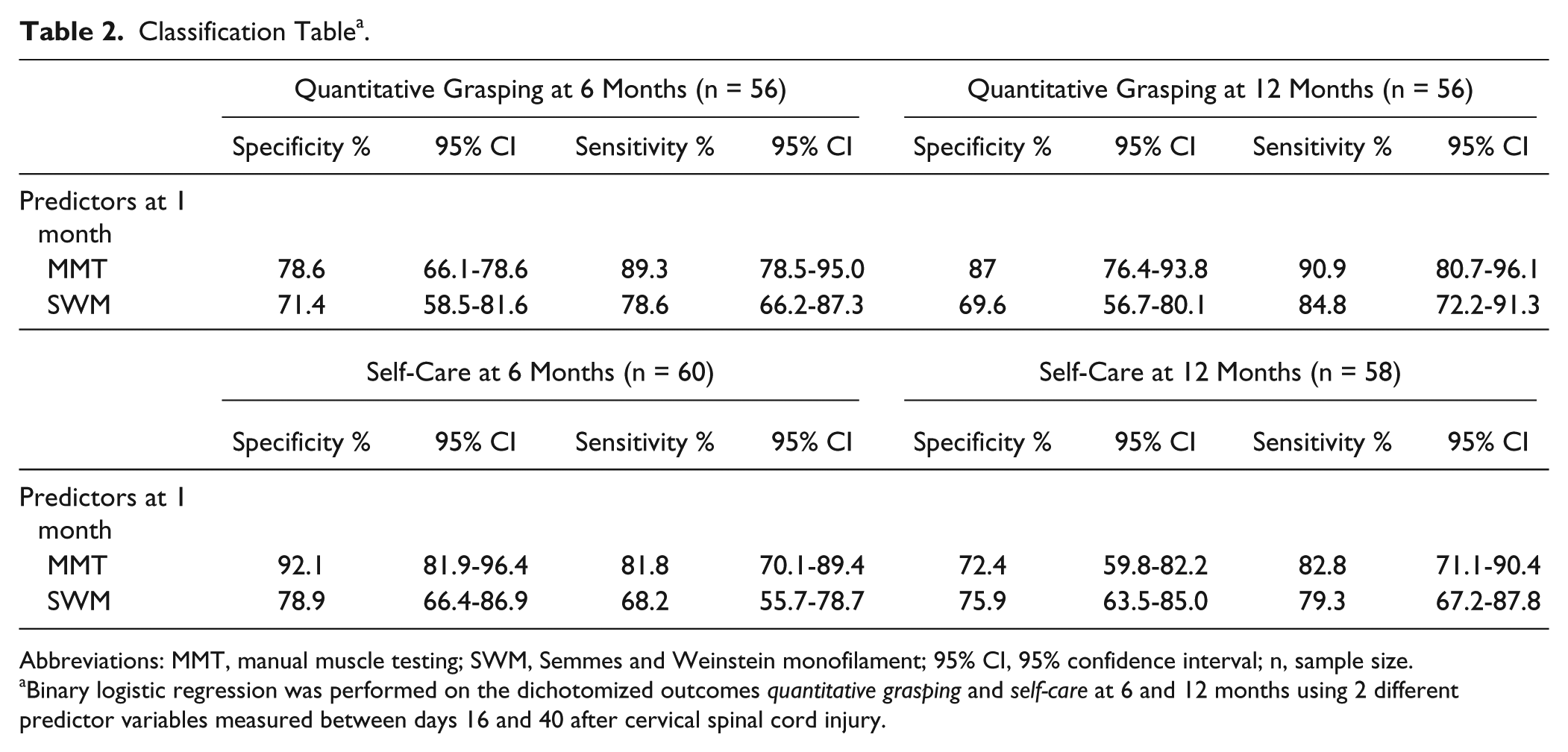
Abbreviations: MMT, manual muscle testing; SWM, Semmes and Weinstein monofilament; 95% CI, 95% confidence interval; n, sample size.
Binary logistic regression was performed on the dichotomized outcomes quantitative grasping and self-care at 6 and 12 months using 2 different predictor variables measured between days 16 and 40 after cervical spinal cord injury.
Receiver Operating Characteristics
The results of the ROC analysis in predicting QtG and self-care outcome at 6 and 12 months were in line with the results of the logistic regression analysis. The AUC value for MMT was larger (ranged from 0.917 to 0.961, P < .001) compared with SWM (ranged from 0.802 to 0.842, P < .001) at 6 as well as 12 months for both outcome measures. Detailed results for ROC analysis are available in Table 3.
Output of Receiver Operating Characteristics (ROC) Analysis a .
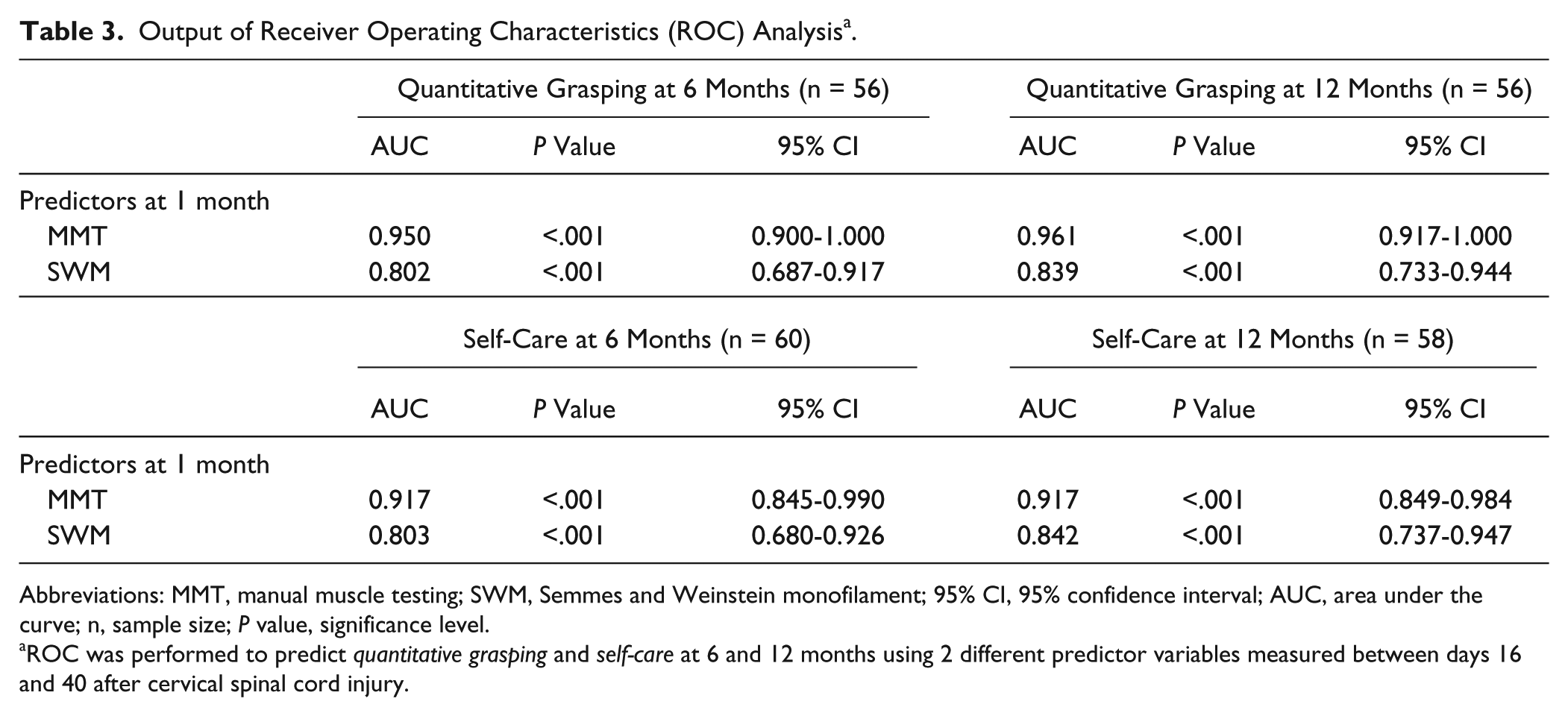
Abbreviations: MMT, manual muscle testing; SWM, Semmes and Weinstein monofilament; 95% CI, 95% confidence interval; AUC, area under the curve; n, sample size; P value, significance level.
ROC was performed to predict quantitative grasping and self-care at 6 and 12 months using 2 different predictor variables measured between days 16 and 40 after cervical spinal cord injury.
URP-CTREE
We analyzed 8 different predictor variables from our heterogeneous cohort of SCI patients. When these variables were placed into the recursive partitioning-based algorithm, well-defined cohorts for QtG and self-care at 6 and 12 months after cervical SCI could be distinguished.
Figure 1A and B and Figure 2A and B show the URP-CTREE for QtG and self-care at 6 and 12 months. We now present in detail how to read the figure for QtG at 6 months (Figure 1A).
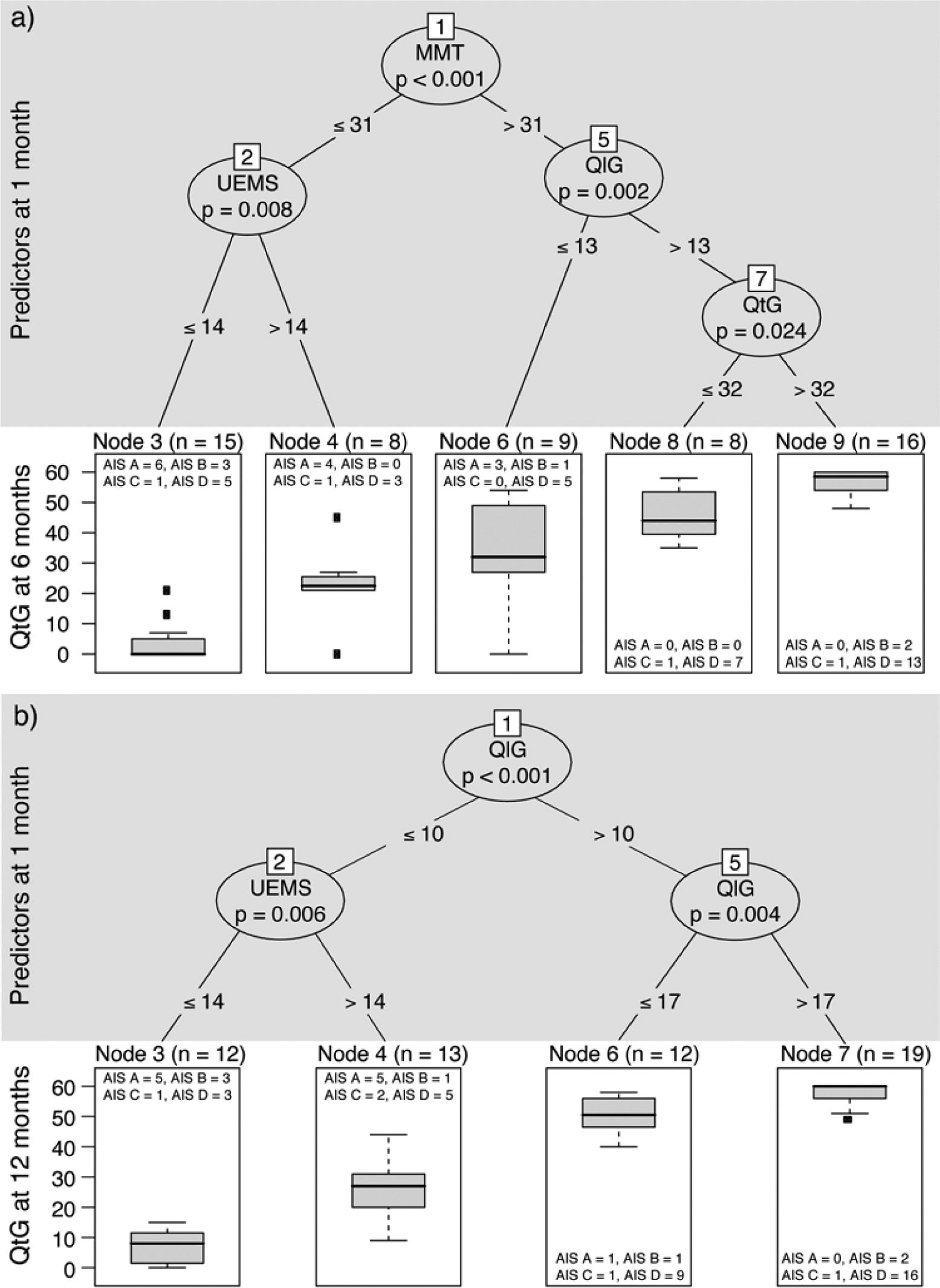
Unbiased recursive partitioning conditional inference tree (URP-CTREE) for quantitative grasping at 6 and 12 months.
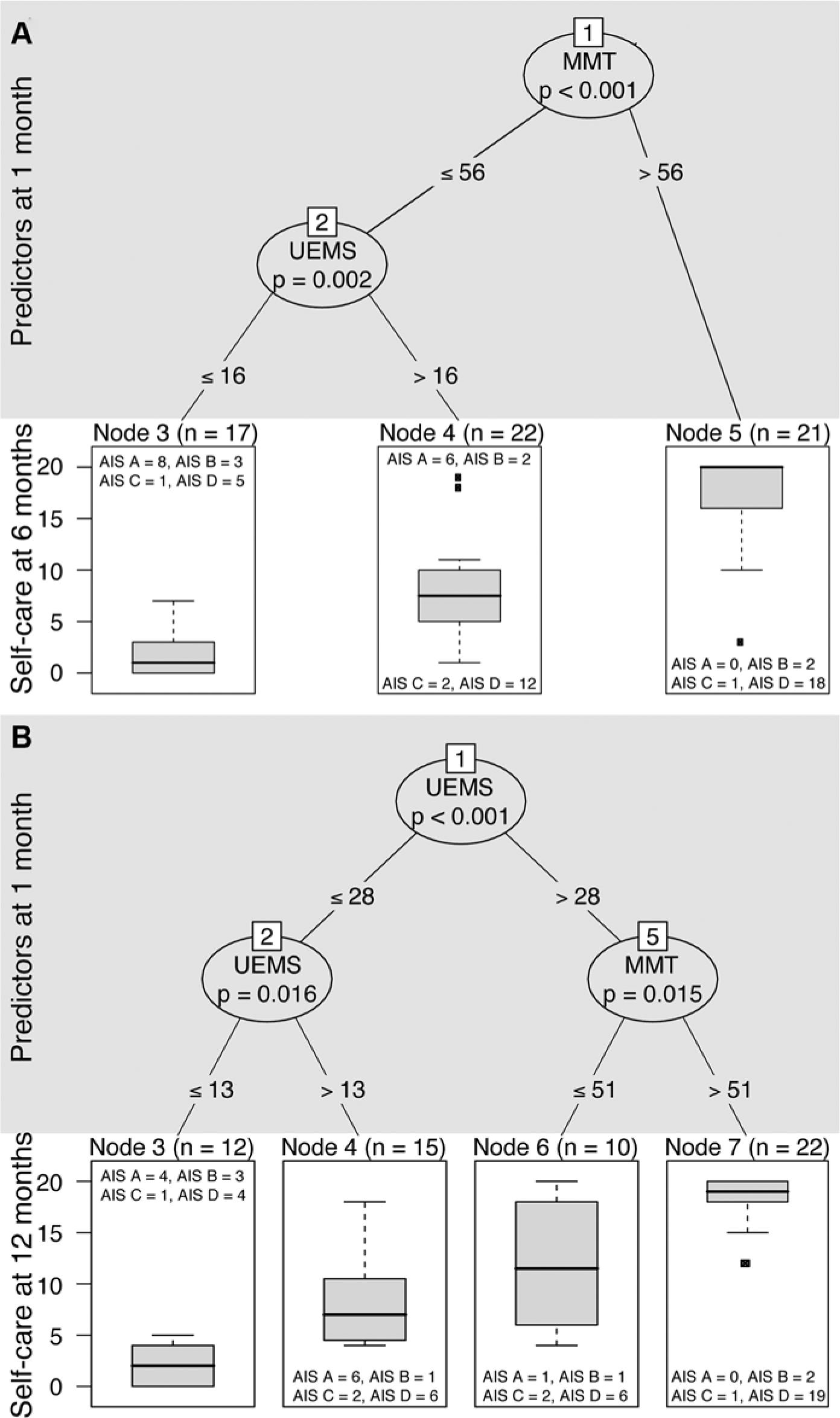
Unbiased recursive partitioning conditional inference tree (URP-CTREE) for self-care at 6 and 12 months.
The algorithm led to a partition of the initial sample (n = 56) into 5 terminal nodes (cohorts). The terminal nodes represent subgroups with different outcomes ranging from low to high values for QtG at 6 months. Initial MMT was selected as a first predictor variable (P < .001) and separates the sample into 2 newly formed subgroups, MMT ≤31 or >31 as indicated by the cutoff value at the “branches.” Below this MMT ≤31 subgroup (n = 23), further separation was achieved with a UEMS cutoff of 14 points (P = .008) giving subgroups UEMS ≤14 (n = 15; least favorable outcome) and UEMS >14 subgroup (n = 8; second least favorable outcome). Proceeding from the MMT >31 subgroup (n = 33), separation was achieved once more through the definition of a QlG cutoff of 13 points (P = .002), giving 2 subgroups: QlG ≤ 13 (n = 9; intermediate outcome) and QlG >13 subgroup (n = 24). This latter grouping (QlG > 13) was further subdivided by QtG score, with a cutoff of 32 showing the largest discrepancy, again with 2 subgroups: QtG ≤32 (n = 8; second most favorable outcome) and QtG >32 (n = 16; most favorable outcome).
Discussion
The aim of this prospective study was to evaluate the value of the GRASSP assessment tool in predicting the outcome of upper limb function and self-care at 6 and 12 months postinjury in individuals with acute cervical SCI. For this purpose, the outcome of upper limb function was assessed based on the performance of hand/upper limb activities (such as the QtG subtest) and ADLs (ie, self-care items in the SCIM III).
The prediction of upper limb function and self-care in patients with acute cervical SCI can be achieved by using the GRASSP tool, of which the motor scoring in particular is of excellent predictive value for clinical outcomes at 6 and 12 months. The reliable prediction of functional outcome categories is essential for improving the stratification of patients for clinical interventions, in which the enrolment of rather homogenous patient cohorts is required. Improved stratification rules will be of benefit in trials assessing the safety and efficacy of interventions in which the detection of even subtle changes is of crucial importance in the evaluation of therapies.
Clinical Outcomes of Upper Limb Function
Given the serious consequences on patients’ independence, quality of life, health care service needs, and their associated socioeconomic costs, there is strong interest in the development of reliable assessment and categorization of upper limb function in tetraplegia. While assessments such as the Van Lieshout test 35 and the Capability of Upper Extremity Test 36 provide important information regarding overall arm and hand usage, they are not designed to provide detailed and reliable information about changes in specific sensory and motor impairments affecting upper limb function. Likewise, the utilization of a global outcome measure such as the SCIM III, although providing clinically meaningful categorization of functioning in ADLs, does not provide insights into the underlying sensorimotor function driving functional recovery. Accordingly, the SCIM III is not well positioned to discern functional improvement arising from actual repair of damaged spinal cord tissue versus rehabilitation training, motivation, and mood factors when performing tasks—whether those tasks are performed bimanually or with compensatory movements—given the SCIM’s focus on gained independence. 26
In contrast, measures designed to capture neurological deficits (eg, the UEMS of the ISNCSCI protocol) 20 that, as opposed to functional readouts, provide detailed scoring of segmental sensorimotor deficits have been proven to be of value in the diagnosis and prognosis of SCI. Clinical experience, backed up by the literature,7,8 shows that recovery of upper limb function is highly variable and an assessment matrix combining neurological and functional readouts for application in acute cervical SCI may be desirable. 13 To this end, the GRASSP was developed in an attempt to demonstrate how changes in impairment (ie, neurological deficit) contribute to complex upper limb function tasks. 15
Prediction of Upper Limb Function
Analysis of a heterogeneous group of patients with acute and subacute cervical SCI revealed that the initial MMT correlated very well both with subsequent upper limb function and self-care at 6 and 12 months and was furthermore superior to the SWM. These findings support previous studies in which significant correlation of MMT and cervical motor levels with self-care in acute and chronic cervical SCI was shown.7,8,37,38 The strong influence of motor impairment on self-care outcomes has been shown in several studies looking at diverse functional outcome domains, including independence and ambulation.16,17,39-41 The impact of recovery of sensation, however, although shown to be critical after peripheral nerve damage, 42 is of less obvious relevance in SCI. While recordings of somatosensory evoked potentials correlate with the sensory impairment and have some predictive value for outcome and recovery of hand function, the immediate impact on complex arm/hand function is less marked. 19 In a recent study using the GRASSP, however, it was noted that preserved sensation positively affects upper limb function, 43 although the nature and degree of these relationships during the course of recovery is unknown.
The significant role of MMT as a predictor variable with a high sensitivity and specificity in upper limb function and self-care at 6 and 12 months was also demonstrated using logistic regression and ROC. Both models corroborate the high within-sample validity of using MMT within GRASSP as predictor variable. SWM, although less influential than MMT, was also able to predict outcome of self-care and upper limb function and might be specifically applicable for prediction when motor assessments are limited (for instance when key motor muscles are not defined above C5) or when muscle activation is hindered by other factors, such as limb fractures or bruising. For the logistic regression and ROC analysis, the SCIM-SS and the GRASSP subtest QtG were converted into 2 dichotomous outcome measures (“dependent” vs “independent” for self-care; “non-functional” vs “functional” for grasping), which represented a wide range of upper limb performance in all subgroups. Logistic regression and ROC analysis do not, however, provide sufficient information about the distribution of outcomes.
URP-CTREE
Few studies to date have examined the stratification of outcomes of upper limb function and self-care in acute tetraplegia.7,8 For ambulation, recent studies have developed prediction rules in acute SCI,16,17,44 primarily based on regression analysis with the attendant, aforementioned limitation in terms of providing information about outcomes distribution. For this reason, we applied URP-CTREE to predict upper limb function and self-care as outcome measures at 6 and 12 months based on different predictor variables assessed at 1 month after injury. The results showed that URP-CTREE enables the prediction of the distribution of different outcomes in acute cervical SCI and the definition of more homogenous outcome cohorts. Again, in line with logistic regression and ROC analyses, MMT remained the strongest predictor for outcome of upper limb function and self-care.
MMT, as defined in the GRASSP, includes a greater number of muscles compared to the ISNCSCI protocol (UEMS) by incorporating distal (extensor digitorum, opponens pollicis, flexor pollicis longus, flexor digitorum profundus [tendon to third digit], first dorsal interosseus, and abductor digiti minimi) and proximal (anterior deltoid) muscle groups. This expanded combination of distal and proximal muscle groups probably contributes to the high outcome prediction seen in this study, lending further support to the continued development of the GRASSP as a standardized assessment tool of upper limb function. Similar findings were reported in a recent review of upper extremity impairment after stroke in which it was concluded that the whole limb is important for overall function. 45
Using URP-CTREE, we were able to show that predictors in the model demonstrated significantly differentiated predictive capacity when compared with the logistic and ROC models, including SWM and MMT as single predictors. Studies that assess the significance of combining individual parameters to improve outcome prediction are sparse.16,17 We provide evidence that the combination of MMT with other predictors, such as QlG and QtG, can improve outcome prediction.
Interestingly, URP-CTREE identified UEMS as a predictor specific to individuals with less favorable functional outcomes. For patients with more favorable functional outcomes, MMT in combination with QlG and QtG demonstrated predictive utility. These data reveal that the combination of MMT strength and dexterity (QlG and QtG) interact to predict improved outcomes of upper limb function, supporting the findings of a previous study. 46 The GRASSP permits the gathering of more comprehensive information (especially in motor incomplete lesions) and is capable of disentangling neurological and functional changes.
In contrast, for self-care outcomes, URP-CTREE demonstrated that the tests of muscle strength (MMT and UEMS) were useful predictor variables while QlG and QtG were not. This finding supports those of a previous study that demonstrated that GRASSP subtests QlG and QtG were not superior to the muscle strength tests (UEMS and MMT) in estimating self-care independence. 37
Limitation
True external validity of the proposed prediction models can only be proven through confirmatory analysis of an independent data set. Many clinical assessments like UEMS, SCIM, and GRASSP are analyzed as sum scores of different items and treated as continuous variables, even though they are ordinal scales. We acknowledge that this could produce misleading results where summed scores do not represent a consistent scoring metric.
Conclusion
The GRASSP is a feasible and reliable assessment tool for the prediction of upper limb function and self-care outcomes in individuals with acute cervical SCI. The GRASSP at 1 month can accurately predict functional outcome at 6 and 12 months, even in a heterogeneous group of individuals across a wide spectrum of neurological recovery. Prediction of outcomes can be used to inform rehabilitation goals and regimens and can be applied in improved stratification of patients in evaluation of interventions. The additional application of URP-CTREE permits insights into the distribution of outcome categories on which clinical trial outcome analysis and stratification may be based.
Footnotes
Acknowledgements
We thank the patients with SCI who participated in this study and occupational therapists at the participating centers: Spinal Cord Injury Center, Hohe Warte, Bayreuth, Germany; Orthopädische Universitätsklinik, Heidelberg, Germany; Unfallklinik Murnau, Germany; Balgrist University Hospital, Zurich, Switzerland; and the Swiss Paraplegic Center, Nottwil, Switzerland. Furthermore we thank Dr Aurelio Tobón (Nottwil) for performing the clinical neurological examinations, Mr Tim Killeen (Balgrist) for critically reviewing the article and his invaluable assistance with English language editing, and Dr Doris Maier (Murnau) and Dr Rüdiger Rupp (Heidelberg) for their collaboration on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Swiss Paraplegic Center, Nottwil, Switzerland, and funded by the NeuroRehab Clinical Research Priority Program at the University of Zurich, Switzerland.