
Abstract
Background. Motor capability is commonly assessed inside the clinic, but motor performance in real-world settings (ie, outside of the clinic) is seldom assessed because measurement tools are lacking. Objective. To quantify real-world bilateral upper-limb (UL) activity in nondisabled adults and adults with stroke using a recently developed accelerometry-based methodology. Methods. Nondisabled adults (n = 74) and adults with chronic stroke (n = 48) wore accelerometers on both wrists for 25 to 26 hours. Motor capability was assessed using the Action Research Arm Test (ARAT). Accelerometry-derived variables were calculated to quantify intensity of bilateral UL activity (ie, bilateral magnitude) and the contribution of both ULs to activity (magnitude ratio) for each second of activity. Density plots were used to examine each second of bilateral UL activity throughout the day. Results. Nondisabled adults demonstrated equivalent use of dominant and nondominant ULs, indicated by symmetrical density plots and a median magnitude ratio of −0.1 (interquartile range [IQR] = 0.3), where a value of 0 indicates equal activity between ULs. Bilateral UL activity intensity was lower (P < .001) and more lateralized in adults with stroke, as indicated by asymmetrical density plots and a lower median magnitude ratio (−2.2; IQR = 6.2, P < .001). Density plots were similar between many stroke participants who had different ARAT scores, indicating that real-world bilateral UL activity was similar despite different motor capabilities. Conclusions. Quantification and visualization of real-world bilateral UL activity can be accomplished using this novel accelerometry-based methodology and complements results obtained from clinical tests of function when assessing recovery of UL activity following neurological injury.
Keywords
Introduction
Many daily tasks require that both upper limbs (ULs) work together in a complementary fashion to accomplish a goal (eg, writing with one hand while stabilizing a piece of paper with the other hand).1,2 As such, recovery of bilateral UL function after stroke is desirable. To assess bilateral UL function, valid and reliable measures are required. Kinematic analyses are commonly used in laboratory settings to assess UL movement parameters (eg, velocity, accuracy, efficiency),3,4 whereas standardized assessments (eg, Jebsen Hand Function Test, 5 Action Research Arm Test [ARAT] 6 ) are commonly used in clinical settings to measure UL function.
These approaches assess motor capabilities (ie, what a person “can do”) in structured research and clinical settings, but they do not measure motor performance (ie, what a person actually does) in unstructured environments (eg, at home, work, and in the community). The distinction between capability and performance has been shown in previous studies, where participants were more likely to use their nonparetic limb during spontaneous task conditions (ie, motor performance) despite adequate motor capability of the paretic UL observed during forced-use conditions.7,8 Thus, motor capability and motor performance are different constructs and should be assessed separately. 9
One approach to measuring motor performance is the use of self-report questionnaires. Unfortunately, self-report questionnaires can be subject to report bias as a result of cognitive impairment following stroke (eg, impaired comprehension, memory recall, attention10-12) and social desirability (eg, desire to please the doctor or therapist, embarrassment over not completing more activity 13 ). Furthermore, often, only moderate correlations are observed between self-reported and direct measurement (eg, heart rate monitoring, double-labeled water, accelerometry) of physical activity. 14
As an alternative to self-report questionnaires, wrist-worn accelerometry has emerged as a tool to assess motor performance that occurs throughout the day. We refer to this activity as real-world UL activity to emphasize that it occurs outside of structured settings. 15 The small size and portability make it possible for accelerometers to be worn while individuals go about their day-to-day activities. Although one cannot determine the specific actions performed from accelerometry recordings (eg, cutting with a fork and knife vs writing 16 ), it nevertheless is a useful index of real-world UL function. 17 To date, accelerometry has been used to quantify duration and intensity of daily UL activity of the ULs separately and then compare UL activity between limbs.17-21 Whereas this practice provides general information about how active one limb is relative to the other (eg, paretic UL relative to the nonparetic UL), it does not provide information about how both ULs are used together during task performance.
Recently, we developed an accelerometry-based methodology that quantifies bilateral UL activity by calculating 2 variables—the bilateral magnitude and the magnitude ratio—to, respectively, quantify intensity of bilateral UL activity and the contribution of each UL to activity on a second-by-second basis. 16 Using tasks performed in a laboratory setting, these variables were able to distinguish high-intensity tasks from low-intensity tasks and tasks that were completed using both hands from tasks that were completed relatively one handed. This methodology has potential use for measuring bilateral UL activity in real-world settings.
The purpose of the current study was to examine real-world bilateral UL activity in nondisabled adults and adults with chronic stroke as they went about their normal, daily routine. We examined both summary statistics and second-by-second values for the bilateral magnitude and magnitude ratio because we hypothesized that second-by-second values would vary greatly with respect to the summary statistics. Using density plots to visualize each second of data, we show that bilateral UL activity varies throughout the day and that bilateral UL activity differs between nondisabled adults and adults with chronic stroke.
Methods
Participants
Nondisabled adults and adults with chronic stroke participated in this cross-sectional study. Nondisabled adults were recruited through HealthStreet, a community-based recruitment program operated by Washington University School of Medicine in St Louis. Inclusion criteria were the following: (1) age >30 years, (2) ability to follow commands, and (3) dwelling in the community. Exclusion criteria included a self-reported history of neurological condition or significant UL impairment.
Adults with chronic stroke participated in a randomized controlled trial (NCT 01146379) investigating the dose-response effect of task-specific training on UL function. Adults with stroke were recruited from the Cognitive Rehabilitation Research Group and the Brain Recovery Core databases at Washington University School of Medicine in St Louis, which contain contact information for adults with stroke who consented to being contacted for participation in research studies. This study analyzed only pretreatment (ie, baseline) data.
Inclusion criteria were (1) diagnosis of an ischemic or hemorrhagic stroke; (2) sufficient cognitive skills to participate, as determined by a score of 0 to 1 on items 1b and 1c of the National Institutes of Health Stroke Scale (NIHSS) 22 ; (3) unilateral upper-extremity weakness, defined by a score of 1 to 3 on item 5 of the NIHSS; (4) motor capability as determined by a score of 10 to 48 on the ARAT (maximum score = 57 and indicates normal motor ability)6,23; (5) dwelling in the community; and (6) at least 6 months poststroke. Exclusion criteria included (1) inability to follow 2-step commands, (2) psychiatric diagnosis, (3) other neurological diagnosis, and (4) pregnancy.
All participants provided informed consent and were compensated for their time. This study was approved by the Human Research Protection Office of Washington University and conformed to the Declaration of Helsinki.
Procedure
Participants completed a 1- to 2-hour lab visit. They provided demographic and health information and completed study assessments that examined factors related to UL activity, which have been reported elsewhere.15,24 Specific factors of interest for the present study included self-reported hand dominance (prestroke hand dominance for adults with stroke) and motor capability of the paretic UL (as measured by the ARAT). Accelerometers were placed on both wrists, proximal to the ulnar styloid. Accelerometers were initialized and synchronized using ActiLife 6 proprietary software (ActiGraph, Pensacola, FL). Participants were instructed to wear the accelerometers for the subsequent 24 hours (including sleep) while they went about their normal, daily routines, with permission to remove the devices when bathing or showering. Accelerometers were returned to the lab during a subsequent visit.
Accelerometry
Wrist-worn accelerometry has established validity and reliability for measuring UL activity in nondisabled adults and adults with stroke.19,20,25,26 GT3X+ Activity Monitors (Actigraph, Pensacola, FL) were used to measure activity. These wireless devices are small (38 × 37 × 18 mm3), contain a solid-state accelerometer that has a dynamic range of ±6 gravitational units, and store data locally. Accelerations were recorded along 3 axes at 30 Hz. Accelerometry data were downloaded using ActiLife 6 software, which band-pass filtered data between frequencies of 0.25 and 2.5 Hz, used a proprietary process to remove acceleration due to gravity, down-sampled data to 1 Hz (ie, 1 s) samples, and converted acceleration into activity counts (0.001664g/count). 27 ActiLife 6 was also used to visually inspect the accelerometry data to ensure that the accelerometers functioned properly during the recording period.
Primary Variables of Interest
Accelerometry data were used to calculate 2 primary variables of interest: the bilateral magnitude and the magnitude ratio. The bilateral magnitude quantifies the intensity of activity across both ULs, whereas the magnitude ratio quantifies the contribution of each UL to activity. Validation of these variables as measures of bilateral UL activity and a description of how they are calculated has been reported previously. 16 Briefly, accelerometry data were exported from ActiLife 6 software to MATLAB R2011b (Mathworks; Natick, MA) and processed using custom-written software. For each second of data, accelerations were combined across axes into a single vector magnitude value using the equation √(x2 + y2 + z2). The bilateral magnitude was calculated for each second of activity by summing the vector magnitude of both ULs. 16 Bilateral magnitude values of 0 indicate that no activity occurred across either UL, whereas increasing bilateral magnitude values indicate increasing UL activity intensity.
The magnitude ratio was calculated for each second of activity by dividing the vector magnitude of one UL by the vector magnitude of the contralateral UL. 16 For nondisabled adults, the nondominant UL was divided by the dominant UL; for adults with stroke, the paretic UL was divided by the nonparetic UL. The calculated values were then transformed using a natural logarithm to prevent skewness of positive, untransformed values. 20 Magnitude ratios could not be accurately calculated for seconds when unilateral UL activity occurred (because 0 would appear in the numerator or denominator); therefore, seconds when unilateral dominant/nonparetic UL activity occurred were assigned a constant value of −7, whereas seconds when unilateral nondominant/paretic UL activity occurred were assigned a value of +7. Magnitude ratio values of 0 indicate that both ULs contributed equally to activity. Negative values indicate more dominant/nonparetic UL activity relative to the nondominant/paretic UL, and the opposite is true for positive values. Because examination of UL activity was the purpose of this study, seconds when neither UL was active (ie, the bilateral magnitude was equal to 0) were removed from analysis.
Secondary Variables of Interest
Four secondary variables were calculated—durations of (1) dominant/nonparetic unilateral, (2) nondominant/paretic unilateral, (3) simultaneous, and (4) total UL activity—to summarize general UL activity that occurred during a typical day. Data were dichotomized into active or not active based on whether or not an activity count was recorded for each second. Unilateral UL activity was defined as seconds when only one UL was active, and simultaneous UL activity was defined as seconds when both ULs were active. Duration of total UL activity was obtained by summing the duration of unilateral and simultaneous UL activity, thus reflecting the duration of time when either UL was active.
Statistics and Examination of Accelerometry-Derived Variables
IBM SPSS Statistics for Windows, Version 21 (IBM Corp, Armonk, NY) was used. Normality of accelerometry-derived variables was assessed using Kolmogorov-Smirnov tests. For individual-level data, median values for the bilateral magnitude and magnitude ratio were calculated because these variables were not normally distributed. For group-level data, summary statistics (ie, means and standard deviations or medians and interquartile ranges [IQRs]) were calculated for each variable. Note that the IQR represents the range of the middle 50% of data values for a given variable. Parametric (ie, independent samples t tests) and nonparametric (ie, Pearson’s χ2 tests, Mann-Whitney U tests) analytical tests were used to examine relationships among demographic variables within and between groups and differences in study variables between groups. Differences in study variables within groups based on hand dominance (nondisabled adults) and side affected by stroke (adults with stroke) were also examined. Spearman correlations were used to investigate the association between motor capability (ie, ARAT scores) and primary variables of interest. All tests of significance were 2 tailed and the criterion for significance was α <.05.
Two-dimensional density plots were created using bivariate histograms to examine the bilateral magnitude (y-axis, bin width: 20 activity seconds) and magnitude ratio (x-axis, bin width: 0.2 units) for each second of real-world UL activity. The duration (ie, number of seconds) with which a given bilateral magnitude-magnitude ratio combination occurred is depicted by color. Increasing bilateral magnitude values indicate increasing intensity of UL activity across one limb (unilateral activity) or both limbs (simultaneous activity). Magnitude ratio values of −7 depict seconds when dominant/nonparetic unilateral UL activity occurred, and values of +7 depict seconds when nondominant/paretic unilateral UL activity occurred. Magnitude ratios from −6 to +6 depict seconds when simultaneous UL activity occurred. A magnitude ratio of 0 indicates equal contribution from both ULs. Increasing negative values indicate increasing dominant/nonparetic UL activity relative to the contralateral limb, whereas increasing positive values indicate increasing nondominant/paretic UL activity relative to the contralateral limb.
Results
Description of Participants
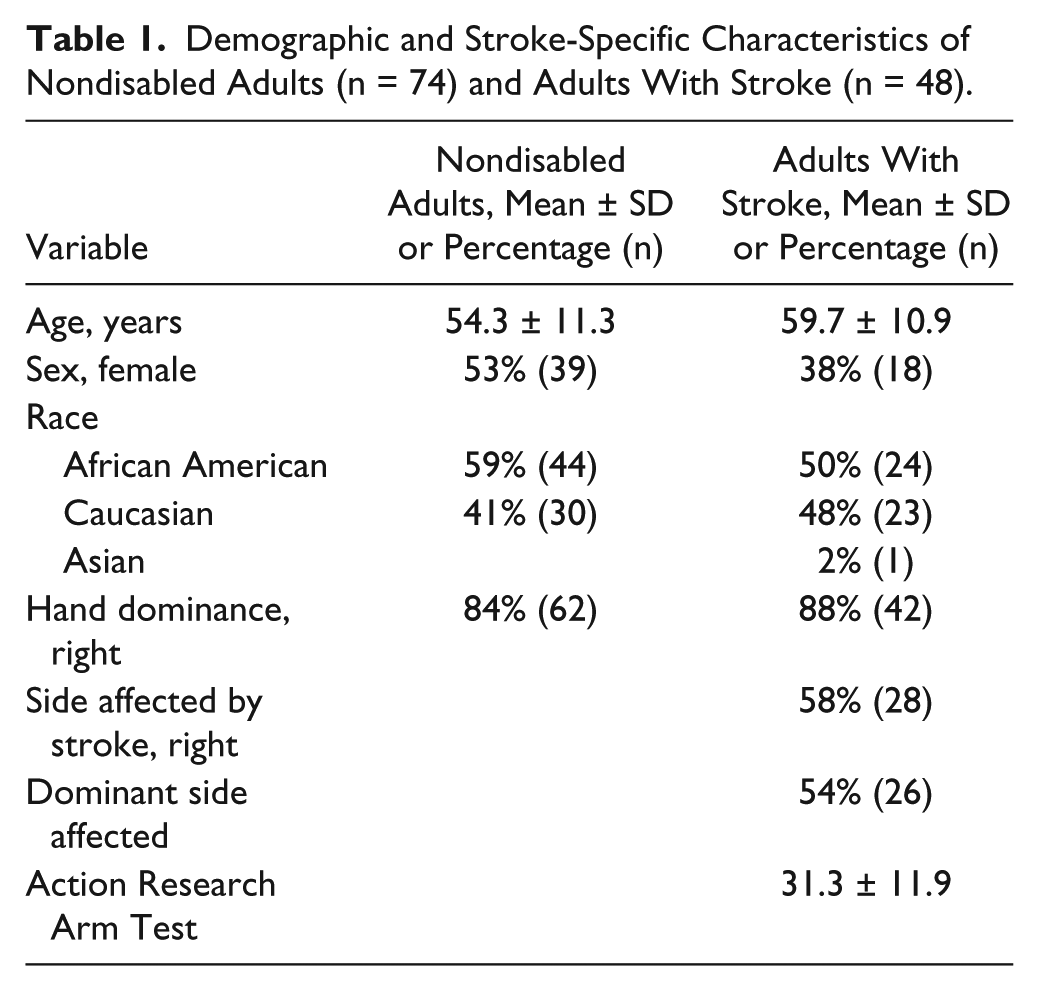
Accelerometry data were available for 74 nondisabled adults and 48 adults with stroke. Demographic information and stroke-specific characteristics are displayed in Table 1. Adults with stroke were 5 years older on average than nondisabled adults (P = .01). There were no differences in sex, race, or hand dominance between groups (for all values, χ2 < 2.7, P > .10). Stroke participants can be characterized as having mild-to-moderate deficits, based on ARAT scores. Median time since most-recent stroke was 0.9 (IQR = 1.3) years, and median number of strokes was 1 (IQR = 0). Nondisabled adults wore accelerometers for 25.0 (IQR = 0) hours, and adults with stroke wore accelerometers for 26.0 (IQR = 0) hours (P < .001).
Demographic and Stroke-Specific Characteristics of Nondisabled Adults (n = 74) and Adults With Stroke (n = 48).
Primary Variables of Interest
Nondisabled Adults
Data for 3 individual participants are first presented to facilitate interpretation of the bilateral magnitude, magnitude ratio, and the density plots. Figure 1A displays data for a participant whose median bilateral magnitude was 98.3 activity counts (IQR = 128.5) and median magnitude ratio was −0.49 (IQR = 7.47), indicating that he performed a great deal of low-intensity UL activity, and dominant UL activity slightly exceeded nondominant UL activity. The magnitude of the IQRs indicate that second-by-second bilateral magnitude and magnitude ratio values varied greatly with respect to median values; this is also illustrated by the spread of values in Figures 1A to 1C. Dominant unilateral activity (left side of figure) slightly exceeded nondominant unilateral UL activity (right side of figure), and low-intensity (ie, bilateral magnitude < 200 activity counts) unilateral activity occurred often (ie, red color). The majority of total UL activity consisted of simultaneous UL activity (middle of figure). Patterns of activity between ULs were similar, as indicated by the roughly symmetrical appearance of the middle portion of the figure.
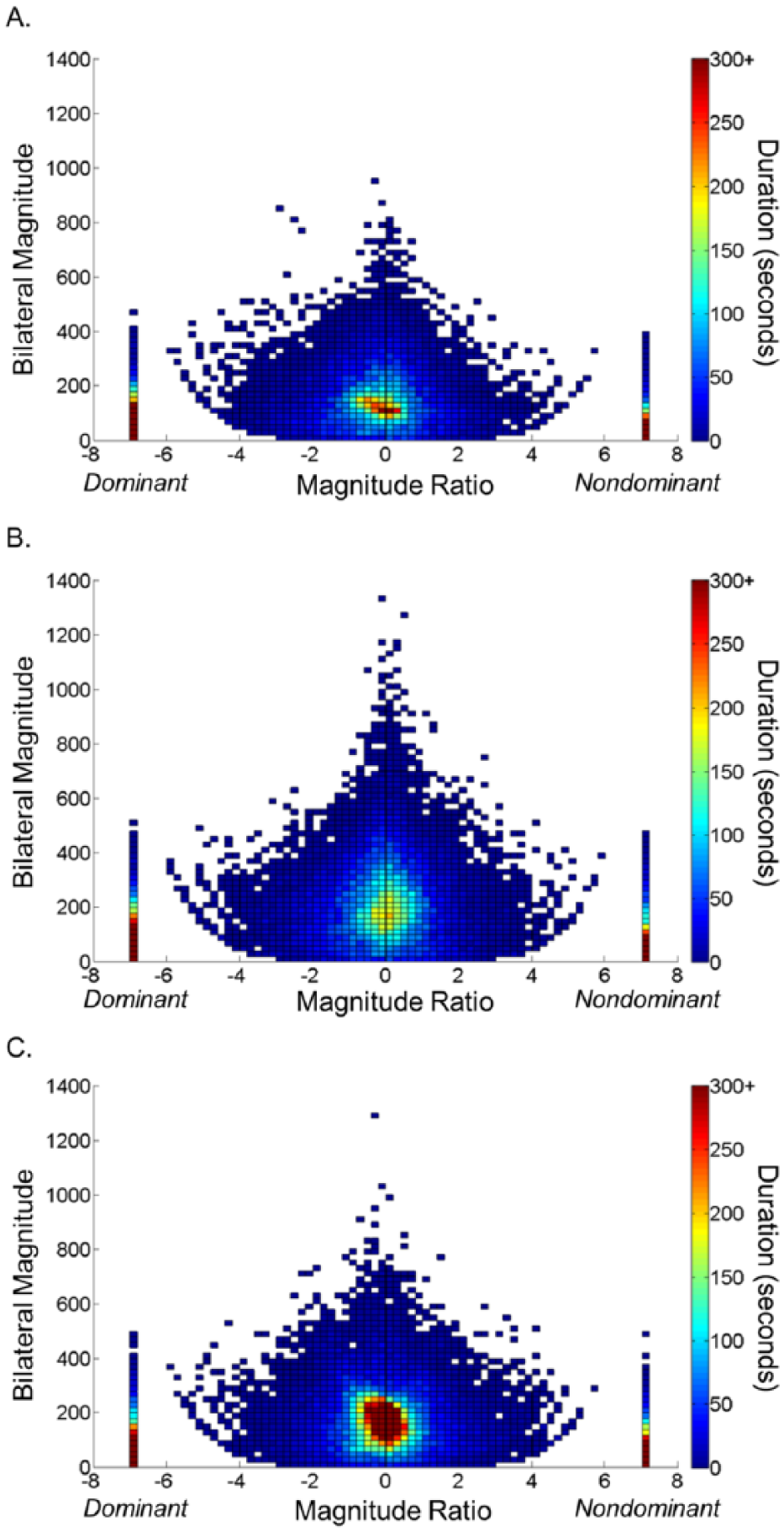
Density plots showing 25 hours of real-world bilateral upper-limb (UL) activity in 3 nondisabled adults. A. Total UL activity (9.6 hours) was low in this participant. B. Total UL activity (11.9 hours) and median bilateral magnitude and median magnitude ratio values were higher in this participant. C. Total UL activity (13.7) and median bilateral magnitude and magnitude ratio values were highest in this participant. Despite differences in total UL activity, each density plot was symmetrical in overall shape, indicating that patterns of dominant and nondominant UL activity were similar.
Figure 1B provides data from a second participant whose median bilateral magnitude was a little higher (141.6 activity counts, IQR = 194.5) and median magnitude ratio was closer to 0 (−0.13, IQR = 2.63). Figure 1C displays a third example participant whose median bilateral magnitude was even higher (152.2 activity counts, IQR = 128.4) and median magnitude ratio was nearly 0 (−0.06, IQR = 1.30). Figures 1B and 1C are closer to symmetry than 1A, though the differences are slight. This pattern of slightly asymmetrical to nearly pure symmetry was consistent across the 74 nondisabled adults.
Three additional features of the density plots require explanation. First, the rounded or bowl-shaped bottoms of the density plots occur when activity is of low intensity and one UL is moving at a relatively greater intensity compared with the opposite UL. The rims of the bowl shape represent increasing intensity of activity, where one hand is accelerating and the other is relatively but not completely still. An example of this would be sorting objects with one hand while the other secures the container. 16 Second, the “warm glow” in the bottom center of each plot indicates that real-world dominant and nondominant UL activity is often closely matched to perform activities of low to moderate intensity. Examples of such activity include cutting food with a knife and fork and sorting small objects using both hands. 16 Third, the concavity that is seen when the magnitude ratio approaches 0 and the bilateral magnitude increases occurs when UL activity becomes increasingly symmetrical and intense as a result of shared kinematic and kinetic properties between ULs. Examples of this kind of activity include folding towels and placing an object on a shelf with both hands. 16
Group-level data for nondisabled adults are presented in the upper half of Table 2. Group median values indicate that a large portion of real-world UL activity consisted of low-intensity activity that was completed using both ULs to a similar degree. IQR values for the bilateral magnitude (median = 176.5; IQR = 34.3 activity counts) and the magnitude ratio (median = 2.66; IQR = 1.53) demonstrate that the middle 50% of second-by-second values varied with respect to median values. Within-group analysis indicated that neither the median bilateral magnitude (Mann-Whitney U test: U = 349.0; Z = −0.3; P = .5) nor the median magnitude ratio (Mann-Whitney U Test: U = 306.0; Z = -01.0; P = .3) differed based on whether nondisabled adults were right- (n = 62) or left-hand (n = 12) dominant.
Values of Accelerometry-Derived Variables for Nondisabled Adults (n = 74) and Adults With Stroke (n = 48).
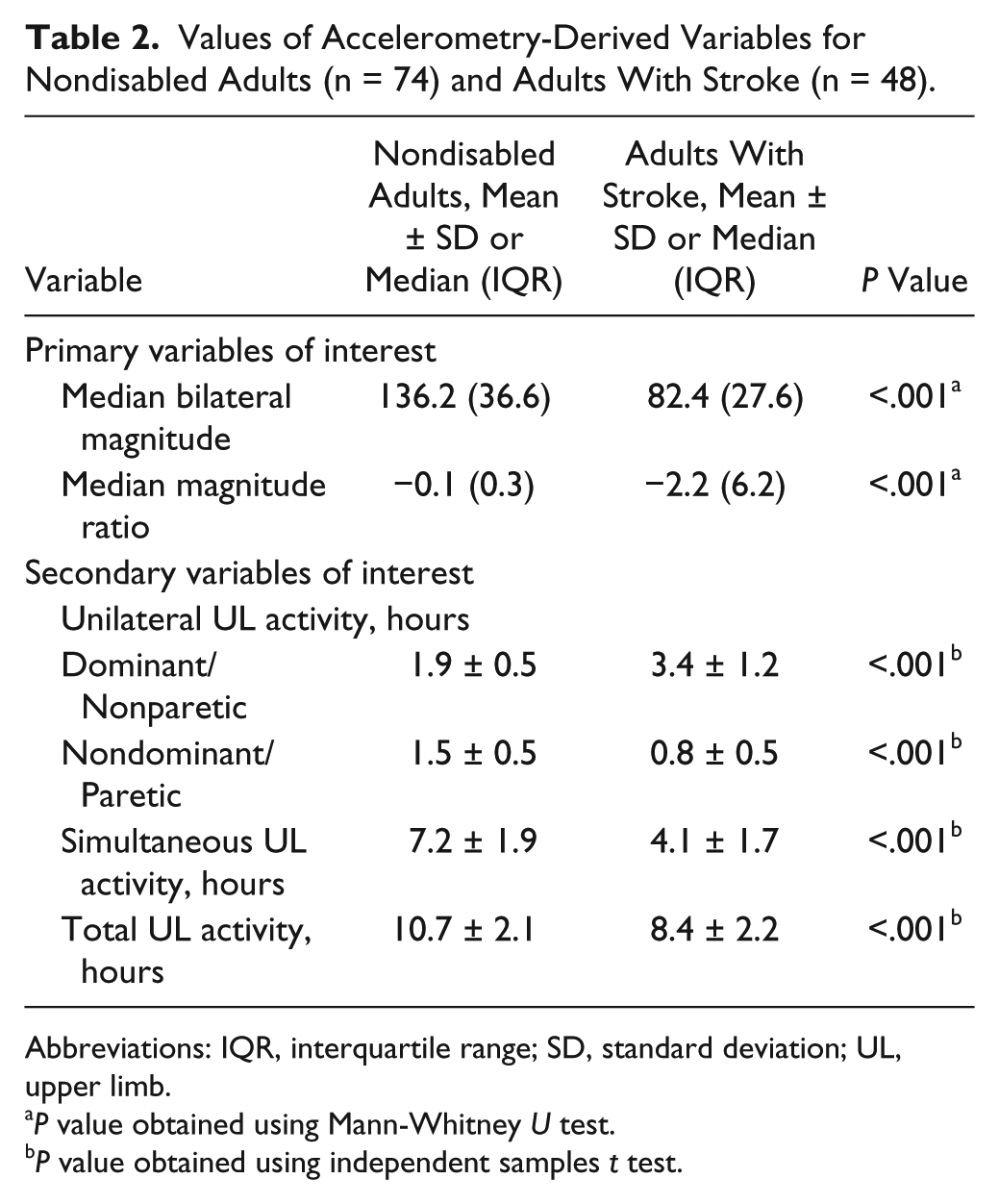
Abbreviations: IQR, interquartile range; SD, standard deviation; UL, upper limb.
P value obtained using Mann-Whitney U test.
P value obtained using independent samples t test.
Adults With Stroke
Data for 6 individual participants with stroke are presented in Figure 2. The left half of the figure displays data for participants with a paretic dominant UL, and the right half displays data for participants with a paretic nondominant UL. Each row displays data for participants with lower (top row), moderate (middle row), and higher (bottom row) motor capability as indicated by ARAT scores. Figure 2A shows data for a participant with low motor capability (ARAT = 10) whose median bilateral magnitude was 89.7 (IQR = 116.0) activity counts and median magnitude ratio was −7.0 (IQR = 5.85), indicating that real-world UL activity for this participant was of low intensity and completed mostly with the nonparetic UL. The IQR also indicates that second-by-second values varied with respect to median values. Visual inspection of the density plot reveals that both unilateral and simultaneous activity consisted mainly of nonparetic UL activity (magnitude ratio from −7 to 0). Paretic UL activity during unilateral (magnitude ratio = +7) and simultaneous activity (concavity observed for magnitude ratios from 0 to +6) was low.
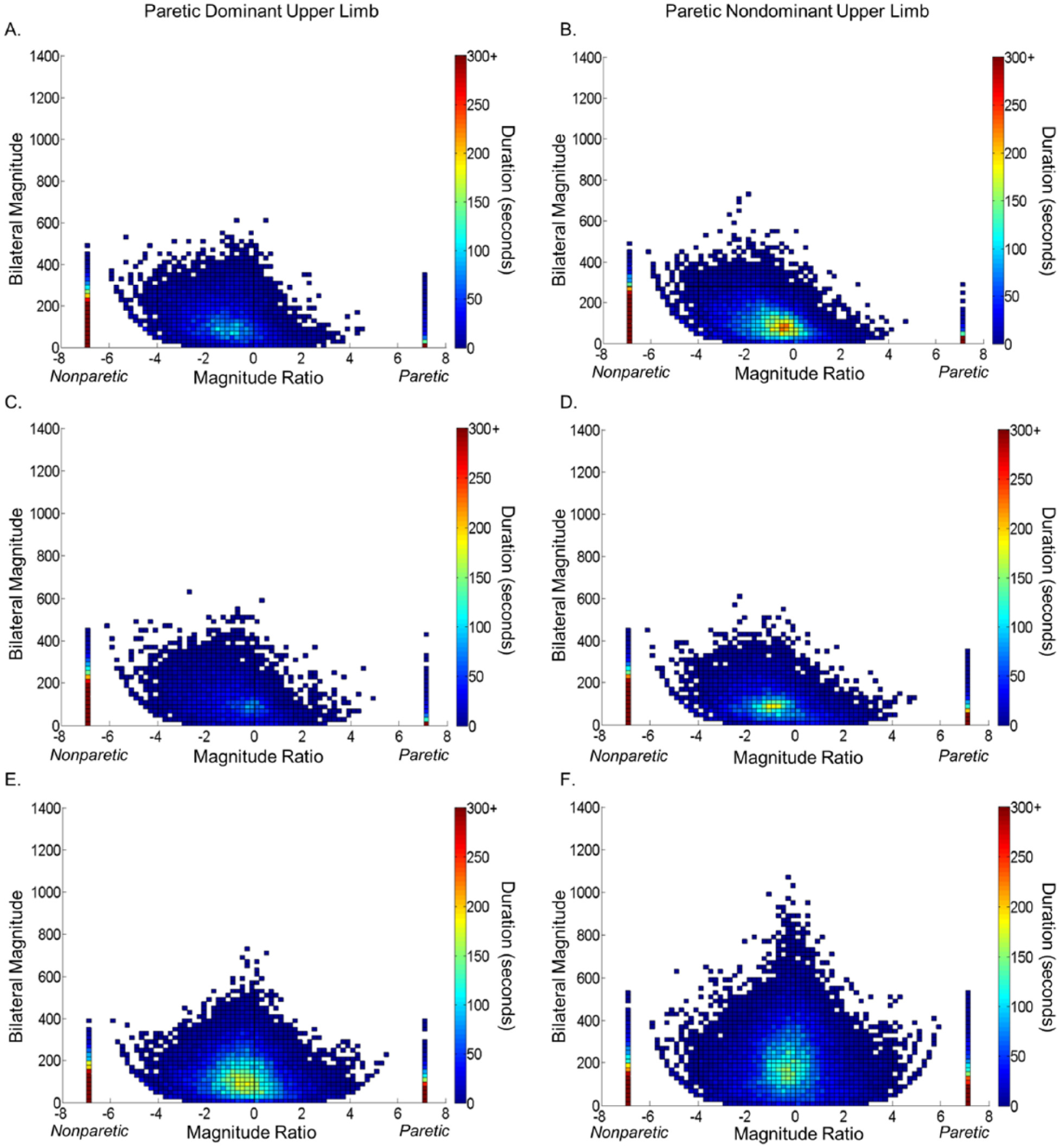
Density plots showing 26 hours of real-world bilateral upper-limb (UL) activity in 6 adults with stroke. Participants in the left-side column had paretic dominant ULs, whereas participants in the right-side column had paretic nondominant ULs. Individual data are displayed from participants with lower (A: Action Research Arm Test [ARAT] = 10; B: ARAT = 10), moderate (C: ARAT = 36; D: ARAT = 38), and higher motor capabilities (E: ARAT = 46; F: ARAT = 48). Despite higher ARAT scores, the participants in C and D have density plots similar to that of participants in A and B.
Figure 2B shows data for another participant with the same motor capability (ARAT = 10) and similar median bilateral magnitude (77.3 activity counts, IQR = 98.9) and magnitude ratio (−7.0, IQR = 6.03) values, but whose nondominant side was affected by stroke. Figures 2A and 2B are similar.
Figures 2C and 2D show data from participants with moderate motor capabilities, affected on the dominant (Figure 2C; ARAT = 36; median bilateral magnitude = 77.5 activity counts, IQR = 111.6; median magnitude ratio = −7.0, IQR = 6.0) and nondominant sides (Figure 2D; ARAT = 38; median bilateral magnitude = 66.3 activity counts, IQR = 87.0; median magnitude ratio = −7.0, IQR = 6.20), respectively. Despite greater motor capabilities, the data in Figures 2C and 2D look very similar to those in 2A and 2B.
Figures 2E and 2F show data from participants with higher motor capabilities, affected on the dominant (Figure 2E; ARAT = 46; median bilateral magnitude = 86.6 activity counts, IQR = 115.8; median magnitude ratio = −0.80, IQR = 5.24) and nondominant sides (Figure 2F; ARAT = 48; median bilateral magnitude = 133.4 activity counts, IQR = 186.6; median magnitude ratio = −0.5, IQR = 3.65), respectively. These statistics and the more symmetrical density plots more closely resemble data from nondisabled individuals in Figure 1. In addition to engaging in more simultaneous UL activity, the participant in Figure 2F also performed UL activity at greater intensities.
Group-level statistics, displayed in the upper half of Table 2, support visual examination of Figure 2. Median bilateral magnitude values in adults with stroke were lower than in nondisabled adults, indicating lower intensity of real-world UL activity. Median magnitude ratio values in adults with stroke were more negative than in nondisabled adults, indicating increased activity of the nonparetic UL relative to the paretic UL. IQR values for the bilateral magnitude (median = 115.9 activity counts; IQR = 34.3) and the magnitude ratio (median = 6.62; IQR = 1.2) demonstrate that the middle 50% of second-by-second values varied with respect to median values.
Differences were seen in 1 of the 2 primary variables based on whether the participants’ pre-stroke dominant UL was affected by stroke. There were no differences in median bilateral magnitude values between participants with paretic dominant (n = 26) versus nonparetic dominant (n = 22) ULs (Mann-Whitney U test: U = 225.0, Z = −1.3, P = .2). The median magnitude ratio was more negative, however, in participants with a paretic nondominant UL (median = −5.0, IQR = 5.6) than a paretic dominant UL (median = −0.88, IQR = 2.5; Mann-Whitney U Test: U = 148.5, Z = −2.9, P < .01). Motor capability (ARAT score) was weakly correlated 28 with median bilateral magnitude values (rs = 0.30; P = .04) and moderately correlated with median magnitude ratio values (rs = 0.66, P < .001; Figure 3). Visual analysis of Figure 3, however, illustrates that 33% (16/48) of participants had a median magnitude ratio of −7 (ie, at least 50% of total UL activity consisted of unilateral nonparetic UL activity) despite variable ARAT scores (range = 10-42), which underscores the distinction between capability and performance.
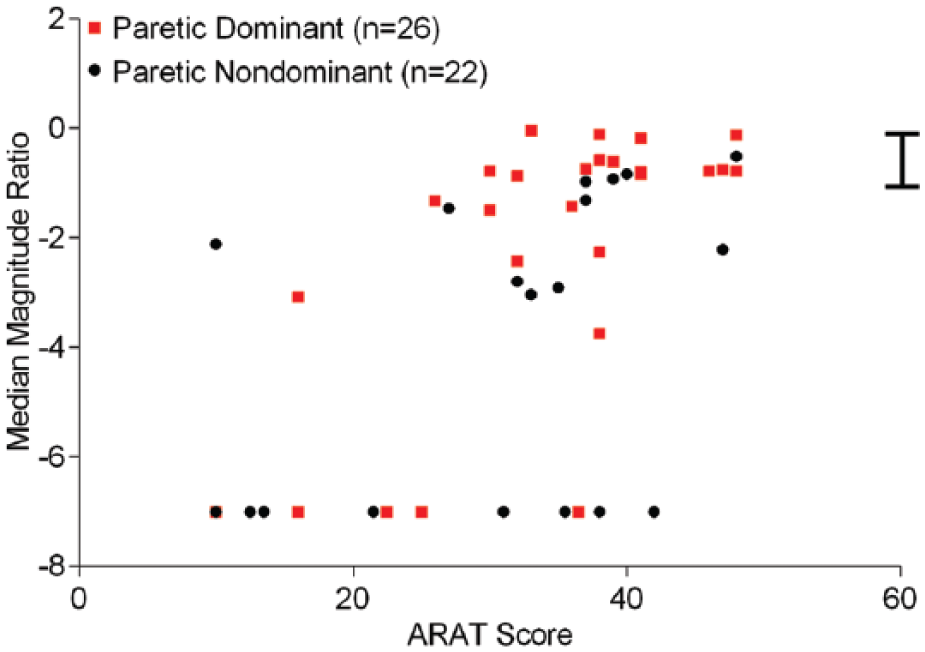
Scatterplot of ARAT score versus the median magnitude ratio for adults with stroke. Median magnitude ratio values were more negative in participants with a paretic nondominant UL (circles) than in participants with a paretic dominant UL (squares). There were 5 participants with a magnitude ratio of −7 and an ARAT score of 10. Despite a Spearman correlation of 0.66, 16/48 (33%) participants had a median magnitude ratio of −7, indicating that at least 50% of total UL activity consisted of nonparetic unilateral UL activity. The vertical hatched bar specifies the middle 50% (ie, 25th and 75th percentiles) of median magnitude ratio values in nondisabled adults.
Secondary Variables of Interest
Additional variables that quantified duration of UL activity by group are displayed in the lower half of Table 2. Duration of dominant/nonparetic UL activity was greater in adults with stroke than in nondisabled adults, whereas duration of nondominant/paretic UL activity was less. Simultaneous UL activity made up 67% (7.2/10.7 hours) of total UL activity in nondisabled adults but only 49% (4.1/8.4 hours) of total UL activity in adults with stroke. Even though nondisabled adults wore the accelerometers for 1 hour less (25 vs 26 hours), duration of simultaneous and total UL activity were greater in nondisabled adults than in adults with stroke.
Discussion
This study quantified real-world bilateral UL activity during a typical day in nondisabled adults and adults with chronic stroke using wrist-worn accelerometry. We calculated summary statistics that demonstrated that intensity of bilateral UL activity (bilateral magnitude) was lower and bilateral UL activity was more lateralized (the magnitude ratio was more negative) in adults with stroke than in nondisabled adults. Examination of individual- and group-level descriptive statistics (ie, median and IQRs) for bilateral magnitude and magnitude ratio values confirmed our hypothesis that second-by-second values varied greatly with respect to summary statistics. Visual representation of second-by-second UL activity using density plots supported this finding as well. Furthermore, the density plots clearly show that patterns of real-world bilateral UL activity differed between nondisabled adults and adults with stroke and importantly, between adults with stroke despite similar motor capabilities.
It was striking that in nondisabled adults, the dominant and nondominant ULs were active to a similar degree. This trend was observed in individual- and group-level (see Table 2) data. This observation challenges the assumption that the nondominant UL is used only to assist the dominant UL. Our results do not dispute the laboratory findings of others indicating increased dominant UL accuracy during the performance of dynamic tasks (eg, manipulating) and increased nondominant UL accuracy during the performance of static tasks (eg, stabilizing)29,30 or that the dominant UL can execute complex tasks more efficiently than the nondominant UL. 31 Rather, our results extend these laboratory results to provide evidence that complementary, usually simultaneous, actions of the ULs make up a significant portion of real-world, everyday UL activity.
It was not surprising that real-world bilateral UL activity was less symmetrical (lower magnitude ratios) and less intense (lower bilateral magnitudes) in adults with stroke compared with nondisabled adults. Inside the laboratory, Han et al 8 demonstrated increased use of the nonparetic UL during a spontaneous reaching task. Similarly, Uswatte et al 17 used accelerometry to calculate the ratio of paretic-to-nonparetic UL movement in adults with stroke and demonstrated that duration of paretic UL movement was less than nonparetic UL movement (ie, ratio of paretic-to-nonparetic movement = 0.56). The observation by Uswatte et al has now been confirmed across many studies.15,20,21,32 The lower duration of simultaneous UL activity and higher duration of nonparetic unilateral UL activity in adults with stroke compared with nondisabled adults in this study is a further indication that real-world bilateral UL activity is reduced in adults with stroke.
At first glance, one may wonder if the reduction in bilateral UL activity is a direct result of motor capability. We observed moderate associations between ARAT scores and median bilateral magnitude and magnitude ratio values, and we also observed similar density plots from participants with varying ARAT scores. These results imply that motor capabilities are not necessarily a direct reflection of real-world performance and may be an objective quantification of the phenomenon of learned nonuse described by Taub and others.33-35 The findings here from people living in the community are consistent with findings from an inpatient rehabilitation setting, 36 where improvements in paretic UL motor function, as measured by clinical tests of function, were not associated with increased daily use of the paretic UL, as measured by accelerometry. Together, our results and others highlight the critical point that objective quantification of real-world performance is imperative in both rehabilitation research and clinical practice.
Prestroke hand dominance affected real-world bilateral UL activity in this study. Paretic UL activity was lower than nonparetic UL activity to a greater degree (ie, median magnitude ratios were more negative) in participants with a paretic nondominant UL. We speculate that this was because participants still had full functional use of their dominant UL to complete daily activity and, therefore, were less motivated to use their paretic nondominant UL, whereas individuals whose dominant UL was affected by stroke were more motivated to regain functional use of their dominant UL. A similar explanation was given by Harris and Eng 37 after observing less impairment in the paretic UL of adults with chronic stroke when the dominant side was affected. These explanations are also consistent with our earlier observation that duration of paretic UL activity was greater in adults whose dominant UL was affected (ie, ratio of paretic-to-nonparetic UL activity = 0.70) than in adults whose nondominant UL was affected (ratio = 0.57). 15
Three limitations may alter the interpretation of our data. First, adults with stroke wore the accelerometers for 1 hour longer than did nondisabled adults for practical reasons. Despite the longer wearing duration, we still observed clear differences between groups. It is possible that the magnitude of those differences likely would have been greater had nondisabled adults worn the accelerometers for an additional hour. Second, despite the 0.25- to 2.5-Hz filter of ActiLife 6, abrupt accelerations while a passenger was in a moving car were recorded during preliminary tasks (unpublished data), resulting in potential overestimation of UL activity. The risk of overestimation is small, however, because the participants in this study spent a majority of their time in sedentary activity.15,24 Third, the effect of walking on UL activity was not reported in this study. Because walking was included, the values presented here might be considered overestimations of real-world UL activity, though overestimation is likely to be low because of the sedentary nature of the participants. There are distinct advantages related to cost, availability of accelerometers, patient and clinician compliance, and simplifying data processing when only wrist-worn accelerometers are used. Future research, however, should examine the effect of walking on real-world UL activity.
Conclusions
Simultaneous UL activity makes up a significant portion of daily activity in nondisabled adults. This finding alone has significant implications for how interventions are selected and delivered to patients with stroke (eg, task-specific training with both hands instead of just one). Results from community-dwelling participants with stroke highlight the importance of assessing UL activity outside of the clinic and not simply motor capability inside the clinic or laboratory. If the goal of rehabilitation following stroke is to improve daily function, then UL activity in a patient’s real-world environment must be assessed. We show that this can feasibly be accomplished via calculation of the bilateral magnitude, magnitude ratio, and density plots obtained from accelerometry data. Finally, measuring real-world UL activity over time will help patients, clinicians, and researchers assess recovery of real-world UL motor performance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Washington University Institute of Clinical and Translational Sciences (Grant UL1 TR000448) from the National Center for Advancing Translation Sciences of the National Institutes of Health (NIH). Additional NIH support included T32 HD7434-18, TL1 TR000449, and R01 HD068290.