
Abstract
Background. While wrist-worn accelerometers have been used to measure upper extremity use in the past, they primarily measure arm motion and lack the ability to capture functional hand opening and grasping activities which are essential for activities of daily living. Objectives. To characterize real-world functional hand opening and grasping activities captured over multiple days in adults with stroke and in matched controls using a novel wrist-worn device. Methods. Twenty-eight individuals (fourteen individuals with stroke and 14 healthy controls) wore the devices on both wrists for 3 days. Functional hand activity was characterized by daily hand counts, hourly hand counts, and asymmetry between hands. The Mann–Whitney U test was used to evaluate differences in functional hand activities between the two groups. Results. The stroke group had 1480 and 4691 daily hand counts in their affected and nonaffected hands, respectively. The control group had 3559 and 5021 daily hand counts in their nondominant and dominant hands, respectively. Significantly fewer daily hand counts (P = .019), fewer hourly hand counts (P = .024), and a larger asymmetry index (P = .01) of the affected hand in the stroke group were found compared to that of the nondominant hand in the control group. Conclusions. Real-world functional upper extremity activity can be measured using this novel wrist-worn device. Unlike wrist-worn accelerometers, this wrist-worn device can provide a measurement of functional grasping activity. The findings have implications for clinicians and researchers to monitor and assess real-world hand activity, as well as to apply specific doses of repetitions to improve neural recovery after stroke.
Introduction
About 88% of individuals with stroke experience long-term functional impairments of their affected upper limb, 1 limiting their ability to perform activities of daily living and negatively influencing their quality of life. Clinical guidelines, systematic reviews, and meta-analyses2-5 provide strong evidence in support of intensive repetitive task-oriented and task-specific practice for poststroke rehabilitation. The number of repetitions is a critical component driving neural plasticity, ultimately leading to functional recovery. 6
Animal studies on neuroplasticity after stroke suggest hundreds of repetitions of challenging grasp movements per day can promote changes in the brain.7,8 However, the amount of movement practice provided during stroke rehabilitation has been shown to be small compared to that obtained in animal studies. 9 The optimal number of repetitions to maximize functional recovery and drive neural plasticity is unknown. Quantifying the repetitions of functional hand movements is essential for monitoring and determining the optimal dose for poststroke upper extremity (UE) rehabilitation.
Accelerometers have been widely used to quantify the number of steps in walking 10 and UE activity. 11 Normative data indicate that a daily walk of 4000-18,000 steps is typical in healthy adults, 12 and such information is useful for exercise prescription in rehabilitation. For example, the Centers for Disease Control and Prevention suggests the daily target of 10,000 steps. 13 Although wrist-worn accelerometers can also provide information on UE use, such as duration and magnitude, it calculates UE use based on the acceleration of the forearm, not based on any hand motion. 14 The ability to open and close the hand is essential for activities of daily living. Grasp movements are also easy for a consumer to understand, similar to a pedometer which captures step counts.
Our previous study showed that a novel wearable wrist-worn device, TENZRTM Neuro Tracker, is able to reliably and consistently detect the number of repetitions of functional grasp movements for 12 discrete tasks over 30 repetitions each in individuals with stroke. 15 The purpose of the study is to measure functional grasp movements in individuals with chronic stroke and healthy controls throughout all activities over multiple days using a novel wrist-worn device, TENZRTM Neuro Tracker. This study is the first to provide preliminary daily metrics of functional grasp movements. We hypothesized that 1) it is feasible to use the device to characterize the amount of functional grasp movements over multiple days, and 2) less functional hand activities in the affected UE would be found in individuals with stroke than the controls.
Methods
Participants
Twenty-eight individuals were recruited: fourteen adult community-dwelling individuals with stroke and 14 age- and sex-matched controls. Sample size estimation was based on information from a previous study 16 that showed significant differences (effect size of 1.4) in the duration of use between the affected UE in stroke participants and nondominant UE in controls. With 90% power and an alpha of .05, thirteen participants per group were required. The data were collected in the home and community setting. Participants with stroke were eligible if they (1) were >18 years old; (2) had a stroke more than 3 months ago; (3) were right-hand dominant by self-report, (4) had difficulty using the affected UE; (5) had some voluntary movement in the affected UE, including the ability to lift the affected arm to chest level and hold for 5 seconds, some ability to extend the affected wrist, and some ability to grasp and release an object such as a cup handle; (6) were living in the community; (7) were able to understand and follow instructions. Stroke participants with severe pain that prevented movement in the affected UE were excluded. Control participants were eligible if they (1) were >18 years old; (2) were right-hand dominant by self-report; (3) had no neurological conditions besides a stroke; (4) had no musculoskeletal disorders affecting the UE. Participants gave written informed consent to participate. The University of British Columbia Research Ethics Boards approved the study protocol (H13-01301).
Device
A minimal viable product of the wrist-worn device (TENZRTM Neuro Tracker V4. X, BioInteractive Technologies Inc.) (Figure 1) was used. A minimal viable product is a version with sufficient features to be usable by initial customers to provide feedback to improve the product. The TENZR Neuro Tracker is a custom version of the TENZR sensing wristband, developed by BioInteractive Technologies for this application. The device uses a multi-sensor sensing approach to detect reach-to-grasp activity. A key component of the technology is Force Myography, a method to detect the state of the hand by monitoring the surface forces on the wrist musculo-tendonous complex proximal to the hand. The sensing principle underlying the Force Myography technique is that a musculo-tendonous complex will stiffen as the muscles within it contract. In Force Myography, pressure sensors are used to measure the surface stiffness of the musculo-tendonous complex which is indicative of the contraction status of the muscles within the complex.
17
The Force Myography signal, captured by the device at the wrist, is sensitive to both (1) finger movement and grip force exertion and (2) wrist movement. In the case of the TENZR device, the Force Myography sensors are configured to detect a change in wrist angle and finger/grip activity within a rolling window, that is, to detect a change in amplitude of the Force Myography signal indicative of finger/grip and wrist movement activity. The system outputs a hand count (ie, a functional reach-to-grasp movement is detected) in the event that inertial movement of the arm is detected before or after the finger/grip and wrist activity.15,18 The combination of an arm reaching movement and a hand grasping/releasing movement approximates the initial interaction with an object (ie, reach and grasp) and/or final interaction with an object (ie, release and arm move away). For the device to detect a subsequent distinct hand count, a slight pause of .1–.2 seconds in between the next reach and grasp movements is required. The system has been configured to be as sensitive as possible to the changes in wrist and finger/grip activity in relation to the baseline noise present in the signals. A key drawback of this configuration is that the system is unable to distinguish between different types of grasp types and object interactions with minimal wrist and finger/grip movements which could produce signals below the configured sensitivity and hence may be undetected. The sensitivity of the system to a representative sample of reach to grasp-type activities and the appropriate lack of sensitivity (ie, true negatives) of the system to just arm movements was confirmed in a series of studies.18-20” Our previous study with a small sample of mild-to-moderately impaired stroke participants showed that the device is able to capture hand counts over a limited set of tasks up to 30 repetitions with good reliability and accuracy.
15
For example, we showed that pouring water resulted in an average of 2 hand counts due to the forward reach with hand grasp and then release and move away.
15
Image of TENZR device for the right hand. Labels indicating the right elbow and right hand were to ensure the correct orientation and placement of the device.
Procedures
All participants were asked to wear one device on both wrists continuously during waking hours for 3 days in their daily lives. Participants were asked to take off and charge the devices before going to sleep and put the devices on once they woke up. We did not discriminate between weekend or weekdays as we expected most of the counts to be generated during activities of daily living (eg, self-care and meal preparation). As the devices were not waterproof, participants were asked to take off the devices for water-related activities (eg, swimming), showering, and washing dishes. Participants were instructed to record the time on an activity log (Supplemental Appendix 1) when they took off the devices and put back on again. An information sheet that contained the instructions on the wearing schedule, device charging, and activity logs was provided to ensure compliance. Individuals with stroke also completed two clinical assessments on a separate day and when the devices were not worn. The Fugl-Meyer Upper Extremity Assessment (FM-UE) 21 was administered to characterize UE impairment. The Rating of Everyday Arm-use in the Community and Home (REACH) Scale 22 was used to characterize how the affected UE was being used in their daily lives. The REACH scale is a self-report measure that has two separate scales; one for dominant-side stroke and the other for nondominant-side stroke. Both scales have 6 categories of use that range from “No Use” to “Full Use.”
Data Analysis
Functional hand activity was characterized by daily hand counts (counts/day), hourly hand counts (counts/hour), and an asymmetry index. Daily hand counts represent the total hand counts recorded over the 3-day period divided by the number of days worn. Hourly hand counts were determined to account for variation in hand counts due to differences in wearing time and were calculated by total hand counts divided by number of hours worn. Wearing time was determined by visually inspecting the data to confirm that the devices were worn for the planned time period and that the data matched the activity log. For individuals with stroke, the asymmetry index was calculated by taking the value of the difference between the unaffected and affected UE hand counts and dividing by the sum of them [(nonaffected − affected hand counts)/(nonaffected + affected hand counts)]. For healthy controls, the asymmetry index was calculated by taking the index between the value of the difference between the dominant and nondominant UE hand counts and the sum of them [(dominant − nondominant hand counts)/(dominant + nondominant hand counts)]. An asymmetry index equal to zero suggests that both UEs had the same hand counts. A positive asymmetry index indicates that the nonaffected UE (or dominant hand in the healthy controls) had more hand counts compared to the affected UE (or nondominant hand in the healthy controls). In contrast, a negative value indicates that the nonaffected UE (or dominant hand in the healthy controls) had fewer hand counts compared to the affected UE (or nondominant hand in the healthy controls).
Statistical Analysis
Descriptive analysis (mean, standard deviation, frequency, and range) was used to summarize participant characteristics. Independent t-tests were used to evaluate the differences in age and wearing time between the stroke and control groups. The Mann–Whitney U test was done to compare daily hand counts, hourly hand counts, and the asymmetry index between the stroke and control groups. The Spearman rank correlation coefficient was used to examine the relationship between the asymmetry index and the FM-UE. The Wilcoxon Signed Ranks Test was done to evaluate differences in hand counts between the weekdays and weekends. Significant level was set as P < .05. SPSS 25.0 (IBM, Armonk, NY, USA) was used for statistical analysis.
Results
Participants Characteristics.
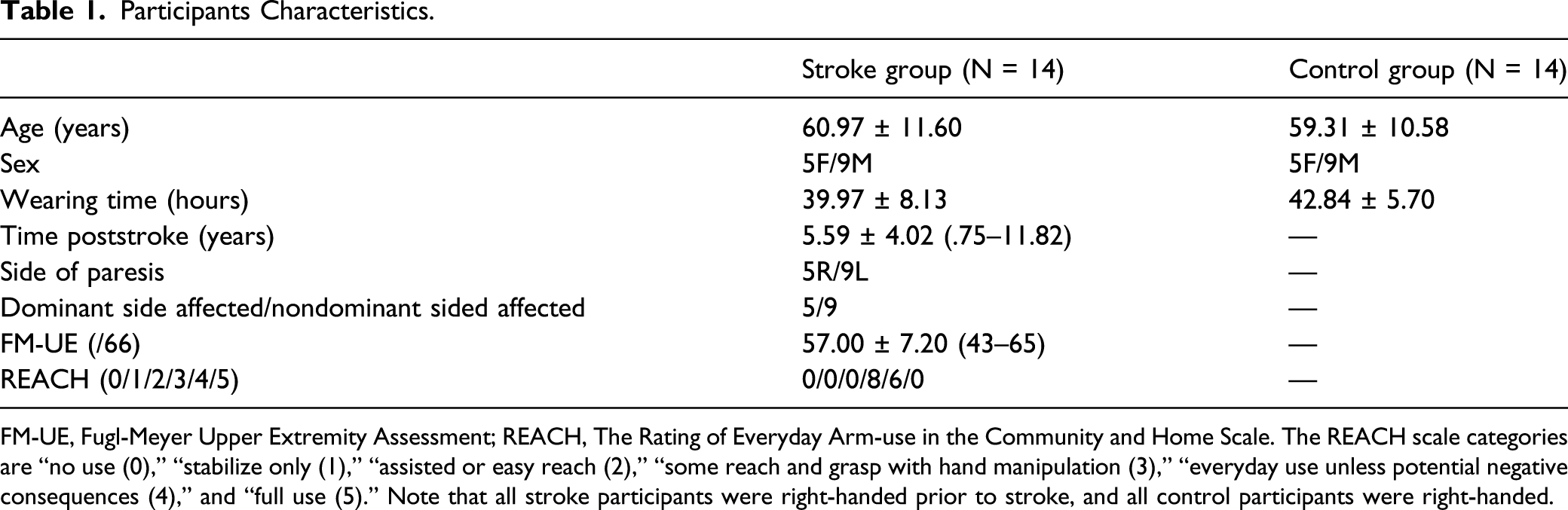
FM-UE, Fugl-Meyer Upper Extremity Assessment; REACH, The Rating of Everyday Arm-use in the Community and Home Scale. The REACH scale categories are “no use (0),” “stabilize only (1),” “assisted or easy reach (2),” “some reach and grasp with hand manipulation (3),” “everyday use unless potential negative consequences (4),” and “full use (5).” Note that all stroke participants were right-handed prior to stroke, and all control participants were right-handed.
Feasibility
Some device failures incurred with the minimal viable product of the wrist-worn device. Device failures included synchronization issues between the wrist-worn device and the software, charging problems, and hardware durability. An interactive process of trial and error was adopted by the research team and the company to improve these issues and ensure that the devices and software performed appropriately before given to the participants. These technical issues were resolved prior to the participants starting the study. However, after the study started, 2 participants reported that the devices did not charge appropriately, and 1 participant reported that the Velcro strap came off. A repair to the device or a replacement for the device was provided in a timely manner to avoid data loss.
Compliance
While some participants (N = 4) reported sweat, tightness, or irritation in their wrists while wearing the devices, all but two participants (N = 26) were compliant to wear the devices for 3 days during their waking hours. One participant in the stroke group and one participant in the control group only wore the devices for two days due to forgetfulness and discomfort while wearing the devices.
Comparison Between Individuals With Stroke and Controls
Figure 2 shows frequency distributions of the daily hand counts of the stroke participants and controls. The distribution of the affected hand counts of the stroke participants is moderately positively skewed (Figure 2A), while the distribution of the nonaffected hand counts of the stroke participants is approximately symmetric (Figure 2B). The distributions of the nondominant and dominant hand counts of the controls are approximately symmetric (Figure 2C and 2D). Histograms of daily counts of stroke participants and controls. 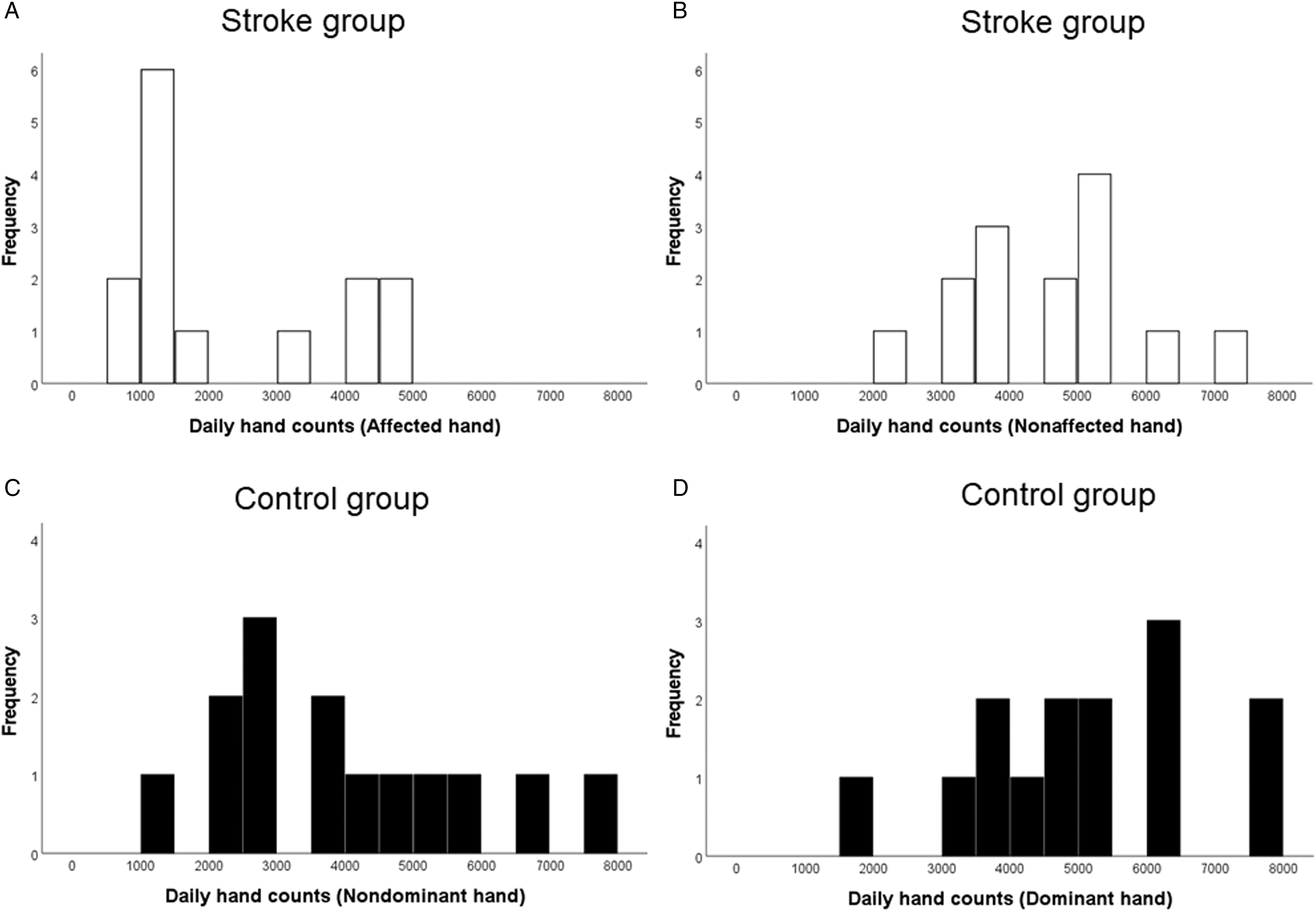
Median (IQR) (Range) and Statistical Results of Functional Hand Activity Variables.
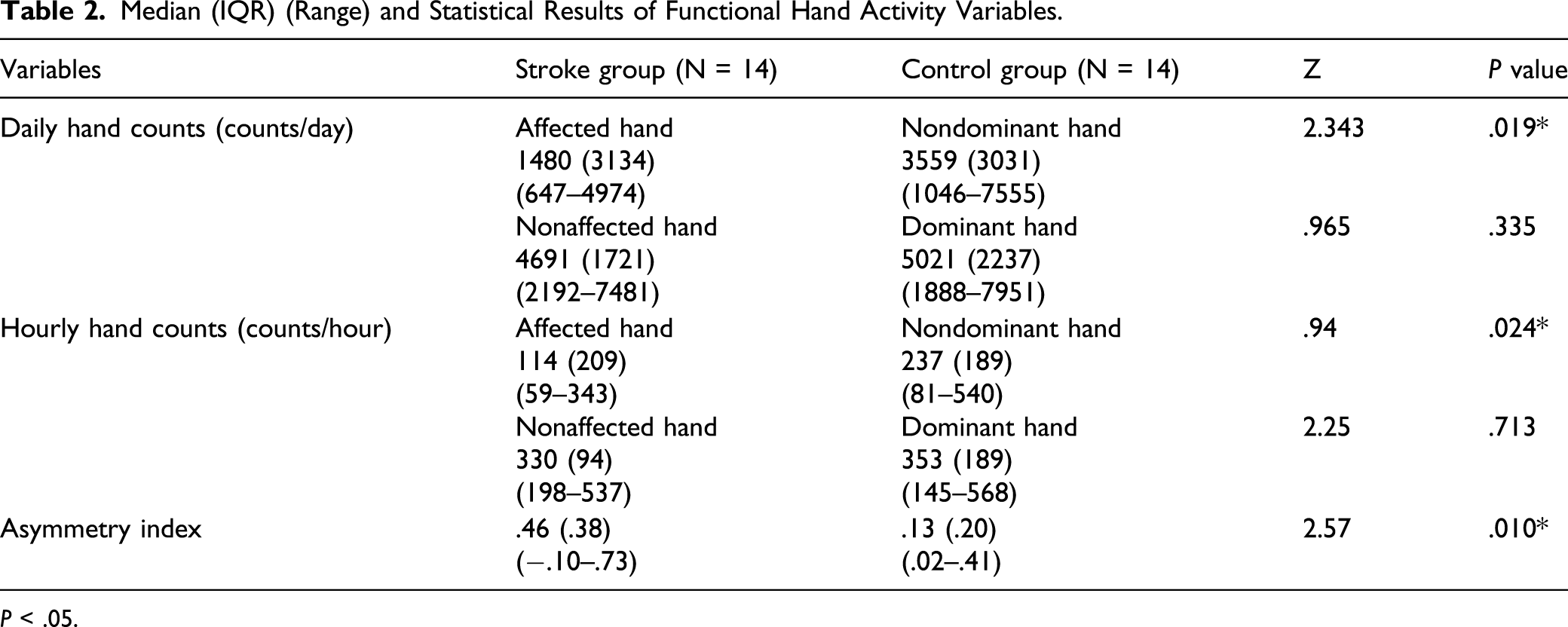
P < .05.
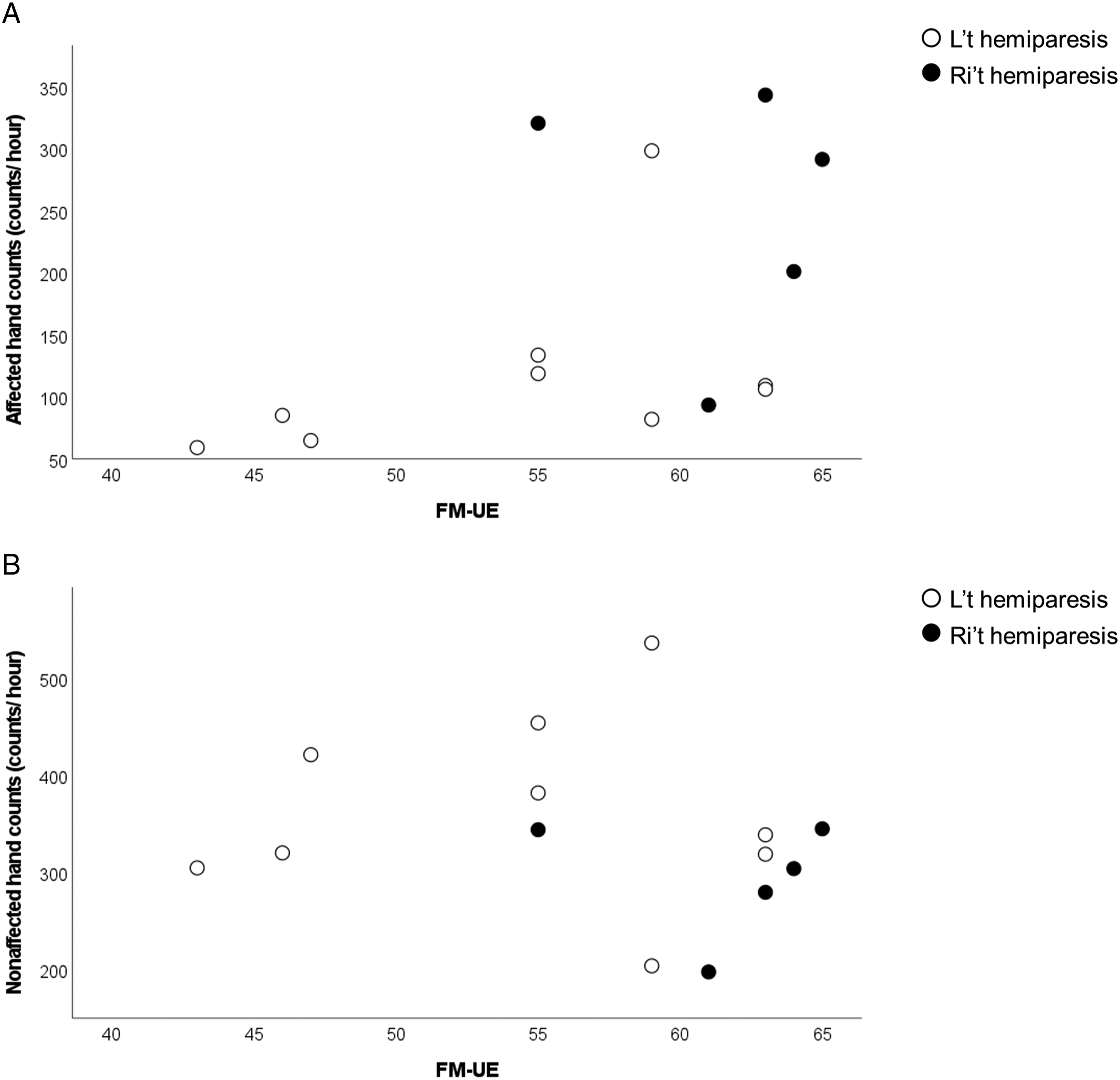
A significantly strong and negative Spearman’s rank-order correlation was found between FM-UE and the asymmetry index (ρ = −.70, P = .005) (Figure 3), indicating that stroke participants with more severe UE motor impairment (lower FM-UE score) had less functional hand activities of the affected hand (larger asymmetry index). There was no significant correlation between the FM-UE scores and hourly hand counts of the affected hand (P = .059) or that of the nonaffected hand (P = .361) (Figure 4). Graphical representations of Spearman Correlation (ρ) test between the FM-UE score and the asymmetry index. Asymmetry index values were closer to 0 in participants with right-sided hemiparesis (black circles) than in participants with left-sided hemiparesis (white circles), indicating a more symmetrical use between both UEs. Note that all participants were right-handed prior to stroke. Scatterplots of the FM-UE score vs 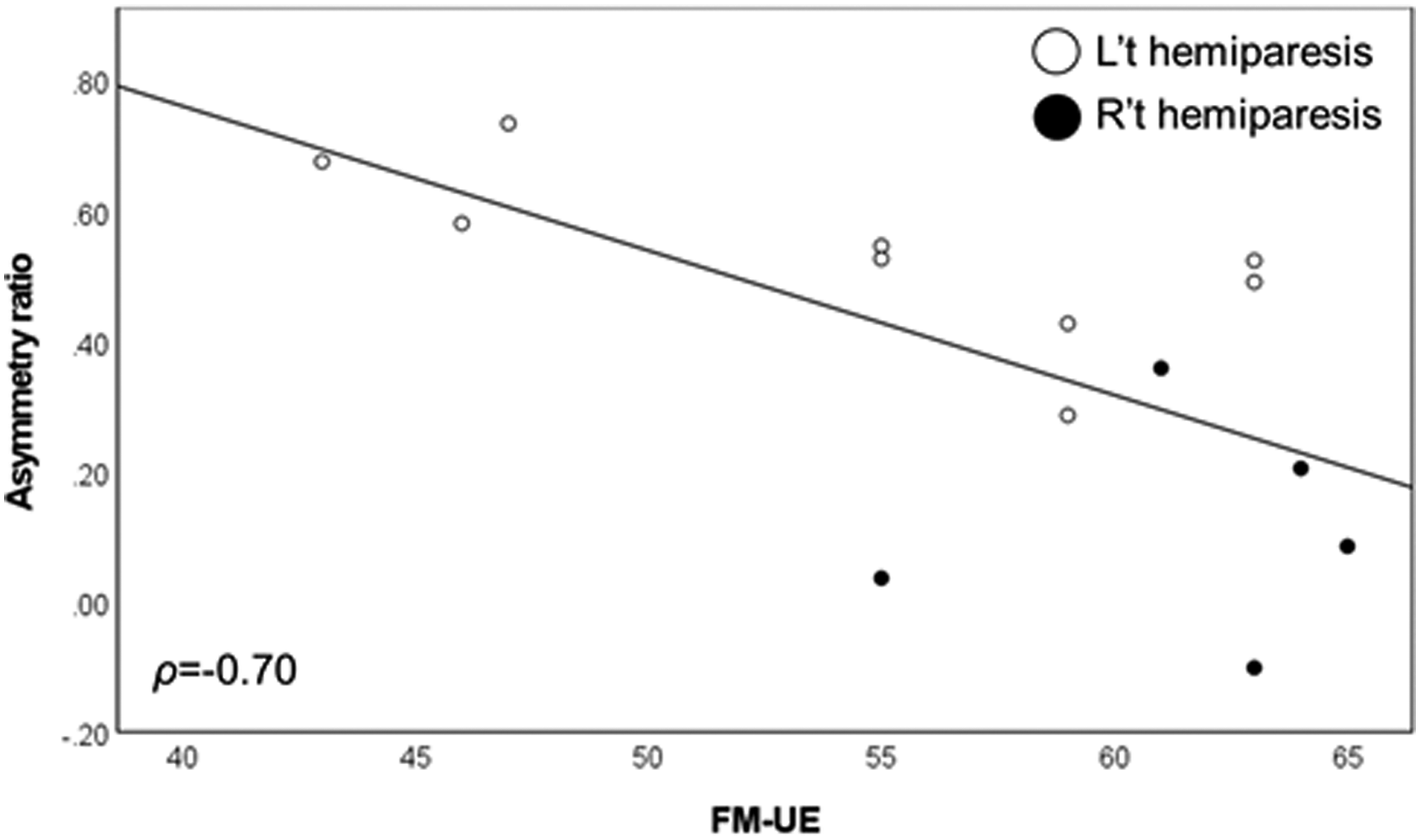
Effect of Hand Dominance in Individuals With Stroke
Visual analysis of Figure 3 illustrates that participants with right-sided hemiparesis (N = 5) had an asymmetry index closer to zero compared to participants with left-sided hemiparesis (N = 9), indicating more equal functional use in both hands, despite similar FM-UE scores (range = 55-65). Visual analysis of Figure 4 reveals that, despite similar FM-UE scores, there is no clear difference in the affected or nonaffected hourly hand counts between right-sided and left-sided hemiparesis.
Discussion
Our study demonstrated that a novel wrist-worn device could capture functional reach-to-grasp movements among individuals with mild impairment after stroke in their everyday lives. This is the first study to present preliminary daily metrics of functional hand activities in individuals with stroke and matched controls in the real-world environment using a novel wrist-worn device. It also extends our previous research on using the novel wrist-worn device, TENZRTM Neuro Tracker, to capture functional hand repetitions in a controlled laboratory setting. 15 The findings support our hypothesis that it was feasible to use the device to measure the amount of functional grasp movements over multiple days in the home and community setting. We also found that stroke participants demonstrated less functional hand activities (ie, reach-to-grasp movements) in the affected UE compared to their age- and sex-matched controls.
Research studies and rehabilitation clinical practice have been using tools such as step counters to record the dose of intervention, provide accountability to patients, and improve motivation by providing feedback on walking activity and setting daily goals. 23 While wrist-worn accelerometers can provide an objective measure for the magnitude and duration of arm movements, the devices are not able to capture purposeful hand grasping activities. A large disparity in the amount of daily functional UE activity was found between stroke participants with mild impairment and healthy controls. Individuals with stroke had 1500 grasp movements on their affected side per day, whereas healthy controls typically had 3500–5000 grasp movements per day. These findings provide preliminary reference values on real-world functional hand use. Although previous studies have assessed functional UE activity through self-report assessments 24 and wrist-worn accelerometers, 14 these estimations may be biased due to the subjective nature of self-report 25 and by the fact that accelerometry captures arm but not hand movement. While animal studies have suggested that hundreds of repetitions are needed to induce neuroplastic changes in the brain,7,8 and meta-analyses have demonstrated that large doses of therapy are positively correlated with clinically meaningful improvements, 26 the current dose of poststroke UE rehabilitation is far less than those achieved in animal studies and clinical trials. 27 As the optimal number of repetitions to facilitate changes in the brain and functional recovery following stroke remains elusive, the data provided in our study provide preliminary reference values that can be used by clinicians to set therapeutic goals, monitor treatment progress, and record exercise dose for poststroke UE rehabilitation. However, larger samples are required to establish population-based norms.
The findings of this study are partially consistent with previous studies which used wrist-worn accelerometers to capture real-world UE use. Similarly, other studies have found a reduction of activity of the affected UE in adults with stroke compared with healthy controls, and found a similar correlation between the amount of use and UE impairment.16,28 However, the amount of use captured by wrist-worn accelerometers between both UEs of individuals with and without stroke in previous studies appears to be higher compared to our results. Previous studies using wrist-worn accelerometers have shown that individuals with stroke with mild impairment used their affected UE 60–80% of the amount found on the nonaffected side,28-30 while our findings found values of approximately 30% (daily hand counts of the affected hand: 1480, daily hand counts of the nonaffected hand: 4691). Likewise, we found that healthy controls used their nondominant hands approximately 70% of the amount found on the dominant side (daily hand counts of the nondominant hand: 3559, daily hand counts of the dominant hand: 5021), whereas previous studies demonstrated that the dominant and nondominant UEs were used to a similar degree.16,28 Although wrist-worn accelerometers have been used widely to quantify UE activities in the real-world environment, 14 the movement detected by accelerometers is not capturing purposeful UE functional movements. Accelerometers measure the acceleration of the body segment, which is typically the distal forearm in poststroke UE studies 24 ; therefore, wrist-worn accelerometers might overestimate the amount of functional upper extremity movements which involve the hand. The novel wrist-worn device (TENZRTM Neuro Tracker) used in this study identifies functional grasp movements when the device detects arm movement (ie, arm acceleration captured by inertial movement units) before or after sensing both wrist activity (ie, wrist flexion/extension detected by proximity sensors) and hand activity (ie, a change in the force myography signal pattern). While we cannot rule out the possibility of other factors (eg, inclusion/exclusion criteria, sample sizes, time poststroke, etc.) that may contribute to the differences in the amount of UE use between our study and other studies, our results highlight the critical need for the novel wrist-worn devices (TENZRTM Neuro Tracker) to provide objective and clinically interpretable information on real-world functional hand use.
While our results indicate that more severe UE impairment may result in less functional use in the affected hand, it also appears that real-world functional hand use is influenced by whether the stroke is on the dominant or nondominant upper extremity side. We found that individuals whose dominant UE was affected by stroke used both sides more equally than individuals whose nondominant side was affected by stroke. It is possible that participants with an affected dominant UE were more motivated to use their affected UE, while participants with an affected nondominant UE were dependent on their dominant UE to carry out daily activities. Similar findings were found in two previous studies by Baily et al11,16 with larger samples.
Beyond the clinical implications of this study, the novel wrist-worn device used in this study will be useful for rehabilitation researchers. The use of the novel wrist-worn device to measure functional hand activities could be used in conjunction with a self-report questionnaire to provide a comprehensive picture of real-life functional UE performance. From engineering and manufacturing perspectives, the device could be coupled with a user interface that provides patients with feedback to increase the functional use of their UE and keep them accountable to the treatment goals.
Limitation
There are some limitations to acknowledge. First, the sample size is relatively small. Second, participants may have felt compelled to increase their UE activities when wearing the wrist-worn devices, which could have led to an overestimation of functional UE use. In addition, we observed substantial differences in individuals with mild impairment and healthy controls; it is likely that functional grasping activity would produce huge differences between people with more severe stroke and controls. Future studies should examine whether the TENZRTM Neuro Tracker can capture functional grasp activities in stroke participants with severe UE impairment or other clinical populations with UE impairment. Last, the results of the study are only generalizable to right-handed people or previously right-handed stroke participants. In addition, the number of left-hand affected and right-hand affected stroke participants was not balanced in this study. Studies have shown that there are differences in motor and functional performance between the dominant and nondominant hands,31-33 and hand dominance may have effects on affected UE function following stroke. 34 Future studies including a larger sample of right- and left-hand dominant participants to perform a variety of daily activities would increase the generalizability of these findings.
Conclusions
This study undertook a preliminary examination of daily metrics of functional UE use (ie, reach-to-grasp) in individuals with stroke and healthy controls by using a novel wrist-worn device. Individuals with stroke typically had 1500 reach-to-grasp movements in their affected hand per day, and healthy controls had 3500 and 5000 reach-to-grasp movements in their nondominant and dominant hands, respectively. These reference values provide objective information on functional UE use in the real-world environment, which can be used to set treatment goals. Moreover, the novel wrist-worn device used in this study can be a useful tool to record the dose of UE practice for research and clinical practice and provide motivation and accountability to patients.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683211041312 – Supplemental Material for Real-World Functional Grasping Activity in Individuals With Stroke and Healthy Controls Using a Novel Wearable Wrist Sensor
Supplemental Material, sj-pdf-1-nnr-10.1177_15459683211041312 for Real-World Functional Grasping Activity in Individuals With Stroke and Healthy Controls Using a Novel Wearable Wrist Sensor by Chieh-ling Yang, Johnson Liu, Lisa A. Simpson, Carlo Menon and Janice J. Eng in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgment
We gratefully acknowledge the research participants.
Declaration of Conflicting Interests
Dr. Menon has a vested interest in commercializing the technology and may benefit financially from its potential commercialization through BioInteractive Technologies. The other authors report no conflicts.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Heart and Stroke Foundation Canadian Partnership for Stroke Recovery (Post-doctoral award to CY), Canada Research Chair Program (JJE), Canadian Institutes of Health Research (Operating Grant FDN 143340 to JJE), Collaborative Health Research Project from the Canadian Institute of Health Research (CPG-170611 to JJE) and Natural Sciences and Engineering Research Council of Canada (CHRP 549589-20 to JJE).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.