
Abstract
Background. Optimal physical therapy strategies to maximize locomotor function in patients early poststroke are not well established. Emerging data indicate that substantial amounts of task-specific stepping practice may improve locomotor function, although stepping practice provided during inpatient rehabilitation is limited (<300 steps/session). Objective. The purpose of this investigation was to determine the feasibility of providing focused stepping training to patients early poststroke and its potential association with walking and other mobility outcomes. Methods. Daily stepping was recorded on 201 patients <6 months poststroke (80% < 1 month) during inpatient rehabilitation following implementation of a focused training program to maximize stepping practice during clinical physical therapy sessions. Primary outcomes included distance and physical assistance required during a 6-minute walk test (6MWT) and balance using the Berg Balance Scale (BBS). Retrospective data analysis included multiple regression techniques to evaluate the contributions of demographics, training activities, and baseline motor function to primary outcomes at discharge. Results. Median stepping activity recorded from patients was 1516 steps/d, which is 5 to 6 times greater than that typically observed. The number of steps per day was positively correlated with both discharge 6MWT and BBS and improvements from baseline (changes; r = 0.40-0.87), independently contributing 10% to 31% of the total variance. Stepping activity also predicted level of assistance at discharge and discharge location (home vs other facility). Conclusion. Providing focused, repeated stepping training was feasible early poststroke during inpatient rehabilitation and was related to mobility outcomes. Further research is required to evaluate the effectiveness of these training strategies on short- or long-term mobility outcomes as compared with conventional interventions.
Introduction
Although the majority of stroke survivors recover some walking function, most walk at slower speeds and for limited distances.1,2 Impaired locomotor function is a primary cause of decreased physical activity and community participation,3,4 which contribute to development of secondary complications. 5 Many interventions to improve locomotor function poststroke have been investigated. Unfortunately, some of the more common physical therapy strategies have demonstrated limited success, including traditional techniques that advocate challenging patients incrementally above their current functional level.6,7 Conversely, emerging data suggest that substantial amounts of practice of higher-level skills, such as upright stepping, can improve walking function of patients poststroke.4,8,9 Providing large amounts of task-specific stepping practice, particularly at moderate to high aerobic intensities, is consistent with established paradigms to improve locomotor performance in the fields of motor control 10 and exercise physiology11,12 and with principles underlying plastic changes throughout the central nervous system. 13 Application of such training early poststroke could also amplify its effects on recovery. 13
Despite these findings, the amount and intensity of locomotor practice observed during inpatient rehabilitation of individuals poststroke remain limited. Observational studies of inpatient physical therapy sessions indicate that patients practice a variety of walking and nonwalking tasks (eg, static balance, strengthening, transfers), with limited amounts of practice of any single behavior. 14 Previous and recent published estimates of total amount of stepping practice during inpatient rehabilitation averages only 250 to 300 steps/session or day,14,15 with slightly greater stepping practice provided during outpatient rehabilitation (average 400-900 steps/session).4,14 The intensity of interventions is also very low, with heart rates (HRs) reaching aerobic training zones for only 2.8 minutes (4.8%) of sessions. 16 In contrast, research interventions that provide focused, high-intensity stepping practice to patients following discharge from inpatient rehabilitation can achieve 5 to 10 times more steps/sessions at aerobic intensities up to 85% of age-predicted HR maximum (HRmax).4,17 In selected studies, the amount of stepping activity performed during training was significantly related to improvements in locomotor outcomes.4,18 Reasons underlying provision of limited walking practice during inpatient rehabilitation are likely complex and multifactorial. Nonetheless, there is little clarity regarding how much stepping practice can feasibly be provided during inpatient rehabilitation because no study has attempted to implement focused stepping training to patients early poststroke within the context of inpatient physical therapy sessions.
The current investigation represents a retrospective analysis of a multidisciplinary initiative to implement an evidence-based stepping program to patients <6 months poststroke during acute inpatient rehabilitation. Within the context of regular physical therapy sessions, physical therapists prioritized therapeutic activities to maximize the amount and aerobic intensity of stepping practice. Our goals were to determine the feasibility of providing focused stepping practice at moderate to high intensities during inpatient rehabilitation and the potential associations with locomotor and nonlocomotor mobility outcomes. We were specifically interested in how prioritizing high-intensity walking training during inpatient rehabilitation may contribute to improvements in mobility outcomes in patients early poststroke.
Methods
Study Sample and Design
Retrospective data analysis was performed from data collection during implementation of the stepping program over a 16-month period (June 2012 to September 2013) during inpatient physical therapy sessions on patients following an initial diagnosis of stroke of <6 months’ duration. All patients on the 2 primary stroke rehabilitation units participated in the stepping program as possible, with exclusion of patients with restrictions in lower-extremity weight bearing (eg, amputation or lower limb fracture). Patient demographic information, training parameters, and outcome assessments were extracted retrospectively from electronic medical records and deidentified. Data were included if patients were 18 to 89 years old and were not pregnant or HIV positive per institutional review board policy. Specific demographics included gender, age, and duration poststroke as well as lesion side, type (ischemic/hemorrhagic), and distribution (classified as cortical [anterior, middle, or posterior], subcortical [lacunar], subtentorial [brainstem or cerebellar], or multiple lesions; see also Kwakkel and Kollen 19 ). The Charlson Comorbidity Index 20 was also calculated, with the most recent stroke not included. Adverse events during the length of stay, including cardiovascular and neurological events, were recorded. All procedures were approved by the Northwestern University review board.
Interventions
The primary goals of the interventions were to maximize volitional stepping practice at high aerobic intensities during regularly scheduled, inpatient physical therapy sessions. The amount of stepping activity was recorded per minute from 7:30
The general intervention strategies to increase the amount of stepping practice at high aerobic intensities have been described previously4,18 in patients >1 month poststroke with less severe physical impairments and performed outside of clinical therapy sessions. These interventions were discussed with the primary physical therapists treating the targeted patient population, and a multistrategy knowledge translation intervention was provided that included education and mentoring to improve adherence to the stepping program. For the current training interventions, however, guidelines regarding the types and environments of stepping tasks were not provided; rather, the treating therapists determined what type of stepping activities would be performed given the personnel available, equipment constraints, and the extent of their patient’s disability. Stepping activities were generally practiced as a continuous task in a specific direction (forward, backward, or sideways) as opposed to stepping or weight shifting in place (part practice).10,24 Stepping was performed on a treadmill and overground/stairs with or without body-weight support or physical assistance as tolerated and deemed appropriate by the treating therapists. Assistance at the limb or pelvis was provided as needed by therapists or elastic bands during stepping practice in more impaired patients, with assistance and weight support reduced as possible to enhance volitional participation. Patients also wore a gait belt or a safety harness attached to overhead support systems to minimize fall risk. The difficulty of stepping activities was progressed as tolerated, which could include reducing physical assistance, increasing speed, and walking in multiple directions, over and around obstacles, on uneven and compliant surfaces, and over curbs and stairs. Use of assistive devices or hand rails, or focus on specific aspects of walking (speed/endurance vs gait patterns) was determined by the treating therapists. No exoskeletal or elliptical robotic devices were utilized; only the treadmills and mechanical lifts on wheeled overground systems were motorized. A rehabilitation aide was also available on each unit to provide additional assistance if required.
During all stepping activities, physical therapists attempted to achieve aerobic intensity (ie, targeted HR ranges) as much as possible, with HRs monitored via pulse oximeters, with the duration during which HRs reached 70% to 85% of age-predicted HRmax documented4,11,18 in 5-minute increments (HR range decreased by15 beats/min if prescribed β-blockers). 25 The Borg Rating of Perceived Exertion 26 (RPE; ordinal 6-20 scale) was also assessed, with scores ≥14 (ie, >13 or “somewhat hard”) targeted and documented similarly. Patients with significant cardiorespiratory disease were not excluded, although targeted HR ranges were reduced as prescribed by the treating physician.
With the primary focus on stepping activities, substantial amounts of practice of nonwalking tasks, including bed mobility, transfers, and standing balance activities, could not be provided. Practice of these other activities was reserved primarily for family training as necessary or during weekly assessments. Patients received occupational or speech therapies as prescribed.
Therapists met with researchers weekly during the first 3 months of the implementation process to discuss potential barriers and facilitators of delivering these interventions in clinical care, including ensuring consistent outcome measure collection, with intermittent, informal meetings over the 16-month duration. During these meetings, feedback was provided to the therapists regarding amounts of stepping practice provided to patients. However, there was no systematic process for providing feedback directly to patients (as investigated previously27,28).
Outcomes
Primary outcomes were assessed weekly and included the 6-minute walk test (6MWT, in meters) and the Berg Balance Scale (BBS). The 6MWT was performed over a nonstandardized walkway, although with standardized instructions to cover as much ground as possible within 6 minutes 29 over a specific course (eg, laps around inpatient hallways ~90 m), with the level of physical assistance (LoA) documented using an ordinal 7-point scale; this scale was similar to the Functional Independence Measure for walking (1 = total assistance [patient performs 0%-24% of task]; 2 = maximum assistance [25%-49%]; 3 = minimal assistance [50%-74%]; 4 = minimum assistance [75%-99%]; 5 = supervision; 6 = modified independent; 7 = independent), without the distance requirements and categorizing contact guard assistance, or incidental contact in case of loss of balance = 5. The rating of contact guard assistance was used to differentiate between minimal physical assistance for forward progression or with loss of balance as compared with incidental contact in case of loss of balance; Functional Independence Measure walking subscore (FIM-Walk) was recorded separately. The BBS is a reliable 14-item, 56-point ordinal scale to assess postural stability in sitting and standing. 30 Walking speeds determined during a 10-m walk test are not presented here given the inconsistent documentation of LoA at admission and discharge. Furthermore, historical comparative data of the primary outcomes (6MWT) were available for patients poststroke during inpatient rehabilitation during the year prior to implementation strategies, although standardization procedures for the 6MWT limited testing to only those patients who did not require physical assistance (LoA ≥5). Accordingly, these data are not presented here.
Secondary outcomes included individual FIM 31 scores for bed mobility (FIM-Bed), toilet transfers (FIM-Toilet), and walking subscore (FIM-Walk). Additional baseline assessments performed during clinical evaluations included the following: manual muscle testing of paretic lower-extremity strength using a standard 0- to 5-point scale averaged over the dorsiflexors, plantarflexors, hip/knee flexors, and extensors 32 ; the Postural Assessment Scale for Stroke (PASS) 33 ; and combined FIM motor scores (FIM-Motor) and FIM-Cognitive score. 34 Daily stepping activity (steps/day) was recorded as soon as possible following admission (median [interquartile range, IQR] = 4 (3-6) days following admission), with placement and removal of the accelerometers by therapy or nursing staff each day. If the availability of accelerometers was limited, patients did not wear the monitors if stepping was not a goal or early during their length of stay in patients with PASS scores <10. Physical therapists were encouraged to document peak HR, peak RPE, and the amount of time (5-minute increments) patients were able to achieve the targeted intensities of RPE ≥14 (RPE was utilized secondary to blunted cardiac responses with specific medications).
Analysis
Demographic information, training interventions, and admission and discharge outcomes were tabulated, with outcomes utilized only if performed within the first and last week of the length of stay. Missing data were imputed only for 6MWT on initial admission, with 0 m entered for distance, and total assistance (score = 1) entered for LoA if separate documentation of admission FIM-Walk indicated total assistance or no attempt. Analyses were similar both with and without imputed data, with the former presented.
Data were not normally distributed (Shapiro-Wilk tests) and are, therefore, presented using medians and IQRs. Spearman’s correlation analyses determined associations between selected demographic, training, and admission data with primary and secondary outcomes at discharge and change (Δ) scores from admission (adjusted α = .0005 with 100 comparisons). Additional analyses were performed to determine the contributions of steps per day as compared with demographic, training, and baseline data. Stepwise, multiple linear regression models were calculated to estimate the contributions of independent predictors to outcomes. Specific factors included age, gender, lesion distribution and laterality, Charlson Comorbidity Index, days poststroke, physical therapy in minutes per day, steps per day, and admission scores for paretic leg strength, BBS, and the primary outcomes at admission (11-14 data sets per independent predictor). Additional training characteristics of cardiovascular or perceived exertion (HR or RPE) were not utilized in the regressions because of inconsistent documentation (see Results section). The admission PASS was also not utilized secondary to the high correlation with admission BBS (r = 0.87). Subsequent hierarchical linear regression determined the independent contributions of steps per day to primary outcomes. Data transformation of 6MWT (square root) and BBS (2/3 power) was performed to ensure normalized residuals of regression models, although the resultant analysis revealed similar predictors to the raw data, with the latter presented. Collinearity was monitored, with variance inflation factors <3.0 considered acceptable.
Conditional logistic regression was also performed to evaluate contributions of independent predictors to discharge walking function and discharge location. Walking function at discharge was dichotomized for those who could or could not walk with only contact guard assistance or less (LoA ≥5 vs LoA ≤4) at discharge for >50 m (approximating FIM-Walk distances for estimates of community mobility). Discharge location was dichotomized for home versus other setting (eg, skilled nursing or other hospital setting). Receiver operating characteristic analysis was performed using the primary predictors identified from the logistic regression at the first and second week of admission. The area under the curve (AUC) was identified as well as the highest combined sensitivity and specificity (Youden’s Index), the associated cutoff scores that best distinguished LoA ≤4 versus ≥5, and discharge location (home vs other). All analyses were performed using SPSS v21 as described above for the entire data set, with data analyzed separately for those who required physical assistance to walk at admission (LoA ≤ 4).
Results
Clinical implementation of the training paradigm occurred on 2 inpatient units, with data collected on 201 patients over 16 months. Table 1 provides demographic data and baseline measures at admission. More than 80% of patients (n = 161) were admitted <30 days poststroke, and only 15 between 60 and 180 days poststroke. Admission FIM-Motor and FIM-Cognition scores indicated that >80% of patients presented initially with severe deficits. 34 Physical assistance during the 6MWT (LoA ≤ 4) was required for 79% of patients.
Demographic and Baseline Assessments of Patients on Admission, and Training Activities During the Length of Stay.
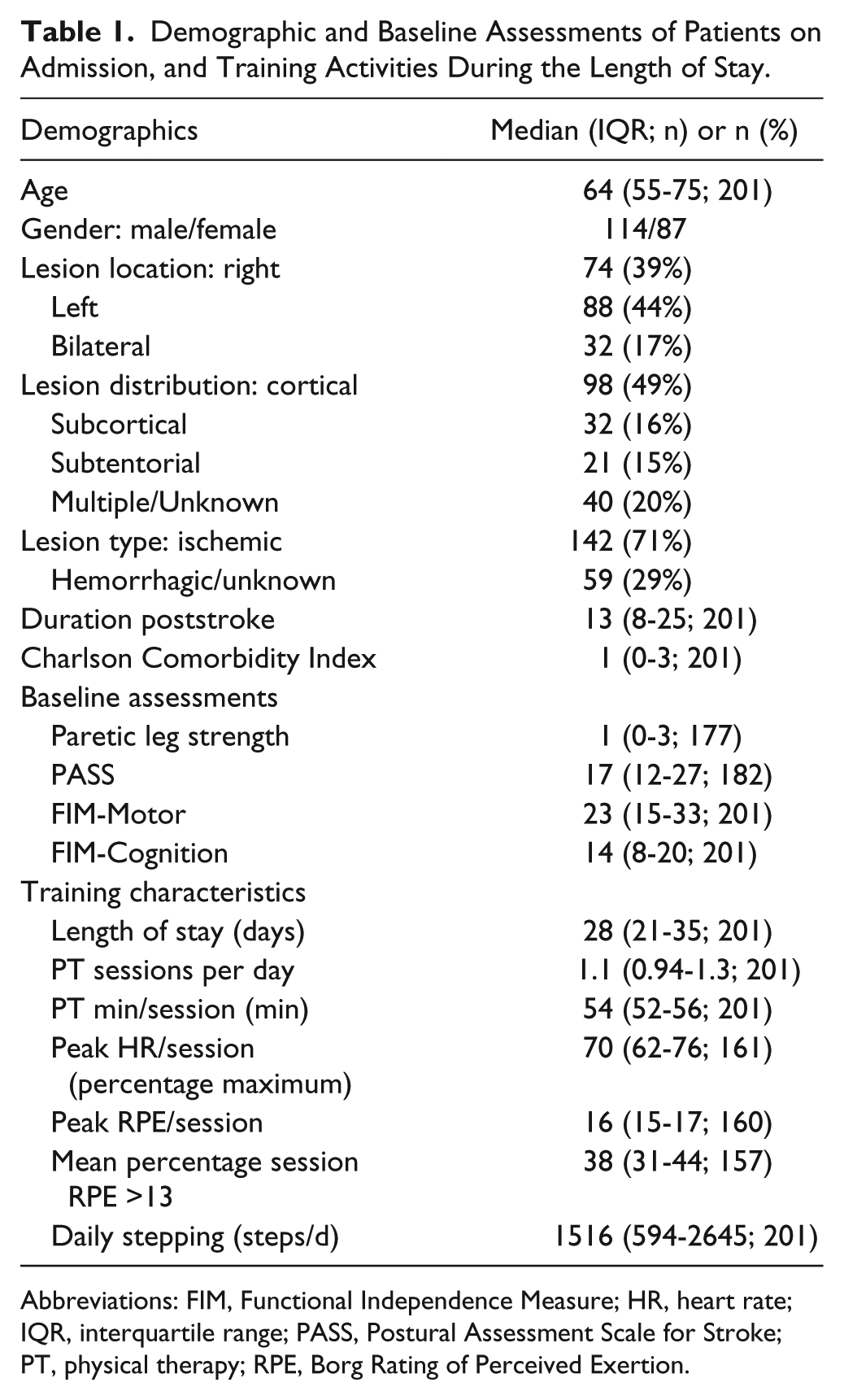
Abbreviations: FIM, Functional Independence Measure; HR, heart rate; IQR, interquartile range; PASS, Postural Assessment Scale for Stroke; PT, physical therapy; RPE, Borg Rating of Perceived Exertion.
Table 2 details the physical therapy interventions throughout the length of stay, with a median of 1.11 sessions/d, or 54 minutes/d. Measures of training intensity were documented at least once in 80% of patients, although only during 28% to 33% of sessions, with the available data indicating that patients were able to reach a moderate to high exercise intensity for an extended duration (median = 70% HRmax, and 38% duration at RPEs ≥14). A total of 14 patients experienced a new-onset or suspected stroke (n = 7; 3.4%) or another cardiopulmonary event (n = 7) outside of therapy and were discharged; 10 returned to inpatient rehabilitation. The median steps per day throughout the length of stay was 1516 (594-2645) steps/d; lower number of steps per day were achieved during the first versus second week (715 [222-1764] to 1308 [484-2689]). An example of variations in daily stepping across patients is depicted in Figure 1, which delineates the stepping activity of 2 patients who required maximal assistance (red; LoA = 2) and moderate assistance (blue; LoA = 3) during 6MWT at admission. Single-day steps per minute are presented at day 8 postadmission and 5 days prior to discharge (Figures 1A and 1B), with stepping activity clustered during physical therapy sessions. Steps per day during weekdays throughout the length of stay are also presented (Figure 1C), with the line and light band indicating median steps per day and IQR across the population. The patient who initially required maximal assistance (red) was able to achieve 1000 to 1500 steps on selected days, although the average stepping activity across the length of stay was near the 25th quartile. Conversely, the average stepping activity of the other patient (blue) was approximately the 75th percentile, with oftentimes 3000 to 7000 steps/d achieved.
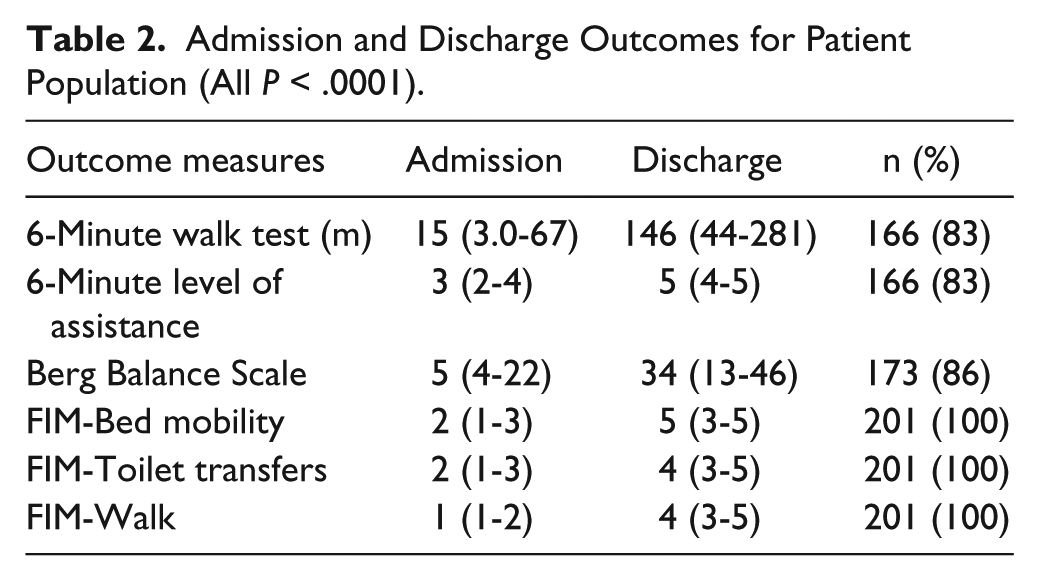
Admission and Discharge Outcomes for Patient Population (All P < .0001).
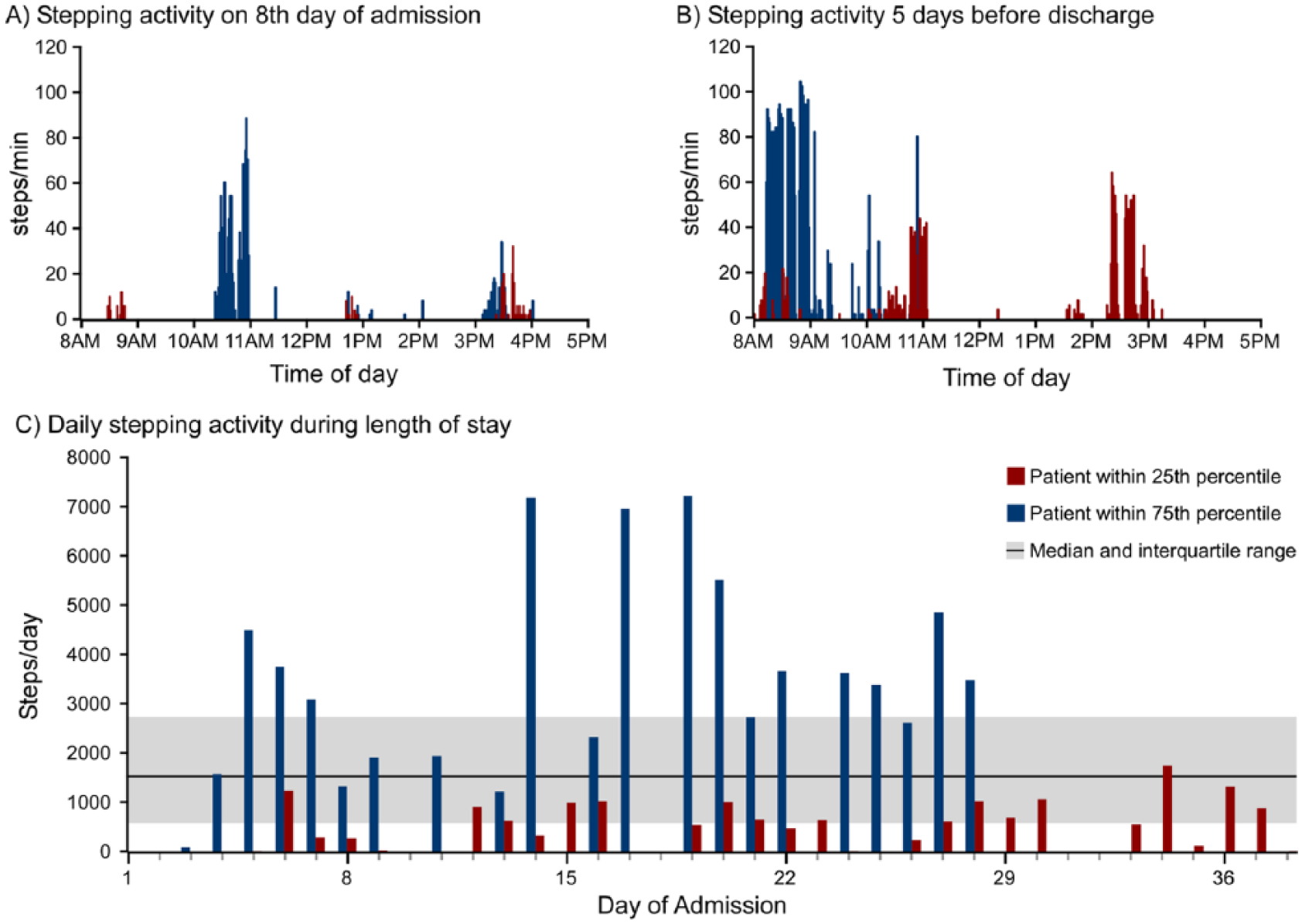
Individual single-day stepping activity (steps/day) at 8 days of length of stay (A) and 5 days prior to discharge (B) of 2 individuals at the 25th (blue) and 75th percentiles (red) of stepping activity. C. The number of steps per day throughout the length of stay in both patients is presented, with the horizontal line and shaded area representing the median and interquartile range of the steps per day of the population, respectively.
Correlation analyses indicated that the number of steps per day was not correlated to demographic data with the exception of duration poststroke (r = −0.31). Rather, it demonstrated significant correlations with training activities, including a negative correlation with length of stay (r = −0.30) but positive associations with minutes per day of physical therapy (r = 0.47), peak HR (0.39), and percentage time spent at RPE >13 (r = 0.60). The number of steps per day was also correlated with baseline paretic leg strength (r = 0.49), BBS (r = 0.62), 6MWT (r = 0.61), and LoA (r = 0.55).
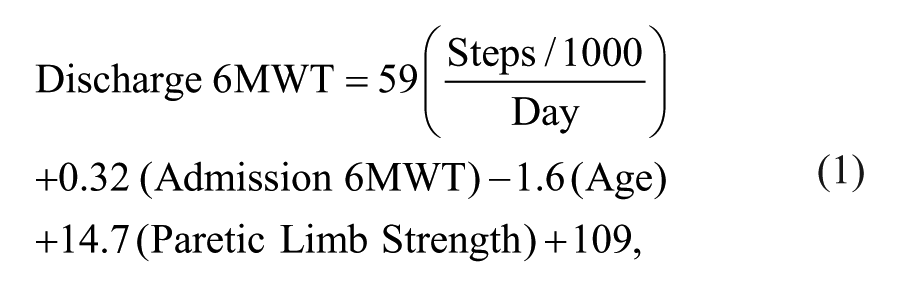
Stronger correlations were observed between stepping activity and discharge outcomes. Table 2 details these outcomes at admission and final discharge for all patients, indicating median 6MWT improvements of 93 m (27-203), increases in LoA by 1 (0-2), and BBS improvements of 14 (5-28). Supplementary Table 1 provides the correlation coefficients between discharge and Δ in outcomes and selected demographic, training, and baseline measures. The highest correlation coefficients were observed between the number of steps per day and discharge outcomes (all P < .0005), with strong to moderate correlations between stepping activity versus 6MWT (r = 0.87) and Δ6MWT (r = 0.65; Figure 2). Slightly lower correlations were observed with BBS scores and number of steps per day (discharge BBS: r = 0.78; ΔBBS: r = 0.40). Stepwise linear regressions for discharge 6MWT and BBS are provided in Equations 1 and 2, with significant predictors contributing 69% and 62% of the total variance (r2). Hierarchical linear regression analysis indicated that steps per day independently accounted for 20% of the variance in discharge 6MWT and 11% in BBS.
Similar predictors contributed to both Δ6MWT and ΔBBS (Supplementary Table 2), with steps per day independently contributing 31% and 18% of the variance, respectively. The number of steps per day was the primary predictor of discharge FIM scores and secondary for all ΔFIM scores.
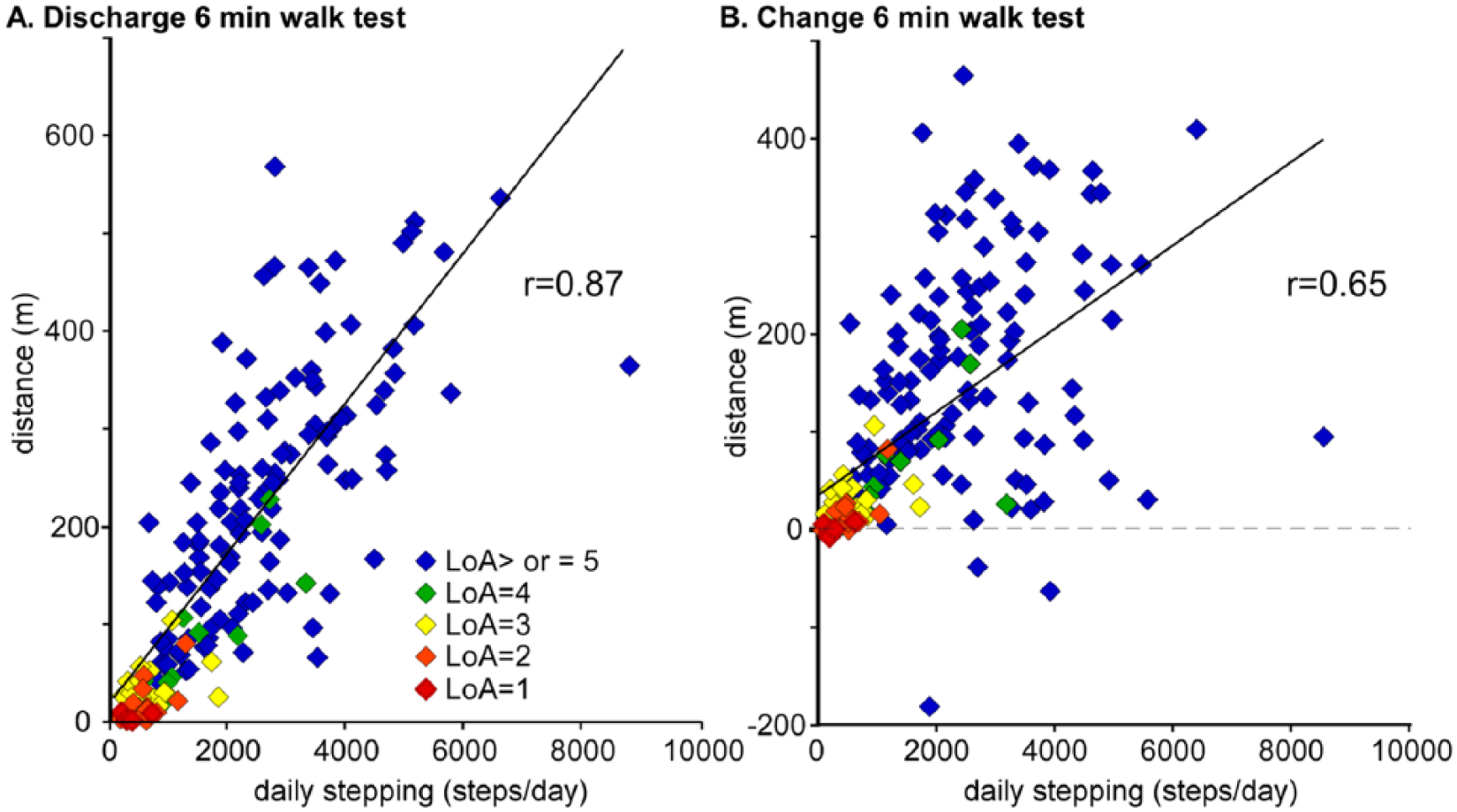
Relation between steps per day and discharge 6MWT (A) and Δ6MWT (B) in patients who required different levels of assistance (LoAs) at discharge (LoA of 1 = red; 2 = orange; 3 = yellow; 4 = green; ≥5 = blue).
At final discharge, 71% of patients required contact guard assistance or less (LoA ≥ 5) during the 6MWT (vs 21% at admission). For patients with LoA ≤4 at admission, 63% walked with LoA ≥5 at discharge. In Table 3, we detail the number of patients at a specific LoA on admission (1-5) and the number (percentage) of those at a specific discharge LoA as well as the median number of steps per day for each LoA. For example, 22 patients required total assistance to walk during the 6MWT at admission, although only 2 still required total assistance at discharge, and 9 patients (35%) required LoA ≥5. Median stepping activity for those at LoA ≤3 at discharge was <500 steps/d, whereas median stepping for those at LoA ≥4 at discharge was >1000 steps/d.
Number and Percentage of Patients at Admission and Discharge (DC) Level of Assistance (LoA) During the 6MWT, With Stepping Activity per DC LoA.
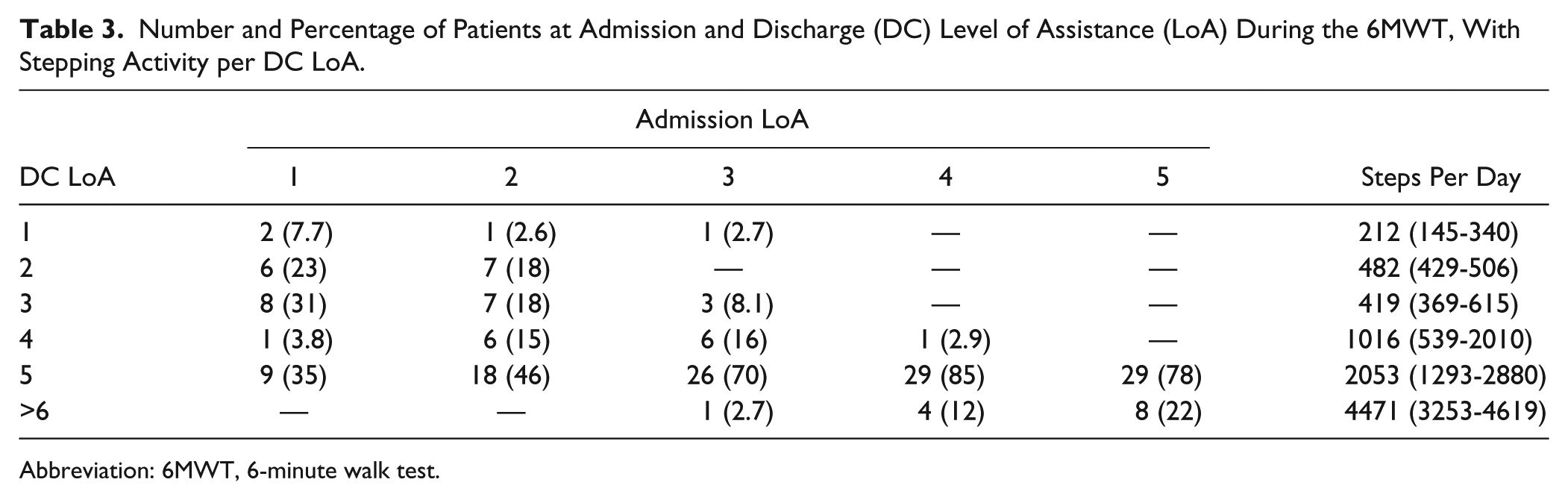
Abbreviation: 6MWT, 6-minute walk test.
Conditional logistic regressions were calculated to determine the primary predictors of patients’ ability to ambulate at LoA ≥5 at discharge 6MWT and discharge location (home or other) following inpatient rehabilitation (Supplementary Table 3). Steps per day and admission BBS were identified as the primary variables for LoA ≥5 at discharge, with consistent findings following inclusion only of patients who required assistance at admission (ie, exclusion of LoA ≥5 at admission). Logistic regressions were also calculated to determine discharge location (home vs other) from inpatient rehabilitation. Inclusion of key discharge outcomes (6MWT, LoA, and BBS) revealed LoA ≥5 at discharge and age as primary predictors of home discharge. With exclusion of discharge outcomes, stepping activity and age were the primary predictors of discharge location. More directly, step per day was strongly associated with LoA at discharge, which was in turn related to discharge location.
Receiver operating characteristic analyses were performed to evaluate the ability of average steps per day and BBS at the first and second week of admission to predict walking ability with contact guard assistance or less during discharge 6MWT for ≥50 m (ie, LoA ≥5 vs ≤4). Table 4 indicates the AUCs and Youden’s indices with associated sensitivity and specificity and cutoff scores for both steps per day and BBS during the first 2 weeks. In addition, median (IQR) steps per day and BBS are provided at the first and second week and separated for those with LoA ≤4 versus ≥5; we further separated the latter group according to who required assistance on admission. For stepping activity, a significantly larger AUC was observed at the second versus the first week, with much larger sensitivity/specificity but similar cutoff scores (1000-1100 steps/d). Evaluation of steps per day over the first 2 weeks indicated large increases in stepping activity primarily for those who were able to achieve LoA ≥5 at discharge. Similar findings were observed for BBS, with larger AUCs and Youden’s indices at the second (10.5) versus the first week (5.5 points). Individuals requiring contact guard or less assistance (LoA ≥5) at discharge demonstrated larger BBS gains over the first 2 weeks, whereas very little improvement in BBS was observed in patients with discharge LoA ≤4.
Receiver Operating Characteristic (ROC) Analyses and Weekly Responses for BBS and Stepping Activity.
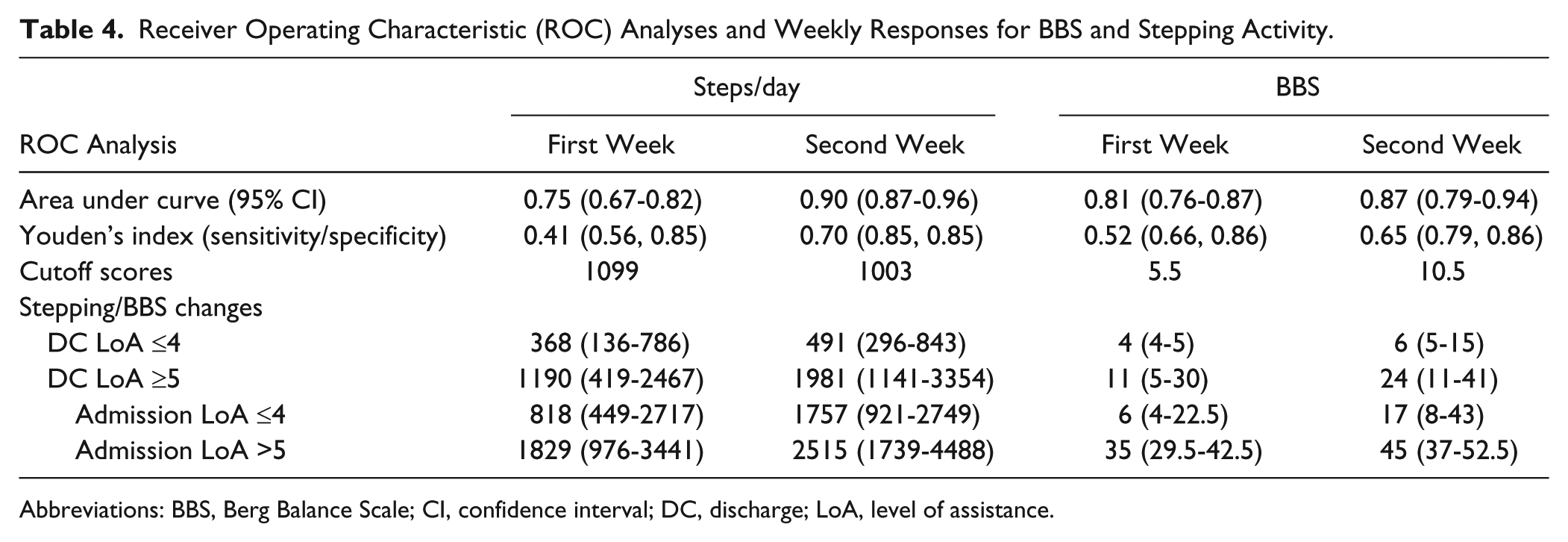
Abbreviations: BBS, Berg Balance Scale; CI, confidence interval; DC, discharge; LoA, level of assistance.
Discussion
The present study details the feasibility of providing focused stepping practice to patients early poststroke during inpatient rehabilitation and its relation to mobility outcomes. Similar training strategies have been applied to patients >1 month poststroke or later 18 but have not been implemented within the context of inpatient physical therapy and with patients who often require substantial physical assistance to walk. The observed median of ~1500 steps/d is 5 to 6 times greater than published reports of steps per session or daily repetitions of lower-limb exercise during traditional inpatient rehabilitation.14,15 Patients were able to perform stepping practice at a high intensity for a longer duration per session (38% of sessions) as compared with published estimates (4.8% of sessions 16 ), although these data should be interpreted with caution because of low response rates. Furthermore, the percentage of patients who experienced a significant adverse neurological or cardiopulmonary event was consistent with normative data. 35 This latter finding points toward the preliminary safety of this protocol, consistent with a recent meta-analyses indicating the relative safety of aerobic training in patients poststroke. 9
The findings of strong to moderate correlations between steps per day and improvements in locomotor and nonlocomotor outcomes, including discharge location, are consistent with data from more controlled studies involving individuals with chronic locomotor impairments poststroke.4,18 Whereas other factors previously identified as determinants of walking outcomes, such as age, 36 strength, and balance 37 were also significant predictors, stepping activity demonstrated the highest correlation above and beyond these other variables. Reasons for this finding are not entirely clear, although the amount of stepping practice could better reflect the capacity of neuromuscular and cardiovascular systems (ie, strength, balance, cardiovascular endurance) as compared with any single measure of impairment. Providing focused training may also contribute to gains in motor function, which could in turn facilitate motor recovery. The lack of a comparison group or more controlled experimental testing prohibits identification of a causal relationship between stepping activity and outcomes. Nonetheless, the data represent what may be achieved when a modifiable treatment variable, such as amount of stepping practice, is prioritized during inpatient rehabilitation therapies to presumably affect locomotor outcomes.
The present data contrast with previous findings suggesting little relationship between stepping activity recorded during single observations and measures of walking performance, 14 although the present findings are consistent with more recent data demonstrating a positive relationship between stepping activity (repetitions 15 or time 28 ) and locomotor outcomes. In these latter studies, however, the amount or time of stepping practice was generally still very low, and the correlation between stepping activity and changes in locomotor outcomes presented in the current study (r = 0.65 or r2 = 0.42 for 6MWT) are greater than those presented previously (r2 = 0.26 for 10-m walk 15 ). The stronger correlations observed in this study likely represent both the functional limitations of the patients and the therapists’ ability to maximize stepping practice. For example, despite attempts to maximize stepping activity across patients, the median number of steps per day were <500 steps/d in patients who required at least moderate assistance at discharge. Although the amount of practice is almost double that of stepping activity typically performed in the clinical inpatient setting,14,15 the lack of substantial early improvements in selected outcomes (ie, BBS scores) mirror the small changes in stepping activity that these patients were able to achieve. Conversely, stepping practice increased substantially in those who required less assistance at discharge (LoA ≥ 5), which accompanied their larger gains in walking function and balance. Analyses of these relationships appear to predict recovery of walking function fairly accurately, although such predictions are valid only if focused stepping practice is prioritized.
The findings that stepping activity was significantly related to improvements in nonwalking activities such as BBS, bed mobility, and transfers are of additional interest because these tasks were not the focus of therapeutic interventions. Practice of these tasks certainly occurred during weekly assessments and family training and likely during occupational therapy as deemed appropriate by the treating therapists. However, attention to these tasks during physical therapy sessions was minimal as compared with traditional rehabilitation.14,38 Such improvements may have resulted from the substantial amounts of stepping practice provided, where performance of unpracticed mobility tasks may improve with practice of higher-level skills, as suggested previously.39,40
The primary limitations of this investigation include the lack of a control group and long-term follow-up to evaluate the comparative efficacy following discharge. Given these limitations, the primary objective of the present study was to apply training strategies established in previous trials on patients early poststroke within the constraints of inpatient rehabilitation and without stringent inclusion criteria. Performing controlled, randomized trials that manipulate physical therapy interventions billed to third-party payers is difficult, and many studies assess experimental interventions in addition to standard or usual rehabilitation care (eg, Duncan et al 41 and Pohl et al 42 ). Future studies may attempt to evaluate the potential effectiveness of these stepping strategies applied during inpatient rehabilitation early poststroke, including the use of various feedback strategies of stepping activity to patients and therapists. 28 However, comparisons with more conventional interventions will likely require alternative (nonrandomized) study designs. Evaluation of these interventions using a prospective design may also minimize any potential selection bias associated with retrospective investigations and may improve response rates with outcomes (eg, 10-m walk) and interventions (intensity measures).
Despite these limitations, evaluation of the present data may provide the basis for initial comparisons to estimate expected changes for future studies. For example, gains in 6MWT in patients with LoA ≤4 at admission (median [IQR] Δ6MWT = 87 [26-198] m) compare favorably with those described in patients with nonambulatory stroke receiving robotic-assisted gait training (76 [34-138] m) to control physical therapy (35 [9-73] m). 42 Furthermore, improvements in balance (median [IQR] ΔBBS = 14 [5-28]) are comparable to those achieved in traditional rehabilitation 43 or following circuit training interventions 38 (mean Δ = 6-12 points), where specific balance tasks were practiced more extensively. Application of this high-intensity intervention within the constraints of regular rehabilitation appears to elicit sufficient gains in locomotor function while not compromising other functions.
Conclusions
In summary, the present data suggest that delivery of large amounts of focused, repeated stepping practice in patients with severe motor deficits poststroke during inpatient physical therapy sessions is feasible. Furthermore, such stepping activity is related to gains in locomotor and nonlocomotor mobility outcomes, including discharge LoA and location (home vs other). The training strategies utilized were consistent with mechanisms underlying plastic changes in the nervous system 13 and with training principles utilized to enhance motor skill acquisition 10 and exercise performance 12 in healthy individuals. The interventions did not require substantial additional assistance (one rehabilitation aide as available), nor were automated (ie, robotic) devices utilized. Rather, therapists prioritized practice of these higher-level walking skills early poststroke in an attempt to improve mobility outcome as opposed to utilizing more traditional strategies that gradually progress the difficulty of practiced tasks based on the patient’s current functional level. 39 Further work is required to adequately assess the efficacy of these strategies early poststroke to improve long-term outcomes, particularly as compared with more traditional rehabilitation interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by National Institute of Disability and Rehabilitation Research-H133B031127 and H133B140012, the Chicago Blackhawks Foundation, the Bullock Foundation, and a Henry Betts Award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.