
Abstract
Background. After inpatient stroke rehabilitation, many people still cannot participate in community activities because of limited walking ability. Objective. To compare the effectiveness of 2 conceptually different, early physical therapy (PT) interventions to usual care (UC) in improving walking 6 months after stroke. Methods. The Locomotor Experience Applied Post-Stroke (LEAPS) study was a single-blind, randomized controlled trial conducted in 408 adults with disabling hemiparetic stroke. Participants were stratified at baseline (2 months) by impairment in walking speed: severe (<0.4 m/s) or moderate (0.4 to <0.8 m/s). Between 2 and 6 months, they received either only UC (n = 143) or UC plus 36 therapist-provided sessions of either (1) walking training on a treadmill using body-weight support and practice overground at clinics (locomotor training program [LTP], n = 139) or (2) impairment-based strength and balance exercise at home (home exercise program [HEP], n = 126). Results. LTP participants were 18% more likely to transition to a higher functional walking level: severe to >0.4 m/s and moderate to >0.8 m/s than UC participants (95% confidence interval [CI] = 7%-29%), and HEP participants were 17% more likely to transition (95% CI = 5%-29%). Mean gain in walking speed in LTP participants was 0.13 m/s greater (95% CI = 0.09-0.18) and in HEP participants, 0.10 m/s greater (95% CI = 0.05-0.14) than in UC participants. Conclusions. Progressive PT, using either walking training on a treadmill and overground, conducted in a clinic, or strength and balance exercises conducted at home, was superior to UC in improving walking, regardless of severity of initial impairment.
Keywords
Introduction
The Locomotor Experience Applied Post-Stroke (LEAPS) trial compared 2 conceptually different rehabilitation interventions: (1) task-specific walking training on a treadmill with partial body-weight support coupled with overground walking delivered in a rehabilitation center either 2 (early locomotor training program [E-LTP]) or 6 months after stroke (late [L]-LTP) and (2) an impairment-based progressive strength and balance exercise program delivered in the home 2 months after stroke (home exercise program [HEP]). 1 The LEAPS participants were adults who at 2 months poststroke still had not achieved unlimited community ambulation (≥0.8 m/s walking speed) and thus could walk either only in the home or on a limited basis in the community. 2
Deferral of treatment for one-half of the participants randomized to LTP until 6 months poststroke (L-LTP group) provided the basis for this planned secondary analysis comparing the effects of E-LTP and HEP combined with usual care (UC) with UC alone at 6 months poststroke. 3 HEP was originally conceptualized as a control intervention, one that would match LTP in dose, intensity, and goal-oriented focus, but because of the lack of an explicit walking component, it was not expected to have an important impact on the level of functional walking ability. The amount and type of UC were not managed by LEAPS investigators. Thus, UC physical therapy (PT) was provided based on practice standards across our 6 regional sites.
This analysis addresses a clinically important question for practitioners and patients: are current practices of postacute PT as effective in improving the likelihood of functional walking after stroke as the progressive interventions used in the LEAPS trial? 4
Methods
Study Design
The LEAPS trial was a multicenter, single-blind randomized controlled trial, stratified by walking impairment level at 2 months after onset of stroke. We classified severe impairment as walking at <0.4 m/s and moderate impairment as walking at 0.4 to <0.8 m/s. Proportional randomization to protocol intervention groups (LTP, HEP) and UC was 7:6:7. Physical therapists conducting baseline and postintervention assessments were blinded as to the intervention group. The LEAPS protocol and primary outcomes have been reported.1,3
Study Population and Screening
Participants were recruited from 6 inpatient rehabilitation sites in California and Florida. Inclusion criteria were age ≥18 years, stroke within 45 days, residual paresis in the lower extremity, ability to walk 10 feet with no more than 1-person assistance and follow a 3-step command, physician approval for participation, self-selected 10-m walking speed less than 0.8 m/s, and living in the community by the time of randomization. Exclusion criteria included dependence in activities of daily living (ADL) prior to stroke, exercise contraindications, preexisting neurological disorders, and inability to travel to the treatment site. 1
Interventions
The LTP and HEP programs were controlled for exercise frequency (90 minute sessions, 3 times per week) and duration (12-16 weeks), for a total of 30 to 36 exercise sessions. LTP included stepping on a treadmill with partial body-weight support for 20 to 30 minutes at 3.2 km/h (0.89 m/s or 2.0 miles/h) with manual assistance as needed, followed by a progressive overground walking program sustained for 15 minutes, provided in an outpatient facility by 2 physical therapists and a rehabilitation technician, as needed. HEP included progressive flexibility, range of motion, upper- and lower-extremity strength, coordination, and static and dynamic balance exercises provided by a physical therapist in the home. No specific walking activity was undertaken.
In addition to the LTP and HEP interventions, all participants were allowed to receive any prescribed usual and customary care during this 6-month trial. Participants were instructed to submit a monthly calendar logging the date and duration of all UC PT sessions. LEAPS study personnel reviewed the logs with participants by phone, monthly.
Outcomes
The primary outcome measure in the present report was the proportion of participants who improved their functional level of walking at 6 months poststroke—the same outcome used for the 1-year poststroke analysis already reported. 3 Improved functional walking level at 6 months after stroke was defined as the ability to walk independently at a speed of 0.4 m/s or higher if entry speed was <0.4 m/s or at 0.8 m/s if initial walking speed was 0.4 to <0.8 m/s.1,3,5 Secondary walking outcomes included changes in 10-m walking speed, 6 distance walked in 6 minutes, 7 and number of steps taken per day measured with a step activity monitor. 8 Other outcome measures included the Fugl-Meyer assessment of lower-extremity motor impairment (FM-LE), total sensory and motor FM scores,9,10 the Berg Balance Scale (BBS), 11 the Activities-Specific Balance Confidence (ABC) Scale, 12 the ADL/Instrumental ADL (IADL) Scale, physical mobility and participation domains of the Stroke Impact Scale, 13 and the modified Rankin Scale as a measure of overall disability. 14
Adverse Events
Death, life-threatening adverse events (stroke, myocardial infarction, and fracture caused by a fall), rehospitalization, and new disability or incapacity that led to more than 48 hours of limitation in ADL were considered serious adverse events. 1 Minor adverse events included a fall with no fracture, dyspnea during treatment, an open sore or blister, cuts, muscle soreness or pain that persisted for more than 48 hours, dizziness/faintness, diaphoresis, hypertension or hypotension during exercise that halted the intervention for the day, and deep venous thrombosis. 1
Statistical Analysis
To examine the effectiveness of LTP and HEP interventions relative to UC, we conducted an intention-to-treat logistic regression analysis with successful recovery of walking at 6 months poststroke as the dependent variable. Odds ratios for the primary outcome were calculated relative to UC, adjusting for baseline walking impairment category (severe, moderate), clinical site, stroke type, side of hemiparesis, presence of depression, and age. The planned imputation method for missing data reduced to the last-observation-carried-forward approach because none of the dropped out participants had a related adverse event.1,3
Paired t tests were used to compare within-group improvements, and analysis of variance (ANOVA) was used to assess differences across the 3 groups for the secondary outcome measures, followed by pairwise comparisons with Bonferroni adjustment for multiple testing. The Kruskal-Wallis procedure was used to compare the groups on the number of steps taken in the community. To determine the effect of number of UC visits on walking speed change, a separate linear regression analysis was conducted. All statistical analyses were performed using SAS software, version 9.1 (SAS Inst Inc, Cary, North Carolina).
All tests for statistical significance were 2-tailed. The threshold α value was set at .05.
Results
Baseline Characteristics
Of 5289 stroke admissions from April 2006 through June 2009, 4909 patients were screened for study eligibility, and 3137 were excluded (Figure 1). At the second screening 2 months after stroke onset, 1364 patients were excluded. The most common reasons for exclusion were the presence of one or more major coexisting medical conditions, absence of residual paresis in the leg on the side of the body affected by stroke, absence of a primary diagnosis of stroke, no expectation of home discharge, a self-selected walking speed greater than 0.8 m/s, and refusal to provide informed consent. Also, 19 persons did not pass the exercise tolerance test before randomization. Of the 408 participants included in the intention-to-treat analysis, 139 were assigned to LTP (delivered at 2 months poststroke), 143 to UC (UC only at 2 months poststroke, and then LTP at 6 months), and 126 to exercise delivered in the home at 2 months poststroke. Participants who completed the study were 62.0 ± 12.7 years old; 54.9% were men. and 22.1% were African American (Table 1). Also, 71% had ischemic stroke, and 99.5% had modified Rankin scores of 2 to 4 (slight disability to moderately severe disability). Participants were randomized 63.8 ± 8.5 days poststroke; 53.4% walked at <0.4 m/s, and 46.6% walked at 0.4 to 0.79 m/s. Stratified randomization by site resulted in no significant site differences in the percentage of participants receiving the 3 treatments. However, randomization was not done by therapist, so individual therapists provided differentce mixes of the 3 protocol treatments. Major comorbidities were hypertension, diabetes, and cardiovascular disease. More than a third had arthritis or musculoskeletal complaints. The baseline characteristics of those who were lost to follow-up at 6 months are presented in Table 1. The distribution of participants randomized to each intervention group and relative to the number of therapists conducting the interventions at each site is reported in Table 2.
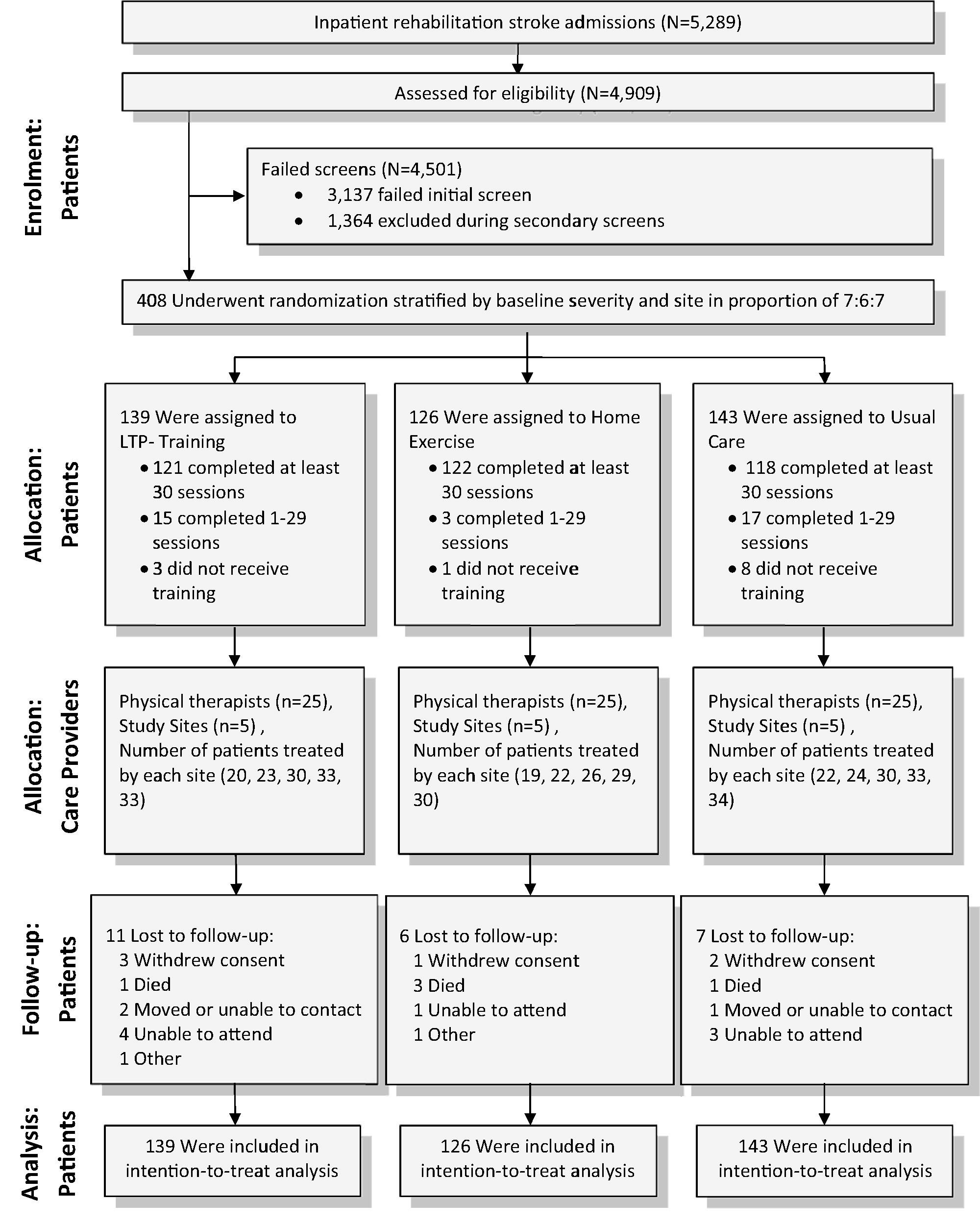
Consort diagram.
Baseline Characteristics by Intervention Group for All Participants and for Those Who Were Lost to Follow-up.
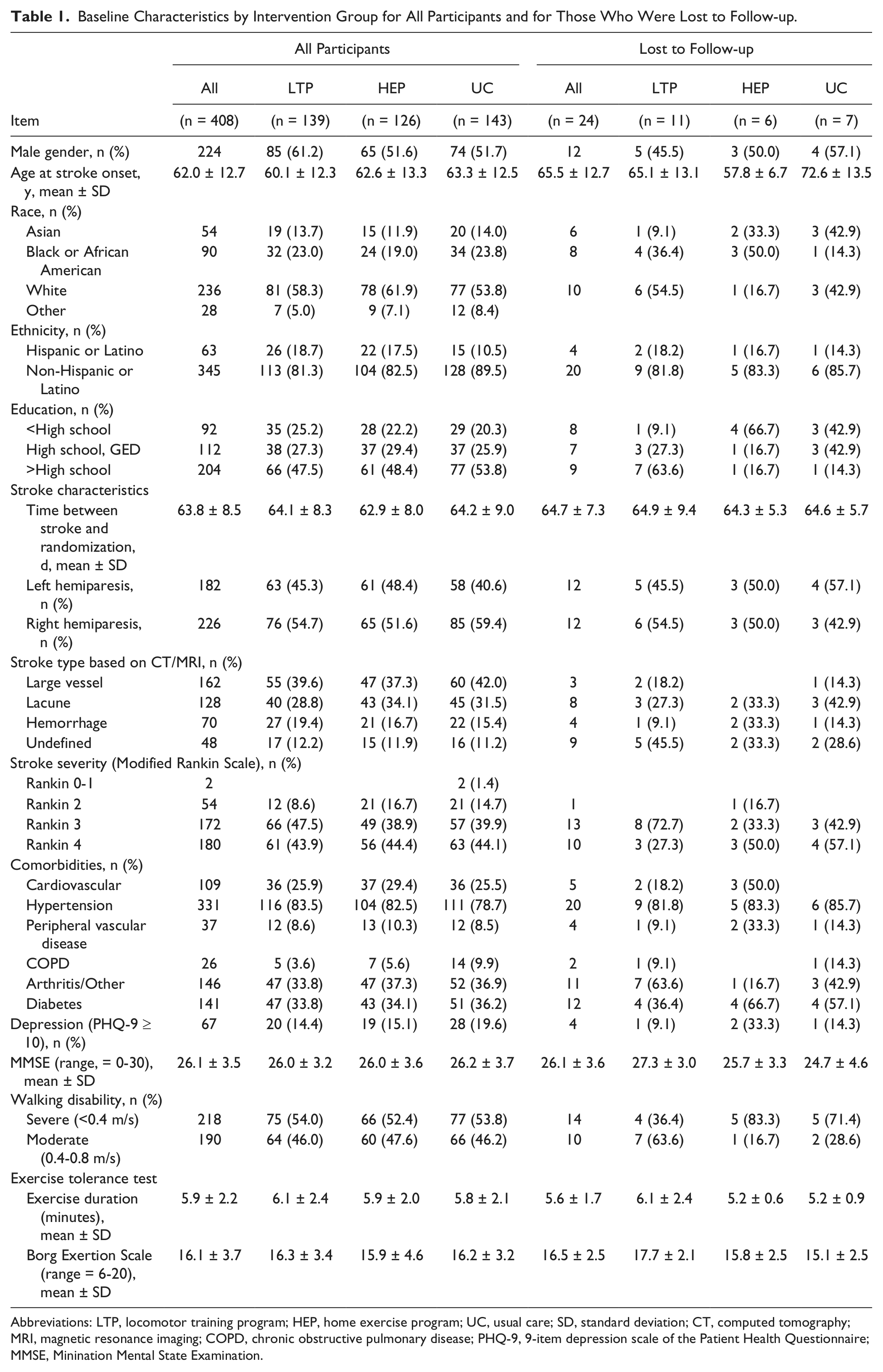
Abbreviations: LTP, locomotor training program; HEP, home exercise program; UC, usual care; SD, standard deviation; CT, computed tomography; MRI, magnetic resonance imaging; COPD, chronic obstructive pulmonary disease; PHQ-9, 9-item depression scale of the Patient Health Questionnaire; MMSE, Minination Mental State Examination.
Number of Participants and Therapists by Study Site.
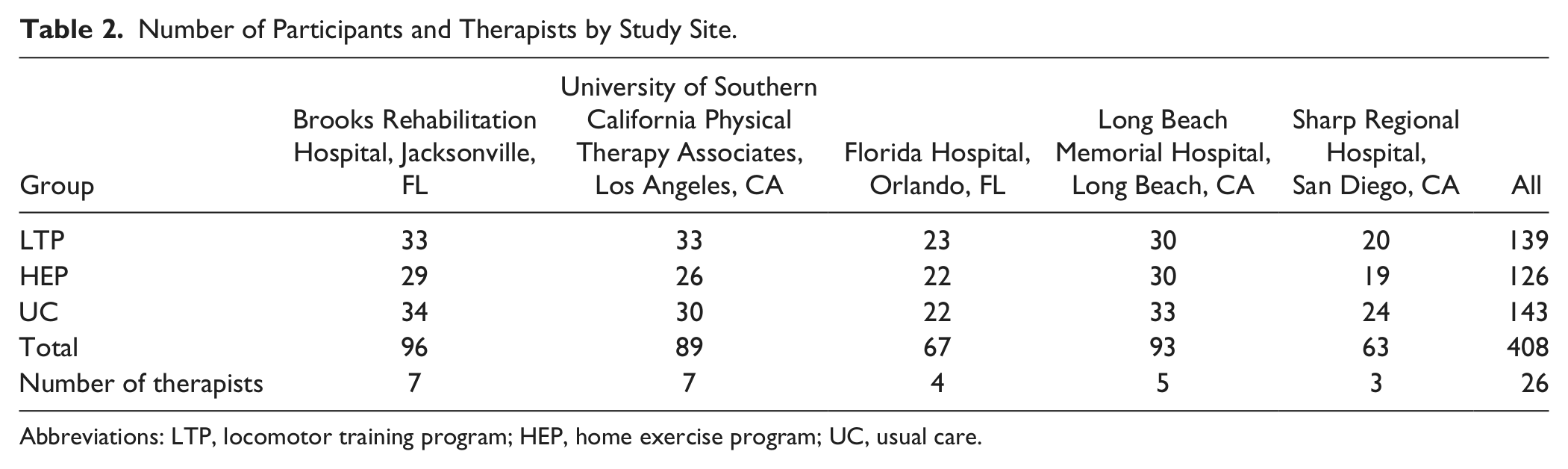
Abbreviations: LTP, locomotor training program; HEP, home exercise program; UC, usual care.
Interventions
The percentage of participants who did not complete the intervention at 6 months was 13% for LTP and 3% for HEP (P < .001). The LTP group completed an average of 33 ± 7 sessions and the HEP group 36 ± 3 sessions. Session duration for LTP was 83 ± 6 minutes and for HEP 76 ± 10 minutes. LTP progression from the first 3 to last 3 sessions was evident for treadmill walking time (mean ± SD = 14 ± 5 to 23 ± 5 minutes), treadmill speed (1.7 ± 1.7 to 2.0 ± 0.4 miles/h), percentage body-weight support (31.0 ± 6.1 to 11.8 ± 8.5), and overground training level of difficulty (56% transitioned to a higher level). For the HEP group, the number of repetitions, resistance, and level of difficulty increased for upper- and lower-extremity flexor and extensor exercises, as did sitting and standing balance activities across the intervention period.
The amount of usual and customary rehabilitation after acute hospitalization was highly variable within each group. The median number of UC PT visits was 7 for LTP (range, 0-56), 13 for HEP (range, 0-86), and 11 for UC only (range, 0-69). Of 408 participants, 21.6% did not receive any PT after their inpatient rehabilitation hospitalization. The proportion that received no PT outside the study was higher for the LTP group (30.9%) than HEP (15.9%) and UC groups (17.5%). The average length of time for UC visits was 53 ± 14 minutes for LTP, 54.0 ± 11 for HEP, and 53 ± 14 for UC only.
Outcomes
At 6 months, 50.4% of LTP, 49.2% of HEP, and 32.2% of UC participants had improved to a higher functional walking level (Table 3). The difference between LTP and UC was 18% (95% confidence interval [CI] = 7%-29%) and between HEP and UC, 17% (95% CI = 5%-29%). The adjusted odds ratio for achieving a higher functional walking level with LTP compared with UC was 1.94 (95% CI = 1.18-3.21; P = .010) and for HEP compared with UC, 2.04 (95% CI = 1.22-3.42; P = .007). There was no difference in gains between LTP and HEP, and severity of initial walking impairment had no impact on gains. Site of treatment had no impact on gains either.
Number of Patients (%) by Intervention Group for Dichotomous Outcomes, Serious Adverse Events, and Multiple Falls. a
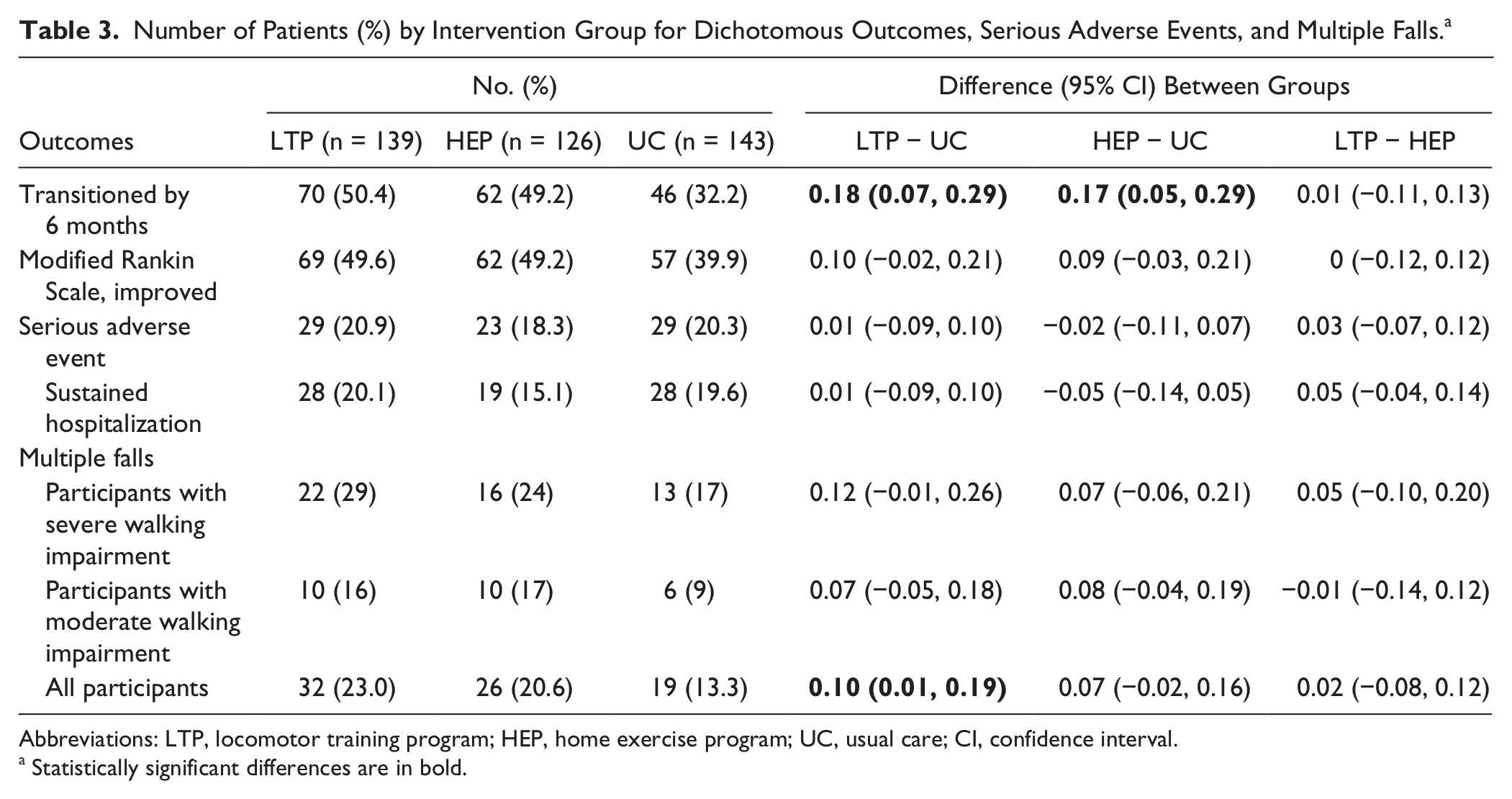
Abbreviations: LTP, locomotor training program; HEP, home exercise program; UC, usual care; CI, confidence interval.
Statistically significant differences are in bold.
From baseline, all 3 groups improved their walking speed (P < .0001; Figure 2), 6-minute walk distance, and number of community steps taken per day (Table 4). However, LTP and HEP groups had greater walking speed increases (LTP, 0.25 ± 0.21 m/s; HEP, 0.23 ± 0.20 m/s) than the UC group (UC, 0.13 ± 0.14 m/s; P < .0001), corresponding to medium effect sizes of 0.72 and 0.56, respectively (Table 3). The difference in walking speed gain between LTP and UC was 0.13 m/s (95% CI = 0.09-0.18) and between HEP and UC, 0.10 m/s (95% CI = 0.05-0.14).
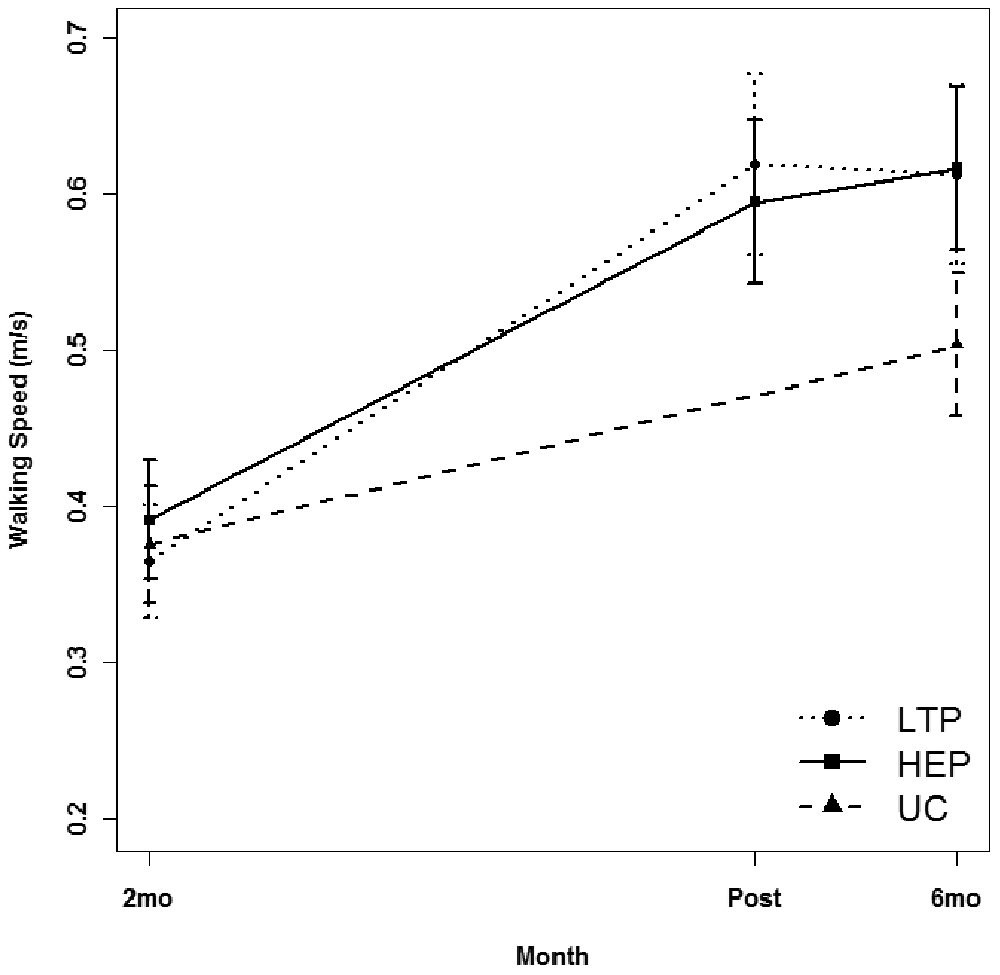
Comparison of mean walking speed for the locomotor training program (LTP), home exercise program (HEP), and usual care (UC) groups at 2 months (2mo) and 6 months (6mo) poststroke; in addition, LTP and HEP mean walking speeds after 30 to 36 sessions of intervention (Post) were plotted.
Mean (SD) for Main Continuous Outcomes at Baseline and 6 Months, by Group, Mean (SD) of Outcome Changes Within Groups, and Mean (95% CI) of Differences in Outcome Changes Between Groups.
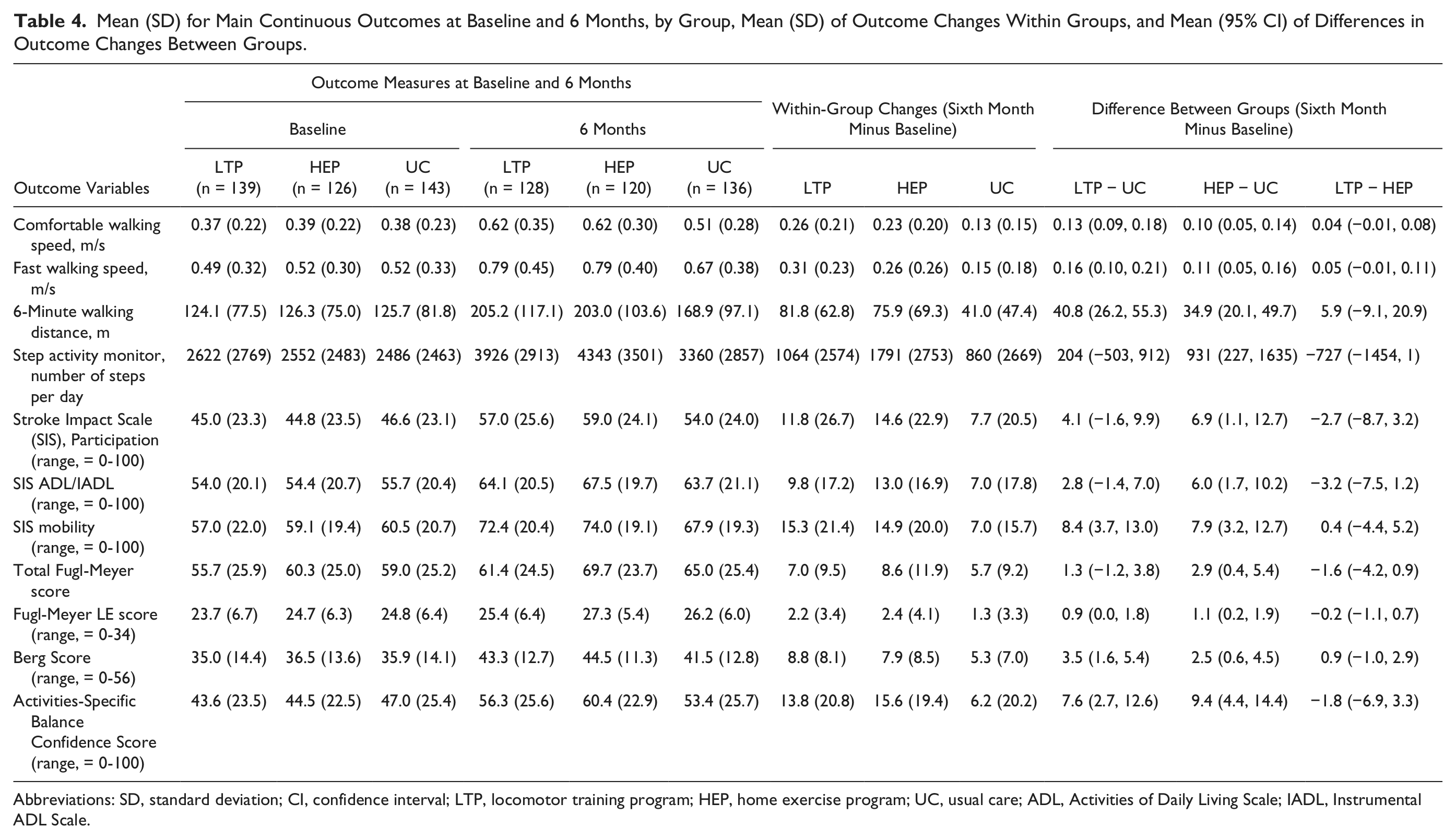
Abbreviations: SD, standard deviation; CI, confidence interval; LTP, locomotor training program; HEP, home exercise program; UC, usual care; ADL, Activities of Daily Living Scale; IADL, Instrumental ADL Scale.
All 3 groups also significantly improved (P < .0001) from baseline in ADL/IADL, physical mobility and social participation, motor recovery (FM), balance score (BBS), balance confidence (ABC Scale), and modified Rankin score (Table 4). With Bonferroni adjustment for multiple testing, the LTP and HEP groups improved more than the UC group in BBS score, ABC Scale score, and physical mobility (P < .0014). In addition, there were trends toward more improvement in the LTP and HEP groups, relative to the UC group, in community steps taken, ADL/IADL, social participation, motor recovery (FM-LE), and modified Rankin scale (Table 4).
UC Postacute Rehabilitation
The number of UC PT visits provided in addition to the 30 to 36 visits received by the LTP and HEP groups was not associated with changes in walking speed (P = .287). However, within the UC-only group (n = 139), a positive association was observed between number of PT visits (median = 11, range = 0-69) and walking speed change (P = .049), adjusting for age and baseline walking speed but not for multiple comparisons.
Adverse Events
There were no between-group differences in total serious adverse events incurred between randomization and 6 months poststroke (Table 3, P = .86). In all, 41% of participants reported at least 1 fall (1.7% had an injurious fall), but no significant differences were found across groups. Overall, 19% experienced multiple falls (LTP, 23%; HEP, 21%; and UC, 13%; P = .09). The LTP group had a greater risk of multiple falls than the UC group. Minor adverse events were reported by 21% of participants, with no significant differences between LTP and HEP, except that the HEP group reported fewer incidents of dizziness/faintness during exercise (0%) than the LTP group (7.9%, P = .001).
Discussion
This study demonstrates the benefits of physical rehabilitation and the potential for gains in functional walking between 2 and 6 months after stroke in participants who had been discharged from inpatient rehabilitation. Of particular importance is that the benefit occurred during the period in which rehabilitation is customarily offered to patients with hemiparesis, and costs are usually covered by Medicare. Standardized PT interventions that included either a progressive task-specific LTP provided in an outpatient clinic or a progressive strength and balance exercise program provided in the home, both in substantial doses, were more effective in improving walking ability than postacute stroke physical rehabilitation provided according to current community practices in California and Florida. HEP and LTP initiated at 2 months after stroke produced equivalent outcomes at the 6-month assessment, as they did at 1 year. 3
The change in walking speed at 6 months poststroke achieved by the UC group (0.13 m/s) was only 52% of that achieved by the LTP group (0.25 m/s) and 57% of that achieved by the HEP group (0.23 m/s), whether initial walking impairment was severe or moderate. The effect sizes for LTP and HEP relative to UC were 0.72 and 0.56, respectively, which rank as medium. The changes in walking speed for the LTP and HEP groups exceeded the minimal clinically important difference for walking speed for patients poststroke during the subacute period (0.16 m/s) 15 and minimal clinically important differences (0.175-0.19 m/s) 16 anchored to changes in Modified Rankin score, patient-perceived change in walking ability, and physical therapist–perceived change in walking ability. In comparison, the walking speed change for the UC group did not reach the established minimal clinically important differences. Our findings of significantly greater improvement in secondary measures of physical mobility, balance (BBS), and balance confidence (ABC) by the LTP and HEP groups compared with the UC group are consistent with known correlations of walking speed with other measures of impairment, activity, and participation. 5
The differences in the results of the 2 interventions tested by LEAPS and those of UC were clinically important. In the LTP group, 18% more patients than in the UC group achieved a transition to a higher level of functional walking ability. The corresponding value in the HEP group was 17%. Transitioning to a higher level of walking ability as a result of increased walking speed poststroke is associated with improvements in mobility and participation. Household ambulators (<0.4 m/s walking speed) poststroke who transition to limited community (≥0.4 m/s and <0.8 m/s) or full ambulatory status (≥0.8 m/s) demonstrate significantly greater changes in mobility and participation, based on the Stroke Impact Scale, compared with stroke survivors who do not transition. 5 Similarly, those who transition from limited community to unlimited ambulatory status also demonstrate significant changes in participation in contrast to persons who do not transition. 5 In the LEAPS trial, the number needed to treat to yield 1 additional patient transitioning to a higher functional walking level was 6. Thus, a relatively small number of patients must be treated to yield 1 additional success when structured, progressive forms of therapy are provided in adequate dose. LEAPS is the largest clinical trial to test conceptually based, well-defined interventions for walking after disabling stroke, so the findings are likely to generalize to people with similar hemiparesis after stroke who are discharged home after inpatient rehabilitation but still are disabled in walking.
Usual Care
The number and duration of UC therapy sessions were carefully monitored, but the content was not. Other studies, however, have described UC after postacute rehabilitation hospitalization, whether delivered in the home or in the outpatient clinic.17,18 Duncan et al 17 observed that the number of PT visits averaged 8.7 (±5.3), and average visit duration was 45.6 (±12.2) minutes. They found an even greater percentage of individuals who did not receive any UC (46%) than we did (21.6%). A survey by the Center for Disease Control of 21 states and the District of Columbia (2005) indicated that 60.3% of stroke patients receive no outpatient rehabilitation therapy and that this proportion was higher than expected if clinical practice guidelines on rehabilitation had been followed. 19 Duncan et al 17 found that therapy was focused on improving strength in 50% of patients, mobility in 50%, balance in 48%, range of motion in 21%, ADL/independent ADL in 14%, and endurance in 8%. There was considerable variability in the type of exercise used. Exercise directed toward improving endurance and strength was progressed in only 13% to 28% of patients. Lang et al 18 reported that outpatient treatment sessions averaged 36 minutes, and the number of repetitions of task practice was relatively small (eg, lower-extremity active exercise included 33 repetitions, and transfers were repeated 10 times). High variability across patients in the number of repetitions and activity type was also observed. Lang et al 18 suggested that with an average of 7 different activities practiced within each outpatient session, the opportunity for more intense practice may have been limited. Thus, UC-only PT, with a median of 11 visits and average duration of 52.5 (±13.5) minutes, may not have provided a high enough dose of practice with a concentrated emphasis on progression of skill training and neuromuscular challenge to achieve maximal gains in mobility.
For both LEAPS interventions, even with their very different training techniques (ie, task-specific training vs impairment-based training), participant baseline ability was used to set goals, and participant ability was challenged during each training session. Therapists delivering both HEP and LTP were trained to rigorously advance progression in every session, and participants were engaged in setting goals for practice. Feedback about mobility and exercise during PT has a positive effect on subsequent performance. 20 For LTP, progression occurred in the form of increased body weight load, stepping time, treadmill speed, and independence on the treadmill and in overground walking. During HEP, progression was achieved by increasing the number of repetitions, resistance, and task and balance difficulty. Other than pointing to the effects of greater structured practice, our data do not enable us to measure how such factors may have been responsible for the greater efficacy of HEP and LTP relative to UC.
With the number of UC PT visits (median 11 visits, range 0-69) observed for the UC-only group, improvements in walking speed did not reach those achieved by the LTP and HEP groups. A greater number of UC visits in the UC-only group was weakly but significantly associated with improvement in walking speed. However, the number of UC PT visits received in addition to LTP and HEP sessions did not seem to affect the final walking speed of these groups. The significant advantage of LTP and HEP in achieving meaningful changes in walking compared with only UC may be attributable to standardization, higher dose, the rigor of progression and challenge, and the specific features of these therapies, that is, task-specific walking training and impairment-based exercise.
Our results might lead to the inference that HEP and LTP were superior to UC simply by virtue of the greater quantity and intensity of therapy received. However, as noted, there was but a weak relationship between number of UC sessions and gains in walking speed. Furthermore, because HEP and LTP achieved similar results, it does not mean that they did so by the same mechanisms. It is possible that the same neuroplastic mechanisms can be engaged by the 2 different treatments or the 2 treatments engage different but complementary mechanisms. Despite possible differential engagement at the individual participant level, at the population level, the 2 treatments appear to be equivalent. In addition, the conduct of HEP in the home may have enhanced its efficacy. Learning research provides much evidence that retention is dependent on the extent of commonality between circumstances at training and circumstances at time of retrieval.21,22 Our trial did not address the issue of whether task-specific training has less conceptual validity than generally thought or whether training on a treadmill with body-weight support is less task specific than usually considered.
A higher risk of multiple falls in the LTP group than in the UC group may hypothetically be attributed to multiple factors (eg, medications, vision, urinary incontinence, balance, and home environment). 23 Because mobility skills were challenged during training, the LTP group may have taken greater risks during ambulation or transfers in the home and community than the HEP or UC groups. 24 On the other hand, the HEP group received home-based therapy, and treatments (eg, strength and balance training) were practiced where most falls occur—in the home. This may have had an effect in reducing falls risk.
The 1-year outcomes of the LEAPS trial determined that the task-specific locomotor training was not superior to the impairment-based exercise program. 3 However, the comparison at 6 months poststroke of LTP and HEP with UC determined that both interventions were superior to UC in terms of the proportion of participants that transitioned to a higher functional level of walking. Just as for the 1-year outcomes, 50.4% of those who received LTP and 49.2% of those who received HEP successfully transitioned to a higher functional level of walking at 6 months. Although this success rate is significant and clinically meaningful for LTP and HEP groups, nearly half of our participants (49.6% in the LTP and 50.8% in the HEP group) did not achieve a successful outcome after 30 to 36 sessions. However, 68% of the UC group did not achieve a successful outcome. Further studies are needed to evaluate the conceptual bases and mechanisms of effect for the interventions (eg, neuromuscular benefit, home-based vs clinic-based therapy, patient preference), to examine the appropriate therapy dose, and to combine or augment these interventions 25 to increase the proportion of individuals who transition to a higher level of functional walking ability.
Limitations
The characterization of UC was limited to the number of PT visits and the time spent in a PT session. No information was collected on the goals that were addressed during the PT sessions (eg, transfers, bed mobility, and ambulation) or the particular interventions that were used (eg, neuromuscular reeducation, balance training, and gait training). Other forms of physical rehabilitation, such as occupational therapy, may also have been provided and may have affected functional gains. The reason for the modest number of UC visits received by each patient is not known, but it could reflect acceptance of functional status, prescribing practices, accessibility to care, and psychosocial reasons.
Summary
Standardized, progressive, goal-oriented, and individualized HEP and LTP programs delivered with substantial frequency, intensity, and duration were more effective in improving functional walking ability than PT provided according to current usual practices. Improvements in walking speed in the LTP and HEP groups were twice those of UC and exceeded thresholds for minimal clinically important differences. These findings suggest that more structured and progressive PT interventions, using task-specific or impairment-based training, have the potential for better rehabilitation outcomes for persons disabled after stroke.
Footnotes
Acknowledgements
The following is a list of LEAPS investigators at various centers. Wake Forest University Administrative Coordinating Center: Pamela Duncan, PT, PhD, and Alethea Amponsah; Duke University Administrative Coordinating Center: Sarah Hayden, Mysha Sissine, and Quishi Feng, PhD; Brooks Rehabilitation Hospital, Jacksonville, FL: Deborah Stewart, MD, Trevor Paris, MD, and Joann Gallichio, PT, DSc; Florida Hospital, Orlando, FL: Mitchell Freed, MD, Michelle Dolske, PhD, Craig Moore, PT, and Bettina Brutsch, PT; Long Beach Memorial Hospital, Long Beach, CA: H. Richard Adams, MD, Diehma Hoang, MD, and Anita Correa, PT; Sharp Rehabilitation Center, San Diego, CA: Jerome Stenehjem, MD, Roxanne Hon, MD, and Molly McLeod, PT; University of Southern California: David Alexander, MD; UCLA Medical Center: Julie Hershberg, DPT, and Samneang Ith-Chang, DPT; Florida Clinical Coordinating Center, University of Florida: Andrea L. Behrman, PT, PhD, and Dorian K. Rose, PT, PhD; California Clinical Coordinating Center, University of Southern California: Julie K. Tilson, DPT, MS; Data Management and Analysis Center, University of Southern California: Steven Cen, PhD, Chris Han, MS, and James Gardner; University of Florida, Gainesville, FL: Yunfeng Dai, MS, and Xiaomin Lu, PhD. Consultants: Anatole D. Martin, PhD, and Richard Schofield, MD, University of Florida. Steering Committee: Pamela Duncan, PT, PhD, Wake Forest University; Andrea L. Behrman, PT, PhD, Samuel S. Wu, PhD, and Stephen Nadeau, MD, University of Florida; Stanley P. Azen, PhD, University of Southern California; Bruce H. Dobkin, MD, University of California, Los Angeles; and Sarah K. Hayden, Duke University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from National Institute of Neurological Disorders and Stroke and the National Center for Medical Rehabilitation Research (RO1 NS050506).
Authors’ Note
Trial registration: NCT0024391. There is no commercial interest of the authors relevant to the subject of the article. ClinicalTrials.gov NCT00243919.