
Abstract
Background. Obstacle crossing is a balance-challenging task and can cause falls in people with Parkinson’s disease (PD). However, programs for people with PD that effectively target obstacle crossing and dynamic balance have not been established. Objective. To examine the effects of virtual reality–based exercise on obstacle crossing performance and dynamic balance in participants with PD. Methods. Thirty-six participants with a diagnosis of PD (Hoehn and Yahr score ranging 1 to 3) were randomly assigned to one of three groups. In the exercise groups, participants received virtual reality–based Wii Fit exercise (VRWii group) or traditional exercise (TE group) for 45 minutes, followed by 15 minutes of treadmill training in each session for a total of 12 sessions over 6 weeks. Participants in the control group received no structured exercise program. Primary outcomes included obstacle crossing performance (crossing velocity, stride length, and vertical toe obstacle clearance) and dynamic balance (maximal excursion, movement velocity, and directional control measured by the limits-of-stability test). Secondary outcomes included sensory organization test (SOT), Parkinson’s Disease Questionnaire (PDQ39), fall efficacy scale (FES-I), and timed up and go test (TUG). All outcomes were assessed at baseline, after training, and at 1-month follow-up. Results. The VRWii group showed greater improvement in obstacle crossing velocity, crossing stride length, dynamic balance, SOT, TUG, FES-I, and PDQ39 than the control group. VRWii training also resulted in greater improvement in movement velocity of limits-of-stability test than TE training. Conclusions. VRWii training significantly improved obstacle crossing performance and dynamic balance, supporting implementation of VRWii training in participants with PD.
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disease. With progression of the disease, patients may demonstrate postural instability, gait dysfunction, difficulty managing functional tasks, such as obstacle crossing, and frequent falls.1-4 More than two thirds of community-dwelling individuals with PD experience falls once per year, and tripping over obstacles is the major cause of these falls. 5 During obstacle crossing, participants with PD usually step their leading foot closer to the obstacle than age-matched controls because of their smaller steps, which may result in hitting the obstacle and subsequent falls. 6 These individuals also adopt a conservative strategy during obstacle crossing and maintain their center of mass (COM) more medially to their stance leg. 7 This alteration reduces the distance between the center of pressure (COP) and COM throughout the obstacle crossing task compared with normal older adults. 8 Therefore, strategies to improve balance and obstacle crossing ability may help improve functional ability and to reduce the incidence of falls.
Some patients with PD may lack satisfactory to drug regimens or surgical options, and they still have considerable symptoms while on medications. The lack of satisfactory treatment options provides motivation to investigate the effects of exercise on functional improvement. Stretching, strengthening, balance exercise, and gait training improve motor function, balance, and gait performance in participants with PD.9-13 Treadmill training has also been used widely in participants with PD to improve gait performance and walking economy.14-16 However, the effects of such training on obstacle-crossing performance has not yet been investigated. Combining resistance, aerobic, balance, stretching, and treadmill training are likely to be optimal for improving gait speed in participants with PD. 17 Whether the combination of training can carry-over to obstacle crossing performance need further investigation.
Virtual reality (VR) systems are novel and potentially useful technologies that allow users to interact with a computer-generated scenario. 18 Augmented visual, sensory, and auditory feedback are provided when subjects performing tasks in virtual environment. 19 VR training has been used in older adults and stroke patients to improve postural control, increase mobility, and reduce fall risk.20-24 In PD participants, VR training has been demonstrated to improve sensory organization. 25 VR combining treadmill training was also reported to improve gait performance during usual and complex challenging condition (dual task and obstacle crossing) in PD participants. 26 However, VR combining different types of exercise on obstacle-crossing and balance performance has not yet been explored. Recently, the gaming industry has developed a variety of affordable and accessible VR systems, such as Wii Fit, that have been reported to improve functional ability in PD participants, such as timed up and go (TUG), sit to stand, unipedal stance, balance, walking speed, and overall quality of life.27-30 These effects, however, have yet to be validated in a randomized controlled trial. Furthermore, whether this VR-based Wii Fit exercise is more effective than traditional exercise, especially regarding its effects on advanced gait function such as obstacle crossing, warrants investigation.
Therefore, the purpose of this study was to elucidate the effects of VR-based Wii Fit exercise on obstacle crossing and dynamic balance ability in participants with PD by comparing the results of Wii Fit training, traditional exercise, and a no-exercise control.
Methods
Participants
Participants were recruited from a medical center in Taiwan and were diagnosed with idiopathic PD by a neurologist. The diagnostic criteria were at least 2 of the 4 features (resting tremor, bradykinesia, rigidity, and asymmetric onset) in which the resting tremor or bradykinesia must be present. 31 All participants met the following inclusion criteria: (a) Hoehn and Yahr stages I to III, (b) ability to walk independently without any walking aids, (c) stable medication usage, (d) with or without deep brain stimulation, and (e) a score of ≥24 on the Mini-Mental State Examination (MMSE). The exclusion criteria were as follows: (a) unstable medical condition; (b) history of other neurological, cardiopulmonary, or orthopedic diseases known to interfere with participation in the study; (c) past history of seizure; (d) use of cardiac pacemaker; and (e) vision deficits. In total, 43 individuals were identified as potential participants for this study. Of these, 36 participants provided informed consent, which was approved by the Institutional Human Research Ethics Committee of Chang Gung Medical Foundation (Figure 1).
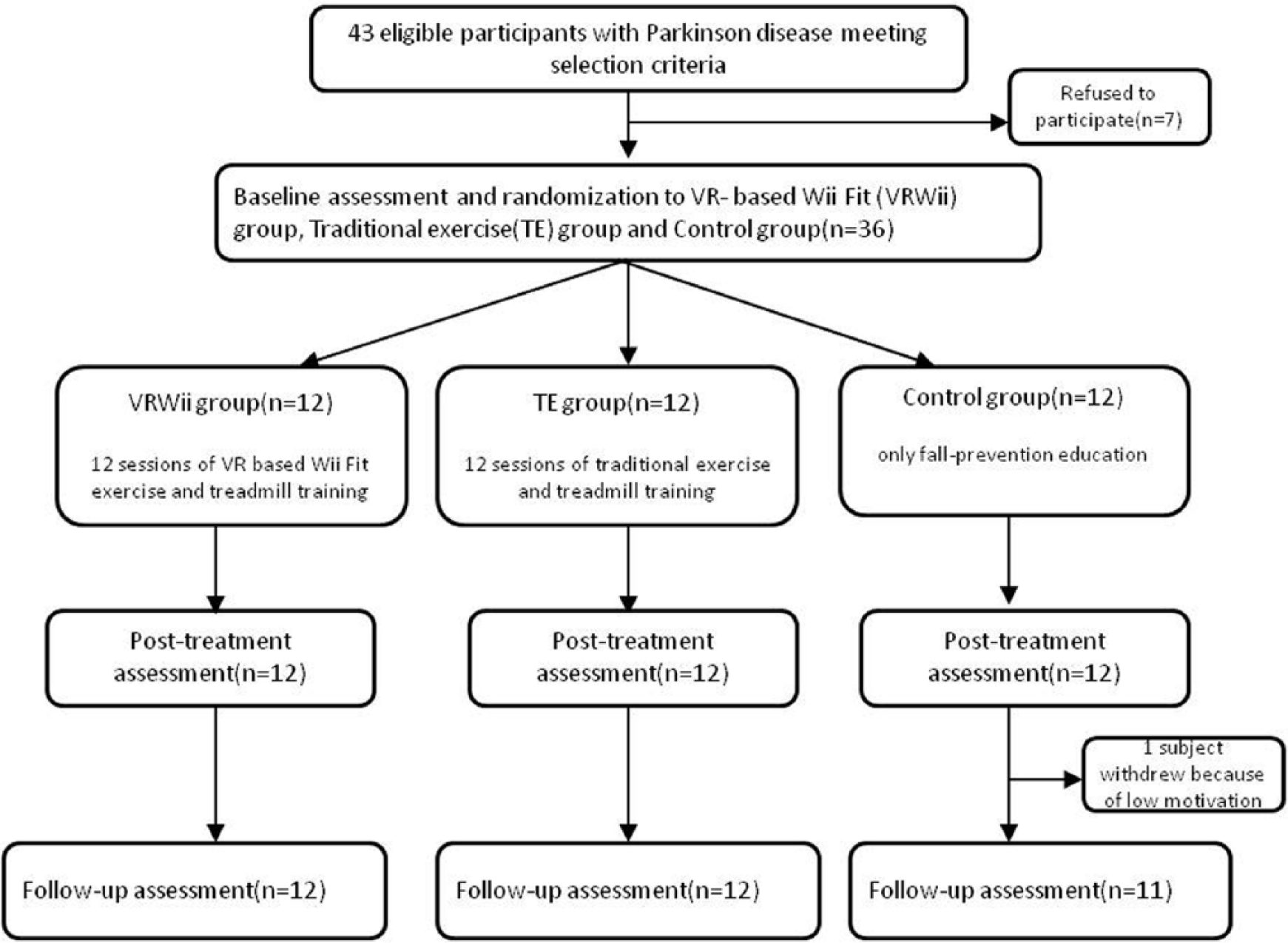
Flowchart of participants recruited in this study.
Experimental Design
This study was a single-blinded, stratified, randomized controlled trial. The stratification was achieved based on the Hoehn and Yahr stage as follows: stage 1 to 1.5, stage 2 to 2.5, and stage 3. An individual who was not involved with the study selected sealed envelopes to assign participants to 1 of the 3 groups. Participants received VR-based Wii Fit exercise (VRWii group) or traditional exercise (TE group) for 45 minutes with additional treadmill training for 15 minutes. The exercise was administered for a total of 12 sessions (2 sessions per week) over a 6-week period by the same physical therapist. Individuals in the control group received only fall-prevention education, such as minding the environmental factors (slippery surface, obstacles, stairs, uneven ground) after the baseline assessment and were encouraged to carry out their regular exercise. All outcomes were measured the day before intervention (pre), the day after completing the intervention (post), and the 30th day after completing the intervention (follow-up) by the same rater blinded to group assignment. The measurement and intervention were conducted with patients in the “on” state.
Interventions
Traditional Exercise (TE)
This program included 10 minutes of stretching exercises, 15 minutes of strengthening exercises, and 20 minutes of balance exercises in each session as described below.
Stretching exercises: The stretching exercises focused on upper body and upper and lower extremities with gentle joint extension and flexion and trunk rotation in a standing position. Deep breathing was emphasized during the exercise.
Strengthening exercise: The strengthening exercises focused on the lower extremity muscles that are important for posture, balance, and gait. Participants performed the following exercises in standing position: (a) one leg forward/sideward swing, (b) stepping up and down, (c) multidirectional leg raising, (d) heel and toe raising, and (e) squatting. Participants performed 3 sets of 10 to 15 repetitions for each activity. Participants used ankle weights that started at 1 kg and were gradually increased to 2 kg for each leg. Natural breathing was emphasized during the exercise.
Balance exercises: The balance exercises were combinations of dynamic balance training and sensory integration training. The dynamic balance training exercises were symmetric weight shifting with slow and fast speed, catching and throwing balls, and multidirectional stepping in a standing position. The sensory integration training exercises included single leg stance with eyes open and closed and standing on foam with eyes open and closed.
The progressions in both TE and VRWii group included adding more weights during strengthening exercise, increasing the number of repetitions, and increasing difficulty of exercise, such as increasing the height of the blocks during the stepping-up exercise, increasing the forward/sideward stepping distance during the stepping exercise, holding the squatting position for longer duration during the squatting exercise. The criteria for progression were determined by the ability of the participant to perform the activities without difficulty and by the perceived exertion (Borg rate of perceived exertion <13, somewhat hard).
Virtual Reality–Based Wii Fit Exercise
The Wii Fit Plus gaming system and Wii Fit balance board (Nintendo Phuten Co, Ltd, Taiwan) were used for VRWii exercise. The Wii Fit balance board is a novel system that tracks changes in the COP during exercise. A virtual environment was displayed on a screen with a 230 cm width and height in front of the participant. Through avatar technology, images were projected on the screen through a projector. The virtual character provides instantaneous visual and auditory feedback. Participants can imitate the virtual character and adjust their own movements according to feedback (knowledge of the performance) in real time (<20 ms lag between player and avatar movement). At the end of the game, the Wii Fit system also provides the total score on the screen (knowledge of the results). In each Wii Fit exercise session, participants underwent 10 minutes of yoga exercises, 15 minutes of strengthening exercises, and 20 minutes of balance games as described below.
Yoga exercises: The yoga exercises were emphasized more on muscle stretching. This program included sun-salutation modified lunges, chair pose, tree pose with arms straight above the head and palms together, and table top in standing position.
Strengthening exercises: The exercise program, intensity, and principle of adding ankle weights were similar to the strengthening exercise program emphasized in the TE group, but in this case, the strengthening exercises were performed in a VR-based environment.
Balance games: The balance games included the soccer heading, marble balance, ski slalom, and balance bubble. When performing these games, participants needed to shift their COM as quickly and accurately as possible to hit the soccer, put the rolling marble in the hole, ski without hitting the obstacles, and navigate the bubble through the maze without popping it.
Treadmill Training
Participants in both exercise groups received treadmill training (Biodex, Shirley, NY) after the above exercise training sessions to enhance the effects of exercise training. Each treadmill session lasted 15 minutes. The treadmill speed was set at 80% of the individual’s overground comfortable walking speed and was increased by an increment of 0.2 km/h per 5 minutes as tolerated. A safety harness without body weight support was provided during treadmill training to prevent falls.
Primary Outcomes
Obstacle-Crossing Performance
The Liberty system (Polhtemus, Inc, Colchester, VT) was used to measure spatial temporal variables during obstacle crossing. This system is an electromagnetic motion capture device for tracking 3-dimensional movement at a speed of 240 updates per second. Two sensors were attached to the top of the second toe of each foot. These sensors recorded the 3-dimensional positioning of the foot. The validity and reliability of the Liberty system have been previously established. 32 Obstacle crossing required participants to walk on a 10-meter walkway with an obstacle positioned in the middle of the walkway. The obstacle was a plastic crossbar (60 cm long and 1.5 cm in diameter) supported by 2 vertical posts. The height of the obstacle was 20% of the subject’s leg length (14-20 cm) to emulate the height of a curb or stair. During obstacle crossing trials, participants initiated walking, stepped over the obstacle, and continued to walk to the end of the walkway at a comfortable speed without any constrain. Three obstacle-crossing variables were analyzed as follows:
Crossing stride length: The distance from the heel-strike of the leg before the obstacle to the heel-strike of the same leg after crossing the obstacle.
Crossing stride velocity: The velocity from the heel-strike of the leg before the obstacle to the heel-strike of the same leg after crossing the obstacle.
Vertical toe-obstacle clearance: The vertical distance between the toe sensor of the leg and the obstacle when the toe of the leg was directly above the obstacle.
Dynamic Balance Performance
Dynamic balance was assessed by the Balance Master system (NeuroCom International, Inc, Clackamas, OR). Limits of stability (LOS) testing was used to document dynamic balance performance. 33,34 To assess the LOS, the subject stood on the forceplate and shifted his or her center of gravity (COG) to reach a maximal distance in the target direction as quickly and accurately as possible without moving the feet. The directions assessed included forward, right, and left. Because of insignificant difference between right and left direction, data from the right and left directions were averaged to indicate sideward control. Movement velocity (MV), maximum excursion (ME), and directional control (DC) were collected during the LOS test in this study. MV is defined as the average speed in degrees/second in a specific direction. ME is defined as the farthest distance traveled by the COG during the trial. DC is defined as the amount of movement in the intended direction minus the amount of extraneous movement. A DC score of 100% indicates that the participant does not deviate from a straight path during the test.
Secondary Outcomes
Sensory Integration Ability
The sensory organization test (SOT) was assessed using the Balance Master system to evaluate sensory integration ability. The equilibrium score was obtained under each of 6 visual and support surface conditions (SOT1-SOT6). Through sway of the visual surround and support surfaces, inaccurate information was delivered to the somatosensory, visual, and vestibular systems. The SOT scores used in this study are the weighted averages from all equilibrium scores to indicate sensory integration ability. 35
The 39-Question Parkinson’s Disease Questionnaire
This questionnaire was developed to assess the quality of life of patients with PD. 36 This questionnaire contains 8 dimensions with 39 items and assesses mobility, activities of daily living, emotions, stigmas, social issues, cognition, communication, and body pain. Subjects filled out the questionnaire according to the presence of problems during the previous month. The validity of the 39-question Parkinson’s Disease Questionnaire (PDQ39) was reported previously. 37 A higher score represents a poor quality of life. The Chinese version of the PDQ39 was used in this study. 38
Falls Efficacy Scale–International
The Falls Efficacy Scale–International (FES-I) is widely used in elderly persons to indicate concerns about falling. There are 16 items assessing functional tasks and social-related activities, and scoring ranges from 1 to 4. Subjects rated the items according to their concerns about falling. A higher score indicates a greater concern about falling. The validity of the FES-I has been reported for older adults.39,40
Timed Up and Go Test
For the Timed Up and Go (TUG) test, participants were asked to stand up from a chair, walk 3 m, turn around, return to the chair, and sit down. The time taken to complete this task was measured with a stopwatch. This test has been demonstrated to have high reliability in people with PD. 41
Statistical Analysis
Descriptive statistics were generated for all variables, and distributions of variables were expressed as mean ± standard deviation. Intergroup differences among baseline characteristics were evaluated using the 1-way analysis of variance (ANOVA) or χ2 analysis with significant level at P < .05. Change values were calculated by subtracting the baseline data from the post-training data or by subtracting the baseline data from the follow-up data. To analyze intergroup improvement, the changes values were analyzed using a 1-way ANOVA with group as a factor, followed by Tukey post hoc test. As change values (between post and pre, and between follow-up and pre) in 1-way ANOVA were examined twice, the significance level was corrected with a Bonferroni correction (P = .025) to reduce the possibility of statistical error.
Results
Thirty-six participants were randomly assigned to the control, TE, or VRWii groups (n = 12 for each group). None of the participants reported any adverse events. One participant in the control group withdrew at the time of follow-up because of low motivation (Figure 1). No significant group differences in baseline demographic characteristics were found (Table 1). Similarly, no significant group differences were noted in the outcome measures at preintervention assessment (Tables 2-4).
Demographic Characteristics of Included Participants.
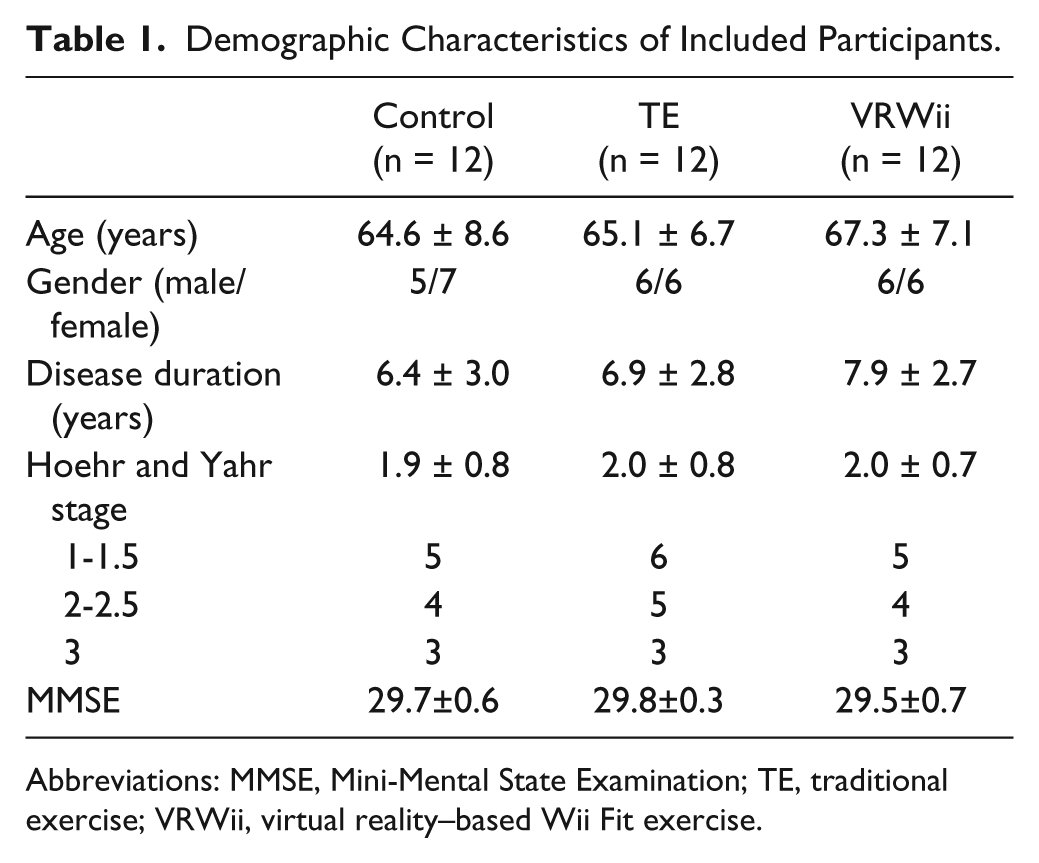
Abbreviations: MMSE, Mini-Mental State Examination; TE, traditional exercise; VRWii, virtual reality–based Wii Fit exercise.
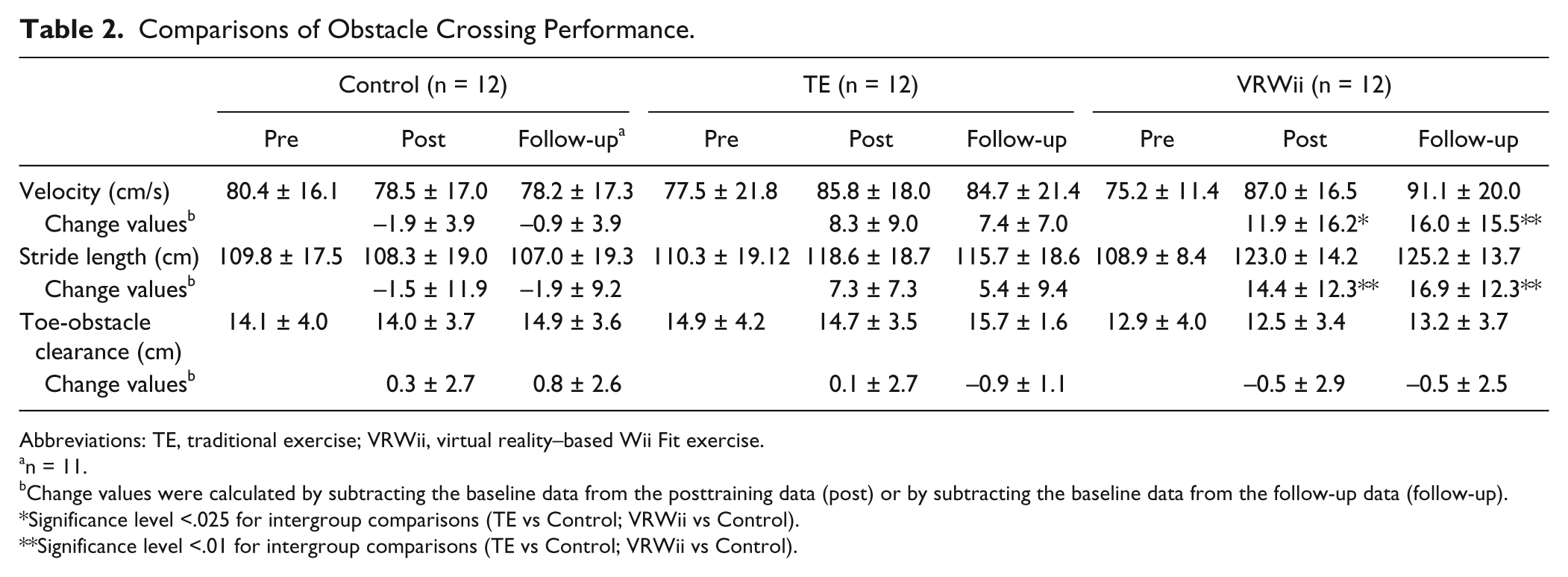
Comparisons of Obstacle Crossing Performance.
Abbreviations: TE, traditional exercise; VRWii, virtual reality–based Wii Fit exercise.
n = 11.
Change values were calculated by subtracting the baseline data from the posttraining data (post) or by subtracting the baseline data from the follow-up data (follow-up).
Significance level <.025 for intergroup comparisons (TE vs Control; VRWii vs Control).
Significance level <.01 for intergroup comparisons (TE vs Control; VRWii vs Control).
Comparisons of Dynamic Balance and SOT Score.
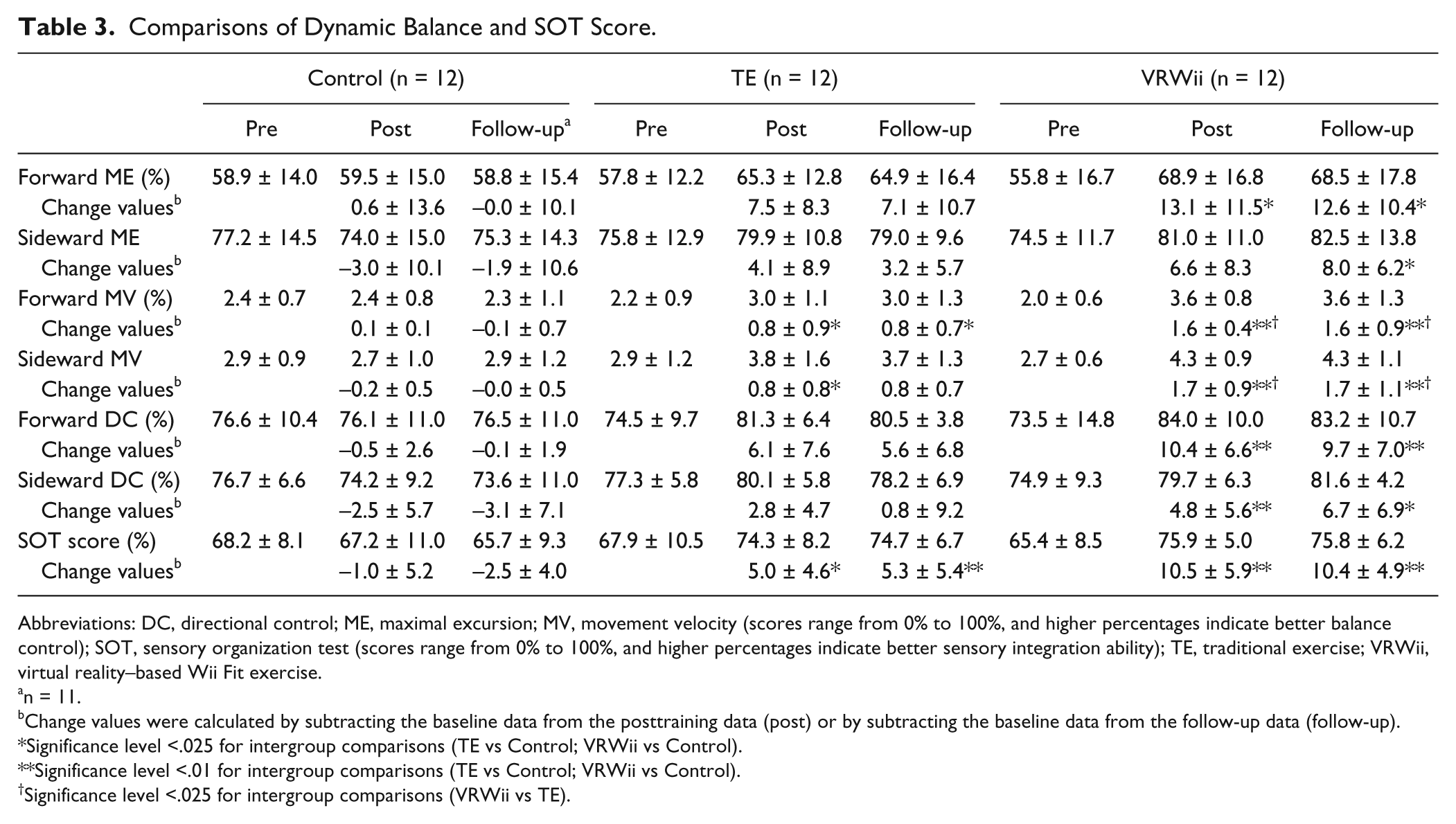
Abbreviations: DC, directional control; ME, maximal excursion; MV, movement velocity (scores range from 0% to 100%, and higher percentages indicate better balance control); SOT, sensory organization test (scores range from 0% to 100%, and higher percentages indicate better sensory integration ability); TE, traditional exercise; VRWii, virtual reality–based Wii Fit exercise.
n = 11.
Change values were calculated by subtracting the baseline data from the posttraining data (post) or by subtracting the baseline data from the follow-up data (follow-up).
Significance level <.025 for intergroup comparisons (TE vs Control; VRWii vs Control).
Significance level <.01 for intergroup comparisons (TE vs Control; VRWii vs Control).
Significance level <.025 for intergroup comparisons (VRWii vs TE).
Comparisons of TUG, PDQ39, and FES-I.
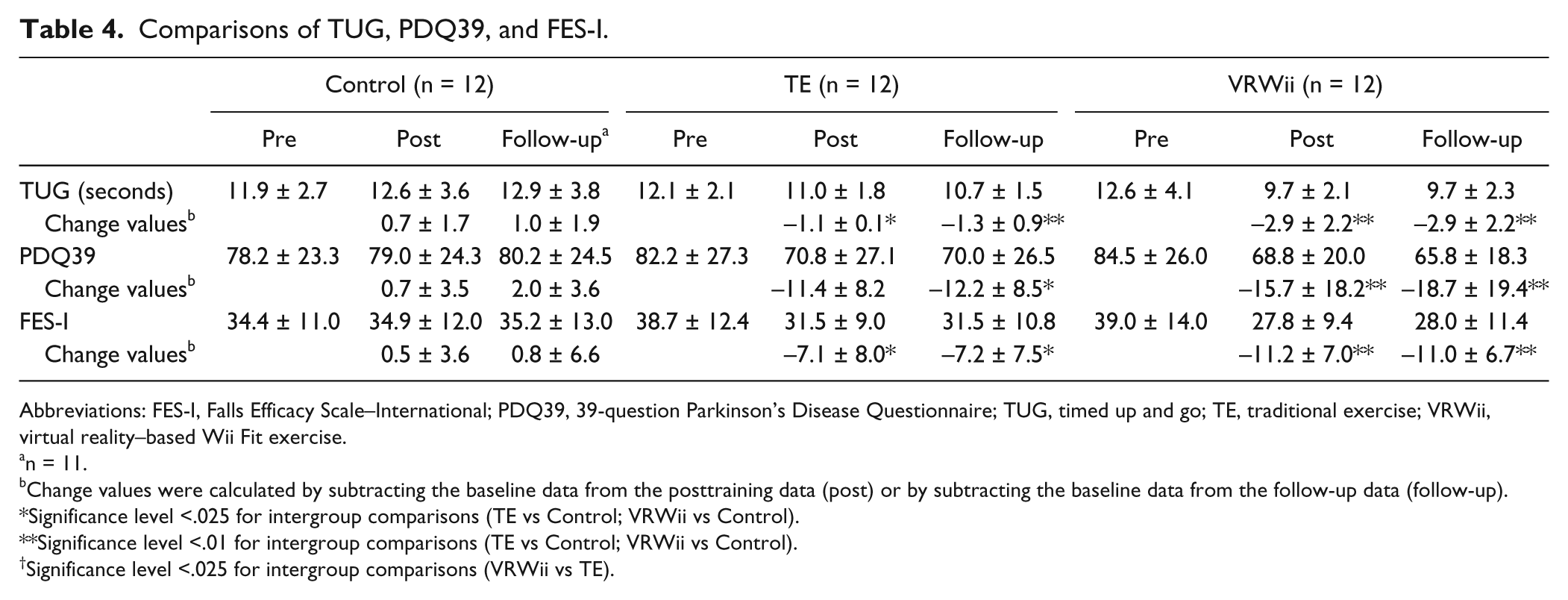
Abbreviations: FES-I, Falls Efficacy Scale–International; PDQ39, 39-question Parkinson’s Disease Questionnaire; TUG, timed up and go; TE, traditional exercise; VRWii, virtual reality–based Wii Fit exercise.
n = 11.
Change values were calculated by subtracting the baseline data from the posttraining data (post) or by subtracting the baseline data from the follow-up data (follow-up).
Significance level <.025 for intergroup comparisons (TE vs Control; VRWii vs Control).
Significance level <.01 for intergroup comparisons (TE vs Control; VRWii vs Control).
Significance level <.025 for intergroup comparisons (VRWii vs TE).
Obstacle-Crossing Performance
The results of the obstacle crossing performance evaluation are shown in Table 2 and Figure 2. The VRWii group showed significant improvements in crossing stride length and velocity compared with the control group after training and at the 1-month follow-up (stride length, VRWii vs control, P = .003 at posttraining, P = .001 at follow-up; stride velocity, VRWii vs control, P = .011 at posttraining, P = .001 at follow-up); however, no significant difference between the VRWii and the TE groups was found. The participants contacted the obstacle in 2% of the trials (15 failure trials out of total 642 trials with 6 leading foot toe contact and 9 trailing foot toe contact).
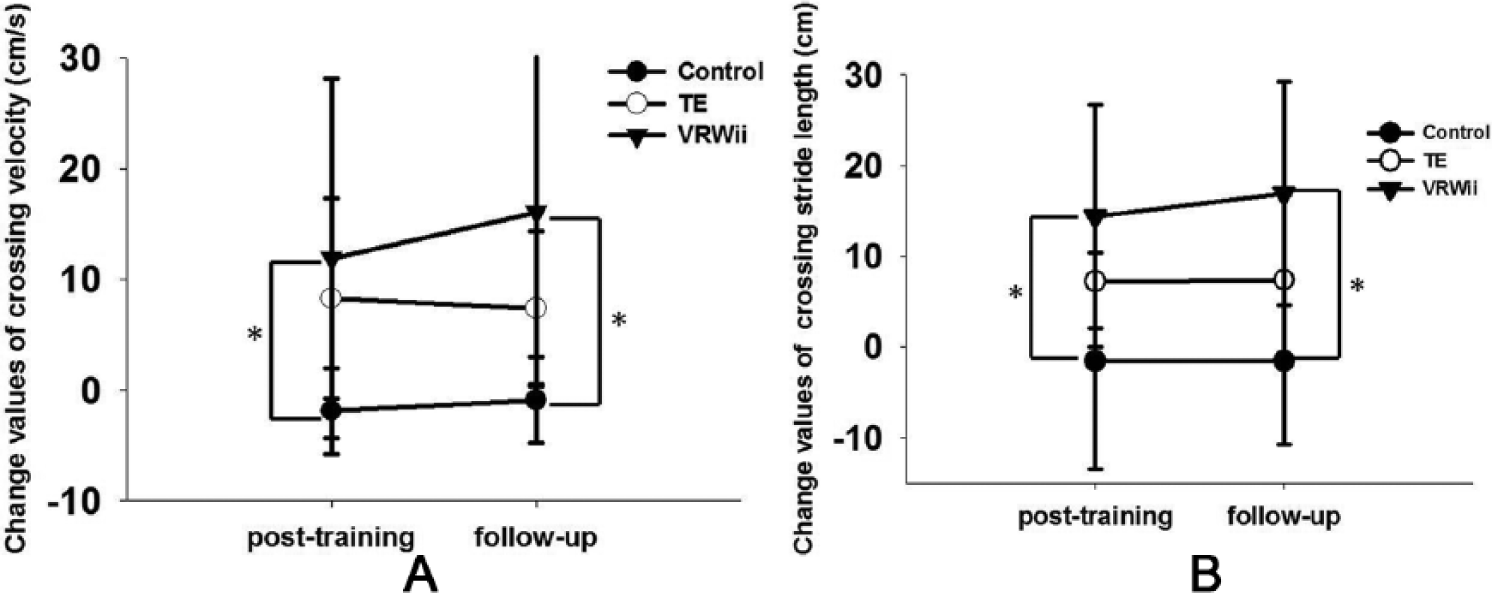
Change values of crossing velocity (A) and change values of crossing stride length (B) at post and follow-up. VRWii group showed significant improvements in crossing velocity (P = .011) and stride length (P = .003) compared with the control group after training. The improvements at posttraining were retained at follow-up (crossing velocity, P = .001; crossing stride length, P = .001).
Dynamic Balance and Sensory Organization Test
The results of dynamic balance assessment are shown in Table 3. Both the VRWii and the TE groups exhibited significant improvements in MV and SOT compared with the control group after training and at the 1-month follow-up (forward MV, VRWii vs control, P < .001 at posttraining, P < .001 at follow-up, TE vs control, P = .015 at posttraining, P = .012 at follow-up; sideward MV, VRWii vs control, P < .001 at posttraining, P < .001 at follow-up, TE vs control, P = .004 at posttraining; SOT, VRWii vs control, P < .001 at posttraining, P < .001 at follow-up, TE vs control, P = .015 at posttraining, P = .001 at follow-up). Moreover, the VRWii group exhibited greater improvement than the TE group on MV (forward MV, VRWii vs TE, P < .001 at posttraining, P < .001 at follow-up; sideward MV, VRWii vs TE, P < .001 at posttraining, P < .001 at follow-up). The VRWii group also showed significant improvements in ME and DC compared with the control group after training and at follow-up (forward ME, VRWii vs control, P = .023 at posttraining, P = .014 at follow-up; sideward ME, VRWii vs control, P = .011 at follow-up; forward DC, P = .001 at posttraining, P = .002 at follow-up; sideward DC, P = .006 at posttraining, P = .012 at follow-up).
Timed Up and Go
The results of TUG analysis are shown in Table 4. Both the VRWii and the TE groups showed significant improvement in TUG results compared with the control group after training and at follow-up (VRWii vs control, P < .001 at posttraining, P < .001 at follow-up; TE vs control, P = .025 at posttraining, P = .008 at follow-up).
PDQ39 and FES-I
Both the VRWii and TE groups showed significant improvements in PDQ39 and FES-I scores compared with the control group at follow-up (PDQ39, VRWii vs control, P = .004 at posttraining, P = .001at follow-up, TE vs control, P = .022 at follow-up; FES-I, VRWii vs control, P < .001 at posttraining, P = .001 at follow-up, TE vs control, P = .019 at posttraining, P = .021 at follow-up); however, there was no significant difference between the VRWii and TE groups in the PDQ39 and FES-I results (Table 4).
Discussion
In this study, we demonstrated that 12 sessions of VRWii as part of a multifaceted training intervention is effective in improving obstacle-crossing performance in participants with PD compared with control group. Such improvement is accompanied by concurrent increases in dynamic balance control and sensory integration ability, and these improvements persisted for at least one month. We further demonstrated that the VR-based Wii Fit exercise is more effective than traditional exercise in improving MV in LOS test. The LOS test can indicate balance control in participants with PD. 42 In addition, the LOS is useful in the prospective assessment of falls risk in PD patients.43,44 Therefore, the VRWii as part of a multifaceted training intervention can exert better results than traditional intervention with both statistical and clinical meaningfulness.
The relationship between obstacle-crossing performance and dynamic balance has been demonstrated in our previous study, in which crossing stride length and velocity correlated with ME, MV, DC in the LOS test, and SOT. 45 In the present study, we designed the treatment program according to these influencing factors and noted that improved dynamic balance and SOT after 12 sessions of VRWii training coincides with improved crossing performance. Obstacle crossing is a balance demanding task that requires control of single leg support and COM forward shifting 46 which are core programs of our balance exercise. With improved balance, the individuals may move their COM further, faster and more correctly. 47 Meanwhile, with improved SOT, the individuals may process sensory information (vision, vestibular, and somatosensory) more accurately in order to control their trunk and limbs in response to sensory challenges. 48 Therefore, participants in the VRWii group demonstrated increased stride length and velocity strategies during obstacle crossing. Previous studies reported that individuals with PD place their leading foot closer to the obstacle and more often hit the obstacle. 6 Therefore, a longer stride length may reduce the risk of the leading foot hitting the obstacle. 49 Also, a faster crossing velocity may represent an effective motor coordination strategy. However, this safe and efficient crossing strategy was not achieved with the traditional exercise training. Previous studies indicated that participants with PD can adjust the vertical toe-obstacle clearance in response to different obstacle heights, although the short stride length remains. Therefore, PD participants have greater difficulty in lengthening their step over the obstacle than increasing the foot height during the obstacle crossing.6,50 Our results suggest that VRWii training is especially effective in increasing the horizontal crossing length and velocity as opposed to improving vertical toe clearance in participants with PD.
Previous studies on exercise intervention found that PD participants improved their dynamic balance after 20 sessions over 10 weeks of training. 13 In the present study, participants in both exercise groups showed significant improvements in MV of LOS test as compared with the control. However, VRWii exercise resulted in additional improvements in ME and DC, which are key factors of crossing performance. 45 Furthermore, the MV was improved more in the VRWii group than the TE group, suggesting that incorporating VRWii training into the exercise program is effective for patients with PD for improving balance and obstacle crossing ability.
Virtual reality–based Wii Fit exercise was more effective than traditional exercise on improving dynamic balance which may be due to the following factors. First, VR is a form of external feedback. In this study, knowledge of performance and knowledge of results were provided during training in the form of auditory and visual feedback. Participants were then able to make corrections according to the feedback to enhance their motor performance. Previous studies reported that PD participants rely more on external cues or feedback to execute movement as a result of an internal trigger deficit. 36 Second, some of our VRWii gaming programs require either attention or problem-solving ability. Active participation in cognition-demanding programs may activate cognitive pathway networks and consolidate the learning effect. 18 Third, observation of the virtual performance on the screen may also facilitate the participation of mirror neurons. Activation of mirror neurons located in cerebral cortices may help to make connections in the neural network that enhance learning and motor performance. 51 Taken together, these possibilities may help participants with PD improve their mobility and balance control, as demonstrated in the LOS test. It should also be noted that treadmill training was part of our training program. The effect of treadmill training is known to improve gait performance and balance, thus we included the treadmill training after VR-based Wii Fit exercise (VRWii group) and traditional exercise (TE group) for 15 minutes to enhance the effects of exercise training. Therefore, the improvements in both exercise groups could also partly be attributed to the treadmill training.
A previous study indicated that an increase in the weighing of sensory inputs is required to prepare for an ensuing change in direction. 52 During TE and VRWii training, the participants were required to adjust their joint angles to shift their body weight and to move the head and trunk. These changes in joint angles and head positions stimulated somatosensory and vestibular receptors to enhance the central integration ability, as demonstrated by the results of SOT.
Improvement in dynamic balance (ME, MV, and DC) and SOT may also increase functional ability in daily life, including transitioning between sitting and standing position, turning, and walking. These functional tasks are key components of TUG. In addition, the training effect also extended to patients’ concerns about falling as indicated by the improvement in FES-I. The questions identified in FES-I are not just limited to basic daily activities at home but also contain social activities outside the home. After training, patients may become more confident in balance-demanding tasks, such as walking on a slippery or uneven surface, walking up or down a slope, and walking in a place with crowds. The significant improvement in PDQ39 scores for both the TE and VRWii groups further supported the notion that exercise not only increases physical function but also increases emotional well-being, social support, cognition, and communication, and decreases bodily discomfort. The significant improvements observed in TUG, fall efficacy, and quality of life in patients with PD in the present study support the benefits of both traditional and VRWii training.
The small sample size of our study is one of the limitations. A larger randomized controlled clinical trial is needed to validate the reported benefits of the VR intervention. Despite the small sample size, the statistical power is relatively strong for our outcomes (crossing velocity, 0.96; crossing stride length, 0.94). In addition, the therapist was not blinded to the exercise group and, although unavoidable, this limitation may introduce bias. Also, the FES-I does not represent the real incidence of falls, and therefore the reduction of fall incidence after training warrants further follow-up, especially for PD patients with a history of falls. Furthermore, it should be noted that both interventions included treadmill training to enhance the effects of exercise training. However, this may dilute the distinction between the VR Wii and TE groups. In summary, VRWii as part of a multifaceted training intervention is effective in improving obstacle-crossing performance, dynamic balance, functional ability, and quality of life in PD patients. These improvements can persist for at least 1 month. These findings support the inclusion of VRWii training in the exercise program for participants with PD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by the National Science Council (NSC 100-2314-B-010-022-MY2) and Aim for the Top University Plan (101AC-P508) of the Ministry of Education of the Republic of China.