
Abstract
Background. People with Parkinson’s disease and freezing of gait (FOG+) have more falls, postural instability and cognitive impairment compared with FOG−. Objective. To conduct a secondary analysis of the V-TIME study, a randomized, controlled investigation showing a greater reduction of falls after virtual reality treadmill training (TT + VR) compared with usual treadmill walking (TT) in a mixed population of fallers. We addressed whether these treadmill interventions led to similar gains in FOG+ as in FOG−. Methods. A total of 77 FOG+ and 44 FOG− were assigned randomly to TT + VR or TT. Participants were assessed pre- and posttraining and at 6 months’ follow-up. Main outcome was postural stability assessed by the Mini Balance Evaluation System Test (Mini-BEST) test. Falls were documented using diaries. Other outcomes included the New Freezing of Gait Questionnaire (NFOG-Q) and the Trail Making Test (TMT-B). Results. Mini-BEST scores and the TMT-B improved in both groups after training (P = .001), irrespective of study arm and FOG subgroup. However, gains were not retained at 6 months. Both FOG+ and FOG− had a greater reduction of falls after TT + VR compared with TT (P = .008). NFOG-Q scores did not change after both training modes in the FOG+ group. Conclusions. Treadmill walking (with or without VR) improved postural instability in both FOG+ and FOG−, while controlling for disease severity differences. As found previously, TT + VR reduced falls more than TT alone, even among those with FOG. Interestingly, FOG itself was not helped by training, suggesting that although postural instability, falls and FOG are related, they may be controlled by different mechanisms.
Introduction
People with Parkinson’s disease (PD) and freezing of gait (FOG+) are often referred by neurologists to engage in rehabilitation programs because of the increased fall risk associated with FOG.1,2 Yet, work to date does not allow drawing firm conclusions regarding training benefits in this patient cohort. As for effects on freezing severity, a recent meta-analysis suggested that nonspecific exercise was not effective to alleviate freezing, as assessed with self-reported questionnaires. 3 An exercise program targeting a number of fall risk factors, that is, balance, leg strength, and FOG, also did not reduce fall risk or FOG, but improved balance, mobility scores, and fear of falling. 4 Results of more recent work, investigating the effects of resistance versus balance training in FOG+, demonstrated no effects on balance outcomes nor on FOG severity, irrespective of training arm. 5 In contrast, an uncontrolled study showed that community-based group exercise for FOG+ had positive effects on balance, gait, and FOG. 6 When gait was the specific target for exercise, it was shown that FOG+ generally responded equally well to rehabilitation compared with FOG−, when testing interventions such as dual task gait training and cued gait training.7,8 However, other studies suggested that unlike FOG−, FOG+ had compromised retention of motor learning, as applied to writing training and motor sequence learning.9,10 Repeated exposure to postural perturbations during one training session on a movable balance platform also showed overall less improvements in FOG+ than FOG−. 11
The manifest cognitive decline and disease progression, which partly underlie FOG, may not only explain a higher fall risk but also contribute to an inability to have sustained benefits from training. 12 This raises the question as to whether tackling both motor and cognitive functions rather than motor alone would be more beneficial for people with FOG versus those without.7,12,13
The V-TIME study, a large EU-funded international randomized controlled trial (RCT) on fall prevention, showed a greater beneficial effect of treadmill training augmented by virtual reality (TT + VR) on fall risk compared with standard treadmill walking (TT) in fall-prone older people including subjects with PD. 14 The V-TIME study was based on the very premise that combining motor-cognitive training would be better than just physical exercise to strengthen cognitive brain networks 15 or the interplay between motor and cognitive circuitry. 13 The VR-based intervention was also custom-made for older individuals and addressed a variety of cognitive challenges, such as executive and navigation tasks.
The above considerations motivated us to conduct a secondary analysis of the V-TIME study, investigating whether training motor-cognitive domains together (TT + VR) is more beneficial to providing treadmill training only (TT) in FOG+ as opposed to FOG−. The main outcomes of interest were balance and falls. We chose the Mini Balance Evaluation System Test (Mini-BEST) test as our primary outcome of this exploratory analysis. In previous work, we found that this multifaceted test of postural control discriminated between FOG+ and FOG−. 16 We hypothesized that TT + VR, due to targeting motor and cognitive correlates of FOG synergistically, would lead to better or equal results in FOG+ on the Mini-Best test and falls compared with FOG−. Given earlier findings on the lack of retention in FOG+, our second research question examined whether training gains were sustained over a period of 6 months in a similar way in both subgroups. Here, we expected that FOG+ would show reduced retention compared with FOG−. We also assumed that TT + VR would have a better effect on freezing severity compared with TT in the FOG+ subgroup alone. Indirectly, therefore, this study tested that if FOG, postural instability, and falls responded comparably to training (irrespective of training mode) that this would point to similar underlying neural substrates among these outcomes.
Methods
Study Design
This analysis was based on a subset of subjects who participated in the RCT titled “Virtual reality Treadmill combined Intervention to improve Mobility and reduce falls in the Elderly” (FP7 project V-TIME-278169). Five clinical partners were involved from Israel (Tel Aviv Sourasky Medical Center), Belgium (Katholieke Universiteit Leuven), the United Kingdom (Newcastle University), Italy (University of Genoa), and the Netherlands (Radboud University Medical Center Nijmegen). Eligible subjects were assigned randomly to an intervention group consisting of treadmill training plus VR (TT + VR) or a control group entailing treadmill training alone VR (TT). Originally, the dataset consisted of 130 PD patients. The current subanalysis involved 121 patients with PD, as FOG scores from 9 patients were unavailable. Patients were assessed 1 week before training, 1 week after the 6-week intervention, and 6 months after training.
Participants
A total of 77 patients with FOG (FOG+) and 44 without FOG (FOG−) were included in this analysis. The FOG+ group was defined based a score >1 on the New Freezing of Gait Questionnaire (NFOG-Q). 17 Recruitment took place between January 2012 and January 2015. All participants provided written informed consent in accordance to the Declaration of Helsinki. The study was approved by ethics committees in each of the 5 clinical sites separately and registered under trial NCT01732653.
Participants were included if they were between 60 and 90 years old, had been diagnosed based on the UK Brain Bank criteria, Hoehn and Yahr (H&Y) stage II or III, were on anti-Parkinsonian medication, were able to walk at least 5 minutes without assistance, had adequate hearing and vision (as evaluated by the whisper test and Snellen test, respectively), and had experienced 2 or more falls in the previous 6 months (self-reported). Exclusion criteria comprised psychiatric comorbidity, clinical diagnosis of dementia or other severe cognitive impairment (Mini-Mental State Examination [MMSE] score <24), history of stroke, traumatic brain injury or neurological disorders other than PD, rheumatic and orthopedic diseases, acute lower back or lower extremity pain, peripheral neuropathy, and an inability to comply with the training.
Training
A detailed description of the intervention and the RCT findings were published previously.14,18 In brief, participants exercised 3 times per week over a period of 6 weeks with each session lasting approximately 45 minutes in both training arms. Exercise programs were supervised by therapists (mean years of experience 5.2 ± 3.2 years, range 1-9 years), who were trained in the delivery methods prior to the first patient-in. Regular fidelity checks were performed across centers to ensure uniformity. 18 Both arms received walking exercises on a treadmill, whereby gait speed and walking duration were progressively increased throughout the 6-week intervention using predetermined levels and criteria for progression. 18 In the beginning of each training week, over-ground gait speed was measured over 10 m. Based on this, treadmill speed was set at 80% of over-ground gait velocity in the first week. This was increased to 90% in the second week and was aimed to go up with 10% from the third week. Walking duration was also increased from 20 to 45 minutes throughout the 6 weeks and a gradual reduction of handrail support was introduced until none was needed. As for the VR progression milestones, every week obstacle levels were increased in height and depth, visibility was reduced from daylight to darkness, distractors in the environment were increased from calm to busy and navigation signposts were reduced from many to none to stimulate memory functions. Progression was, however, subject to participant’s performance and ability. 18
The VR intervention was designed to tackle fall risk by training obstacle negotiation in a complex and interactive virtual environment. It included obstacles appearing at different sizes, frequencies and visibility, requiring step adjustments in both height and length. In addition, the VR environment posed a cognitive load using a navigation task and by adding visual and auditory distractors, stimulating attention, executive function, dual-tasking, planning, and response selection. Visual and auditory feedback on performance and results were provided during training and summarized at the end of each session in both arms of the study. Details on the amount of visual and auditory feedback as derived from the VR intervention are described in previous studies.14,18 Training progression was modulated by gradually increasing the walking speed, duration, and difficulty levels in the VR environment.
Outcomes
Testing was conducted by blinded testers for group allocation, using standardized guidelines across centers. Training occurred in a separate room from testing to ensure that blinding was maintained. The trainer also delivered the intervention on an individual basis and at separate moments to avoid contamination between groups.
All assessments were performed when patients were in the on-medication state. Following the first medication anamnesis, test times were determined to allow testing in a stable on-period, which was standardized for subsequent tests. Testers also telephoned participants a day prior to each test to verify time of medication intake. For this analysis, we focused on the Mini-BEST, as pathology in static and dynamic postural control likely underlies both FOG and fall risk. The validity and reliability for this scale in PD are well established.19,20 Other freezing-related outcomes were number of falls, assessed pretraining (by self-report of retrospective fall frequency) and at 6 months’ follow-up. During the 6 months after training, falls were recorded through a falls calendar, which was provided as a paper version, web-based calendar or a smartphone application according to individual preference. Each fall was directly indicated on the calendar. FOG severity was assessed with the NFOG-Q. 17
Secondary outcomes included executive function as assessed by the Trail Making Test part B (TMT-B). We chose this test for its psychometric properties 21 and its ability to discriminate between FOG+ and FOG−. 22 Other secondary outcomes included 2 tests of overall mobility (Short Physical Performance Battery[ SPPB], Four Square Step Test [FSST]), balance confidence (Falls Efficacy Scale–International [FES-I]), and daily activity (Physical Activity Scale for the Elderly [PASE]). Descriptor variables included age, gender, years of education, global cognitive function using the MMSE and Montreal Cognitive Assessment (MoCA), and disease severity, assessed by Hoehn & Yahr (H&Y) staging, Unified Disease Parkinson’s Disease Rating Scale motor part (III) (MDS-UPDRS-III) and disease duration.
Statistical Analyses
Statistical analysis was performed using IBM SPSS software (version 22). Demographic characteristics were compared between groups using independent t tests and chi-square statistics. Generalized linear mixed-effects models were used with Group (FOG+/FOG−), Training arm (TT/TT + VR), and Time (pre, post, 6 months’ follow-up) as fixed effects. We also used UPDRS-III as a continuous covariate to adjust for differences in disease severity, while avoiding colinearity. As this analysis was a secondary analysis, no a priori power analysis was carried out. All models controlled for within-subject differences by including participants as random effects. Falls were examined using a negative binomial regression, with no exposure variable included. For all analyses, alpha was set at .05 and post hoc analyses were carried out using Bonferroni tests.
Results
Group demographics are presented in Table 1. Age, cognition, gender, and fall rates were similar in FOG+ and FOG− at baseline. The FOG+ group had worse disease profiles, as might be expected, shown by higher disease duration (P = .008), H&Y (P < .001), and UPDRS-III scores (P = .02). Furthermore, FOG+ had lower balance scores on the Mini-BEST (P = .044) and more fear of falling (P = .006).
Demographic Characteristics of PD Groups and Training Arms.
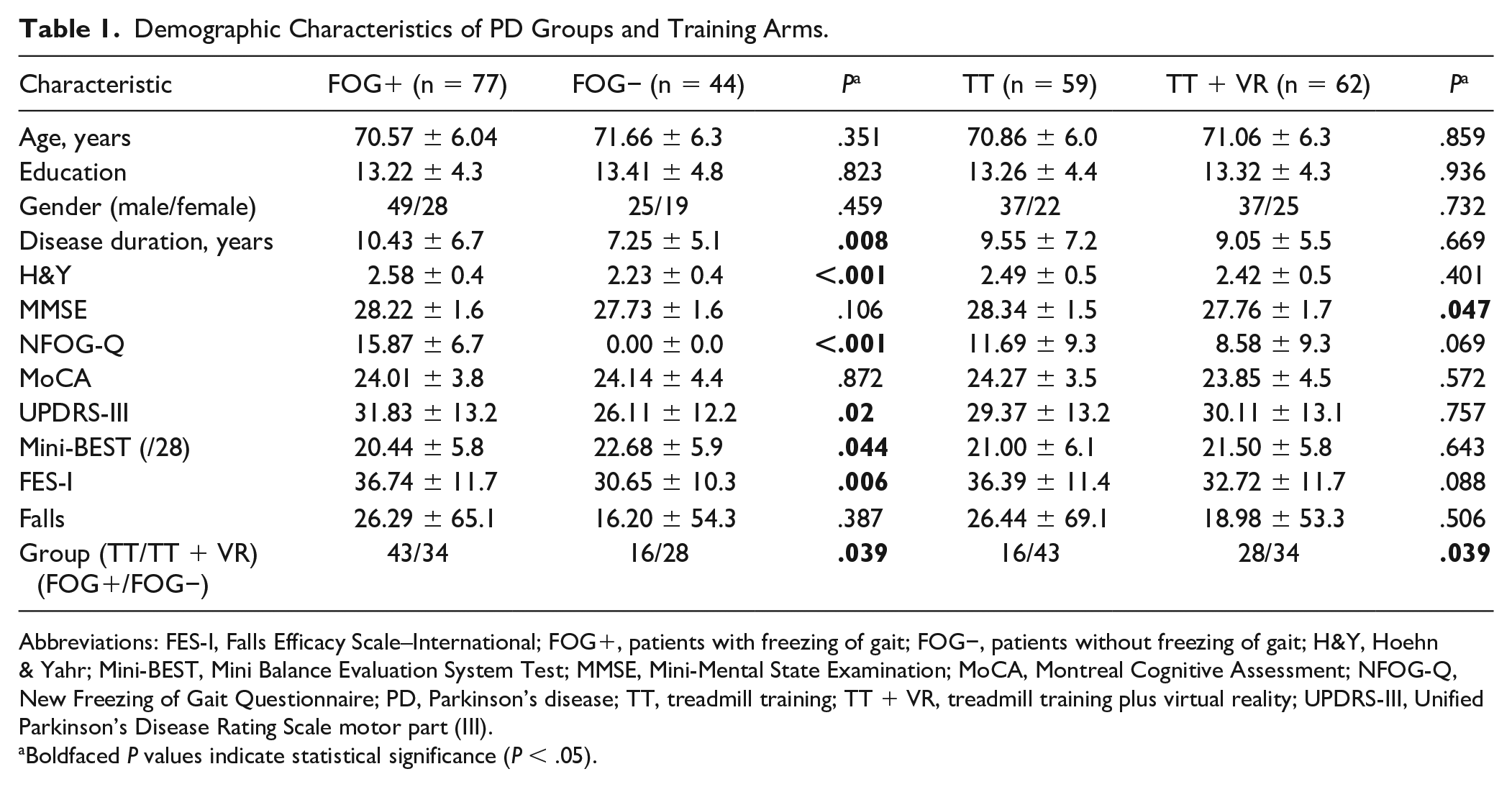
Abbreviations: FES-I, Falls Efficacy Scale–International; FOG+, patients with freezing of gait; FOG−, patients without freezing of gait; H&Y, Hoehn & Yahr; Mini-BEST, Mini Balance Evaluation System Test; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; NFOG-Q, New Freezing of Gait Questionnaire; PD, Parkinson’s disease; TT, treadmill training; TT + VR, treadmill training plus virtual reality; UPDRS-III, Unified Parkinson’s Disease Rating Scale motor part (III).
Boldfaced P values indicate statistical significance (P < .05).
The distribution of the 2 FOG groups differed between both training groups. Of the FOG+ group, 43 were in TT versus 34 in TT + VR. Of the FOG− group, 16 were included in TT and 28 in TT + VR. No differences were present between TT and TT+VR training arms at baseline. Within each FOG-subgroup, participants in the two training arms were well matched with regard to all baseline characteristics (Table 1/Supplementary Material). Only within FOG−, disease duration was slightly longer in the VR compared with those in the TT arm (P = .044).
Effect on Balance, Falls, and Freezing of Gait
An overview of these results is provided in Table 2 and presented in Figures 1 and 2. Overall, no 3-way interactions between, time, training modes, and FOG subgroups were found and most results indicated significant time effects only after controlling for disease severity. The primary outcome, balance performance as evaluate by the Mini-BEST scores, improved in both groups immediately after training (P = .001), irrespective of training arm and subgroup. However, improvements were not retained at 6 months and declined in a similar fashion across subgroups and training arms.
Primary and Secondary Outcome Measures Pre- and Postintervention and at 6 Months’ Follow-up. a
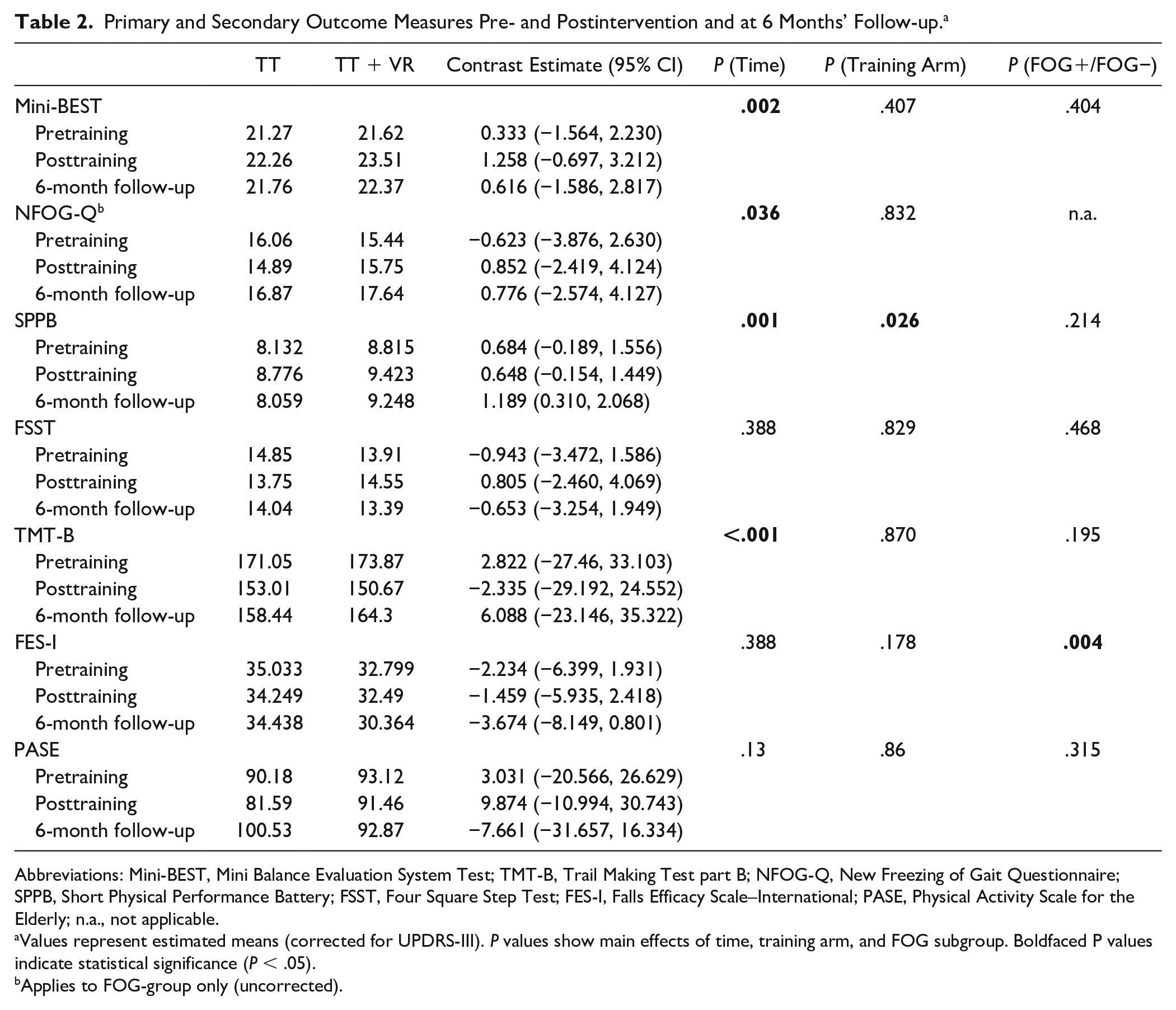
Abbreviations: Mini-BEST, Mini Balance Evaluation System Test; TMT-B, Trail Making Test part B; NFOG-Q, New Freezing of Gait Questionnaire; SPPB, Short Physical Performance Battery; FSST, Four Square Step Test; FES-I, Falls Efficacy Scale–International; PASE, Physical Activity Scale for the Elderly; n.a., not applicable.
Values represent estimated means (corrected for UPDRS-III). P values show main effects of time, training arm, and FOG subgroup. Boldfaced P values indicate statistical significance (P < .05).
Applies to FOG-group only (uncorrected).
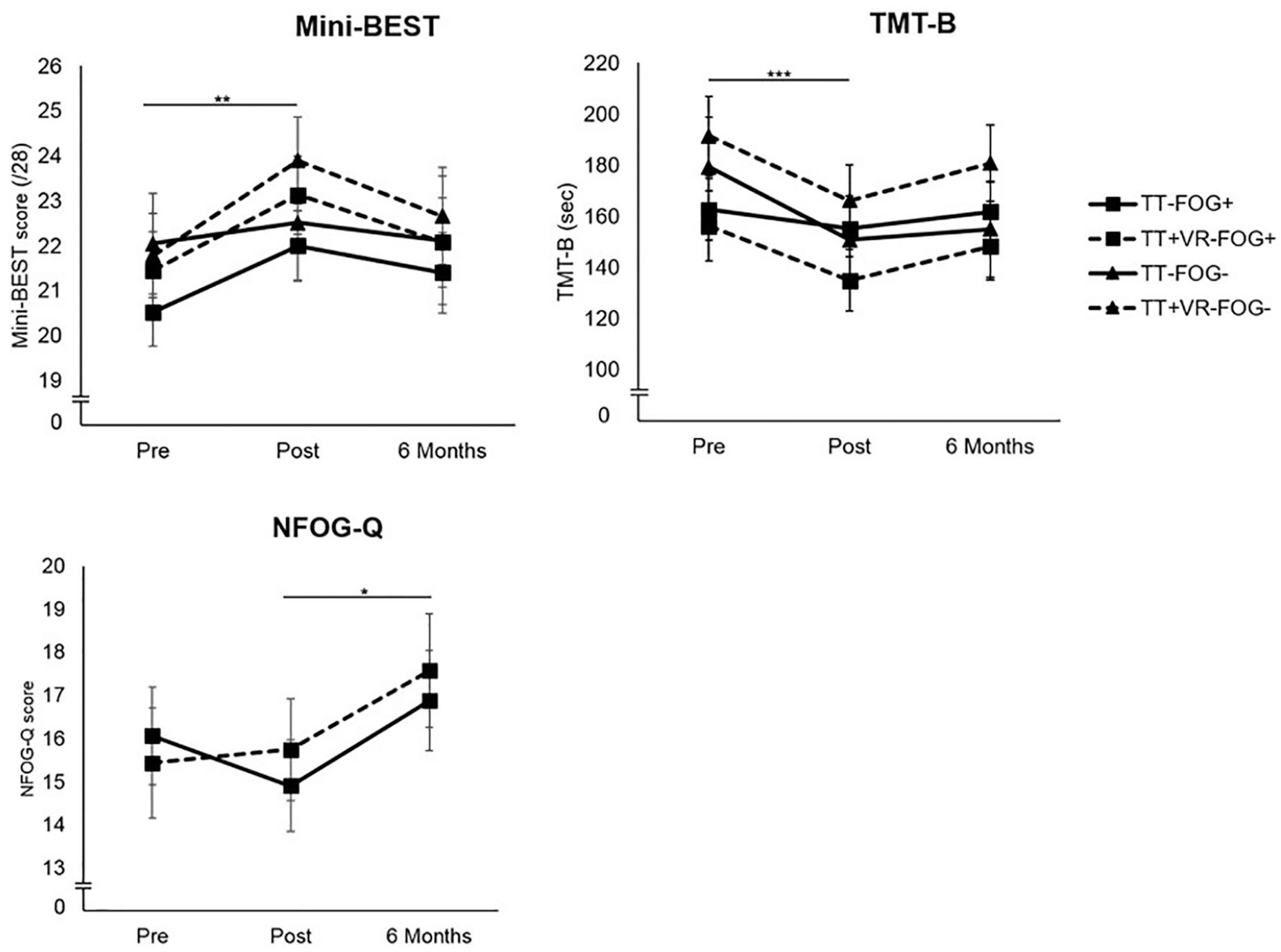
Results on balance, executive function, falls and freezing of gait in the treadmill training with virtual reality (TT + VR) and treadmill training (TT) arms pre- and posttraining and at 6 months’ follow-up. No differences between freezing of gait (FOG) subgroups were apparent and therefore not individually displayed. Estimated means and standard errors are shown. *P < .05, **P < .01, ***P < .001.
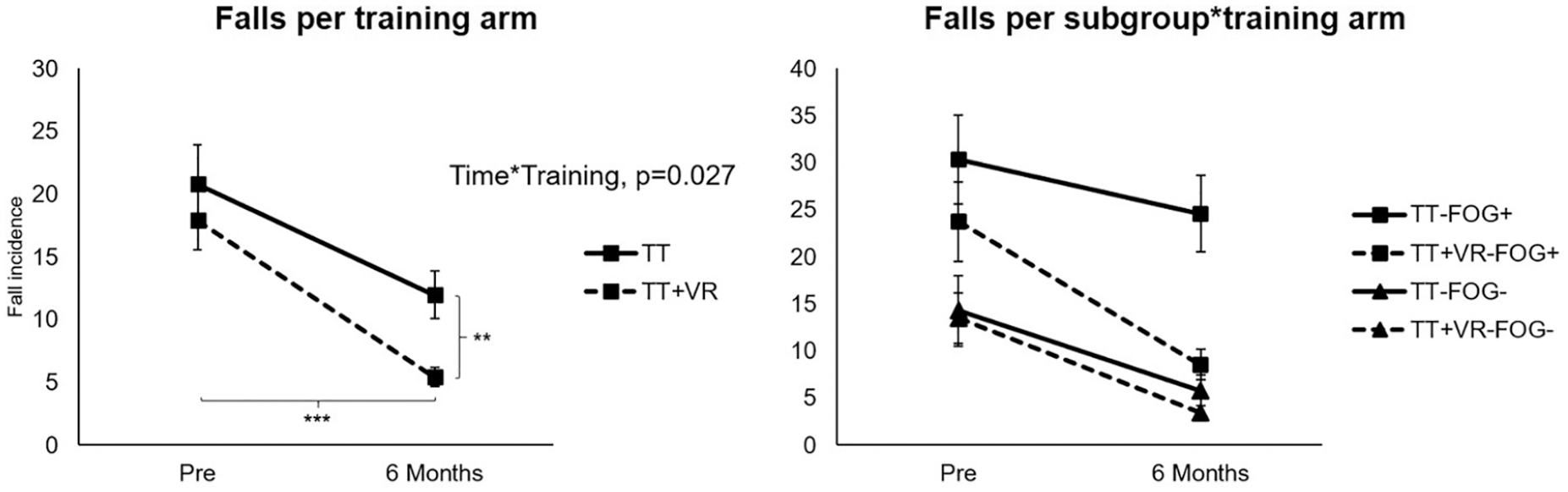
Training effects on falls in both Parkinson’s disease (PD) groups with and without freezing of gait (FOG) and training arms with and without virtual reality (VR) pre- and posttraining and at 6 months’ follow-up. An Intervention × Time interaction (P = .027) showed a significantly greater reduction of falls in the TT + VR group in both FOG+ and FOG−. Fall incidence rate was lower in the VR group than in TT alone (incidence rate ratio [IRR] 0.35, 95% CI 0.21-0.57). Fall rates were generally higher in FOG+ compared with FOG− (P < .001). *P < .05, **P < .01, ***P < .001.
A Training Arm × Time interaction (P = .027) did show a significantly greater reduction of falls in the TT + VR group in both FOG+ and FOG− as compared with the TT group (P = .008). Fall rates were significantly lower after 6 months than at baseline in the VR group (5.39 [95% CI 4.09-7.21]; P < .001), while this was not significantly different in the TT group (11.95 [95% CI 8.76-16.31]; P = .099). Another main effect for fall rate was found for the FOG subgroup (P < .001), indicating that FOG+ had overall higher fall rates even after correcting for disease severity (slightly different from the baseline unadjusted fall rates in Table 1). When we analyzed the effects of training on FOG severity in FOG+ only, the NFOG-Q scores did not improve after both training modes. Additionally, FOG severity increased at 6 months compared with posttraining assessment (P = .037) and got worse beyond baseline levels.
Effects on Other Outcomes
The results of training on the secondary outcomes are presented in Table 2. As above, no 3-way interactions between, time, training modes, and FOG subgroups were apparent. A significant effect of time was found for executive function (TMT-B scores) (P < .001), indicating that both groups benefited equally from both training modes. Overall mobility performance (SPPB scores) significantly improved immediately after training in both arms (P = .001), but improvements were not retained at 6 months (P = .030). Furthermore, SPPB scores were generally higher in the TT + VR group compared with the TT group (P = .026), but no interactions were found with time or subgroup. Fear of falling, as assessed with the FES-I, was overall higher in FOG+ (P = .004), but this was influenced neither by training (P = .388) nor by training mode (P = .178). No intervention-related changes were found on other mobility measures, such as the FSST and PASE.
Discussion
This study investigated the effectiveness of treadmill training with (TT + VR) and without virtual reality (TT) on balance and falls differentiating between PD patients with and without FOG. We hypothesized that TT + VR would be more, or at least as, beneficial for FOG+ compared with FOG−. In contrast, we found that FOG+ gained as much as FOG− from TT and TT + VR, as their postural instability, executive function, and general mobility improved to an equal degree. We also found that despite more severe clinical profiles, higher fall rates, and more fear of falling than FOG−, FOG+ reported a greater reduction of fall rates after TT + VR compared with TT. The second hypothesis, that FOG+ would show less retention of training effects compared with FOG−, was also rejected as both groups consistently showed loss of training benefits after 6 months. As for the effects on FOG itself, which could only be determined in the FOG+ group, neither TT + VR nor TT influenced this symptom. Disappointingly, freezing severity even increased considerably in both training arms at the 6-month follow-up.
In line with what was presented for a wider group of fall-prone older adults, 14 both FOG− and FOG+ improved postural instability and cognitive function after both training modes, but did not retain these effects after cessation of the intervention. In FOG+, executive dysfunction is usually more pronounced compared with FOG−. 12 Yet, here we could establish that complex training addressing motor-cognitive integration was as beneficial for this subgroup, at least in the short term. This may partly be explained by the fact that at baseline FOG+ and FOG− had similar cognitive scores on generic tests (MoCA and MMSE). The results also show, overall, that long-term retention of treadmill intervention was equally impaired in both PD subgroups. Other studies indicated shorter retention of motor learning in FOG+ compared with FOG− after complex dual-task interventions and writing training. 9 Providing motor-cognitive rehabilitation on a regular basis and for a longer period might improve long-term retention. However, the optimal frequency and intensity to sustain training gains is not yet clear in PD and would need more frequent test moments. Recent study showed that, irrespective of the presence of FOG, the effects of intensive balance training for 10 weeks were predicted to disappear completely after 14 months without training. 23
The rate of falls was significantly lower at 6 months’ follow-up, with a larger effect of TT + VR over TT alone. Training with VR may have led to increased attention while negotiating obstacles in the real world, as a result of which tripping risks may have been reduced, the most common cause of near-falls among fallers with PD. 24 The VR environment also stimulated cognitive and visual processing, such as focused attention, response selection, and planning while walking. 18 As walking is a complex task, requiring integration of motor, cognitive, perceptual resources for dynamic postural control and bilateral coordination, 25 combined motor-cognitive training may have enhanced these processes in both FOG+ and FOG−. Recent frameworks for rehabilitation, specifically targeted at FOG, promote integration of cognitive and motor components.6,26-28 The present results strengthen the use of such approaches in clinical practice, at least for ameliorating falling, even when targeting extremely fall-prone individuals such as those with FOG.
Although falls, postural control, and FOG co-occur and are likely etiologically intertwined, 29 the self-reported measure of FOG, the NFOG-Q, did not improve after training, unlike postural instability (the Mini-BEST test) and falls. Most strikingly, FOG deteriorated significantly with time beyond baseline levels, which was not the case for falls and postural instability as tested in both FOG+ and FOG−. Although speculative, these discrepant results support the notion that these phenomena are governed by not only partially overlapping but also distinct neural pathways.30,31 We recently published a review of the literature to determine whether there is evidence to claim that FOG and postural instability have common mechanisms. 29 We found that the findings on medication suggested that non-dopaminergic mechanisms were even more involved in postural instability than in FOG. Common neural pathways for modulation of FOG and postural instability likely incorporate the mesencephalic locomotor region (MLR) and the cerebellum.32,33 Still, motor imagery data revealed that the latero-rostral part of the MLR might regulate balance, whereas the medial-caudal MLR appeared more involved in gait. 34 The effectors of balance and gait, primarily concerning the trunk and leg muscles, have different somatotopic representations in various brain regions, which would also account for the limited overlap between the 2 phenomena. All this, and the fact that training had such contradictory effects would suggest that the occurrence of FOG episodes are etiologically different than falls, although postural instability and cognitive capacity may mediate both these phenomena.
Our results are different than those of a series of studies that tested the effects of interventions specifically designed to alleviate FOG. A recent pilot study on the efficacy of a 6-week supervised training to reduce FOG demonstrated consistent improvements of FOG, gait, and balance. 6 Similarly, 12 sessions of curved treadmill walking led to gains in both FOG and functional walking maintained for at least 1 month. 35 Also, 8 sessions of 20-minute dual motor-cognitive virtual reality training by stepping-in-place led to a reduction in the number of FOG episodes. 36 Various modes of action observation, by watching FOG-alleviating videos as well as undergoing physical training, led to significant improvements in FOG severity with good retention at follow-up.37-39 Together, these results could signify that motor-cognitive therapy needs to be specifically designed to alleviate FOG. In contrast, the TT + VR training of the present study, although relevant for FOG, was designed to target falls and mobility, but was not specifically aimed at tackling FOG. The evidence above highlights the importance of tailored and intensive programs, addressing both FOG triggers and modifiers, in order to alleviate FOG.
Limitations
Falls were reduced when assessed over a total period of 6 months. However, measures of postural instability were captured immediately after training as well as at follow-up. Future work should incorporate more frequent and parallel measures of fall rates, balance, and FOG scores to understand how the changes over time in these outcomes are interrelated. In addition, it is possible that changes in FOG occurred that were not captured by the NFOG-Q, as responsiveness of this scale is still unknown. Although the groups were relatively large, this secondary analysis was not powered for this subanalysis and did not account for center effects, as none were found in the previous analysis of the V-TIME study. 14 Therefore, our findings could have suffered from type II error. In addition, the unequal group sizes between FOG+ and FOG−, especially within training arms, must also be acknowledged.
Conclusions
Despite the higher risk of falls, people with FOG benefited equally from treadmill training with and without VR with regard to improving their balance and reducing fall risk compared with their nonfreezing counterparts. Overall, the present exploratory findings identified a similar training potential in FOG+ and FOG−, as well as a similar decline of practice effects after a period without training. Interestingly, freezing itself was not alleviated by combined motor and cognitive training and deteriorated importantly over the 6 months follow-up period. While the current positive results of treadmill training in people with FOG are encouraging, they also point to the need to specifically target rehabilitation to the origins of FOG in order to be able to modify this complex problem.
Supplemental Material
Supplementary_materials – Supplemental material for Do Patients With Parkinson’s Disease With Freezing of Gait Respond Differently Than Those Without to Treadmill Training Augmented by Virtual Reality?
Supplemental material, Supplementary_materials for Do Patients With Parkinson’s Disease With Freezing of Gait Respond Differently Than Those Without to Treadmill Training Augmented by Virtual Reality? by Esther M. J. Bekkers, Anat Mirelman, Lisa Alcock, Lynn Rochester, Freek Nieuwhof, Bastiaan R. Bloem, Elisa Pelosin, Laura Avanzino, Andrea Cereatti, Ugo Della Croce, Jeffrey M. Hausdorff and Alice Nieuwboer in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We cordially thank all the V-TIME participants for engaging in the study.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JMH has received grant support from the National Institutes of Health (NIH), the Michael J. Fox Foundation for Parkinson’s Research, the EU (H2020), the United States Israel Binational Science Foundation, the Israeli Science Foundation, and the National Multiple Sclerosis Society. JM and AM submitted a patent application on the use of virtual reality, the intellectual property rights for which are held by the Tel Aviv Medical Center. JMH has or currently serves on the Movement Disorders Society Technology Task Force and on Michael J. Fox Foundation task force on gait, on the board of the International Society for the Measurement of Physical Behavior, and on advisory boards for Sanofi and Biogen. AM has received grant support from the Michael J. Fox Foundation for Parkinson’s Research, the Israeli Science Foundation and Ministry of Science and Technology. She serves on the Gait Advisory committee for Michael J. Fox Foundation for Parkinson’s Research and, on advisory boards for Biogen. BRB currently serves as Associate Editor for the Journal of Parkinson’s Disease, serves on the editorial of Practical Neurology and Digital Biomarkers, has received honoraria from serving on the scientific advisory board for Abbvie, Biogen, UCB, and Walk with Path, has received fees for speaking at conferences from AbbVie, Zambon, Roche, GE Healthcare, and Bial, and has received research support from the Netherlands Organization for Scientific Research, the Michael J. Fox Foundation, UCB, Abbvie, the Stichting Parkinson Fonds, the Hersenstichting Nederland, the Parkinson’s Foundation, Verily Life Sciences, Horizon 2020, the Topsector Life Sciences and Health, and the Parkinson Vereniging.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the European Commission (FP7 project V-TIME-278169).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.