
Abstract
Background. High-intensity training aims to improve hand function in children with unilateral spastic cerebral palsy (USCP). However, the extent to which skill training is required is not known. Objectives. To compare the effects of intensive bimanual training with and without structured progression of skill difficulty, on manual dexterity, bimanual hand use, daily functioning, and functional goals in children with USCP. Method. Twenty-two children were randomized to structured practice group (SPG) or unstructured practice group (UPG), and received 6 h/d training during 15 days. Children from the SPG were engaged in fine and gross motor bimanual activities, with skill progression and goal training. Children from UPG performed the same activities without skill progression or goal training. Participants were evaluated before, immediately and 6 months after training by a physical therapist blinded to group allocation. The primary outcomes were the Jebsen-Taylor Test of Hand Function (JTTHF) and Assisting Hand Assessment (AHA). Secondary outcomes included the Canadian Occupational Performance Measure (COPM), Pediatric Evaluation of Disability Inventory (PEDI), and ABILHAND-Kids. Results. Both groups showed similar improvements in the JTTHF, AHA, ABILHAND-Kids, COPM-satisfaction, and PEDI (P < .05). A significant interaction in the COPM-performance scale (P = .03) showed superior improvements of the SPG immediately, but not 6 months, after the intervention. Conclusions: Children from both groups demonstrated improvements in dexterity and functional hand use. This suggests that for intensive bimanual approaches, intensive training at such high doses may not require structured practice to elicit improvements. However, there may be immediate added benefit of including goal training.
Keywords
Unilateral spastic cerebral palsy (USCP) is characterized by motor impairments mainly lateralized to one side of the body, with the resulting impaired hand function affecting functional activity and participation. Increasing evidence supports the use of 2 treatment approaches based on motor learning principles, constraint-induced movement therapy (CIMT) and intensive bimanual training. CIMT involves physical restraint of the less-affected upper extremity (UE) along with intensive, skilled practice of the more-affected hand.1-10 Bimanual training involves practice of functional and play activities requiring the use of both hands.10-20 Hand-arm bimanual intensive training (HABIT) is a highly structured form of bimanual training.11,13,19,21 Both CIMT and HABIT were designed with the idea that intensity of training22,23 and progression of skill difficulty 24 are essential to improve motor function. They include part and whole practice, and modifying tasks to elicit desired movements and to ensure successful use of the more-affected hand.21,24,25 Recently, several randomized trials have shown both approaches result in improvements in unimanual and bimanual measures.12-18,20,26,27
There is evidence to suggest that the behavioral demands of the tasks and motor skill training may elicit cortical reorganization 28 underlying concurrent functional outcomes. For optimal efficacy, it is believed that training must be challenging, involve progressive increase of behavioral demands and active participation. Studies of skilled training in animals show plasticity of UE cortical representation, whereas those animals receiving unskilled training (repetition only) did not.28,29 Friel et al 30 investigated mechanisms for restoring motor function after unilateral corticospinal system damage in cats during early postnatal development. They compared skilled practice of the affected limb in a reaching task along with restraint of the unaffected forelimb limb in one group of cats (analogous to CIMT) with restraint only (analogous to forced use 31 ) in another group. The skilled training group had improvements in motor skills of the affected limb along with expansion of the motor map, whereas the restraint-only group did not demonstrate plastic changes. Thus, skilled training is an important element in animal models of rehabilitation.
In humans, the extent to which skill training is required during intensive training is not well-understood. Uswatte et al 32 found similar outcomes of shaping and task-practice without skill progression during CIMT in adult stroke patients’ hand function. The extent to which skilled practice is required for pediatric UE rehabilitation approaches is not known. One precision grip study in children with USCP demonstrated that task repetitions alone could lead to better motor performance of this task. 22 It is conceivable that intensity alone may be the key element to improvements in hand function; that is, at such high doses, specific components may not be important.
In the present study, we compare the effects of intensive bimanual training with and without structured progression of skill difficulty, on manual dexterity (Jebsen-Taylor Test of Hand Function, JTTHF) bimanual hand use (Assisting Hand Assessment, AHA), daily functioning (ABILHAND-Kids, Pediatric Evaluation of Disability Inventory, PEDI) and functional goals (Canadian Occupational Performance Measure, COPM) in children with USCP. We hypothesized that children in the structured practice group (SPG) would have greater improvements compared to children in the unstructured practice group (UPG) on all measures.
Method
Participants
Participants were recruited from area clinics, our Web site (http://www.tc.edu/centers/cit/), and online support groups. Potential participants were first screened via e-mail/telephone. Those between the ages of 6 and 13 years with congenital hemiplegia were invited to receive an on-site physical examination or an examination videotaped by their physical/occupational therapist. The inclusion criteria were established based on prior HABIT trials11-13: (1) the ability to lift the more-affected arm 15 cm above a table and grasp light objects, (2) mainstreamed in school, and (3) demonstrated ability to follow instructions during screening/testing. Exclusion criteria included (1) health problems unassociated with cerebral palsy, (2) current/untreated seizures, (3) visual problems interfering with treatment/testing, (4) severe muscle tone at any joint (Modified Ashworth score >3.5), (5) orthopedic surgery on the more-affected hand within 1 year, and (6) botulinum toxin in the more-affected UE within the past 6 months or intended treatment within the study period. Informed consent was obtained from participants and caregivers. The study was approved by the Teachers College Institutional Review Board.
Procedures
General Procedures
Three bimanual training day-camps were conducted at the university from July 2010 to July 2012. Participants (6-8 each camp) were randomized offsite using concealed allocation stratified by age and JTTHF screening score, into an SPG and UPG. Each camp had 3 to 4 children per group, each group separated in different rooms.
Participants in each group were engaged in treatment 6 h/d for 15 consecutive weekdays (90 hours) during school recess by trained interventionists. These included graduate students in kinesiology/neuroscience, speech pathology, and psychology, and undergraduates. The interventionists were not aware of the study hypotheses or that different procedures would be carried out in each room. The pretreatment training, administered by the supervisors, was standardized during a 2-hour session based on established manual of procedures, before interventionists were assigned to a group and child. Group training focused on procedures common to the 2 groups, strategies to engage children in use of hands, safety and data logging procedures. Additional training was provided specific to each group during the interventions and daily team meetings. Interventionists and children in each room were kept partitioned at all times, and interventionists were instructed not to discuss the camp with each other outside of treatment hours. The 2 treatment rooms had supervisors, who were not blinded to the study hypotheses, and were responsible for ensuring treatment fidelity. The SPG was supervised by a physical therapist who modeled and ensured uniformity of treatment. The UPG was supervised by a nonclinician who ensured that interventionists did not provide structured practice or graduation of task complexity. Emphasis in this group was to engage children to use the more-affected hand in play activities. Both groups were monitored by an occupational therapist and a nonclinician who followed all the activities, to avoid possible confounds in the specificities of each training modality (ie, skill progression).
Room design permitted participants to work individually with their interventionist or in groups (1:1 interventionist:participant ratio). Interventionists were paired with children prior to randomization based on age, gender, and caregiver input. Interventionists avoided verbal prodding to use the more-affected hand, and instead provided tasks necessitating the use of both hands and established rules prior to each activity, allowing the child to choose which hand to use for different components of a bimanual activity. Caregivers were instructed to engage participants in bimanual activities for 1 h/d during and for 6 months following the intervention and document practice using home activity logs. No information regarding training of functional goals at home or skill progression was provided for either group.
Structured Practice Procedures
Children from the SPG were engaged in age-appropriate fine and gross motor bimanual activities using motor learning approaches consistent with HABIT. 23 Activities were selected by considering the role of the more-affected hand increasing in complexity from a nondominant passive assist (eg, stabilizing paper while drawing) to active manipulator (eg, reorienting paper while cutting) using increasingly complex bimanual coordination and participants’ interests. Task demands were graded and participants were engaged in active problem solving.
Children participated in whole and part task practice. Whole task practice involved sequencing successive movements within the context of tasks (eg, card games). The activities were performed continuously for at least 15 to 20 minutes. The spatial and temporal coordination of targeted movements were practiced within the context of completing the task. Part task practice21,25 required breaking down motor skills into smaller components (eg, playing-card turning to promote forearm supination), while increasing repetitions and skill requirements. This served to provide specificity/intensity of treatment by requiring as many targeted repetitions as possible over repeated 30-second intervals. Part practice included both bilateral symmetrical (eg, reaching toward object(s) with both hands) and asymmetrical (eg, pulling apart objects) movements. Task difficulty was graded by varying the spatial and temporal constraints, or by providing tasks that require progressive skilled use of the more-affected hand as performance improved. Task- and age-specific knowledge of results were provided for encouragement. 23 Supervisors instructed interventionists regarding the main focus of the treatment (eg, reaching) for each child based on his or her pronounced movement deficits, interests, and potential for improvement. Activity logs were collected, which included activities performed, time on task including part/whole practice, the number of repetitions, task performance and skill progressions.
Practice of functional goals established by caregivers was based on children’s interests and abilities. Goal training was performed up to 30 min/d during camp. With the exception of goals, tested task items were never trained.
Unstructured Practice Procedures
Children from the UPG were engaged in age-appropriate fine and gross motor bimanual play activities (with the exception of functional goal practice) with the same activities without any adaptations or progression. As in the SPG, rules were established requiring use of their more-affected hand. Activities were selected from the same battery of choices as that of the SPG, according to child’s interest and willingness to use the more-affected hand. Interventionists were trained only to provide activities that require the use of both hands in a playful and enjoyable context. Thus, the aim of the unstructured training was to provide children opportunities to use their more-affected hand in bimanual play activities, without considering how this hand was used or how use could be improved or challenged. Interventionists were specifically told “these children receive excessive therapy during the year, and that our purpose was to provide a fun, supportive environment to avoid frustration or perception that activities were therapeutic.” Thus, the focus of training was only to keep the more-affected hand involved in the performance of the activities. Supervisors ensured that no increase in task complexity, verbal prompts how to use the more-affected hand or gradation of tasks demands were provided. Such supervision happened throughout the intervention and in daily meetings with interventionists. Activity logs were collected, which included activities performed and the time spent in these activities.
Measures
Participants were evaluated directly prior to treatment (pretest), within 2 days (“immediate”) and 6 months after treatment by a physical therapist blinded to group allocation (verified following testing). Two primary outcome measures were used to quantify bimanual and unimanual outcomes under the International Classification of Functioning and Health (ICF) “activity and participation” domain. 33
The AHA version 4.3 34 quantifies the effectiveness with which a child with unilateral disability uses his or her affected (assisting) hand in bimanual activity. The AHA has excellent validity/reliability. 35 The test was videotaped and scored offsite by an experienced evaluator blind to group assignment. Data were reported in logit-based units (AHA-units).
The JTTHF is a standardized test of simulated functional tasks quantifying the time to complete a battery of unimanual activities. 36 The activities include flipping index cards, object placement, simulated eating, stacking checkers, and manipulating empty and full cans. Reliability for children with nonprogressive hand disabilities is high. 37
Four secondary measures were also used (ICF “activity and participation domain”).
To establish/evaluate children’s functional goals we conducted the COPM with caregivers. The COPM identifies and measures changes in functional problems considered relevant by clients through interview, and is valid/reliable.38-40 The most relevant functional goals to be accomplished are defined, ranked in importance, and rated on performance and satisfaction.38-40 In this study, caregivers selected the goals and rated the child’s performance and level of satisfaction since these are abstract concepts for children of this age.
The ABILHAND-Kids is a valid/reliable questionnaire assessing manual ability of children. 41 The test comprises a list of manual activities in which the caregivers score the amount of difficulty children with cerebral palsy may experience during their performance in activities of daily living that required hand use. Data were reported in logit-based units.
To assess children’s daily functioning, caregivers were interviewed using the PEDI, a valid/reliable test 42 focusing on child’s functioning in daily living activities at home. 43 Children’s self-care functional skills and caregiver assistance were assessed.
A subset of 13 children (7 in SPG, 6 in UPG) wore an activity monitor (Manufacturing Technology Inc, Fort Walton Beach, FL, #7164; 5.1 cm × 2.6 cm × 1.5 cm, 42.9 g) on each wrist during a continuous 3-hour period in camp on the seventh or eighth intervention day to determine how much the children in each group moved. The units sample (10 Hz) and store summed values in memory, and data are downloaded to a personal computer. The number of accelerations is measured as activity counts (0.01664 g for an acceleration of 2.13 g directed parallel to the x-axis with a frequency of 0.75 Hz), which were used to determine the percentage of time each hand was used. 34
Statistical Design
Sample size calculations were performed based on JTTHF scores derived from an earlier HABIT trial. 13 A mean decrease from 380.84 to 249.58 seconds (131.25 ± 121.86 seconds) for the HABIT group was reported. With significance level = .05, 1 − β = 0.80, µ1 − µ2 = 131.25, and σ = 121.86, and estimated 10% dropout, 11 participants in each group were required. Intention-to-treat principles were employed.
A 2 (group) × 3 (test sessions) analysis of variance with repeated measures on test sessions was performed using SPSS 15 for all measures except the COPM. Since goal performance may be influenced by development and practice in ongoing care (follow-up), a 2 (group) × 2 (pre/post) analysis of performance was performed on the COPM. The overall group-by-test session interaction tested whether the pattern of change between sessions varied across groups. Newman-Keuls post hoc tests were used to compare pretest and each of the posttests.
Results
Patient Flow
Patient flow is shown in the CONSORT diagram (Figure 1). During recruitment (June 2010-2012), 86 individuals were screened. Ultimately, 22 qualified individuals agreed to participate and were randomized into the SPG and UPG (see Figure 1 legend for details). One child from the UPG proved to have developmental dyspraxia and was not provided the intended treatment (ie, requiring sequential instructions, analogous to part practice) and the AHA was not usable. The child and the matched pair from the SPG were excluded. Thus, 20 participants (10 per group) completed the study. Table 1 describes participant characteristics. There were no significant group differences in baseline scores for any measure.
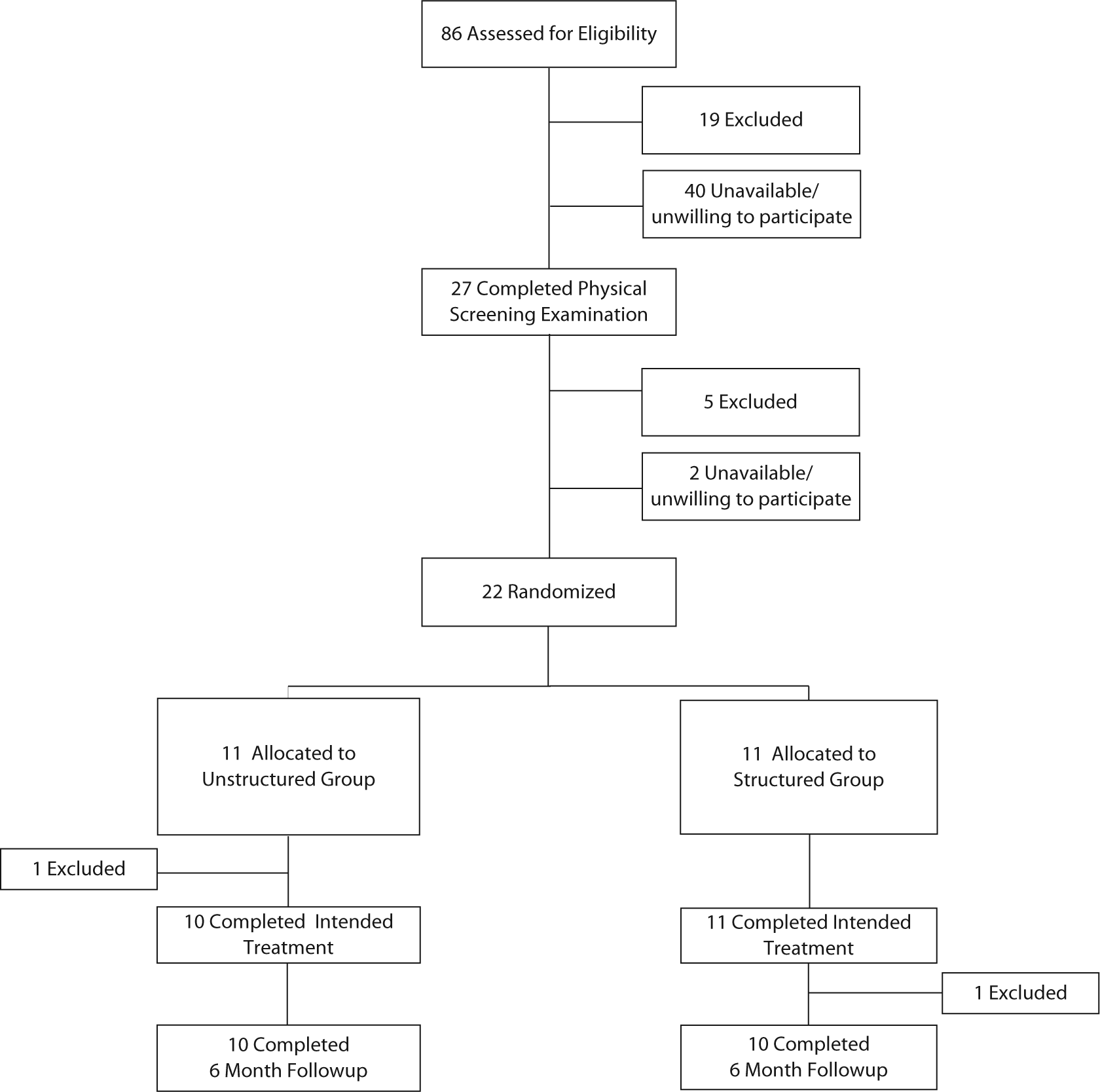
CONSORT flow diagram showing progress through the stages of the study, including flow of participants, withdrawals, and inclusion in analyses. A total of 86 individuals potentially met the study criteria and were invited to undergo physical screening. Twenty-two children qualified for the study and were randomized into the structured practice group (SPG) or unstructured practice group (UPG). One child from the UPG proved to have apraxia and was not provided the intended treatment. The child and the matched pair from the SPG were excluded.
Baseline Participant Characteristics.
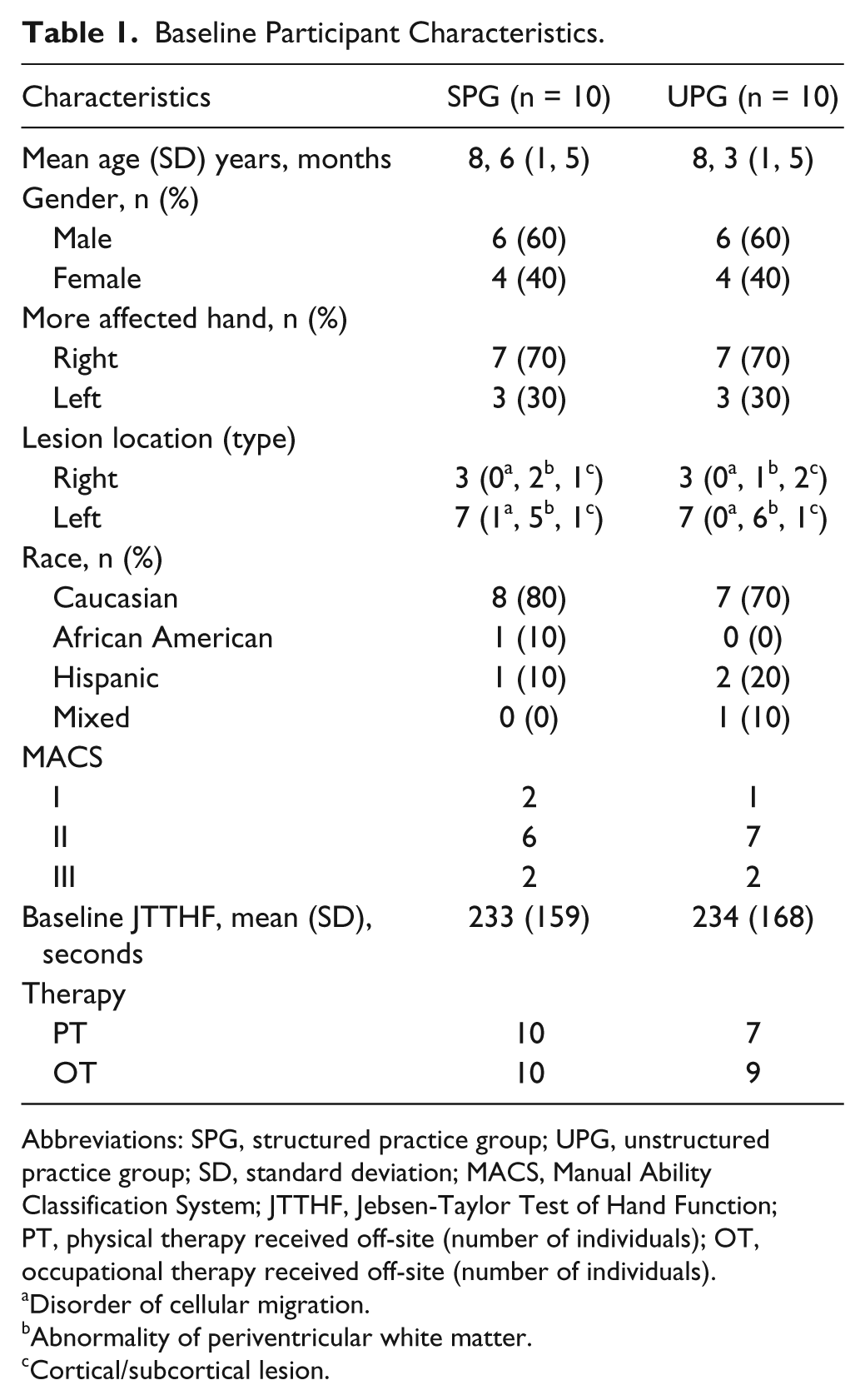
Abbreviations: SPG, structured practice group; UPG, unstructured practice group; SD, standard deviation; MACS, Manual Ability Classification System; JTTHF, Jebsen-Taylor Test of Hand Function; PT, physical therapy received off-site (number of individuals); OT, occupational therapy received off-site (number of individuals).
Disorder of cellular migration.
Abnormality of periventricular white matter.
Cortical/subcortical lesion.
Treatment Characteristics
Activity logs showed both groups spent more than 90% of time engaged in activities that required the use of the more-affected hand (SPG, 94.3%; UPG, 98.9%). In the SPG, whole task practice accounted for 87.8% of the time, and the remaining 12.2% comprised part task practice. Only whole practice occurred for the UPG. The accelerometry data for the subset of children who wore it indicated that on average the less-affected hand moved 79% and the more-affected hand moved 74% of the time for the SPG, and the less-affected hand moved 82% and the more-affected hand moved 68% for the UPG (P > .05, paired t test between the SPG and UPG). Thus, there was no difference in the amount of more-affected UE use between groups.
On average, activities for the SPG progressed in difficulty 55.4 times (standard deviation [SD] = 35.4, range = 11-117) throughout the intervention. Skill progression was not reported or observed for the UPG.
Manual Dexterity and More-Affected Hand Use in Bimanual Activities
For the JTTHF, there was a 65.9-second (28.1%) and a 77.4-second (33.2%) decrease in time for the SPG and UPG, respectively (Table 2, Figure 2A). Newman-Keuls post hoc tests revealed a significant improvement between the pretest and immediate posttest that was maintained at 6 months. For the AHA, there was an increase of 2.3 and 2.8 AHA-units for the SPG and UPG, respectively (Figure 2B, Table 2). Post hoc tests revealed a significant improvement between the pretest and immediate posttest, but a return to baseline levels at 6 months, which was uncorrelated with age. There were no group × test session interactions for either measure.
Results.
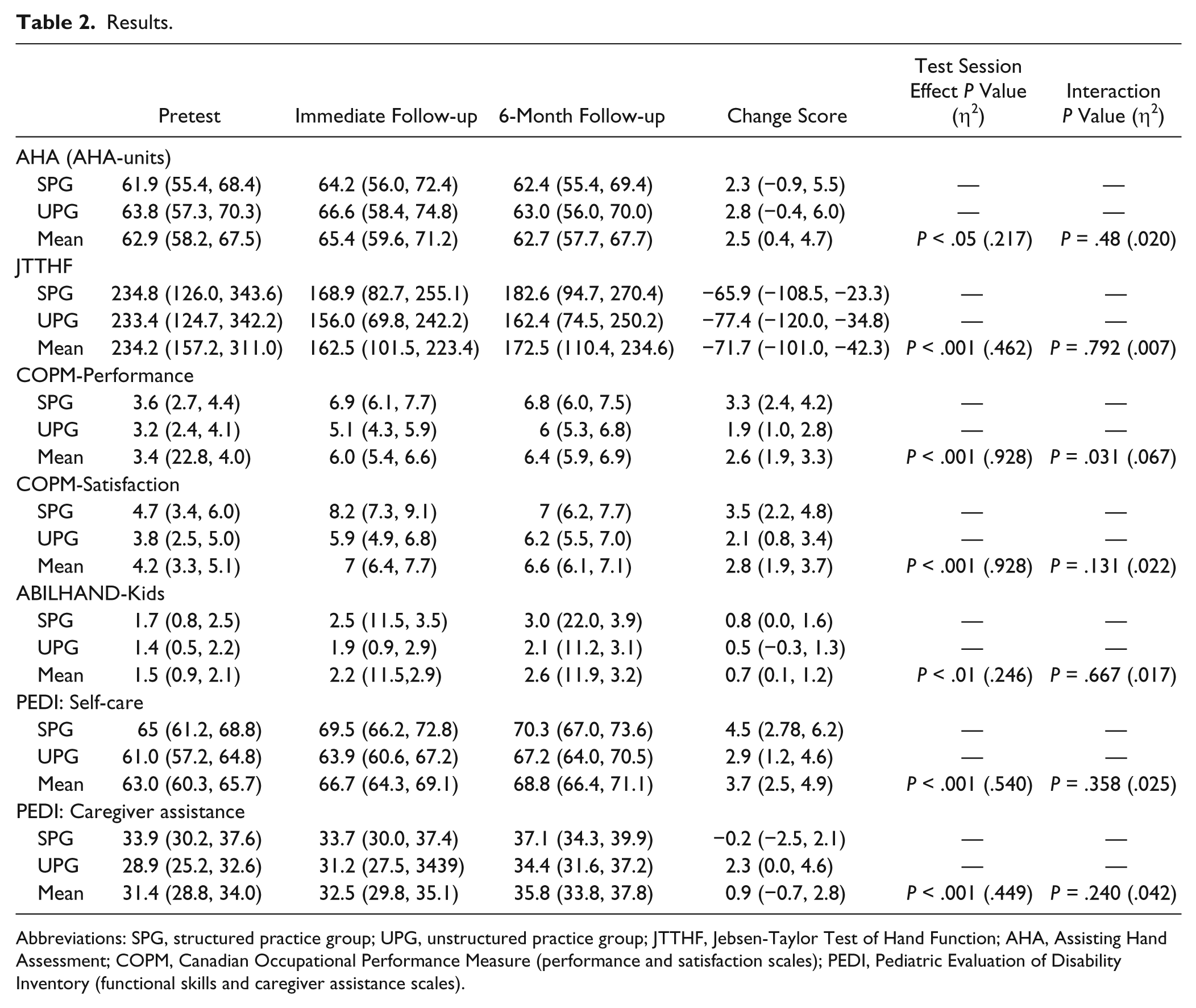
Abbreviations: SPG, structured practice group; UPG, unstructured practice group; JTTHF, Jebsen-Taylor Test of Hand Function; AHA, Assisting Hand Assessment; COPM, Canadian Occupational Performance Measure (performance and satisfaction scales); PEDI, Pediatric Evaluation of Disability Inventory (functional skills and caregiver assistance scales).
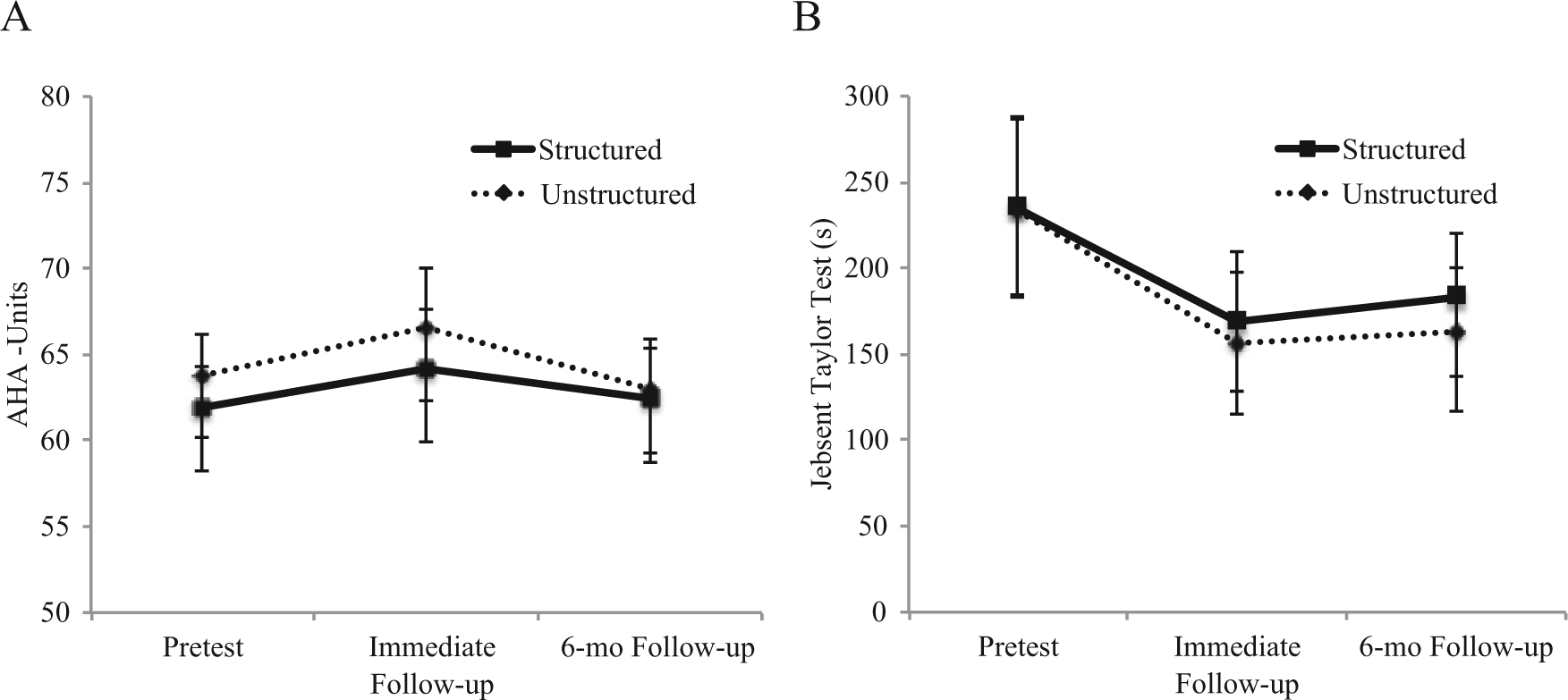
(A) Mean ± standard error of the mean (SEM) scaled logit scores on the Assisting Hand Assessment (AHA); higher scores represent better performance. (B) Mean ± SEM time to complete the 6 timed items (writing excluded) of the Jebsen-Taylor Test of Hand Function. Faster times correspond to better performance. The potential maximum allowable time to complete each item was 180 seconds, resulting in a maximum score of 1080 seconds.
Functional Goals and Daily Functioning
The majority of goals were bimanual (remaining goals were unimanual with the more-affected hand). Most of the goals comprised self-care activities (eg, dressing, grooming, and eating), followed by play (eg, ball activities). At camp, the SPG spent on average 370 minutes practicing goals whereas the UPG did not practice goals. At home, children spent 165 and 184 minutes for the SPG and UPG, respectively, practicing goals. Both groups presented significant improvements after the intervention on satisfaction and on performance, but there was a significant group × test session interaction, with greater improvement for the SPG (Table 2). This difference was no longer present at 6 months (paired t test). There was no correlation (Pearson) between the amount of home practice of goals and COPM improvement.
For the ABILHAND-Kids, both groups presented significant improvement with no group × test session interactions. Both groups improved on the functional self-care skills and caregiver assistance scale of the PEDI, with no significant interaction. Post hoc tests indicated significant improvements for the functional self-care skills at immediate posttest that were maintained at 6 months. However, the caregiver assistance scale was only significantly higher at the 6-month follow-up.
Control Group
It is conceivable that the similar improvements were simply because of repeating the tests over a 3-week period. To determine whether that was likely the case, we subsequently conducted the tests twice, 3 weeks apart, in a group of 10 (nonrandomized) children with USCP (mean age = 8.9 years, 5 males, 5 females) who did not receive treatment. There were no significant changes in the AHA (test 1 = 65.5 AHA-units [sd = 12.4]; test 2 = 64.8 AHA-units [SD = 14.3]), JTTHF (test 1 = 496.1 seconds [SD = 306.6]; test 2 = 465.8 seconds [SD = 315.9]), ABILHAND-Kids (test 1 = 1.6 logits [SD = 1.3]; test 2 = 1.6 logits [SD = 1.1]), PEDI functional skills self-care (test 1 = 61 [SD = 7.57]; test 2 = 63.3 [SD = 6.93]), or PEDI caregiver assistance (test 1 = 35.7 [SD = 3.2], test 2 = 36.7 [sd = 5.7]).
Discussion
To our knowledge, this study is the first to compare components of pediatric intensive bimanual rehabilitation protocols. Children from both the SPG and UPG demonstrated improvements in dexterity and functional use of the hands. This suggests that at least for such intensive bimanual approaches, training may not require structured practice to elicit improvements in clinical measures, and that the emphasis can be placed on fun activities that require use of both hands. However, considering that the SPG showed superior improvements in functional goals, there may be added benefit of including goal training. These findings are discussed in relation to other treatment approaches and neuroplasticity in animal and humans.
Similar dexterity improvements for both groups did not support our hypothesis of greater improvements for the SPG, and are not in agreement with animal model studies that point to the importance of skilled training in the acquisition of motor skills.28-30 However, in a study in which squirrel monkeys were exposed to a reaching task that did not involve skilled training, the animals showed improvements in the number of pellet retrievals and increase in speed to retrieve them. 28 Thus, it is possible that even without skilled training, intensive use of the more-affected hand leads to improvements in the speed to perform unimanual tasks. 28 Improvements in both groups are analogous to the similar improvements in the amount and quality of more-affected hand use between a group of adults with hemiparetic stroke submitted to CIMT regardless of whether shaping was used. 28 However, as acknowledged by the authors, it is not possible to conclude that skilled training is not relevant as the task practice group was submitted to some elements of shaping, such as verbal feedback and information related to the individual’s performance. 32 In the present study, we carefully monitored children’s activities during play activities from both groups. However, it was not possible to monitor every interaction or to avoid verbal feedback and encouragement.
This study suggests that bimanual structured practice may not be essential for improvements. The structure of intensive protocols is not well described in the literature. Some authors describe protocols comprising 1 interventionist to 2 children,14-16 or combining caregivers’ and therapists actions, 44 which may reduce the amount of skilled training. Nevertheless, these studies report improvements in hand function.15,44 The high intensity in both groups seems to be the main contributor to the similar improvements in dexterity as the (albeit nonrandomized) post hoc control group did not demonstrate changes in the same measures. Only part practice, skill progression, and goal training differed. Intensity is considered an important ingredient in motor learning, as it leads to repetitions of movements and the development of new motor strategies. 23 Thus, in intensive protocols the amount of practice is seemingly more important than what is practiced. However, these results may be dose dependent, as it is possible that at lower intensity, other components (eg, specificity of training) may be more important. 10 The low number of movement repetitions resulting from usual and customary schedules of physical/occupational therapy may partly explain the lack of evidence for these approaches. 45 Thus, it is possible that skilled practice is important in such low dose interventions.
One unexpected result was the lack of maintenance of AHA increases at the 6-month follow-up. Although it seems contrary to previous studies documenting persistent changes on this outcome following CIMT or HABIT,3,13,15 the lack of retention may be because of the age of the participants, who were generally older than those from other studies. Eliasson et al 46 reported no change in AHA following CIMT in 8- to 17-year-old children. We concur with their suggestion that changes in bimanual function are harder to achieve in older children. 46 It is possible that at older ages, dexterity (eg, JTTHF) and functional use (eg, COPM, PEDI, ABILHAND-Kids) may improve and be maintained, but children may have well established their own strategies to use the more-affected hand in the performance of bimanual activities, and that this strategy is more difficult to change. Goal performance was the only measure to improve differentially, that is, greater initial gains for the SPG. These results corroborate studies that found superior improvements on goal performance when goals are practiced.13,47 If the 6-month follow-up data are compared, the differences were no longer significant. As children from the SPG had the opportunity to practice some of the goals and this practice involved skill progression, it is possible that structured training contributed to the development of strategies to perform relevant functional goals. 47 Such information confirms the need of specific and direct training for the accomplishment of goals related to the use of hands by children with USCP, but the end result over a longer period may not differ.
Limitations
Although the interventions were administered in separate rooms and the groups and interventionists were blinded to the study questions, as mentioned above it is not possible to ensure that skill progression did not occur in the UPG. It is possible that children from either group could have been self-motivated to challenge themselves. However, the children, interventionists and families were not aware of the differences in the protocols provided for each group.
It is also possible that when caregivers selected goals for the COPM, they might be aware of the functional activities that are relevant to their children. This may have motivated goal practice despite that caregivers from both groups were not instructed to practice these goals at home and no information in how to progress performance of these goals was offered during the intervention period. On average, goal practice totaled ~3 hours, which is a small fraction of the amount of treatment time. Moreover, the children and interventionists from the USG were not aware of the goals. Furthermore, it is possible that there were indeed differences between groups that either was not measured (eg, ICF body structure and function level) or that the employed measures were not sensitive enough to detect. Finally, the study may have been underpowered to detect group differences. However, as indicated by the η2 values (Table 2), the differences in changes were extremely small (favoring the UPG) and would require an extremely large sample size for this difference to be statistically significant, which would bring the clinical significance of such changes into question.
Clinical Implications
The present study shows that the intensive nature of bimanual practice seems to be the main contributor for improvements in manual dexterity. It is not known whether these findings would hold true at lower dosages. It may be possible to combine interventions that involve bimanual play with specific functional training. This may reduce the costs of the provision of high-intensive interventions without compromising the benefits. This possibility needs to be tested in a larger cohort of children.
Footnotes
Acknowledgements
We thank Ashley Chinnan for evaluations, and Jason Carmel, MD, for neurological consulting, Carol Garber for use of her lab, and volunteer interventionists for their dedicated efforts, and the participants and families who participated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Thrasher Research Fund and CVS Caremark.