
Abstract
Background. Constraint-induced movement therapy (CIMT) promotes hand function using intensive unimanual practice along with restraint of the less-affected hand. CIMT has not been compared with a treatment with equivalent dosing frequency and intensity in children with cerebral palsy (CP). Objectives. The authors report a randomized trial comparing CIMT and a bimanual intervention (hand-arm intensive bimanual therapy; HABIT) that maintains the intensity of practice associated with CIMT but where children are engaged in functional bimanual tasks. Methods. A total of 42 participants with hemiplegic CP between the ages of 3.5 and 10 years (matched for age and hand function) were randomized to receive 90 hours of CIMT or an equivalent dosage of functional bimanual training (HABIT) conducted in day-camp environments. A physical therapist blinded to treatment allocation tested hand function before and after treatment. The primary outcomes were changes in Jebsen-Taylor Test of Hand Function (JTTHF) and Assisting Hand Assessment (AHA) scores. Secondary measures included the Goal Attainment Scale (GAS). Results. Both the CIMT and HABIT groups demonstrated comparable improvement from the pretest to immediate posttest in the JTTHF and AHA (P < .0001), which were maintained at 6 months. GAS, however, revealed greater progress toward goals for the HABIT group (P < .0001), with continued improvement across test sessions for both groups (P < .0001). Conclusions. Both CIMT and bimanual training lead to similar improvements in hand function. A potential benefit of bimanual training is that participants may improve more on self-determined goals.
Keywords
Introduction
Cerebral palsy (CP) is the most common pediatric physical disability, with congenital hemiparesis comprising one of the most common forms. 1 Strong evidence supporting any upper-extremity treatment approach is lacking.2,3 Yet there is increasing evidence that hand function in individuals with CP does improve during development4-6 and with intensive practice.7,8
One means to achieve intensive practice is constraint-induced movement therapy (CIMT), involving concurrent physical restraint of the less-affected hand and unilateral training of the hemiplegic hand.9-11 There is increasing evidence supporting the efficacy of pediatric CIMT,2,12,13 and its clinical use is proliferating.
Nevertheless, CIMT is potentially invasive, 14 and it is uncertain whether improved hemiparetic hand use results in improved function. Children with hemiplegic CP have impaired bimanual coordination above and beyond their unimanual impairments,15-17 which may underlie some functional limitations. Furthermore, studies of CIMT (including our own)18,19 have not compared it with other, equally intense treatments. Thus, it is unknown whether similar improvements in hand function can be achieved with an equally intensive bimanual treatment.
We report a randomized clinical trial comparing CIMT and a bimanual intervention (hand-arm intensive bimanual therapy, HABIT)20,21 that maintains the same dosing frequency and intensity and the progressive task-specific practice associated with CIMT, but children are engaged in functional bimanual rather than unimanual tasks. HABIT has a proposed neuroscientific rationale13,22 and is a formalized approach that has an equal amount of personal interaction and intensity as CIMT, encourages functional gains, 23 and has preliminary evidence suggesting efficacy.15,21 Yet bimanual training is different from CIMT because of the type of activities practiced. Based on theories of motor learning (practice specificity),24,25 we hypothesized that the unimanual training associated with CIMT would lead to greater improvements in unimanual dexterity, whereas bimanual training would lead to greater improvements in bimanual hand use and goal attainment.
Method
Participants
Participants were recruited from clinics in the NYC area, our Web site (http://www.tc.edu/centers/cit/), ClinicalTrials.gov (NCT00305006), and online support groups. Potential participants were first screened via e-mail and/or telephone. Those between the ages of 3.5 and 10 years with congenital hemiplegia were invited to receive an on-site physical examination or an examination videotaped by their physical or occupational therapist. The inclusion criteria were established based on prior CIMT and HABIT trials19,20: (1) ability to extend wrist >20° and fingers at the metacarpophalangeal joints >10° from full flexion, (2) the ability to lift the more affected arm 15 cm above a table surface and grasp light objects, (3) >50% difference in the Jebsen-Taylor Test of Hand Function (JTTHF) score between the 2 hands and a time below the maximum possible (1080 s) of the paretic hand, (4) mainstreamed in school and a Kaufman Brief Intelligence test score >70, and (5) demonstrated ability to follow instructions during screening and complete the testing. Exclusion criteria included the following: (1) health problems unassociated with CP, (2) current/untreated seizures, (3) visual problems interfering with treatment/testing, (4) severe muscle tone (Modified Ashworth score > 3.5), (5) orthopedic surgery on the paretic hand within 1 year, (6) botulinum toxin therapy in the upper extremity within the past 6 months or intended treatment within the study period, and (7) balance problems precluding wearing a sling. Informed consent was obtained from participants and caregivers. The study was approved by the University Institutional Review Board.
Procedures
General intervention procedures
CIMT and HABIT procedures share in common intensive progressive task practice based on motor learning approaches. They differ in that CIMT requires hand restraint and progression of unimanual tasks, whereas in HABIT, there is absence of restraint, and tasks are progressed bimanually. We first describe the common procedures followed by procedures specific to CIMT and HABIT.
Six HABIT and CIMT day camps were conducted at the University from July 2007 to 2009. The day camps were held in 2 separate rooms. Participants in 1 room received CIMT, and the other received HABIT; 2 to 5 children participated in each treatment at each camp. Participants were engaged in treatment 6 h/d for 15 consecutive weekdays (adjusted for holidays; 90 hours, making up any missed hours) during school recess by trained interventionists. Eight of the interventionists (out of 42 interventionist/child pairs) were physical or occupational therapists (PT/OT; 3 in the CIMT group and 5 in the HABIT group). The remaining interventionists were graduate students in Kinesiology, Neuroscience, Speech Pathology, or Psychology programs and undergraduates. Despite a higher level of knowledge and awareness of how to interact in a therapeutic manner, the PT/OT interventionists were required to provide only the specific procedures related to CIMT/HABIT and were restrained from using other treatment modalities. The expected outcomes were not discussed with interventionists. The pretreatment training, administered by the supervisors, was standardized based on the established manual of procedures for each treatment and reinforced by supervisors and during daily meetings. Each room was always supervised by additional experienced PTs/OTs, who modeled and ensured uniformity of treatment.
Participants worked individually with their interventionist or in groups (1:1 interventionist to participant ratio always maintained). Interventionists were paired with children prior to randomization using family-centered approaches considering caregiver and supervisors’ best judgment based on the child’s age and gender. Emphasis was placed on making participation enjoyable. With the exception of goals (see the following), tested task items were never trained. Children participated in whole and part task practice. Whole task practice involved sequencing successive movements within the context of tasks (eg, card games). The activities were performed continuously for at least 15 to 20 minutes. Targeted movements and spatial and temporal coordination were practiced within the context of completing the task. Part task practice (analogous to “shaping”)19,20 required breaking down motor skills into smaller components (eg, playing-card turning to promote forearm supination) while increasing repetitions and skill requirements. It also increased intensity of treatment by requiring as many repetitions as possible over repeated 30-s intervals (typically a minimum of 5 intervals).
Task difficulty was graded by varying the spatial/temporal constraints or by providing tasks that required progressive skilled use as performance improved. Task difficulty was increased when the participant was successful on 7 of 10 repetitions. Task performance was recorded, and task- and age-specific knowledge of results was provided for encouragement.26-28
Supervisors instructed interventionists regarding the main focus of the treatment (eg, supination) for each child, based on his/her pronounced movement deficits, interests, and potential for improvement. Data activity logs were collected, which included activities performed, time spent in part/whole practice, and the number of repetitions.
Caregivers were instructed to engage participants in home practice (unimanual without restraint for CIMT and bimanual for HABIT) for 1 h/d during and for 6 months following the intervention and document practice using activity logs.
CIMT procedures
CIMT was modified to be child focused (for details see Gordon et al 19 ). Participants’ less-affected hands were restrained with slings, and unimanual activities were performed with the paretic hands. The sling was strapped to participants’ trunks with the distal end sewn shut and was continuously worn except when toileting or during breaks (not >15 min/d).
Participants performed fine-motor and manipulative gross-motor activities that elicit general movements of interest and that included a range of age-appropriate, unimanual functional and play activities. The interventionist provided assistance where appropriate. For example, during scissor use, the child cut paper while the interventionist held and rotated the paper.
HABIT procedures
HABIT 20 did not use a physical restraint, but instead, participants were engaged in age-appropriate fine- and gross-motor bimanual activities using motor learning approaches. 28 Activities were selected by considering the role of the paretic hand, increasing in complexity from a nondominant passive assist (eg, stabilizing paper while drawing) to active manipulator (eg, reorienting paper while cutting) using increasingly complex bimanual coordination and participants’ interests. Task demands were graded, and participants were engaged in active problem solving.
Interventionists avoided verbal prodding to use the paretic hand and instead constrained the environment by providing tasks necessitating the use of both hands to elicit desired movements. Part practice included both bilateral symmetrical (eg, reaching toward object[s] with both hands) and asymmetrical (eg, pulling apart objects) movements.
Measures
Participants were evaluated directly prior to treatment (pretest), within 2 days (“immediate”), and 1 and 6 months after treatment by a physical therapist blinded to group allocation (verified following testing). Two primary outcome measures were used to quantify unimanual capacity and bimanual performance under the International Classification of Functioning and Health (ICF) “activity and performance” domain. 29
The Assisting Hand Assessment (AHA, version 4.3,30,31) quantifies the effectiveness with which a child with unilateral disability uses his/her affected (assisting) hand in bimanual activity. It has excellent validity and reliability (interrater = .97, intrarater = .99). 31 The test was videotaped and scored off-site by an experienced evaluator blinded to group allocation.
The JTTHF is a standardized test of simulated functional tasks quantifying the time to complete a battery of unimanual activities. 32 The activities performed with the paretic hand include flipping index cards, object placement, simulated eating, stacking checkers, and manipulating empty and full cans. Reliability for children with stable hand disabilities is high (.95-.99). 33 To determine whether the less-affected hand was affected by the restraint (CIMT) or use (HABIT), we also measured the JTTHF for this hand before and immediately after CIMT/HABIT.
Three secondary measures were also used. The dissociated movements (ICF “body function”) and grasp (ICF “body function” and “activity and performance”) subtests of the Quality of Upper Extremity Skills Test (QUEST) 34 were used to characterize dissociation of distal and proximal upper-extremity movements and attainment of specific grasp patterns of the 2 hands (ICF activity and performance and body function/structure). The sum score for both hands is converted to a standardized score (maximum = 100).
The Goal Attainment Scale (GAS; ICF “activity and performance” and “participation”) was used to quantify progress on established goals before group assignment (1 functional and 1 play goal defined by caregivers and/or older participants). Goals were assessed for appropriateness based on age and current abilities and scaled off-site by a physical therapist. The goals were practiced up to 30 min/d. However, because emphasis was placed on embedding practiced movements into fun activities rather than providing “goal-training” as is often done in traditional occupational/physical therapy, interventionists were given latitude as to how much training was provided (if at all) within the 30-minute limit. The CIMT group was unable to practice bimanual goals and, instead, practiced unimanual movement components comprising the goal. Goal achievement 35 was rated by the caregiver and verified by a physical therapist. Scores were transformed to standardized T scores (mean = 50; standard deviation = 10) 35 :

where x j is the attainment score, n the number of scales, and P the expected correlation of scales (P = .3). A T score of 50 indicates that goals were attained.
Children wore activity monitors (Manufacturing Technology Inc, Fort Walton Beach, Florida, #7164; 5.1 cm × 2.6 cm × 1.5 cm, 42.9 g) 36 on their wrists during the AHA test sessions. The units sample (10 Hz) and store summed values in memory and data were downloaded to a PC. The number of accelerations is measured as activity counts (0.01664 g for an acceleration of 2.13 g directed parallel to the x-axis at 0.75 Hz), which were used to determine the percentage of time each hand was used while performing AHA activities. 21
Statistical Design
Sample size calculations were performed based on AHA scores derived from an earlier HABIT trial. 21 A mean improvement of 0.94 ± 0.54 logits for the HABIT group was reported. With α = .05, 1 − β = 0.80, and an estimated 20% dropout, 21 participants in each group were required. Intention-to-treat principles were used.
A 2 (Group) × 4 (Test Sessions) ANOVA with repeated measures on test sessions was performed on raw and log-transformed AHA, JTTHF, QUEST, and accelerometry data using SPSS 15. Since the findings were qualitatively similar, only analyses of raw data are reported. The overall Group × Test Session interaction tested whether the time course differed between treatment groups. Planned comparisons were used between the pretest and each of the posttests and the immediate posttest with the 1- and 6-month posttest. Bonferroni corrections were used, resulting in a significance level of P < .01. A 2 (Group) × 3 (Posttests) ANOVA with repeated measures on posttests was performed on the GAS T scores, with the group factor indicating whether one group had greater goal attainment.
Results
Patient Flow
Patient flow is shown in the CONSORT flow diagram (Figure 1). During recruitment (June 2007-2009), 183 individuals were screened. Ultimately, 44 qualified individuals agreed to participate and were randomized into the HABIT or CIMT group (see Figure 1 legend for details). Participants (4-10 in each camp) were randomized offsite using concealed allocation stratified by age and JTTHF screening score. A total of 42 participants (21 in each group) completed the study. Table 1 describes participant characteristics. There were no significant group differences in baseline scores for any measure (Table 2).
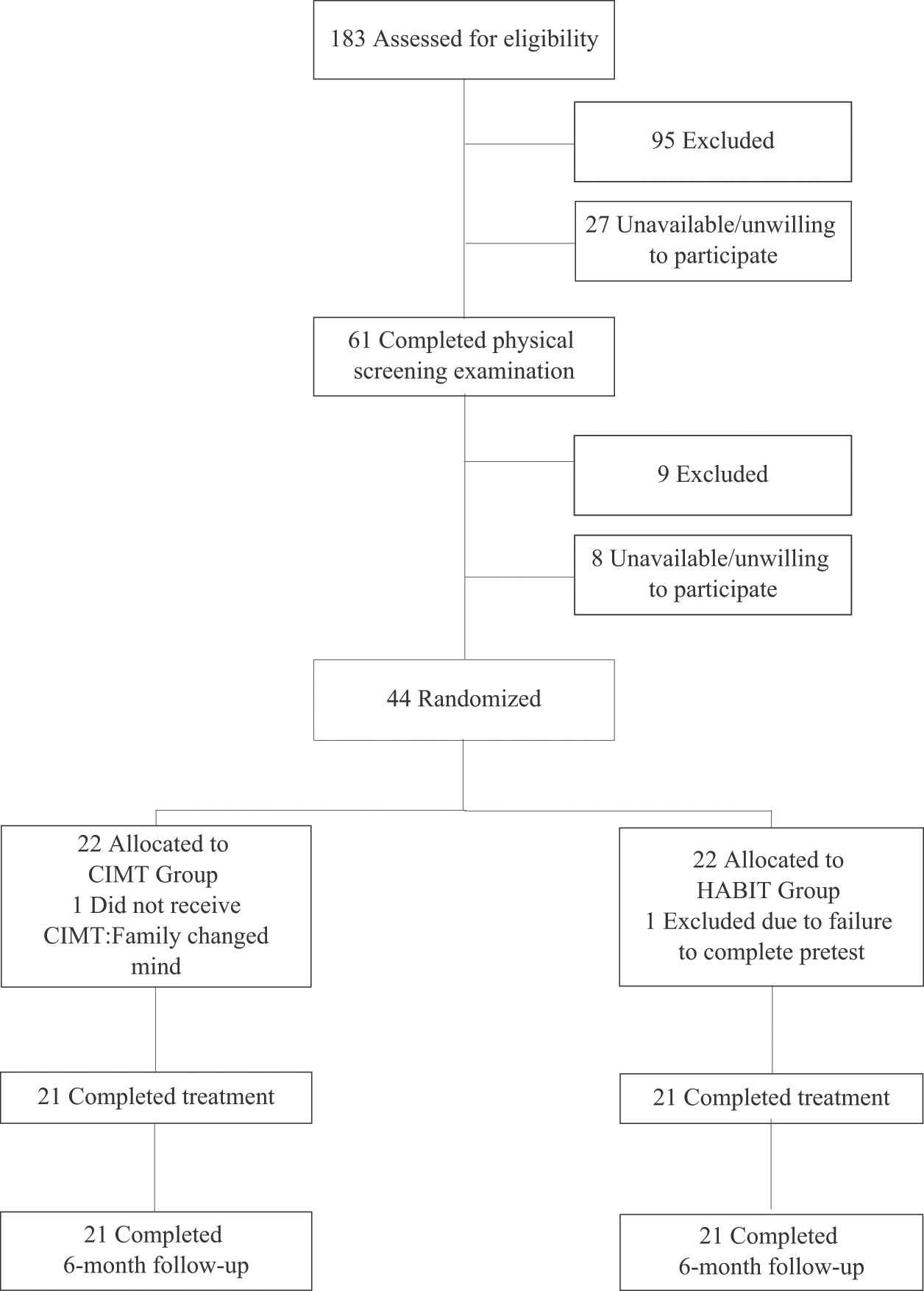
CONSORT flow diagram showing progress through the stages of the study, including flow of participants, withdrawals, and inclusion in analyses. A total of 183 individuals were screened via telephone/e-mail, and 95 of these were excluded for the following reasons: too old (n = 11), too young (n = 35), poor cognition (n = 11), wrong diagnosis (n = 22), botulinum toxin treatment within prior 6 months or planned within study period (n = 2), uncontrollable seizures (n = 7), prior CIMT within 6 months (n = 5), surgery (n = 1), and disease too severe (n = 1). A total of 88 individuals potentially met the study criteria and were invited to undergo physical screening; 27 individuals chose not to undergo physical screening. Of the remaining 61 individuals, 9 were excluded on the basis of the physical exam: too severe (n = 8) and too mild (n = 1). Of these individuals who qualified, 8 chose not to participate: not available during day-camp period (n = 5) and hardship associated with participating (n = 3). Ultimately, 44 of the remaining individuals agreed to participate and were randomized into the HABIT or CIMT group. One participant dropped out after randomization (unaware of group allocation), and another was excluded after the intervention for inability to comply with testing procedures. A total of 21 individuals from each group completed the intervention and subsequent posttests. Abbreviations: CIMT, constraint-induced movement therapy; HABIT, Hand-Arm Intensive Bimanual Therapy.
Baseline Participant Characteristics
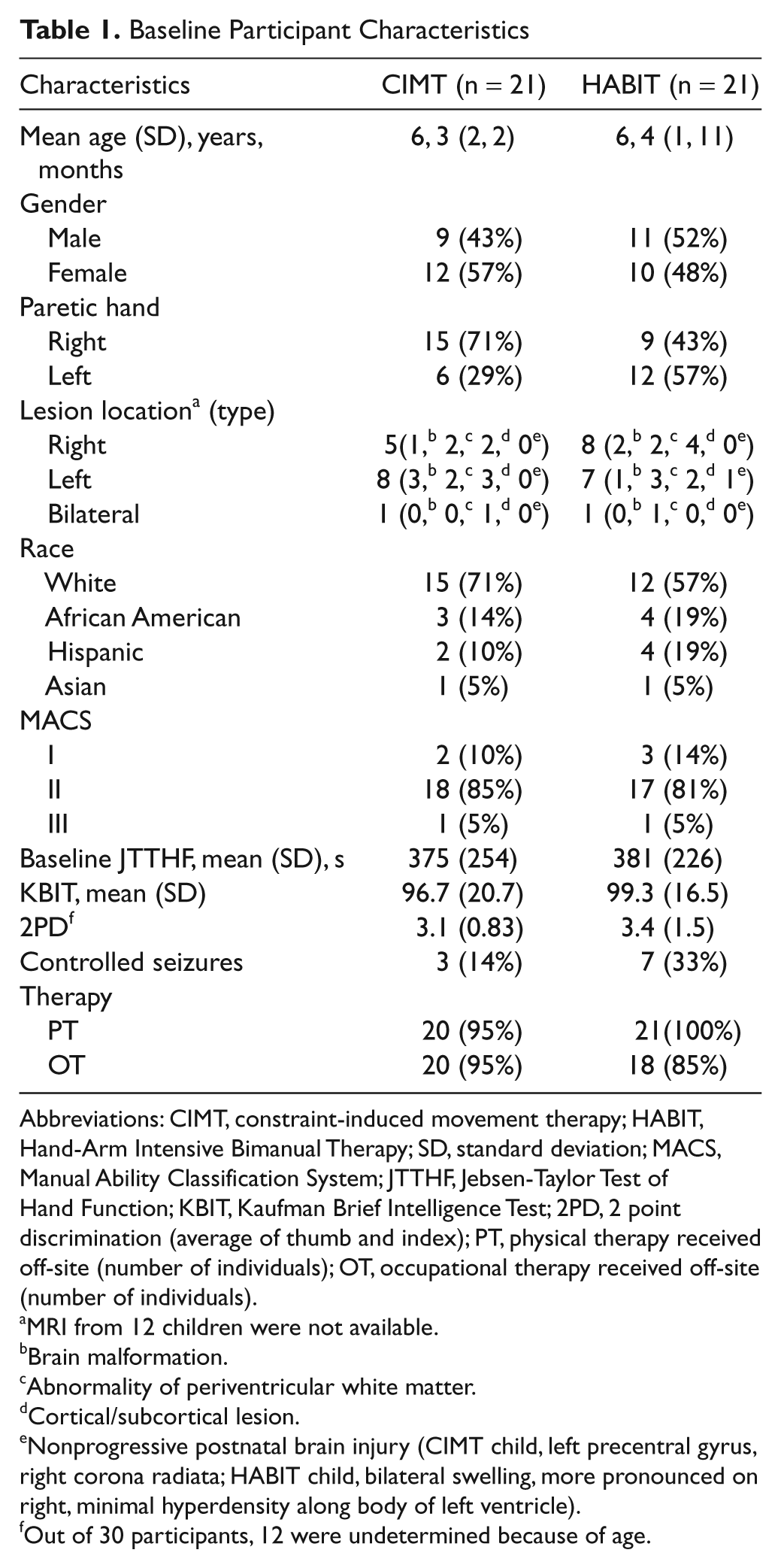
Abbreviations: CIMT, constraint-induced movement therapy; HABIT, Hand-Arm Intensive Bimanual Therapy; SD, standard deviation; MACS, Manual Ability Classification System; JTTHF, Jebsen-Taylor Test of Hand Function; KBIT, Kaufman Brief Intelligence Test; 2PD, 2 point discrimination (average of thumb and index); PT, physical therapy received off-site (number of individuals); OT, occupational therapy received off-site (number of individuals).
MRI from 12 children were not available.
Brain malformation.
Abnormality of periventricular white matter.
Cortical/subcortical lesion.
Nonprogressive postnatal brain injury (CIMT child, left precentral gyrus, right corona radiata; HABIT child, bilateral swelling, more pronounced on right, minimal hyperdensity along body of left ventricle).
Out of 30 participants, 12 were undetermined because of age.
Results
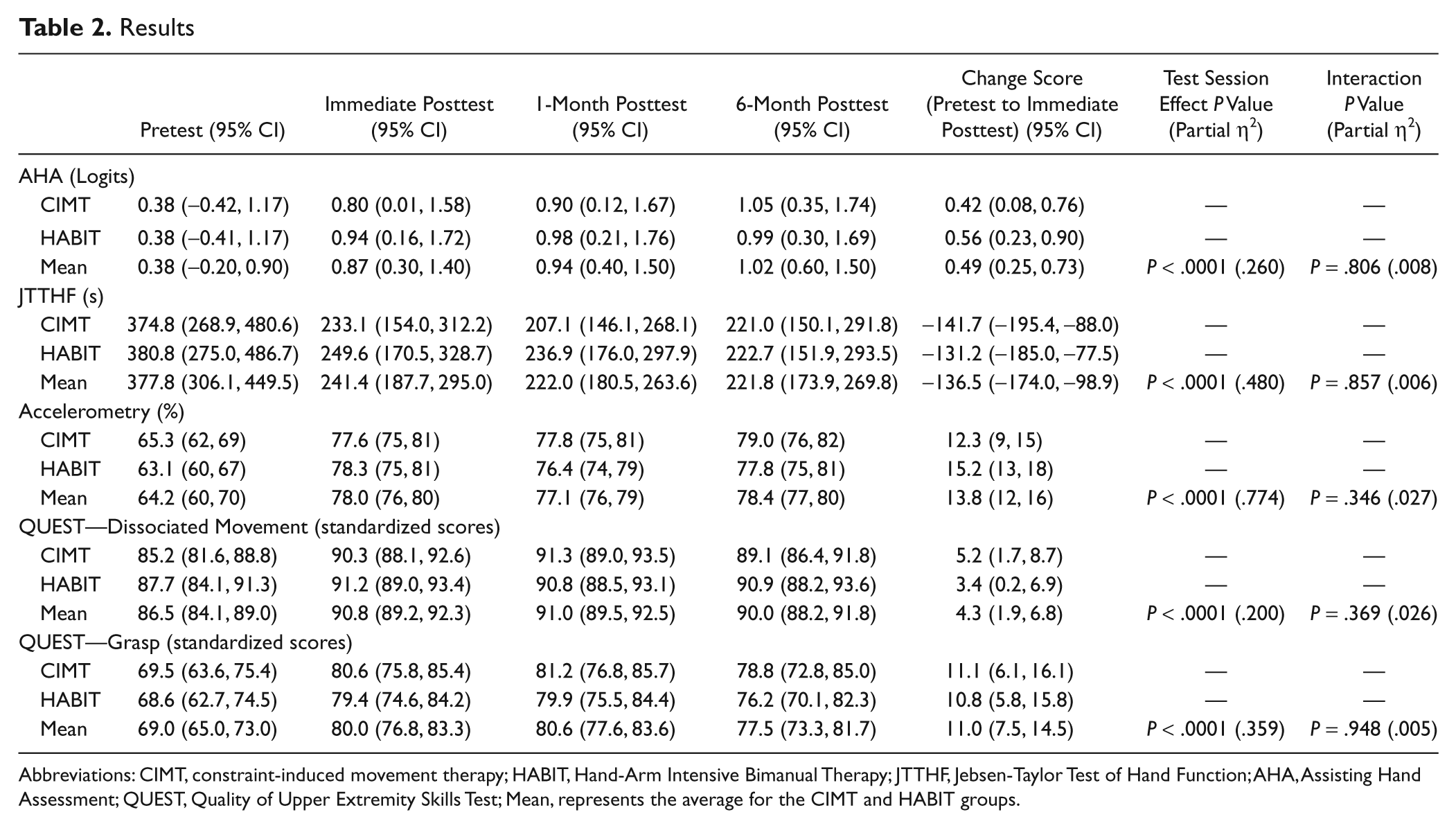
Abbreviations: CIMT, constraint-induced movement therapy; HABIT, Hand-Arm Intensive Bimanual Therapy; JTTHF, Jebsen-Taylor Test of Hand Function; AHA, Assisting Hand Assessment; QUEST, Quality of Upper Extremity Skills Test; Mean, represents the average for the CIMT and HABIT groups.
Treatment Characteristics
Participants in the HABIT and CIMT groups completed all 90 hours of treatment and averaged 79% and 81% of the time in structured practice, respectively (remaining time was spent in transitioning between tasks, toileting, etc). Children spent 17% and 16% of the practice time, respectively, in part practice, with the remainder in whole practice. Direct observation by the supervisors and monitoring of daily logs confirmed that both treatment protocols were completely adhered to and only the intended treatments were received. Home logs indicated that children averaged 286 minutes of the requested 360 min/wk engaging in home practice during the 6 months following the intervention.
No adverse events were reported. Participants stopped usual and customary care (UCC) during the treatment but resumed afterward (proportion receiving therapy was similar between groups: P > .05, Table 1). There were no changes to preexisting therapy.
Quality and Amount of Movement
Table 2 shows the means for the HABIT and CIMT groups at each time point and the pretest to immediate posttest difference for all measures. For the JTTHF, there was a 141.7 s (37.8%) and a 131.2 s (34.5%) decrease for the CIMT and HABIT groups, respectively (Figure 2A). Similarly, the AHA scaled logit scores improved 2.24 and 3.0 points for the CIMT and HABIT groups, respectively (Figure 2B). Planned comparisons revealed that the changes were attributed to differences between the pretest and immediate posttest that were maintained over the 6 months. There were no Group × Test Session interactions for either primary measure.
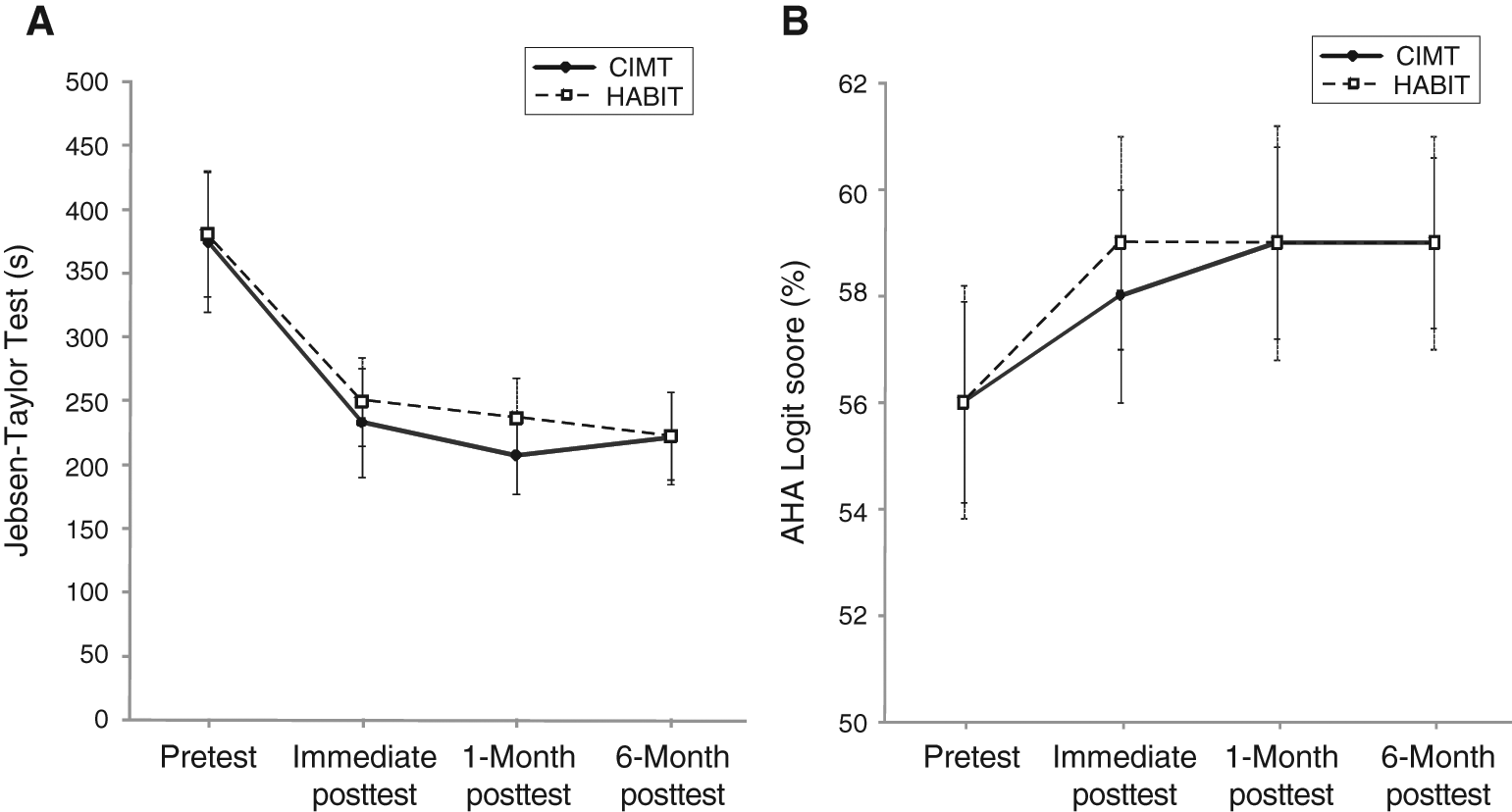
A. Mean ± standard error of the mean (SEM) time to complete the 6 timed items (writing excluded) of the Jebsen-Taylor Test of Hand Function. Faster times correspond to better performance. The maximum allowable time to complete each item was 180 s, resulting in a maximum score of 1080 s. B. Mean ± SEM scaled logit scores on the AHA; higher scores represent better performance. Abbreviations: CIMT, constraint-induced movement therapy; HABIT, Hand-Arm Intensive Bimanual Therapy; AHA, Assisting Hand Assessment.
There was no difference in the less-affected hand JTTHF for either group (CIMT change score = 6.1, 95% confidence interval [CI] = −3.5, 15.7; HABIT change score = 5.2, 95% CI = −0.8, 11.3; P > .05 in both cases).
To account for the asymmetric distribution of right- and left-side hemiparesis across the 2 groups, we repeated the analyses adding side as an additional factor. There was no effect of side or group interaction for either measure.
A main effect of testing session was also seen for secondary measures (QUEST dissociated movements and grasp subtests, and the accelerometry, Table 2) for both treatments. QUEST changes were largely a result of increased scores for the paretic hand (P < .001, not shown separately in Table 2). However, scores for the less-affected hand increased slightly (raw score pretest to immediate posttest across both groups, 23.3 to 23.9) for the grasp (P < .001) but not for the dissociated movements subtest. Accelerometry results indicated that the less-affected hand moved ~91% and the paretic hand ~64% of the time for each group at baseline. Hand use increased ~14% for both groups (ie, making up half of the baseline difference) for the hemiparetic hand, whereas it remained unchanged for the less-affected hand. The changes did not correlate with AHA scores changes (r = −0.041) but did correlate with JTTHF changes (r = 0.48; P < .001).
Goal Attainment
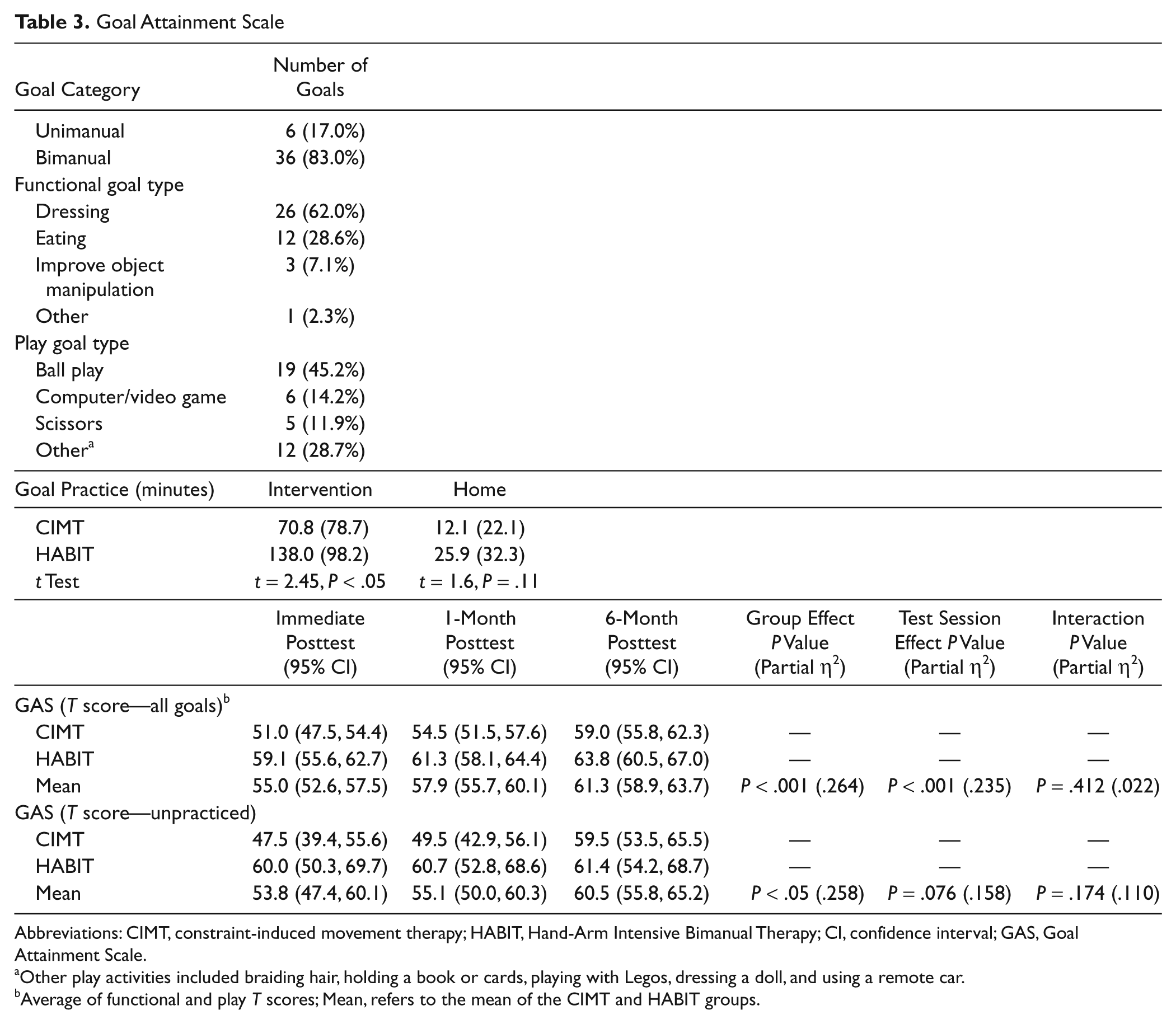
Goal characteristics and attainment are described in Table 3. The majority of goals were bimanual (remaining goals were unimanual with paretic hand). All goals were related to the ICF “activity and performance” domain. The HABIT group spent more intervention time practicing goals than the CIMT group, but home time practice of goals did not significantly differ between groups.
Goal Attainment Scale
Abbreviations: CIMT, constraint-induced movement therapy; HABIT, Hand-Arm Intensive Bimanual Therapy; CI, confidence interval; GAS, Goal Attainment Scale.
Other play activities included braiding hair, holding a book or cards, playing with Legos, dressing a doll, and using a remote car.
Average of functional and play T scores; Mean, refers to the mean of the CIMT and HABIT groups.
Both groups achieved (T score of 50) or exceeded their expected level of goal performance and continued to improve across test sessions. However, the HABIT group made greater progress than the CIMT group, as indicated by significant group differences in their T scores across all test sessions (Table 3). The combined amount of camp and home practice time did not correlate with GAS T scores (r = 0.06) at immediate posttest.
Approximately 25% of the identified goals were not practiced in either group during the interventions or at home. However, the T scores for these unpracticed goals were significantly higher for the HABIT group (Table 3). These scores appeared to improve across test session, but the improvement and interaction with group was not statistically significant.
Predictors of Improvement
Participants with higher initial JTTHF scores had greater absolute (r = 0.69), but not percentage change in, JTTHF scores for CIMT and HABIT. Neither age nor any other variable was related to primary measure improvement for either treatment.
Finally, in the present study, only 8 of the 42 participants were assigned a physical or occupational therapist for the intervention. There was little difference in AHA or JTTHF changes (as evidenced by small mean differences and overlapping distributions) regardless of whether the interventionist was a PT/OT or not (PT/OT AHA change score = 1.37, 95% CI = −1.11, 3.86; non-PT/OT AHA change score = 2.91, 95% CI = 1.47, 4.35; PT/OT JTTHF change score = 118.9, 95% CI = 48.8, 189.0; non-PT/OT JTTHF change score = 140.6, 95% CI = 98.4, 182.9). Similar absences of differences were observed for the secondary measures.
Discussion
Bimanual training and CIMT resulted in similar improvements in the primary measures, which did not support our hypothesis of specificity of training. This suggests that improvements in hand function associated with CIMT can be achieved with an equally intensive bimanual approach. However, there was specificity of training for goal attainment, whereby the HABIT group made better progress on established goals and transfer to unpracticed goals. These findings have important implications, given the increasing popularity and potential invasiveness of CIMT. It is important to note that our results suggest that intensive progressive task-specific training improves hand function.
Both CIMT and Bimanual Training Improve Hand Function
In agreement with our quasirandomized CIMT/HABIT trial, 15 there were significant changes in all measures following CIMT and HABIT. The partial η2 (Tables 2 and 3) indicated that 26% and 48% of the variance in AHA and JTTHF, respectively, and up to 77% for secondary measures, is attributable to the treatments. Similar findings have been reported following adult stroke cerebral vascular accident (CVA) interventions.37,38 The robust JTTHF changes for both treatments (137 s) were nearly twice those reported in a 13-year follow-up study of hand function development in CP. 4 Yet these improvements were achieved in just 3 weeks and were maintained at the 6-month follow-up.
Since early development of corticospinal tract (CST) is activity dependent, prolonged movement restraint in the developing infant could conceivably affect the restrained hand.13,39 Treatments that potentially promote rebalancing M1 excitability, such as bimanual practice or inhibiting contralesional M1 using transcranial magnetic stimulation, 40 may facilitate recovery. Our findings indicate that bimanual training is an effective alternative to CIMT.
Intensive approaches such as CIMT may be additive over repeated exposures. 41 Thus, emphasis should be placed on providing treatment in a child-friendly manner. There could also be an additive effect of combined (CIMT/bimanual) ingredients. Combined treatment showed improvement compared with a group of participants who received the same cumulative amount of an alternative treatment, although the dosing schedules were different. 42 Our findings of similar improvements in hand function for both treatments may indicate that both dosing schedule and intensity may be important.
Bimanual Training and Goal Attainment
Bimanual training affords learning strategies that have direct impact on daily routines. Although both groups achieved expected goal performance, the attainment was higher for the HABIT group at all test sessions. Goal attainment continued to improve for both groups across test sessions, with the CIMT group appearing to make greater continued gains at the 6-month posttest (but P > .05). Not surprisingly, most goals were bimanual because participants had a well-functioning dominant hand. Performance of bimanual activities in hemiplegic CP is a complex process influenced by internal and external factors, with strategies chosen based on the least negative alternative. 43 Thus, improved bimanual performance is functionally important, and bimanual training allows direct practice of these goals.
It would not be surprising that goals that are practiced more improve more. However, despite the greater goal practice in the HABIT group, this was not the case because the amount of practice did not correlate with GAS improvements. It is particularly interesting that there was greater improvement even for unpracticed goals for the HABIT group. Thus, there was better transfer of practice from other bimanual skills to goal achievement. This transfer could be a result of improvements in the ability to coordinate movements between the 2 hands and/or increased problem solving (identified as important for plasticity) 44 required during bimanual performance, given the increased degrees of freedom. Accordingly, action planning in children with hemiplegia may improve following a combined CIMT/bimanual training. 45
Therapeutic Considerations
One potential advantage of CIMT is that the restraint allows the interventionist to focus solely on the more affected hand. Our protocol relies on a 1-to-1 interventionist to child ratio. In the absence of this possibility, the restraint may result in greater intensity because participants would have no choice but to use their more-affected hand (ie, forced use). However, the restraint would preclude opportunity to practice functionally meaningful (bimanual) movements.
The similar improvements regardless of whether or not interventionists were clinicians suggest that the 1-to-1 ratio can be maintained in an economically feasible manner. The similarity is likely a result of the fact that preintervention training is standardized, and clinicians were required to closely adhere to standardized procedures and not administer therapeutic techniques incompatible with motor learning approaches used by HABIT and CIMT. 28 Both treatments were supervised by PT/OTs, who maintained the integrity of the standardized training, which may have further reduced differences.
Limitations
There may be individual differences that make 1 treatment more effective for a given individual or yield a response difference that depends on the hemiparetic side. There was an unequal distribution of side of hemiparesis in each group. However, when this was taken into account, the results did not change.
It is conceivable that the measures used are not sensitive enough to detect subtle differences between treatment outcomes. For example, there could be differential changes in the spatial–temporal coordination of the hands that can only be determined kinematically. Furthermore, although the sample size was fairly large for a physical rehabilitation study, differences may emerge with a larger and more diverse sample.
We did not randomize interventionist assignment or include a no-treatment/UCC group. However, for the latter, nearly all the improvement occurred at the immediate posttest. Although we only had 1 pretest, the JTTHF during screening (~1 month prior) and at pretest did not significantly differ. Furthermore, earlier studies of CIMT4,18 and HABIT 21 indicate that these measures do not change over 6 months in a UCC group.
Finally, treatment efficacy may differ at lower dosages (ie, the 90 hours may wash out differences). In fact, an earlier 60-hour HABIT study found that hand function began to return toward baseline at 1-month posttest, 21 whereas we did not find this following 60 hours of CIMT 18 (albeit using different measures) or for either 90-hour treatment here. 46 Further research is required to establish both optimal ingredients, dosage responses, and feasibility in real-world settings.
Footnotes
Acknowledgements
We thank Pamela Wareham and Cecile Grobert for assistance in analyzing data; Sandeep Prabu for evaluations; Ellen Romein for scoring AHA assessments; Lena-Krumlinde Sundholm for a critical discussion; Robert Palisano for assistance in goal attainment scaling; Steven Wolf for helpful comments on an earlier draft of this manuscript; Jennifer Schneider for behind-the-scenes support and data analysis; Ruth Nass, MD, and Jason Carmel, MD, for neurological consulting; Carol Garber for use of her laboratory; our evaluators and volunteer interventionists for their dedicated efforts; and the participants and families for their participation.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: this work was supported by a grant from the Thrasher Research Fund and CVS Landmark Cares.