
Abstract
Background. The properties of the mirror neuron system suggest a new type of upper limb (UL) rehabilitation in children with unilateral cerebral palsy (UCP), based on observation of action therapy followed by execution of a variety of observed movements (AOT). Objective. We tested the effects of AOT in the Upper Limb Children Action Observation Training (UP-CAT) trial. Methods. In a randomized, evaluator-blinded, block-designed trial, 24 UCP children with mild to moderate hand impairment were assigned to 2 groups. The experimental group observed, 1 hour per day for 3 consecutive weeks, video sequences of unimanual or bimanual goal-directed actions and subsequently executed observed actions with the hemiparetic UL or both ULs. The control group performed the same actions in the same order as the experimental sample, but had watched computer games. The Assisting Hand Assessment (AHA) scale was the primary outcome measure; the Melbourne assessment and ABILHAND-Kids were secondary ones. Outcomes were assessed at 1 week (T1), 8 weeks (T2), and 24 weeks (T3) after the end of the training. Results. The experimental group improved more (P = .008) in score changes for the AHA at the primary endpoints T1 (P = .008), T2 (P = .019), and T3 (P = .049). No between-group significant changes were found for ABILHAND-Kids or Melbourne assessment. Conclusions. UP-CAT improved daily UL activities in UCP children, suggesting a new rehabilitation approach based on a neurophysiological model of motor learning.
Keywords
Introduction
Cerebral palsy (CP), with a prevalence ranging between 2 and 3 per 1000 live births, is the largest cause of childhood physical disability in the industrialized societies. 1 Children with unilateral cerebral palsy (UCP) represent 30% to 40% of the general population of CP children, their upper limb (UL) being generally more affected than the lower limb.2,3 Unimanual activities are often preserved, as they are performed by the nonaffected UL; nevertheless, activity and participation of children are severely impaired as most daily activities are bimanual.4,5
Several models of intervention are currently available, targeting deficits in UL function and aiming at reducing activity limitations. 6 In a recent systematic review and meta-analysis, 7 4 main interventions have been outlined—intramuscular botulinum toxin A combined with UL training, constraint-induced movement therapy, hand-arm bimanual intensive training, and neurodevelopmental treatment. Unfortunately, randomized controlled trials (RCTs) that measure clinical results in children with hemiplegia are scarce.8 -11 New interventions strategies, based on solid methodological and scientific grounds are needed. 12
Recent neurophysiological evidences on motor control and learning have disclosed some interesting opportunities for rehabilitation. Brain imaging data in humans showed that both imagery and actual execution of hand actions activate similar structures of the sensorimotor cortex.13,14 Moreover, it was shown in both monkeys and humans the existence of a neural system, whose core regions are ventral premotor and inferior parietal cortex, that is activated both when individuals perform goal-directed motor acts (eg, grasping an object) and when they observe someone else performing the same or a similar motor act.15,16 This system has been dubbed the mirror neuron system (MNS) and may play an important role in action understanding, imitation, and motor learning. 17 Functional magnetic resonance imaging studies have shown that action observation, combined with actual replication of the observed action, induces a strong activation of the MNS, along with marked improvement in motor learning efficacy.18,19
These results have fostered the development of rehabilitation protocols based on the observation of meaningful actions followed by their execution (Observation to Imitate [OTI]).20,21 This approach, often labeled Action Observation Treatment (AOT) and based on the OTI paradigm, has been used with promising results in pilot studies on adults with stroke,22,23 Parkinson’s disease,24,25 and during recovery from orthopedic surgery. 26
Knowledge on the ontogeny of the MNS and its role during infancy is still scarce and mostly indirect. Many studies provided evidence that newborns 27 and infants 28 are able to imitate others’ individual gestures. Activation of the motor cortical areas during action observation in infants has been reported.29,30 In addition, a recent pilot study performed in children with CP suggests positive effects on UL function after a rehabilitation program based on AOT. 31
We recently proposed 32 an original paradigm of UL rehabilitation, called Upper Limb Children Action Observation Training (UP-CAT) and we have designed, according to CONSORT 12 Statement, and registered a RCT based on this approach.
We first hypothesized that UCP children receiving the UP-CAT would demonstrate significantly greater improvement than the control group immediately after the training, and secondly that this effect would be retained at the follow-up 2 and 6 months later. Furthermore, we hypothesized that, since MNS activity is related to action goals, regardless of the movement’s kinematic properties, the observed improvement would be greater in the goal-relatedness of UL use, rather than in UL kinematics.
Methods
This randomized, evaluator-blinded, block-designed trial has been described elsewhere 32 and will be briefly summarized. The study was conducted in 2 clinical centers: the Department of Developmental Neuroscience of IRCCS Stella Maris (Pisa, Italy) and the Unit of Children Rehabilitation of IRCCS S. Maria Nuova Hospital (Reggio Emilia, Italy). This trial was approved by the Ethical Committee of both Institutions and was registered at http://www.clinicaltrials.gov (identifier NCT01016496). All parents provided written informed consent to the treatment.
Study Population and Randomization
Between June 2009 and September 2010, UCP children between 5 and 15 years were enrolled according to the following inclusion criteria: (a) confirmed diagnosis of spastic UCP; (b) grade ≤2 on the Modified Ashworth Scale 34 ; (c) grade between 4 and 8 on the House Functional Classification System (HFCS),35,36 that is, children whose hand ability ranged from “fair passive assist” impaired hand, able to grasp object and hold it weakly (level 4), to a complete “spontaneous use” of the hand that moves independently of the other hand (level 8); (d) cognitive level within normal limits; (e) absence of attentional or sensory impairments; (f) no history of seizures or seizures well controlled by therapy; and (g) living near 1 of the 2 clinical centers with parents able to commit to an intensive therapy program for 3 weeks. Children who had sustained previous orthopedic surgery or botulinum toxin A injection in the UL within 6 months prior to study entry were excluded.
After obtaining the informed consent, the participants were block randomized into pairs according to HFCS activity level (grades 6-8 vs 4-5), using a computer-generated set of random numbers. All randomization, sequence generation, and preparation of group allocation materials were performed by researchers who had no direct contact with the clinical aspects of the trial.
Interventions
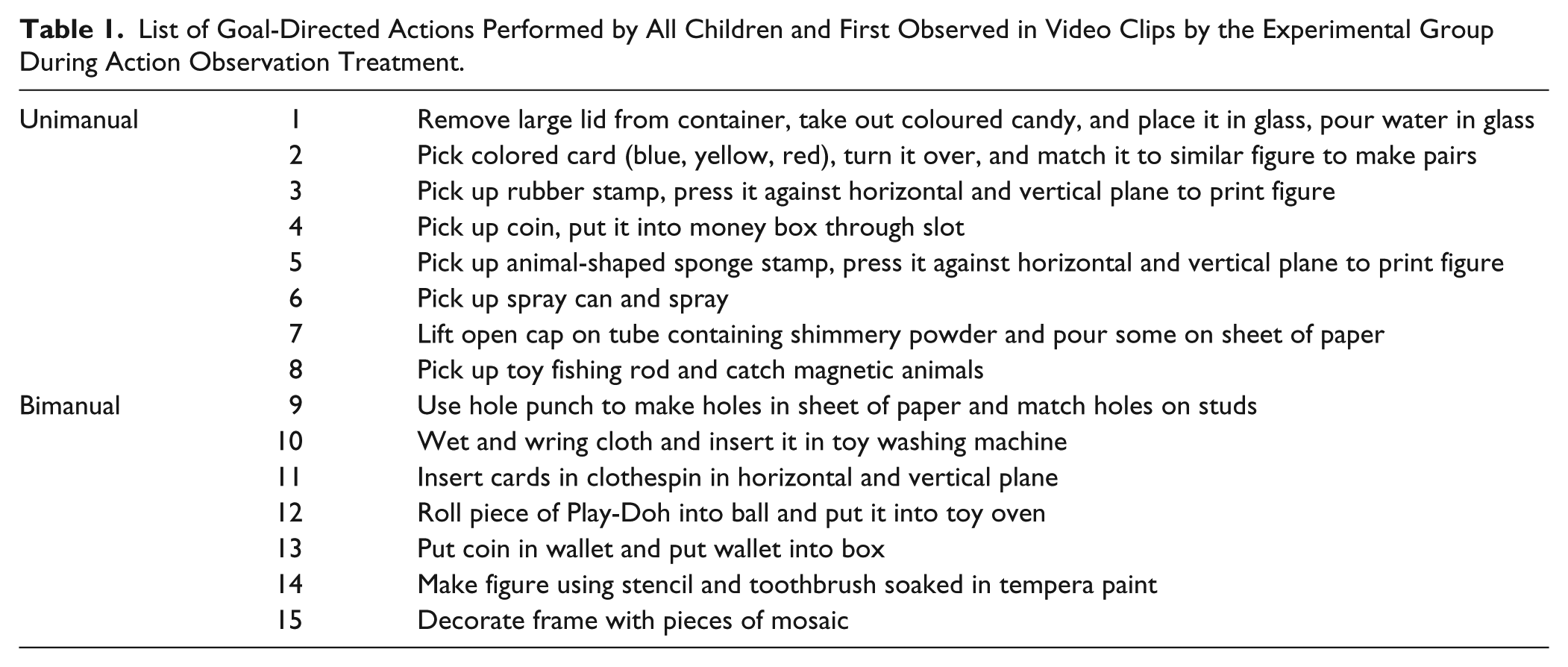
We planned 15 sets of daily life UL exercises (eg, fill up a glass of water or pick up a coin and put it in a money box; Table 1). Each set was composed by 3 sequential UL goal-related actions of increasing complexity. In order to grade the activities according to the range of children capabilities, 2 series of sets were conceived in relation to the HFCS level. The exercises used the same material but differed in type of movement (ie, range of movement, type of grasp) to guarantee the feasibility of the proposed activity both in terms of movements and goal. During the rehabilitation sessions, each child from both groups sat on a chair with both arms placed on a table in front of a large monitor screen (22 inches) positioned at 1 m. A staff member sat at the child’s affected side to prompt attention during task execution. The experimental group performed the UP-CAT protocol, which required the observation of video sequences showing unimanual or bimanual goal-directed actions followed by the execution of the observed actions either with their plegic UL for unimanual or with both ULs for bimanual actions. Each video sequence lasted 3 minutes and showed one goal-directed action that was repeated a number of times, depending on the duration of the video (minimum 15 times). Then the child was required to perform the same observed action for 3 minutes in the exact order and with the same objects as shown in the video. The therapist encouraged the child by providing verbal suggestions without performing any demonstration. The child had to continuously repeat the observed action for 3 minutes. Subsequently, the same video sequence was replayed a second time. Every day, 3 different goal-directed actions of increasing complexity were observed and imitated for a total time of about 60 minutes, including resting intervals. Children underwent 15 rehabilitation sessions on 15 consecutive working days for a total of 45 different goal-directed actions. Children from the control sample watched computer games and then were verbally instructed to perform the same UL actions and in the same order as the experimental group. More details on the rehabilitation protocol have been reported elsewhere. 32
List of Goal-Directed Actions Performed by All Children and First Observed in Video Clips by the Experimental Group During Action Observation Treatment.
Outcomes
Trained child therapists blind to group assignment evaluated all enrolled children at baseline (T0, before the training), and at 1 week (T1), 8 weeks (T2), and 24 weeks (T3) after the end of the training. As primary outcome we adopted the Assisting Hand Assessment (AHA) 33 test, which evaluates the spontaneous use of the assisting hand during a semistructured play session with specific toys. As secondary outcome we selected the Melbourne Assessment of Unilateral Upper Limb Function (MUUL). 37 Both these assessments were videotaped and then scored by observers who were blind as to the group allocation and assessment order. Moreover, to evaluate bimanual home and community activities, parents filled out the ABILHAND-Kids questionnaire, 38 following the same experimental assessment time schedule. Parents were blinded to the group assignment.
Statistical Methods
The RCT was designed to evaluate the actual efficiency of OTI in improving bimanual UL activity performance. According to CONSORT guidelines, the sample size estimates were based on projected treatment effect on the primary outcome measure (AHA). The AHA scale responsiveness to change has been shown in a study in which Eliasson et al 39 used this scale as the outcome measure in evaluating the effects of a modified model of constraint-induced movement therapy. The authors reported a significant effect size of 1.16. The statistical analysis indicated that, to detect a 1.16 effect size at a significant level of .05 and 80% power, a minimum sample size of 12 subjects per group was required. Clinical data were analyzed by means of the Statistical Package for Social Sciences (SPSS, version 20.0). Means and standard deviation of the rehabilitation scores for both groups were calculated to identify potential baseline differences between groups. As a first step, between-group differences for all selected outcome measures were evaluated at T0, by means of Mann–Whitney U independent sample test, to verify that the 2 groups had the same baseline.
To test our first hypothesis the between-group differences for the primary and secondary outcome measures were evaluated at the primary endpoint (T1), compared with T0, by means of Mann–Whitney U independent sample test. This same test was performed for the differences between T2 and T3 and baseline (T0), to test the secondary hypothesis, that is, whether an effect was retained at following checks. This last hypothesis was also examined by Wilcoxon matched-pairs signed rank test between T0 and the subsequent assessments (T1, T2, and T3) for each group in the primary outcome measure. Bonferroni corrections were used, resulting in a significance level of P < .0166, to account for multiple comparisons. To detect if significant changes were correlated to the level of HFCS, we performed a correlation analysis between the change scores of primary endpoint time (T1) and baseline versus HFCS for the primary outcome measure.
Results
Recruitment and Study Population
As indicated in Figure 1, 24 children were enrolled out of 66 assessed for eligibility at the 2 centers. A total of 42 children were excluded because either they did not meet the inclusion criteria or parents declined participation. Thereafter, no subjects missed any follow-up sessions; children and parents maintained their interest on the trial and no adverse events were detected. The experimental and control groups had similar demographic and clinical baseline characteristics (see Table 2). No differences in baseline scores for AHA (P = .31), MUUL (P = .40), and ABILHAND-Kids (P = .56) between groups were found.
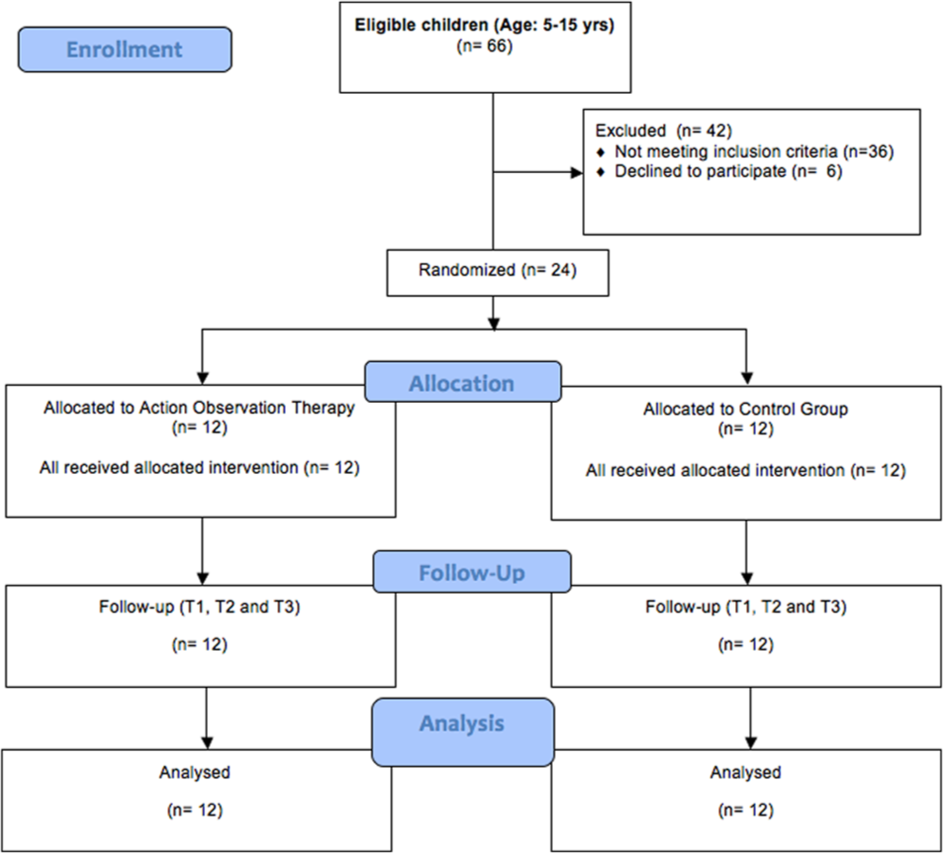
Flow diagram of Upper Limb Children Action Observation Training (UP-CAT) study aimed to compare the results of observation of upper limb goal-directed actions followed by execution (action observation therapy) to observation of no relevant computer games followed by the execution of the same actions (control group). No children enrolled missed any follow-up sessions.
Main clinical characteristics of experimental and control cases.
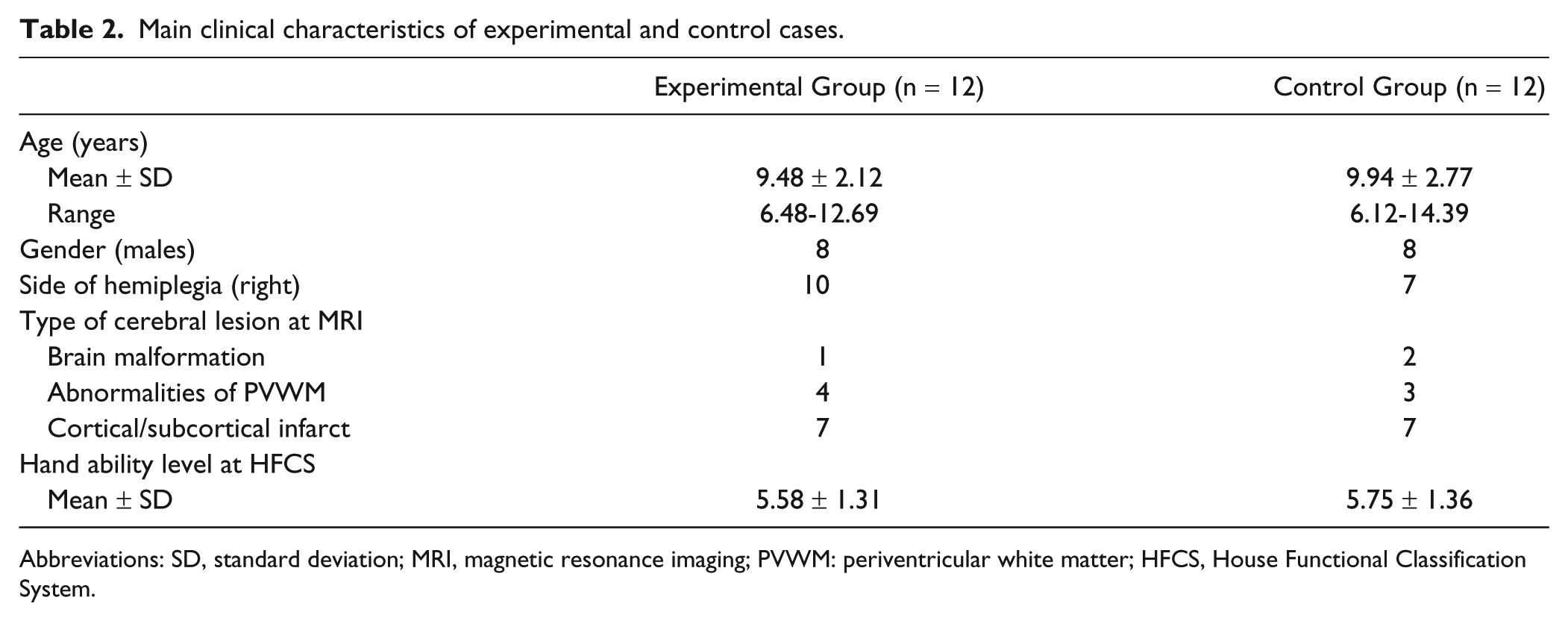
Abbreviations: SD, standard deviation; MRI, magnetic resonance imaging; PVWM: periventricular white matter; HFCS, House Functional Classification System.
Table 3 shows between-group results for the primary and secondary outcome measures.
Between-Group Differences.
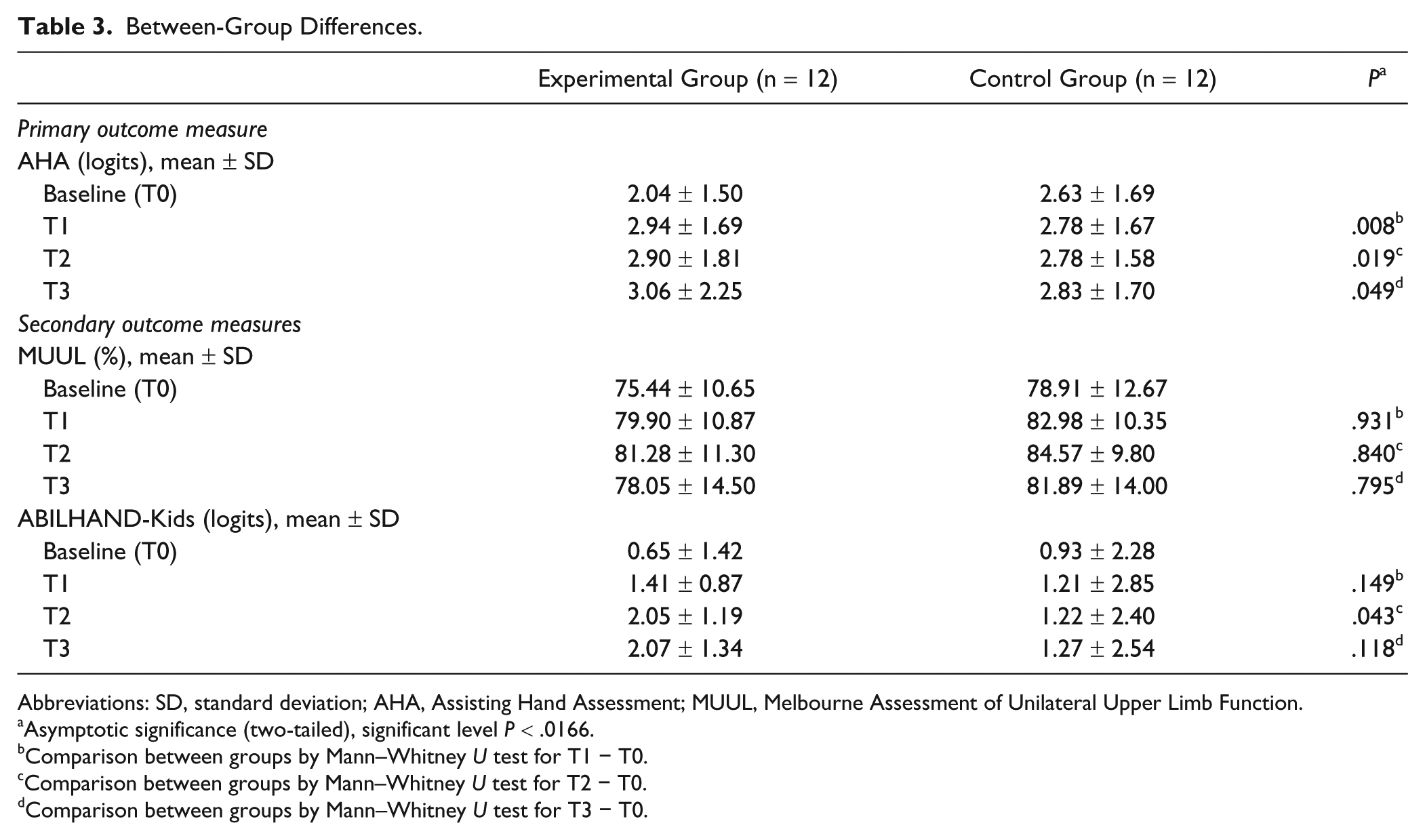
Abbreviations: SD, standard deviation; AHA, Assisting Hand Assessment; MUUL, Melbourne Assessment of Unilateral Upper Limb Function.
Asymptotic significance (two-tailed), significant level P < .0166.
Comparison between groups by Mann–Whitney U test for T1 − T0.
Comparison between groups by Mann–Whitney U test for T2 − T0.
Comparison between groups by Mann–Whitney U test for T3 − T0.
Primary Outcome
Assisting Hand Assessment
At the primary endpoint (T1) between-group difference in the changes was significant (P = .008) and this difference tended to remain at T2 and T3, although at the limits of statistical significance (T2 − T0, P = .019; T3 − T0, P = .049; Table 3).
Within-group differences were significant at all follow-up assessments (T1, T2, and T3) versus T0 (P = .005, .016, and .007, respectively) in the experimental group but not in the control group (P = .09, .44, and .37, respectively).
Moreover, the changes observed in the experimental group were greater than the recommended smallest detectable difference (SDD; >.76 logits) 40 in contrast to the control group.
Finally, no correlation was found between the changes scores of T1 and T0 versus level of HFCS (Pearson .526, P = .079).
Secondary Outcomes
Melbourne Assessment of Unilateral Upper Limb Function
Between-group differences in the changes were significant neither at T1 (P = .93) nor at T2 and T3 (T2 − T0, P = .84, T3 − T0, P = .79).
However, the SDD for both groups was smaller than the clinically significant level of 8.9% 41 at all time points.
ABILHAND-Kids
At T1 between-group differences in the changes were not significant (P = .15) and so also at T2 and T3 (T2 − T0, P = .14, T3 − T0, P = .12).
Discussion
In this RCT study, we proposed a 3-week paradigm of intensive UL action observation training in a group of children with hemiplegia. Our results indicate that this new rehabilitation approach is effective in improving UL activity performance in daily activities and that these effects tend to persist over time. In fact, immediately at the end of the planned training, between-group changes were statistically significant at AHA, the primary outcome measure. Moreover, within-group analysis indicates a significant improvement of the experimental group that continued in the follow-up assessments, whereas the control group remained unchanged. At ABILHAND-Kids no between-group differences were found. MUUL scores did not statistically change at between-group analysis and the within-group score changes did not reach the SDD, that is, the minimum change for a clinically significant change. Similar findings, that is, significant changes at MUUL scores, but below clinical significance, were recently reported in children with CP after a rehabilitation program based on AOT. 31
The main thrust for the UP-CAT was to detect the functional modifications induced by the OTI in motor-impaired children. OTI does make a real difference between the experimental and the control group, since both groups executed the same actions, but only the former was allowed to observe the actions before being required to perform them. The idea that this approach should elicit an improvement in children with motor impairments stems from the properties of the MNS, which has been shown to be very active during the imitation of previously observed actions.18,42 Based on this hypothesis, AOT rehabilitation programs have been tested in adult patients affected by various types of brain pathologies with results better than those obtained by a control intervention.22,23,25,43,44 The challenge of UP-CAT was to apply this new model as an option in children rehabilitation. Our intervention design was different from those proposed in adults.22,44 Our intervention included unimanual and bimanual actions to foster the use of the affected UL in a range of daily activities requiring both types of performances. Each video presented to the subjects lasted 3 minutes, a time sufficient to engage and maintain child’s attention. In addition, the actions were presented only from a first-person perspective to allow an immediate motor identification with the observed UL. 32 In fact, the presentation of actions from third person perspective would have required the children to perform an additional mental rotation, a skill that may not have been acquired yet 45 or may be impaired.46,47 Finally, videos showed actions belonging to the UL motor repertoire of the enrolled children, that is, the actions were graded according to the child’s baseline motor impairment, as indicated by the HFCS. The setting of all proposed exercises was the same for all children, but the type of required movement (ie, range of motion, reach trajectory, hand orientation, and opening, etc) was simplified for the more severely impaired participants.
The results obtained, as assessed with the AHA, show a change in the use of UL in daily activity but not in action kinematics, as measured by the MUUL, as found in the action observation programs in adults.22,23,44 This raises the issue of whether motor learning is more kinematic or goal-oriented in UCP children. A closer inspection of the video recordings taken during the exercise sessions seems to indicate that observation elicits in children a marked propensity to preserve the task proficiency, by selecting movements that guarantee the outcome goals, regardless of the kinematic resemblance with the observed model. We might speculate that children exploit the property of the MNS to activate goal representation15,48 -50 rather than its capacity to provide direct and detailed instructions on each movement subcomponent, thus emphasizing the execution of the action as a whole.
Interestingly, the AHA and ABILHAND-Kids measures provide different types of results. The AHA evaluates the spontaneous use of the assisting hand in semistructured play, whereas ABILHAND-KIDS provides a raw score for manual daily activities, not taking into account the involvement of a single hand (be it the affected one or not) or of both hands. A child could obtain the same score while executing an activity with one hand (healthy hand) or with both hands. In addition, AHA and not ABILHAND-KIDS scores reveal that a child improves the efficiency of his affected hand in bimanual activities, by enhancing the use of the assisting hand.
So far, there are no standard intervention protocols for UL management in children with CP. Rehabilitation programs vary in terms of duration, intensity of training and frequency. Furthermore, they are mostly based on changes induced by physiotherapy, orthotics, or medications, for example, for spasticity, aimed at modifying the expression of centrally generated motor schemas (“bottom-up” approach). None of these protocols has been proven to have an advantage over the others, besides often being time consuming and costly.
In this study we approached the issue of motor rehabilitation in children from a completely different perspective, as we aimed at directly inducing a functional modification of the cortical components underpinning the action organization, exploiting the peculiar features of the MNS. Among the major advantages of using this “top-down” model is the possibility of recruiting a very early ability of children, namely that of imitating by observation. 51
To the best of our knowledge there is only one study, recently published, that deals with AOT treatment, applied to a small group of children with various types of CP. 31 The results of MUUL showed a rapid gain immediately subsequent to the intervention, with a statistically significant difference between the experimental and control groups, but with a score gain that, as in our study, was much lower than the recommended SDD for this test, that is, 8.9%. 41 A gain lower than SDD value may not reflect a true change in function but rather a “chance” occurrence or an error in measurement and therefore, even if statistically significant, it does not meet the requirement for a real improvement. 41 Unfortunately, no other outcome measures or any longer term follow-up checks were provided. 31
A limitation of the present study is the small number of children enrolled, which was, however, adequate according to power analysis for our primary outcome. Moreover, the homogeneity of the sample, owing to the stringent inclusion criteria, besides a careful statistical treatment of the data provides a high reliability of the obtained results. Moreover, the type of intervention, tailored according to the severity of hand motor impairment, is clearly described in terms of video presentation, setting, object sequences, and therapist behavior. 32 The effectiveness of exercise tailoring is confirmed by the lack of significant correlation between functional changes and HFCS levels. It should also be noted that the task proposed to the children sustained their attention across all sessions. A further important implication of this study is the constant involvement of the families to prevent interruption of the rehabilitation program.
Conclusions
Action observation training appears to be effective in improving affected UL daily actions with effects that persist at 6 months. Our therapeutic protocol was inexpensive and time efficient and should be an easily reproducible rehabilitation program.
Footnotes
Acknowledgements
We acknowledge the contribution of physical therapists Elisa Sicola, Roberta Di Pietro, and Maria Cristina Filippi for the arrangement of exercises and of Valentina Burzi, Caterina Di Gioia, Francesca Foti, and Eliana Parente (all MDs) for videos collection and medical checks. We also thank Vincent Corsentino for reviewing the English of the article and Giuseppe Rossi for statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grants for this trial have been obtained from Emilia Romagna Region (Regional Research Project “New perspectives on rehabilitation in adults and children with motor disorders, autistic spectrum disorders, and in disorders of empathic communication: the role of mirror-neuron system”) and the Italian Ministry of Health (RC 2010-2011).