
Abstract
Background. Although functional task-specific training is a viable approach for upper extremity neurorehabilitation, its appropriateness for older populations is unclear. If task-specific training is to be prescribed to older adults, it must be efficacious and feasible, even in patients with cognitive decline due to advancing age. Objective. This cross-sectional study tested the efficacy and feasibility of upper extremity task-specific training in older adults, including those with lower cognitive scores. Methods. Fifty older adults (age 65-89 years) without any confounding neuromuscular impairment were randomly assigned to a training group or no-training group. The training group completed 3 days (dosage = 2250 repetitions) of a functional upper extremity motor task (simulated feeding) with their nondominant hand; the no-training group completed no form of training at all. Both groups’ task performance (measured as trial time) was tested at pre- and posttest, and the training group was retested 1 month later. Efficacy was determined by rate, amount, and retention of training-related improvement, and compared across levels of cognitive status. Feasibility was determined by participants’ tolerance of the prescribed training dose. Results. The training group was able to complete the training dose without adverse responses and showed a significant rate, amount, and retention of improvement compared with the no-training group. Cognitive status did not alter results, although participants with lower scores on the Montreal Cognitive Assessment were slower overall. Conclusions. Task-specific training may be appropriate for improving upper extremity function in older adults, yet future work in older patients with specific neurological conditions is needed.
Introduction
Functional task-specific training is emerging as a viable approach to upper extremity neurorehabilitation, particularly following stroke.1-4 During training, individuals repetitively practice tasks that are meaningful to daily life, such as manipulating a lock and key, opening and closing a door, or using an utensil.5-7 The clinical utility of this approach, however, depends on its ability to promote and capture changes in motor function across a wide age range of patients, including older adults, given the high percentage of adults over age 65 currently receiving therapy. 8
There are 2 important factors that must be considered when addressing issues related to neurorehabilitation in older adults. First, the “normal” aging process 9 may impede the course of standard neurorehabilitation. For example, older adults tend to learn new motor skills at a slower rate and to a lesser extent than young adults.10,11 Thus, older patients may require more training to induce a therapeutic effect (ie, efficacy). Furthermore, if more task-specific training is needed for older patients, then they must be able to tolerate these extended training sessions (ie, feasibility). Little research has, however, addressed the efficacy and feasibility of task-specific training in older adults.
Second, “abnormal” aging (eg, mild cognitive impairment, dementia) can be quite common in late adulthood, 12 which may further reduce an older patient’s ability to perform and/or learn a motor skill. 13 For example, gait disturbances become more apparent in older patients with mild cognitive impairment and Alzheimer’s disease when under dual-task conditions, but not under single-task conditions. 14 This interaction between cognition and movement has not, however, been systematically studied in the neurorehabilitation literature.
Therefore, the primary aim of this study was to examine the efficacy and feasibility of upper extremity task-specific training in a sample of older adults without confounding neuromuscular impairment. We hypothesized that adults age 65 years and older would show measurable learning effects (efficacy) in response to a high dose of training on a functional upper extremity motor task without adverse effects (feasibility). To address the question of “abnormal” aging and neurorehabilitation, a secondary aim of the study was to investigate the impact of cognitive impairment on training in these older adults. We hypothesized that lower cognitive status would reduce the efficacy and feasibility of the training dose, compared with normal cognitive status.
Methods
Participants
Fifty-five older adults (≥65 years old) were recruited from the local community and assisted-living facilities. Recruitment was based on individuals who contacted the lab with interest in participating as a result of approved postings throughout Cache County. Based on preliminary trial time data (8 participants), a priori power calculations indicated that at least 32 participants (16 training and 16 no-training) were needed to provide 80% power with an α level of .05. Exclusion criteria included one or more self-reported neurological conditions (eg, Parkinson’s disease, Huntington’s disease, stroke, or transient ischemic attack) or acute or chronic musculoskeletal conditions that could affect motor function. Based on these criteria, 5 participants were excluded from this study. Informed consent was obtained prior to study participation, and this study was approved by the university institutional review board.
Measures
Participants’ cognitive and sensorimotor functions were characterized prior to the task-specific training. Global cognitive status was measured with the Montreal Cognitive Assessment (MoCA 15 ), which is a reliable, easily administered, and brief cognitive screening test (max score = 30; “normal” score cutoff ≥ 26). Tactile sensation was measured with Semmes Weinstein monofilaments (Touch-Test, North Coast Medical, Inc, Gilroy, CA) at the distal end of the left and right index fingers only. Maximal grip strength of the nondominant hand was tested via hand dynamometer (Jamar, Sammons-Preston-Rolyan, Bolingbrook, IL16,17) as the average of 3 consecutive measurements. Hand dominance was determined using a modified Edinburgh Handedness Questionnaire. 18
The functional upper extremity motor task used in this study was a task that simulated feeding. As noted in our previous studies,19,20 this multijoint coordination task has been adapted from the simulated feeding subtest of a clinical assessment 21 that objectively assesses hand function for activities of daily living. This task required participants to spoon beans (kidney, raw) at a time from a center proximal “start” cup to 3 distal “target” cups as fast as possible. The cups (9.5 cm in diameter) were secured to a board (60.5 cm × 40.0 cm), with 3 target cups secured radially at 45°, 90°, and 135° around the start cup at a distance of 16 cm (Figure 1).22,23 The start cup was oriented along the participant’s midline and 15 cm in front of the seated participant.
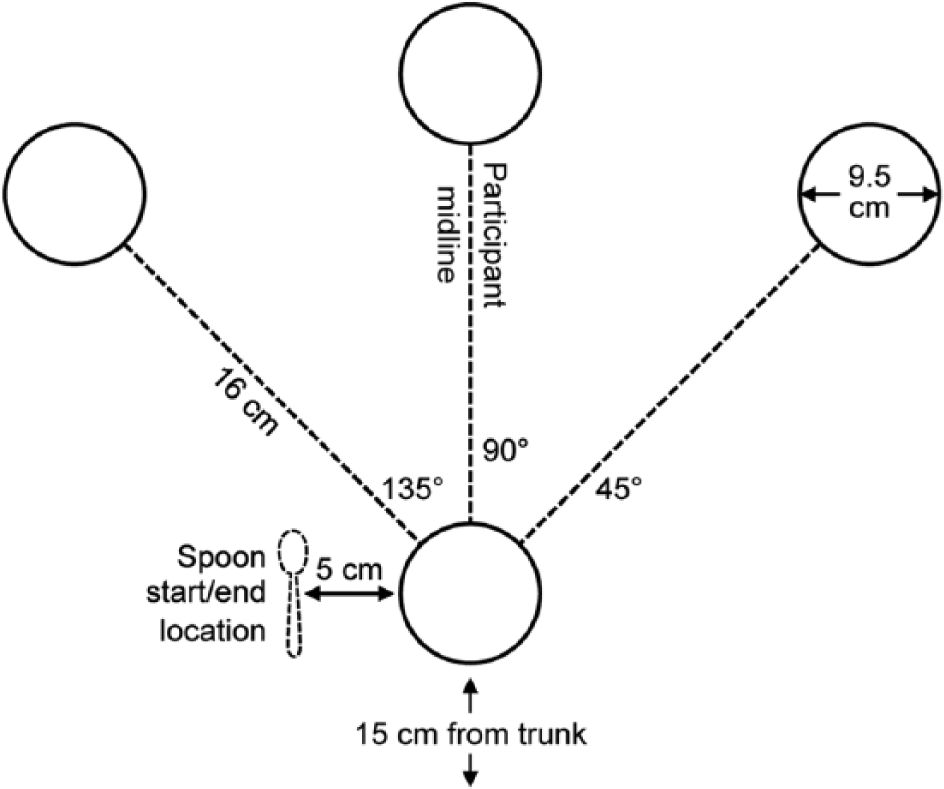
Top view of the simulated feeding task.
One repetition of the motor task consisted of spooning 2 beans at once from the start cup to a target cup with the nondominant hand,19,24 with one trial equaling 15 repetitions. During each trial, participants moved first to the ipsilateral target cup, next to the center target cup, and then to the contralateral cup, relative to the hand used (left vs right). They repeated this sequence 5 times to complete the trial. Each trial began when the participants picked up the spoon (plastic, 5.21 g) and ended when they returned the spoon to its start location (5 cm lateral to the start cup). The measure of performance for each trial was the time taken to complete the 15 repetitions (ie, “trial time”), with faster times indicating better performance. All trials were timed to the nearest 100th of a second via stopwatch. In contrast to some experimental or therapeutic approaches, 25 participants were given no explicit feedback (ie, knowledge of performance or results) after each trial, and they were not encouraged to adopt any specified pattern of upper extremity kinematics during training.
Experimental Protocol
Task-specific training on the functional motor task was completed over 3 consecutive days (Figure 2). All data were collected in an individual setting (rather than group) within the Motor Rehabilitation and Learning Laboratory at Utah State University. Each assessment described above, including the MoCA, was completed on Day 1, prior to any motor task performance. Following the pretest measurement of “baseline” nondominant hand motor performance, participants were randomly assigned to a training group or no-training group via simple randomization 26 to avoid bias in this open study. Overall, the dose of task-specific training for the training group was 2250 total repetitions (15 repetitions/trial × 50 trials/day × 3 days). This dose has been shown previously to be feasible and efficacious for adults with chronic mild to moderate hemiparesis after stroke.6,20,27,28
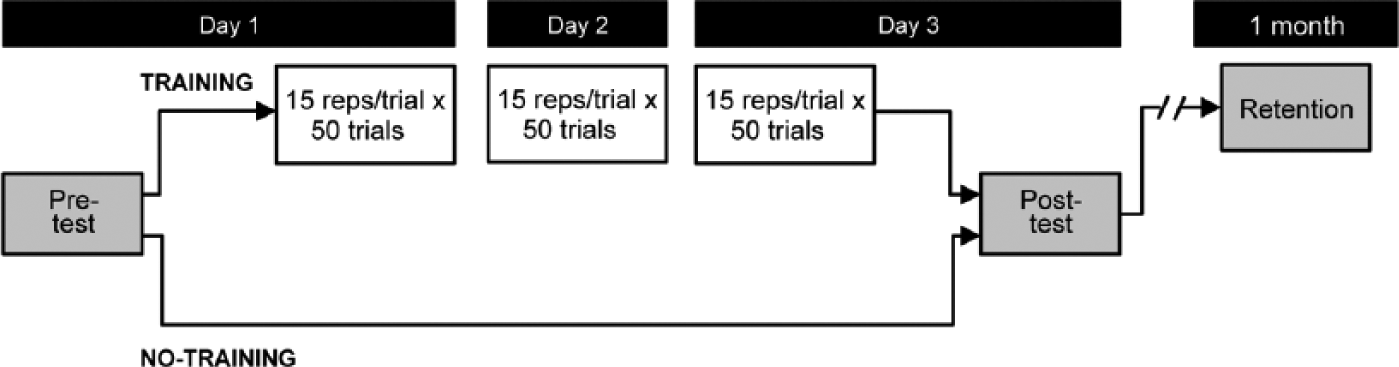
Experimental schedule for training and no-training groups.
Dependent Variables
Feasibility was determined by the participants’ completion (and therefore “tolerance”) of the prescribed dose of task-specific training without adverse effects, such as fatigue and boredom. Efficacy was evaluated by the rate, amount, and retention of improvement in task performance. To measure the rate of improvement in response to task-specific training, we generated performance curves by plotting trial time (measured in seconds) as a function of trial number (trial 1-150), and modeled the data using an exponential decay function:

where a is the final trial time value that the exponential decay function approaches (ie, asymptote), b is the scale of the learning from the first trial time to the value a, x is the trial number, and c is the rate at which learning occurs (ie, the decay constant). In this model, the exponential decay constant, 1/c, is the number of trials needed to obtain (1 − e−1) or 63.2% of the final learned amount (or asymptote, a). This approach has been used previously to quantify upper extremity motor adaptation in healthy and clinical populations.29-31 Thus, we used the value c as the rate of improvement in this study. Given the design of this study, no data on rate of trial-by-trial improvement were collected in the no-training group, as they did not complete any training.
Immediately following training on Day 3, participants in the training group completed an additional trial of the functional motor task to establish their posttest performance (Figure 2). Posttest evaluation occurred within 5 minutes of the last training trial (eg, a short break was given based on participant request). Participants in the no-training group were also tested on Day 3, although they did not train in between their pre- and posttest sessions. The difference in pre- and posttest trial times for the training and no-training groups was used to measure the amount of improvement in response to training (see section Statistical Analyses), and to assess whether test–retest alone induced any motor learning. Grip strength was also measured again in both the training and no-training groups at posttest to ensure that any improvements in motor performance were due to task-specific training rather than changes in strength.
To measure the retention of improvement, participants in the training group were then retested 1 month (30-35 days) after Day 3 on 2 trials (15 repetitions each) of the functional motor task. As with improvement rate, no retention data were collected in the no-training group, given that preliminary data and previous studies 19 showed no short-term change in performance when no training has occurred. Each training group participant’s retention at 1 month was expressed as the average of his/her 2 trial times to account for performance stability and washout (as recommended in earlier studies32,33). The difference in pretest and retention trial times for the training groups was used to quantify retention, as was any difference between posttest and retention.
Efficacy was further tested by comparing the rate, amount, and retention of improvement based on participant’s global cognitive status. Participants were assigned post hoc to 1 of 2 MoCA categories, based on the clinical cutoff score of 26. 15 Although MoCA scores can be analyzed as a continuous measure in cases of large sample sizes and broad score ranges (0-30), current convention treats MoCA performance as a dichotomous variable,34-36 particularly in cross-sectional studies. Thus, participants were categorized as <26 or ≥26, and we operationally defined “cognitive impairment” as a score <26 for purposes of this study. To account for any potential relationship between cognitive impairment and age, we calculated a Pearson product–moment correlation coefficient (r2) across participants using least squares regression and determined whether there was a significant linear relationship within our sample between MoCA score and age. Since the “oldest old” (85+ years 37 ) typically have (a) lower cognitive scores and (b) slower movements (ie, more bradykinetic) than the “young old” (65-74 years 38 ), we used this analysis to ensure that any differences in trial times associated with MoCA scores were not simply the result of the oldest participants moving the slowest.
Statistical Analyses
The SAS statistical software program JMP 10.0 (SAS Institute Inc, Cary, NC) was used for all statistical analysis (α = .05). T tests and χ2 tests were used to determine whether the training and no-training groups were matched for age, sex, general cognitive status, tactile sensation, and pretest nondominant hand grip strength.
To examine the efficacy of training, we first calculated the rate of improvement for each participant in the training group and used a 95% confidence interval to test whether the average rate was significantly different from zero. This determined whether participants in the training group had a significant rate of improvement. To test whether cognitive impairment affected the rate of improvement due to training, we compared rates between MoCA categories (<26 vs ≥26) using an independent T test.
A second test of efficacy compared of the amount of improvement in trial time between sessions (pretest vs posttest) based on group (training vs no-training) and MoCA category (<26 vs ≥26) using a 2 × 2 × 2 repeated-measures analysis of variance (ANOVA). Session was a within-subject factor, while group and MoCA category were between-subject factors. This analysis further tested whether cognitive impairment affected the amount of improvement due to training.
Our third test of efficacy compared the retention of improvement at 1 month to performance at earlier sessions (pretest and posttest) based on MoCA category using a 3 × 2 repeated-measures ANOVA. This final analysis also tested whether cognitive impairment affected the retention of improvement due to training. In all the aforementioned analyses, post hoc analyses were conducted when warranted using the Tukey–Kramer Honestly Significant Difference (HSD) test.
Results
Group Characteristics
Table 1 summarizes the characteristics for the training (n = 23) and no-training (n = 27) groups. The groups were not significantly different on global cognition (P = .52), age (P = .58), sex (P = .20), sensation level (P = .47), nondominant grip strength at pretest (P = .83) or at posttest (P = .83, not shown). Table 1 also shows that we were able to recruit evenly across a wide range of ages (65-89 years). Regression analysis indicated a weak relationship between MoCA score and age (r2 = .25).
Group Characteristics.
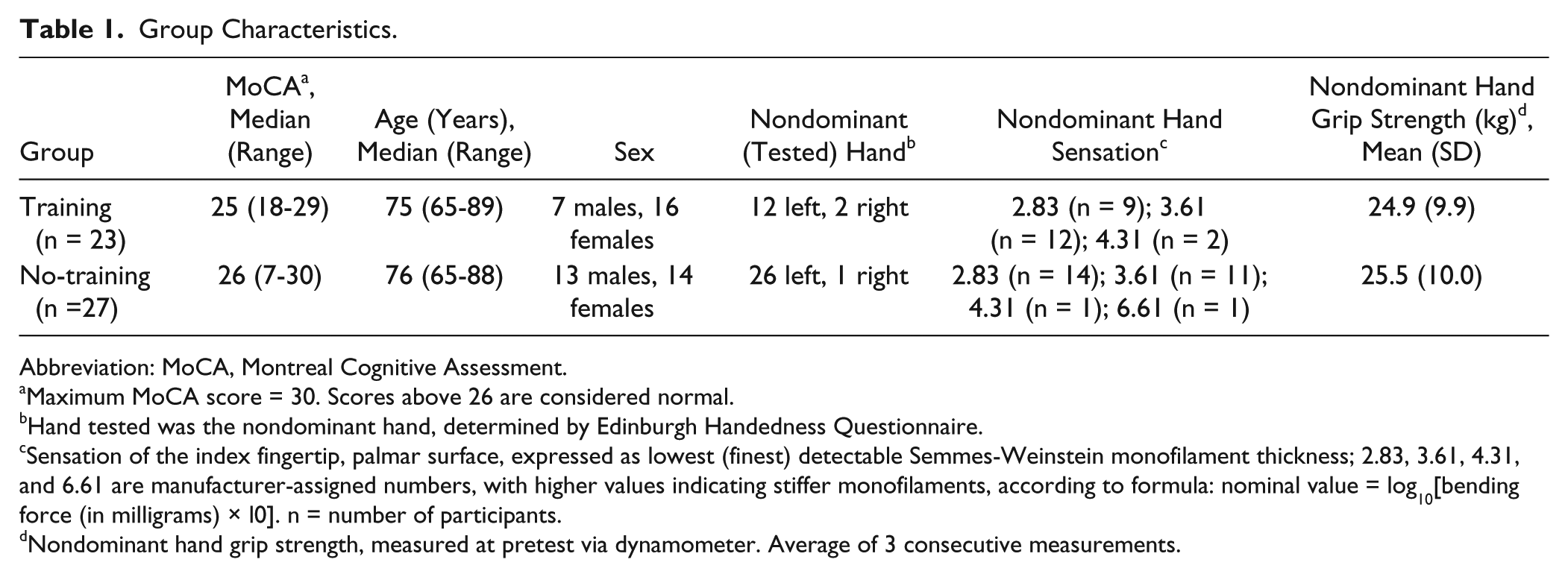
Abbreviation: MoCA, Montreal Cognitive Assessment.
Maximum MoCA score = 30. Scores above 26 are considered normal.
Hand tested was the nondominant hand, determined by Edinburgh Handedness Questionnaire.
Sensation of the index fingertip, palmar surface, expressed as lowest (finest) detectable Semmes-Weinstein monofilament thickness; 2.83, 3.61, 4.31, and 6.61 are manufacturer-assigned numbers, with higher values indicating stiffer monofilaments, according to formula: nominal value = log10[bending force (in milligrams) × l0]. n = number of participants.
Nondominant hand grip strength, measured at pretest via dynamometer. Average of 3 consecutive measurements.
Efficacy of Training
Figure 3 illustrates the rate, amount, and retention of improvement due to training. The rate of improvement can be seen in the mean performance curve for the training group (Figure 3A). In addition, the 95% confidence interval ranged from 0.030 to 0.088, indicating that the learning rates were significantly different from zero. The mean rate was such that maximal learning effects were achieved after ~27 trials (or 405 repetitions), although some participants learned much faster (eg, 101 repetitions) and some much slower (eg, 2483 repetitions). Figure 3B shows the amount of improvement in trial time for both the training and no-training groups from pretest to posttest. Repeated-measures ANOVA indicated a significant interaction between session (pretest vs posttest) and group (training vs no-training) for trial time (F1,46 = 13.94, P < .001). Post hoc analyses revealed that mean trial time for the training group was significantly lower (ie, faster) at posttest compared with pretest (P < .001), whereas the no-training group showed no significant change from pretest to posttest (P = .87). Moreover, mean trial times at pretest were similar between the training and no-training groups (P = .99), indicating that both groups’ baseline performances were comparable at the start of the study. The lack of change in grip strength from pretest to posttest (see section Group Characteristics) also suggests that the training group’s improvements were not attributable to increased strength due to training.
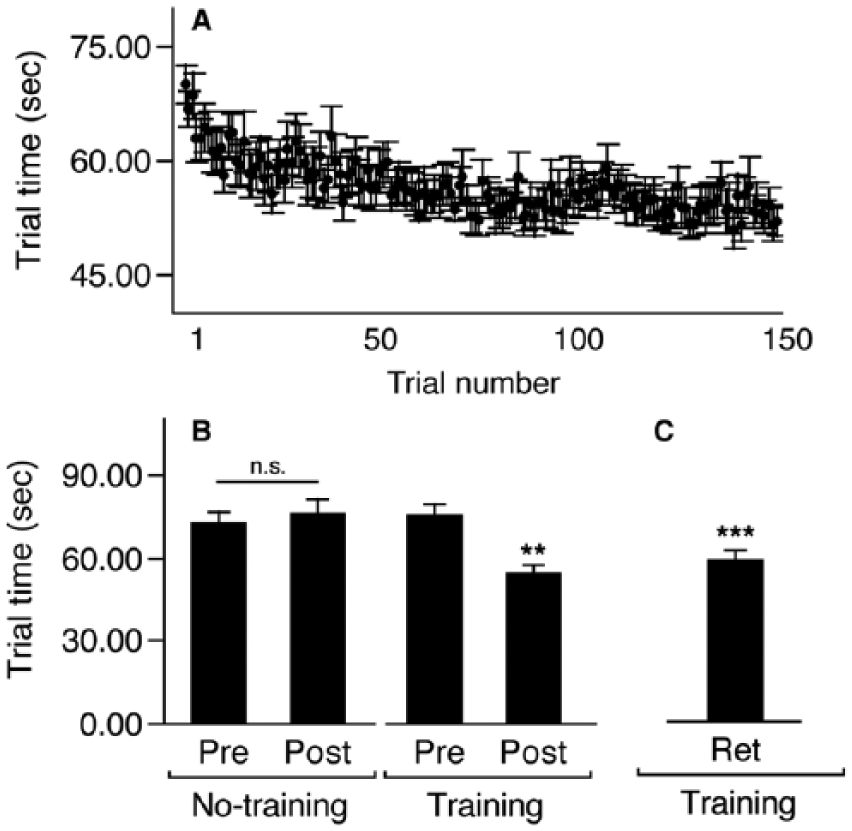
(A) Mean trial times for the training group over the course of 150 training trials (50 trials/day × 3 days). (B) Mean trial time at pretest and posttest for the no-training and training groups. Posttest trial times were significantly lower in the training group only (**P < .01; n.s. = non-significant). (C) Mean trial time at retention (1-month follow-up) for the training group only. Retention trial time was significantly lower than pretest (***P < .0001), but not significantly different from posttest.
In addition to significant rates and amounts of improvement, Figure 3C shows mean trial time for participants in the training group 1 month later (“retention”). Not only did trial times improve from pretest to posttest (Figure 3B), but the improvements were also retained 1 month later, as shown by the main effect of session (F2,21 = 23.17, P < .0001) on trial time. Trial times at 1 month after training were still significantly lower (ie, faster) compared to pretest (P < .0001), and were not significantly different from posttest (P = .41).
Feasibility of Training
All eligible participants completed the study (n = 50). However, 2 participants in the training group (8.7%) were unable to complete the entire dose over 3 days due to self-reported fatigue or lack of interest on Day 1 (ie, asked to stop and complete remaining trials on a consecutive, fourth training day). Four participants in the training group (17.4%) also verbally expressed, impromptu at the end of Day 3, that they had experienced boredom at some point. No other adverse effects were reported in this study in either the training or no-training groups. Thus, the training dose evaluated in this study was tolerated by a range of older adults.
Relationship Between Cognitive Impairment and Efficacy/Feasibility
While Figure 3 shows the overall comparison between the training and no-training groups, it does not differentiate between levels of cognitive status. Rather, Figure 4 shows comparisons within groups between participants with and without cognitive impairment. Although we hypothesized reduced efficacy/feasibility in those with lower cognitive status, our data collectively showed no effect of MoCA category on any measure. As illustrated by the performance curves in Figure 4A, there was no significant difference in the improvement rates between participants with MoCA scores <26 (mean ± SE =.051 ± .02) and ≥26 (.070 ± .02), P = .62. Thus, regardless of MoCA category, participants in the training group learned the functional motor task at comparable rates.
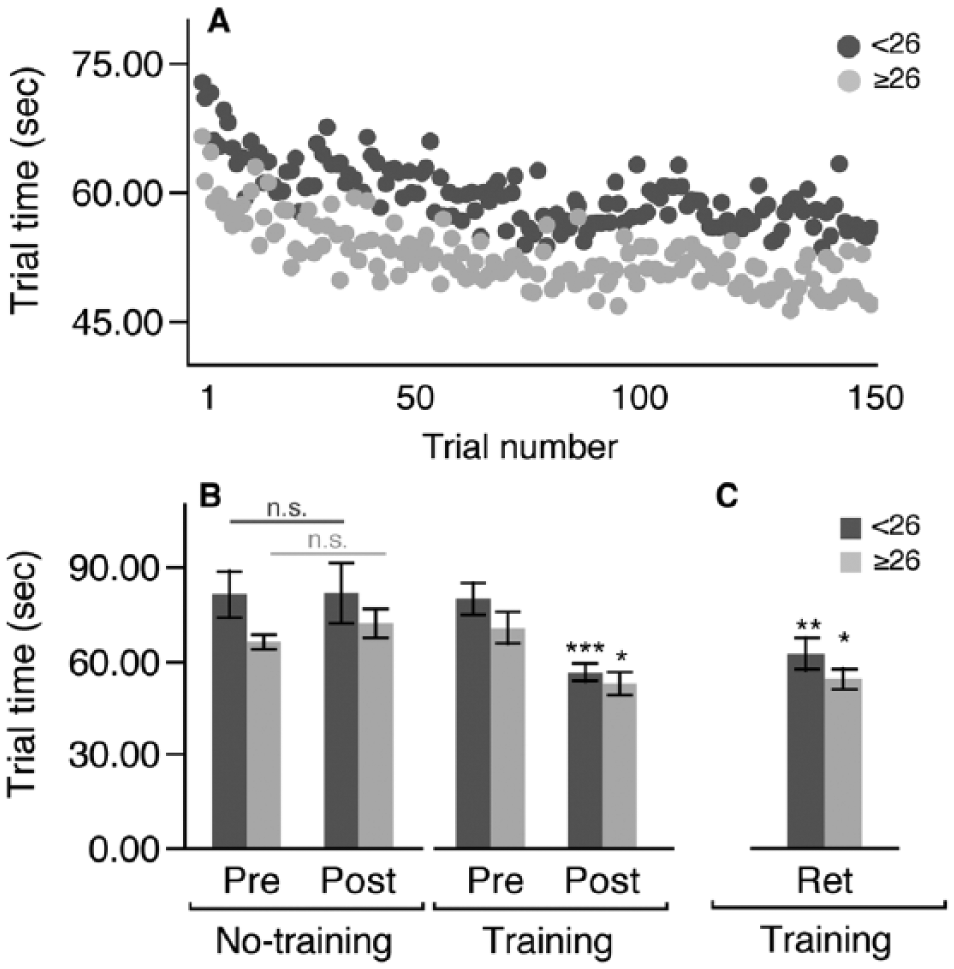
(A) Mean trial times over the course of 150 training trials within each Montreal Cognitive Assessment (MoCA) category. Error bars have been omitted for visual clarity. (B) Mean trial time at pretest and posttest for the no-training and training groups. Posttest trial times were significantly lower in the training group only in both MoCA categories (*P < .05; ***P < .0001; n.s. = nonsignificant). (C) Mean trial time at retention (1-month follow-up) for the training group only. Retention trial time was significantly lower than pretest in both MoCA categories (*P < .05; **P < .01), but not significantly different from posttest.
MoCA category also did not affect the amount of improvement due to training (Figure 4B). Repeated-measures ANOVA indicated (a) no significant 3-way interaction between session (pretest vs posttest), group (training vs no-training), and MoCA (<26 vs ≥26) on trial time (F1,46 = 0.002, P = .96) and (b) no significant 2-way interactions between group and MoCA category (F1,46 = 0.46, P = .50) or session and MoCA category (F1,46 = 0.85, P = .36). There was, however, a significant main effect of MoCA (F1,46 = 4.60, P < .05) on trial time. Thus, regardless of group or session, trial times were higher (ie, slower) for participants with MoCA scores below the cutoff. This bradykinetic effect is also captured in Figure 4A, such that the performance curve for the <26 category is shifted upward relative to that for the ≥26 category.
Figure 4C further shows the lack of effect of MoCA category on training efficacy. When comparing retention of improvement, there was no significant interaction between session and MoCA category (F2,21 = 0.59, P = .55) or a main effect of MoCA category (F1,21 = 2.56, P = .13) on trial time. Thus, regardless of MoCA category, participants retained their training-related improvements in motor performance one month after training.
Although 91% of the participants in this study tolerated the dose of training over the 3-day administration period (see section Group Characteristics), the 2 participants in the training group who required an additional fourth day due to fatigue on Day 1 had MoCA scores below 26. They nevertheless completed the full training dose, and all other participants with scores <26 tolerated the 3-day training period, suggesting that the training’s feasibility is not affected by cognitive impairment.
Discussion
The purpose of this study was to test the efficacy and feasibility of functional upper extremity task-specific training for adults age 65 years or older without any confounding neuromuscular impairment. Results showed that a high dose of training on a functional motor task (2250 repetitions of simulated feeding) was efficacious, yielding significant learning effects that were measured as the rate, amount, and retention of improvement, and was feasible, based on their completion and tolerance, without adverse effects. Moreover, participants’ cognitive status and strength did not affect these measures or their ability to tolerate the dose. Thus, task-specific training may be appropriate for upper extremity neurorehabilitation in older populations, including the oldest old and those with some degree of cognitive impairment.
An important finding from this study is that the improvements in trial time associated with a set dose of task-specific training were retained 1 month later. In prior studies, older adults have been shown to partially retain experience-dependent adaptations for 1 to 7 days after upper extremity training.39-41 Participants in those studies were required to specifically adapt their motor output in order to reduce reaching errors induced by systematic, computer-driven perturbations in visual feedback (ie, visuomotor adaptation). Results from the current study not only extend the potential timeframe of retention for older adults (up to 1 month) but also broadens the types of tasks that can be used to probe for retention. Our functional motor task allowed participants to manipulate a physical object (the spoon) using whichever grip type they wanted, and to transport the beans using whichever upper extremity movement pattern they wanted in order to successfully complete a trial (ie, a “discovery learning” approach 42 ). This approach reflects how a patient may relearn a functional motor skill in real-world settings, either in therapy or at home, and may be useful for future investigations of motor learning that are clinically relevant.
The learning effects observed in this study, namely, the rate, amount, and retention, may be partly due to the relatively high dose of functional upper extremity task-specific training (2250 repetitions over 3 days) that was administered in this study, compared with standard clinical rehabilitative practice.43,44 Recent research has started to quantify the dose–response relationship for upper extremity neurorehabilitation treatments very similar to the approach taken in this study,45,46 and has documented across a number of clinical trials and controlled experiments that patient groups who receive more therapy improve beyond those who receive less. Those studies benchmark an important step in providing an evidence-based approach to physical rehabilitation, whereby clinicians can and should prescribe doses of therapy (defined as the amount of practice/repetitions rather than the time spent in therapy; see Lang et al 44 for rationale) based on a set of standard criteria. Our results also provide evidence that older adults, including the oldest-old and those with some level of cognitive impairment, can tolerate high doses of upper extremity task-specific training that have been feasible and effective for other neurologic populations.6,28
Although the older adults in this study appeared to tolerate the tested dose of training, they did not have any known conditions or diseases that are often associated with sensorimotor or neuromuscular deficits (eg, stroke, Parkinson’s disease). While this sample allowed us to test for “pure” age-related effects in the absence of confounding comorbidities, these results are limited and should be interpreted with caution. Other limitations to this study include the short duration of training (3 days) and the lack of current knowledge regarding how improvements on the feeding task are related to other functional or clinical outcomes (eg, Fugl-Meyer, activities of daily living, etc). We also acknowledge that the primary “outcome” measure and the training protocol were identical in this study; this was necessary, however, to quantify efficacy in the context of motor learning. 47 Thus, future studies are needed to address (a) the expected outcomes of older patients with specific neurological conditions in response to task-specific training as an intervention; (b) the selection, prescription, and administration of tasks by clinicians within therapy; and (c) the generalization of training to other tasks. Ongoing studies from this laboratory are in fact investigating the degree to which the learning effects shown here are transferrable in older adults, relative to younger participants with and without a history of stroke.19,20,24
While global cognitive status did not appear to affect the extent to which participants in this study learned (or retained) the functional motor task, the lack of interaction between MoCA category and the other factors in this study does not preclude the role of cognitive factors in neurorehabilitation. In fact, our finding that participants with lower MoCA scores had slower movements overall suggests that their bradykinesia may be in part related to cognitive factors,48,49 and not simply an effect of age (ie, the oldest participants having the longest trial times), given the weak relationship between MoCA score and age in our sample (noted in section Group Characteristics). Nevertheless, the MoCA (a) is a gross measure of global cognition, (b) does not thoroughly assess visuospatial abilities or working memory, and (c) does not at all test aspects of cognition that are highly related to motor learning, specifically implicit memory.50,51 Thus, its ability to detect or predict deficits in motor learning is minimal. Our data showed, however, that some participants in this study learned the task faster (ie, in fewer trials) than others. Although experimental brain imaging techniques are able to correlate specific neural features with rates of motor adaptation, 52 there is a current lack of clinical neuropsychological tools that capture implicit memory function directly. Thus, one’s rate of motor learning may, in fact, be useful in quantifying one’s implicit memory. Furthermore, it may potentially serve as a clinical predictor of one’s success in therapy. 53 More work is needed to establish the extent to which measures of motor learning (such as rate, amount, etc) are not only related to specific cognitive deficits that may be present in neurological populations but can also indicate neurorehabilitative outcomes in these populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Utah State University Office of Research and Graduate Studies (RC #28037) and the Marriner S. Eccles Foundation.