
Abstract
Background. Although task-specific training is emerging as a viable approach for recovering motor function after stroke, there is little evidence for whether the effects of such training transfer to other functional motor tasks not directly practiced in therapy. Objective. The purpose of the current study was to test whether training on one motor task in individuals with chronic hemiparesis poststroke would transfer to untrained tasks that were either spatiotemporally similar or different. Methods. In all, 11 participants with chronic mild to moderate hemiparesis following stroke completed 5 days of supervised massed practice of a feeding task with their affected side. Performance on the feeding task, along with 2 other untrained functional upper-extremity motor tasks (sorting, dressing) was assessed before and after training. Results. Performance of all 3 tasks improved significantly after training exclusively on 1 motor task. The amount of improvement in the untrained tasks was comparable and was not dependent on the degree of similarity to the trained task. Conclusions. Because the number and type of tasks that can be practiced are often limited within standard stroke rehabilitation, results from this study will be useful for designing task-specific training plans to maximize therapy benefits.
Keywords
Introduction
Task-specific training is emerging as a viable neurorehabilitative approach for improving motor function after stroke.1,2 It is based on the fundamental principle that repeated practice is the best way to learn a particular task. 3 Unfortunately, an individual often loses the ability to perform a number of tasks after stroke, many more so than can be practiced feasibly within the current rehabilitation setting.4,5 It is assumed that the effects of training on 1 task in therapy will transfer to other tasks that have not undergone training, yet very little is known about whether this is true. Transfer, in this sense, is the gain in the proficiency of 1 motor task as a result of practice on some other motor task. 6 To what degree does motor training transfer after task-specific training? Given that “there is currently a dearth of evidence on which to construct rehabilitation interventions that are accurately targeted, properly framed, and credibly measured”7(p2033), it is critical to understand (1) if task-specific training transfers and (2) how much transfer occurs.
One challenge in addressing these questions experimentally is the substantial differences between functional upper-extremity motor tasks that may be practiced within task-specific training. For example, an individual may repeatedly practice sorting coins with the affected limb. 8 This task would be markedly different from other tasks such as feeding or dressing oneself, not only in terms of movement goals but also in terms of spatiotemporal characteristics of the movements. 9 Previous studies in neurologically intact individuals have used point-to-point reaching paradigms to demonstrate how the effects of motor training can transfer, but the amount of transfer is incomplete even when the context is similar to the training condition.10,11 Such results from motor tasks bearing little resemblance to real-world actions suggest that little to no transfer of training would occur between more naturalistic upper-extremity actions involving the entire upper extremity. Naturalistic actions are purposeful and multistep,12-15 often recruiting many degrees of freedom and differing substantially in how “successful” performance is defined. We recently found, however, that performance on 1 novel yet naturalistic motor task (simulated dressing) improved significantly following a single session of training on another task that was spatiotemporally quite different (simulated feeding). 16 Performance on a novel, nonmotor cognitive task (associative recognition) did not, however, improve following training on the feeding task, indicating that the transfer effects were specific to the motor domain and not a result of changes in overall arousal. Moreover, no improvements on the dressing task were observed in individuals who did not train on the feeding task, indicating that the transfer effects were experience dependent. By establishing this proof of principle in neurologically intact individuals, we now address whether motor training can transfer in individuals with chronic poststroke hemiparesis and whether the amount of transfer depends on the degree of similarity between the trained and untrained tasks.
The purpose of this study was to test whether 5 consecutive days of training on 1 motor task would transfer to 2 other untrained tasks in individuals with chronic hemiparesis poststroke. All tasks were performed with the affected upper extremity. We hypothesized that training on the feeding task would improve motor performance not only on that task but also on 2 tasks that were not trained (sorting and dressing). We also hypothesized that because the sorting task was spatiotemporally similar to the feeding task, the amount of transfer would be greater in the sorting task than in the dressing task. In this study, the amount of transfer was measured as the degree of improvement from before to after training on the feeding task. Results from this study have direct and immediate implications for maximizing the benefits of task-specific training after stroke by providing evidence that can be used to guide clinicians’ selection of which tasks to practice.
Methods
Participants
A total of 11 adults with chronic upper-extremity hemiparesis following stroke participated in this study. Of these participants, 9 were right-handed, based on self-report; 5 participants had right-side hemiparesis and 6 had left-side hemiparesis. Participants were recruited from the Brain Recovery Core Stroke Registry at Washington University in St Louis based on the presence of unilateral hemiparesis. Potential stroke participants were included if they (1) had a diagnosis of ischemic or hemorrhagic stroke by a stroke neurologist; (2) had persistent hemiparesis with a score of 1 to 3 on the Motor Arm item of the National Institutes of Health Stroke Scale (NIHSS), indicating mild to moderate impairment; and (3) had the ability to follow 2-step commands. Potential participants were excluded from the study if they (1) had severe hemispatial neglect as evidenced by a score of 2 on the Extinction and Inattention items of the NIHSS or (2) were unable to give informed consent. This study was approved by the Washington University Human Research Protection Office and was conducted in compliance with the Helsinki Declaration. All participants provided informed consent prior to beginning the study.
Several clinical tests were used to characterize participants. Maximum grip strength (in kg) of the affected and unaffected sides was measured using a dynamometer (Jamar, Sammons-Preston-Rolyan, Bolingbrook, Illinois)17,18 before and after training. The Action Research Arm Test (ARAT) was used to quantify upper-extremity function.19-24 An ARAT score of 57 indicates normal function. Spasticity of the elbow flexors was assessed on the affected side using the Modified Ashworth Scale. 25 Cutaneous sensation was measured with Semmes Weinstein monofilaments (Touch-Test, North Coast Medical, Inc, Gilroy, California) applied to the palmar surface on the distal phalange of the index finger. The Trail-Making Test B was used to assess cognitive function, specifically switching attention.26,27 Results from these tests are shown in Table 1, along with other descriptive characteristics. Time poststroke ranged from 12 to 156 months, and severity of sensorimotor impairment and functional limitation ranged from mild to moderate, as shown by measures of strength and sensation and scores on the ARAT.
Participant Characteristics. a
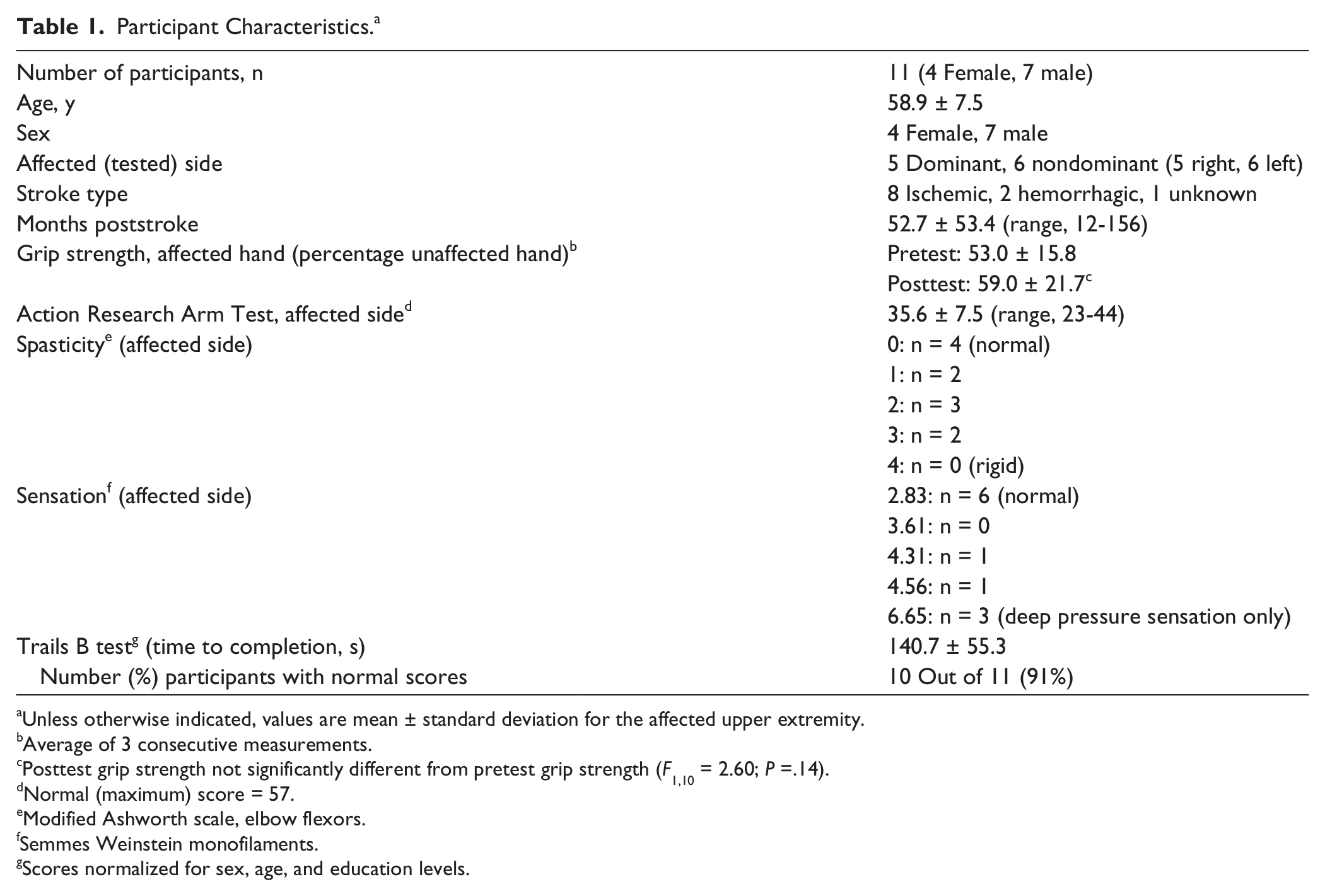
Unless otherwise indicated, values are mean ± standard deviation for the affected upper extremity.
Average of 3 consecutive measurements.
Posttest grip strength not significantly different from pretest grip strength (F1,10 = 2.60; P =.14).
Normal (maximum) score = 57.
Modified Ashworth scale, elbow flexors.
Semmes Weinstein monofilaments.
Scores normalized for sex, age, and education levels.
Experimental Design
General procedure
This study used a mixed-model design to evaluate the transfer of training from 1 motor task to 2 other untrained motor tasks. 16 For all tasks, participants sat in a chair behind a table (76 cm × 51 cm) that was adjusted to be as low as possible without contacting the thighs. All motor tasks were completed with the affected upper extremity and were graded according to motor ability on an individual basis.
Each participant completed the study over the course of 5 days (Figure 1). Prior to training on day 1, participants completed one 30-s trial of all 3 tasks to establish their pretest motor performance with their affected upper extremity. They then completed 50 more trials of the trained task with their affected upper extremity in a massed practice training session. On days 2 to 5, participants received additional training only on that task (50 trials/d), resulting in 250 total trials over the course of 5 days. Immediately following the training session on day 5, participants completed one 30-s trial of all 3 tasks to determine their posttest motor performance. In both the pretest and posttest sessions, the order of the motor tasks was randomized using the random permutation function in MATLAB (MathWorks, Inc, Natick, Massachusetts) for each participant.

Diagram of training schedule across 5 days: training sessions comprised 50 trials, lasting 30 s each, of only 1 motor task. Gray shading indicates sessions (pretest and posttest) in which all motor tasks were completed, under both single- and dual-task conditions. Order of trials and conditions within each session was randomized.
Trained motor task: feeding
The trained motor task was a simulated feeding task that required spooning beans from one cup to another (Figure 2, left panel). At the start of each feeding trial, participants picked up a metal spoon with their most affected hand and spooned 1 bean at a time from one cup away from their body to another cup. The first cup contained 70 beans that were distributed evenly across the bottom. The cups were secured to a wooden board, which was centered in line with the participant’s shoulder. Participants spooned as many beans as possible per trial in the target direction, and the total number of beans in the target cup was recorded after each trial. Only 1 bean was counted per repetition if >1 bean was transferred at a time. That is, a successful repetition in the feeding task was one in which at least 1 bean was transferred. Participants were given no information about their performance strategy during training and were only given verbal feedback about the number of successful repetitions after each trial. Thus, a “discovery learning approach” was taken in this study,28-30 in which participants adapt their movement strategies based on trial and error over time. The measure of performance for each feeding trial was the number of successful repetitions. Prior to the experiment, participants were tested on whether they could spoon at least 2 beans (2 successful repetitions) within 30 s. Only 4 of the 11 participants did so. For the remaining 7 participants, a piece of cylindrical foam was used to cover the spoon’s handle (Figure 2, left panel). This graded the feeding task according to the individual’s ability.
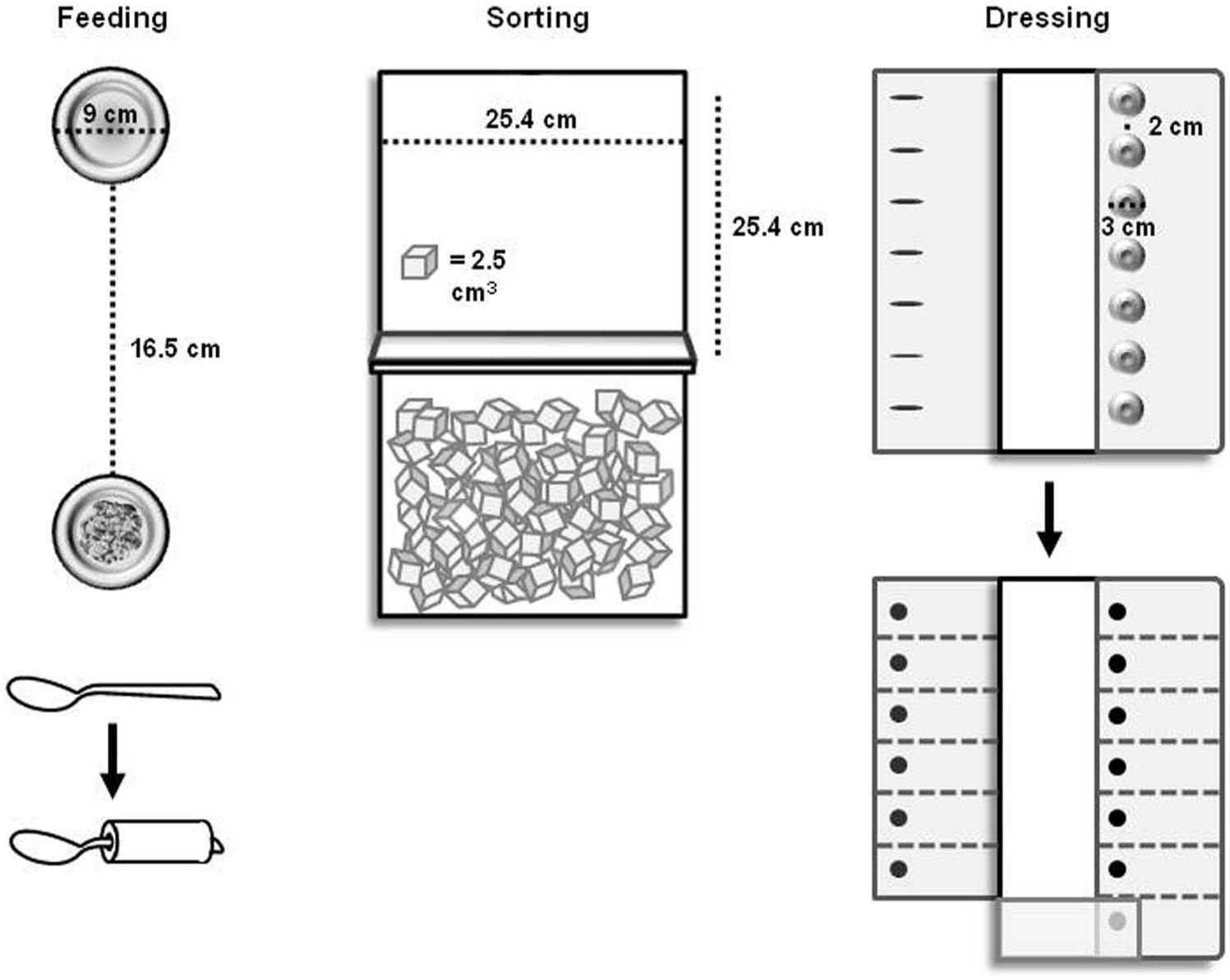
Motor tasks: top view of the trained task (feeding) and untrained tasks (sorting and dressing). Adapted versions of the feeding task and dressing task are shown beneath each task, respectively, as indicated by arrows.
Untrained motor tasks: sorting and dressing
Participants were also tested on 2 other motor tasks before and after training: sorting and dressing. They did not train on either task. The sorting task required participants to transport blocks 1 by 1 from one box to another box away from their body (Figure 2, middle panel). The dimensions of each box were 8.5 × 25.4 × 24.4 cm3. The boxes were separated by a partition that was 18 cm high and were centered in line with the participant’s shoulder. Participants transported as many blocks as possible per trial with their most affected hand. The measure of performance for each sorting trial was the number of blocks transported.
The apparatus used in this task was the Box and Blocks Test. 31 In its standardized clinical use, the boxes are oriented side by side, requiring individuals to transport blocks in the mediolateral direction across the midline. In this study, however, the boxes were oriented such that participants were required to transport blocks in the anteroposterior direction in the hemispace ipsilateral to the affected side. This configuration required participants to move in a direction similar to the feeding task.
The second untrained motor task was a dressing task in which buttons were fastened sequentially. At the start of each dressing trial, participants began buttoning the bottom of 7 buttons (3 cm in diameter) that were sewn 2 cm apart to plain-weave cotton fabric (Figure 2, right panel). Both fabric pieces were secured to a wooden board, with the placket centered in line with the participant’s shoulder. The button side of the fabric was folded onto the board, whereas the buttonhole side of the fabric was unfolded onto the table prior to each trial, lateral to the affected upper extremity. Participants fastened as many consecutive buttons as possible per trial with their affected hand. If all 7 buttons were fastened in less than 30 s, participants were instructed to completely unfasten each button in the reverse order until the trial ended. The measure of performance for each dressing trial was the number of buttons fastened/unfastened.
Prior to the experiment, participants were tested on whether they could fasten a single button within 30 s. Only 2 of the 11 participants did so. The remaining 9 participants were tested on an adapted dressing task in which medium-stress dot-on-dot Velcro was fastened rather than buttons. This enabled the dressing task to be graded down according to the individual’s ability.
Task similarity
Movement kinematics were similar between the feeding task and the sorting task, whereas kinematics in the dressing task were different. To illustrate the similarities/differences between tasks, shoulder and elbow flexion angles during individual trials of each motor task in a single participant are provided (Figure 3A); more positive values indicate extension direction. Relative to the feeding task (black line), the sorting task (dashed line) is spatiotemporally similar, given the repetitive and consistent shoulder and elbow flexion/extension patterns as the hand moves back and forth between the cups or boxes in the anterior-posterior direction, respectively (Figure 3B). The dressing task (gray line) is different, seen both in its joint angle patterns (Figure 3A) and hand paths (Figure 3B) because this participant fastened buttons over the course of the 30-s trial. Thus, the sorting task was considered more similar to the feeding task than the dressing task was. All 3 motor tasks, however, were selected because they simulate activities of daily living32-37 that are relevant and meaningful to one’s ability for self-care.38,39
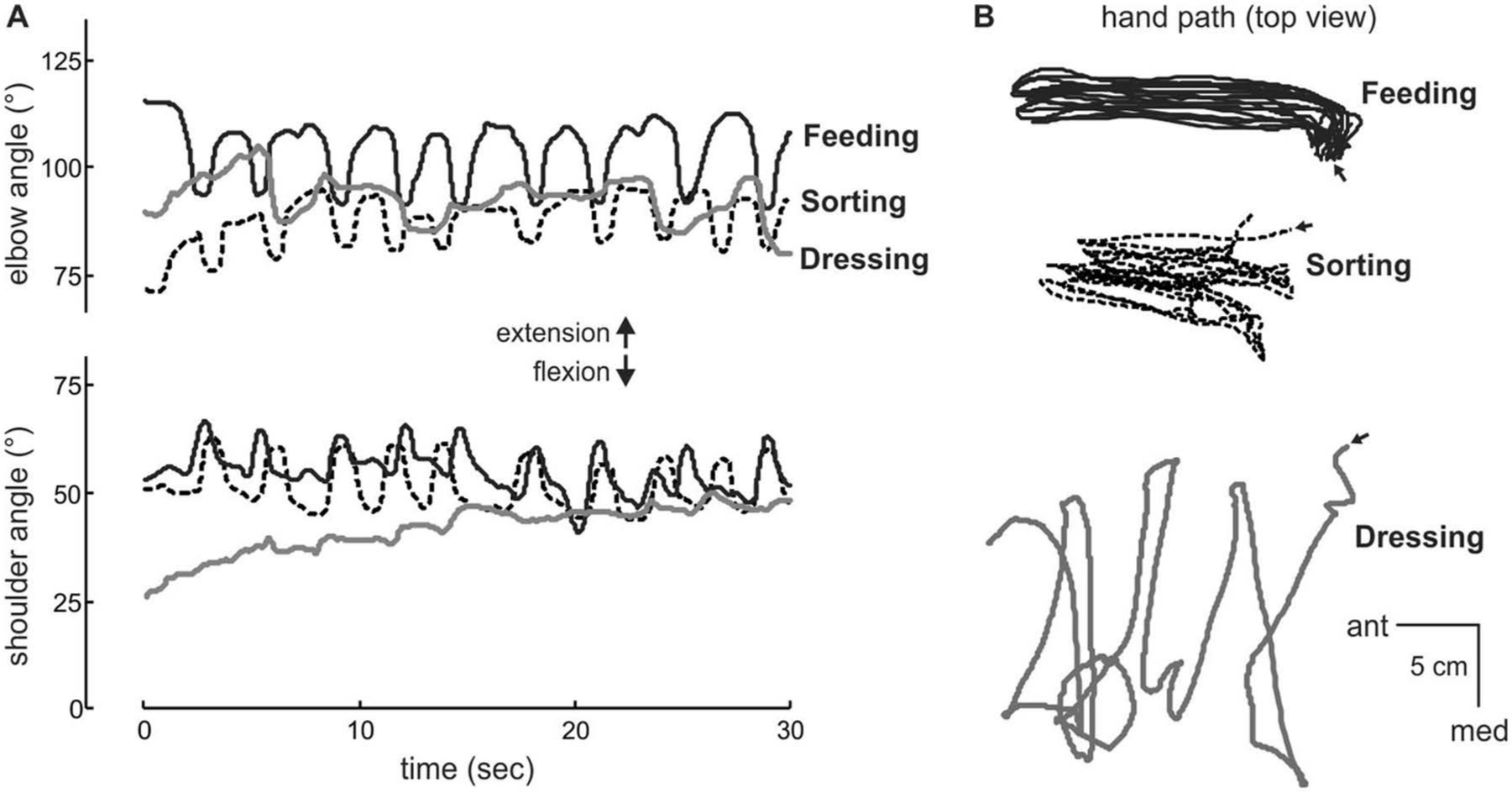
Spatiotemporal characteristics and training schedule of motor tasks: feeding (black), sorting (dashed), and dressing (gray). (A) Shoulder and elbow flexion angle and (B) hand path in the horizontal plane (top view; arrows indicate start of trial) during individual 30-s trials for a single participant. Note the similarity between feeding and sorting tasks in terms of movement kinematics. 3D position data of the upper-extremity segments were collected with an electromagnetic tracking system with 4 sensors (The Motion Monitor, Innovative Sports Training, Chicago, Illinois). Sensor locations were as follows: midsternum, upper arm, forearm, and back of hand. Kinematic data were collected at 50 Hz and low-pass filtered at 6 Hz using a second-order Butterworth filter.
Task automaticity: an additional probe of transfer
It is possible that over the course of training, participants’ motor performance on the feeding task would become more “automatic” with practice. This is based on the theory that the more learned a task is, the more automatic it is. 40 Thus, if the effects of training did transfer to the 2 untrained tasks, they too should become more automatic than prior to training. Automaticity is easily tested using a dual-task condition41-43 and may be operationalized by the amount of dual-task interference (ie, degradation in performance of at least 1 task under dual-task condition compared with performance by itself44,45). We recently tested whether dual-task conditions were feasible for detecting transfer in neurologically intact individuals 16 and found that both the trained and untrained tasks showed improved automaticity following a single session of training. To test whether similar effects occurred in this study following 5 sessions of training in individuals with chronic poststroke hemiparesis, we evaluated individuals’ motor performance under dual-task conditions at pretest and posttest in the same manner shown in Figure 1. This was to further probe the transfer of training.
In the dual-task condition, participants performed each motor task (feeding, sorting, and dressing) and a nonmotor auditory vigilance task concurrently. Prior to performing any motor task, all participants performed 2 trials of the auditory task in which they listened to recordings of 35- letter sequences. Each 30-letter sequence consisted of a random series of the same 4 letters (A, G, M, and O) at 1 Hz. Prior to each sequence, participants were instructed to pay attention to the number of times a target letter was heard. The target letter was A, G, M, or O and was changed for each trial. Immediately after each sequence, participants were asked to verbally report the number of times a target letter was heard. The primary measure of performance for the auditory task was the number of listening errors per trial, which was calculated as the difference between the reported and correct number of times the target letter was heard. This difference was expressed as an absolute value, such that a score of 1 error was the overestimating or underestimating of the number of target letters by 1. Our previous study 16 provides additional methodology details for this task.
Data Analysis
JMP 8.0 (SAS Institute Inc, Carey, North Carolina) was used for all statistical analyses. The Shapiro-Wilk test was used to verify normal distribution of each variable. To test whether training on the feeding task (1) improved feeding performance and (2) transferred to the sorting and dressing tasks, we used 1-way repeated-measures analyses of variance (ANOVAs) with time (pretest vs posttest) as the within-subject factor. Because the units of performance (ie, beans, blocks, and buttons) differed between tasks, separate ANOVAs were performed for the feeding, sorting, and dressing tasks. Significant differences between pretest and posttest performances of the untrained motor tasks would indicate that training had transferred.
To test whether the dual-task condition interfered with each task’s motor performance, we used 2 × 2 mixed-model ANOVAs, with time (pretest vs posttest) and condition (motor task only vs dual task) as within-subject factors. Separate ANOVAs were performed for the feeding, sorting, and dressing tasks.
All participants’ pretest and posttest motor performances were normalized to their unaffected side’s performance (normal = 100%). This normalization allowed for direct comparison of how much each task improved relative to other tasks. Improvement was calculated as normalized posttest performance minus normalized pretest performance. To determine whether more transfer occurred to a spatiotemporally similar task (sorting) compared with a different task (dressing), we used a 1-way repeated- measures ANOVA with task (feeding vs sorting vs dressing) as the within-subject factor. For all ANOVAs in this study, Tukey-Kramer honestly significant different tests46,47 were used for post hoc analysis when warranted based on the criterion for statistical significance (α = .05).
Results
Effects of Motor Training
As expected, feeding performance improved with training (Figure 4A). There was an effect of time on the number of successful repetitions per trial (F1,10 = 68.5; P < .0001), indicating that participants spooned more beans per trial after training (posttest) compared with before training (pretest; Figure 4B). Over the 5 days of training on the feeding task, the median number of successful repetitions per trial was 9. Thus, the number of repetitions achieved by each participant with the affected upper extremity per day was approximately 450 (9 repetitions/trial × 50 trials/d).
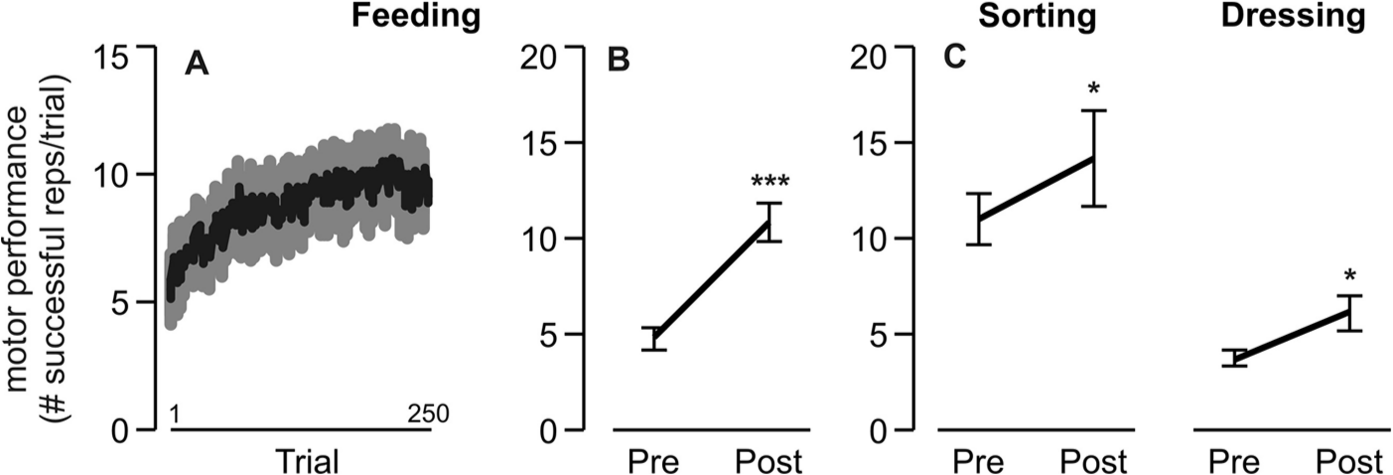
Effects of motor training: mean ± standard error motor performance on the (A) feeding task per trial over the course of 250 training trials; (B) feeding task before (pre) and after (post) training; and (C) untrained sorting and dressing tasks before (pre) and after (post) training. ***P < .0001; *P < .05.
Although participants did not train on the sorting or dressing tasks with their affected arm, performance on these tasks also improved from pretest to posttest (Figure 4C). There was an effect of time on the number of successful repetitions per trial in the sorting (F1,10 = 5.4; P < .05) and dressing (F1,10 = 8.2; P < .05) tasks.
Preserved Effects of Training Under Dual-Task Conditions
Pretest and posttest performance on all 3 motor tasks was also evaluated under dual-task conditions. Results presented here focus on the statistical comparisons that determined whether automaticity of the trained and untrained tasks improved. There was a significant effect of time on listening performance (F2,10 = 3.8; P < .05), such that listening errors were greater during pretest compared with listening only (post hoc P < .05; Figure 5A). This occurred even though participants were instructed to prioritize the auditory task. Instead, participants appeared to maintain their motor performance during pretest at the cost of the listening performance, as evidenced by no significant main effect of condition (single vs dual task) for the sorting (F1,10 = 1.0; P = .32) and dressing (F1,10 = 1.1; P = .31) tasks. Thus, prior to any motor training, the motor tasks appeared to disrupt the auditory task. By posttest, however, listening performance under dual-task conditions (Figure 5A) was comparable with to listening only (P = .57). Motor performance for all tasks under dual-task conditions also improved significantly after training on only 1 task (Figure 5B), as shown by the main effect of time (pretest vs posttest) for feeding (F1,10 = 187.07; P < .0001), sorting (F1,10 = 7.48; P < .01), and dressing (F1,10 = 16.27; P < .001) performances. Collectively, these results show that after training on 1 motor task, the automaticity of the untrained tasks improved as well, allowing for enough attention to be reallocated back to the auditory task under dual-task conditions with minimal interference.
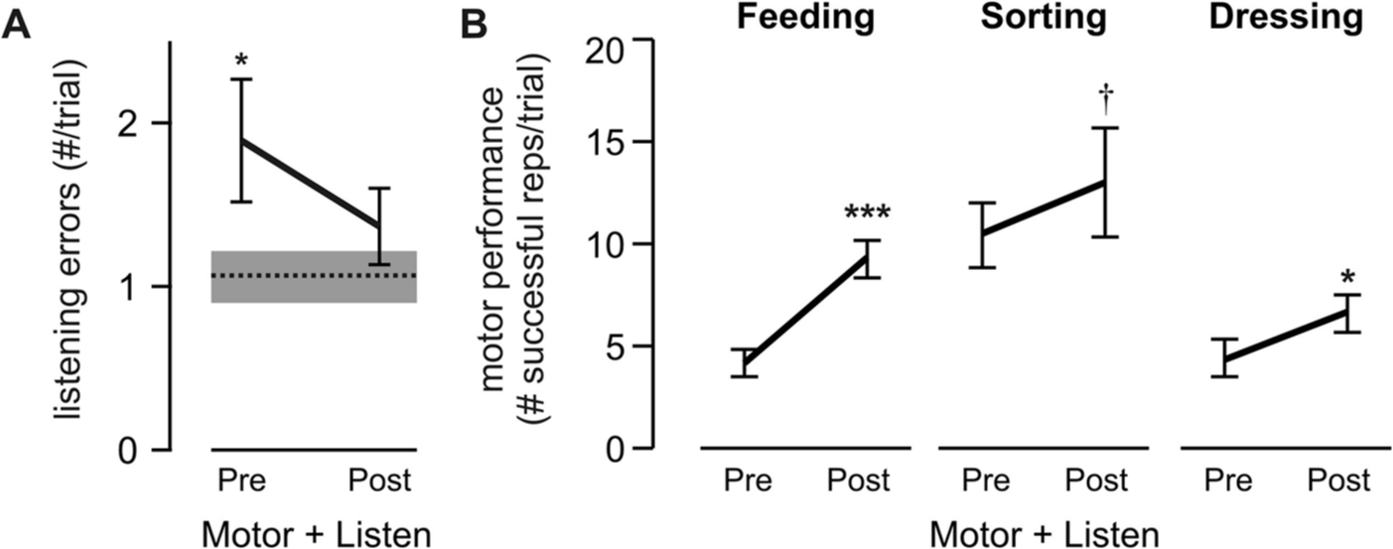
Preserved training effects under dual-task conditions: A. Mean listening error under dual-task conditions (Listen + Motor; collapsed across all motor tasks) before (pre) and after (post) motor training. Dashed line indicates mean listening error for the listening-only condition; gray box indicates standard error (SE). B. Mean motor performance per trial before (pre) and after (post) training for the trained (feeding) and the untrained (sorting, dressing) tasks under dual-task conditions (Listen + Motor). Error bars indicate SE. Note similarity in trend to Figure 3B. ***P < .0001; *P < .05; †P < .1.
Magnitude of Improvement Across Motor Tasks
The magnitude of improvement across tasks was examined with normalized scores (see Methods). Figure 6A shows a participant in all 3 motor tasks at pretest and posttest. Not surprisingly, the trained feeding task improved the most. Although the untrained tasks (sorting and dressing) also improved, the amount of improvement was (1) comparable with and (2) less than that of the feeding task. This effect was consistent across participants (Figure 6B). There was a main effect of motor task (feeding vs sorting vs dressing) on the amount of improvement in motor performance (F2,10 = 9.38; P < .01). Post hoc analyses revealed that the trained feeding task showed more improvement compared with the untrained sorting (P < .01) and dressing (P < .05) tasks. The amounts of improvement on the 2 untrained tasks were not different from each other (P = .50).
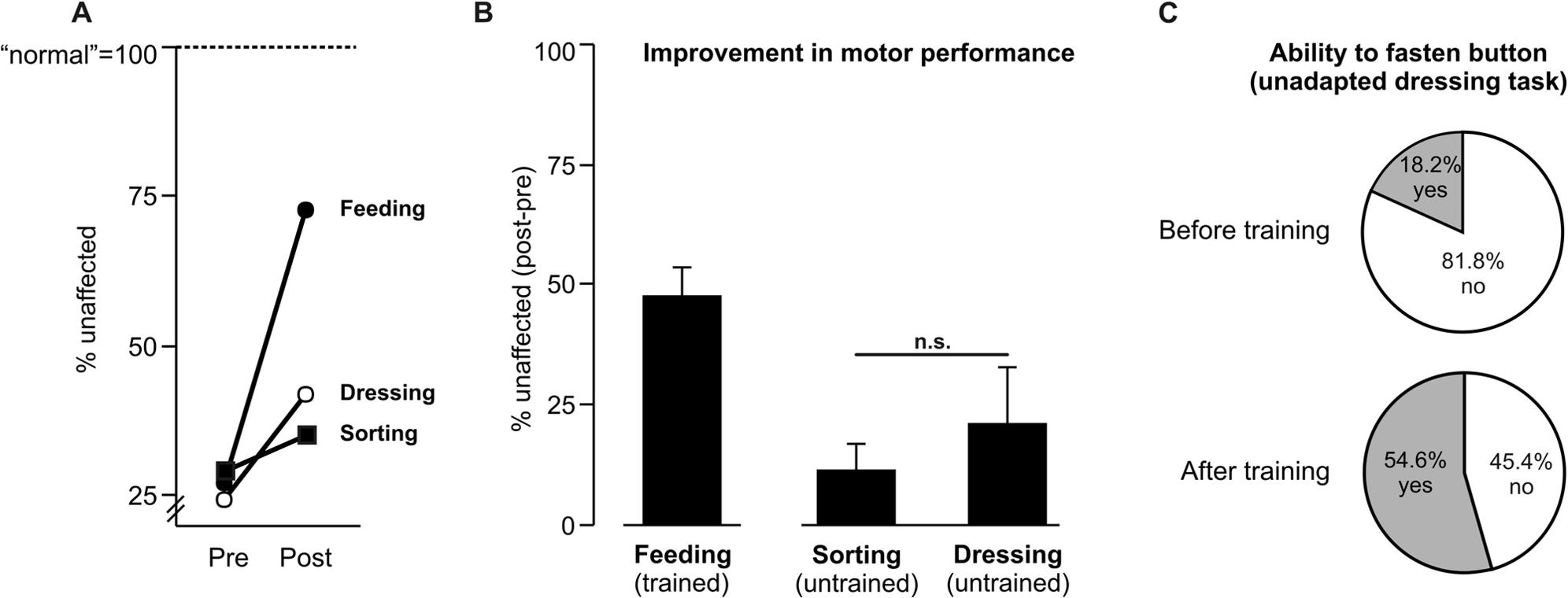
Magnitude of improvement as a result of transfer: A. Motor performance on all 3 tasks for a single participant with moderate hemiparesis (ARAT [Action Research Arm Test] score = 26) before (pre) and after (post) training, normalized to unaffected arm performance (100% = normal). B. Mean improvement in motor performance from pretest to posttest on all 3 motor tasks as a result of training only on one (feeding). The amount is expressed as percentage change relative to the unaffected side. Error bars indicate standard error. C. Change in ability to fasten buttons from before to after training on the dressing task. The percentage of participants is based on n = 11.
Prior to the experiment, participants were tested on whether they could fasten a single button within 30 s. Only 2 of 11 participants did so. After training only on the feeding task, more participants (6 of 11) were able to fasten >1 button within 30 s compared with before training (χ2(2, n=22) = 3.28; P < .10), indicating progression to a more challenging, unadapted version of the dressing task. These data are represented in Figure 6C, further illustrating improvement on a motor task that was substantially different from the one that was practiced during training.
Discussion
We tested whether 5 consecutive days of training on 1 motor task would transfer to 2 other untrained tasks in individuals with chronic mild to moderate hemiparesis poststroke. Results supported the first hypothesis that training on the feeding task would improve motor performance not only on that task but also on 2 other tasks that were not trained (sorting and dressing). Results did not, however, support the second hypothesis that the amount of transfer would be greater in the sorting task than in the dressing task because of its spatiotemporal similarity to the feeding task. Instead, the amount of transfer (ie, improvement from pretest to posttest) was comparable. Collectively, these results provide evidence for the effects of task-specific training after stroke to potentially generalize to a wider range of motor tasks beyond that which is practiced.
Given the increased prevalence of task-specific training in neurorehabilitation after stroke, 1 the question of whether the effects of training on 1 motor task will transfer to other unpracticed tasks is important. Numerous factors may limit exactly how many tasks can be practiced during standard therapy (eg, time, available space, and patient/clinician characteristics), but undoubtedly, the number and range of tasks needing practice exceed those that can be practiced feasibly within the allotted amount of rehabilitation.4,5 Thus, any task-specific training treatment plan must consider the amount of expected transfer in order to maximize its benefits.
Although the clinical importance of transfer is indisputable, little research has been done directly in (1) the clinical populations currently being treated with task-specific training and (2) the tasks currently being used within task-specific training. Previous studies in neurologically intact adults have demonstrated in experimental tasks with few degrees of freedom (ie, planar point-to-point reaching or sequential finger flexion with limb support) that the amount of transfer to novel conditions of the same task is relatively small.48-53 Nevertheless, this work has provided considerable evidence that the nervous system can and does generalize movement-related information. This work is, however, unable to predict the following: Does training on a more complex, functional task that recruits more degrees of freedom facilitate more transfer? Or does the diversity among movement patterns and goals minimize or even prevent any transfer? Prior to the current study, it was unclear whether transfer would be expected between more functional tasks involving many steps and degrees of freedom, that is, tasks that are practiced during task- specific training after stroke, such as sorting silverware or drinking from a glass.2,8,54 We recently tested this in a group of neurologically intact individuals and found that the effects of repetitive training on 1 functional task are transferrable to another functional task. 16 The tasks in this previous study were similar to the tasks performed in the current study. By demonstrating the effects of transfer between functional upper-extremity motor tasks as a result of repetitive training in individuals with chronic mild to moderate hemiparesis after stroke, we now provide novel quantitative findings that address both a specific population and a task set that are relevant clinically.
More Task Similarity, More Transfer?
In the current study, participants trained on 1 motor task (feeding) but were tested on 2 other untrained motor tasks (sorting and dressing) before and after training. The sorting task was relatively similar to the feeding task in terms of movement kinematics, whereas the dressing task was not (Figure 3A). Although we expected that the degree of similarity would predict the amount of transfer between tasks,55-57 we found that the sorting and dressing tasks showed comparable improvement. Although the sample size for this study was small (n = 11), these novel findings may suggest that matching the spatiotemporal characteristics of tasks may not necessarily promote additional transfer. Moreover, the motor tasks had different movement goals. The goals of the feeding, sorting, and dressing tasks were to spoon beans, pick up blocks, and fasten buttons, respectively. Previous work has suggested that movements with similar motor goals share common adaptive structures,11,58 and although more transfer might be expected experimentally when the goals of tasks overlap, this study demonstrates that transfer can occur even when the goals are quite disparate. More research across a broader range of both upper- and lower-extremity motor tasks is needed to test the limits of transfer. Nevertheless, these results are encouraging because clinicians will often take an individualized approach when determining activities of interest and specific tasks to address during treatment sessions.8,59
More Task Practice, More Transfer?
We provide evidence that the benefits of a high, but relatively brief, dose of functional upper-extremity training (approximately 2250 repetitions over 5 days) can transfer to other untrained upper-extremity tasks that are markedly different from the task that was practiced. This is consistent with recent findings demonstrating that following stroke, high doses of task-specific locomotor training over a 6-week intervention also improved other lower-extremity tasks that were not practiced and that were functionally very different from the trained task. 60 Collectively, these findings support the idea that even after 1 or more years poststroke, transfer can and does occur as a result of training. It is likely that the generalized benefits in the 6-week intervention are in part a result of increased limb strength and/or coordination.60-62 The training in the current study was only for 5 days, and no significant changes in strength (ie, grip strength; Table 1) were observed. This suggests that the mechanism underlying transfer in the current study may be related more to neural reorganization rather than muscular conditioning, following high doses of functional activity over only a few days.
It is still unclear whether even higher doses of training will yield even more transfer. In this study, the median number of successful repetitions achieved per day of training on the feeding task was 450, which is comparable with that from other work in which high doses of task-specific upper-extremity training (average 322 repetitions/d 8 ) have yielded sustained improvements in clinically evaluated motor function. Future research in a larger sample is needed to determine whether and how the amount of transfer can be enhanced with more practice to maximize the functional benefits of a given intervention.
Conclusions
Results from this study suggest that the effects of upper-extremity task-specific training can transfer to other untrained tasks in individuals with chronic mild to moderate hemiparesis after stroke. Because the number and type of tasks that can be practiced are often limited within standard stroke rehabilitation, our findings will be useful for optimizing the design of task-specific training plans to maximize the generalization of training to other tasks that may also need improvement.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by National Institutes of Health R01HD055964, T32HD007434 to the Program in Physical Therapy at Washington University School of Medicine, and American Heart Association 10POST4140091.